Back to Journals » OncoTargets and Therapy » Volume 9
Internal mammary sentinel lymph node biopsy: abandon or persist?
Received 16 February 2016
Accepted for publication 7 May 2016
Published 27 June 2016 Volume 2016:9 Pages 3879—3882
DOI https://doi.org/10.2147/OTT.S106519
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Min Li
Peng-Fei Qiu, Yan-Bing Liu, Yong-Sheng Wang
Breast Cancer Center, Shandong Cancer Hospital and Institute, Jinan, Shandong, People’s Republic of China
Abstract: Although the 2009 American Joint Committee on Cancer incorporated the internal mammary sentinel lymph node biopsy (IM-SLNB) concept, there has been little change in surgical practice patterns due to the low visualization rate of internal mammary sentinel lymph nodes with the traditional injection technique. Meanwhile, as internal mammary lymph nodes (IMLN) metastases are mostly found concomitantly with axillary lymph nodes (ALN) metastases, previous IM-SLNB clinical trials fail to evaluate the status of IMLN in patients who are really in need (only in clinically ALN negative patients). Our modified injection technique (periareolar intraparenchymal, high volume, and ultrasonographic guidance) significantly improved the visualization rate of internal mammary sentinel lymph nodes, making the routine IM-SLNB possible in daily practice. IM-SLNB could provide individual minimally invasive staging, prognosis, and decision-making for breast cancer patients, especially for patients with clinically positive ALN. Moreover, IMLN radiotherapy should be tailored and balanced between the potential benefit and toxicity, and IM-SLNB-guided IMLN radiotherapy could achieve this goal. In the era of effective adjuvant therapy, within the changing treatment approach – more systemic therapy, less loco-regional therapy – clinicians should deliberate the application of regional IMLN therapy.
Keywords: breast cancer, internal mammary lymph node, axillary lymph node, sentinel lymph node biopsy
A Letter to the Editor has been received and published for this article.
Introduction
As a first-echelon nodal drainage site in breast cancer, the status of axillary lymph nodes (ALN) and internal mammary lymph nodes (IMLN) is valuable both for regional staging and treatment choice.1 Patients with IMLN metastases had a worse prognosis than those who did not, independent of their ALN status.1,2 The prognosis of patients with IMLN metastases only was similar to those with ALN metastases only; suggesting that regional disease in either nodal chain has the same prognostic relevance. In brief, the status of IMLN also provides important prognostic information for breast cancer patients. The status of ALN has been well established in breast cancer patients. However, accurate regional staging could not be achieved just with the status of the ALN alone, which might lead to under-stage and under-/over-treatment. Interest in metastases to IMLN culminated with the extended radical mastectomy,3 but this radical surgical procedure was abandoned due to its extra complications, longer operation time, and lack of survival benefit.4 Imaging techniques, such as ultrasound, magnetic resonance imaging, and positron emission tomography/computed tomography, could usually detect metastatic lesions larger than 5 mm, but due to the deep anatomical location and small size of IMLN, the sensitivity of current imaging techniques cannot satisfy the clinical practice. Therefore, an optimal method to evaluate the status of IMLN is still lacking so far.
The internal mammary sentinel lymph node biopsy (IM-SLNB) provided a less invasive method for assessing IMLN than surgical dissection, and may affect decision-making for regional and systemic therapy.1 However, routine performance of the IM-SLNB in breast cancer patients remains a subject of debate. Opponents point out that the IM-SLNB has no clinical relevance because internal mammary sentinel lymph nodes (IMSLN) metastases rarely influence adjuvant systemic treatment strategy.5,6 Besides, they suggest that the presence of IMSLN metastases did not affect overall survival independent of other prognostic factors.6 Proponents of routine IM-SLNB advocate that the presence of IMLN metastases is associated with a poorer prognosis in a small but substantial patient group, and that these metastases should therefore be treated with appropriate systemic therapy and IMLN radiotherapy.7,8 As a reflection of this ongoing debate, the National Comprehensive Cancer Network Clinical Practice Guidelines do not recommend routine IM-SLNB, however it is recommended to strongly consider radiotherapy to IMLN for patients with positive ALN or tumor >5 cm, noting “radiotherapy should be given to the IMLN that are clinically or pathologically positive; otherwise the treatment to the IMLN is at the discretion of the treating radiation oncologist” on this topic.9 In this article, the technical matter, indication, and clinical significance of IM-SLNB are discussed, and we would like to identify the breast cancer patients who may benefit from this minimally invasive diagnostic technique.
