Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Interleukin-6 in Cerebrospinal Fluid Small Extracellular Vesicles as a Potential Biomarker for Prognosis of Aneurysmal Subarachnoid Haemorrhage
Authors Yao Y, Fang X, Yuan J, Qin F, Yu T, Xia D ![]() , Li Z, Lai N
, Li Z, Lai N
Received 29 January 2021
Accepted for publication 26 April 2021
Published 11 May 2021 Volume 2021:17 Pages 1423—1431
DOI https://doi.org/10.2147/NDT.S304394
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Yang Yao,1,2,* Xinggen Fang,1,* Jinlong Yuan,1 Feiyun Qin,1 Tao Yu,1 Dayong Xia,1,3 Zhenbao Li,1 Niansheng Lai1,3
1Department of Neurosurgery, First Affiliated Hospital of Wannan Medical College (Yijishan Hospital of Wannan Medical College), Wuhu, 241001, Anhui Province, People’s Republic of China; 2Department of Nursing, The First Affiliated Hospital of Wannan Medical College (Yijishan Hospital of Wannan Medical College), Wuhu, 241001, Anhui Province, People’s Republic of China; 3Key Laboratory of Non-Coding RNA Transformation Research of Anhui Higher Education Institution (Wannan Medical College), Wuhu, 241001, Anhui Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Niansheng Lai; Zhenbao Li
Department of Neurosurgery, First Affiliated Hospital of Wannan Medical College (Yijishan Hospital), 2 West Zheshan Road, Wuhu, 241001, Anhui Province, People’s Republic of China
Tel +86-15155308793
Fax +86-05535739594
Email [email protected]; [email protected]
Objective: Aneurysmal subarachnoid hemorrhage (aSAH) is a severe form of stroke characterized by high rates of mortality and disability. Identifying circulating biomarkers is helpful to improve outcomes. In this study, for the first time, we identify interleukin-6 (IL-6) in cerebrospinal fluid (CSF) small extracellular vesicles (sEVs) as potential biomarkers for prognosis of aSAH.
Methods: We extracted small extracellular vesicles from the CSF of 103 aSAH patients and 40 healthy controls in a prospective observational study. Subsequently, we measured IL-6sEVs levels using an enzyme-linked immunosorbent assay. Results were statistically analyzed to determine the function of IL-6sEVs for disease monitoring of aSAH.
Results: CSF IL-6 sEVs showed distinct pattern differences between healthy controls and aSAH patients. The concentration of IL-6sEVs in CSF is significantly correlated with the severity of aSAH patients. The areas under the receiver operating characteristic curves of IL-6sEVs for identifying severe aSAH patient from aSAH patients were 0.900. After multivariate logistic regression analysis, IL-6sEVs were associated with neurological outcome at 1 year. IL-6sEVs levels were greater and positively associated with disease processes and outcome.
Conclusion: There is a neuroinflammatory cascade in aSAH patients. IL-6sEVs in CSF may be a biomarker for the progression of aSAH.
Keywords: subarachnoid hemorrhage, cerebrospinal fluid, small extracellular vesicles, interleukin-6, biomarker
Introduction
Aneurysmal subarachnoid hemorrhage (aSAH) is a type of hemorrhagic stroke associated with 45% mortality and disability, which occurs at young ages and accounts for 5–7% of all strokes.1,2 The primary factors determining outcome include characteristics of the initial hemorrhage, which can lead to early brain injury (EBI) and may be related to delayed cerebral ischemia (DCI).3 Recently, researchers found that EBI after aSAH may predict unfavorable outcomes.4,5 These findings suggest the importance of pathological processes in EBI after aSAH, related to changes including microcirculation insufficiency, breakdown of ionic homeostasis, neuroinflammation, and microvascular contraction.6–8 A reliable, early, economical and non-invasive method is urgently in need to screen patients so as to improve outcomes.
Several studies focused on small extracellular vesicles (sEVs), which are lipid membrane vesicles that cross the blood-brain barrier (BBB) and mediate long-distance intercellular communications, assisting in transferring proteins, lipids, and ribonucleic acid for subsequent regulation of gene expression in target cells.9,10 sEVs are also secreted by brain cells passing through the BBB and can be tested in cerebrospinal fluid (CSF).11,12 sEVs can be enriched from CSF and can be used to detect various proteins, lipids, and nucleic acids.13 Secreted sEVs might be biomarkers that reflect pathophysiological processes in central nervous system (CNS) diseases. Recent studies have measured sEVs contents, finding a variety of proteins and functional ribonucleic acid species as biomarkers for cerebral ischemia.14–18
There is substantial evidence that the inflammatory response occurs very early after SAH and assists in EBI progression after SAH.4,6,19 Potential biomarkers include inflammatory cytokines such as interleukin-1β (IL-1β), IL-6, IL-8, IL-18, and tumor necrosis factor-alpha (TNF-α).20–22 IL-6 is a pro-inflammatory cytokine that increases in response to infection, tissue injury and other diseases.14,23,24 Studies reported that elevated IL-6 levels induce neuroinflammation and may be closely associated with the outcomes of aSAH.20,25,26 Nevertheless, screens for the expression IL-6 of sEVs in CSF of aSAH patients have not yet been reported.
