Back to Journals » Psychology Research and Behavior Management » Volume 18
Intergenerational Psychological Capital, Disability, and Depressive Symptoms in the Shadow of Functional Deprivation Among Middle-Aged and Older Adults in China
Authors Zhang J ![]() , Zhang D, Xue X, Wang X, Ding S
, Zhang D, Xue X, Wang X, Ding S ![]() , Ma Y
, Ma Y
Received 20 July 2025
Accepted for publication 11 October 2025
Published 28 October 2025 Volume 2025:18 Pages 2237—2257
DOI https://doi.org/10.2147/PRBM.S552384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Jiahao Zhang,1,2 Dan Zhang,2 Xizi Xue,3 Xuming Wang,1,2,4 Shuangshuang Ding,5 Yinbiao Ma1,2,6
1School of Economics and Management, Dalian University of Technology, Dalian, 116024, People’s Republic of China; 2Graduate School of Education, Dalian University of Technology, Dalian, 116024, People’s Republic of China; 3School of Economics and Management, Beijing Jiaotong University, Beijing, 100044, People’s Republic of China; 4School of Government, Baoshan University, Baoshan, Yunnan, 678000, People’s Republic of China; 5School of Public Administration and Policy, Dalian University of Technology, Dalian, 116024, People’s Republic of China; 6School of Teacher Education, Baoshan University, Baoshan, Yunnan, 678000, People’s Republic of China
Correspondence: Dan Zhang, Graduate School of Education,Dalian University of Technology, Dalian, 116024, People’s Republic of China, Email [email protected] Xizi Xue, School of Economics and Management, Beijing Jiaotong University, Beijing, 100044, People’s Republic of China, Email [email protected]
Background: Depression represents a major public health challenge worldwide, especially in middle-aged and older adult populations. Although intergenerational support plays an established role in promoting psychological well-being, the mechanisms underlying this relationship remain inadequately understood. A crucial and frequently neglected element in this dynamic is functional deprivation—defined as the decline in the capacity to perform basic and instrumental activities of daily living (ADL/IADL). This loss substantially undermines autonomy and increases vulnerability to depression. The present study introduces the first-introduced construct of Intergenerational Psychological Capital (IPC) as a protective factor that may mitigate the detrimental mental health effects of functional deprivation.
Objective: This study examines the protective influence of Intergenerational Psychological Capital (IPC) on depressive symptoms in middle-aged and older adults. We test a moderated mediation model in which functional autonomy deprivation serves as a mediator, and disability operates as a moderator affecting the pathway between IPC functional autonomy deprivation and depression.
Methods: We analyzed five waves of CHARLS data (2011– 2020) comprising 33,369 valid observations using Stata 17.0. A moderated mediation analysis was conducted through hierarchical regression modeling, testing the relationships among intergenerational psychological capital, functional autonomy deprivation, disability, and depression with adjusted standard errors and sociodemographic controls.
Results: IPC was significantly associated with reduced depressive symptoms (β=− 0.088, p< 0.001. Functional autonomy deprivation partially mediated this relationship (IPC →mediator: β =− 0.019, p< 0.001; mediator →depression: β = 0.809, p< 0.001). Furthermore, disability significantly moderated this mediated pathway: the buffering effect of IPC on functional autonomy deprivation was more pronounced among adults with disabilities, though its overall protective effect on depression was partially attenuated in this group.
Conclusion: These findings indicate that IPC alleviates depression both directly and indirectly through reducing functional autonomy deprivation. However, the presence of disability constrains the full benefits of IPC, highlighting the need for inclusive mental health interventions that address both functional capacity and intergenerational psychological resources.
Keywords: intergenerational psychological capital, IPC, depressive symptoms, disability, functional autonomy deprivation, restrictive context, moderated mediation model
Introduction
The Global Burden of Depression in Aging Populations
Promoting mental health is fundamental to social prosperity and sustainable development. In recent years, depression has been increasingly recognized as a critical global public health challenge.1–4 Characterized by persistent low mood, diminished interest or pleasure, and significant cognitive impairment,5–7 this disorder demonstrates a particularly high prevalence among middle-aged and older adult populations, with notably alarming rates observed in individuals over the age of 45.8,9 It is projected that by 2030, major depressive disorder (MDD) will become the leading cause of the global disease burden.10
Epidemiology and Impact of Depression in China Among Middle-Aged and Older Adults in China
Nationally representative data from China reveal a 12-month prevalence of depressive disorders reaching 4.1% among adults aged 50–64 and 3.8% among those aged 65 and above, establishing depression as one of the most common mental disorders within these demographic groups.11 The condition significantly elevates the risk of developing chronic diseases including cardiovascular disease and diabetes,12 imposes substantial emotional and economic burdens on families,13 and adversely affects broader societal productivity and long-term economic growth.1,14,15 Consequently, depression represents not only a formidable threat to individual health but also a serious challenge to public health resources and sustainable economic development.2,16
Psychological Capital as a Protective Framework
Existing research has identified numerous determinants influencing depression risk, including macroeconomic factors, technological accessibility, population dynamics, and environmental conditions.1,2,5,6,14,16 In recent years, psychological capital has gained recognition as a key protective factor against depression. Defined by dimensions such as hope, optimism, resilience, and self-efficacy, psychological capital enables individuals to maintain mental well-being and adapt to adverse life conditions.17 As a malleable personal resource, psychological capital demonstrably improves mental health outcomes and influences work-related attitudes and behaviors.18–20 Empirical evidence consistently shows a significant negative correlation between psychological capital and depressive symptoms, indicating that higher levels of this resource are associated with reduced depressive symptomatology.21
Expanding the Concept to Intergenerational Psychological Capital
Despite these advances, the extant literature predominantly conceptualizes psychological capital as an internally generated individual attribute,18,20,22 largely overlooking its potential construction through dynamic intergenerational relationships, particularly among middle-aged and older adults. To this end, we formally introduce the theory of Intergenerational Psychological Capital (IPC) as a novel construct developed to capture these overlooked dynamics. It is first advanced in this research and conceptually framed as: the positive psychological resources that are cultivated, sustained, and enhanced through reciprocal intergenerational relationships and exchanges, encompassing the development of shared hope, collective resilience, mutually reinforced efficacy, and optimized optimism within family systems across generations.
Within the Chinese cultural context where familial ties maintain profound significance, support from adult children—especially financial transfers—transcends mere material fulfillment. As established by Fan and Lei,23 both objective and subjective financial circumstances are significantly associated with depressive symptoms and overall mental health among Chinese older adults, highlighting the fundamental importance of economic factors in psychological well-being. When perceived by aging parents as embodying filial piety, emotional connection, and familial commitment, such support may facilitate the development of intergenerational psychological capital. This process enhances emotional stability, reinforces a sense of control, and fosters positive future expectations through ongoing relational exchanges and family interactions.24,25
To our knowledge, this represents the first systematic attempt to conceptualize psychological capital as an intergenerationally constructed resource emerging from family relationships, rather than viewing it solely as an individual-level attribute. We humbly propose that this perspective may offer a valuable extension to existing psychological capital theory by emphasizing the relational origins and social embeddedness of these psychological resources.
Such culturally embedded capital may serve as an accessible and effective psychological resource, particularly in contexts where formal mental health support remains limited. Furthermore, psychological capital represents a well-established protective factor against depression in middle-aged and older adults, offering substantial buffering effects.26 Nevertheless, the specific mechanisms through which intergenerational psychological capital influences depressive symptoms in this population require further theoretical elaboration and empirical investigation.
The Mediating Role of Functional Autonomy Deprivation
The relationship between intergenerational psychological capital and depressive symptoms may be importantly mediated through functional autonomy deprivation. This concept emphasizes that impairments in performing basic and instrumental activities of daily living not only signal declining health but may also trigger loss of self-efficacy, reduced social engagement, and eventual social isolation. As demonstrated by recent research, limitations in activities of daily living (ADL) show significant associations with depressive symptoms among older adults, with those reporting more severe depressive symptoms also experiencing more negative social interactions and diminished sense of belonging.27 Within the specific context of our study focusing on middle-aged and older adults, the relationship with ADL dependence is particularly salient. Advanced age typically accompanies various physical diseases or symptoms that may lead to ADL limitations,28 and the co-occurrence of depression with such conditions often exacerbates physical health problems related to ADL.29 These physical constraints operate through dual mechanisms: they directly restrict individuals’ ability to participate in activities, while simultaneously creating psychological barriers that discourage engagement due to concerns about social dignity and self-presentation.
Within such contexts, economic and emotional support from adult children may serve to mitigate these challenges by enhancing living standards, improving quality of life, facilitating emotional communication, and strengthening social connections, thereby collectively supporting the mental health of middle-aged and older adults facing functional autonomy deprivation.
The Moderating Role of Disability Status
This psychological mechanism may be further moderated by individual disability status. Disability extends beyond physiological limitations to represent a form of structural social vulnerability that substantially affects individuals’ access to external resources, shapes psychological responses, and influences overall resilience.30 Individuals with physical limitations may experience more profound emotional impacts from declining functional abilities, potentially making intergenerational psychological capital particularly beneficial for this group. Simultaneously, for older adults with disabilities who face limited resource access, the symbolic meaning embedded in children’s support—such as the fulfillment of family responsibilities and the reinforcement of emotional bonds—may carry heightened significance, thereby amplifying psychological benefits.31 Consequently, disability status may differentially influence the pathway from intergenerational psychological capital through functional autonomy deprivation to depression, warranting careful empirical examination.
