Back to Journals » Risk Management and Healthcare Policy » Volume 18
Interactions Between Pharmaceutical Companies and Patient Advocacy Groups in Japan: A Qualitative and Quantitative Interview Study
Authors Kikuchi A ![]() , Hara A, Ozaki A, Sakata N, Saito H, Tanimoto T, Maeda H
, Hara A, Ozaki A, Sakata N, Saito H, Tanimoto T, Maeda H ![]()
Received 15 July 2025
Accepted for publication 25 October 2025
Published 27 November 2025 Volume 2025:18 Pages 3769—3779
DOI https://doi.org/10.2147/RMHP.S553983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Ayaka Kikuchi,1 Asuka Hara,1 Akihiko Ozaki,2,3 Natsuya Sakata,2,4 Hiroaki Saito,2,5 Tetsuya Tanimoto,2 Hideki Maeda1
1Regulatory Science, Faculty of Pharmacy, Meiji Pharmaceutical University, Kiyose, Japan; 2Medical Governance Research Institute, Minato-ku, Japan; 3Department of Breast and Thyroid Surgery, Jyoban Hospital of Tokiwa Foundation, Iwaki, Japan; 4School of Medicine, Faculty of Medicine, Akita University, Akita, Japan; 5Department of Gastroenterology, Sendai Kousei Hospital, Sendai, Japan
Correspondence: Hideki Maeda, Regulatory Science, Faculty of Pharmacy, Meiji Pharmaceutical University, Kiyose, Japan, Tel +81-42-495-8952, Email [email protected]
Purpose: In Japan, the financial relationship between pharmaceutical companies and patient advocacy groups is considered to be weak; however, limited studies have examined this relationship. The financial relationship and issues surrounding the relationship between the two parties remain unclear.
Patients and Methods: This study investigated the relationship between Japanese patient support groups and pharmaceutical companies by interviewing 10 pharmaceutical companies and examining the underlying challenges. Conducted from 2022 to 2023, this research employed a qualitative and quantitative interview survey using a prospective study design. Interview content was transcribed, coded, and categorized.
Results: In 70% of the pharmaceutical companies, the most common type of work with patient advocacy groups was listening to the patient’s voice, and 90% of the pharmaceutical companies worked to understand patients’ needs. Pharmaceutical companies viewed patient advocacy groups as partners in hearing the voices of patients. Regarding the relationship between the two parties, 60% of the pharmaceutical companies believed that the current guidelines were sufficient, despite some problems with the regulations, systems, and the number of group activities.
Conclusion: Compared with other countries, groups in Japan are unique in their relationships, size, history, and culture. These results indicate that in Japan, listening to the issues and voices of patients and their families is emphasized rather than financial support. Consequently, there was less concern about compromising the independence of patient advocacy groups, unlike those overseas. Regarding the problems in the relationship between patient advocacy groups and pharmaceutical companies, although the regulations make it difficult for these groups and companies to interact, immediate improvement of the regulations was deemed unnecessary. They prioritize collaboration to listen to the voices of patients. We considered that in Japan, unlike other countries, there is less risk that the independence of patient advocacy groups will be compromised by large amounts of financial support.
Keywords: patient organization, pharmaceutical company, Japan, collaboration
Introduction
Patient advocacy groups play a critical role in society. In addition to being a place where patients can support each other and share the latest necessary information, including information from overseas, patient advocacy groups are involved in conveying messages to society, including policy proposals, and play crucial roles for patients and society.1,2 Patient advocacy groups have also become increasingly involved in healthcare and medical research and have become indispensable to the efforts of the pharmaceutical industry in “realizing patient-centered medical care”, particularly in recent years.3–7
In other countries, patient advocacy groups provide philanthropic support, called advocacy, and engage in policy proposals and activities aimed at obtaining the approval of new drugs.3,8–10 Because of the existence of a system that allows the involvement of patient advocacy groups in the approval of new drugs, pharmaceutical companies may become sponsors of patient advocacy groups by making donations to them, in turn involving patient advocacy groups in the approval of new drugs.11 Studies in the United States, Europe, and Australia have questioned the large financial support provided by pharmaceutical companies to patient advocacy groups.1,4,11–13 It cannot merely be for obtaining approval within that country. For example, obtaining the US Food and Drug Administration approval in the United States makes it easier to obtain approval in other countries and increases the likelihood for a new drug to be approved worldwide.14 In other countries, patient advocacy groups operate primarily on the basis of funds obtained from pharmaceutical companies and other sources; thus, it has been highlighted that large donations impair the independence of patient advocacy groups and prevent them from operating in a patient-centered manner.3,11,15 Thus, patients’ voices may be distorted, and their needs are ignored for the benefit of pharmaceutical companies.1,4
In recent years, Japan has also seen a movement to incorporate patient voices into drug development and post-marketing activities based on the concept of patient-centered care. However, Japan’s universal health insurance system allows patients to easily access medications without actively seeking them out. Unlike overseas, there is no system enabling patient participation in the drug approval process, and even prescription drug advertising to patient groups is prohibited. Consequently, while financial ties between pharmaceutical companies and patient support groups are presumed to be weak, little research has been conducted on this relationship. As a result, the details of the financial relationship between pharmaceutical companies and patient advocacy groups, their perceptions of each other, the problems in the relationship between patient advocacy groups and pharmaceutical companies, and the uniqueness of the relationship in Japan are largely unknown. This information is considered extremely important in the search for appropriate relationships between pharmaceutical companies and patient advocacy groups.