Therefore, we hypothesized that aSAH causes changes in levels of IL-6 in sEVs in the CNS and that these sEVs are released into CSF where they may act as ideal biomarkers for aSAH. We extracted sEVs from the CSF of healthy controls and aSAH patients to measure expression levels of IL-6 in sEVs. We measured the IL-6 sEVs expression levels in aSAH patients, to evaluate possible connections between inflammatory response biomarkers and disease progression.
Methods
Ethics
Study participants were recruited from the Department of Neurosurgery, The First Affiliated Hospital of Wannan Medical College, Wuhu City, China. The study was performed following the Declaration of Helsinki. The Ethics Committee of the First Affiliated Hospital of Wannan Medical College approved all experiments. Participants or valid proxies provided written informed consent before the study.
Study Design
Patients with aSAH were recruited from March 2016 to August 2017. Out of 326 patients, CSF was collected from 103 patients with aSAH within the 48 h after hemorrhage after external ventricular drainage or lumbar puncture. Exclusion criteria were as follows: admission later than 72 h after ruptured aneurysm; non-aneurysmal SAH; liver, kidney, heart or lung insufficiency or infectious diseases; rebleeding after admission and poor outcomes upon admission without any treatment. From healthy controls, CSF was obtained during spinal anesthesia before surgery (n=40).
The WFNS grade is a tool that determines the scales of SAH–induced EBI. Initial clinical status was accessed using the World Federation of Neurological Surgeons (WFNS) grade on admission.27 aSAH patients were classified as mild aSAH with WFNS grades of I–III, and severe aSAH with WFNS grades IV and V. The modified Fisher scale was used to calculate the amount of blood of aSAH patients. The amount of blood on computed tomography (CT) was evaluated using the modified Fisher scale on admission.27 Cerebral vasospasm was diagnosed using computed tomography angiography, digital subtraction angiography, magnetic resonance angiography, or transcranial Doppler according to maximum mean flow velocity (MMFV) > 120 cm/s, and Lindegaard ratios > 3.28–30 Hydrocephalus and DCI were classified as present or absent based on CT scans or magnetic resonance imaging (MRI). DCI was confirmed as a new focal neurological deficit, consciousness disorder, or a new infarct based on CT scans or MRI.31
Surgical clip or endovascular coil was performed in all patients with aSAH. Functional outcome was assessed using the Modified Rankin Scale (mRS) using structured WeChat or telephone interviews by two trained nurses.32 At the end of the follow-up period, patients with mRS scores 0–2 were classified as having good outcomes, and those with mRS scores 3–6 were classified as having poor outcomes. All participants received a follow-up at 1-year after aSAH. Tables 1 and 2 summarize the basic characteristics of the population.
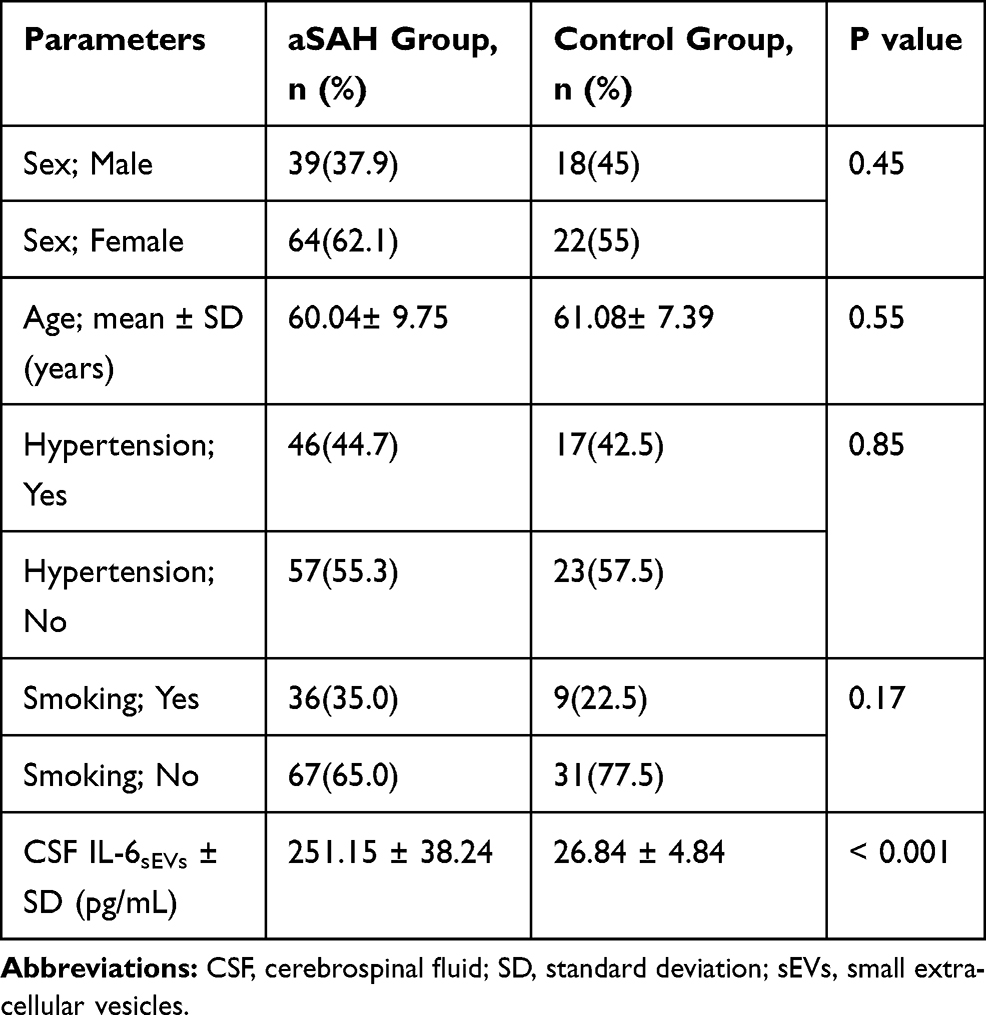 |
Table 1 Characteristics and Clinical Data of Study Population |
 |
Table 2 Clinicopathological Features of aSAH |
CSF Processing
CSF specimens were centrifuged at 500 rpm and 4 °C for 10 minutes. The upper layer was transferred into a RNase/DNase-free 1.5mL Eppendorf tube. CSF specimens were divided into aliquots and stored at −80°C.