Research Gaps and Current Contributions
Several significant gaps persist in the current literature: a lack of integrative theoretical models that capture the psychological pathways linking intergenerational dynamics and depression; insufficient attention to effect heterogeneity across different vulnerable groups, particularly individuals with disabilities; and an overreliance on cross-sectional or short-term longitudinal data that limits the generalizability of findings. The present study addresses these limitations by constructing a moderated mediation model utilizing five waves of nationally representative CHARLS data (2011–2020) to investigate how intergenerational psychological capital alleviates depression through reducing functional autonomy deprivation, and how this pathway is moderated by disability status. Our research offers three primary contributions: extending psychological capital research into intergenerational and relational dimensions; reconceptualizing functional autonomy deprivation as a psychological pathway rather than merely a health outcome; and incorporating the critical dimension of structural vulnerability into models examining emotional health disparities among older adults.
Theoretical Framework and Hypotheses
Dual Mechanisms of Intergenerational Psychological Capital: Emotional and Functional Pathways
The concept of “Intergenerational Psychological Capital” (IPC) offers a theoretically nuanced framework for understanding how support from adult children contributes to the psychological well-being of aging parents. Moving beyond perspectives that primarily consider the material utility of financial transfers, IPC directs scholarly attention to the symbolic meanings, relational significance, and positive psychological resources potentially cultivated within intergenerational relationships. Although the specific terminology of IPC is still emerging in the empirical literature, its conceptual foundations are firmly grounded in existing sociological and psychological research, particularly building upon the work of Luthans et al on psychological capital and Cong and Silverstein on intergenerational support.22,24,25
Substantial evidence indicates that financial support from adult children serves dual functions: it addresses practical needs while simultaneously fostering psychological resources such as resilience, self-esteem, and a sense of social embeddedness, which are instrumental in reducing vulnerability to depressive symptomatology.32 Strong empirical support comes from Wu et al33 and Xia et al34 who demonstrate negative associations between children’s financial support and depressive symptoms among Chinese older adults in both short-term and long-term contexts. Crucially, however, these psychological benefits emerge primarily when financial support is perceived by aging parents as representing emotional investment and familial commitment rather than merely material transfer. Empirical studies consistently report that older adults who receive consistent support interpreted in this manner demonstrate markedly higher levels of psychological well-being,31,35,36 and robust evidence links such meaningful intergenerational support to the amelioration of depressive symptoms in later life.37 Within the distinctive context of Chinese society, financial assistance is deeply embedded in the cultural norm of filial piety, and its receipt often signifies to aging parents the fulfillment of culturally prescribed expectations, thereby enhancing subjective happiness.38 The regular provision of resources is frequently interpreted by older adults not merely as monetary aid but as a tangible representation of emotional investment and filial devotion. This perception profoundly reinforces their sense of self-worth and affirms their valued position within the family unit, while also enhancing feelings of belonging and well-being as demonstrated by Liu et al36 and Zhan et al.31
Confronting the challenges associated with physical decline and the loss of previous social roles, the positive affective resources engendered by supportive intergenerational exchanges can serve as a critical buffer against feelings of loneliness and helplessness, thereby diminishing the risk of depressive outcomes.24 Moreover, reliable financial assistance bolsters older adults’ perceptions of future security and control,38 which is particularly crucial amidst health declines and economic precarity. This sustained support effectively mitigates existential anxieties and emotional distress. Furthermore, intergenerational support can activate and sustain older adults’ meaning-making systems. When individuals perceive themselves as maintaining significant familial roles, their sense of purpose and existential meaning is powerfully reinforced, acting as a protective factor against depression.39
Consequently, from an IPC perspective, financial support from children transcends its instrumental material function when it is perceived as representing emotional commitment and family solidarity. It operates as a vehicle for social affirmation, emotional connection, and the reaffirmation of self-worth, thereby establishing a multifaceted psychological mechanism that helps mitigate depressive symptoms among the elderly. Grounded in this refined theoretical reasoning and the accompanying empirical evidence, this study posits Hypothesis H1: Financial support from adult children contributes to the formation of Intergenerational Psychological Capital, which in turn alleviates depressive symptoms among middle-aged and older adults.
Mediating Pathway of Functional Autonomy
Within the context of intensifying global population aging, intergenerational support is increasingly recognized as a critical psychosocial resource for older adults’ mental health.40 Moving beyond purely economic interpretations, this study introduces Intergenerational Psychological Capital (IPC) as a latent construct encompassing emotional connection, perceived control, and future-oriented optimism derived from intergenerational relationships. Rather than viewing financial support merely as material transfer, we argue that it serves as a carrier of profound symbolic meaning—affirming dignity, sustaining identity, and strengthening relational bonds.41
Functional Autonomy Deprivation refers to the experienced loss of capacity to perform activities essential for independent living, encompassing both objectively assessed declines in physical function (as measured by BADL/IADL scales) and the perceived weakening of personal agency and self-efficacy. This construct does not imply external coercion but rather captures the multifaceted loss of autonomy that many older adults face due to age-related physical decline, in a manner consistent with the psychosocial model of disability.
The influence of IPC on depressive symptoms is theorized to operate specifically through the mediating pathway of Functional Autonomy Deprivation. This construct reflects not only objective declines in physical function—as captured by BADL/IADL measures—but also the subjective loss of agency and self-efficacy that often accompanies aging-related disability.42,43 Empirical evidence suggests that financial support from adult children may slow this multidimensional functional decline through multiple mechanisms: reducing financial barriers to healthcare, facilitating access to supportive services, reinforcing emotional security, and promoting healthier lifestyles through improved resource pooling within the family.44,45
Given that financial support from adult children can alleviate depressive symptoms through these diverse pathways, it may be conceptualized as a concrete manifestation of Intergenerational Psychological Capital (IPC). Beyond its material utility, such support embodies relational commitment, filial empathy, and generational solidarity, which together enhance the older adults’ sense of meaning, belonging, and identity continuity. When internalized as IPC, these resources not only mitigate objective functional decline but also strengthen psychological resilience against the emotional distress associated with loss of autonomy. Thus, IPC serves as a critical psychosocial resource that translates intergenerational support into sustained mental health benefits.
From a life-course perspective, ADL/IADL limitations often serve as early markers of declining mental health.46 Such limitations may restrict social activities, intensify feelings of loneliness and helplessness, and trigger negative emotional cycles. According to the “Cumulative Disadvantage Theory”, continuous physical decline accumulates psychological detriments, gradually weakening the effects of external resources.47 It can trigger cycles of social isolation, reduced self-worth, and emotional distress—a process consistent with Cumulative Disadvantage Theory48. Within this framework, we propose that IPC helps counteract such decline by reinforcing autonomy and meaning even in the face of physical vulnerability.
Therefore, when older adults face BADL/IADL impairments, their psychological capital—such as self-esteem, sense of control, and future expectations—may be eroded, exacerbating the risk of depression. Based on this theoretical framework, this study proposes Hypothesis H2: Functional autonomy (ADL) partially mediates the relationship between IPC and depressive symptoms.
Moderating Effects of Disability: A Three-Pathway Model
Physical disabilities become more common with advancing age.48 In middle and old age, physical disability constitutes a critical vulnerability, reflecting not only physiological decline but also reduced capacity in daily activities, social engagement, and emotional regulation. Drawing on Resource Vulnerability Theory,49 this study conceptualizes disability as a form of structural constraint that limits access to external resources and profoundly shapes how individuals perceive and utilize those resources.
Disability may interfere with the beneficial effects of intergenerational support on mental health through three interrelated mechanisms: first, by reducing the practical effectiveness of such support in restoring functional capacity;50 second, by intensifying emotional reactivity to functional loss51 (eg, ADL impairments); and third, by altering the symbolic meaning of support, thereby modifying the cognitive-emotional pathways through which Intergenerational Psychological Capital (IPC) alleviates depressive symptoms. Building upon the foundational mediation model involving IPC, functional autonomy deprivation, and depressive symptoms, this study introduces physical disability as a key moderating variable. Disability should not be treated merely as a statistical covariate but as a constitutive condition that shapes resource needs, sense of agency, and social self-perception, thereby influencing how intergenerational resources translate into psychological health outcomes.
Consistent with Resource Vulnerability Theory,49 individuals with disabilities demonstrate greater reliance on external support and increased sensitivity to the emotional and symbolic dimensions of care.52 For disabled older adults, financial and emotional support from their children provides not only material assistance but also conveys profound symbolic meanings—affirming belonging, sustaining personal value, and strengthening emotional bonds. Under these conditions, the protective effect of IPC against feelings of inadequacy and despair becomes particularly pronounced.
Therefore, this study proposes Hypothesis H3a: Disability significantly moderates the pathway from IPC to functional autonomy deprivation.
At the same time, disability often entails chronic pain, mobility limitations, and psychosocial sequelae such as eroded self-efficacy, social isolation, and role marginalization4². These experiences can intensify emotional responses to further functional loss, potentially leading to emotional exhaustion and collapse of coping capacity. Consequently, among disabled individuals, declines in ADL functioning may produce a “context-amplified” effect on depressive symptomatology. This study thus proposes Hypothesis H3b: Disability significantly moderates the pathway from functional autonomy deprivation to depressive symptoms.
From a symbolic interactionism perspective,44 intergenerational support constitutes not only resource transfer but also, and more importantly, a symbolic process that reaffirms identity and maintains social connectedness. For older adults with disabilities—who often experience eroded functional ability and social roles—support from their children takes on heightened symbolic significance. It serves as a powerful social message: “You are still valued and cared for”. Consequently, individuals with disabilities may be more likely to internalize intergenerational support as psychological capital, thereby enhancing emotional resilience and reducing vulnerability to depression. Hence, Hypothesis H3c is proposed: Disability significantly moderates the direct effect of intergenerational psychological capital on depressive symptoms.
The overall conceptual model is presented in Figure 1.
