Back to Journals » Vascular Health and Risk Management » Volume 12
International normalized ratio self-testing and self-management: improving patient outcomes
Authors Pozzi M, Mitchell J, Henaine AM, Hanna N, Safi O, Henaine R
Received 25 May 2016
Accepted for publication 12 August 2016
Published 12 October 2016 Volume 2016:12 Pages 387—392
DOI https://doi.org/10.2147/VHRM.S85031
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Matteo Pozzi,1 Julia Mitchell,2 Anna Maria Henaine,3 Najib Hanna,4 Ola Safi,4 Roland Henaine2
1Department of Adult Cardiac Surgery, “Louis Pradel” Cardiologic Hospital, Lyon, France; 2Department of Congenital Cardiac Surgery, “Louis Pradel” Cardiologic Hospital, Lyon, France; 3Clinical Pharmacology Unit, Lebanese University, Beirut, Lebanon; 4Pediatric Unit, “Hotel Dieu de France” Hospital, Saint Joseph University, Beirut, Lebanon
Abstract: Long term oral anti-coagulation with vitamin K antagonists is a risk factor of hemorrhagic or thromebomlic complications. Periodic laboratory testing of international normalized ratio (INR) and a subsequent dose adjustment are therefore mandatory. The use of home testing devices to measure INR has been suggested as a potential way to improve the comfort and compliance of the patients and their families, the frequency of monitoring and, finally, the management and safety of long-term oral anticoagulation. In pediatric patients, increased doses to obtain and maintain the therapeutic target INR, more frequent adjustments and INR testing, multiple medication, inconstant nutritional intake, difficult venepunctures, and the need to go to the laboratory for testing (interruption of school and parents’ work attendance) highlight those difficulties. After reviewing the most relevant published studies of self-testing and self-management of INR for adult patients and children on oral anticoagulation, it seems that these are valuable and effective strategies of INR control. Despite an unclear relationship between INR control and clinical effects, these self-strategies provide a better control of the anticoagulant effect, improve patients and their family quality of life, and are an appealing solution in term of cost-effectiveness. Structured education and knowledge evaluation by trained health care professionals is required for children, to be able to adjust their dose treatment safely and accurately. However, further data are necessary in order to best define those patients who might better benefit from this multidisciplinary approach.
Keywords: oral anticoagulation, vitamin K antagonists, international normalized ratio, INR self-management, INR self-testing
Introduction
Long-term oral anticoagulation with vitamin K antagonists could display the risk of hemorrhagic or thromboembolic complications. The occurrence of these potentially life-threatening complications depends on the accuracy of oral anticoagulant treatment. A periodic laboratory testing of international normalized ratio (INR) and a subsequent dose adjustment are therefore mandatory.
Long-term oral anticoagulation is a public health concern as, for instance, ~1% of the French population requires vitamin K antagonists. Moreover, it was associated with the highest rate of hospitalization due to iatrogenic effects in France during 2007.1 Several studies proposed guidelines for administrating and monitoring oral anticoagulation with vitamin K antagonists in children,2 with many difficulties in their use in this population especially in infants under the age of 12 months. Different reasons could explain this problem: the lack of patients’ education, the complex pharmacokinetics and drug interactions of vitamin K antagonists, the need for continuous monitoring and dose adjustments, and patients’ compliance.3
The use of home testing devices to measure INR has been suggested as a potential way to improve the comfort and compliance of the patients and their families, the frequency of monitoring and, finally, the management and safety of long-term oral anticoagulation. Indeed, current practice guidelines suggest the strategy of self-management for patients treated with vitamin K antagonists who are motivated and can demonstrate competency in self-management strategies, including the self-testing equipment (Class IIb).4
In pediatric patients, increased doses to obtain and maintain the therapeutic target INR, more frequent adjustments and INR testing, multiple medication, inconstant nutritional intake, difficult venepunctures, and the need to go to the laboratory for testing (interruption of school and parents work attendance) highlight these difficulties.5 The purpose of this section of our paper is to review the most relevant published studies of self-testing and self-management of INR for adult patients and children on oral anticoagulation.
Methods
We considered only randomized controlled trials comparing the effects and the clinical outcomes of self-testing or self-management of oral anticoagulation therapy with standard monitoring and care, including personal physicians and anticoagulation hospitals or clinics. We included studies focusing on adult patients and children on oral anticoagulation therapy irrespective of the indication for treatment.
