Back to Journals » Clinical Interventions in Aging » Volume 17
Interactions Between EIP on AHA Reference Sites and Action Groups to Foster Digital Innovation of Health and Care in European Regions
Authors Illario M, De Luca V ![]() , Onorato G, Tramontano G, Carriazo AM, Roller-Wirnsberger RE
, Onorato G, Tramontano G, Carriazo AM, Roller-Wirnsberger RE ![]() , Apostolo J, Eklund P, Goswami N
, Apostolo J, Eklund P, Goswami N ![]() , Iaccarino G, Triassi M, Farrell J, Bousquet J
, Iaccarino G, Triassi M, Farrell J, Bousquet J
Received 7 June 2021
Accepted for publication 22 February 2022
Published 2 April 2022 Volume 2022:17 Pages 343—358
DOI https://doi.org/10.2147/CIA.S323723
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Maddalena Illario,1– 3 Vincenzo De Luca,1 Gabrielle Onorato,2 Giovanni Tramontano,2,3 Ana Maria Carriazo,2,4 Regina Elisabeth Roller-Wirnsberger,5 Joao Apostolo,6 Patrik Eklund,7 Nandu Goswami,8 Guido Iaccarino,9 Maria Triassi,1 John Farrell,2 Jean Bousquet2,10
1Dipartimento di Sanità Pubblica, Università degli Studi di Napoli Federico II, Naples, Italy; 2Executive Board, EIP on AHA Reference Sites Collaborative Network, Brussels, Belgium; 3Research & Development Unit, Azienda Ospedaliera Universitaria Federico II, Naples, Italy; 4Deputy Regional Ministry, Regional Ministry of Health and Families of Andalusia, Seville, Spain; 5Department of Internal Medicine, Medical University of Graz, Graz, Austria; 6Health and Care Sciences Research Unit, Escola Superior de Enfermagem de Coimbra, Coimbra, Portugal; 7Department of Computing Science, Umeå University, Umeå, Sweden; 8Division of Physiology, Medical University of Graz, Graz, Austria; 9Dipartimento di Scienze Biomediche Avanzate, Università degli Studi di Napoli Federico II, Naples, Italy; 10MACVIA-France, Fondation partenariale FMC VIA-LR, Montpellier, France
Correspondence: Maddalena Illario, Dipartimento di Sanità Pubblica, Università degli Studi di Napoli Federico II, Via Sergio Pansini n.5, Naples, 80131, Italy, Tel +39 0817464211, Fax +39 0817464212, Email [email protected] Nandu Goswami, Division of Physiology, Medical University of Graz, Neue Stiftingtalstraße 6, Graz, 8010, Austria, Tel +43 31638573852, Fax +43 31638579005, Email [email protected]
Abstract: The article describes some of the achievements of the European Innovation Partnership on Active and Healthy Ageing (EIP on AHA), after eight years in operation. These results were achieved thanks to the collaborative work of the action groups (AGs) and reference sites (RSs). RS regional ecosystems include key organisations committed to investing in innovation to foster active and healthy ageing. The AGs are groups of professionals committed to sharing their knowledge and skills in active and healthy ageing. This article reports on the approach used by the EIP on AHA to bring together experts and regions in identifying and addressing these challenges. Synergies between AGs offered substantial support to RSs, allowing regional health and care priorities and challenges to be identified and pursued through AG commitments. Building upon the experiences of the EIP on AHA, the Reference Sites Collaborative Network has set up a number of thematic action groups that bring together multidisciplinary experts from across Europe to address the main health and social care challenges at regional, national and European level.
Keywords: active and healthy ageing, digital health, health policy, health innovation
Introduction
The European Innovation Partnership on Active and Healthy Ageing (EIP on AHA) was launched in 2012 within the Innovation Union policy of the European Commission (EC) and was operational until December 2020. The aim was to tackle the challenges of demographic changes in European Union (EU) Member States and regions.1 The EIP on AHA had two main pillars: “Reference Sites” and “Action Groups”. This paper will provide an overview of the aims, structures, activities and main results of the EIP on AHA (many of which have persisted), evaluating its successes and areas where it faced challenges in order to help explain this complex structure and understand how such collaborative, interdisciplinary and transnational initiatives can deliver improved outcomes for all and particularly older European citizens.
After eight years of activity, many achievements have been obtained through commitments or collaborative work of the Action Groups (AGs) as well as through the extensive work carried out by Reference Sites (RSs) in the RSCN (Reference Sites Collaborative Network).2,3 However, they were often working in silos and there was an unclear strategy on how to reduce fragmentation between EIP on AHA members’ individual commitments, AGs and RSs activities.
An Action Group (AG) is a community of professionals, entrepreneurs, researchers and experts committed to working on active and healthy ageing in the several knowledge areas that affect it. AGs facilitate knowledge sharing and increase the value of national and local experiences, helping to identify areas for improvement and therefore targeted investment at European level.
There were six AGs in the EIP on AHA:
- Adherence to prescription (AG A1);
- Falls prevention (AG A2);
- Lifespan Health Promotion and Prevention of age-related frailty and disease (AG A3);
- Integrated care (AG B3);
- Independent living solutions (AG C2);
- Age friendly environments (AG D4).
