Back to Journals » Local and Regional Anesthesia » Volume 13
Interfascial Plane Blocks and Laparoscopic Abdominal Surgery: A Narrative Review
Authors Jones JH ![]() , Aldwinckle R
, Aldwinckle R
Received 18 July 2020
Accepted for publication 23 September 2020
Published 23 October 2020 Volume 2020:13 Pages 159—169
DOI https://doi.org/10.2147/LRA.S272694
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
James Harvey Jones, Robin Aldwinckle
Department of Anesthesiology and Pain Medicine, University of California Davis Medical Center, Sacramento, CA, USA
Correspondence: James Harvey Jones
Department of Anesthesiology and Pain Medicine, University of California Davis Medical Center, 4150 V Street, PSSB Suite 1200, Sacramento, CA 95817, USA
Tel +1 (916) 734-5031
Fax +1 (916) 734-7980
Email [email protected]
Abstract: Laparoscopic abdominal surgery has become a mainstay of modern surgical practice. Postoperative analgesia is an integral component of recovery following laparoscopic abdominal surgery and may be improved by regional anesthesia or intravenous lidocaine infusion. There is inconsistent evidence supporting the use of interfascial plane blocks, such as transversus abdominis plane (TAP) blocks, for patients undergoing laparoscopic abdominal surgery as evidenced by variable patterns of local anesthetic spread and conflicting results from studies comparing TAP blocks to local anesthetic infiltration of laparoscopic port sites and multimodal analgesia. Quadratus lumborum (QL) and erector spinae plane (ESP) blocks may provide greater areas of somatic analgesia as well as visceral analgesia, which may translate to more significant clinical benefits. Aside from the locations of the surgical incisions, it is unclear what other factors should be considered when choosing one regional technique over another or deciding to infuse lidocaine intravenously. We reviewed the current literature in attempt to clarify the roles of various regional anesthesia techniques for patients undergoing laparoscopic abdominal surgery and present one possible approach to evaluating postoperative pain.
Keywords: transversus abdominis plane block, interfascial plane block, laparoscopic abdominal surgery, pain
Introduction
There are several options for analgesia following laparoscopic abdominal surgery.1,2 It is unclear, however, if regional anesthesia is a beneficial component of multimodal analgesia for all laparoscopic abdominal surgeries.3 Peripheral regional techniques may differ for upper and lower abdominal surgeries, thus presenting a challenge when reviewing their clinical benefits, and particularly when comparing these blocks to epidural analgesia.4,5 Epidural analgesia has been essential to postoperative outcomes related to enhanced recovery after colorectal surgery.6 However, interfascial plane blocks may not reliably produce clinically significant benefits when compared to multimodal analgesia.3
Studies investigating transversus abdominis plane (TAP) blocks for laparoscopic abdominal surgery present conflicting results. Numerous studies suggest that TAP blocks should be incorporated into ERAS protocols.7–10 In fact, a review of laparoscopic urological surgery concluded that TAP block should be “an indispensable component” of these protocols.10 However, recent reviews in major anesthesia journals remain skeptical and suggest that TAP block may not offer clinically significant benefits in analgesia following laparoscopic abdominal surgery when added to multimodal analgesia, as presented in Table 1.3,11 Furthermore, a meta-analysis investigating TAP block for abdominal surgeries in adult patients concluded “marginal clinical benefit likely from [the reported] magnitude of opioid reduction” as well as “substantial publication bias.”11
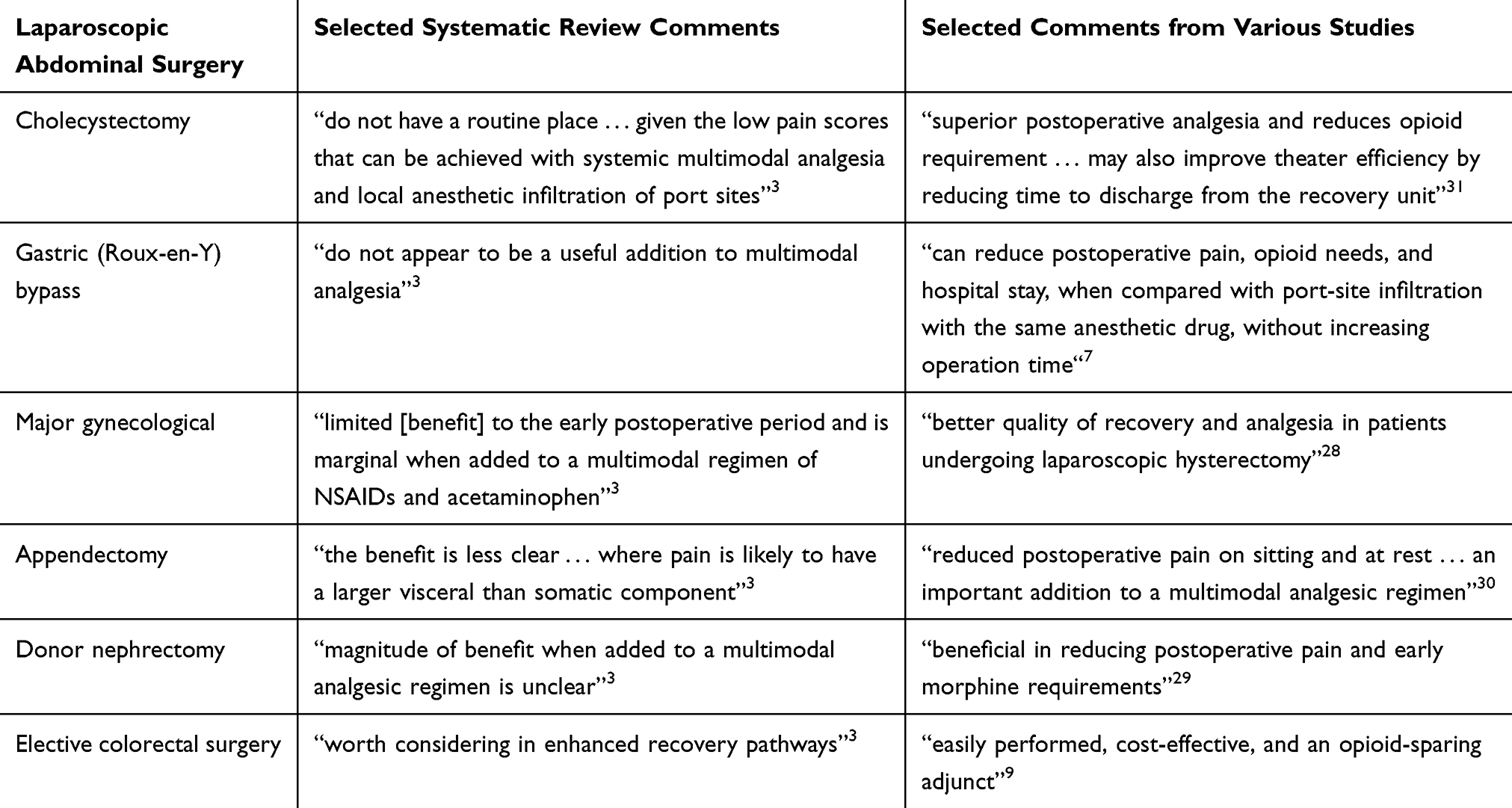 |
Table 1 Selected Comments in Literature Regarding TAP Blocks for Laparoscopic Abdominal Surgeries |
Strong evidence supports the use of continuous intravenous lidocaine infusions to decrease pain scores, opioid consumption, and duration of ileus for patients following laparoscopic abdominal surgeries.12–20 The risk of local anesthetic systemic toxicity (LAST), however, precludes the simultaneous administration of local anesthetic via TAP – or other interfascial plane – block and continuous intravenous infusion. The risk of LAST may also preclude intraoperative lidocaine infusion followed by postoperative interfascial plane block. Therefore, perioperative consultants must select the most appropriate route of local anesthetic administration – intravenous, subcutaneous, neuraxial, paravertebral, or interfascial.