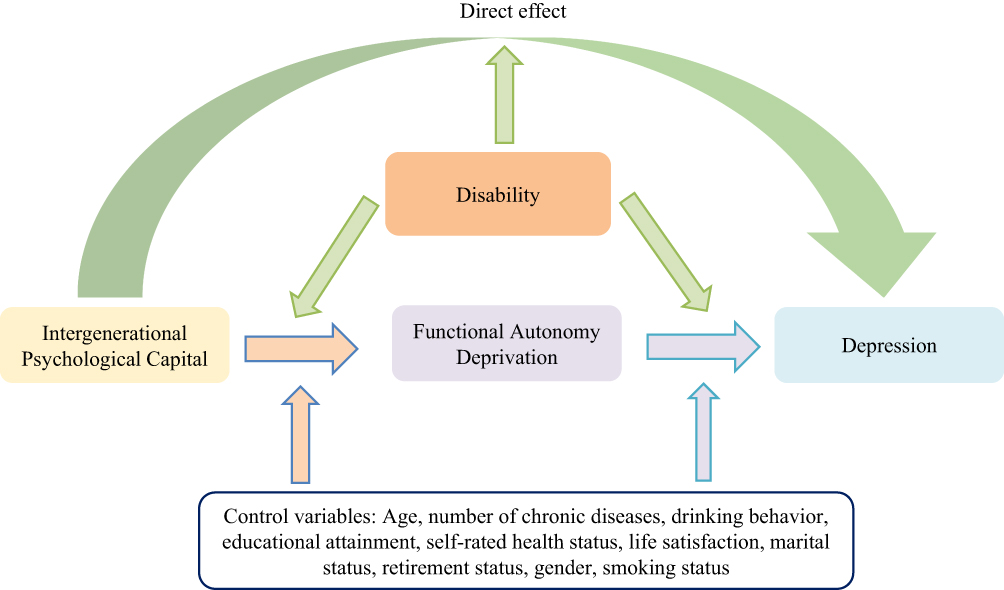 |
Figure 1 The Pathway Model of Intergenerational Psychological Capital, Functional Autonomy Deprivation, and Depression. |
Materials and Methods
Participants
This study utilizes data from the China Health and Retirement Longitudinal Study (CHARLS), a nationally representative, longitudinal survey jointly conducted by Wuhan University and Peking University. Designed to support interdisciplinary research on population aging in China and provide empirical evidence for policymaking, CHARLS collects high-quality micro-level data on Chinese adults aged 45 and above and their households. The baseline survey was launched in 2011 across 28 provinces, municipalities, and autonomous regions (excluding Hong Kong, Macao, Taiwan, Xinjiang, Ningxia, Tibet, and Hainan). Employing a multi-stage stratified sampling strategy, one core respondent was randomly selected from each household. The sample covers approximately 150 counties/districts and 450 villages or urban communities, ensuring broad representation of both urban and rural residents.
This study utilizes five waves of nationally representative data from the China Health and Retirement Longitudinal Study (CHARLS), conducted in 2011, 2013, 2015, 2018, and 2020. After integrating these waves, a pooled cross-sectional dataset was constructed with an initial total of 33,369 observations. To ensure data quality and analytical validity, a rigorous preprocessing procedure was applied. This included cleansing the dataset by excluding records with substantial missing values across key variables of interest. Furthermore, the study specifically focuses on middle-aged and older adults, retaining only individuals aged 45 years and above as the primary study population. All variables were carefully selected and operationalized in accordance with the theoretical framework of this research.
Measures
Dependent Variable
To assess depressive symptoms, we employed the 10-item short form of the Center for Epidemiologic Studies Depression Scale (CES-D), which has been widely used in mental health research. The CHARLS dataset includes responses to this scale, which measures emotional and psychological states over the past week, including feelings of distress, distraction, sadness, lethargy, hope, fear, sleep quality, pleasure, loneliness, and feelings of unspeakable discomfort. Each item is scored from 0 to 3, corresponding to the frequency of occurrence: “rarely or none”, “some”, “occasionally”, and “most of the time”. Positively phrased items (eg, “felt happy”, “felt hopeful”) were reverse-coded. Total scores range from 0 to 30, with higher scores indicating greater depressive symptom severity. The scale has demonstrated strong reliability and validity in both domestic and international studies.1,2,5,6,53,54
Independent Variable
Economic support from children not only signifies material assistance but also conveys emotional recognition, fulfillment of familial obligation, and social endorsement, embodying what is referred to as intergenerational psychological capital.55 We operationalized this concept using the variable childsup, representing the total monetary value (in RMB) of financial support, including cash and in-kind transfers, received by respondents from their children during the survey period. Data were extracted from the CHARLS module on intergenerational economic transfers. To reduce the influence of outliers and improve the normality of distribution, a logarithmic transformation was applied.
Mediating Variable
Functional autonomy was assessed using the Activities of Daily Living (ADL) index, a composite measure of the ability to perform both basic and instrumental daily tasks. The index includes two dimensions: Basic ADL (BADL)-such as dressing, toileting, bathing, eating, getting in and out of bed, and walking—and Instrumental ADL (IADL)-including cooking, shopping, telephone use, medication management, financial management, and household chores.56,57 Based on CHARLS data, we constructed an 11-item ADL score ranging from 0 to 11, with higher scores indicating greater functional impairment and reduced self-care capacity. This measure has been validated in numerous aging and health studies as a reliable predictor of psychological well-being.58
Moderating Variable
Disability status was coded as a binary variable based on CHARLS data: individuals with a disability were coded as 1, and those without a disability as 0. This allowed for empirical testing of the moderating role of disability in the proposed model.
Control Variables
To enhance the validity of our model estimates, we included a set of control variables capturing demographic characteristics, health status, and subjective evaluations, all drawn from CHARLS.
Age (age): Chronological age based on birth date. Prior research has found a positive association between age and depression risk.1
Number of Chronic Conditions (chronic): Includes 14 common chronic diseases such as hypertension, dyslipidemia, diabetes, cancer, chronic lung disease, liver disease, heart disease, stroke, kidney disease, gastrointestinal disorders, emotional or psychological issues, memory problems, arthritis, and asthma (range: 0–14).29
Alcohol Consumption (drink): Binary variable coded 1 if the respondent has ever consumed alcohol, 0 otherwise; alcohol use is significantly linked to depression.59
Education Level (educ): Categorized into four levels: 0 = no schooling or incomplete primary, 1 = primary school, 2 = secondary school, 3 = high school or above. Higher education is associated with greater coping ability.60,61
Self-Rated Health (health): A five-point scale measuring perceived health status, with higher scores indicating better perceived health. Negatively correlated with depression.62
Life Satisfaction (life): Measured on a five-point scale reflecting overall satisfaction with current life, known to positively impact mental health.63
Marital Status (married): Coded 1 if married, 0 if unmarried, divorced, or widowed. Marriage is a key source of social support.64
Retirement Status (retire): Coded 1 if retired, 0 otherwise. Retirement entails role transitions that can influence mental well-being and social networks.65
Gender (sex): Coded 0 for male and 1 for female; women are generally more vulnerable to depressive symptoms.1
Smoking History (smoke): Coded 1 if the respondent has ever smoked, 0 otherwise. Smoking has a documented positive association with depression risk.66
In sum, the inclusion of these covariates helps reduce estimation bias and provides a more rigorous foundation for identifying the determinants of depressive symptoms among older adults in China.
Procedure
Baseline Model
This study investigates the effect of intergenerational psychological capital on depressive symptoms at the individual level. Based on our theoretical assumptions, we posit a linear relationship among the variables and thus employ a baseline linear regression model to examine these associations:

Where CESDi denotes the depressive symptoms of individual, childsupi represents the intergenerational psychological capital, controli includes a vector of control variables, and εi is the error term. A statistically significant a1 would indicate that intergenerational psychological capital is significantly associated with depressive symptoms, thus supporting the hypothesized main effect.
Mediation Model
Following the mediation analysis framework proposed by Wen and Ye,67 we examine whether functional autonomy mediates the relationship between intergenerational psychological capital and depressive symptoms. The mediation model is specified as follows:


Where ADLi indicates the level of functional autonomy of individual i. Equation (2) assesses the effect of intergenerational psychological capital on functional autonomy, while equation (3) includes both predictors to evaluate the mediating role. If c2 in equation (3) is statistically significant, mediation is supported. If both c1, c2 are significant, this implies a partial mediation effect. To strengthen the robustness of the mediation findings, we also conduct a Sobel test.68
Moderated Mediation Model
Drawing on the moderated mediation framework proposed by Wen and Ye,69 we further examine whether structural functional disability moderates the mechanisms through which intergenerational psychological capital influences depressive symptoms. Specifically, we estimate regression models (4), (5), and (6) to assess the potential moderating role of physical disability in three key pathways.
If the interaction term in model (4) is statistically significant, it indicates that physical disability moderates the relationship between intergenerational psychological capital and functional autonomy deprivation. If the interaction term in model (5) is significant, it suggests that physical disability moderates the association between functional autonomy deprivation and depressive symptoms. Likewise, a significant interaction effect in model (6) would imply that physical disability moderates the direct link between intergenerational psychological capital and depressive symptoms.



Empirical Results and Analysis
Baseline Regression
To comprehensively understand the sample characteristics, we conducted descriptive statistical analyses of the primary variables, as presented in Table 1. Utilizing data from five waves (2011, 2013, 2015, 2018, and 2020) of the China Health and Retirement Longitudinal Study (CHARLS), our study encompasses 82,802 individual observations. After data cleaning, the final analytical sample comprised 33,369 observations.
