")
Back to Journals » Clinical Ophthalmology » Volume 18
International Multicenter, Myopic and Myopic Astigmatism Femto LASIK, Customized by Automated Ray-Tracing Ablation Profile Calculation: A Postmarket Study
Authors Kanellopoulos AJ , Maus M, Bala C , Hamilton C, Lemonis S, Jockovich ME, Khoramnia R
Received 15 August 2023
Accepted for publication 26 January 2024
Published 20 February 2024 Volume 2024:18 Pages 525—536
DOI https://doi.org/10.2147/OPTH.S435581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Anastasios John Kanellopoulos,1,2,* Matthias Maus,3,* Chandra Bala,4,* Cody Hamilton,5,* Sissimos Lemonis,6,* Maria Elena Jockovich,5,* Ramin Khoramnia7,*
1LaserVision Ambulatory Surgical Unit, Athens, Greece; 2Department of Ophthalmology, NYU Grossman School of Medicine, New York City, NY, USA; 3Sehkraft Augenzentrum, Köln, Germany; 4PersonalEyes, Sydney, NSW, Australia; 5Alcon Vision, LLC, Fort Worth, TX, USA; 6Alcon Deutschland GmbH, Freiburg, Germany; 7Department of Ophthalmology, University of Heidelberg, Heidelberg, Germany
*These authors contributed equally to this work
Correspondence: Anastasios John Kanellopoulos, LaserVision Ambulatory Surgical Unit, An Thocha 17, Athens, 115 21, Greece, Tel +30 (210) 7472777, Fax + 30 (210) 7472789, Email [email protected]
Purpose: To assess the safety and efficacy of a customized ablation treatment (InnovEyes) to correct myopia and myopic astigmatism with femtosecond laser-assisted in situ keratomileusis (Femto LASIK).
Patients and Methods: In this prospective, nonrandomized, multicenter study, 113 patients (225 eyes) with preoperative myopia less than − 9.0 diopters (D) and astigmatism 0 to − 4.0 D (based on InnovEyes refraction) underwent wavefront, tomography, and biometry assessment using a single diagnostic device (InnovEyes sightmap). These data were imported and used unmodified by the InnovEyes algorithm to automatically calculate and optimize correction of lower- and higher‑order aberrations (HOAs) treated by the EX500 ablation profile. Visual acuity, refractive error, HOAs, and patient satisfaction were evaluated over 3 months.
Results: A total of 106 patients (212 eyes) completed the study and were included in the analysis. Mean preoperative manifest refraction spherical equivalent (MRSE) was − 3.38± 1.76 D. At Month 3, uncorrected distance visual acuity was 20/20 or better in 208/212 (98.1%) eyes, and it was the same as, or better than, the preoperative best-corrected distance visual acuity (CDVA) in 162/212 (76.4%) eyes; 76/212 (35.8%) eyes gained ≥ 1 line of CDVA. MRSE was within ± 0.5 D in 195/212 (92.0%) eyes. Additionally, 201/209 (96.2%) eyes had no change (defined as a change between − 0.1 μm and 0.1 μm, inclusive) in HOAs, and 105/106 (99.1%) patients reported to be satisfied with the results.
Conclusion: Customizing ray-tracing Femto LASIK with this platform appeared safe and effective in correcting myopic astigmatism and also achieved a significant percentage of eyes gaining lines of vision, potentially by addressing HOAs, along with a consistently high level of patient satisfaction.
Keywords: myopic astigmatism, higher-order aberrations, manifest refraction spherical equivalent, corrected distance visual acuity
Introduction
The goal of refractive surgery is to provide patients with the best possible visual performance after surgery, such as postoperative-uncorrected distance visual acuity (UDVA) equal to or better than preoperative best-corrected distance visual acuity (CDVA). To achieve this, accurate calculation methods are required during treatment planning. Standard laser-assisted in situ keratomileusis (LASIK) ablation profile‑planning methods do not routinely take into consideration the individual position and properties of the multiple optical elements of the eye,1 ie, anterior cornea, posterior cornea and pachymetry, anterior chamber depth, anterior surface of the crystalline lens, posterior surface of crystalline lens, and axial length.
The InnovEyes platform (Alcon, Fort Worth, TX, USA) automatically utilizes individual wavefront, tomography, and biometry diagnostic data captured by a single diagnostic device, the InnovEyes sightmap (Alcon, Fort Worth, TX, USA). These measurements are applied to generate the personalized virtual eye model, which is then used to further calculate lower-order aberrations (myopia with or without astigmatism) and higher-order aberrations (HOAs) via an automated ray-tracing algorithm.1 The algorithm uses Snell’s law to calculate the optical path of light rays as they pass through the eye and then simulates adjustment of the anterior surface of the cornea until it corresponds to the ideal target (eg, plane) wavefront; a customized ablation profile is generated at the planning station or the WaveLight EX500 excimer laser (Alcon, Fort Worth, TX, USA) to perform the femtosecond LASIK (Femto LASIK) procedure. The algorithm also provides an enhanced precompensation calculation that considers laser efficiency, corneal epithelial remodeling, and expected biomechanical changes.2 This new algorithm is an evolution of the established wavefront optimization3 and was designed based on empirical data of already treated patients by comparing the achieved versus the targeted ablation volume and topography. In addition to rotational symmetric aberration, the new precompensation now balances nonrotation aberrations for the specific correction considering the individual anticipated postoperative topography. The benefits are precise translation of the planned ablation decoupling correction of aberrations from inducing new aberration, as well as not increasing spherical aberration irrespective to the correction of sphere. All calculations are performed automatically, theoretically not requiring additional manual surgeon input in the treatment planning beyond validating these data. The InnovEyes sightmap is registered as a class IIb product and has been European Conformity–marked for clinical use since November 2019. It includes diagnostic options specifically and exclusively built to provide data for personalized and other ablations of the WaveLight platform, export to which is unique to InnovEyes sightmap. The InnovEyes platform has not yet been commercially launched.