The composition of the AGs was multi-sectoral and multi-level, covering local, regional, national and European levels. Stakeholders ranged from academia to public authorities, and included large industry and SMEs, health and care organisations, investors and innovators, as well as end-users and patient associations. They were self-managed and independent. The AGs defined action plans in which they identified overall priorities, objectives and activities.4
Reference Sites are ecosystems aimed at adopting and transferring creative and practicable solutions to improve the quality of life and health of older people and the whole community, increasing equity and social sustainability. The Reference Sites bring together leading regional organisations committed to investing in innovation for active and healthy ageing and supporting the transfer and dissemination of such innovation across Europe. A Reference Site is typically based on a “Quadruple Helix” model, which ensures collaboration between actors from different sectors to better understand the organisational, technical and financial challenges facing the region. The regional health and social care authorities are key stakeholders in the Reference Site. Such “Quadruple Helix” approach ensures that a wide range of participants (public bodies and healthcare providers/industry/academia/civil society) are brought together in a coherent partnership to understand and address the challenges of delivering health and care services to an older population. Indeed, collaborations can drive structural change far beyond the scope that any particular organisation could achieve on its own.
Furthermore, Reference Sites facilitate the transfer and adaptation of knowledge from European regions to local realities, and vice versa, with the aim of promoting regional, social and economic development in the long term.3
The EIP on AHA also implemented three cross-cutting initiatives: The “Blueprint on Digital Transformation of Health and Care (Blueprint)”, “Innovation to Market (I2M)”, and “Monitoring Assessment Framework for the EIP on AHA (MAFEIP)”.
The Blueprint5 was an iterative process operated between the EC and the stakeholders (policy makers and other key opinion leaders) to digitally innovate health and care in Europe. It represented the political vision of the EIP on AHA and followed the scaling up strategy for AHA.6
Innovation to Market (I2M)7 aimed to promote the matching of demand and supply of digital health and care solutions in a cross-border context. This horizontal action is part of the EC strategy on the digital transformation of health and care in the digital single market.8
MAFEIP9 is a tool for the monitoring and assessment of the impact of innovative solutions and approaches to support evidence-based decision-making for all institutions and users in the health and care sector.
Potential Value of Interactions Between Reference Sites and Action Groups
The main aim of the RSs was to implement regional stakeholder coalitions that support the research, development and adoption of new solutions and enable the large-scale adoption and transferability of good practices within their region. Developing effective and sustainable synergies with AGs offered greater support to RSs in that regional health and care priorities and challenges could be identified and taken forward through AG commitments. This frontend identification of regional commitments based on real health and care challenges and priorities helped, at the back end of the process, to ensure that recommendations from the AGs were implemented as part of regional health and care plans. In addressing regional challenges and priorities, it was important that AGs developed synergies amongst themselves so as to ensure that a holistic view was taken in the development of recommendations and solutions. Building synergies between RSs and AGs and between different AGs accelerated the development, deployment and adoption of innovative health and social care, linking health and care services to the patient/user. The user was placed at the centre of the solution design and development process. This enabled the adoption of delivery models and digital solutions for AHA that have had real impact, and that made a real contribution to the sustainability of services, thus driving innovation forward.2 The following section describes some successful examples of interactions between AGs and RSs. Some of these arose from within RSs and were further supported and accelerated by activities within AGs. Other examples of solution provision were rooted in AGs activities, reaching out to become fully implemented in regions and RSs.
An Integrated Care Pathway for Airway Diseases
Allergic Rhinitis and Its Impact on Asthma of the Mobile Airways Sentinel Network
Allergic Rhinitis and its Impact on Asthma of the Mobile Airways Sentinel networK (MASK-ARIA) is considered a good practice by DG Santé in digital and patient-centred care.4
The MASK-ARIA initiative led to the development of tools to support healthcare professionals in shared decision making through an interoperable electronic decision support system (e-CDSS).10 MASK-ARIA has also developed an interoperable web-based questionnaire for physicians,11 a questionnaire for the screening and management of allergic diseases (CARAT®) and a sentinel network for air quality during pollen seasons.
From this initiative, the MASK-air® app was developed. It is linked to an electronic platform for monitoring allergic diseases and asthma.12 The app aims to support patient decision-making to improve the management of asthma and rhinitis through a patient-centred approach. The app is freely available on Android and iOS in 27 countries and 20 languages. MASK-air® complies with the General Data Protection Regulation (GDPR), governing the processing of personal data in the European Union (EU).13
A Twinning Project for Rhinitis and Asthma
A twinning project allowed the transfer of innovations developed by MASK-ARIA from the MACVIA-France RS (MASK-air®)14 and Porto@ageing (CARAT®)15 to 22 other Reference Sites12 across Europe (Figure 1). Transnational collaboration with scientific organisations and health authorities has allowed comparison of the phenotypic characteristics of rhinitis and asthma multimorbidity in adults and the older people in the regions involved.