Modified injection technique with high visualization rate
Although the 2009 American Joint Committee on Cancer incorporated the IM-SLNB concept, there has been little change in surgical practice patterns due to the low visualization rate of IMSLN with the traditional radiotracer injection technique.5–8 As Chen et al summarized, superficial injection of radiotracer was unable to identify IMSLN, while intraparenchymal injection (peritumoral, intratumoral, or subtumoral) was more reliable.1 Unfortunately, with this injection method, the internal mammary hotspots in lymphoscintigraphy were seen only in a small proportion of patients (range from 13% to 37%), which has been the restriction for the biopsy of IMSLN to date.1,5–8 In our ongoing study, we tried injecting radiotracer with a modified technique (periareolar intraparenchymal, high volume, and ultrasound guidance), and got a high lymphoscintigraphy visualization rate of IMSLN (71.1%, 248/349, latest data).10,11 This might provide a technical feasibility of IM-SLNB, therefore, IM-SLNB could be performed routinely in clinical studies and daily practice, and might potentially impact treatment decision-making.
IM-SLNB should be performed in clinically ALN-positive patients
Although several studies indicated that the presence of IMSLN metastasis rarely influenced adjuvant treatment strategy and did not affect overall survival,5,6 it should be interpreted with caution due to the limitation of their study population. Studies of SLNB (both axilla and internal mammary) have been limited to the clinically ALN-negative patients, and it is adequate for the axillary staging. However, more attention should be focused on the IM-SLNB in clinically ALN-positive patients, as IMLN metastasis is mostly found concomitantly with ALN metastasis.4 Huang et al retrospectively analyzed 2,269 patients who received extended radical mastectomy, and showed that the incidence of IMLN metastasis was 4.4%, 18.8%, 28.1%, and 41.5% for patients with negative ALN, 1~3 positive ALN, 4~6 positive ALN, seven or more positive ALN, respectively.12 Veronesi et al also showed that the incidence of IMLN metastases increased dramatically from 9.1% in negative ALN to 29.1% in positive ALN patients.3 In our ongoing study, the IMSLN metastasis rate was only 8.1% in clinically ALN-negative patients, and adjuvant treatment was altered in a small proportion. However, the IMSLN metastasis rate was 20.5% in clinically ALN-positive patients, and individual radiotherapy strategy could be guided with the IM-SLNB results.13 As a consequence, previous IM-SLNB studies failed to evaluate the status of IMLN in patients who really were in need. We can see from the above results that there is a group of patients (clinically ALN-positive) who could really benefit from the IM-SLNB (Table 1). Therefore, we recommend that the research of IM-SLNB should be performed in patients with clinically positive ALN.14
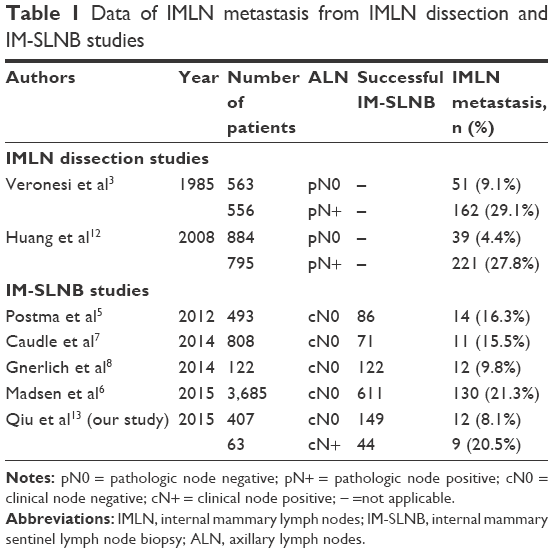 | Table 1 Data of IMLN metastasis from IMLN dissection and IM-SLNB studies |
Tailored radiotherapy under the IM-SLNB guidance
Regional nodal irradiation as a component of breast cancer radiation has been shown in numerous randomized trials and meta-analyses to have a significant impact on loco-regional control, breast cancer mortality, and overall survival.15 Recently, the DBCG-IMN study indicated that IMLN irradiation increased overall survival in patients with early-stage node-positive breast cancer,16 their exploratory subset analysis suggested that patients at the greatest risk for IMLN involvement will benefit most from the treatment; this suggestion ideally should be confirmed in other studies. The results of the NCIC MA.20 trial (n=1,832) and the European Organization for Research and Treatment of Cancer 22,922/10,925 trial (n=4,004) have also shown that additional regional irradiation to the IMLN and medial supraclavicular lymph nodes significantly improves the disease-free survival and distant metastasis-free survival in high-risk IMLN metastasis patients (positive ALN and/or medial/central tumor location).17,18 However, these eligibility criteria (high-risk