An earlier manual version of the algorithm has been tested using separate diagnostic devices to acquire wavefront, tomography, and biometry data in patients with a mean preoperative manifest refraction spherical equivalent (MRSE) of −5.92±1.72 diopters (D); under these conditions, 93/111 (83.8%) eyes and 16/21 (76.2%) eyes achieved UDVA of 20/20 or better at 3 months and 12 months, respectively.4,5 In a separate study, InnovEyes sightmap and the InnovEyes algorithm have been tested clinically in a small cohort of patients, with 40/40 (100%) eyes achieving UDVA of 20/20 or better at 6 months.6
To evaluate potential benefits of InnovEyes customization, this study was designed to determine the safety and efficacy of the WaveLight EX500 excimer laser system for Femto LASIK correction, using this InnovEyes automated ablation customization in a prospective study involving several international centers and surgeons using a uniform protocol. The study investigated a wider array of functional endpoints and, for the first time, included a subjective assessment of patient satisfaction.
Materials and Methods
Study Design
This prospective, single-arm, multicenter, interventional study was conducted between July 2020 and September 2021 at four sites (two in Germany, one in Australia, and one in Greece) and registered with the German Clinical Trials Register (www.drks.de/drks_web/; ID: DRKS00020388). The study was conducted in accordance with the ethical principles contained within the Declaration of Helsinki. The protocol was reviewed and approved by an Independent Ethics Committee or Institutional Review Board at each site (Ärztekammer Nordrhein Ethik-Kommission and Ethikkommission der Medizinischen Fakultät Heidelberg, Germany; Bellberry HREC, Australia; Laser Vision Ethics Committee, Greece). Informed consent was obtained from every patient prior to the initiation of any study-specific procedures.
Eligible patients received bilateral InnovEyes customized Femto LASIK treatment and were followed for 3 months across a total of six visits (screening, surgery, Day 1, Week 1, Month 1, and Month 3).
All patients in the study were aged ≥21 years and were required to have: myopia up to −11.00 D, with or without astigmatism up to −4.50 D, with wavefront-measured spherical equivalent (SE) <−12.00 D at diameter of the optical zone = 4 mm; CDVA of 20/20−2 or better (≤0.04 logarithm of the minimum angle of resolution [logMAR]); <0.75 D MRSE difference between cycloplegic refraction and manifest refraction; <0.50 D MRSE difference between wavefront-measured refraction at 4 mm and subjective manifest refraction; and stable refraction (within ±0.50 D) as determined by MRSE for a minimum of 12 months prior to surgery, verified by consecutive subjective refractions, medical records, or prescription history. Patients were instructed not to wear contact lenses for ≥2 weeks (rigid or toric contact lenses) or 3 days (soft contact lenses) prior to the first refraction, to establish stability, and through the day of surgery. Patients were excluded from the study if they had ocular conditions (other than high myopia) that may have predisposed them to future complications (such as ectasia, history or evidence of active or inactive corneal disease, evidence of retinal vascular disease, keratoconus or keratoconus suspect, or glaucoma or glaucoma suspect by exam findings and/or family history), had undergone previous intraocular or corneal surgery, aimed to achieve monovision, or were pregnant or breastfeeding. Preoperative and calculated postoperative corneal pachymetry were also taken into consideration in patient selection.
Procedure
Site-specific standard of care for patients undergoing Femto LASIK procedures was followed before and after surgery. Aberrometry, biometry, wavefront refraction, and corneal tomography assessments were performed at the screening visit using the InnovEyes sightmap device. These data were imported into the InnovEyes ray-tracing algorithm, which generated a virtual eye model for each eye studied, from which a customized ablation profile was generated following ray-tracing calculations.1 Corneal flaps were created using a WaveLight FS200 femtosecond laser (Alcon, Fort Worth, TX, USA) or FEMTO LDV™ Z6 femtosecond laser (Ziemer Ophthalmic Systems, Port, Switzerland). InnovEyes Femto LASIK treatments were performed with the WaveLight EX500 excimer laser. All treated eyes were targeted for emmetropia with the automated InnovEyes-calculated customized ablation without nomogram adjustment.
Study Assessments
CDVA and UDVA were assessed using an Early Treatment Diabetic Retinopathy Study (ETDRS) chart. CDVA, UDVA, and photopic manifest refraction were assessed at Week 1, Month 1, and Month 3 visits; UDVA was also assessed at Day 1. InnovEyes sightmap assessments were performed at Month 1 and Month 3 visits. Month 3 data are presented. All patients were provided a satisfaction-related 6-question subset of questions from the US Food and Drug Administration (FDA) Patient-Reported Outcomes With LASIK (PROWL) questionnaire at Month 3:
1) What is your current satisfaction with result of LASIK surgery?
2) Did you achieve the goals you had for LASIK surgery?
3) Are you happy or unhappy you had LASIK surgery?
4) If you could do it all over again, would you decide to have LASIK performed?