Reviews and meta-analyses of analgesic techniques for laparoscopic surgery disagree regarding which approach to patient care is most appropriate.2,3,6,9–11,21–26 Additional investigation is necessary to more clearly define patient groups that most benefit from TAP blocks (and other regional anesthesia techniques) and lidocaine infusions. Current literature suggests that each technique may offer some clinical benefits. However, it is unclear how to decide on one technique over the other. This review presents one plausible approach to treating pain following laparoscopic, non-colorectal, surgery utilizing Carnett’s sign.
Methods
Articles were identified with PubMed database searches utilizing the following key terms in the English language: “laparoscopic surgery”; “abdominal surgery”; “regional anesthesia”; “transversus abdominis plane block”; “quadratus lumborum block”; “retrolaminar block”; “erector spinae plane block”; “modified BRILMA”; and “serratus intercostal plane block.” Additional studies were identified by reviewing the bibliographies of selected publications.
Transversus Abdominis Plane Blocks
Numerous studies indicate that TAP blocks can effectively provide analgesia following laparoscopic abdominal surgery, thus increasing their popularity in ERAS protocols.7–10,27–31 However, anesthesia and pain medicine literature continue to question the utility of TAP blocks in these cases.3,11 This discrepancy in evidence, or interpretation of evidence, makes it difficult to identify best clinical practices. Table 1 displays representative comments from current literature that demonstrate this controversy. There are several limitations of TAP blocks including variable spread of local anesthetic; unclear superiority to local anesthetic infiltration of trocar insertion sites and multimodal analgesia; and unclear clinical impact.
Local Anesthetic Spread
TAP blocks depend on high volumes of local anesthetic injected between the internal oblique and transversus abdominis muscles to anesthetize the following nerves: intercostal (T7-T11), subcostal (T12), iliohypogastric (L1), and ilioinguinal (L1).3,32 TAP blocks were originally performed without ultrasound-guidance utilizing the “lumbar triangle of Petit,” which has the following boundaries: posteriorly, the latissimus dorsi muscle; inferiorly, the iliac crest; anteriorly, the external oblique muscle; and the floor of this “triangle” is made up of the internal oblique muscle.33 The exact size and location of the “lumbar triangle of Petit” varies greatly, particularly in obese patients.34 Therefore, ultrasound-guided techniques supplanted the blind approach, but produced variable results.
Ultrasound-guided TAP blocks are performed in various locations and the expected pattern of analgesia varies greatly depending on the approach.35 For upper abdominal surgeries, the subcostal approach is most recommended as this may provide analgesia for the T6-T9 anterior cutaneous nerves.36 For lower abdominal surgeries, the lateral or posterior approaches are both appropriate.37 Widespread cutaneous sensory analgesia of the midabdomen has also been suggested with oblique subcostal TAP.38
Prior studies have demonstrated inconsistent cutaneous sensory loss from ultrasound-guided TAP blocks.39,40 A study on healthy volunteers showed contrast enhancement posteriorly to the paravertebral space with landmark-guided TAP block whereas injections via subcostal and mid-axillary approaches spread more anteriorly.41 Furthermore, cadaveric dissections have demonstrated the complicated branching patterns of thoracolumbar nerves, which may account for variability in analgesia patterns.42 Overall, sensory blockade with TAP blocks is commonly described as patchy with areas of cutaneous analgesia that are not consistent with classic dermatomal distribution patterns.3,40,41,43,44 These variable objective signs of nerve blockade make it difficult to study and assess the clinical effectiveness of TAP blocks.
Multimodal Analgesia
TAP blocks have not consistently demonstrated clinically significant, superior analgesia when compared to local anesthetic infiltration of trocar insertion sites and multimodal analgesia.3
If TAP blocks only provide analgesia via blockade of cutaneous nerves, then superior analgesia would not be expected with TAP blocks compared to local anesthetic infiltration of trocar insertion sites, yet this is not consistently supported by current literature. A study comparing bilateral TAP blocks to local anesthetic infiltration reported no statistically significant differences in pain scores at 4 hours and 24 hours following laparoscopic cholecystectomy as well as no significant difference in analgesic use during the first 24 hours postoperatively.45 In contrast, a meta-analysis comparing TAP block with wound infiltration for laparoscopic and open abdominal surgeries reported superior analgesia (as measured by decreased pain scores at rest and with movement at 8 hours and 24 hours postoperatively) in patients who had received TAP blocks.26 Therefore, our current understanding of TAP blocks and pain following abdominal surgery is likely incomplete.