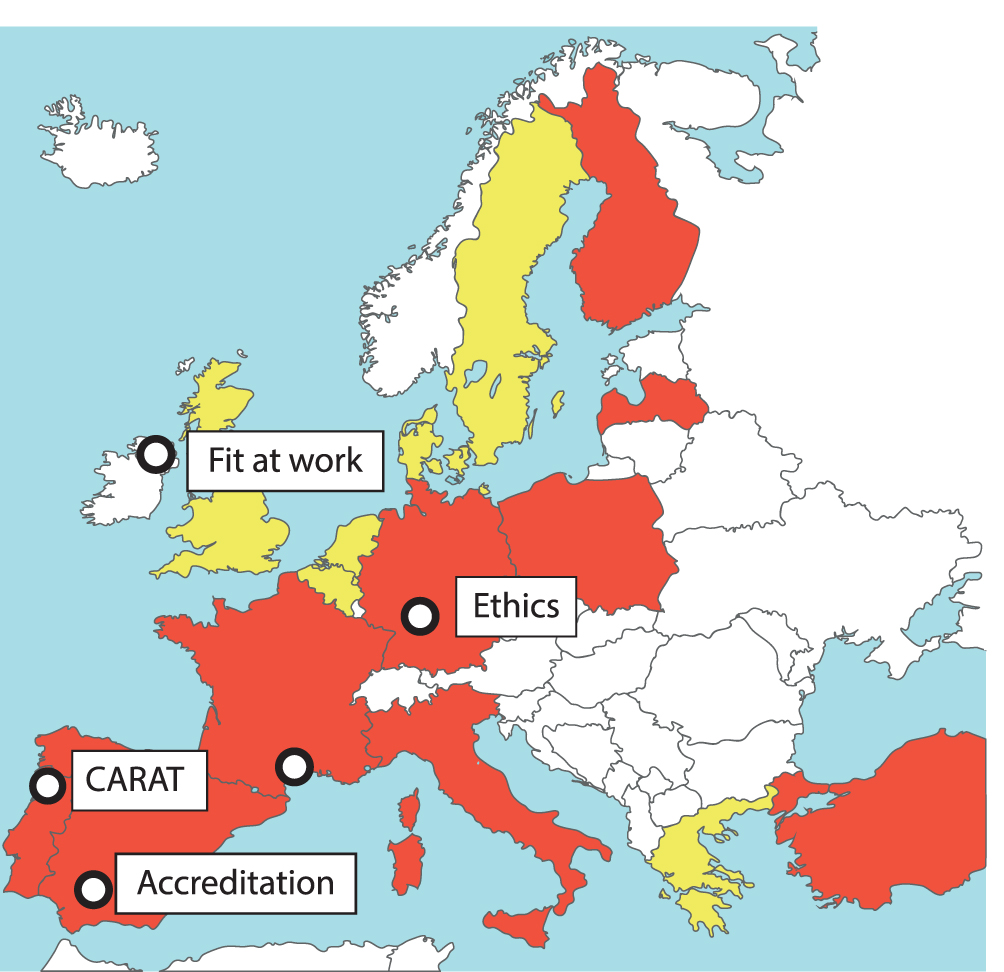 |
Figure 1 Participating countries in the MASK-ARIA twinning. In yellow, countries with a twinning activity. In red, twinning in the entire country. The twinning RS originator is: MACVIA-France. The twinning RS adopters are: Aragon, Campania, Catalonia, City of Helsinki, Ageing@Coimbra, Heraklion, Kohln-Bonn, Life Tech Valley, Liguria, Lodz, Medical Delta, Milan Metropolitan – Bergamo Province, NHS24, Northern Ireland, Olomuc, Pays de la Loyre, Porto4Age, Apulia, Piedmont, Southern Denmark, Nouvelle Aquitaine, Turkey. Twinning organizations in Sweden and Lithuania are not RSs. |
This twinning project resulted in the enrolment of more than 1050 patients, of whom more than 200 were aged over 65 years. The twinning network also resulted in an EIT Health grant (POLLAR: Impact of air pollution on asthma and rhinitis).16
A Twinning Project for Severe Asthma
The results of the first twinning prompted MASK-ARIA to initiate a second twinning, including more than 130 centres in 27 countries worldwide, in order to reduce the burden of severe asthma in an older adult population.
Dealing with Frailty in Older Adults Through ICT-Supported Integrated Services
The Personalised ICT Support Service for Independent Living and Active Ageing (PERSSILAA) is an A3 AG commitment built upon an EU project, aimed at assessing the health status of community-dwelling older adults. Through an interoperable ICT solution, PERSSILAA develops service modules for the screening, prevention intervention and monitoring of frailty in older adults as well as citizen empowerment.17,18 In the initial validation in the Netherlands, 3.777 older adults were screened for frailty before preventative ICT strategies were trialed for a subsample.19
This approach to frailty prevention and management in Campania is in line with regional priorities for health innovation and active ageing. It lies in the framework of a proactive, person-centred ecosystem, supporting the adoption of innovative, validated solutions that have been piloted by the stakeholders of the ProMIS (Programma Mattone Internazionale Salute) regional network.20
Twinnings for the Transfer of Good Practices on Frailty Domains
Through the interaction between Campania Reference Site and the A3 Action Group of the EIP on AHA, it was possible to identify and implement innovative approaches to the prevention and management of frailty, integrating the biomedical paradigm of frailty with the “bio-psycho-social” paradigm.21 Structured collaboration with other RSs has been identified as a valuable opportunity to transfer good practices addressing frailty domains, for which several twinnings have been established. A table summarising the twinning experiences is provided below (Table 1).