5) Would you recommend LASIK surgery to a friend or family member?
6) Why would you not have LASIK done again or not recommend it to a friend or family member?
Efficacy Endpoints
The primary efficacy endpoint was the percentage of eyes with absolute MRSE within ±0.25 to ±1.00 D at Month 3. Additionally, five exploratory efficacy endpoints were also assessed: percentage of eyes with UDVA of 20/12.5 through 20/25 or better at postoperative visits; percentage of eyes that achieved UDVA equal to or better than the preoperative CDVA; percentage of eyes with CDVA of 20/10 through 20/20 at postoperative visits; percentage of eyes that achieved manifest refraction cylinder within ±0.25, ±0.50, and ±1.00 D at Month 3 of those treated for astigmatism >1.00 D; preoperative and Month 3 mean HOAs (coma, trefoil, spherical aberration, root mean square of HOAs [RMSh] = total HOAs).
Safety Endpoints
The primary safety endpoint was the percentage of eyes with any serious, non–flap-related ocular adverse event (AE) at postoperative visits. The following five supportive additional safety endpoints were also evaluated: percentage of eyes with CDVA worse than 20/40 (for eyes with preoperative CDVA of 20/20 or better); percentage of eyes with loss of ≥2 lines of CDVA versus preoperative values; percentage of eyes with a manifest refractive astigmatism increase of >2.00 D of absolute cylinder versus preoperative refraction; percentage of eyes experiencing ocular AEs; and summary of patient satisfaction survey at Month 3.
Statistical Analysis
This study did not include any hypothesis testing of the efficacy or safety endpoints. The formal sample size calculation was based on a safety detection rate of 3%. The planned analyses were based on recommendations from the American National Standards Institute (ANSI) Z80.11−2021 (R2017) and International Organization for Standardization (ISO) 14155:2011 standards.7,8 Astigmatism vector analysis was performed using AstigMATIC software (available for download from http://www.lasikmd.com/media/astigmatic).9
Results
Demographics and Other Baseline Characteristics
The study enrolled 136 patients. Following screening, 113 patients (225 eyes) underwent surgery. The full analysis set (FAS) consisted of 111 patients (222 eyes). One patient successfully treated bilaterally was excluded from the FAS due to pregnancy at screening, which was not reported until the patient was seen at the Month 3 postoperative visit. Another patient had an AE in the first eye and was excluded from the FAS due to unsuccessful surgery in the first eye. Additionally, 5 patients (10 eyes) discontinued the study after surgery due to being lost to follow-up or other causes. A total of 106 patients (212 eyes) completed the study and were included in the analysis.
Patients had a mean age of 30.3 years, and 64/112 (57.1%) patients were female. The majority of eyes fell into the categories of manifest refraction sphere values of >−1.0 to ≤−4.0 D (145/222 [65.3%] eyes) and manifest refraction cylinder of 0.0 to ≤−1.00 D (179/222 [80.6%] eyes). Demographics and baseline characteristics are summarized in Table 1. The mean preoperative RMSh was 0.104±0.033 μm.
 |
Table 1 Demographics and Baseline Characteristics |
Efficacy Results
Visual and refractive outcomes are shown in the standardized graphs in Figure 1. At Month 3, UDVA was 20/20 or better in 208/212 (98.1%) eyes and CDVA was 20/20 or better in 222/222 (100%) eyes (Figure 1A). Mean UDVA was −0.126 logMAR, which represented a mean change of −1.019 logMAR from baseline. At Month 3, 162/212 (76.4%) eyes had equivalent or better postoperative UDVA than preoperative CDVA, with most eyes either having no change (148/212 [69.8%] eyes) or an improvement (56/212 [26.4%] eyes) in lines of visual acuity (Figure 1B). Mean logMAR CDVA at all postoperative visits was better than preoperative mean CDVA; at Month 3, mean CDVA was −0.150 logMAR. Post hoc analysis of lines of change from preoperative CDVA to Month 3 CDVA showed that 135/212 (63.7%) eyes had no change, 68/212 (32.1%) gained 1 line, 8/212 (3.8%) gained 2 lines, and 1/212 (0.5%) lost 1 line of visual acuity (Figure 1C).