Analgesia from TAP blocks may not be limited to direct, peripheral nerve blockade. Systemic analgesia via vascular and lymphatic transport may also occur as well as posterior spread to the paravertebral space.41 A prospective, randomized study investigated the potential benefits of TAP blocks when added to local anesthetic infiltration following laparoscopic cholecystectomy.46 The authors concluded that the combination of local anesthetic infiltration of trocar insertion sites and ultrasound-guided posterior TAP block did not yield statistically significant differences in VAS (Visual Analog Scale) scores compared to local anesthetic infiltration alone, and TAP blocks were associated with lower patient satisfaction.46
Multimodal analgesia may limit the ability of investigators to identify clinically significant differences in analgesia with TAP blocks compared to control despite statistically significant differences. A randomized, double-blind study compared bilateral ultrasound-guided posterior TAP blocks to placebo blocks in patients following laparoscopic cholecystectomy.47 VAS pain scores while coughing were significantly lower in the TAP group versus the placebo group [area under the curve for the first 24 postoperative hours (AUC/24 h) (SD): 26 mm (13) versus 34 mm (18); P = 0.05; 95% confidence interval: 0.5–15 mm], and median morphine consumption 0–2 hours postoperatively was less in the TAP group versus placebo group [median morphine consumption (interquartile range): 5 mg (0–5) vs 7.5 mg (5–10)].47 Although this study demonstrated beneficial effects of TAP blocks in reducing pain and opioid requirements, the investigators concluded that these effects were “probably rather small.”47 As shown in Table 1, the benefits of TAP blocks are likely of limited clinical significance when added to multimodal analgesia for many laparoscopic abdominal surgeries.3
The high volume of local anesthetic required for TAP blocks may preclude the safe administration of intravenous lidocaine via continuous infusion. Therefore, the anesthetist must decide if greater benefit would be expected from intravenous lidocaine as opposed to TAP block. Multiple studies on patients undergoing open or laparoscopic abdominal surgeries have demonstrated enhanced analgesia with lidocaine infusions.23,24,48,49 Unlike TAP blocks, lidocaine infusions are easy to administer despite patient factors (such as morbid obesity) and the efficacy of intravenous lidocaine is not impacted by the location of surgical incisions. Furthermore, lidocaine infusions do not require additional skillsets (such as ultrasound-guided needle advancement or structure recognition with sonoanatomy), are not invasive, and do not present risks of infection, bleeding, and needle trauma. Additionally, lidocaine infusions may be particularly effective in patients with chronic pain conditions, which may be challenging to treat perioperatively.50
Clinical Impact
Statistically significant improvements in postoperative analgesia and reductions in opioid consumption may only be clinically significant if they promote enhanced recovery after surgery or lead to higher quality of recovery. Components of ERAS protocols that may be impacted by postoperative pain management include early post-procedure mobilization, early transition to oral pain medications, increased patient satisfaction with care, and decreased length of hospital stay. Measurements of quality of recovery, as determined by the QoR-15 questionnaire, that may be associated with postoperative pain management include sleep, pain intensity (moderate or severe), and nausea or vomiting.51 Studies have demonstrated improvements in the components of ERAS protocols with TAP blocks.7–10 However, a large meta-analysis and comprehensive systematic review challenge these proposed benefits.3,11
Statistically significant reductions in opioid consumption may not always be clinically significant and warrant invasive pain therapies. A systematic review investigated the effects of TAP block on early and late pain at rest and movement as well as opioid consumption following laparoscopic surgery.21 Significant improvements were noted in early pain at rest [weighted mean difference (WMD) (99% CI) −2.41 (−3.6 to −1.16) (0–10 numerical scale), P < 0.001] and late pain at rest [WMD (99% CI) −1.33 (−2.19 to −0.48) (0–10 numerical scale), P = 0.001] in patients who received TAP blocks as well as reductions in postoperative opioid consumption [WMD (99% CI) −5.74 (−8.48 to −2.99) mg IV morphine, P < 0.001].21 Notably, the effect of TAP block on late pain at rest was greater for lower quality studies and TAP block was not superior to control in reducing early and late pain with movement.21 In response to this review’s reported decrease in opioid consumption with TAP block, a systematic review commented that only a “marginal clinical benefit [is] likely from this magnitude of opioid reduction in the postoperative period” and surmised substantial publication bias with respect to reductions in opioid consumption and effects on analgesia.11
Pain following laparoscopy is multifactorial and includes tissue trauma from trocar insertion sites, inflammation, and pneumoperitoneum.1,52,53 Presumably, the main difference in pain between laparoscopic abdominal surgeries is varying amounts of visceral manipulation. Therefore, all laparoscopic abdominal surgeries would be expected to experience a similar degree of benefit from the appropriate TAP approach (subcostal, lateral, or posterior). This theory is confounded by a review that concluded that TAP blocks are “worth considering” for elective laparoscopic colorectal surgeries, but not recommended routinely for other laparoscopic abdominal surgeries.3
Quadratus Lumborum Block
There are three main injection sites for QL blocks, as demonstrated by their nomenclature. Lateral QL blocks (previously known as QL1 blocks) are performed by injecting local anesthetic at the lateral border of the QL muscle and deep to the transversus abdominis aponeurosis, thus distinguishing it from a posterior TAP block.54 Posterior QL blocks (previously known as QL2 blocks) are performed by injecting local anesthetic posterior to the QL muscle and anterior to the erector spinae muscles.55 Transmuscular, or anterior, QL blocks (previously known as QL3 blocks) are performed by injecting local anesthetic between the QL and psoas muscles.56 Overall, successful QL blocks are expected to provide analgesia for the T7-T12 dermatomes, but variable patterns of analgesia have been reported with each approach.25,57–60
The mechanism by which QL block provides analgesia remains unclear. The anterior and middle layers of the thoracolumbar fascia envelope the QL muscle before inserting on the lumbar transverse processes, thus providing access to the paravertebral space. Therefore, QL blocks may serve as indirect paravertebral blocks and lead to more widespread analgesia compared to peripheral truncal blocks.25,61 However, paravertebral spread of local anesthetic with QL block has been challenged by fresh cadaver dissections and alternative mechanisms for analgesia have been suggested, including blockade of pain receptors within the thoracolumbar fascia.62,63
QL blocks require visualization of deep structures, thus patient factors (such as obesity) and provider inexperience with ultrasound-guided regional anesthesia may preclude safely performing these blocks. Various complications have been reported with QL block, which may impede patient recovery and increase hospital length of stay. For example, spread of local anesthetic to the paravertebral space may lead to sympathectomy and hypotension.64 Lower extremity weakness has also been reported.57 Abdominal branches of lumbar arteries pass between the erector spinae and quadratus lumborum muscles. Therefore, the risk of bleeding may be higher with QL blocks than more peripheral truncal blocks, particularly in the presence of anticoagulation, and may require compliance with appropriate guidelines. Lastly, poor recognition of sonoanatomy and improper needle guidance may cause direct trauma to structures near the QL muscle or within the retroperitoneal space.