Against this background, in this study, we interviewed pharmaceutical companies about current collaborative activities, impressions of patient organizations, and Japan’s unique characteristics to examine their actual relationship with patient advocacy groups in Japan and assess related issues.
Materials and Methods
Design
This was a qualitative and quantitative content analysis study of pharmaceutical companies using semi-structured interviews. Since this topic has not been sufficiently researched, we attempted to understand the overall trend of the topic by observing the frequency using quantitative content analysis after coding it using qualitative content analysis. This study complies with the Standards for Reporting Qualitative Research.16 (S1 Appendix).
Sampling and Survey Participants
We recruited representatives responsible for patient advocacy group departments at the top 20 pharmaceutical companies in Japan, ranked by 2021 sales, as potential interviewees.17 Since no similar domestic research existed, the interview content was carefully formulated within the research team. Furthermore, due to the small number of companies interviewed, no pilot study was conducted. They decided whether to participate in the interview after receiving an explanation and providing consent. Consent was requested by briefly explaining the purpose of the interview to the participants, and the interview was conducted on participants who provided consent. The participants were also asked whether they permitted video recording during the interview. If consent was obtained, recording (video recording) was done. All consents were obtained in writing. An interview form was sent in advance to the interview participants, who were requested to complete the interview form in advance. The interview was conducted using the semi-structured interview method.18
Interviews were conducted online from August 18, 2022 to May 17, 2023 according to the interview form based on a comprehensive assessment of the COVID-19 infection situation.
Data Collection and Analysis
The interviews covered four major questions and nine sub questions (S2 Appendix). The interviews were transcribed verbatim by a professional transcription service. After delivery, the research team checked the content and corrected any errors. Subsequently, mixed content analysis was performed based on Mayring (2014).19 First, qualitative content analysis was conducted on the interviews to extract meaningful codes. This was done through a process where one person first performed the coding, and then another person reviewed the codes that had been generated. Next, quantitative content analysis was performed on the extracted codes to identify overall trends by observing the frequency of code occurrence. This counts how many companies each code emerged from in interviews, then calculates the percentage of companies where the code appeared, using the 10 interviewed companies as the denominator. The transcribed data were stored after anonymization.
Results
The top 20 Japanese companies in terms of sales in 2021 were surveyed, and 11 companies agreed to participate in the interview (Figure 1). Of these, 10 companies had records of implementation. The survey was conducted on these 10 companies.
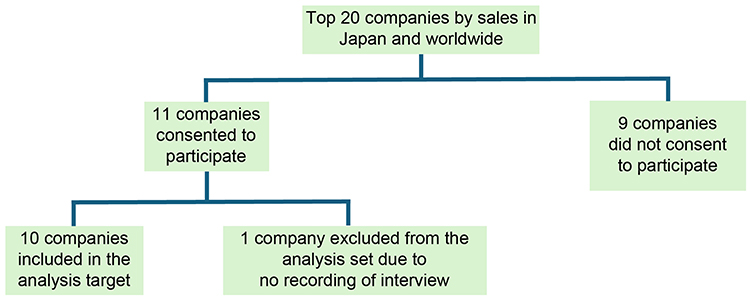 |
Figure 1 Flowchart of selection of pharmaceutical companies for the survey. |
In Table 1, the majority of respondents were in their 50s (50%), male (60%), currently in the patient department and the corporate department (both 30%), and manager and head/general manager (both 30%). When companies were surveyed for diseases and areas of focus with multiple responses allowed, the most common responses were cancer and immune systems (both 40%), followed by vaccine and circulatory systems (both 30%).