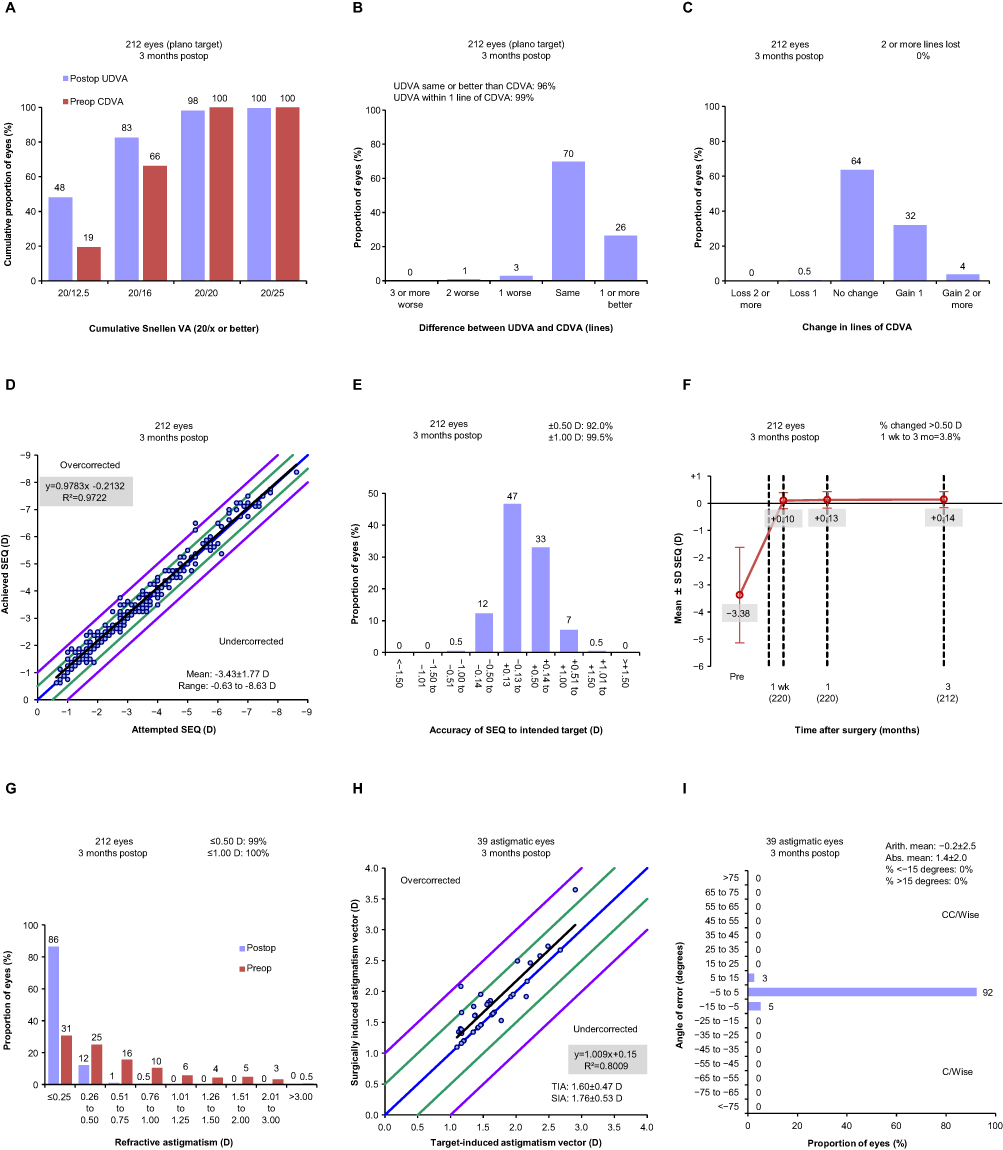 |
Figure 1 Refractive and visual outcomes at Month 3. Abbreviations: Abs, absolute; Arith, arithmetic; CDVA, corrected distance visual acuity; C/Wise, clockwise; CC/Wise, counterclockwise; D, diopter; logMAR, logarithm of the minimum angle of resolution; mo, month; MRSE, manifest refraction spherical equivalent; postop, postoperative; preop, preoperative; SD, standard deviation; SEQ, spherical equivalent refraction; SIA, surgically induced astigmatism; TIA, target-induced astigmatism; UDVA, uncorrected distance visual acuity; VA, visual acuity; wk, week. Notes: (A) Cumulative postoperative UDVA compared with preoperative CDVA. (B) Line difference between postoperative UDVA and preoperative CDVA. A line is 0.1 logMAR. (C) Change in lines between preoperative and postoperative CDVA. (D) Attempted versus achieved spherical equivalent refraction. (E) Spherical equivalent refraction accuracy. (F) MRSE stability at screening, Week 1, Month 1, and Month 3. (G) Refractive astigmatism. (H) Target‑induced astigmatism versus surgically induced astigmatism. (I) Refractive astigmatism angle of error. For panels showing the proportion of eyes, for clarity, numbers ≥1 are displayed as integers and those <1 are shown to 1 decimal place, and in all cases, the total is 100%. |
At Month 3, of 212 eyes, absolute MRSE within ±0.25, ±0.50, or ±1.00 D was observed in 157 (74.1%), 195 (92.0%), and 211 (99.5%) eyes, respectively (Figure 1E). There was a very strong correlation between attempted and achieved SE refraction (R2=0.972, Figure 1D). MRSE had a high level of stability postoperatively, with a mean change of 0.033 D from Week 1 to Month 1, and 0.010 D from Month 1 to Month 3 (Figure 1F). Of the 39 eyes treated for preoperative astigmatism >1.00 D, the number of eyes achieving manifest refraction cylinder within ±0.25 D, ±0.50 D, and ±1.00 D was 32 (82.1%), 37 (94.9%), and 39 (100%), respectively, at Month 3. Across the whole population of patients, 209/212 (99%) eyes had refractive astigmatism within ±0.50 D (Figure 1G). The relationship between target-induced astigmatism and surgically induced astigmatism and the refractive astigmatism angle of error are shown in Figure 1H and I, respectively. Astigmatism vector analyses are shown in Figure 2.