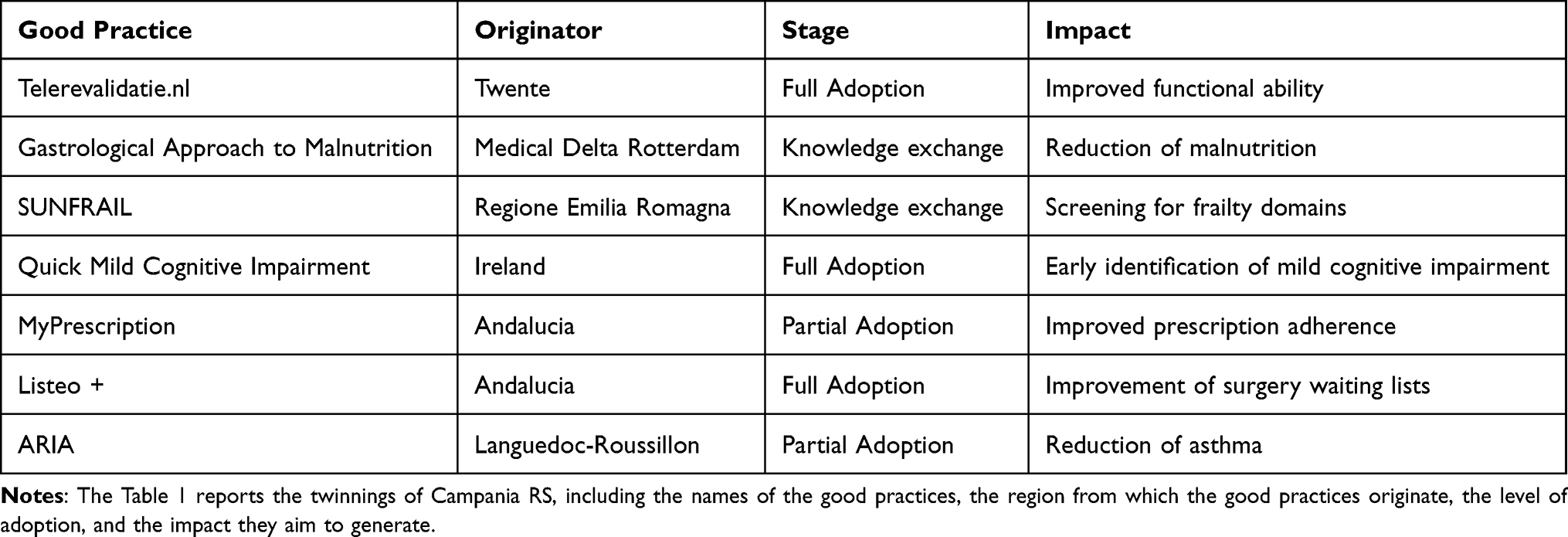 |
Table 1 Campania Twinnings Summary |
ARIA in Campania
“ARIA in Campania” is the Italian version of MASK-air®. It is used as a multi-sectoral pathway for rhinitis and related multi-morbidity in older adults, through the involvement of pharmacists and physicians in the territory.4
Quick Mild Cognitive Impairment Screen – Development and Twinning
The Quick Mild Cognitive Impairment (Qmci) screen is an innovative short cognitive screening tool that was developed as part of the EIP on AHA, aimed at identifying subjects with mild cognitive decline. The multi-centre study conducted in Campania, Italy validated the Italian version of the Qmci screen (Qmci-I), obtaining normative data.22 A subsequent study made it possible to clarify the diagnostic properties of the Qmci-I in the classification of MCI subtypes.23 Twinning initiatives between sites in Ireland, Italy, Spain, Portugal and in the second round, Crete (Greece), to develop translations of an electronic version of the Qmci screen were also successful, contributing to the creation of the RAPid Community COGnitive screening (RAPCOG) programme24 that was developed by Ireland’s RS.25
ICT-Supported Adapted Physical Activity
ITALY.TELEREVALIDATIE.NL is a web-based solution for prescribing adapted physical activity to chronic disease patients and community-dwelling older adults. It provides tailored information and a personalised training programme with an instructional video and adherence monitoring tool26 that has been integrated in the Adapted Physical Activity offer of the Sport Service of Federico II University Hospital.
A Gastrological Approach to Malnutrition
The gastrological approach is an ICT-supported personalised intervention. It includes screening, assessment and monitoring tools as well as personalised interventions aimed at improving food intake in older adults.27 An inter-professional gastro-team manages the digital Modular Gastrological Platform (MGP) empowering patients on cooking processes in order to benefit from healthy and delicious meals. A new training for chefs is currently being designed and implemented by NECTAR Erasmus+ project.
Screening for Frailty in Community-Dwelling Older Adults
SUNFRAIL is a 9-item tool developed according to the bio-psycho-social model of frailty, aimed at the early identification and prevention of frailty in older people in the context of primary care. It aims to develop, validate and test an innovative intervention model to improve the detection, prevention and treatment of frailty and the management of multi-morbidity.28
Monitoring Adherence to Prescription
myPrescription is a mobile app enabling the management of multiple drug treatments prescribed by professionals. It schedules alarms for the administration of the drugs. In addition, myPrescription offers a barcode reader to access all the information of a given medication.
A Living Lab for Active and Healthy Ageing
ICT tools have been transferred to Campania to address the need for the implementation of integrated health and care services, and for multidisciplinary paths at home or in common aggregation points (Living Labs). “Living Lab per l’Invecchiamento Sano e Attivo” (LISA) is an interactive and integrated approach based on collaboration between the territorial social and healthcare services and the community. Its aim is to improve the independent living of older adults, helping them to play an active role in society29 (Figure 2).
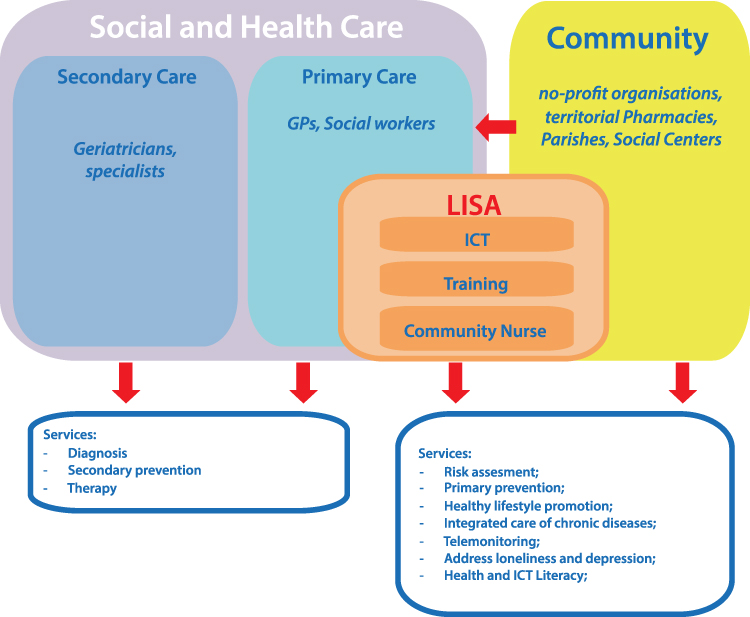 |
Figure 2 LISA (Living Lab per l’Invecchiamento Sano e Attivo – Living Lab for Active and Healthy Ageing) is an approach for the integration of social and health services addressing prevention of frailty in community-dwelling older adults in Campania. The approach takes advantage of information technology, health literacy programs and non-health services offered by new professional figures to support older people in preventing and managing chronic non-communicable diseases. |
Healthy Ageing Promotion Through Digital Solutions
The “En Buena Edad” Platform
“En Buena Edad”30 is one of the Andalusian commitments of the EIP on AHA A3 AG. It is a digital platform aimed at facilitating communication among elderly people, professionals and families, for the promotion of active and healthy ageing in Andalusia. It offers information, tools and resources in the field of health promotion, citizen participation, safety and lifelong learning opportunities.