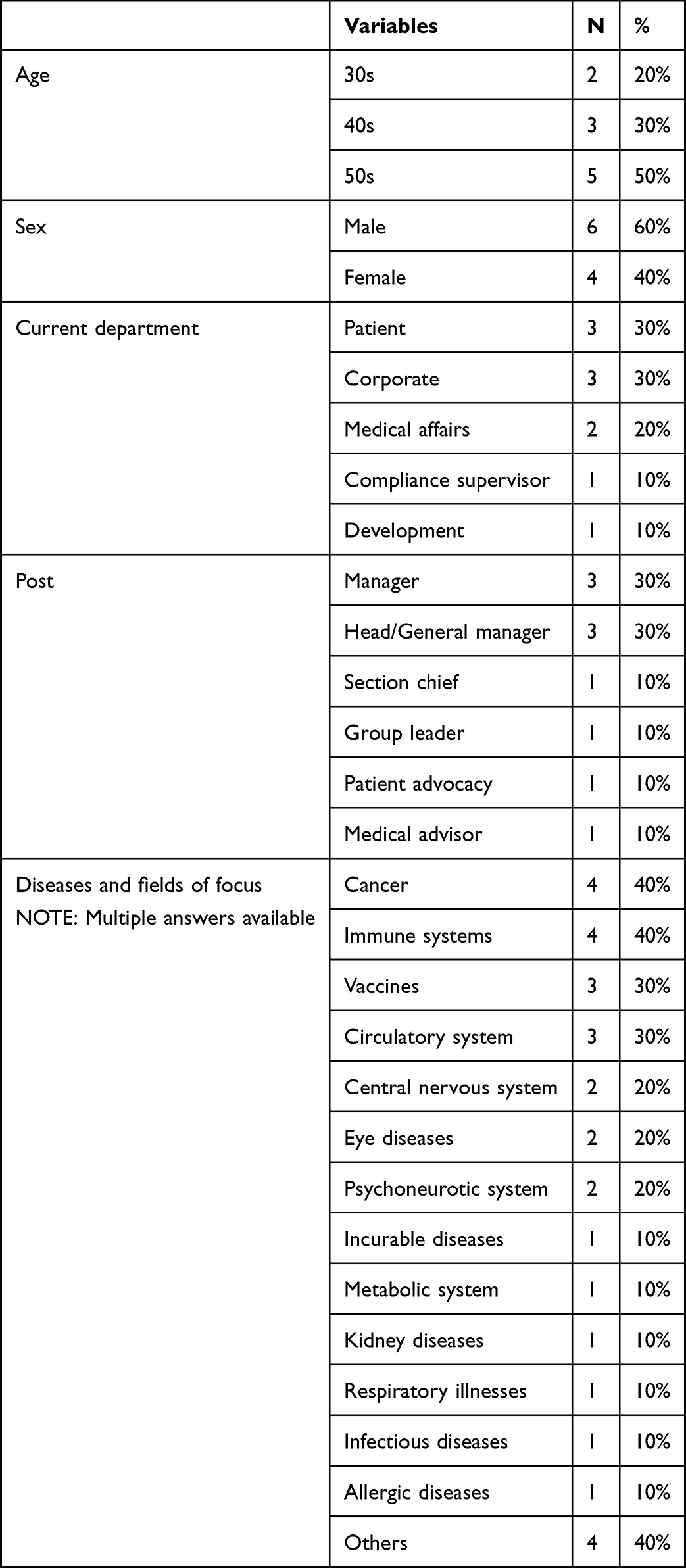 |
Table 1 Background Information of Respondents |
Each question below allows multiple responses unless otherwise noted, and the percentages indicate the number of companies that provided the response.
In Table 2, for 1–1 “Please provide details of the work your company has commissioned and the support it provides to patient advocacy groups”, “Listening to patient’s voice” (70%), including exchange of opinions to be used in development, was the most common response, followed by “financial support” (60%), including donations and advertising support, activities related to “clinical trials”, such as protocol supervision, and “disease awareness” (both 50%). For 1–2 “Why does your company collaborate with patient advocacy groups?”, the overwhelming majority of responses was “understanding the needs” of patients at 90%. For 1–3 “What areas does your company focus on when collaborating with patient advocacy groups?”, “cancer” and “rare diseases” (40%), and “immune systems” (30%) were relatively common responses. In some cases, the respondents answered “product possession” (30%) and “focus areas” (20%) for their companies, whereas others answered “not determined” (20%). For 1–4 “Do you have any patient advocacy groups that have turned down requests for work or support from your company in the past? If so, please give specific reasons”, 80% of the companies had experienced rejection by patient advocacy groups. A wide range of responses were given as reasons, but none of them were common. The responses included “inaccessible to target patient” (30%), when there were no patients within the patient advocacy groups that the companies were looking for or it was not possible to find them; “requests not matched” (20%), when patients were hesitant to provide information and collaboration was not possible; “no suitable person for lecture/supervision” (20%), when patients did not have adequate knowledge and speakers or clinical trial protocol supervisors could not be found; “lack of spare time” (20%), when patient advocacy groups were too busy; and “no network” (10%) for patient advocacy groups to contact each patient. In contrast, pharmaceutical companies sometimes declined requests from patient advocacy groups, with “not sincere” (20%), “different objectives” (20%) regarding how to use financial support, and “lack of budget” (10%) of the companies as reasons.