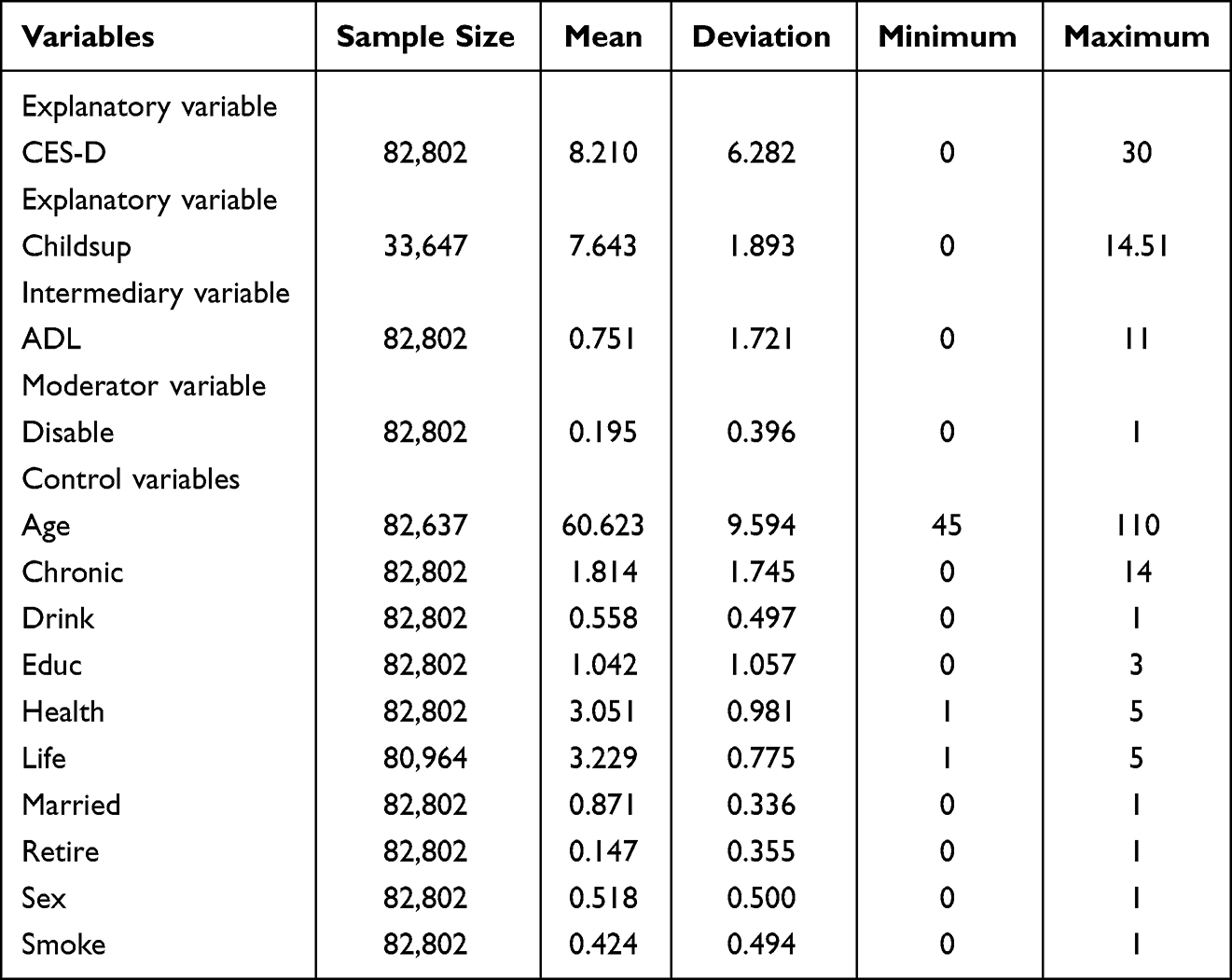 |
Table 1 Descriptive Statistical Analysis of Variables |
The dependent variable is the CES-D depression score, with a sample mean of 8.210 (SD = 6.282) and a maximum value of 30, indicating substantial individual differences in depressive symptoms among participants.
The key independent variable, intergenerational psychological capital, is operationalized through financial support provided by children (childsup). Among 33,647 valid observations, the average support score is 7.643 (SD = 1.893), suggesting a moderate concentration of support levels within the sample.
Functional autonomy deprivation is measured via the Activities of Daily Living (ADL) index, encompassing both Basic (BADL) and Instrumental (IADL) components, with scores ranging from 0 to 11. The sample mean is 0.751 (SD = 1.721), where higher scores denote greater functional impairment. This indicates that while most middle-aged and older adults maintain a degree of independence, functional decline remains a pertinent concern.
Structural functional disability (SFD) is represented by a binary variable indicating disability status. Approximately 19.5% of the sample reports having a disability, highlighting that nearly one-fifth of middle-aged and older adults experience significant functional limitations or major health issues.
Regarding control variables, the average age is 60.62 years, with a maximum of 110 years, reflecting considerable age diversity. Chronic conditions are prevalent, with individuals reporting an average of 1.814 diseases. Health behaviors reveal that 55.8% of participants consume alcohol, and 42.4% smoke. Educational attainment is relatively low, averaging 1.042 on a scale corresponding to primary to junior high school education. Marital status shows that 87.1% are married, and only 14.7% are retired. Gender distribution is nearly balanced, with males comprising 51.8% of the sample.
Overall, the sample exhibits typical characteristics of China’s middle-aged and elderly population: advanced age, significant health risks, and a high degree of economic dependency. These features provide a robust foundation for subsequent analyses of depressive symptom mechanisms and offer broad generalizability.
Pearson correlation analyses among all variables are detailed in Table 2. All correlation coefficients are below 0.4, and the average Variance Inflation Factor (VIF) is 1.43, mitigating concerns of multicollinearity. Most variables show significant correlations with depression levels, justifying their inclusion in regression models. Specifically, CES-D scores are significantly negatively correlated with intergenerational psychological capital (β=−0.128, p<0.001), providing preliminary support for Hypothesis H1. Further analysis indicates that intergenerational psychological capital is negatively correlated with functional autonomy deprivation (ADL), while depression levels are positively correlated with ADL, suggesting a potential mediating role of functional autonomy deprivation between intergenerational psychological capital and depression.
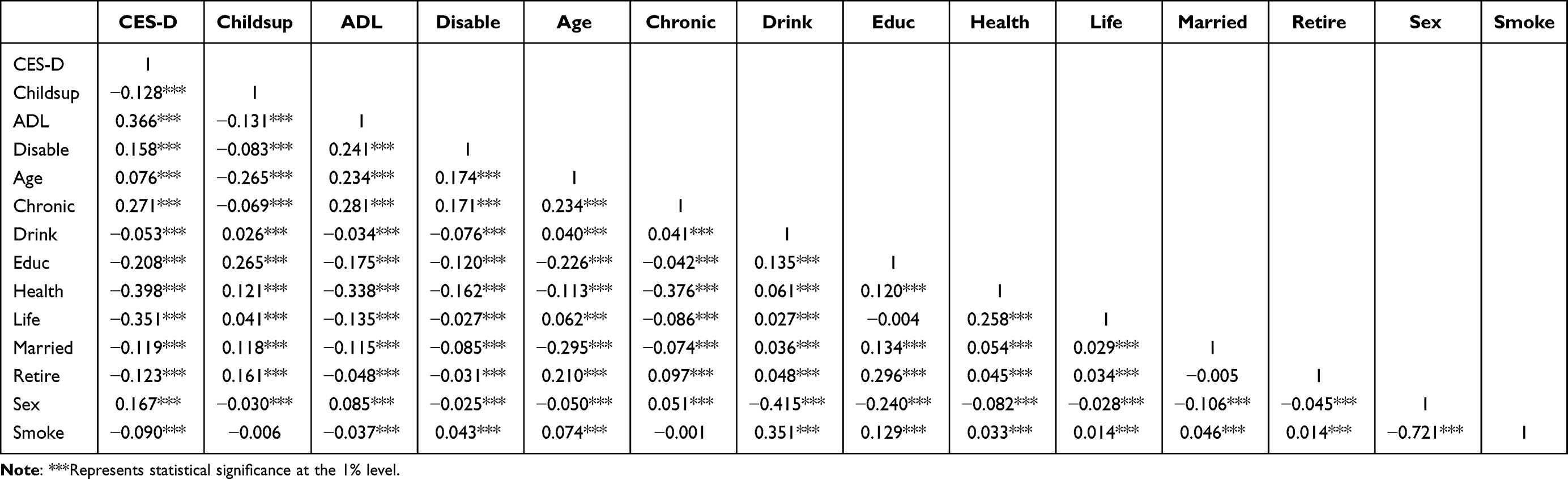 |
Table 2 Correlation Analysis of Key Variables |
Building upon these correlations, we constructed multiple regression models to explore the mechanisms through which intergenerational psychological capital, functional autonomy deprivation, and structural functional disability influence depression levels. Detailed regression results are presented in Table 3, with key findings summarized as follows:
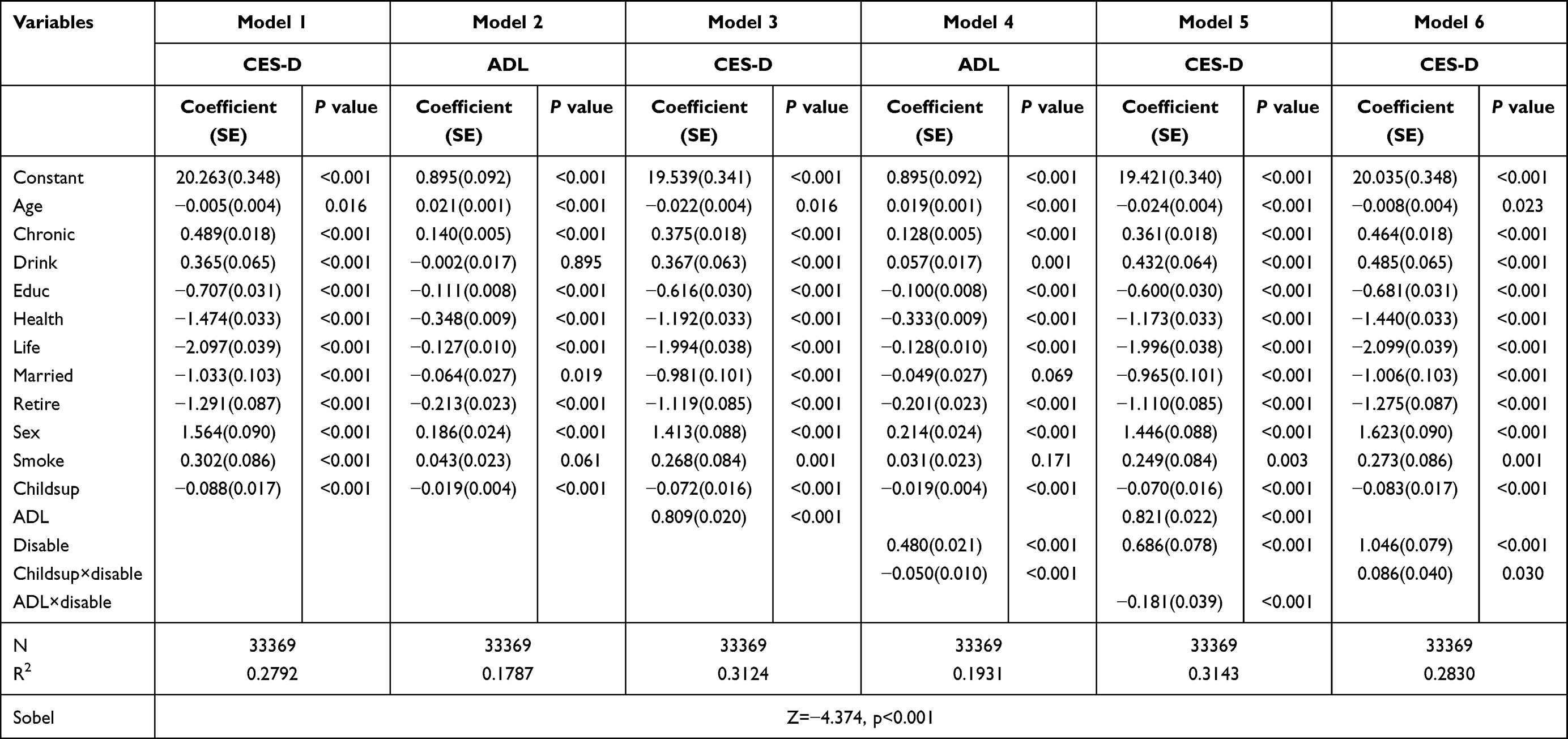 |
Table 3 Baseline Regression Results |
- Intergenerational Psychological Capital Alleviates Depressive SymptomsModel 1 in Table 3 examines the relationship between intergenerational psychological capital and depressive symptoms. The regression results indicate that higher levels of intergenerational psychological capital are associated with lower depressive symptom (β=−0.088, p<0.001), providing strong support for Hypothesis H1.