Twinning with Scotland’s Reference Site
During the initial development of the platform, a twinning activity was set up. The twinning activities carried out under the Scale-AHA Coordination and Support Action (CSA)31 facilitated learning about the Scottish self-management collaborative platform: Living it Up. The twinning allowed learning in the design and management of platforms aimed at citizens, in particular the elderly, starting from the experiences and results of Living it Up. The Twinning enabled synergies to be created between regions, including relevant experts and stakeholders, to facilitate knowledge transfer and long-term learning.
Representatives from Andalusia had the opportunity to visit and study in detail the Scottish platform “Living it Up”. In-depth sessions regarding upload of contents, dissemination activities, validation, and others were shared among participants.
“En Buena Edad” is a platform of services for people over 65 and their families to promote active and healthy ageing. It is part of the Andalusian Health Plan and the Andalusian Plan for the Promotion of Personal Autonomy and the Prevention of Dependency.
En Buena Edad aims to provide a centralised tool for the provision of information, tools and advice on active ageing, supporting older people in decision-making and providing a space for communication with professionals and stakeholders. The platform gathers best practices for active ageing and scientific evidence for their dissemination. European Regional Development Funds (ERDF) were used for the development and implementation of the platform.
Highlights of Twinning Activites
The design process started at the end of 2015. Between the last quarter of 2016 and the first quarter of 2017, the participatory design phase of the digital platform (“Design thinking” methodology) was completed. The En Buena Edad platform was launched in 2018. Its development involved the participation of health and social services professionals as well as professionals from other areas (education, justice, planning, etc.), public and private companies related to the sector and associations of older people as well as citizens in general. Using a design thinking methodology, more than 400 people participated in the design in three different ways: (i) scientific committee: representatives of comprehensive plans and strategies of the public health system of Andalusia (Regional Ministry of Health of Andalusia); (ii) partnership committee with 29 public and private institutions and (iii) provincial meetings, where 363 people participated representing citizens, institutions, and other sectors.32,33
Today the platform is fully implemented and operative (www.enbuenaedad.es). The tool is used in daily life and offers information on the four pillars of healthy ageing: health, safety, participation and long-life learning, with a total of 1064 contents (662 by platform users). The Platform is available in Spanish. English and French versions are partially developed.
Transferring Action Group Commitments to the Reference Site of Styria, Austria
Since 2013, the Medical University of Graz (MUG) has committed to collaborate under the umbrella of the A3 AG, leading the innovation processes on frailty prevention and management. Following successful application and set up of the Styrian Reference Site, the inter-twinning between the activities of MUG and the partners in the A3 AG and regional stakeholders in the Reference Site led to sustainable development and innovation.
Development of an Ecosystem for Active and Healthy Ageing in Styria
In a one-year project, funded by the Government of Styria, partners within the RS, and under the co-lead of MUG, developed a framework of an ecosystem on active and healthy ageing using a mixed model approach including stakeholders from macro-meso and micro level in the province of Styria, (Austria). Nine recommendations for the deployment of a healthy ageing region could be derived from the key results.34 Figure 3 shows humans, institutions and legal bodies and their position in the Active and Healthy Ageing Ecosystem of Styria, according to results from the study presented in the current publication.
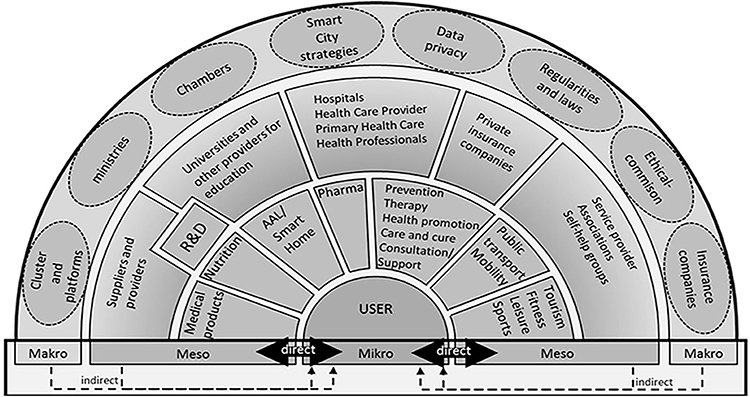 |
Figure 3 Styrian Reference Site ecosystem. The figure shows the mapping of the relevant stakeholders of the Styria Reference Site Ecosystem, highlighting the communication paths and relationships between them. Notes: Reproduced from Borrmann M, Lindner S, Hofer-Fischanger K, et al. Strategy for Deployment of Integrated Healthy Aging Regions Based Upon an Evidence-Based Regional Ecosystem-The Styria Model. Front Med (Lausanne). 2020;7:510475. Creative Commons license and disclaimer available from: http://creativecommons.org/licenses/by/4.0/legalcode.34 |
Based on this model and the continuous interaction between MUG and Styria Reference Site, partners decided to make use of the regional capacity and condense the action in model-regions, focusing on topics that had been detected as strengths during the first phase of co-creation.