Quadratus Lumborum Block and Laparoscopic Abdominal Surgery
QL blocks may improve analgesia following laparoscopy.25,65–67 A prospective randomized controlled study reported statistically significant reductions in postoperative pain with movement and at rest with posterior QL block compared to control up to 24 hours following laparoscopic gynecologic surgery.65 The posterior QL block was also shown to improve postoperative pain and decrease tramadol usage for the first 24 hours postoperatively in patients following laparoscopic cholecystectomy compared to sham block in a double blind study.66 This result was confounded by a randomized controlled trial that reported no statistically significant differences with posterior QL block compared to placebo in patients undergoing laparoscopic gynecological surgery with regards to the following outcomes: quality of recovery, postoperative pain, and postoperative fentanyl requirements.68 Transmuscular QL block was shown to decrease opioid consumption and improve postoperative outcomes (such as recovery of intestinal function, mobilization time, and incidence of postoperative nausea and vomiting) in patients following laparoscopic nephrectomy.67
The current medical literature has not consistently reported statistically significant differences in analgesia or quality of recovery when comparing QL blocks to TAP blocks. A prospective, randomized controlled study comparing ultrasound-guided subcostal TAP block and posterior QL block in patients following laparoscopic cholecystectomy demonstrated comparable postoperative fentanyl requirements as well as similar VAS and DVAS (Dynamic Visual Analog Scale) scores immediately postoperatively and at 1 hour, 6 hours, 12 hours, and 24 hours postoperatively.69
Overall, there appears to be some evidence suggesting the effectiveness of QL block in providing analgesia following laparoscopy.25,65–67 Because analgesia with QL block rivals, but does not always exceed that achieved from TAP block, the role of QL block requires additional investigation. The potential for paravertebral spread and resultant visceral analgesia may favor QL block over TAP block for patients expected to have significant visceral pain due to chronic pain syndromes, opioid tolerance, or significant intraoperative visceral manipulation.60 Additionally, the QL muscle is more posterior than the internal oblique and transversus abdominis muscles, thus allowing for the placement of continuous QL block catheters perioperatively without interfering with the surgical field. Therefore, QL blocks may be appropriate alternatives to TAP blocks when abdominal wall musculature is distorted.
Erector Spinae Plane Block
Analgesia from erector spinae plane (ESP) blocks depends on the spread of local anesthetic into the paravertebral space via the costotransverse foramina.70 ESP blocks were originally used to treat thoracic neuropathic pain.70 The role of ESP blocks has now expanded to include postoperative analgesia in patients following thoracic and abdominal surgeries. The optimal site for injection depends on the desired dermatomal coverage. For abdominal surgeries, local anesthesia is deposited beneath the erector spinae muscle at the levels of the T7-T9 transverse processes to anesthetize the T7-T11 dermatomes.71 Retrolaminar block is performed more medially, on the lamina, and is expected to provide a similar distribution of analgesia when compared to ESP block, yet the utility of retrolaminar block for laparoscopic abdominal surgery has not been thoroughly investigated.72
Erector Spinae Plane Block and Laparoscopic Abdominal Surgery
Evidence promoting ESP blocks for laparoscopic abdominal surgery comes predominantly from studies investigating pain following laparoscopic cholecystectomy.73–76 A prospective, randomized controlled study demonstrated effective analgesia with ESP block as evidenced by lower pain scores in the first 3 hours following laparoscopic cholecystectomy as well as decreased tramadol consumption for the first 12 hours postoperatively.75 In a single blind, prospective, randomized trial, ESP block was shown to reduce postoperative tramadol consumption and pain scores compared to oblique subcostal TAP block in patients following laparoscopic cholecystectomy.73
Overall, ESP blocks appear to provide similar analgesia following laparoscopic cholecystectomy when compared to QL block.77 It is unclear, however, if ESP blocks improve additional postoperative outcomes, such as resolution of ileus, patient mobilization, and hospital length of stay. Similar to QL blocks, the anticipated spread of local anesthetic into the paravertebral space with ESP blocks may yield greater analgesia for patients with visceral hyperalgesia secondary to chronic pain syndromes or opioid tolerance.
Other Interfascial Plane Blocks
Analgesia for open abdominal surgeries has been demonstrated following blockade of the lateral branches of the intercostal nerves in the mid-axillary line at the 8th rib, a technique called the modified BRILMA, or serratus intercostal plane block (SIPB).78,79 The analgesic efficacy of this block has been questioned for midline abdominal incisions, however, and may require concomitant rectus sheath blocks to provide significant analgesia following laparoscopic cholecystectomy.80 Blockade of thoracoabdominal nerves through perichondrial approach (TAPA) has provided effective analgesia for various open and minimally invasive procedures.81,82 Rectus sheath blocks and ilioinguinal/iliohypogastric blocks may also provide clinically significant analgesia following laparoscopic abdominal surgeries, but are limited in their expected ranges of analgesia.83,84 Further investigation is needed to draft clinical guidelines regarding each regional technique.
Approaches to Clinical Practice Today
There are markedly different recommendations in the current literature regarding the role of TAP blocks for laparoscopic abdominal surgery.1,3,7–11,21,22,28–31,35,45,47,85,86 Although lidocaine infusions, TAP blocks, QL blocks, and ESP blocks offer several potential benefits to patients, it is unclear what factors should be considered when deciding among them.
Intraperitoneal Access and Visceral Pain
Multiple approaches describe safe entrance to the intraperitoneal cavity, which may affect options for regional anesthesia. The open-entry, or Hasson, technique describes placement of a blunt trocar through a subumbilical incision to insufflate the intraperitoneal cavity.87 In contrast, the closed-entry technique describes insertion of a Veress needle in the umbilical region to insufflate the intraperitoneal cavity.87 Abdominal wall nerve blocks that provide analgesia to the T10 thoracoabdominal nerve should provide sufficient cutaneous analgesia for the Hasson and closed-entry techniques. Alternatively, Lee-Huang point or Palmer’s point may serve as more appropriate entry sites for patients with prior abdominal operations or significant scar tissue.87 With these alternative entry points, analgesia of thoracoabdominal nerves higher than T10 would be required. Therefore, lateral or posterior TAP blocks may not provide sufficient cutaneous analgesia. Cutaneous analgesia of only the entry point used for intraperitoneal access, however, is not entirely sufficient for postoperative analgesia following laparoscopic surgery. It should be further emphasized that analgesia from TAP block may not be dermatomal.40,43,44
Given the proximity of QL and ESP blocks to the paravertebral space, these techniques may provide more reliable visceral analgesia compared to TAP blocks. Therefore, the impact (or expected impact) of visceral pain on a patient’s postoperative course may serve as a key element when deciding between regional anesthesia techniques. Additionally, the posterior needle insertion sites used for QL and ESP blocks may allow for catheters to be placed preoperatively that will not interfere with the surgical field.
Regional Anesthesia Following Failure of Multimodal Analgesia
Current evidence suggests that TAP blocks may not provide clinically significant benefits beyond local anesthetic infiltration and multimodal analgesia for many laparoscopic abdominal surgeries.3,11 However, all patient populations have not been equally represented in the medical literature. For example, patients with chronic abdominal pain, hyperalgesia or allodynia of the abdominal wall, or opioid tolerance may experience clinically significant improvements in analgesia and reductions in opioid consumption with TAP blocks.