- Functional Autonomy Deprivation Partially Mediates the Relationship Between Intergenerational Psychological Capital and DepressionTo elucidate the pathway through which intergenerational psychological capital affects depressive symptoms among middle-aged and older adults, we introduced functional autonomy deprivation as a mediating variable. Utilizing baseline regression and Bootstrap methods, we tested the significance of the mediating effect. The analysis reveals that intergenerational psychological capital has a significant negative impact on depressive symptoms (β=−0.088, p<0.001), consistent with Model 1.
Further, as shown in Model 3 of Table 3, incorporating functional autonomy deprivation reduces the regression coefficient of intergenerational psychological capital from −0.088 to −0.072 (p< 0.001), indicating a partial mediation effect. Intergenerational psychological capital is significantly negatively associated with functional autonomy deprivation (β=−0.019, p<0.001), while functional autonomy deprivation significantly predicts higher depression levels (β=0.809, p<0.001). The Bootstrap method (5000 resamples) yields a 95% confidence interval for the indirect effect of [−0.023, −0.009], excluding zero and confirming the significance of the mediation effect. These findings collectively support Hypothesis H2.
The empirical results endorse the “intergenerational psychological capital—functional perception—mental health” pathway, suggesting that the alleviating effect of intergenerational psychological capital on depression is partially mediated by enhanced life control and autonomy. In other words, support from children not only provides emotional comfort but also promotes daily functioning, stabilizes emotional well-being, reinforces a sense of competence, reduces dependency, and mitigates feelings of helplessness.
This aligns with the theoretical expectations of the “resource conversion model”,70 which posits that the utility of resources is often realized through intermediary mechanisms within the individual’s capability system. Additionally, our study addresses the chain reaction between functional loss and psychological distress, highlighting that in the context of population aging and evolving family structures, children’s support serves as an embedded capability buffer, offering both emotional and functional protection.
In summary, functional autonomy deprivation partially mediates the relationship between intergenerational psychological capital and depressive symptoms, underscoring the importance of both emotional support and functional independence in maintaining mental health among the elderly. This provides new empirical evidence for understanding the complex interplay between support, function, and psychological well-being.
The Moderating Effect of Disability Status
To further investigate the mechanisms through which intergenerational psychological capital influences depressive symptoms, we introduced disability status as a moderating variable, focusing on its role within the “intergenerational psychological capital—functional autonomy deprivation—depressive symptoms” pathway. Drawing on the theoretical framework of “restrictive vulnerability context”,30,70 we posit that disability represents not only a physiological limitation but also a critical social context influencing resource reception, transformation, and psychological responses.
- Moderating Effect of Disability on the Relationship Between Intergenerational Psychological Capital and Functional Autonomy DeprivationAs illustrated in Model 4 of Table 3, disability status significantly negatively moderates the impact of intergenerational psychological capital on functional autonomy, with an interaction term coefficient of β=−0.050 (p<0.001). The moderation effect is depicted in Figure 2, where the solid line represents non-disabled individuals and the dashed line represents disabled individuals. The effect is more pronounced among the disabled group, indicating that financial support from children more effectively mitigates functional autonomy impairment in this population. These findings suggest that in the context of restrictive vulnerability, the marginal benefits of intergenerational psychological capital are amplified, potentially due to enhanced feelings of control and emotional support among disabled individuals.
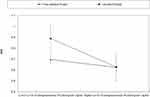
Figure 2 Moderating Effect of Disability on the Pathway from Intergenerational Psychological Capital to Functional Autonomy Deprivation.
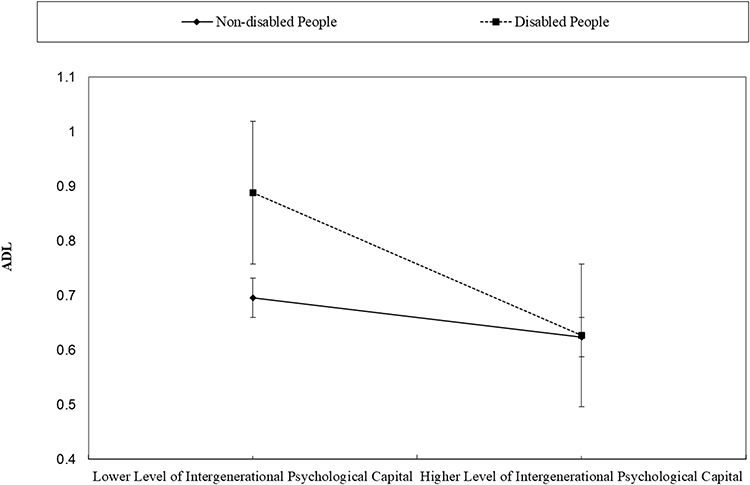
- Moderating Effect of Disability on the Relationship Between Functional Autonomy Deprivation and Depressive SymptomsIn examining the pathway from functional autonomy deprivation to depressive symptoms, disability status again exhibits a significant moderating effect, with an interaction term coefficient of β=−0.181 (p<0.001). As shown in Figure 3, the increase in depression levels associated with declining functional autonomy is less steep among disabled individuals compared to their non-disabled counterparts. This finding deviates from traditional views that disability and functional loss jointly exacerbate mental health risks. However, from the perspective of “constraint-based vulnerability”, individuals living with long-term functional limitations may develop stronger psychological adaptation mechanisms, including anticipatory adjustments, self-perception recalibration, and social rationalization of dependency.42 These mechanisms may attenuate the emotional response to further functional decline.
Moreover, disabled individuals often have higher expectations of social support,71 lower subjective social comparison benchmarks, and may benefit from institutionalized care mechanisms, all of which can alleviate the psychological impact of functional loss. Consequently, in our sample, the marginal effect of functional deprivation on depression is more pronounced among non-disabled individuals, explaining the significant negative interaction term. This highlights the heterogeneity in depression mechanisms across different health statuses and emphasizes the need for tailored policy and psychological interventions that consider varying emotional vulnerabilities to functional loss.
Figure 3 Moderating Effect of Disability on the Relationship Between Functional Autonomy Deprivation and Depressive Symptoms.
- The Moderating Role of Disability in the Relationship Between Intergenerational Psychological Capital and Depressive SymptomsTo further examine the differential processes of resource conversion under conditions of constrained vulnerability, this study investigates the moderating effect of physical disability on the relationship between intergenerational psychological capital and depressive symptoms. Results from the moderated regression analysis indicate that intergenerational psychological capital significantly predicts lower levels of depressive symptoms (β=−0.181, p<0.001). However, this effect varies significantly by disability status, as evidenced by a positive interaction term (childsup×disable: β=0.086, p=0.030), suggesting that disability status positively moderates this relationship.