Isolation of sEVs from CSF Samples
sEVs were isolated using miRCURY Exosome Kits (from Cell/Urine/CSF; Qiagen, Valencia, CA) following the manufacturer’s protocol. Briefly, 400μL of the precipitation buffer B was added to 1 mL of CSF samples and mixed well at 4 °C for 60 minutes, followed by centrifugation at 10,000 g for 30 minutes at 25 °C. The sEVs were harvested by removing the supernatants. The sEVs were resuspended in 100 μL of resuspension buffer, and were then ready for further analysis. Then, sEVs were lysed using 1% Triton X-100 lysis buffer (Beyotime, P0013) that contained protease and phosphatase inhibitor cocktails. The lysates were stored at −80°C.
Western Blot Analysis
The 20 μg samples of total protein of sEVs samples were separated using SDS-PAGE, and were electrophoretically transferred to PVDF membranes (Millipore). The membranes were blocked with 5% skim milk. Western bloting proceeded incubated using primary antibodies. The primary antibodies used were as follows: mouse anti-CD63 (1:1000, Abcam), and rabbit anti-Alix (1:1000, Abcam). Appropriate HRP-conjugated anti-rabbit, or anti-mouse (1:5000, Beyotime) secondary antibodies were incubated for 2 h at room temperature. Western blots were visualized using an enhanced chemiluminescence (ECL) kit (Beyotime).
Transmission Electron Microscopy (TEM)
sEVs were adsorbed on formvar-carbon coated grids for 1 h, and subsequently transferred to drops of PBS three times for 5 minutes. Samples were stained with uranyl acetate and lead citrate (Sigma-Aldrich). After three time washings for 30 seconds in deionized water, grids were air-dried overnight and finally scanned under a JEOL JEM-1400 transmission electron microscope at 80 kV.
Enzyme-Linked Immunosorbent Assay (ELISA)
The concentrations of IL-6 and tetra-spanning exosome marker CD81 in sEVs of CSF were measured using specific enzyme-linked immunosorbent kits (Elabscience Biotechnology, China) according to the manufacturer’s instructions. The mean values for all the determinations of CD81 in the patient cohort were set at 1.00 and the relative values for each specimen were used to normalize their recovery. The final concentration of IL-6 was analyzed using optical density (OD) values. Two laboratory technicians measured all ELISAs without knowledge of the clinical information.
Statistical Analysis
Statistical comparisons were analyzed using MedCalc version 15.0.0 (MedCalc Software bvba, Ostend, Belgium). Data were expressed as mean ± standard deviation (SD). The Mann–Whitney U-test was performed to assess statistical significance between the two groups and the Kruskal–Wallis test was performed for statistical significance between more than two groups. The Spearman rank correlation coefficient analysis was used to assess the relationships among the variables. Receiver operating characteristic (ROC) curves were constructed to calculate the optimal thresholds of IL-6 for evaluating outcomes of aSAH. A multivariable logistic regression model was generated to assess factors that are associated with the outcomes after adjusting for risk factors that yielded P < 0.1 in the univariate analyses. A P-value of < 0.05 was considered significant.