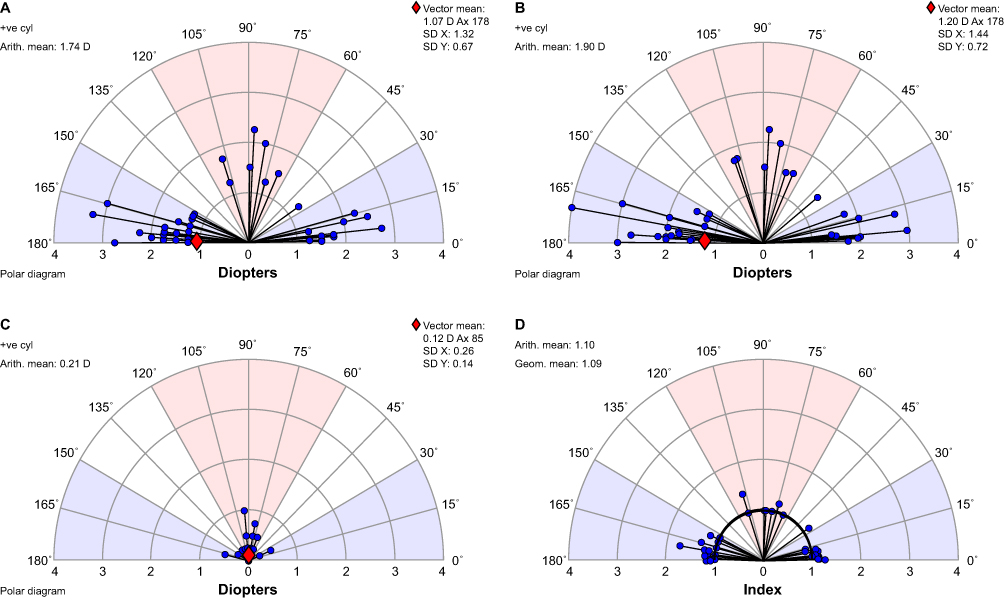 |
Figure 2 Astigmatism vector analyses at Month 3. Abbreviations: Arith, arithmetic; Ax, axis; cyl, cylinder; D, diopter; Geom, geometric; SD, standard deviation; +ve, positive. Notes: Vector analyses of (A) target-induced astigmatism, (B) surgically induced astigmatism, (C) difference vector, and (D) correction index. |
HOAs were calculated from the coefficient values collected from the InnovEyes sightmap and adjusted to an optical zone of 4 mm (Table 2). Analysis of the number of eyes with a change from baseline in HOAs (RMSh) by category of increase in total HOAs, decrease in total HOAs, and no change (defined as a change between −0.1 µm and 0.1 µm, inclusive) showed 201/209 (96.2%) eyes had no change in total HOAs at Month 3.
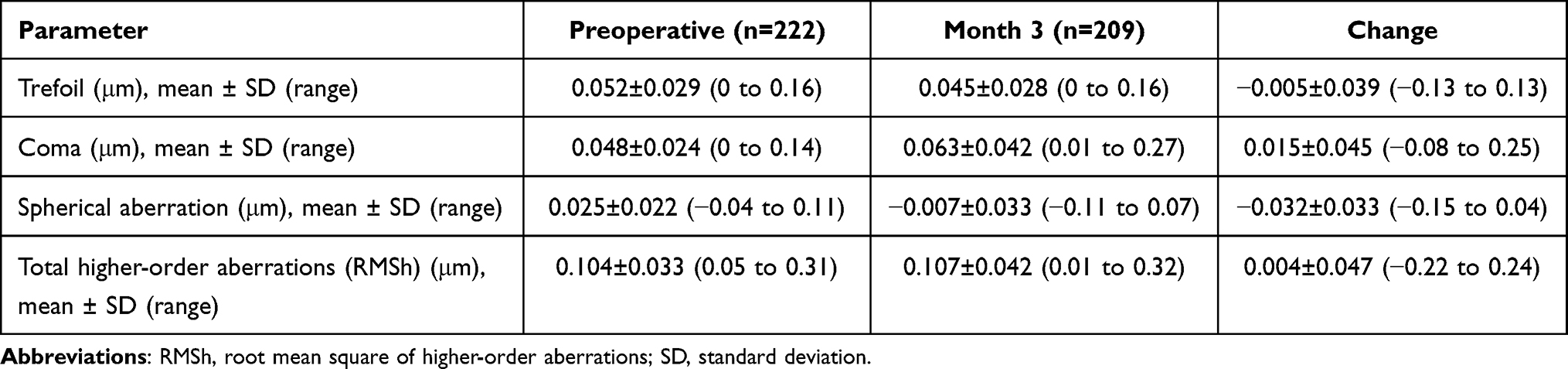 |
Table 2 Higher-Order Aberrations |
Safety Results
There were two serious non–flap-related AEs recorded for the same eye: a foreign body in the eye and the surgical procedure to remove it. Both events were deemed not to be related to the procedure or the device. Three eyes had a transient reduction in measured CDVA of ≥2 lines at Month 1 and/or Week 1. By Month 3, none of the eyes had lost ≥2 lines.
At Month 3, 105/106 (99.1%) patients reported that they were satisfied with their results, were happy they had undergone Femto LASIK surgery, would decide to have it again, and would recommend it to a friend or family member. All patients fully or partially achieved their set goals for LASIK surgery. The 1 patient who reported being very dissatisfied achieved CDVA and UDVA of 20/16 in the right eye, and 20/20 in the left eye at Month 3, which improved on preoperative values. The same patient reported that they would not have LASIK again or recommend it because they did not like the procedure or the results. Detailed responses on satisfaction and happiness are reported in Figure 3.