Integrated Nutritional Care for People Discharged from Acute Care
Under the auspices of MUG, an evidence-based nutrition documentation tool (NDoc) was developed involving many partners from the A3 action group of EIP on AHA. Furthermore, this tool was regionally validated for clinical usability. Once this process was concluded, the research results were translated into the electronic health record system of the Styrian Hospitals (KAGES) and scaled up within the whole reference site. It is nowadays part of every discharge record of patients discharged from public hospitals in our reference site.35
Evidence Based Health Tourism for Older Patients with Complex Care Needs
Based on the capacities detected during the design of the Styrian Ecosystem for Active and Healthy Ageing, partners from the A3 AG started a structured collaboration with partners from the tourism and re-creation sectors of the Region of Bad Radkersburg. The Reference Site Styria organised the first Alpe-Adria Meeting for Active and Healthy Ageing with participation from Austria, Slovenia and Italy.36 The main focus was a collaboration between medical specialties, other healthcare professionals, and local tourism offers in order to adapt and offer interventions for evidence-based secondary and tertiary care prevention during recreation and health tourism.
Fall Prevention Initiatives Started by the Styrian Insurance Provider
Working very closely with A2 AG key stakeholders, a 12-week physical activity programme for falls prevention has been established by the Styrian health insurance (ÖGK). The training programme aims to promote mobility in people above 65 and, therefore, to improve independence and prevent the risk of serious falls. Led by a sports scientist and physiotherapist with a specialization in falls prevention, the participants are instructed through different exercises that aim at improving balance and strength, but also cognitive function. This innovative initiative is provided in cooperation with older adults with other key centres in active and healthy ageing: eg the MUG or the Graz geriatric centre (GGZ).
Establishment of a Network for All Stakeholders in Healthcare for Ageing
The Styrian network for geriatric medicine (Netzwerk Altersmedizin Steiermark) has been established (i) to enhance cooperation between GGZ and the MUG, (ii) to establish quality standards for medical treatment and care in older people and (iii) to jointly organise medical congresses and advanced training events for health professionals.
Together with the Human Technology Cluster Styria and AAL Austria, supported by the Styrian Health Care fund, the Styrian governor, the mayor of Graz and other agencies involved in ageing care, the first conference on Active and Healthy Ageing was held from the 10th to 12th October 2019 at the MUG. The conference was attended by more than 380 participants, including local and national key stakeholders in ageing care.
Commitments and Projects for the Promotion of Active and Healthy Ageing in Coimbra, Portugal
The synergies and collaborations established between the different members of Ageing@Coimbra RS, through the work of the AGs, drive the creation, development, and dissemination of innovative solutions for AHA covering a significant population. The concept, structure and mission of Ageing@Coimbra were used to inspire other RS candidates in Poland, Spain and Portugal.37
A Coordinated Approach for the Management of Multimorbidity and Polypharmacy
The Stimulating Innovative Management of Polypharmacy and Adherence in the Elderly (SIMPATHY) EU project focused on integrated care models to mitigate inappropriate polypharmacy and reduce problems related to low adherence. The SIMPATHY A1 AG good practice was a strong contributor to the safe, efficient, effective and sustainable deployment of health resources from the point of view of both health systems and society.38 Starting from the SIMPATHY experience, Ageing@Coimbra developed a white paper on the management of multi-morbidity in older adults. It resulted in (i) a coordinated approach between healthcare professionals and the transition of healthcare levels, (ii) a tool for professional development, and (iii) an exchange of good practices between pharmacists in different countries (eg collaboration between the Portuguese Pharmaceutical Society and the Valencian Association of Pharmacists).
A Collaborative Work for Falls Prevention
Aging@Coimbra’s stakeholders are active members of the A2 AG, working on developing:
- prevention of falls in nursing homes;
- implementation of the Humanitude Care Methodology (HCM) in long-term care;
- contributions to fall prevention, Multimodal exercise and Branch chained amino acids (BCAAs) supplementation on falls prevention, physical functioning and psychological health in institutionalised older adults.
In the context of personalised health management and the prevention of falls, Ageing@Coimbra developed collaborative work in the Fall Prevention for Dissemination Network, for the dissemination and implementation of best practices in falls prevention across Europe.39
Address Frailty by Sharing Knowledge and Good Practices
The FOCUS40 project aims to share approaches and good practices to address frailty in Europe. The project enabled the meta-analyses of available evidence from frailty screening tools, epidemiological studies and intervention studies in frail older adults’ health care.41,42
Robotics Service in Assisted Living Environments
Ageing@Coimbra’s members of the C2 AG participated in the GrowMeUp project, aimed at developing robotics services in assisted living environments to help older adults remain active and independent for longer.43 In this focus, some of the commitments are for the development of interoperable independent living solutions:
- Cognitive training and physical stimulation for people at risk of developing cognitive impairment (CogniViTra);
- Rose-Robot Sensing Tele-Ecography;
- Better conditions at work and home to enable active healthier lifestyles (H2020 Smartwork and H2020 Homes4Life);
- Cognitive and physical rehabilitation at home through assistive technologies (project ReHab).
Healthy Living Room for a Participatory Community
HeaLIQs4Cities is a D4 commitment aimed at boosting healthy lifestyles by promoting the interaction between citizens and academia, healthcare enterprises and local government. Citizens were engaged in a Healthy Living Room to test Innovative technologies and to receive simple and accurate messages about healthy lifestyles. In 2019, the LIQs Mobile Healthy Living Room reached citizens in rural areas in the neighbourhoods of Coimbra. Besides the individual lifestyle assessment and recommendations, LIQs promoted a participatory community programme aiming to encourage healthier behaviours and environments.