Results
Patient Characteristics
In this pilot study, a total of 103 aSAH patients and 40 health controls were recruited. Healthy controls included 24 patients with inguinal hernias and 16 with uterine fibroids. The mean age ±SD of aSAH patients was 60.04± 9.75 years (range, 40–83 yr); there were 64 females and 39 males. CSF was collected at 48 h after aSAH or was obtained during spinal anesthesia before surgery in each healthy control. We excluded 223 patients for reasons listed in Figure 1. The detailed characteristics are summarized in Tables 1 and 2. There were no significant differences in age or sex ratio between the aSAH patients and healthy controls.
 |
Figure 1 Inclusion criteria flowchart for the population investigated in this study. |
sEVs Characterization
Transmission electron microscope image showed that sEVs were spherical with sizes of 30–150 nm, similar to the reported sEVs (Figure 2A). There were no significant differences in the size or shape of sEVs between aSAH patients and healthy controls. The Western blotting analysis showed that CD63 and Alix were expressed in sEVs (Figure 2B).
 |
Figure 2 Characterization of exosomes. (A) Transmission electron microscopy of isolated plasma exosomes. Bar, 100 nm. (B) Western blotting analysis of exosome markers (CD63 and Alix). |
IL-6sEVs Levels in CSF of aSAH Patients and Healthy Controls
The concentrations of IL-6sEVs were measured in 103 aSAH samples and 40 control samples. The CD81-normalized levels of IL-6sEVs in CSF were significantly higher at one day after operation than in control samples (aSAH: 251.15 ± 38.24 pg/mL; controls: 26.84 ± 4.84 pg/mL, P<0.001) (Figure 3).
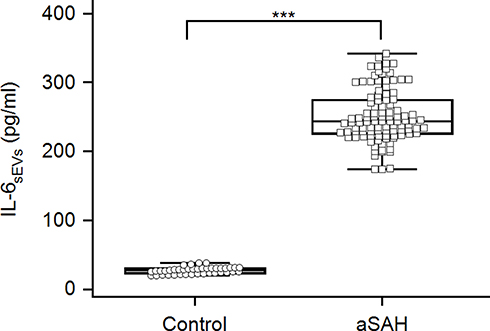 |
Figure 3 Expression of IL-6sEVs in aSAH patients and healthy controls. ***P <0.001. |
Relationships of IL-6sEVs of CSF with aSAH Severity
As illustrated in Figure 4A, comparison of the severe aSAH patients with mild had significantly higher IL-6sEVs levels (mild aSAH:228.58 ±22.75 pg/mL; severe aSAH: 280.25±34.38 pg/mL, P<0.001). To determine the utility of IL-6sEVs for the identification of patients with severe aSAH, we used ROC curve analysis and found that the area under the ROC of IL-6sEVs was 0.900 (95% CI: 0.825–0.950; P<0.001) and Youden index was 0.70 (Figure 4B). The highest accuracy was found at a cutoff expression value of 247.89, where the positive predictive value, negative predictive value, sensitivity, and specificity to identify severe aSAH were 84.1, 86.4, 82.22, and 87.93%, respectively.
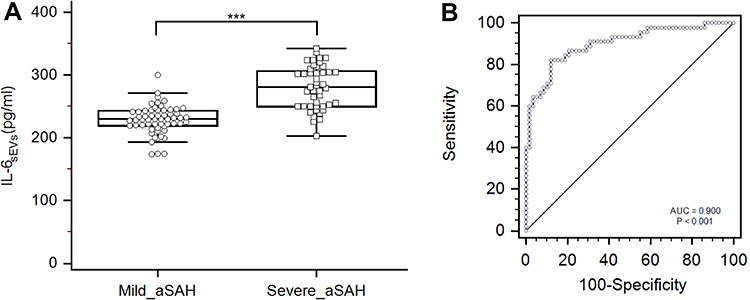 |
Figure 4 (A) Relative levels of IL-6sEVs in aSAH patients with severe aSAH and those with mild aSAH. (B) ROC curves to distinguish severe from mild aSAH patients. ***P <0.001. |
To further delve into the relationships between the levels of IL-6sEVs in CSF and WFNS grade, we used Spearman’s analysis. In the aSAH patients, there were close relationships between the levels of IL-6sEVs (ρ = 0.710; 95% CI: 0.599 to 0.794; P<0.001) and aSAH severity according to the WFNS grade.