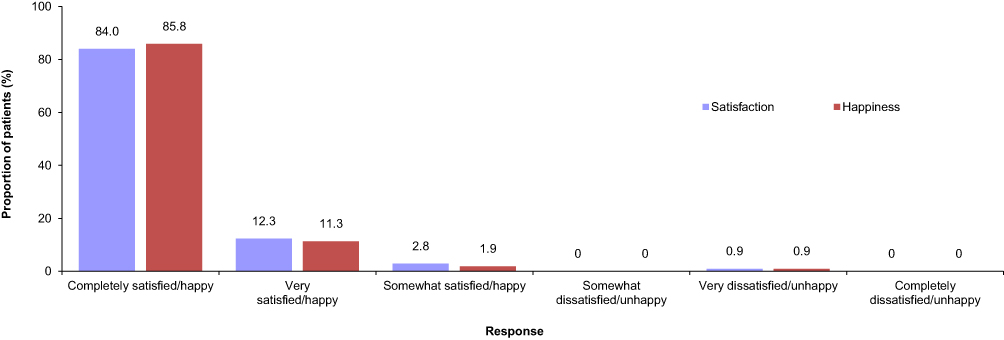 |
Figure 3 Patient satisfaction at Month 3. Abbreviations: Femto LASIK, femtosecond-assisted LASIK; LASIK, laser-assisted in situ keratomileusis; PROWL, patient-reported outcomes with LASIK. Notes: Detailed responses from the PROWL questionnaire on current satisfaction with results of Femto LASIK surgery and happiness/unhappiness that they had Femto LASIK surgery (n=106 patients). |
No eyes with preoperative CDVA of 20/20 or better had postoperative CDVA worse than 20/40, and no eyes had an absolute increase in manifest refractive astigmatism (>2.00 D of absolute cylinder).
Discussion
This study built upon previously published work by assessing the safety and efficacy of the automated InnovEyes Femto LASIK treatment based on data registered by a single device, the InnovEyes sightmap, in a larger cohort of patients across a wider variety of endpoints and with the addition of satisfaction assessment.
Data from this study suggest that the InnovEyes treatment has a good safety profile, with only two reported non–flap-related serious AEs, which were not attributed to the procedure or device. Moreover, this study is the first to report patient satisfaction with InnovEyes, with 105/106 (99.1%) patients stating they were satisfied and happy with their Femto LASIK treatment.
Concerns following Femto LASIK surgery included complications from the procedure, as well as the introduction of visual effects related to HOA. In this study, no corneal haze, diffuse lamellar keratitis, or epithelial ingrowth were observed.
Two prospective clinical studies have previously assessed safety and efficacy of the ray-tracing algorithm used by InnovEyes. The earlier one, authored by Schumacher et al,4 used multiple instruments to provide biometry, tomography, and wavefront patient data to the algorithm, as well as a variety of different excimer lasers and flap-making equipment. The wavefront measurements were performed under cycloplegia, whereas the current study used noncycloplegic measurements for treatment planning. At Month 3, among a total of 111 eyes, UDVAs of 20/16 and 20/20 or better were achieved in 68 (61.3%) and 93 (83.8%) eyes, respectively; of note, these results were less positive than those reported in this paper, where UDVAs of 20/16 and 20/20 or better were achieved in 175 (82.5%) and 208 (98.1%) of 212 eyes, respectively. Compared with the work presented here, the study had a higher threshold of preoperative refractive error, only including eyes with SE refraction >4.00 D of myopia or astigmatism >2.00 D, resulting in a mean preoperative MRSE of −5.92±1.72 D.4 Preoperative MRSE in the present study was only −3.38±1.76 D, which, combined with the differences in equipment and cycloplegia described above, could explain the discrepancies in the visual acuity outcomes. This would be consistent with the results from some patients from Schumacher et al, who were followed-up past 3 months; among those, patients with preoperative SE refractive error of −4.00 to 5.00 D showed superior outcomes at Month 6 compared with patients with preoperative SE refractive error >−5.00 D.5 Different LASIK treatments were also compared: 16/21 (76.2%) eyes achieved UCVA of 20/20 or better at Month 12 with ray-tracing, which exceeded the rates from wavefront-optimized (61.6%) and topography-guided (70.0%) LASIK, but was lower than with wavefront-guided (92.3%) LASIK.5 In these studies, the ablation and refraction were solely based on the ray-tracing calculation, which was applied unaltered for sphere and astigmatism.4,5
The second, an independent study authored by Kanellopoulos et al,6 used the current version of the InnovEyes algorithm with the InnovEyes sightmap and WaveLight EX500 excimer laser in 25 consecutive patients (50 eyes) with preoperative myopia ≤−9 D and astigmatism ≤−6 D. At Month 6, 40/40 (100%) eyes achieved UDVA of 20/20 or better and 26/40 (65%) eyes gained 1 or more lines of CDVA. RMSh increased to 0.35 µm from a preoperative value of 0.25 µm.6 UDVA results were very similar to those reported in this study and, although a higher proportion of eyes gained lines in CDVA, the proportion of eyes with no change or an improvement in CDVA was equivalent (40/40 [100%] in Kanellopoulos et al versus 211/212 [99.5%] eyes in the present study). RMSh values were slightly higher at baseline (0.25 μm in Kanellopoulos et al versus 0.104 μm in the present study) and increased slightly postoperatively (to 0.35 μm in Kanellopoulos et al versus 0.107 μm in the present study), although most patients treated had higher SEs in Kanellopoulos et al compared with the present study.6
The InnovEyes platform used in this study incorporates technological advancements compared with the systems used in the earlier studies described above. It uses various examinations to recreate geometric and optical properties of the eye through a single diagnostic device using the same adjustment means (corneal vertex), as opposed to multiple separate devices that use different adjustment means. Calculations of the eye model and ablation profile, as well as iterative testing and optimization of the postoperative cornea, are performed automatically rather than requiring manual oversight. The priority of the optimization of the postoperative cornea aims for correlation of the attainable to the target calculated ray-tracing. The system also allows wavefront examination to be conducted with undilated pupils, rather than necessitating cycloplegia, and incorporates cyclotorsion alignment, which was not available in the previous studies. Additionally, its precompensation matrix has been enhanced based on results from prior studies to further optimize the consideration of rotation and nonrotation symmetric aberrations.