Results
In the adult population, we identified 20 published randomized controlled trials that met the inclusion criteria (Table 1). Fourteen trials included patients on oral anticoagulant treatment for any indication.6–19 Four trials considered only patients on lifelong oral anticoagulation after heart valve replacement with a mechanical prosthesis.20–23 Two trials included only patients on long-term anticoagulation for atrial fibrillation.24,25 Twelve trials analyzed the strategy of self-management6,8,10,12–15,17–19,21,25 while seven trials the strategy of self-testing.7,11,16,20,22–24 Gadisseur et al reported the results of both self-management and self-testing.9
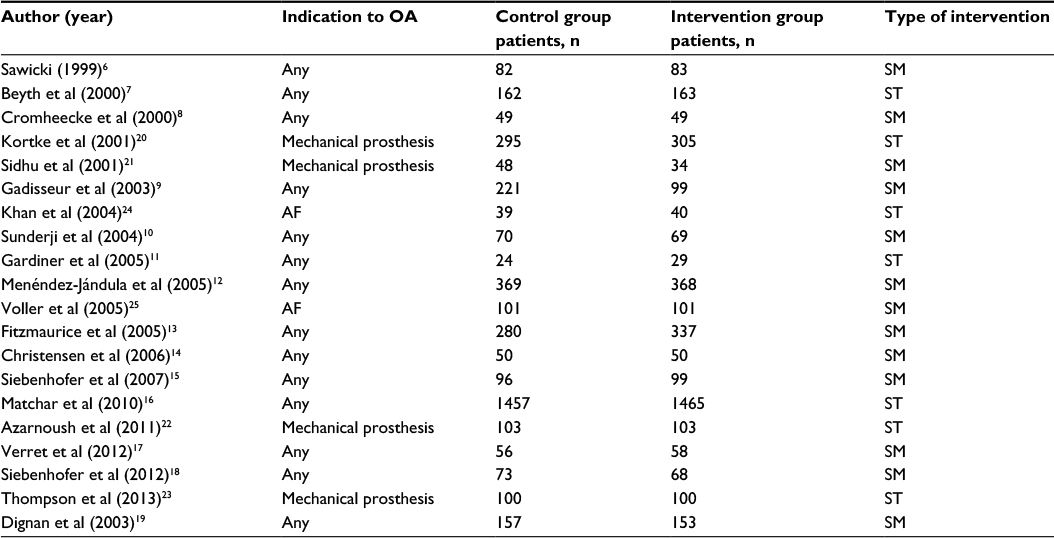 | Table 1 Most relevant published randomized controlled trials reporting self-testing and self-management of oral anticoagulation Abbreviations: AF, atrial fibrillation; OA, oral anticoagulation; SM, self-management; ST, self-testing. |
In the pediatric population, we identified only one randomized controlled trial that met the inclusion criteria.26 Jones et al in 2011 published a review of the literature concerning oral anticoagulation therapy in children, and they demonstrated that time in therapeutic range was from 39% to 81% but they did not describe randomized trials of either self-testing or self-management.27
Clinical effectiveness
The best way to evaluate the clinical efficacy and safety of self-testing and self-management is the control of the anticoagulant effect. The simplest indicators of the anticoagulant effect are the mean INR within the target range and the mean time spent within the target range. Owing to our review of the literature, nine trials reported mean INR within the target range.6,8–10,12,15,20,21,25 Every single trial showed a better INR control in the self-testing or self-management group but this improvement was statistically significant only in five trials.12,15,20,21,25 Improvements ranged from 3% to 17% (Table 2). Moreover, 14 trials analyzed the mean time spent within the INR target range (Table 3).7,9–17,21–24 Among these trials, 12 documented an improvement in the self-testing or -monitoring group,7,9,10,13–17,21–24 but the statistical significance was reached only in five trials.7,15,16,21,22 Finally, two trials did not show a beneficial effect in the intervention group.11,12
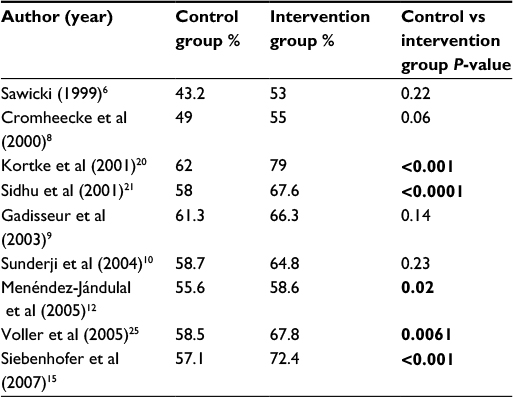 | Table 2 Mean INR within target range Note: Bold indicates statistical significance (P-value <0.05). Abbreviation: INR, international normalized ratio. |
 | Table 3 Mean time spent within INR target range Note: Bold indicates statistical significance (P-value <0.05). Abbreviations: INR, international normalized ratio; NS, not significant. |
Even if self-testing or self-management of oral anticoagulation is more effective or, at least, as effective as conventional care management, some authors argued against the correlation between improvement of INR control and decrease in major complications and call into serious question the usefulness of evaluating the safety of oral anticoagulation by using the percentage of mean INR and/or time within target range.12