Relationships of IL-6sEVs in CSF with Clinical Outcomes of aSAH Patients
The mRS scores were higher in patients with higher expression of IL-6sEVs than in those with lower expression (P < 0.001; Figure 5A). In univariate analysis, WFNS grade, modified Fisher score, cerebral vasospasm, acute hydrocephalus, DCI and IL-6sEVs levels were prognostic factors 1 year post-SAH (P < 0.1). The higher levels of IL-6sEVs closely correlated with poor outcomes at 1 year post-SAH after the multivariable logistic regression analysis (P < 0.001; Table 3). ROC curves revealed that the levels of IL-6sEVs had a robust predictive value to discriminate poor outcomes, with an area under the curve (AUC) value of 0.947 (95% CI: 0.884 to 0.981; P<0.001; Figure 5B) and Youden index was 0.75, where the sensitivity and specificity to identify poor outcomes were 84.21% and 90.77%, respectively. Additionally, ROC curves showed that the combined expression of IL-6sEVs and clinical parameters (WFNS grade, modified Fisher score, cerebral vasospasm, acute hydrocephalus and DCI) had a significantly higher predictive value to discriminate poor outcomes, with an area under the curve value of 0.968 (95% CI: 0.913 to 0.993; P<0.001; Figure 5B) and Youden index was 0.88, where the sensitivity and specificity to identify poor outcomes were 97.37% and 90.77%, respectively. These findings suggest that prognostic prediction may be improved by the detection of the levels of IL-6sEVs in CSF.
 |
Table 3 Multivariable Logistic Analyses of Risk Factors with Poor Outcome in aSAH Patients at 1-Year |
 |
Figure 5 (A) Relative levels of IL-6sEVs in aSAH patients with good outcome and those with poor outcome. (B) ROC curves to distinguish SAH patients with poor outcomes. ***P <0.001. |
Discussion
We measured CSF sEVs in healthy controls and aSAH patients. We found that the CSF-circulating IL-6sEVs levels revealed distinct differences between healthy controls and aSAH patients. The CSF circulating IL-6sEVs levels were higher in severe aSAH patients than in mild aSAH patients. Finally, the CSF circulating IL-6sEVs levels were associated with outcomes in aSAH patients.
Several pro-inflammatory cytokines are related to aSAH.21 IL-6 played an essential role in brain injury and was linked to aSAH in several studies.20,26,33 The high levels of IL-6 in the extracellular fluid of cerebral microdialysis were associated with high intracranial hypertension and unfavourable outcome.34–36 A clinical study showed that IL-6 in CSF was a marker for predicting cerebral vasospasm after SAH.37 Other studies showed that the expression levels of IL-6 in CSF were associated with outcomes in aSAH patients.21,25,33 Elevated IL-6 levels in CSF may induce neuroinflammation and may be closely linked to the progression of delayed cerebral ischemia after SAH.24 IL-6 and TNF-α in CSF could be essential biomarkers for disease prediction and disease monitoring in SAH patients.22 Another study reported that the expression levels of IL-6 in CSF were biomarkers for ventricular infection.38 Another study reported that the determinations of IL-6 in CSF could be a useful diagnostic biomarker for predicting shunt dependency in aSAH patients with acute hydrocephalus.39 Others reported that levels of IL-6 in serum were elevated, and were associated with outcome in aSAH patients.26,40 However, many previous studies also showed that measuring IL-6 levels in circulation may be insufficient.33,41 CSF sEVs might directly reflect the situation in the brain, and peripheral circulating might have little effect on proinflammatory cytokines in CSF sEVs. For these reasons, the measurement of IL-6sEVs levels in CSF, as opposed to in CSF or circulating blood, may be better reflect the actual IL-6 levels in aSAH. Therefore, in the present study, we determined whether IL-6sEVs in CSF could serve as a biomarker to discriminate aSAH patients from healthy controls.
The main findings of this study were that the levels of IL-6sEVs in CSF were elevated in aSAH patients, suggesting they might serve as a biomarker for the outcome of aSAH. IL-6sEVs expression may be used to discriminate severe aSAH from mild aSAH. ROC curves with areas under the curves were constructed. The sensitivity and specificity shown in ROC curves were high for IL-6sEVs levels. IL-6sEVs was a good predictor of neurologic outcome, whereas WFNS grade and modified Fisher score were not. These results suggest that IL-6 may be involved in the occurrence, development, and repair of aSAH. Other CNS diseases may be associated with neuroinflammation as well. One study reported that inflammatory cytokines in CSF sEVs are elevated in acute encephalitis.11 Proinflammatory cytokines in the exosomes derived from CSF were elevated in patients with spinal cord injury.42 For these reasons, IL-6sEVs may not be fitted to distinguish aSAH from other CNS diseases. Moreover, the pathogenesis of aSAH is complex and involves many pathophysiological processes, including inflammation, oxidative stress, apoptosis, autophagy and neuronal regeneration.
Although the present study aimed to investigate the CSF-circulating IL-6sEVs levels as potential biomarkers correlated with disease severity and outcome in aSAH patients, there were a few methodological limitations. First, this was a retrospective study with a wide age range and a small number of patients. Second, CSF was taken from aSAH patients after surgery and during medical treatment. The expression of IL-6sEVs in CSF may be induced by changes during surgery and drugs treatment.