The InnovEyes platform was used in a recently published retrospective analysis of real‑world data from 200 patients.10 This study included patients with similar baseline characteristics and achieved similar efficacy outcomes to the present prospective multicenter study. At Month 3, among a total of 400 eyes, UDVAs of 20/12.5 and 20/20 or better were achieved in 202 (50.5%) and 400 (100%) eyes, respectively. The mean change in total HOAs preoperatively versus postoperatively was numerically slightly greater than in the present study (0.057±0.125 μm and 0.004±0.047 μm, respectively), but was not clinically significant.10
Other customization treatments that use wavefront or topography data rely on standard eye models; in contrast, the InnovEyes ray-tracing algorithm generates an individualized eye model for each eye of each patient, which is used to calculate a fully customized ablation profile.6 By taking into consideration each patient’s unique optical system, InnovEyes treatment may lead to improved visual outcomes, even in patients who present with low degrees of refractive error and astigmatism. The promising outcomes in this study were achieved in a cohort in which the majority of eyes had manifest refraction sphere >−1.0 to ≤−4.0 D (145/222 [65.3%] eyes) and cylinder ≥0.0 to ≤−1.0 D (179/222 [80.6%] eyes). In addition, this study suggests benefits in a patient population with relatively low levels of preoperative HOAs (RMSh=0.104 μm), whereas other research suggested that customized ablations may only be beneficial in eyes with RMSh >0.3 μm.11,12
The InnovEyes algorithm also provides a built-in compensation for laser efficiency, corneal epithelial wound healing, and biomechanical changes. These calculations are performed automatically, potentially eliminating the requirement for manual treatment planning. Even though this functionality has not been specifically evaluated in this study, we believe that the InnovEyes system may potentially diminish time requirements and reduce the opportunity for human error for surgeons who want to offer their patients fully customized Femto LASIK treatments with clinically demonstrated efficacy and safety outcomes.
Limitations of this study included no hypothesis testing of the endpoints being planned in the present study. Comparison of the results from this study with those of prior studies cannot be used to determine the superiority of InnovEyes Femto LASIK to other types of LASIK. He & Bala reported that the results from their retrospective analysis study using InnovEyes compared favorably with those of wavefront-optimized and topography-guided LASIK treatments from prior studies, but stressed the need for head-to-head studies.10 Inclusion of both eyes from each patient is also a limitation of the present study.
A significant potential benefit of the InnovEyes customized Femto LASIK is reduction in postoperative HOAs, which can lead to visual function side effects. Although wavefront measurements were captured by the InnovEyes sightmap device at the patient’s pupil size under mesopic conditions, HOA values were calculated and displayed for an optical zone of 4 mm. The small area limited the ability to detect any changes in HOA at larger optical zones; therefore, another limitation was that we were not able to confirm the impact of InnovEyes Femto LASIK on scotopic HOAs.
Conclusions
This study suggests that the use of InnovEyes may broaden the patient population that can benefit from an individualized approach, as a larger proportion of eyes achieving UDVA of 20/16 or better at 3 months (175/212 [83%] eyes) was recorded than in many published values for wavefront-optimized (72%–76%),11,13 wavefront-guided (64%–69%),11,14,15 and topography-guided (22%–69%)16,17 LASIK studies in patients with myopia with or without astigmatism. By automatically calculating a customized ablation profile based on each patient’s unique optical system, InnovEyes Femto LASIK provides individualized treatments without the need for manual planning or modification.
The InnovEyes algorithm of the WaveLight EX500 excimer laser in conjunction with InnovEyes sightmap (InnovEyes Femto LASIK) was safe and effective for correction of myopia, with and without astigmatism, with visual function of many eyes markedly improved from baseline, along with high respective levels of patient satisfaction recorded.
Abbreviations
AE, adverse event; ANSI, American National Standards Institute; CDVA, corrected distance visual acuity; D, diopter; ETDRS, Early Treatment Diabetic Retinopathy Study; FAS, full analysis set; FDA, US Food and Drug Administration; Femto LASIK, femtosecond-assisted laser in situ keratomileusis; HOAs, higher-order aberrations; ISO, International Organization for Standardization; LASIK, laser-assisted in situ keratomileusis; logMAR, logarithm of the minimum angle of resolution; MRSE, manifest refraction spherical equivalent; PROWL, Patient‑Reported Outcomes With LASIK; RMSh, root mean square of higher-order aberrations; SE, spherical equivalent; UDVA, uncorrected distance visual acuity.
Data Sharing Statement
The data used and analyzed during the current study are not publicly available and will not be shared due to commercial interests. For additional detail, please contact the study sponsor via https://drks.de/search/en/trial/DRKS00020388.