The use of point-of-care devices for routine INR measurements has demonstrated safety, reliability, and effectiveness in infants and children requiring long-term oral anticoagulation therapy.28,29
Baumann et al in the EMPoWarMENT study26 have studied 28 wafarinized children performing self-testing for >3 months and randomized them to self-testing at home or self-management. The mean age was 10 years,1–19 and 93% were followed during 12 months. Mean number INR test over the study was around 22 either for self-testing or self-management. Time in therapeutic range was 77% for self-testing and 83% for self-management. INRs >5 were not related to warfarin dosing decision but to unexpected illness. Patients with self-management made dose decisions consistent with the guidelines in 90% of time.
Clinical benefits
The ideal endpoint of oral anticoagulation therapy studies is the evaluation of major complications. However, the reduction of oral anticoagulation-related complications – namely, bleeding and thromboembolic events – as a consequence of a better control of the anticoagulant treatment (as discussed earlier) is still a matter of debate.
When we take into consideration previous reviews of the literature calculating the overall effect size, there is general agreement on the reduction of thromboembolic complications determined by self-testing or self-management. Overall, these strategies show a 50% reduction of thromboembolic complications as compared to the control group.3,30,31
Conversely, the analysis of bleeding complications is more challenging. Heneghan et al found a significant one-third reduction of hemorrhagic complications in their review published in 2006,3 but other investigators did not.30,31 These different conclusions should probably be explained by a nonhomogeneous definition of major and minor hemorrhagic complications used in every report.
Finally, the same consideration could be done to the analysis of mortality. In fact, Heneghan et al found different results in their reviews published in 2006 and 2012.3,30 In the former, there was a significant reduction of overall mortality in the self-testing/ self-management group,3 while in the latter the difference was not statistically significant.30 The relative weight of oral anticoagulation control, thromboembolic complications, and bleeding in determining overall mortality is difficult to estimate and other factors may participate in the outcome of patients’ population.
Previous studies in children have shown a rate of bleeding ranging from 0.5% to 1.7% with oral anticoagulation therapy, with only one death reported related to the patient anticoagulation therapy;32 only two prospective studies have reported thromboembolic events with a rate under 2% and 10% per patient year.
In the EMPoWarMENT study, there were no hemorrhagic or thromboembolic events, and baseline time in therapeutic range for the self-monitoring group was less than the self-testing group due to poor adherence in four patients.27 As an answer, it has been now well demonstrated that the ability of parents to use point-of-care monitor and parental knowledge is the major criterion for clinical effectiveness and benefits.