Falls Prevention Programs in Northern European Reference Sites
This group was built from existing falls prevention programmes and guidelines available at European and international levels. Its aim is to describe and share good practices across member states. There was a need to overcome bottlenecks in the twinning and scaling up of falls prevention related good practices due to differences in regional and national health administration models. To this purpose, care pathways and the integration of care involving multiple care sites and multi-professionality had to be described in detail, according to the newly developed INFORMATION&PROCESS models, firstly targeted for Ireland and Scotland. A typical bottleneck was the availability of fragmented data and databases related with falls, injuries and interventions. Indeed, national and regional data sets and databases are typically established and driven locally and with a certain ambition to support studies of various kinds. The size of the smaller data sets is typically less than 1000 cases. Larger data sets, often technically organised as databases, exist (eg in Northern European countries, particularly for quality assurance purposes). For instance, in Sweden, among the National Quality Registries (Nationella kvalitetsregister), there are registries for hip fractures, hip prosthesis and for the management of arthritis. Analytics of these data have been leading to important observations, in turn acting as groundwork for developing various kinds of recommendations and guidelines. Furthermore, the need emerged to expand education programmes to support falls and injury prevention at the individual, organisation and societal levels. This would enable the sharing of innovations with and between health and social care workers and instructors around Europe. Personalisation and self-management are key when aiming at individuals acting to change behavior and routines in order to lower their injury risk, using reinforcement, whether adopted in macro-scale campaigns or micro-scale personal training, to enable the shift from awareness to interest, from interest to desire, and from desire to action.
This is why implementing an injury prevention campaign will have little or no effect on actual outcomes in terms of less injuries, unless the campaign increases awareness of risk factors, stimulating behavioural changes, by stepwise building desire and interest about understanding risk factors, end eventually leading an action towards risk factors. Examples of case study are the following:
The Case of Finland
In Finland, the IKINÄ report for fall prevention for older people, funded and executed by The National Institute for Health and Welfare (THL), was produced as a guideline that was the foundation for a broader scope of national injury prevention initiative, implemented by a prevention network including the Finnish Red Cross and several national authorities. Such network takes advantage of national studies, for example the prospective 20-year follow-up showing effects of recreational gymnastics in prevention of injurious falls in older women,44 and the self-rated fall risk screening tool (KaatumisSeula)45 for the older people. These tools are exploited by multiple stakeholder organisations, such as non-profit, hospitals, and City of Kuopio Elderly Care, a 4-star Reference Site.
The Case of Ireland
The National Strategy for Prevention of Falls and Fractures in Ireland’s Ageing Population started with the AFFINITY National Falls and bone health project 2018–2023.46 This was also as related with the Health Service Executive of Ireland’s Health Service Change Guide47 on information and knowledge on change involving service users. AFFINITY is a whole system, population health improvement project, implementing a National Strategy on the prevention of harmful falls and fractures in older persons (~5M, 13.3% 65 years +). It aims to lead and enable service improvements, scaling up and spread of existing and new quality services for falls and bone health, enhanced by ICT, with multi-stakeholder, multi-professional and multi-sectoral collaborative work. Implementation approaches include: optimizing stakeholder involvement, empowering citizen self-management, supporting older persons to actively age well.
The Case of Sweden
Region Västerbotten includes four regions, Jämtland Härjedalen, Västernorrland, Västerbotten and Norrbotten, with Region Västerbotten committed to Action Group A2, and Region Norrbotten a 4-star Reference Site. Their injury database tracks perilous products in a home and leisure setting, now the most common type of injury, in Sweden, 91% of all trauma deaths 2015–2017 (Table 2).
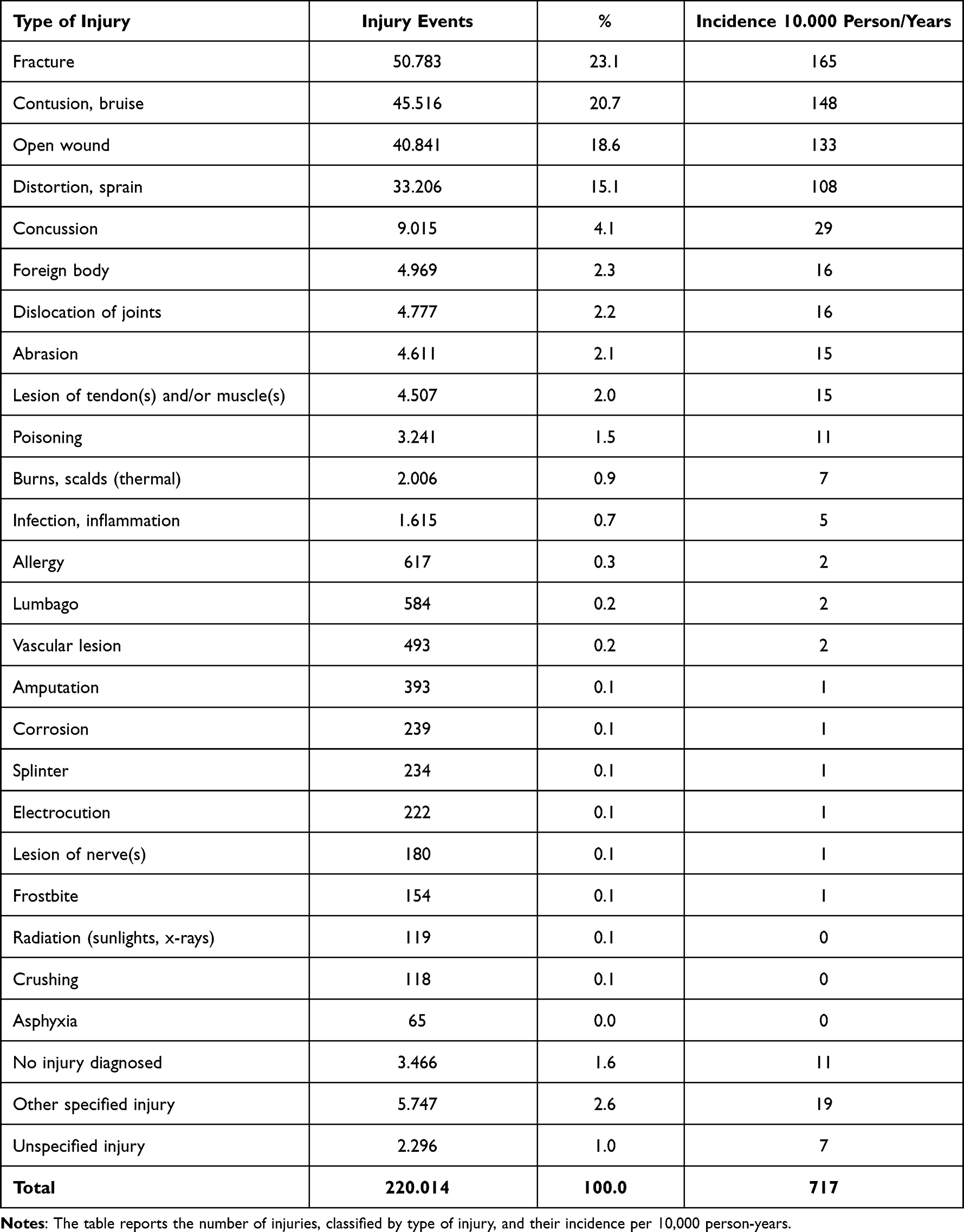 |
Table 2 Sweden’s Injury Data 2015–2017 |
Most events in IDB are from geriatric falls and fall injuries, where the injury mechanism can be suitably analysed with the help of modern IT and AI, given that the many complex and conflicting facilitating and triggering events include the whole spectrum of sociological, pharmacological, medical and political factors. IDB has been extensively used to improve eg road traffic safety,48 and efforts in Region Västerbotten are now directed to provide similar safety in form of effective falls prevention.