patients/no histopathological confirmation of IMLN) might result in over- and under-treatment, because high-risk did not mean IMLN metastasis and low-risk did not mean IMLN negative. Although these trials showed that regional nodal irradiation was generally well tolerated, greater risks of lymphedema, pneumonitis, and cutaneous reactions were observed. Therefore, appropriate identification of patients who could benefit from adjuvant radiotherapy is essential, and should be based on IMSLN metastasis rather than high-risk estimation only. IMLN radiotherapy should be tailored and balanced between the potential benefit and toxicity, and IM-SLNB guidance could achieve this goal.19
Limitations of the IM-SLNB
Even though identification of IMLN metastases has important implications for treatment planning, some surgeons do not routinely perform IM-SLNB due to its limitations. On the one hand, IM-SLNB is an extra procedure that carries an additional risk of intra- and postoperative complications, such as pleural lesion and internal mammary artery bleeding.5–8 Additionally, a separate small parasternal incision may be needed in breast conservation procedures, which can be a cosmetic concern. On the other hand, unlike in the axilla, a back-up lymph node dissection is performed following the SLNB, the basic problem in previous IM-SLNB studies is that the accuracy of IM-SLNB has not been verified directly. Although the distribution of IMSLN exactly coincides with the sites of IMLN metastasis which were reported in the previous studies of extended radical mastectomy,1–3 a validation study (eg, IM-SLNB followed by complete IMLN dissection) might be required to confirm that the IMSLN could accurately reflect the nodal status of the internal mammary basin before its clinical application.
Regional therapy in the era of effective adjuvant therapy
During the past decades, the odds of recurrence at a distant or loco-regional site have decreased dramatically in breast cancer patients, and these encouraging results are due to the application of standardized clinical approaches, such as imaging, pathological analysis, surgery, and radiotherapy, but the near universal application of adjuvant systemic therapy has been thought to be the critical element.20 Adjuvant systemic therapy has been confirmed to be highly effective at reducing the risk of both distant relapse and loco-regional recurrence, and stepwise innovations in systemic therapy have correspondingly further improved overall survival and disease-free survival in breast cancer. It was recognized that the benefit of systemic therapy for loco-regional control has transformed breast cancer therapy pattern, reducing the need for loco-regional therapy among patients with metastatic IMLN. Therefore, with the applications of the effective systemic treatments which would further reduce local recurrence and improve survival, the status of loco-regional therapy in breast cancer might not be so important in the near future.
Conclusion
Progress in multidisciplinary management is improving survival for breast cancer patients, and within the changing treatment approach – more systemic therapy, less loco-regional therapy – clinicians should deliberate the application of regional IMLN therapy. IMLN radiotherapy should be tailored and balanced between the potential benefit and toxicity, and IM-SLNB-guided IMLN radiotherapy could achieve this goal. Moreover, unexpected clinical value might be found in further IM-SLNB clinical trials in clinically ALN-positive patients. Our conclusion is driven by a growing understanding of individualized treatment strategies, which means that some patients will receive more loco-regional therapy, whereas other females will receive less and still have very favorable results.
Acknowledgment
This work was supported by National Natural Science Foundation of China (81502314), Natural Science Foundation of Shandong Province (ZR2014HZ003), Natural Science Foundation of Shandong Province (ZR2015PH025) and Medical and Health Science Technology Development Program of Shandong Province (2015WS0162).
Disclosure
The authors declare no conflict of interest.