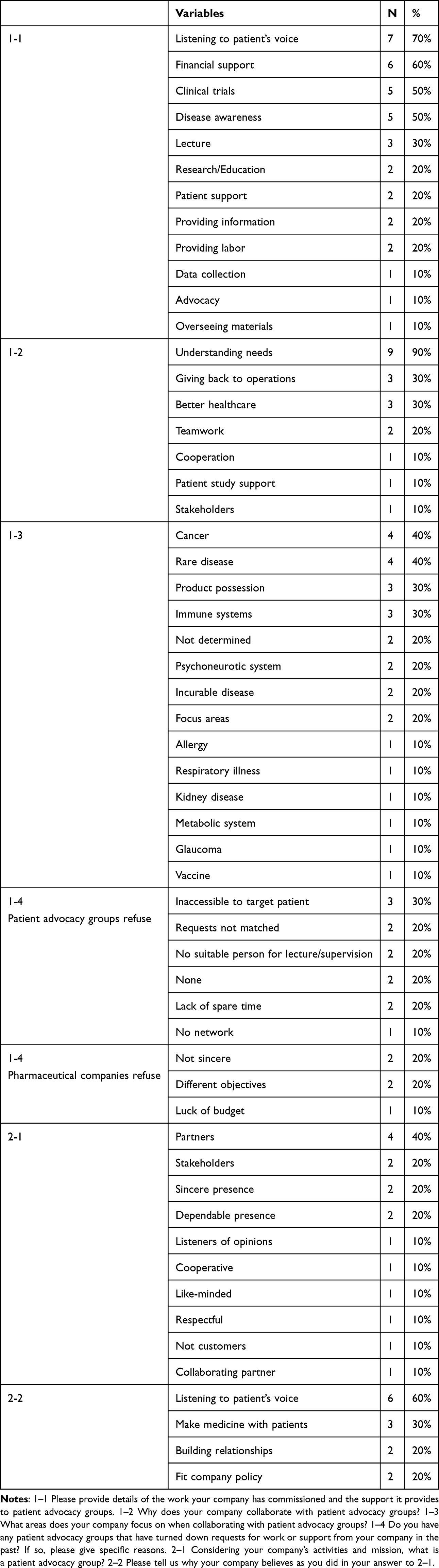 |
Table 2 Answers to Questions 1 and 2 |
For 2–1 “In light of your company’s activities and mission, what is a patient advocacy group?”, many companies answered “partners” (40%), followed by “stakeholders”, “sincere presence”, and “dependable presence” (all 20%). No responses expressed a negative impression of the patient advocacy groups. For 2–2 “Please tell us why your company believes as you did in your answer to 2–1”, the most common response was “listening to patient’s voice” (60%), indicating that the companies value the patient’s opinions because they want to develop drugs that meet patient needs.
In Table 3, for 3–1 “Are there any problems in your company’s relationship with patient advocacy groups? If so, please let us know”, the most common responses were “regulations and systems”, such as the lack of donation standards and difficulties in interpreting current regulations, and “lack of activity and overload of work for the group” (both 40%). They were followed by “difference in awareness” between patient advocacy groups and pharmaceutical companies (30%), indicating that patient advocacy groups perceive pharmaceutical companies as for-profit companies and have difficulty collaborating with them and that it is difficult to avoid the impression of a conflict of interest among the public. In Figure 2, the responses of each company to 3–2 “Would you say that current guidelines on financial relationships between pharmaceutical companies and patient advocacy groups are adequate?” were divided into “adequate” and “not adequate”, with 60% being “adequate” and 40% being “not adequate”. The companies that responded “adequate” rated that the minimum necessary information was included to ensure transparency and was open to flexible interpretation. Some companies cited the fact that each company has set its own guidelines and that no problems are currently occurring as the reason. Some companies indicated that a review would become necessary if collaboration with patient advocacy groups and financial support to them increase in the future. The companies that responded “not adequate” indicated that the guidelines are brief and only provide a rough outline and that there is room for reconsideration. They wanted specific rules, such as criteria for the consideration of donations. However, some respondents said that it would be acceptable if the guidelines of each company were strict, and some appreciated the fact that even in their current form, the guidelines serve as a deterrent to large donations by companies.