One possible approach to pain following laparoscopy is to first determine if the pain is originating from viscera or the abdominal wall. Subjective descriptions of pain as being diffuse or poorly localized may suggest visceral pain.88 Testing for Carnett’s sign may provide a more objective method to distinguish abdominal wall pain from visceral pain.89–91 To perform this test, the site of maximum abdominal tenderness is identified; the patient then folds his or her arms before lifting the head and shoulders off of the examination table, thus contracting the abdominal wall musculature. If this maneuver increases pain or causes no change in pain (a positive Carnett’s sign), then pain at the abdominal wall is an important element of that patient’s pain complaint. If this maneuver decreases pain (a negative Carnett’s sign), then the patient’s pain is likely of visceral origin. Carnett’s sign has been validated for helping diagnose chronic abdominal wall pain in outpatient settings and used in the acute care setting, but has not been validated for postoperative use with abdominal incisions.89–91 The utility of Carnett’s sign in selecting one regional anesthesia technique over another in the postoperative setting remains unclear. Although interfascial plane blocks that are more likely to provide visceral analgesia may be one option for patients with a negative Carnett’s sign, this approach may not be suitable for evaluating pain after all laparoscopic surgeries or for all interfascial plane blocks.
Other factors that may help identify the most appropriate nerve block include patient comorbidities, such as history of chronic abdominal pain (and the potential for allodynia or hyperalgesia of the abdomen), opioid use (and associated opioid tolerance), and anticoagulation; the specific surgery, such as the locations of incisions, extent of visceral manipulation (and expected amount of visceral pain), and whether or not local anesthetic catheters should be placed preoperatively; and the experience of the proceduralist with ultrasound-guided regional anesthesia. These expanded, more patient-focused, ERAS protocols may consist of QL or ESP catheters for cases with significant visceral manipulation or for patients who suffer from chronic pain. These factors, along with many others, are presented in Table 2. It should be noted that the elements of this table are only theoretical considerations in selecting one block over another and not currently supported by evidence. Further research is needed to identify patient populations and surgeries that would most benefit from one technique over the other, or when subcutaneous infiltration of surgical sites in combination with multimodal analgesia would serve as the most appropriate therapy.
 |
Table 2 Factors That Might Aid in Selecting One Analgesia Technique Over Another |
Conclusions
Analgesia following laparoscopic abdominal surgery is a key component of perioperative management. TAP, QL, and ESP blocks provide varying levels of cutaneous analgesia with or without visceral analgesia. However, there are significant limitations in interpreting the current evidence regarding these techniques, most notably because of small sample sizes, exclusion of patients with chronic pain conditions, and a paucity of studies that compare these techniques to each other and subcutaneous infiltration of surgical sites in a prospective, randomized design. Intravenous lidocaine infusion provides analgesia, does not require additional skillsets, and is not impacted by anticoagulants. At this time, a stepwise approach to patient care is most appropriate.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
All authors made a significant contribution to the work reported, including the conception and design of the manuscript, as well as the acquisition of studies and the analysis and interpretation of publications’ findings; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Not applicable/no funding was received.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Sjovall S, Kokki M, Kokki H. Laparoscopic surgery: a narrative review of pharmacotherapy in pain management. Drugs. 2015;75(16):1867–1889.
2. Ortiz J, Rajagopalan SA. Review of local anesthetic techniques for analgesia after laparoscopic surgery. J Minim Invasive Surg Sci. 2014;3(2):e11310.
3. Chin KJ, McDonnell JG, Carvalho B, Sharkey A, Pawa A, Gadsden J. Essentials of our current understanding: abdominal wall blocks. Reg Anesth Pain Med. 2017;42(2):133–183. doi:10.1097/AAP.0000000000000545
4. Pirrera B, Alagna V, Lucchi A, et al. Transversus abdominis plane (TAP) block versus thoracic epidural analgesia (TEA) in laparoscopic colon surgery in the ERAS program. Surg Endosc. 2018;32(1):376–382. doi:10.1007/s00464-017-5686-7
5. Qin C, Liu Y, Xiong J, et al. The analgesic efficacy compared ultrasound-guided continuous transverse abdominis plane block with epidural analgesia following abdominal surgery: a systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2020;20(1):52. doi:10.1186/s12871-020-00969-0
6. Levy BF, Tilney HS, Dowson HM, Rockall TA. A systematic review of postoperative analgesia following laparoscopic colorectal surgery. Colorectal Dis. 2010;12(1):5–15. doi:10.1111/j.1463-1318.2009.01799.x
7. Ruiz-Tovar J, Garcia A, Ferrigni C, et al. Laparoscopic-guided Transversus Abdominis Plane (TAP) block as part of multimodal analgesia in laparoscopic Roux-en-Y gastric bypass within an Enhanced Recovery After Surgery (ERAS) program: a prospective randomized clinical trial. Obes Surg. 2018;28(11):3374–3379. doi:10.1007/s11695-018-3376-8
8. Favuzza J, Delaney CP. Outcomes of discharge after elective laparoscopic colorectal surgery with transversus abdominis plane blocks and enhanced recovery pathway. J Am Coll Surg. 2013;217(3):503–506. doi:10.1016/j.jamcollsurg.2013.03.030
9. Kim AJ, Yong RJ, Urman RD. The role of transversus abdominis plane blocks in enhanced recovery after surgery pathways for open and laparoscopic colorectal surgery. J Laparoendosc Adv Surg Tech A. 2017;27(9):909–914. doi:10.1089/lap.2017.0337
10. Shahait M, Lee DI. Application of TAP block in laparoscopic urological surgery: current status and future directions. Curr Urol Rep. 2019;20(5):20. doi:10.1007/s11934-019-0883-7
11. Baeriswyl M, Kirkham KR, Kern C, Albrecht E. The analgesic efficacy of ultrasound-guided transversus abdominis plane block in adult patients: a meta-analysis. Anesth Analg. 2015;121(6):1640–1654. doi:10.1213/ANE.0000000000000967