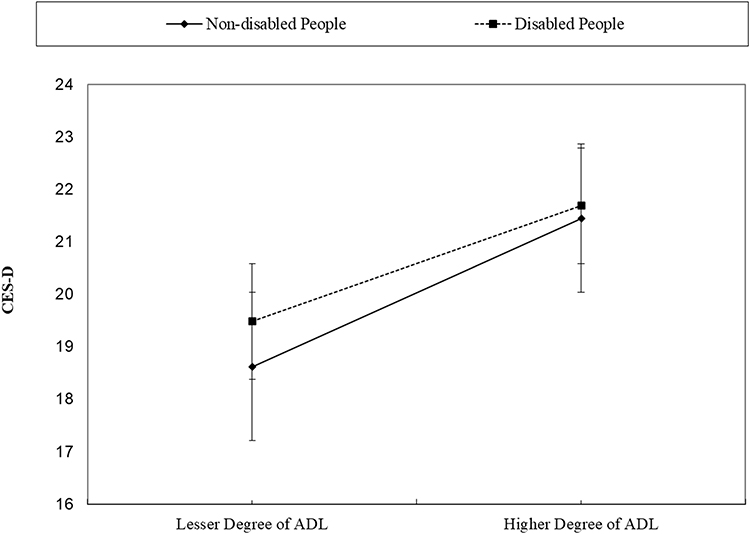
Specifically, as illustrated in Figure 4, the mitigating effect of intergenerational psychological capital on depressive symptoms is more pronounced among non-disabled individuals, whereas this psychological buffering effect is notably attenuated among those with disabilities. Although individuals with disabilities also benefit from support provided by their children, the restrictive and vulnerable contexts they face impose greater constraints on the internalization of intergenerational resources, thereby diminishing the marginal benefits for emotional improvement.
 |
Figure 4 Interaction Plot of the Moderating Effect of Disability on the Relationship Between Intergenerational Psychological Support and Depressive Symptoms. |
This finding deviates from the initial hypothesis that high-risk groups are more reliant on external support, indicating that physical disability not only constitutes an objective functional impairment but may also influence the perception and reception of social resources through subjective pathways. Individuals with disabilities, when confronted with chronic health issues, physical dependence, and social isolation, may exhibit more stable and defensive emotional responses, rendering them less susceptible to modulation by external support. This phenomenon, termed the “resource-blunting effect”, highlights potential limitations within the psychosocial support mechanisms for health-vulnerable populations.
Consequently, it is imperative to reassess the conditions under which intergenerational psychological capital operates, particularly concerning the obstacles in resource conversion and the diminished sense of subjective efficacy within disabled contexts. This insight not only enriches the theoretical framework concerning the pathways through which psychological capital influences depressive symptoms but also underscores the necessity of incorporating heterogeneous moderating mechanisms of structural health vulnerabilities in mental health interventions.
Conclusions and Discussion
Utilizing data from five waves (2011, 2013, 2015, 2018, and 2020) of the China Health and Retirement Longitudinal Study (CHARLS), this study systematically examines the mechanisms through which intergenerational psychological capital influences depressive symptoms among middle-aged and older adults in China, with particular emphasis on the mediating role of functional autonomy deprivation and the moderating effect of physical disability. The findings provide substantial theoretical and empirical insights that extend current understandings of the relationship between intergenerational support and psychological well-being, while also prompting critical reflection on the socio-cultural specificities of filial piety within contemporary Chinese society, including its evolving manifestations in the context of rapid urbanization and changing family structures.
This study provides evidence that financial support from adult children serves as a form of intergenerational psychological capital, which is associated with reduced depressive symptoms among middle-aged and older adults in China. This relationship is partially mediated through the preservation of functional autonomy and is further moderated by disability status. Rather than making generalizable claims about dignity or moral outcomes, we emphasize that support perceived as embedded with emotional meaning can strengthen psychosocial resources such as self-worth and autonomy, which in turn buffer against depression. These findings underscore the importance of culturally informed support mechanisms within families, particularly in contexts of health vulnerability. The following is a thorough discussion of the conclusion section.
First, this study contributes to the theoretical literature by reconceptualizing financial transfers from adult children not merely as material support, but as a form of intergenerational psychological capital that operates through multidimensional pathways. Building upon and extending classical intergenerational solidarity theory,72 the proposed framework emphasizes three interconnected mechanisms through which economic support acquires psychological significance. First, it functions as an emotional signal, tangibly embodying filial care and responsibility while affirming the continuity of intergenerational bonds. Second, it reinforces socially valued older adult identities by validating the role of the recipient within the family hierarchy, thereby enhancing perceived social worth. Third, it serves as a proxy for bundled support, in which monetary transfers often carry embedded emotional concern and symbolic attention to the parents’ overall well-being, reflecting the multiplex nature of intergenerational relationships in real-world contexts.
As a tangible form of intergenerational emotional expression and responsibility fulfillment, children’s financial assistance significantly alleviates social loneliness and psychological distress among the elderly.44 It reduces anxiety related to “aging without support” and economic insecurity, strengthens the sense of being needed, and thereby enhances life satisfaction and psychological stability.73 Empirical studies have also found that material assistance is often interpreted by the elderly as an “expression of love”, playing an unexpected role in maintaining psychological balance and emotional regulation.38
Second, beyond emotional care and resource transfer, children’s economic support constitutes an external source of “psychological capital”. While some studies suggest that high levels of adult children’s support may be detrimental or have minimal impact on the well-being of the elderly,55,74 this study provides evidence that intergenerational psychological capital significantly alleviates depressive symptoms among middle-aged and elderly individuals. Through economic and emotional support from children, individuals can acquire stronger psychological resources, significantly reducing negative emotional experiences and the risk of psychological distress. As a crucial dimension of social capital, intergenerational support plays a central role in protecting the mental health of middle-aged and elderly individuals. Children’s support not only mitigates anxiety caused by economic pressures but also enhances their sense of life control and social value, thereby significantly reducing the risk of depression. This study extends the theoretical boundaries of positive psychology concerning the composition and formation pathways of psychological capital.
Third, the analysis indicates that the deprivation of functional autonomy may partially mediate the relationship between intergenerational psychological capital and depressive symptoms. This suggests that the beneficial effect of intergenerational support is not confined to direct material or emotional provision but may also operate indirectly through mitigating losses in daily autonomy and self-efficacy. In particular, when older adults experience declines in functional capacity, sustained support from adult children can help counteract perceptions of incompetence or dependency, thereby lowering the likelihood of depression associated with diminished personal control. This finding resonates with the emphasis on autonomy within Self-Determination Theory,75 which highlights the centrality of agency and self-determination to psychological well-being in later life. In this sense, intergenerational psychological capital appears to function both as a direct buffer against distress and as an indirect reinforcement of competence and autonomy. This mechanism aligns with the “resource conversion model”, which posits that the translation of social resources into psychological health is contingent on intermediate capacities and contextual conditions.
Fourth, physical disability significantly moderates these mediating pathways. The analysis suggests that intergenerational psychological capital has a stronger alleviating effect on depressive symptoms among non-disabled individuals, likely reflecting their greater reliance on familial support. Under such circumstances, both tangible transfers and symbolic recognition from children may generate comparatively larger psychological and social-value benefits. At the same time, disability seems to weaken the mediating pathway from functional autonomy deprivation to depressive symptoms, implying that disabled older adults may show attenuated affective reactivity to functional decline. Moreover, the direct effect of intergenerational psychological capital on depressive symptoms appears less pronounced in this subgroup, which may reflect constraints imposed by reduced self-efficacy and weaker perceptions of available social resources.
However, in the pathway from functional autonomy deprivation to depressive symptoms, the affective reactivity of disabled individuals appears attenuated, implying relatively reduced psychological sensitivity to functional loss. More complex still, the direct effect of intergenerational psychological capital on depressive symptoms is significantly weaker among the disabled (as indicated by a positive interaction term). This suggests that the psychological benefits of support may be constrained by impaired self-efficacy and reduced perception of social resources among disabled older adults.
These results not only validate the chained mediation model involving intergenerational psychological capital, functional autonomy deprivation, and depression but also reveal the crucial moderating role of health vulnerability in the resource conversion process. The positive function of intergenerational psychological capital as a key family-level psychological resource is thus contingent on individuals’ functional status and sense of autonomy. Among those with poor health or functional limitations, there appears to be a “conversion barrier” that limits the assimilation of external support into psychological well-being. Consequently, policy interventions should aim not only to provide external support but also to enhance subjective efficacy and functional adaptation mechanisms to facilitate internalization of social resources. This finding underscores the need for targeted social policies that address the heightened vulnerability of disabled older adults, employing precise mechanisms to mitigate their psychological distress. Overall, the pattern offers partial support for the “social dependency-psychological recuperation” vulnerability hypothesis,70 while also highlighting the need for more nuanced theoretical and empirical attention to the complex interplay between disability, support, and mental health.
Limitations and Future Research Directions
First, although this study draws on multi-wave data, its observational design limits the ability to infer causality. Future research could employ strategies such as instrumental variables, propensity score matching, or quasi-experimental methods to enhance causal identification.
Second, the operationalization of intergenerational psychological capital (IPC) is primarily based on children’s financial support. While financial transfers provide a tangible and convenient proxy for familial resources, they cannot fully capture the interpretive and emotional dimensions of intergenerational relations. In reality, financial support often carries symbolic meanings—such as care, respect, or family solidarity—that contribute to psychological capital, yet these meanings were not directly measured. Moreover, non-material support, including emotional sustenance, companionship quality, and relational recognition, was omitted. This conceptual and methodological limitation suggests that future research should adopt multi-dimensional and mixed-methods approaches, integrating quantitative indicators with qualitative tools such as validated scales of perceived emotional support, in-depth interviews, or narrative analysis, to more accurately assess how older adults interpret and internalize intergenerational support as psychological resources.
Third, this study does not address the potential heterogeneous effects of intergenerational support. Factors such as children’s gender, marital status, living arrangements, or emotional intimacy with parents may condition both the formation of IPC and its effects on mental health. Future work should investigate these moderating mechanisms to provide a more nuanced understanding of family dynamics.