References
Chen RC, Lin NU, Golshan M, Harris JR, Bellon JR. Internal mammary nodes in breast cancer: diagnosis and implications for patient management – a systematic review. J Clin Oncol. 2008;26(30):4981–4989. | ||
Livingston SF, Arlen M. The extended extrapleural radical mastectomy: its role in the treatment of carcinoma of the breast. Ann Surg. 1974;179(3):260–265. | ||
Veronesi U, Cascinelli N, Greco M, et al. Prognosis of breast cancer patients after mastectomy and dissection of internal mammary nodes. Ann Surg. 1985;202(6):702–707. | ||
Veronesi U, Marubini E, Mariani L, Valagussa P, Zucali R. The dissection of internal mammary nodes does not improve the survival of breast cancer patients. 30-year results of a randomised trial. Eur J Cancer. 1999;35(9):1320–1325. | ||
Postma EL, van Wieringen S, Hobbelink MG, et al. Sentinel lymph node biopsy of the internal mammary chain in breast cancer. Breast Cancer Res Treat. 2012;134(2):735–741. | ||
Madsen EV, Aalders KC, van der Heiden-van der Loo M, et al. Prognostic significance of tumor-positive internal mammary sentinel lymph nodes in breast cancer: a multicenter cohort study. Ann Surg Oncol. 2015;22(13):4254–4262. | ||
Caudle AS, Yi M, Hoffman KE, et al. Impact of identification of internal mammary sentinel lymph node metastasis in breast cancer patients. Ann Surg Oncol. 2014;21(1):60–65. | ||
Gnerlich JL, Barreto-Andrade JC, Czechura T, et al. Accurate staging with internal mammary chain sentinel node biopsy for breast cancer. Ann Surg Oncol. 2014;21(2):368–374. | ||
National Comprehensive Cancer Network: NCCN Breast Cancer Clinical Practice Guidelines in Oncology (V. 1.2015). Available from: http://www.nccn.org/professionals/physician_gls/PDF/breast.pdf. Accessed June 20, 2016. | ||
Qiu PF, Liu JJ, Liu YB, et al. A modified technology could significantly improve the visualization rate of the internal mammary sentinel lymph nodes in breast cancer patients. Breast Cancer Res Treat. 2012;136(1):319–321. | ||
Cong BB, Cao XS, Qiu PF, et al. Validation study of the modified injection technique for internal mammary sentinel lymph node biopsy in breast cancer. Onco Targets Ther. 2015;8:2705–2708. | ||
Huang O, Wang L, Shen K, et al. Breast cancer subpopulation with high risk of internal mammary lymph nodes metastasis: analysis of 2,269 Chinese breast cancer patients treated with extended radical mastectomy. Breast Cancer Res Treat. 2008;107(3):379–387. | ||
Qiu PF, Cong BB, Zhao RR, et al. Internal Mammary Sentinel Lymph Node Biopsy With Modified Injection Technique: High Visualization Rate and Accurate Staging. Medicine (Baltimore). 2015;94(41):e1790. | ||
Qiu PF, Zhao RR, Liu YB, Wang YS. Internal mammary sentinel lymph node biopsy should still be performed, especially in the patient with clinically positive axillary lymph nodes. Breast. 2013;22(5):999–1000. | ||
Early Breast Cancer Trialists’ Collaborative Group, McGale P, Taylor C, et al. Effect of radiotherapy after mastectomy and axillary surgery on 10-year recurrence and 20-year breast cancer mortality: meta-analysis of individual patient data for 8135 women in 22 randomised trials. Lancet. 2014;383(9935):2127–2135. | ||
Thorsen LB, Offersen BV, Dano H, et al. DBCG-IMN: A population-based cohort study on the effect of internal mammary node irradiation in early node-positive breast cancer. J Clin Oncol. 2016;34(4):314–320. | ||
Whelan TJ, Olivotto IA, Parulekar WR, et al. Regional nodal irradiation in early-stage breast cancer. N Engl J Med. 2015;373(19):307–316. | ||
Poortmans PM, Collette S, Kirkove C, et al. Internal mammary and medial supraclavicular irradiation in breast cancer. N Engl J Med. 2015;373(4):317–327. | ||
Cong BB, Qiu PF, Wang YS. Internal mammary sentinel lymph node biopsy: minimally invasive staging and tailored internal mammary radiotherapy. Ann Surg Oncol. 2014;21(7):2119–2121. | ||
Burstein HJ, Morrow M. Nodal Irradiation after Breast-Cancer Surgery in the Era of Effective Adjuvant Therapy. N Engl J Med. 2015;373(4):379–381. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.