12. De Oliveira GS, Duncan K, Fitzgerald P, Nader A, Gould RW, McCarthy RJ. Systemic lidocaine to improve quality of recovery after laparoscopic bariatric surgery: a randomized double-blinded placebo-controlled trial. Obes Surg. 2014;24(2):212–218. doi:10.1007/s11695-013-1077-x
13. Dunn LK, Durieux ME. Perioperative use of intravenous lidocaine. Anesthesiology. 2017;126(4):729–737. doi:10.1097/ALN.0000000000001527
14. Kaba A, Laurent SR, Detroz BJ, et al. Intravenous lidocaine infusion facilitates acute rehabilitation after laparoscopic colectomy. Anesthesiology. 2007;106(1):11–16. doi:10.1097/00000542-200701000-00007
15. Kim TH, Kang H, Choi YS, et al. Pre- and intraoperative lidocaine injection for preemptive analgesics in laparoscopic gastrectomy: a prospective, randomized, double-blind, placebo-controlled study. J Laparoendosc Adv Surg Tech A. 2013;23(8):663–668. doi:10.1089/lap.2012.0542
16. Kim TH, Kang H, Hong JH, et al. Intraperitoneal and intravenous lidocaine for effective pain relief after laparoscopic appendectomy: a prospective, randomized, double-blind, placebo-controlled study. Surg Endosc. 2011;25(10):3183–3190. doi:10.1007/s00464-011-1684-3
17. Lauwick S, Kim DJ, Michelagnoli G, et al. Intraoperative infusion of lidocaine reduces postoperative fentanyl requirements in patients undergoing laparoscopic cholecystectomy. Can J Anaesth. 2008;55(11):754–760. doi:10.1007/BF03016348
18. Saadawy IM, Kaki AM, Abd El Latif AA, Abd-Elmaksoud AM, Tolba OM. Lidocaine vs. magnesium: effect on analgesia after a laparoscopic cholecystectomy. Acta Anaesthesiol Scand. 2010;54(5):549–556. doi:10.1111/j.1399-6576.2009.02165.x
19. Tikuisis R, Miliauskas P, Samalavicius NE, Zurauskas A, Samalavicius R, Zabulis V. Intravenous lidocaine for post-operative pain relief after hand-assisted laparoscopic colon surgery: a randomized, placebo-controlled clinical trial. Tech Coloproctol. 2014;18(4):373–380. doi:10.1007/s10151-013-1065-0
20. Wongyingsinn M, Baldini G, Charlebois P, Liberman S, Stein B, Carli F. Intravenous lidocaine versus thoracic epidural analgesia: a randomized controlled trial in patients undergoing laparoscopic colorectal surgery using an enhanced recovery program. Reg Anesth Pain Med. 2011;36(3):241–248. doi:10.1097/AAP.0b013e31820d4362
21. De Oliveira GS, Castro-Alves LJ, Nader A, Kendall MC, McCarthy RJ. Transversus abdominis plane block to ameliorate postoperative pain outcomes after laparoscopic surgery: a meta-analysis of randomized controlled trials. Anesth Analg. 2014;118(2):454–463. doi:10.1213/ANE.0000000000000066
22. Keir A, Rhodes L, Kayal A, Khan OA. Does a transversus abdominis plane (TAP) local anaesthetic block improve pain control in patients undergoing laparoscopic cholecystectomy? A best evidence topic. Int J Surg. 2013;11(9):792–794. doi:10.1016/j.ijsu.2013.05.039
23. Marret E, Rolin M, Beaussier M, Bonnet F. Meta-analysis of intravenous lidocaine and postoperative recovery after abdominal surgery. Br J Surg. 2008;95(11):1331–1338. doi:10.1002/bjs.6375
24. McCarthy GC, Megalla SA, Habib AS. Impact of intravenous lidocaine infusion on postoperative analgesia and recovery from surgery: a systematic review of randomized controlled trials. Drugs. 2010;70(9):1149–1163. doi:10.2165/10898560-000000000-00000
25. Murouchi T, Iwasaki S, Yamakage M. Quadratus lumborum block: analgesic effects and chronological ropivacaine concentrations after laparoscopic surgery. Reg Anesth Pain Med. 2016;41(2):146–150. doi:10.1097/AAP.0000000000000349
26. Guo Q, Li R, Wang L, Zhang D, Ma Y. Transversus abdominis plane block versus local anaesthetic wound infiltration for postoperative analgesia: a systematic review and meta-analysis. Int J Clin Exp Med. 2015;8(10):17343–17352.
27. Walter CJ, Maxwell-Armstrong C, Pinkney TD, et al. A randomised controlled trial of the efficacy of ultrasound-guided transversus abdominis plane (TAP) block in laparoscopic colorectal surgery. Surg Endosc. 2013;27(7):2366–2372. doi:10.1007/s00464-013-2791-0
28. De Oliveira GS, Milad MP, Fitzgerald P, Rahmani R, McCarthy RJ. Transversus abdominis plane infiltration and quality of recovery after laparoscopic hysterectomy: a randomized controlled trial. Obstet Gynecol. 2011;118(6):1230–1237. doi:10.1097/AOG.0b013e318236f67f
29. Hosgood SA, Thiyagarajan UM, Nicholson HF, Jeyapalan I, Nicholson ML. Randomized clinical trial of transversus abdominis plane block versus placebo control in live-donor nephrectomy. Transplantation. 2012;94(5):520–525. doi:10.1097/TP.0b013e31825c1697
30. Tanggaard K, Jensen K, Lenz K, et al. A randomised controlled trial of bilateral dual transversus abdominis plane blockade for laparoscopic appendicectomy. Anaesthesia. 2015;70(12):1395–1400. doi:10.1111/anae.13234
31. Tolchard S, Davies R, Martindale S. Efficacy of the subcostal transversus abdominis plane block in laparoscopic cholecystectomy: comparison with conventional port-site infiltration. J Anaesthesiol Clin Pharmacol. 2012;28(3):339–343. doi:10.4103/0970-9185.98331
32. Mallan D, Sharan S, Saxena S, Singh TK. Anesthetic techniques: focus on transversus abdominis plane (TAP) blocks. Local Reg Anesth. 2019;12:81–88. doi:10.2147/LRA.S138537
33. Rafi AN. Abdominal field block: a new approach via the lumbar triangle. Anaesthesia. 2001;56(10):1024–1026.
34. Jankovic ZB, Du Feu FM, McConnell P. An anatomical study of the transversus abdominis plane block: location of the lumbar triangle of Petit and adjacent nerves. Anesth Analg. 2009;109(3):981–985. doi:10.1213/ane.0b013e3181ae0989
35. Tsai HC, Yoshida T, Chuang TY, et al. Transversus abdominis plane block: an updated review of anatomy and techniques. Biomed Res Int. 2017;2017:8284363. doi:10.1155/2017/8284363
36. Hebbard P. Subcostal transversus abdominis plane block under ultrasound guidance. Anesth Analg. 2008;106(2):
37. Abdallah FW, Laffey JG, Halpern SH, Brull R. Duration of analgesic effectiveness after the posterior and lateral transversus abdominis plane block techniques for transverse lower abdominal incisions: a meta-analysis. Br J Anaesth. 2013;111(5):721–735. doi:10.1093/bja/aet214
38. Chen Y, Shi K, Xia Y, et al. Sensory assessment and regression rate of bilateral oblique subcostal transversus abdominis plane block in volunteers. Reg Anesth Pain Med. 2018;43(2):174–179.