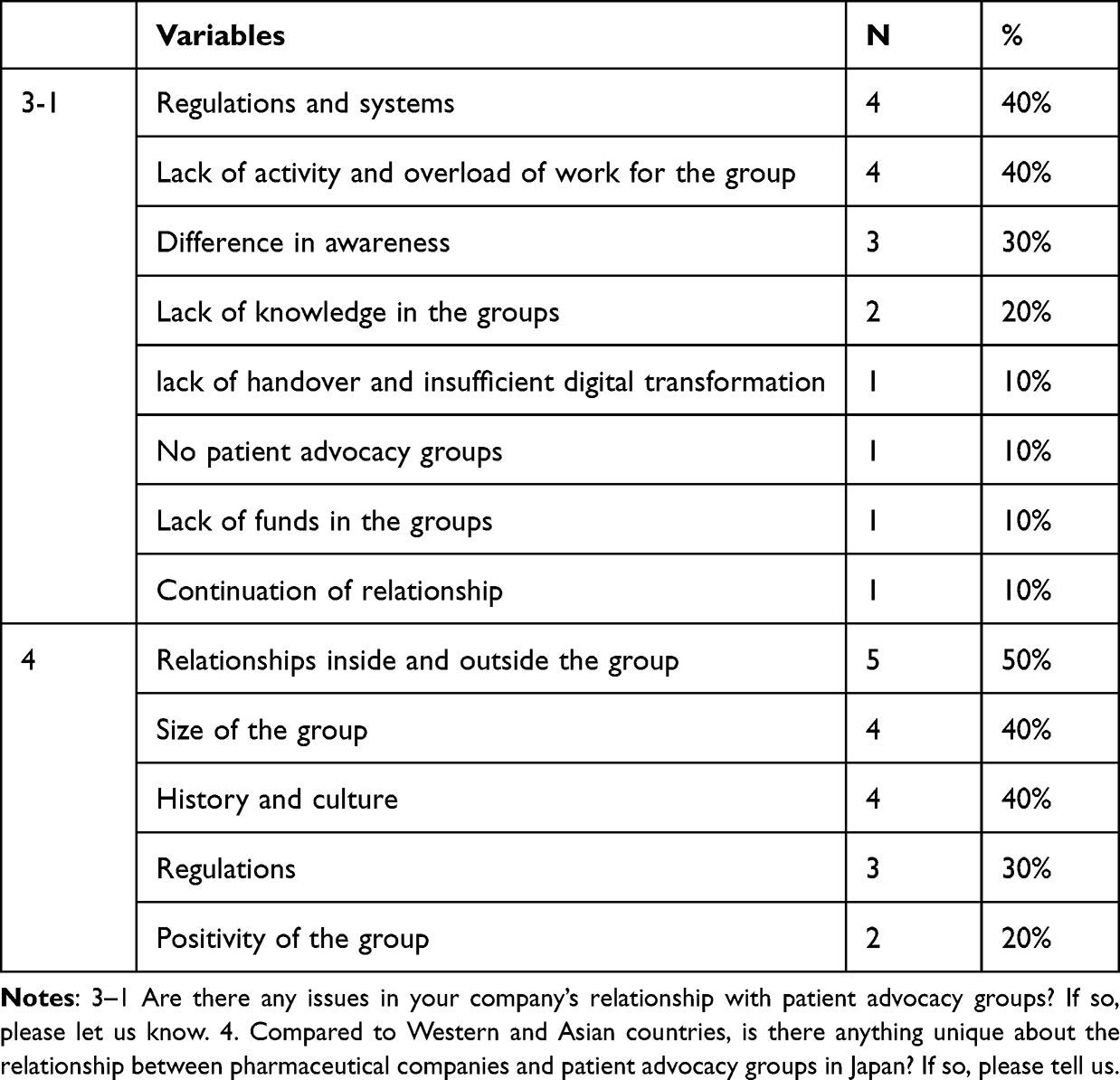 |
Table 3 Answers to Questions 3 and 4 |
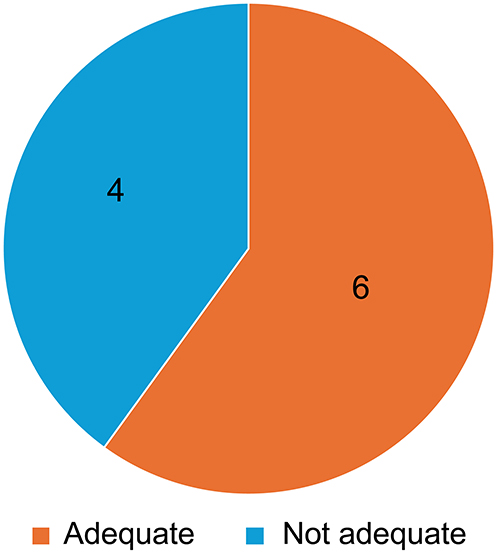 |
Figure 2 Answers to the question: 3–2 Would you say that current guidelines on financial relationships between pharmaceutical companies and patient advocacy groups are adequate?. |
For 4 “Compared with Western and Asian countries, is there anything unique about the relationship between pharmaceutical companies and patient advocacy groups in Japan? If so, please tell us”, half of the companies responded “relationships inside and outside the group” (50%). Specifically, it was highlighted that patient advocacy groups are not as large and more powerful than pharmaceutical companies, as is the case in Europe and the United States, and that the two parties are in a mutually supportive relationship. The next most common responses were “size of the group” and “history and culture” (both 40%). Regarding “size of the group”, it was found that in Japan, each patient group is small, with few nonpatient board members. This indicates the small budget and unsustainability of the groups. For “history and culture”, the respondents answered that patient advocacy groups in Japan had begun in response to harmful side effects, which differs from the origins of patient advocacy groups in other countries. It was also raised that in many cases the groups are operated by the parties concerned as voluntary activities, and there is a difference in culture where donations are few, unlike in other countries, and lobbying is seen as a form of bribery. With respect to “regulations” (30%), it was highlighted that drug promotion regulations in Japan are strict and that there is no need to appeal to the government for access to medicines due to the presence of universal health insurance. Regarding the “positivity of the group” (20%), patient advocacy groups in Japan were found to be conservative and nonpositive.
Discussion
Other Countries
In other countries, large amounts of financial support from pharmaceutical companies to patient advocacy groups have become problematic.4,11,20 Most patient advocacy groups receive funding, and the amount is growing,4 with many receiving donations exceeding USD 10 million per year from companies.1 Companies do not fund patient advocacy groups without reason.4 Funding purposes include philanthropic support, such as for advocacy and disease awareness activities, and support for interactions with parties outside the groups such as policy involvement.12 In addition, there is a high level of activity for commercial purposes, such as the approval of new drugs,1,3,4,21 to the extent that some patient advocacy groups decline financial support because they do not agree with the commercial intentions of pharmaceutical companies.4
Japan
This survey revealed that although pharmaceutical companies also fund patient advocacy groups in Japan, there is an emphasis on efforts to listen to the issues and voices of patients and their families. No commercial-minded responses were provided as to why pharmaceutical companies collaborate with patient advocacy groups, but this may be because of the systemic reason that patients are not allowed to be involved in the approval of new drugs in Japan. In addition, many pharmaceutical companies view patient advocacy groups as partners, and they see as necessary toward achieving a common goal of improving medicines and medical care. In some cases, pharmaceutical companies were unable to collaborate with patient advocacy groups because they could not find one that was active in their area of expertise, but this could be because the disease has not been recognized