Quality of life assessment
The success of an effective oral anticoagulation could be also evaluated with the treatment-related quality of life. Our review of the literature identified six trials that assessed quality of life outcomes.6,8,16,17,18,24
Sawicki et al evaluated at baseline and 6-month follow-up the treatment-related quality of life using a structured questionnaire containing 40 items.6 The 40 items covered five topics: general treatment satisfaction, self-efficacy, strained social network, daily hassles, and distress. General treatment satisfaction and daily hassles scores improved in the self-management group and remained unchanged in the routine care group. The scores of self-efficacy and distress improved in both groups but improved significantly more in the self-management group. The intervention had no significant effect on the strained social network scores. Interestingly, the general treatment satisfaction scores displayed the most pronounced improvement. Other investigators used the same structured questionnaire in order to perform a self-perceived assessment of the quality of care.8,17 As previously outlined, there were significant differences in all five categories of the questionnaire in favor of the self-management group: scores for general treatment satisfaction and self-efficacy were higher in the self-management group whereas the score for daily anxieties, distress, and strain were significantly lower. Moreover, Matchar et al evaluated patients’ satisfaction with anticoagulation, measured with the Duke Anticoagulation Satisfaction Scale, and quality of life, measured with the Health Utilities Index Mark.3,16
At 2 years (the minimum duration of follow-up), patient satisfaction with anticoagulation as measured by the Duke Anticoagulation Satisfaction Scale was greater in the self-testing group than in the clinic-testing group and a cumulative gain in health utilities according to the Health Utilities Index Mark 3 was noted in the self-testing group as compared with the clinic-testing group. Finally, Siebenhofer et al focused attention on elderly patients and found a pronounced improvement in general treatment satisfaction after participation in the self-management program.18
Conversely, Khan et al did not find any difference in quality of life measurements and health beliefs about warfarin between the control and self-monitoring groups using the 36-item United Kingdom Short Form Health Survey and European Quality of Life questionnaire.24
Two main studies have described the quality of life in children on home INR self-testing or self-management.33,34 KIDCLOT-PAC-QL© was the first preliminarily validated inventory to assess quality of life in anticoagulated children; it determined confounders to therapy and may facilitate partnership in care.33 In 2013, Newall et al tried to evaluate the impact of a home INR self-testing on the quality of life of children and their families. In all, 55 parents and 35 children participated; time in therapeutic range was 71%, and parents reported statistically significant improvement in quality of life for themselves, their family, and their child.34
Cost-effectiveness evaluation
Our review identified only one trial performing a costs evaluation.16 In this study, costs were higher in the self-testing group but not significantly different from those in the clinic-testing group (difference = $1,249; P=0.32).
Only one study has been found in the pediatric population as well.35 The home monitoring saved a total of 1 hour and 19 minutes per INR test and has a cost saving to society of $66.83 per INR test compared to traditional care incorporating health sector costs, travel expenses, and lost time.
Discussion
The self-testing and self-management of INR during oral anticoagulation is safe and effective and provides an accurate control of the anticoagulant treatment. Portable devices offer patients a more frequent and regular control of INR, thus reducing the intensity and frequency of supratherapeutic and subtherapeutic values. In fact, it has been demonstrated that there is a linear relationship between the frequencies of INR testing and quality of oral anticoagulation.36
Nevertheless, this accurate control of oral anticoagulation does not automatically translate into a substantial reduction of major complications. In the largest randomized clinical trial – THINRS (The Home INR Study) – weekly home INR testing did not reduce the aggregate outcome of stroke, major bleeding, or death as compared to monthly clinic INR testing.16
In contrast, there is a general agreement in the amelioration of the quality of life provided by the self-testing or self-management of INR. In fact, from a theoretical standpoint, patients should perform their INR measurements in the same laboratory in order to reduce the inter-laboratory variability, which can span from 10% to 30%.37 This dependence from the same laboratory could represent a major limitation of patients’ personal or professional daily activities. Self-testing or self-management of oral anticoagulation might effectively face this limitation and this is clearly witnessed by a global improvement of general treatment satisfaction as compared to standard care.6,8,16–18,24
A structured teaching program is however of outmost importance and plays a key role in self-strategies of oral anticoagulation. This is even more important in children, elderly, or low-level education or social status patients.
Limitations
Our review displays of course several limitations. Firstly, although comprehensive, we could have potentially missed some published studies. Moreover, the analysis of published data was not performed in a statistical manner and without any stratification according to the indications, frequency of tests or the length of the anticoagulant treatment, and different models of standard routine care. Finally, we did not take into consideration the type of education and training and the reasons and rate of dropout of the self-testing/self-management group.
Conclusion
The present review article reported that self-testing and self-management for INR control provided a better control of the anticoagulant effect and improved patients’ and their family quality of life. These findings would be very useful in the actual clinical setting.
And the reviewers would expect that the system and procedure of self-testing and self-management for INR control would evolve to be more user-friendly, and hope that especially in child patients, the novel anticoagulant therapy would be innovated to a stage wherean INR control would not necessary.
They are valuable and effective strategies of INR control. Despite an unclear relationship between INR control and clinical effects, these self-strategies provide a better control of the anticoagulant effect, improve patients’ and their family quality of life, and are an appealing solution in term of cost-effectiveness. For children, structured education and knowledge evaluation by trained health care professionals, children, and their caregivers appear to be able to adjust their dose treatment safely and accurately. Further data are however necessary in order to best define those patients who might better benefit from this multidisciplinary approach.