39. Lee TH, Barrington MJ, Tran TM, Wong D, Hebbard PD. Comparison of extent of sensory block following posterior and subcostal approaches to ultrasound-guided transversus abdominis plane block. Anaesth Intensive Care. 2010;38(3):452–460. doi:10.1177/0310057X1003800307
40. Stoving K, Rothe C, Rosenstock CV, Aasvang EK, Lundstrom LH, Lange KH. Cutaneous sensory block area, muscle-relaxing effect, and block duration of the transversus abdominis plane block: a randomized, blinded, and placebo-controlled study in healthy volunteers. Reg Anesth Pain Med. 2015;40(4):355–362. doi:10.1097/AAP.0000000000000252
41. Carney J, Finnerty O, Rauf J, Bergin D, Laffey JG, Mc Donnell JG. Studies on the spread of local anaesthetic solution in transversus abdominis plane blocks. Anaesthesia. 2011;66(11):1023–1030. doi:10.1111/j.1365-2044.2011.06855.x
42. Rozen WM, Tran TM, Ashton MW, Barrington MJ, Ivanusic JJ, Taylor GI. Refining the course of the thoracolumbar nerves: a new understanding of the innervation of the anterior abdominal wall. Clin Anat. 2008;21(4):325–333. doi:10.1002/ca.20621
43. Aoyama Y, Sakura S, Abe S, Wada M, Saito Y. Analgesic effects and distribution of cutaneous sensory blockade of quadratus lumborum block type 2 and posterior transversus abdominis plane block: an observational comparative study. Korean J Anesthesiol. 2020;73(4):326–333. doi:10.4097/kja.19404
44. Furuya T, Kato J, Yamamoto Y, Hirose N, Suzuki T. Comparison of dermatomal sensory block following ultrasound-guided transversus abdominis plane block by the lateral and posterior approaches: a randomized controlled trial. J Anaesthesiol Clin Pharmacol. 2018;34(2):205–210.
45. Ortiz J, Suliburk JW, Wu K, et al. Bilateral transversus abdominis plane block does not decrease postoperative pain after laparoscopic cholecystectomy when compared with local anesthetic infiltration of trocar insertion sites. Reg Anesth Pain Med. 2012;37(2):188–192. doi:10.1097/AAP.0b013e318244851b
46. Wu L, Wu L, Sun H, Dong C, Yu J. Effect of ultrasound-guided peripheral nerve blocks of the abdominal wall on pain relief after laparoscopic cholecystectomy. J Pain Res. 2019;12:1433–1439. doi:10.2147/JPR.S203721
47. Petersen PL, Stjernholm P, Kristiansen VB, et al. The beneficial effect of transversus abdominis plane block after laparoscopic cholecystectomy in day-case surgery: a randomized clinical trial. Anesth Analg. 2012;115(3):527–533.
48. Sun Y, Li T, Wang N, Yun Y, Gan TJ. Perioperative systemic lidocaine for postoperative analgesia and recovery after abdominal surgery: a meta-analysis of randomized controlled trials. Dis Colon Rectum. 2012;55(11):1183–1194. doi:10.1097/DCR.0b013e318259bcd8
49. Vigneault L, Turgeon AF, Cote D, et al. Perioperative intravenous lidocaine infusion for postoperative pain control: a meta-analysis of randomized controlled trials. Can J Anaesth. 2011;58(1):22–37. doi:10.1007/s12630-010-9407-0
50. Kandil E, Melikman E, Adinoff B. Lidocaine infusion: a promising therapeutic approach for chronic pain. J Anesth Clin Res. 2017;8(1). doi:10.4172/2155-6148.1000697
51. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
52. Aitola P, Airo I, Kaukinen S, Ylitalo P. Comparison of N2O and CO2 pneumoperitoneums during laparoscopic cholecystectomy with special reference to postoperative pain. Surg Laparosc Endosc. 1998;8(2):140–144. doi:10.1097/00019509-199804000-00013
53. Tsai HW, Chen YJ, Ho CM, et al. Maneuvers to decrease laparoscopy-induced shoulder and upper abdominal pain: a randomized controlled study. Arch Surg. 2011;146(12):1360–1366. doi:10.1001/archsurg.2011.597
54. Borglum J, Gogenur I, Bendtsen TF. Abdominal wall blocks in adults. Curr Opin Anaesthesiol. 2016;29(5):638–643. doi:10.1097/ACO.0000000000000378
55. Elsharkawy H, El-Boghdadly K, Barrington M. Quadratus lumborum block: anatomical concepts, mechanisms, and techniques. Anesthesiology. 2019;130(2):322–335. doi:10.1097/ALN.0000000000002524
56. Dam M, Hansen CK, Borglum J, Chan V, Bendtsen TF. A transverse oblique approach to the transmuscular Quadratus Lumborum block. Anaesthesia. 2016;71(5):603–604. doi:10.1111/anae.13453
57. Ueshima H, Hiroshi O. Incidence of lower-extremity muscle weakness after quadratus lumborum block. J Clin Anesth. 2018;44:104. doi:10.1016/j.jclinane.2017.11.020
58. Ueshima H, Otake H, Lin JA. Ultrasound-guided quadratus lumborum block: an updated review of anatomy and techniques. Biomed Res Int. 2017;2017:2752876. doi:10.1155/2017/2752876
59. Ueshima H, Yoshiyama S, Otake H. The ultrasound-guided continuous transmuscular quadratus lumborum block is an effective analgesia for total hip arthroplasty. J Clin Anesth. 2016;31:35. doi:10.1016/j.jclinane.2015.12.033
60. Akerman M, Pejcic N, Velickovic I. A review of the quadratus lumborum block and ERAS. Front Med (Lausanne). 2018;5:44. doi:10.3389/fmed.2018.00044
61. Dam M, Moriggl B, Hansen CK, Hoermann R, Bendtsen TF, Borglum J. The pathway of injectate spread with the transmuscular quadratus lumborum block: a cadaver study. Anesth Analg. 2017;125(1):303–312. doi:10.1213/ANE.0000000000001922
62. Kumar A, Sadeghi N, Wahal C, Gadsden J, Grant SA. Quadratus lumborum spares paravertebral space in fresh cadaver injection. Anesth Analg. 2017;125(2):708–709. doi:10.1213/ANE.0000000000002245
63. Tesarz J, Hoheisel U, Wiedenhofer B, Mense S. Sensory innervation of the thoracolumbar fascia in rats and humans. Neuroscience. 2011;194:302–308. doi:10.1016/j.neuroscience.2011.07.066
64. Almeida C, Assuncao JP. [Hypotension associated to a bilateral quadratus lumborum block performed for post-operative analgesia in an open aortic surgery case]. Rev Bras Anestesiol. 2018;68(6):657–660. English and Portuguese. doi:10.1016/j.bjan.2018.05.003
65. Ishio J, Komasawa N, Kido H, Minami T. Evaluation of ultrasound-guided posterior quadratus lumborum block for postoperative analgesia after laparoscopic gynecologic surgery. J Clin Anesth. 2017;41:1–4. doi:10.1016/j.jclinane.2017.05.015
66. Okmen K, Metin Okmen B, Topal S. Ultrasound-guided posterior quadratus lumborum block for postoperative pain after laparoscopic cholecystectomy: a randomized controlled double blind study. J Clin Anesth. 2018;49:112–117. doi:10.1016/j.jclinane.2018.06.027
67. Zhu M, Qi Y, He H, Lou J, Pei Q, Mei Y. Analgesic effect of the ultrasound-guided subcostal approach to transmuscular quadratus lumborum block in patients undergoing laparoscopic nephrectomy: a randomized controlled trial. BMC Anesthesiol. 2019;19(1):154. doi:10.1186/s12871-019-0825-4
68. Fujimoto H, Irie T, Mihara T, Mizuno Y, Nomura T, Goto T. Effect of posterior quadratus lumborum blockade on the quality of recovery after major gynaecological laparoscopic surgery: a randomized controlled trial. Anaesth Intensive Care. 2019;47(2):146–151. doi:10.1177/0310057X19838765
69. Baytar C, Yilmaz C, Karasu D, Topal S. Comparison of ultrasound-guided subcostal transversus abdominis plane block and quadratus lumborum block in laparoscopic cholecystectomy: a prospective, randomized, controlled clinical study. Pain Res Manag. 2019;2019:2815301. doi:10.1155/2019/2815301
70. Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ. The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med. 2016;41(5):621–627. doi:10.1097/AAP.0000000000000451
71. Chin KJ, Malhas L, Perlas A. The erector spinae plane block provides visceral abdominal analgesia in bariatric surgery: a report of 3 cases. Reg Anesth Pain Med. 2017;42(3):372–376. doi:10.1097/AAP.0000000000000581
72. Onishi E, Toda N, Kameyama Y, Yamauchi M. Comparison of clinical efficacy and anatomical investigation between retrolaminar block and erector spinae plane block. Biomed Res Int. 2019;2019:2578396. doi:10.1155/2019/2578396
73. Altiparmak B, Korkmaz Toker M, Uysal AI, Kuscu Y, Gumus Demirbilek S. Ultrasound-guided erector spinae plane block versus oblique subcostal transversus abdominis plane block for postoperative analgesia of adult patients undergoing laparoscopic cholecystectomy: randomized, controlled trial. J Clin Anesth. 2019;57:31–36. doi:10.1016/j.jclinane.2019.03.012
74. Hannig KE, Jessen C, Soni UK, Borglum J, Bendtsen TF. Erector spinae plane block for elective laparoscopic cholecystectomy in the ambulatory surgical setting. Case Rep Anesthesiol. 2018;2018:5492527.