as a disease and no patient advocacy group exists for it. Another case in which collaboration was not possible was when patients were non-proactive about clinical trials. This result is consistent with that of a survey on patient advocacy groups.22 In addition, regarding issues in the relationship between patient advocacy groups and pharmaceutical companies, pharmaceutical companies find it difficult to foster interaction between patient advocacy groups and pharmaceutical companies in terms of regulations and systems. However, more than half of the respondents believed that there was no need to change current guidelines and regulations and that following the regulations of each company would be adequate. Thus, immediate regulatory improvements were deemed unnecessary. The emphasis on self-regulation rather than legal regulation was consistent with patient awareness.22
Comparison Between Other Countries and Japan
We will now compare the relationship between patient advocacy groups and pharmaceutical companies in Japan and other countries. Pharmaceutical companies often collaborate with patient advocacy groups related to their products, and cancer is a common area of focus for collaboration, similar to other countries.3,21 However, the relationship between pharmaceutical companies and patient advocacy groups in Japan substantially differs from that in other countries. Although donations from pharmaceutical companies to patient advocacy groups are considered to strongly influence their relationships, this survey revealed that in Japan, financial support is not as emphasized as in other countries; thus, there is less concern that this will weaken the independence of patient advocacy groups as in other countries.3,4
Uniqueness of Japan
Patient advocacy groups as well as the relationship between pharmaceutical companies and patient advocacy groups in Japan have some uniqueness when compared with those of other countries. The size of patient advocacy groups in Japan was found to be small, but this could be due to the membership of patient advocacy groups in Japan. In other countries, many nonpatient directors are affiliated with patient advocacy groups, and they are paid a salary, making them similar to corporate organizations. In contrast, patient advocacy groups in Japan are formed as patient-centered communities and are run by concerned parties as volunteers. As a result, it is more difficult for patient advocacy groups in Japan to work together, leading to non-proactive activities and excessive workloads when collaborating with companies. It has been reported that in some parts of the world, companies can manipulate patient advocacy groups by offering money,12 and conversely, patient advocacy groups can exert control over companies by negotiating and lobbying.23 However, considering the above, it appears that patient advocacy groups in Japan are not sufficiently developed to conduct such activities. There are also significant differences in the history of the patient advocacy groups. In other countries, patient advocacy groups have emerged to improve patients’ access to medicines. In contrast, in Japan, universal health insurance allows patients to obtain medicines without much difficulty, and patient advocacy groups have originated from the concept of patients helping each other or Japan’s unique concept of harmful side effects. These are the reasons for the paucity of policy proposals by patient advocacy groups in Japan. Given the aforementioned differences in the size and emergence of patient advocacy groups in Japan, these groups are not sufficiently developed to lobby and make policy proposals.