In summary, IL-6sEVs in CSF may be a reliable biomarker associated with EBI of aSAH. IL-6sEVs in CSF could be another accurate predictor of clinical outcomes. IL-6 is a proinflammatory cytokine that regulates several physiological processes. The indicator may be an early outcome biomarker for aSAH patients, but not an independent one. Future studies are critical to determining whether IL-6sEVs in CSF regulates a regulatory role in disease progression of aSAH and to evaluate its potential as a therapeutic target.
Abbreviations
aSAH, aneurysmal subarachnoid hemorrhage; AUCs, area under curves; BBB: blood-brain barrier; BCA, bicinchoninic acid; CNS, central nervous system; CSF, cerebrospinal fluid; CT, computed tomography; CVs, cerebral vasospasm; DCI, delayed cerebral ischemia; ELISA, enzyme-linked immunosorbent assay; EBI, early brain injury; ECL, enhanced chemiluminescence; IL-6, Interleukin-6; mRS, Modified Rankin Scale; sEVs, small extracellular vesicles; ROC, receiver operating characteristic; SD, standard deviation; SDS-PAGE, sodium dodecyl sulfate-polyacrylamide gels; TEM, transmission electron microscopy; WFNS, World Federation Of Neurosurgical Societies.
Ethics and Consent
Study participants were recruited from the Department of Neurosurgery at The First Affiliated Hospital of Wannan Medical College, Wuhu City, China. The study was performed in accordance with the Declaration of Helsinki. Written informed consent (Version number: SAH20160215) was received from participants or valid proxies (family or a professional not directly involved in the study). All experiments were approved by the Ethics Committee of the First Affiliated Hospital of Wannan Medical College (March 14, 2016).
Acknowledgments
The authors thank all participants and cooperating clinicians, and the department of the Central Laboratory of First Affiliated Hospital of Wannan Medical College for the support of basic facilities and Jiaqi Zhang and Bingbing Zhang for assistance with the sample collection.
Author Contributions
All authors contributed to conception and design, data analysis, drafting the article; agreed to submit to the current journal; gave final approval for the version to be published; and agreed to be accountable for all aspects of the work.
Funding
This work was supported by grants from the National Natural Science Foundation of China (no.81701357), Key Research and Development Program of Anhui province (no.201904a07020034), Funding of “Peak” Training Program for Scientific Research of First Affiliated Hospital of Wannan Medical College (no.GF2019G05), National Natural Science Foundation of Anhui Province (no.1708085QH181), Natural Science Research Project in Higher Education of Anhui Province (no.KJ2018A0253), and Science Research Project of Professional Personnel of First Affiliated Hospital of Wannan Medical College(no.YR201911).
Disclosure
The authors claim no conflicts of interest for this work.
References
1. Lai NS, Zhang JQ, Qin FY, Sheng B, Fang XG, Li ZB. Serum microRNAs are non-invasive biomarkers for the presence and progression of subarachnoid haemorrhage. Biosci Rep. 2017;37(1):BSR20160480. doi:10.1042/BSR20160480
2. Vivancos J, Gilo F, Frutos R, et al. Guía de actuación clínica en la hemorragia subaracnoidea. Sistemática diagnóstica y tratamiento. Neurología. 2014;29(6):353–370. doi:10.1016/j.nrl.2012.07.009
3. Sheng B, Fang X, Liu C, et al. Persistent High Levels of miR-502-5p are associated with poor neurologic outcome in patients with aneurysmal subarachnoid hemorrhage. World Neurosurg. 2018;116(10):e92–99. doi:10.1016/j.wneu.2018.04.088
4. Dou Y, Shen H, Feng D, et al. Tumor necrosis factor receptor-associated factor 6 participates in early brain injury after subarachnoid hemorrhage in rats through inhibiting autophagy and promoting oxidative stress. J Neurochem. 2017;142(3):478–492. doi:10.1111/jnc.14075
5. Witsch J, Kuohn L, Hebert R, et al. Early prognostication of 1-year outcome after subarachnoid hemorrhage: the FRESH score validation. J Stroke Cerebrovasc Dis. 2019;28(10):104280. doi:10.1016/j.jstrokecerebrovasdis.2019.06.038
6. Gris T, Laplante P, Thebault P, et al. Innate immunity activation in the early brain injury period following subarachnoid hemorrhage. J Neuroinflammation. 2019;16(1):253. doi:10.1186/s12974-019-1629-7
7. Huang F, Yi J, Zhou T, Gong X, Jiang H, Yao X. Toward understanding non-coding RNA roles in intracranial aneurysms and subarachnoid hemorrhage. Transl Neurosci. 2017;8:54–64. doi:10.1515/tnsci-2017-0010
8. Rass V, Helbok R. Early brain injury after poor-grade subarachnoid hemorrhage. Curr Neurol Neurosci Rep. 2019;19(10):78. doi:10.1007/s11910-019-0990-3
9. Ramirez SH, Andrews AM, Paul D, Pachter JS. Extracellular vesicles: mediators and biomarkers of pathology along CNS barriers. Fluids Barriers CNS. 2018;15(1):19. doi:10.1186/s12987-018-0104-7
10. Thery C, Witwer KW, Aikawa E, et al. Minimal information for studies of extracellular vesicles 2018 (MISEV2018): a position statement of the International Society for Extracellular Vesicles and update of the MISEV2014 guidelines. J Extracell Vesicles. 2018;7(1):1535750.