Disclosure
The authors report no conflicts of interest in this work.
References
Haute Autorité de Santé. Evaluation de l’auto surveillance de l’INR chez les patients adultes traités par antivitamines K; 2008. Available from: http://www.has-sante.fr/portail/upload/docs/application/pdf/2009-02/rapport_inr_2009-02-11_11-34-20_386.pdf. Accessed February 11, 2009. | ||
Monagle P, Michelson AD, Bovill E, Adams M, Ginsberg J, Freedom R, Williams W. Oral anticoagulation therapy in paediatric patients: a prospective study. Thromb Haemost. 1994;71(3):265–269. | ||
Heneghan C, Alonso-Coello P, Garcia-Alamino JM, Perera R, Meats E, Glasziou P. Self-monitoring of oral anticoagulation: a systematic review and meta-analysis. Lancet. 2006;367(9508):404–411. | ||
Holbrook A, Schulman S, Witt DM, et al; American College of Chest Physicians. Evidence-based management of anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e152S–e184S. | ||
Mariana M. Bonduel: oral anticoagulation therapy in children. Thromb Res. 2006,118(1),85–94. | ||
Sawicki PT. A structured teaching and self-management program for patients receiving oral anticoagulation: a randomized controlled trial. working group for the study of patient self-management of oral anticoagulation. JAMA. 1999;281(2):145–150. | ||
Beyth RJ, Quinn L, Landefeld CS. A multicomponent intervention to prevent major bleeding complications in older patients receiving warfarin. A randomized, controlled trial. Ann Intern Med. 2000;133(9):687–695. | ||
Cromheecke ME, Levi M, Colly LP, et al. Oral anticoagulation self-management and management by a specialist anticoagulation clinic: a randomised cross-over comparison. Lancet. 2000;356(9224):97–102. | ||
Gadisseur AP, Breukink-Engbers WG, van der Meer FJ, van den Besselaar AM, Sturk A, Rosendaal FR. Comparison of the quality of oral anticoagulant therapy through patient self-management and management by specialized anticoagulation clinics in the Netherlands: a randomized clinical trial. Arch Intern Med. 2003;163(21):2639–2646. | ||
Sunderji R, Gin K, Shalansky K, et al. A randomized trial of patient self-managed versus physician-managed oral anticoagulation. Can J Cardiol. 2004;20(11):1117–1123. | ||
Gardiner C, Williams K, Mackie IJ, Machin SJ, Cohen H. Patient self-testing is a reliable and acceptable alternative to laboratory INR monitoring. Br J Haematol. 2005;128(2):242–247. | ||
Menéndez-Jándula B, Souto JC, Oliver A, et al. Comparing self-management of oral anticoagulant therapy with clinic management: a randomized trial. Ann Intern Med. 2005;142(1):1–10. | ||
Fitzmaurice DA, Murray ET, McCahon D, et al. Self management of oral anticoagulation: randomised trial. BMJ. 2005;331(7524):1057. | ||
Christensen TD, Maegaard M, Sørensen HT, Hjortdal VE, Hasenkam JM. Self-management versus conventional management of oral anticoagulant therapy: a randomized, controlled trial. Eur J Intern Med. 2006;17(4):260–266. | ||
Siebenhofer A, Rakovac I, Kleespies C, Piso B, Didjurgeit U. Self-management of oral anticoagulation in the elderly: rationale, design, baselines and oral anticoagulation control after one year of follow-up. A randomized controlled trial. Thromb Haemost. 2007;97(3):408–416. | ||
Matchar DB, Jacobson A, Dolor R, et al. Effect of home testing of international normalized ratio on clinical events. N Engl J Med. 2010;363(17):1608–1620. | ||
Verret L, Couturier J, Rozon A, et al. Impact of a pharmacist-led warfarin self-management program on quality of life and anticoagulation control: a randomized trial. Pharmacotherapy. 2012;32(10):871–879. | ||
Siebenhofer A, Hemkens LG, Rakovac I, Spat S, Didjurgeit U; SPOG 60+ Study Group. Self-management of oral anticoagulation in elderly patients - effects on treatment-related quality of life. Thromb Res. 2012;130(3):e60–e66. | ||