Conclusion
This study clarified the relationship between patient advocacy groups and pharmaceutical companies in Japan and its problems. In Japan, pharmaceutical companies work with patient advocacy groups as partners, with an emphasis on collaboration to listen to patients’ voices. This relationship is unique to Japan and is attributed to the drug approval and review system, strict regulations, historical background and the size of patient advocacy groups in Japan. Although there are some issues that make collaborations difficult because of regulations and the size of the groups, there is no immediate need for improvement. In Japan, it is unlikely that large amounts of financial support and the resulting collapse of independence of patient advocacy groups will become problematic, as is the case overseas, and it is unlikely that the relationship with pharmaceutical companies will become similar to that in other countries in the future.
Limitation
We requested interviews with a total of 20 companies, which are the top 10 companies in Japan and worldwide, respectively, but we did not receive responses from all the companies, and only 10 companies responded. In addition, the results rely solely on information obtained from interviews with pharmaceutical companies, which cannot be verified using other publicly available data and may be one-sided on the part of the companies. The sample size is relatively small, with only 10 companies interviewed, potentially limiting the generalizability of the results.
Furthermore, this study collected perspectives solely from pharmaceutical companies and did not include the viewpoint of patient support organizations.
Data Sharing Statement
The data supporting the results of this study can be obtained from the corresponding author, Hideki Maeda, at [email protected], upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Meiji Pharmaceutical University Ethics Review Committee (Approval number: 202209). The research team briefly explained the purpose of the interview to the interviewees and conducted the interviews after obtaining their consent.
Consent for Publication
The interviewee has provided written consent to publish the results of the research in an academic journal after anonymizing them so that individuals cannot be identified.
Acknowledgments
We thank Crimson Interactive Pvt. Ltd. (Ulatus) – www.ulatus.jp for their assistance with manuscript translation and editing.
Funding
This survey was conducted using research funds obtained from the Regulatory Science Laboratory at Meiji Pharmaceutical University and the Medical Governance Research Institute.
Disclosure
Akihiko Ozaki has received consulting fees from Mnes Inc. and honoraria for lecturers from Kyowa Kirin Corporation, Pfizer Japan Inc., Taiho Pharmaceutical Co., Ltd., and Daiichi Sankyo Co., Ltd, personal fees from Becton, Dickinson and Company; in addition Dr. Ozaki is engaged in ongoing research examining financial and non-financial conflicts of interest among healthcare professionals and pharmaceutical and medical device companies in Japan. Tetsuya Tanimoto has also received consulting fees from Mnes Inc, and Bionics Co., Ltd, personal fees from Medical Network Systems. The other authors have no conflicts of interest to declare.