Fourth, while our models controlled for key demographic and health characteristics, we acknowledge, as rightly pointed out by reviewers, that they did not include more nuanced measures of social network structure and engagement, such as frequency of contact with children, co-residence status, or participation in community activities. The absence of these variables could potentially lead to an overestimation of the effect of intergenerational psychological capital by omitting confounding factors related to social embeddedness. Future research would greatly benefit from incorporating these sophisticated measures of social connectivity to obtain more precise estimates of the unique contribution of psychological resources derived from family relationships.
Fifth, the measurement of functional autonomy relies exclusively on ADL/IADL scales. Although widely used and objective, these scales do not capture subjective aspects such as perceived autonomy, dignity, or role identity. Employing validated psychosocial measures of autonomy would strengthen future investigations of how functional limitations influence psychological outcomes.
In summary, this study underscores that intergenerational psychological capital—conceptualized as resources derived from familial support—constitutes an important mechanism shaping mental health disparities among middle-aged and older adults in China. Functional autonomy emerges as a critical mediator, revealing the micro-level processes through which family structures affect psychological well-being. In the context of rapid population aging and evolving family arrangements, policymakers should not only strengthen public support systems but also foster collaborative, multi-dimensional mental health protection strategies involving families, communities, and societal institutions. Particular emphasis should be placed on functional compensation mechanisms and social integration initiatives that help older adults preserve autonomy and purpose in later life.
Data Sharing Statement
The datasets generated and analyzed during the current study are available in the CHARLS repository.
Ethics Statement
The data utilized in this study were obtained from the China Health and Retirement Longitudinal Study (CHARLS). Each wave of the CHARLS survey has received ethical approval from the Biomedical Ethics Committee of Peking University. The field implementation of this particular wave of the household survey was approved under the ethical review approval number: IRB00001052-11015. All participants provided written informed consent prior to their participation. According to Article 32, Items 1 and 2 of the Ethical Review Measures for Life Science and Medical Research Involving Human Subjects (issued on February 18, 2023, in China), studies using publicly available and de-identified data that comply with the scope of the original informed consent may be exempt from additional ethical review. Therefore, the present study meets these criteria and is exempt from further ethical approval.
Acknowledgments
The authors would like to express their sincere gratitude to Peking University and Wuhan University for providing the CHARLS database, which made this research possible. We are also deeply thankful to every collaborator for their dedicated efforts and invaluable contributions throughout this study. Furthermore, we are deeply honored to acknowledge Professor Liwen Zhang from Dalian University of Technology and Dr. Linfang Deng from Changzhou Institute of Technology. The exceptional insights they offered in their review comments were instrumental in refining this work, and the process of addressing their feedback has had a lasting impact on our development as researchers. Lastly, we extend our appreciation to the anonymous reviewers and the editorial team for their insightful comments and diligent work, which greatly improved the quality of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Yunnan Provincial Federation of Social Sciences - Baoshan University Joint Special Project (No. 24SKZXYB06) and the Yunnan Provincial Department of Education Scientific Research Fund Project (No. 2025J0986).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang J, Zhang J, Lin H, Han Y, Tu J, Nie X. Economic development, weak ties, and depression: evidence from China. J Affect Disord. 2023;334:246–257. doi:10.1016/j.jad.2023.04.097
2. Wang J, Zhang J, Lin H, et al. Come together! Population aggregation, strong tie, and individual depression: a moderated mediating investigation. Curr Psychol. 2024;43(44):34319–34334. doi:10.1007/s12144-024-06969-4
3. Guo Y. Examining how supervisor–student relationship types influence depression in doctoral students: the role of mediating mechanisms. New Dir Child Adolesc Dev. 2025;2025(1):6254499. doi:10.1155/cad/6254499
4. Wu P, Wang R, Lin H, Zhang F, Tu J, Sun M. Automatic depression recognition by intelligent speech signal processing: a systematic survey. CAAI Trans Intell Technol. 2023;8(3):701–711. doi:10.1049/cit2.12113
5. Chen L, Chang L, Lin H, Tu J, Zhou Y, Han Y. Savior or saboteur? A nationwide study on digital economy and depression in China. J Affect Disord. 2024;365:578–586. doi:10.1016/j.jad.2024.08.147
6. Liang Y, Xu N, Yang J, Wang J, Tu J, Lin H. Can network infrastructure construction alleviate individual depression? Evidence from a quasi-natural experiment of “broadband China. Curr Psychol. 2024;43(47):36425–36439. doi:10.1007/s12144-024-07085-z
7. Lou N, Guo R, Han Y, Tu J, Tam VWY, Lin H. The mental health benefits of smart cities: evidence from a quasi-natural experiment in China. J Manage Eng. 2025;41(1):4024065. doi:10.1061/JMENEA.MEENG-6321
8. Bartrés-Faz D, Demnitz-King H, Cabello-Toscano M, et al. Psychological profiles associated with mental, cognitive and brain health in middle-aged and older adults. Nat Ment Health. 2025;3(1):92–103. doi:10.1038/s44220-024-00361-8
9. Sang N, Liu RC, Zhang MH, et al. Changes in frailty and depressive symptoms among middle-aged and older Chinese people: a nationwide cohort study. BMC Public Health. 2024;24(1):301. doi:10.1186/s12889-024-17824-3
10. Malhi GS, Mann JJ. Depression. Lancet. 2018;392(10161):2299–2312. doi:10.1016/S0140-6736(18)31948-2
11. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
12. Whooley MA, Wong JM. Depression and cardiovascular disorders. Annu Rev Clin Psychol. 2013;9(1):327–354. doi:10.1146/annurev-clinpsy-050212-185526
13. Pinquart M, Sörensen S. Differences between caregivers and noncaregivers in psychological health and physical health: a meta-analysis. Psychol Aging. 2003;18(2):250–267. doi:10.1037/0882-7974.18.2.250
14. Wang R, Chen Z, Zhou Y, Shen L, Zhang Z, Wu X. Melancholy or mahjong? Diversity, frequency, type, and rural-urban divide of social participation and depression in middle- and old-aged Chinese: a fixed-effects analysis. Soc Sci Med. 2019;238:112518. doi:10.1016/j.socscimed.2019.112518
15. Liu Y, Liu Z, Liang R, Luo Y. The association between community-level socioeconomic status and cognitive function among Chinese middle-aged and older adults: a study based on the China health and retirement longitudinal study (CHARLS). BMC Geriatr. 2022;22(1):239. doi:10.1186/s12877-022-02946-3
16. Xiangli J, Chang L, Sheng R, et al. The U-shape association between noise and individual depression: nationwide longitudinal evidence from three waves of CHARLS. J Urban Health. 2025;102:593–603. doi:10.1007/s11524-025-00959-y
17. Luo X, Liu H, Sun Z, et al. Gender mediates the mediating effect of psychological capital between physical activity and depressive symptoms among adolescents. Sci Rep. 2025;15(1):10868. doi:10.1038/s41598-025-95186-5
18. Huang S, Yu Z, Shao Y, Yu M, Li Z. Relative effects of human capital, social capital and psychological capital on hotel employees’ job performance. Int J Contemp Hosp Manag. 2021;33(2):490–512. doi:10.1108/IJCHM-07-2020-0650
19. Khan A, Zeb I, Zhang Y, Fazal S, Ding J. Relationship between psychological capital and mental health at higher education: role of perceived social support as a mediator. Heliyon. 2024;10(8):e29472. doi:10.1016/j.heliyon.2024.e29472
20. Zhou X, Zhang S, Zhao X, Namasivayam K, Zheng H. How mentors inspire affective commitment in newcomers: the roles of servant leadership, psychological capital, and feedback-seeking behavior. Int J Hosp Manag. 2024;118:103677. doi:10.1016/j.ijhm.2023.103677
21. Song R, Song L. The relation between psychological capital and depression: a meta-analysis. Curr Psychol. 2024;43(20):18056–18064. doi:10.1007/s12144-024-05626-0
22. Luthans F, Youssef-Morgan CM. Psychological capital: an evidence-based positive approach. Annu Rev Organ Psychol Organ Behav. 2017;4:339–366. doi:10.1146/annurev-orgpsych-032516-113324
23. Fan L, Lei S. Financial well-being, family financial support and depression of older adults in China. Int J Bank Mark. 2023;41(6):1261–1281. doi:10.1108/IJBM-05-2022-0214
24. Cong Z, Silverstein M. Intergenerational support and depression among elders in rural China: do daughters‐in‐law matter? J Marriage Fam. 2008;70(3):599–612. doi:10.1111/j.1741-3737.2008.00508.x
25. Cong Z, Silverstein M. Intergenerational exchange between parents and migrant and nonmigrant sons in rural China. J Marriage Fam. 2011;73(1):93–104. doi:10.1111/j.1741-3737.2010.00791.x
26. Liu X, Wang Z, Zhang C, Zhang C, Peng L, Xu H. Effects of income on subjective well-being in the elderly: complete mediation roles of self-rated health and psychological capital. INQUIRY. 2024;61:469580241284967. doi:10.1177/00469580241284967
27. Li Q, Wu C. Social interaction, lifestyle, and depressive status: mediators in the longitudinal relationship between cognitive function and instrumental activities of daily living disability among older adults. Int J Environ Res Public Health. 2022;19(7):4235. doi:10.3390/ijerph19074235