11. Goswami S, Banerjee A, Kumari B, et al. Differential expression and significance of circulating microRNAs in cerebrospinal fluid of acute encephalitis patients infected with Japanese encephalitis virus. Mol Neurobiol. 2017;54(2):1541–1551. doi:10.1007/s12035-016-9764-y
12. Ohmichi T, Mitsuhashi M, Tatebe H, Kasai T, Ali El-Agnaf OM, Tokuda T. Quantification of brain-derived extracellular vesicles in plasma as a biomarker to diagnose Parkinson’s and related diseases. Parkinsonism Relat Disord. 2019;61:82–87. doi:10.1016/j.parkreldis.2018.11.021
13. Kanninen KM, Bister N, Koistinaho J, Malm T. Exosomes as new diagnostic tools in CNS diseases. Biochim Biophys Acta. 2016;1862(3):403–410. doi:10.1016/j.bbadis.2015.09.020
14. Kerr N, Garcia-Contreras M, Abbassi S, et al. Inflammasome proteins in serum and serum-derived extracellular vesicles as biomarkers of stroke. Front Mol Neurosci. 2018;11:309. doi:10.3389/fnmol.2018.00309
15. Li DB, Liu JL, Wang W, et al. Plasma Exosomal miRNA-122-5p and miR-300-3p as potential markers for transient ischaemic attack in rats. Front Aging Neurosci. 2018;10:24. doi:10.3389/fnagi.2018.00024
16. Wang W, Li D-B, Li R-Y, et al. Diagnosis of hyperacute and acute ischaemic stroke: the potential utility of exosomal microRNA-21-5p and MicroRNA-30a-5p. Cerebrovasc Dis. 2018;45(5–6):204–212. doi:10.1159/000488365
17. Yu P, Chen W. Advances in the diagnosis of exosomal miRNAs in ischemic stroke. Neuropsychiatr Dis Treat. 2019;15:2339–2343. doi:10.2147/NDT.S216784
18. Zhou J, Chen L, Chen B, et al. Increased serum exosomal miR-134 expression in the acute ischemic stroke patients. BMC Neurol. 2018;18(1):198. doi:10.1186/s12883-018-1196-z
19. Liu W, Li R, Yin J, et al. Mesenchymal stem cells alleviate the early brain injury of subarachnoid hemorrhage partly by suppression of Notch1-dependent neuroinflammation: involvement of Botch. J Neuroinflammation. 2019;16(1):8. doi:10.1186/s12974-019-1396-5
20. Ahn SH, Savarraj JPJ, Parsha K, et al. Inflammation in delayed ischemia and functional outcomes after subarachnoid hemorrhage. J Neuroinflammation. 2019;16(1):213. doi:10.1186/s12974-019-1578-1
21. Al-Tamimi YZ, Bhargava D, Orsi NM, et al. Compartmentalisation of the inflammatory response following aneurysmal subarachnoid haemorrhage. Cytokine. 2019;123:154778. doi:10.1016/j.cyto.2019.154778
22. Wu W, Guan Y, Zhao G, et al. Elevated IL-6 and TNF-alpha levels in cerebrospinal fluid of subarachnoid hemorrhage patients. Mol Neurobiol. 2016;53(5):3277–3285. doi:10.1007/s12035-015-9268-1
23. Li Y, Yuan L, Yang J, et al. Changes in serum cytokines may predict therapeutic efficacy of tofacitinib in rheumatoid arthritis. Mediators Inflamm. 2019;2019:5617431. doi:10.1155/2019/5617431
24. Niwa A, Osuka K, Nakura T, Matsuo N, Watabe T, Takayasu M. Interleukin-6, MCP-1, IP-10, and MIG are sequentially expressed in cerebrospinal fluid after subarachnoid hemorrhage. J Neuroinflammation. 2016;13(1):217. doi:10.1186/s12974-016-0675-7
25. Duris K, Neuman E, Vybihal V, et al. Early dynamics of interleukin-6 in cerebrospinal fluid after aneurysmal subarachnoid hemorrhage. J Neurol Surg a Cent Eur Neurosurg. 2018;79(2):145–151. doi:10.1055/s-0037-1604084
26. Zhang W, Sun L, Ma L, Li Z. Clinical significance of changes in IL-6, CRP and S100 in serum and NO in cerebrospinal fluid in subarachnoid hemorrhage and prognosis. Exp Ther Med. 2018;16(2):816–820. doi:10.3892/etm.2018.6231
27. Eagles ME, Jaja BNR, Macdonald RL. Incorporating a modified graeb score to the modified fisher scale for improved risk prediction of delayed cerebral ischemia following aneurysmal subarachnoid hemorrhage. Neurosurgery. 2018;82(3):299–305. doi:10.1093/neuros/nyx165