Dignan R, Keech AC, Gebski VJ, Mann KP, Hughes CF; Warfarin SMART Investigators. Is home warfarin self-management effective? Results of the randomised Self-Management of Anticoagulation Research Trial. Int J Cardiol. 2013;168(6):5378–5384. | ||
Körtke H, Körfer R. International normalized ratio self-management after mechanical heart valve replacement: is an early start advantageous? Ann Thorac Surg. 2001;72(1):44–48. | ||
Sidhu P, O’Kane HO. Self-managed anticoagulation: results from a two-year prospective randomized trial with heart valve patients. Ann Thorac Surg. 2001;72(5):1523–1527. | ||
Azarnoush K, Camilleri L, Aublet-Cuvelier B, Geoffroy E, Dauphin C, Dubray C, De Riberolles C. Results of the first randomized French study evaluating self-testing of the International Normalized Ratio. J Heart Valve Dis. 2011;20(5):518–525. | ||
Thompson JL, Burkhart HM, Daly RC, Dearani JA, Joyce LD, Suri RM, Schaff HV. Anticoagulation early after mechanical valve replacement: improved management with patient self-testing. J Thorac Cardiovasc Surg. 2013;146(3):599–604. | ||
Khan TI, Kamali F, Kesteven P, Avery P, Wynne H. The value of education and self-monitoring in the management of warfarin therapy in older patients with unstable control of anticoagulation. Br J Haematol. 2004;126(4):557–564. | ||
Völler H, Glatz J, Taborski U, Bernardo A, Dovifat C, Heidinger K. Self-management of oral anticoagulation in nonvalvular atrial fibrillation (SMAAF study). Z Kardiol. 2005;94(3):182–186. | ||
Bauman ME, Black K, Baumann ML, Bruce AA, Kuhle S, Bajzar L, Massicotte MP. EMPoWarMENT: Edmonton paediatric wafarin self-management pilot study in children with primarily cardiac disease. Thromb Res. 2010;126(2):e110–e115. | ||
Jones S, Newall F, Manias E, Monagle P. Assessing outcome measures of oral anticoagulation management in children. Throm Res. 2011,127(2);75–80. | ||
Baumann ME, Conroy S, Massicotte MP. Point of care INR measurement in children requiring warfarin: what has been evaluated and future directions. Pedriatr Health. 2008;693(2):651–659. | ||
Newall F, Monagle P, Jonhston L. Home monitoring of oral anticoagulation therapy in children using CoagulChek ™ S point of care monitor and a robust education program. Thromb Res. 2006;118(5):587–589. | ||
Garcia-Alamino JM, Ward AM, Alonso-Coello P, Perera R, Bankhead C, Fitzmaurice D, Heneghan CJ. Self-monitoring and self-management of oral anticoagulation. Cochrane Database Syst Rev. 2010;14(4):CD003839. | ||
Heneghan C, Ward A, Perera R, et al. Self-monitoring of oral anticoagulation: systematic review and meta-analysis of individual patient data. Lancet. 2012;379(9813):322–334. | ||
Marzinotto V, Monagle P, Chan A, Adams M, Massicotte P, Leaker M. Capillary whole blood monitoring of oral anticoagulation in children in outpatient clinics and the home setting. Peadiatr Cardiol. 2000;21(4):347–352. | ||
Bruce AA, Baumann ME, Black K, Newton A, Legge L, Masicotte MP. Development and preliminary evaluation of the KIDCLOT-PAC-QL©: a new health-related quality of life measure for paediatric long term anticoagulation therapy. Throm Res. 2010;126(2)e116–e121. | ||
Jones S, Monagle P, Manias E, Bruce AA, Newall F. Quality of life assesment in children commencing home INR self-testing. Throm Res. 2013;132(1):37–43. | ||
Gaw JR, Crowley S, Monagle S, Jones S, Newall F. The economic costs of routine INR monitoring in infants and children examining point of care devices used within the home setting compared to traditional anticoagulation clinic monitoring. Thromb Res. 2013;132(1):26–31. | ||
Oral Anticoagulation Monitoring Study Group. Prothrombin measurement using a patient self-testing system. Am J Clin Pathol. 2001;115(2):280–287. | ||
Finck KM, Doetkott C, Miller DR. Clinical impact of interlaboratory variation in international normalized ratio determinations. Am J Health Syst Pharm. 2001;58(8):684–688. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.