28. Zhou L, Wang W, Ma X. The bidirectional association between the disability in activities of daily living and depression: a longitudinal study in Chinese middle-aged and older adults. BMC Public Health. 2024;24(1):1884. doi:10.1186/s12889-024-19421-w
29. Jiang CH, Zhu F, Qin TT. Relationships between chronic diseases and depression among middle-aged and elderly people in China: a prospective study from CHARLS. Curr Med Sci. 2020;40(5):858–870. doi:10.1007/s11596-020-2270-5
30. Aneshensel CS. Research in mental health: social etiology versus social consequences*. J Health Soc Behav. 2005;46(3):221–228. doi:10.1177/002214650504600301
31. Zhan Y, Zhan X, Wu M. From financial assistance to emotional care: the impact of intergenerational support on the subjective well-being of China’s elderly. J Happiness Stud. 2025;26(2):17. doi:10.1007/s10902-025-00861-z
32. Levitt MJ, Guacci N, Weber RA. Intergenerational support, relationship quality, and well-being: a bicultural analysis. J Fam Issues. 1992;13(4):465–481. doi:10.1177/019251392013004005
33. Wu Y, Dong W, Xu Y, et al. Financial transfers from adult children and depressive symptoms among mid-aged and elderly residents in China - evidence from the china health and retirement longitudinal study. BMC Public Health. 2018;18(1):882. doi:10.1186/s12889-018-5794-x
34. Xia W, van Wijngaarden JDH, Huijsman R, Buljac-Samardžić M. Effect of receiving financial support from adult children on depression among older persons and the mediating role of social participation. Int J Environ Res Public Health. 2022;19(19):12974. doi:10.3390/ijerph191912974
35. Zhang D, Wang Y, Jiao Y. The impact of social pension schemes on the mental health of the Chinese elderly: a mediating effect perspective of two-way intergenerational support. Int J Environ Res Public Health. 2022;19(14):8721. doi:10.3390/ijerph19148721
36. Liu L. The impacts of depression and chronic diseases on the health of older adults in China: evidence in a system equations framework. Chin Econ. 2022;55(5):343–368. doi:10.1080/10971475.2021.1996551
37. Wang C, Liu Z, Chen T, Wang J, Zhang X, Han B. Intergenerational support and depressive symptoms in old age: the difference between urban and rural China. Front Public Health. 2022;10:1007408. doi:10.3389/fpubh.2022.1007408
38. Huang F, Fu P. Intergenerational support and subjective wellbeing among oldest-old in China: the moderating role of economic status. BMC Geriatr. 2021;21(1):252. doi:10.1186/s12877-021-02204-y
39. Bolger N, Zuckerman A, Kessler RC. Invisible support and adjustment to stress. J Pers Soc Psychol. 2000;79(6):953–961. doi:10.1037/0022-3514.79.6.953
40. Teerawichitchainan B, Pothisiri W, Long GT. How do living arrangements and intergenerational support matter for psychological health of elderly parents? Evidence from Myanmar, Vietnam, and Thailand. Soc Sci Med. 2015;136–137:106–116. doi:10.1016/j.socscimed.2015.05.019
41. Ding Z, Yang Q, Xiong J, Yang L, Yin S. The relationship between filial expectations and depressive symptoms in Chinese older adults: the mediating role of intergenerational social support. J Adult Dev. 2021;28(2):162–169. doi:10.1007/s10804-020-09360-2
42. Verbrugge LM, Jette AM. The disablement process. Soc Sci Med. 1994;38(1):1–14. doi:10.1016/0277-9536(94)90294-1
43. Chi I, Chou KL. Depression predicts cognitive decline in Hong Kong Chinese older adults. Aging Mental Health. 2000;4:148–157. doi:10.1080/13607860050008673
44. Wangliu YQ, Li XH. Function limitations and depressive symptoms among older couples in China: the moderating role of intergenerational support. Curr Psychol. 2025;44(6):5329–5338. doi:10.1007/s12144-025-07603-7
45. Son JH, Kim SY, Won CW, Choi HR, Kim BS, Park MS. Physical frailty predicts medical expenses in community-dwelling, elderly patients: three-year prospective findings from living profiles of older people surveys in korea. Eur Geriatr Med. 2015;6(5):412–416. doi:10.1016/j.eurger.2015.05.003
46. Covinsky KE, Yaffe K, Lindquist K, Cherkasova E, Yelin E, Blazer DG. Depressive symptoms in middle age and the development of later-life functional limitations: the long-term effect of depressive symptoms. J Am Geriatr Soc. 2010;58(3):551–556. doi:10.1111/j.1532-5415.2010.02723.x
47. Ferraro KF, Shippee TP. Aging and cumulative inequality: how does inequality get under the skin? Gerontologist. 2009;49(3):333–343. doi:10.1093/geront/gnp034
48. Sumner J, Lim HW, Chong LS, Bundele A, Mukhopadhyay A, Kayambu G. Artificial intelligence in physical rehabilitation: a systematic review. Artif Intell Med. 2023;146:102693. doi:10.1016/j.artmed.2023.102693
49. Zakour MJ, Gillespie DF. Vulnerability theory. In: Community Disaster Vulnerability: Theory, Research, and Practice. Springer New York; 2013:17–35. doi:10.1007/978-1-4614-5737-4_2
50. Cheung CK, Ngan RMH. Improving older adults’ functional ability through service use in a home care program in Hong Kong. Res Soc Work Pract. 2005;15(3):154–164. doi:10.1177/1049731504270385
51. Carr D, Cornman JC, Freedman VA. Disability and activity-related emotion in later life: are effects buffered by intimate relationship support and strain? J Health Soc Behav. 2017;58(3):387–403. doi:10.1177/0022146517713551
52. King G, Willoughby C, Specht JA, Brown E. Social support processes and the adaptation of individuals with chronic disabilities. Qual Health Res. 2006;16(7):902–925. doi:10.1177/1049732306289920
53. Chen L, Chang L, Lin H, Tu J, Chen X, Han Y. Depressive disorder benefits of cities: evidence from the China. J Affect Disord. 2024;350:420–427. doi:10.1016/j.jad.2024.01.105
54. Han J, Zhang K, Lin H, Chang L, Tu J, Mai Q. The U-shape association between population agglomeration and individual depression: the role of dialect diversity. J Urban Health. 2024;101(4):740–751. doi:10.1007/s11524-024-00890-8
55. Silverstein M, Cong Z, Li S. Intergenerational transfers and living arrangements of older people in rural China: consequences for psychological well-being. J Gerontol B. 2006;61(5):S256–S266. doi:10.1093/geronb/61.5.S256
56. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of illness in the aged: the index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185(12):914–919. doi:10.1001/jama.1963.03060120024016
57. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily Living1. Gerontologist. 1969;9(3_Part_1):179–186. doi:10.1093/geront/9.3_Part_1.179
58. Njegovan V, Man-Son-Hing M, Mitchell SL, Molnar FJ. The hierarchy of functional loss associated with cognitive decline in older persons. J Gerontol A. 2001;56(10):M638–M643. doi:10.1093/gerona/56.10.M638
59. Gémes K, Forsell Y, Janszky I, et al. Moderate alcohol consumption and depression – a longitudinal population-based study in Sweden. Acta Psychiatr Scand. 2019;139(6):526–535. doi:10.1111/acps.13034
60. Cohen AK, Nussbaum J, Weintraub MLR, Nichols CR, Yen IH. Association of adult depression with educational attainment, aspirations, and expectations. Prev Chronic Dis. 2020;17:E94. doi:10.5888/pcd17.200098
61. Fletcher JM. Adolescent depression and educational attainment: results using sibling fixed effects. Health Econ. 2010;19(7):855–871. doi:10.1002/hec.1526
62. Peleg S, Nudelman G. Associations between self-rated health and depressive symptoms among older adults: does age matter? Soc Sci Med. 2021;280:114024. doi:10.1016/j.socscimed.2021.114024
63. Koivumaa-Honkanen H, Kaprio J, Honkanen R, Viinamäki H, Koskenvuo M. Life satisfaction and depression in a 15-year follow-up of healthy adults. Soc Psychiatry Psychiatr Epidemiol. 2004;39(12):994–999. doi:10.1007/s00127-004-0833-6
64. Pan L, Li L, Peng H, et al. Association of depressive symptoms with marital status among the middle-aged and elderly in rural China–serial mediating effects of sleep time, pain and life satisfaction. J Affect Disord. 2022;303:52–57. doi:10.1016/j.jad.2022.01.111
65. Kim JE, Moen P. Retirement transitions, gender, and psychological well-being: a life-course, ecological model. J Gerontol B. 2002;57(3):P212–P222. doi:10.1093/geronb/57.3.P212
66. Luger TM, Suls J, Vander Weg MW. How robust is the association between smoking and depression in adults? A meta-analysis using linear mixed-effects models. Addict Behav. 2014;39(10):1418–1429. doi:10.1016/j.addbeh.2014.05.011
67. Wen Z, Ye B. Analyses of mediating effects: the development of methods and models. Adv Psychol Sci. 2014;22(5):731. doi:10.3724/SP.J.1042.2014.00731
68. Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol Methodol. 1982;13:290–312. doi:10.2307/270723
69. Wen Z, Ye B. Different methods for testing moderated mediation models: competitors or backups? Acta Psychol Sin. 2014;46(5):714. doi:10.3724/SP.J.1041.2014.00714
70. Pearlin LI, Menaghan EG, Lieberman MA, Mullan JT. The stress process. J Health Soc Behav. 1981;22(4):337. doi:10.2307/2136676
71. Lippold T, Burns J. Social support and intellectual disabilities: a comparison between social networks of adults with intellectual disability and those with physical disability. J Intellect Disabil Res. 2009;53(5):463–473. doi:10.1111/j.1365-2788.2009.01170.x
72. Antonucci TC, Jackson JS, Biggs S. Intergenerational relations: theory, research, and policy. J Soc Issues. 2007;63(4):679–693. doi:10.1111/j.1540-4560.2007.00530.x
73. Thoits PA. Mechanisms linking social ties and support to physical and mental health. J Health Soc Behav. 2011;52(2):145–161. doi:10.1177/0022146510395592
74. Umberson D. Relationships between adult children and their parents: psychological consequences for both generations. J Marriage Fam. 1992;54(3):664–674. doi:10.2307/353252
75. Van Lange PAM, Higgins ET, Kruglanski AW. Handbook of Theories of Social Psychology. Sage; 2011:1–568.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.