References
1. McCoy MS, Carniol M, Chockley K, Urwin JW, Emanuel EJ, Schmidt H. Conflicts of interest for patient-advocacy organizations. N Engl J Med. 2017;376(9):880–885. doi:10.1056/NEJMsr1610625
2. Lexchin J. Association between commercial funding of Canadian patient groups and their views about funding of medicines: an observational study. PLoS One. 2019;14(2):e0212399. doi:10.1371/journal.pone.0212399
3. Mulinari S, Vilhelmsson A, Rickard E, Ozieranski P. Five years of pharmaceutical industry funding of patient organisations in Sweden: cross-sectional study of companies, patient organisations and drugs. PLoS One. 2020;15(6):e0235021. doi:10.1371/journal.pone.0235021
4. Parker L, Fabbri A, Grundy Q, Mintzes B, Bero L. “Asset exchange”-interactions between patient groups and pharmaceutical industry: australian qualitative study. BMJ. 2019;367:l6694. doi:10.1136/bmj.l6694
5. House T, O’Donnell K, Saich R, et al. The role of patient advocacy organizations in shaping medical research: the Pompe model. Ann Transl Med. 2019;7(13):293. doi:10.21037/atm.2019.04.28
6. Poortman Y, Ens-Dokkum M, Nippert I. The role of patient organizations in shaping research, health policies, and health services for rare genetic diseases: the Dutch experience. Genes. 2024;15(9):1162. doi:10.3390/genes15091162
7. Stein S, Bogard E, Boice N, et al. Principles for interactions with biopharmaceutical companies: the development of guidelines for patient advocacy organizations in the field of rare diseases. Orphanet J Rare Dis. 2018;13(1):18. doi:10.1186/s13023-018-0761-2
8. Gonzalez AR. Patient advocacy history, evolution and impact on health. JOJ Pub Health. 2018;3(3):555615. doi:10.19080/JOJPH.2018.03.555615
9. Li DG, Singer S, Mostaghimi A. Prevalence and disclosure of potential conflicts of interest in dermatology patient advocacy organizations. JAMA Dermatol. 2019;155(4):460–464. doi:10.1001/jamadermatol.2018.5102
10. Heywood M. South Africa’s treatment action campaign: combining law and social mobilization to realize the right to health. J Hum Rights Pract. 2009;1:14–36. doi:10.1093/jhuman/hun006
11. Fabbri A, Parker L, Colombo C, et al. Industry funding of patient and health consumer organisations: systematic review with meta-analysis. BMJ. 2020;368:l6925. doi:10.1136/bmj.l6925
12. Ozieranski P, Rickard E, Mulinari S. Exposing drug industry funding of UK patient organisations. BMJ. 2019;365:l1806. doi:10.1136/bmj.l1806
13. Mandeville KL, Barker R, Packham A, Sowerby C, Yarrow K, Patrick H. Financial interests of patient organisations contributing to technology assessment at England’s national institute for health and care excellence: policy review. BMJ. 2019;364:k5300. doi:10.1136/bmj.k5300
14. Kang SY, Bai G, Karas L, Anderson GF. Pharmaceutical industry support of US patient advocacy organizations: an international context. Am J Public Health. 2019;109(4):559–561. doi:10.2105/AJPH.2018.304946
15. Herxheimer A. Relationships between the pharmaceutical industry and patients’ organisations. BMJ. 2003;326(7400):1208–1210. doi:10.1136/bmj.326.7400.1208
16. O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
17. Ministry of Health, Labour and Welfare. Statistics on Pharmaceutical and Medical Device Industry, the Japan Pharmaceutical Manufacturers Association DATA BOOK 2025; 2025. Available from: https://www.jpma.or.jp/news_room/issue/databook/en/eo4se300000058qp-att/DATABOOK2025_en.pdf.
18. Kallio H, Pietilä AM, Johnson M, Kangasniemi M. Systematic methodological review: developing a framework for a qualitative semi-structured interview guide. J Adv Nurs. 2016;72(12):2954–2965. doi:10.1111/jan.13031
19. Mayring P. Qualitative content analysis: theoretical foundation, basic procedures and software solution. In: Flick U, editor. The SAGE Handbook of Qualitative Data Analysis. Thousand Oaks, CA: SAGE Publications; 2014:171–185. doi:10.1007/978-94-017-9181-6_13
20. Parker L, Grundy Q, Fabbri A, Mintzes B, Bero L. ‘Lines in the sand’: an Australian qualitative study of patient group practices to promote Independence from pharmaceutical industry funders. BMJ Open. 2021;11(2):e045140. doi:10.1136/bmjopen-2020-045140
21. Gentilini A, Parvanova I. Industry funding of patient organisations in the UK: a retrospective study of commercial determinants, funding concentration and disease prevalence. BMJ Open. 2023;13(6):e071138. doi:10.1136/bmjopen-2022-071138
22. Murayama A, Senoo Y, Harada K, et al. Awareness and perceptions among members of a Japanese cancer patient advocacy group concerning the financial relationships between the pharmaceutical industry and physicians. Int J Environ Res Public Health. 2022;19(6):3478. doi:10.3390/ijerph19063478
23. Gentilini A, Miraldo M. The role of patient organisations in research and development: evidence from rare diseases. Soc Sci Med. 2023;338:116332. doi:10.1016/j.socscimed.2023.116332
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.