28. Bender M, Richter E, Schwarm FP, et al. Transcranial doppler sonography defined vasospasm, ischemic brain lesions, and delayed ischemic neurological deficit in younger and elderly patients after aneurysmal subarachnoid hemorrhage. World Neurosurg. 2020;138:e718–e724. doi:10.1016/j.wneu.2020.03.051
29. Letourneau-Guillon L, Farzin B, Darsaut TE, et al. Reliability of CT angiography in cerebral vasospasm: a systematic review of the literature and an inter- and intraobserver study. AJNR Am J Neuroradiol. 2020;41(4):612–618. doi:10.3174/ajnr.A6462
30. Takano K, Hida K, Iwaasa M, Inoue T, Yoshimitsu K. Three-dimensional spin-echo-based black-blood MRA in the detection of vasospasm following subarachnoid hemorrhage. JMRI. 2019;49(3):800–807. doi:10.1002/jmri.26231
31. Luo YG, Han B, Sun TW, Liu X, Liu J, Zhang J. The association between serum adipocyte fatty acid-binding protein and 3-month disability outcome after aneurysmal subarachnoid hemorrhage. J Neuroinflammation. 2020;17(1):66. doi:10.1186/s12974-020-01743-2
32. Bache S, Rasmussen R, Rossing M, Laigaard FP, Nielsen FC, Moller K. MicroRNA changes in cerebrospinal fluid after subarachnoid hemorrhage. Stroke. 2017;48(9):2391–2398. doi:10.1161/STROKEAHA.117.017804
33. Vlachogiannis P, Hillered L, Khalil F, Enblad P, Ronne-Engstrom E. Interleukin-6 levels in cerebrospinal fluid and plasma in patients with severe spontaneous subarachnoid hemorrhage. World Neurosurg. 2019;122:e612–e618. doi:10.1016/j.wneu.2018.10.113
34. Mellergård P, Åneman O, Sjögren F, Säberg C, Hillman J. Differences in cerebral extracellular response of interleukin-1β, interleukin-6, and interleukin-10 after subarachnoid hemorrhage or severe head trauma in humans. Neurosurgery. 2011;68(1):
35. Zeiler FA, Thelin EP, Czosnyka M, Hutchinson PJ, Menon DK, Helmy A. Cerebrospinal fluid and microdialysis cytokines in aneurysmal subarachnoid hemorrhage: a scoping systematic review. Front Neurol. 2017;8:379. doi:10.3389/fneur.2017.00379
36. Graetz D, Nagel A, Schlenk F, Sakowitz O, Vajkoczy P, Sarrafzadeh A. High ICP as trigger of proinflammatory IL-6 cytokine activation in aneurysmal subarachnoid hemorrhage. Neurol Res. 2010;32(7):728–735. doi:10.1179/016164109X12464612122650
37. Schoch B, Regel JP, Wichert M, Gasser T, Volbracht L, Stolke D. Analysis of intrathecal interleukin-6 as a potential predictive factor for vasospasm in subarachnoid hemorrhage. Neurosurgery. 2007;60(5):828–836. doi:10.1227/01.NEU.0000255440.21495.80
38. Hopkins SJ, McMahon CJ, Singh N, et al. Cerebrospinal fluid and plasma cytokines after subarachnoid haemorrhage: CSF interleukin-6 may be an early marker of infection. J Neuroinflammation. 2012;9:255. doi:10.1186/1742-2094-9-255
39. Wostrack M, Reeb T, Martin J, et al. Shunt-dependent hydrocephalus after aneurysmal subarachnoid hemorrhage: the role of intrathecal interleukin-6. Neurocrit Care. 2014;21(1):78–84. doi:10.1007/s12028-014-9991-x
40. Chaudhry SR, Stoffel-Wagner B, Kinfe TM, et al. Elevated systemic IL-6 levels in patients with aneurysmal subarachnoid hemorrhage is an unspecific marker for post-SAH complications. Int J Mol Sci. 2017;18(12):2580. doi:10.3390/ijms18122580
41. Sarrafzadeh A, Schlenk F, Gericke C, Vajkoczy P. Relevance of cerebral interleukin-6 after aneurysmal subarachnoid hemorrhage. Neurocrit Care. 2010;13(3):339–346. doi:10.1007/s12028-010-9432-4
42. de Rivero Vaccari JP, Brand F
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.