75. Tulgar S, Kapakli MS, Senturk O, Selvi O, Serifsoy TE, Ozer Z. Evaluation of ultrasound-guided erector spinae plane block for postoperative analgesia in laparoscopic cholecystectomy: a prospective, randomized, controlled clinical trial. J Clin Anesth. 2018;49:101–106. doi:10.1016/j.jclinane.2018.06.019
76. Tulgar S, Selvi O, Kapakli MS. Erector spinae plane block for different laparoscopic abdominal surgeries: case series. Case Rep Anesthesiol. 2018;2018:3947281.
77. Aygun H, Kavrut Ozturk N, Pamukcu AS, et al. Comparison of ultrasound guided Erector Spinae Plane Block and quadratus lumborum block for postoperative analgesia in laparoscopic cholecystectomy patients; a prospective randomized study. J Clin Anesth. 2020;62:109696. doi:10.1016/j.jclinane.2019.109696
78. Fernández Martín MT, López Álvarez S, Fajardo Pérez M, Pérez Herrero M. Serratus-intercostal interfascial plane block: alternative analgesia for open nephrectomy? Minerva Anestesiol. 2018;84(7):872–873.
79. Fernández Martín MT, López Álvarez S, Pérez Herrero MA. Serratus-intercostal interfascial block as an opioid-saving strategy in supra-umbilical open surgery. Rev Esp Anestesiol Reanim. 2018;65(8):456–460. doi:10.1016/j.redar.2018.03.007
80. Selvi O, Tulgar S, Senturk O, et al. Is a combination of the serratus intercostal plane block and rectus sheath block superior to the bilateral oblique subcostal transversus abdominis plane block in laparoscopic cholecystectomy? Eurasian J Med. 2020;52(1):34–37. doi:10.5152/eurasianjmed.2019.19048
81. Balaban O, Tulgar S, Ahiskalioğlu A, Thomas DT, Aydin T. Blockage of thoracoabdominal nerves through perichondrial approach (TAPA) for surgical anesthesia after failed erector spinae plane block in mini-laparatomy. J Clin Anesth. 2019;55:74–75. doi:10.1016/j.jclinane.2018.12.054
82. Tulgar S, Senturk O, Selvi O, et al. Perichondral approach for blockage of thoracoabdominal nerves: anatomical basis and clinical experience in three cases. J Clin Anesth. 2019;54:8–10. doi:10.1016/j.jclinane.2018.10.015
83. Maloney C, Kallis M, El-Shafy IA, Lipskar AM, Hagen J, Kars M. Ultrasound-guided bilateral rectus sheath block vs. conventional local analgesia in single port laparoscopic appendectomy for children with nonperforated appendicitis. J Pediatr Surg. 2018;53(3):431–436. doi:10.1016/j.jpedsurg.2017.05.027
84. Zhou Y, Chen M, Zhang Y, Zhou H, Yu X, Chen G. Ilioinguinal/iliohypogastric nerve block versus transversus abdominis plane block for pain management following inguinal hernia repair surgery: a systematic review and meta-analysis of randomized controlled trials. Medicine (Baltimore). 2019;98(42):e17545. doi:10.1097/MD.0000000000017545
85. Dewinter G, Van de Velde M, Fieuws S, D’Hoore A, Rex S. Transversus abdominis plane block versus perioperative intravenous lidocaine versus patient-controlled intravenous morphine for postoperative pain control after laparoscopic colorectal surgery: study protocol for a prospective, randomized, double-blind controlled clinical trial. Trials. 2014;15:476.
86. Oksar M, Koyuncu O, Turhanoglu S, Temiz M, Oran MC. Transversus abdominis plane block as a component of multimodal analgesia for laparoscopic cholecystectomy. J Clin Anesth. 2016;34:72–78. doi:10.1016/j.jclinane.2016.03.033
87. Alkatout I, Mettler L, Maass N, Noe GK, Elessawy M. Abdominal anatomy in the context of port placement and trocars. J Turk Ger Gynecol Assoc. 2015;16(4):241–251. doi:10.5152/jtgga.2015.0148
88. Sikandar S, Dickenson AH. Visceral pain: the ins and outs, the ups and downs. Curr Opin Support Palliat Care. 2012;6(1):17–26. doi:10.1097/SPC.0b013e32834f6ec9
89. Srinivasan R, Greenbaum DS. Chronic abdominal wall pain: a frequently overlooked problem. Practical approach to diagnosis and management. Am J Gastroenterol. 2002;97(4):824–830.
90. Suleiman S, Johnston DE. The abdominal wall: an overlooked source of pain. Am Fam Physician. 2001;64(3):431–438.
91. Thomson H, Francis DM. Abdominal-wall tenderness: a useful sign in the acute abdomen. Lancet. 1977;2(8047):1053–1054. doi:10.1016/S0140-6736(77)91885-2
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.