Acknowledgments
The authors received editorial assistance in the preparation of the manuscript from Chameleon Communications International (London, UK), which was funded by Alcon Vision, LLC and conducted in accordance with Good Publication Practice guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding support for this manuscript was provided to authors by Alcon Vision, LLC (Fort Worth, TX, USA). This work was sponsored by Alcon Vision, LLC. The sponsors participated in the study design; collection, analysis, and interpretation of data; writing the report; decision to submit the report for publication; and preparation, review, and approval of the manuscript. This study was registered with the German Clinical Trials Register (www.drks.de/drks_web/; ID: DRKS00020388).
Disclosure
MM has received consulting fees from WaveLight (a subsidiary of Alcon; Erlangen, Germany) and equipment or other services from Alcon and is a board member of the Refractive Surgery Alliance. CB has received grants, consulting fees, and fees for education events from Alcon; grants from Johnson & Johnson (Irvine, CA, USA); and consulting fees from Hoya (Tokyo, Japan). CH, SL, and MEJ are employees of, and stockholders in, Alcon. RK has received grants, lecture fees, and travel support from Alcon and Johnson & Johnson; has received lecture fees from Carl Zeiss (Oberkochen, Germany), Heidelberg Engineering (Heidelberg, Germany), Bausch + Lomb (Bridgewater, NJ, USA), and Oculus (Wetzlar, Germany); and is an unpaid board member of DGII. All authors report no other conflicts of interest in this study.
References
1. Mrochen M, Bueeler M, Donitzky C, Seiler T. Optical ray tracing for the calculation of optimized corneal ablation profiles in refractive treatment planning. J Refract Surg. 2008;24(4):S446–451. doi:10.3928/1081597X-20080401-23
2. Bueler M, Mrochen M, inventors; Alcon Inc, assignee. Computer program for ophthalmological surgery. United States patent US 20080033408 A1. 2008 Feb 7.
3. Mrochen M, Donitzky C, Wüllner C, Löffler J. Wavefront-optimized ablation profiles: theoretical background. J Cataract Refract Surg. 2004;30(4):775–785. doi:10.1016/j.jcrs.2004.01.026
4. Schumacher S, Seiler T, Cummings A, Maus M, Mrochen M. Optical ray tracing-guided laser in situ keratomileusis for moderate to high myopic astigmatism. J Cataract Refract Surg. 2012;38(1):28–34. doi:10.1016/j.jcrs.2011.06.032
5. Cummings AB, Kelly GE. Optical ray tracing-guided myopic laser in situ keratomileusis: 1-year clinical outcomes. Clin Ophthalmol. 2013;7:1181–1191. doi:10.2147/OPTH.S44720
6. Kanellopoulos AJ. Initial outcomes with customized myopic LASIK, guided by automated ray tracing optimization: a novel technique. Clin Ophthalmol. 2020;14:3955–3963. doi:10.2147/OPTH.S280560
7. American National Standard for Ophthalmics. ANSI Z80.11-2012 (R2017): laser systems for corneal reshaping; 2017. Available from: https://webstore.ansi.org/standards/vc%20(asc%20z80)/ansiz80112012r2017.
8. International Organization for Standardization. ISO 14155:2011: clinical investigation of medical devices for human subjects – Good clinical practice; 2011. Available from: https://www.iso.org/standard/45557.html.
9. Gauvin M, Wallerstein A. AstigMATIC: an automatic tool for standard astigmatism vector analysis. BMC Ophthalmol. 2018;18(1):255. doi:10.1186/s12886-018-0920-1
10. He G, Bala C. Ray-tracing-guided myopic LASIK: real-world clinical outcomes. J Cataract Refract Surg. 2023;49(11):1140–1146. doi:10.1097/j.jcrs.0000000000001286
11. Stonecipher KG, Kezirian GM. Wavefront-optimized versus wavefront-guided LASIK for myopic astigmatism with the ALLEGRETTO WAVE: three-month results of a prospective FDA trial. J Refract Surg. 2008;24(4):S424–S430. doi:10.3928/1081597X-20080401-20
12. WaveLight GmbH. Summary of safety and effectiveness data for a supplemental premarket approval application: waveLight ALLEGRETTO WAVE™ Excimer Laser System and the ALLEGRO Analyzer; 2006. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P020050S004.
13. Kim J, Choi SH, Lim DH, et al. Topography-guided versus wavefront-optimized laser in situ keratomileusis for myopia: surgical outcomes. J Cataract Refract Surg. 2019;45(7):959–965. doi:10.1016/j.jcrs.2019.01.031
14. Mrochen M, Kaemmerer M, Seiler T. Clinical results of wavefront-guided laser in situ keratomileusis 3 months after surgery. J Cataract Refract Surg. 2001;27(2):201–207. doi:10.1016/S0886-3350(00)00827-0
15. Bausch & Lomb Inc. Summary of safety and effectiveness data for Technolas® 217z Zyoptix system for personalized vision correction; 2003. Available from: https://www.accessdata.fda.gov/cdrh_docs/pdf/P990027S006b.pdf.
16. Stulting RD, Fant BS, Bond W, et al. Results of topography-guided laser in situ keratomileusis custom ablation treatment with a refractive excimer laser. J Cataract Refract Surg. 2016;42(1):11–18. doi:10.1016/j.jcrs.2015.08.016
17. Kanellopoulos AJ. Topography-modified refraction (TMR): adjustment of treated cylinder amount and axis to the topography versus standard clinical refraction in myopic topography-guided LASIK. Clin Ophthalmol. 2016;10:2213–2221. doi:10.2147/OPTH.S122345
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.