Personalized Persuasive Strategies to Change the End-Users’ Behaviours
Profiling Motivation Application (PMA) results from a collaborative work between C2 AG on Independent living solutions and D4 on Age-friendly buildings, cities and environments, with a prototype app used since 2018 by different structures of the Reference site Senior Riga, in Latvia.
The problem of acceptance and usage of different technological solutions (ICT or mechanical ones) by older persons is rather well-known.
Older adults’ reluctance in adopting new solutions to be integrated in their daily routines represent the challenge faced by caregivers to install innovative equipment in their home. Professionals (eg psychologist or gerontologue) can establish the required efficient communications with the older adults to overcome hesitancy, but often lack of training to use technologies hinders further adoption.
Hence the need to build a relationship with the user and develop a user-friendly, persuasive script as one of the most important elements for the installation of ICT solutions and for the implementation of any “ageing in place” platforms.
The domain of “persuasive systems”, technologies and strategies aimed at changing the end-users’ behaviors or attitudes, like healthy nutrition or increasing physical exercise, is not new and it is widely used by designer, for instance, of web-applications.49 But the original idea of Lex van Velsen (one of the D4 group members) was not to develop a new persuasive scheme, but rather:
- To create a profiling framework, matching any older person to one of the predefined profiles and
- To develop a set of personalized strategies of persuasion for each of these profiles.
Such predefined profiles allow grouping of those older adults that share the same motivation to work on their health. The most widely known types of motivation are intrinsic (the activity is fun or worthwhile) and extrinsic (money or compliments from others). Personalized persuasive strategies were based on a large-scale study where older adults (whose motivation profile was first established) indicated which persuasive strategies they most appreciated out of a wide range reported in the scientific literature.
Based on Senior Group50 experience, that working on implementation of “Mama-OK” age-in-place solution, the best way is to realise the solution in form of easily understandable, downloadable, and installable Application for mobile devices.
The “Senior Riga” RS (the Latvian-based filial of “Senior Group”) group included professional care managers and application developers who developed, based on the aforementioned theoretical background, the first test version of the “Profiling Motivation Application”, currently used within the Senior Riga reference on their mobile device.51
B3 Action Group’s Contribution to Scaling Up Integrated Care
Since 2014, the B3 Action Group performed a study to develop a maturity model relating to the adoption of ICT in support of integrated care. The Maturity Model provided a way for regions to assess their progress along 12 dimensions of activity, in order to identify their strengths, gaps and areas for improvement in integrated care.
The Model formed the basis for further development as part of two European Commission co-funded projects: SCIROCCO (Scaling Integrated Care in Context) and SCIROCCO Exchange (Capacity building support for integrated care) which is scheduled to conclude in February 2022.
In the SCIROCCO project, the Maturity Model was validated and developed into an online self-assessment tool for integrated care.52 The SCIROCCO Exchange project has focused on maximising the value and impact of the Maturity Model and online self-assessment Tool by developing an online Knowledge Management Hub.
Smart Healthy Age-Friendly Environments
In 2017, the EC launched a call for strategic initiatives in health and care. The Smart Healthy Age-Friendly Environments (SHAFE) proposal had been the most voted. The SHAFE proposal aims to facilitate the creation of healthy and friendly environments for all ages through a holistic multisectoral approach that promotes the use of new technologies.53
The COST Action International Interdisciplinary Network on Smart Healthy Age-friendly Environments (NET4Age-Friendly) is built upon the SHAFE concept and works as an international network that engage all levels of society with the intrinsic aim of promoting the development of local, regional or national inclusive ecosystems (composed of a quadruple helix of citizens, public authorities, companies, and researchers) which interact and coordinate at the international level. This brings an inspiring and fruitful new way of cooperation that fosters knowledge and promotes grassroot implementation at a broader scale, combining top-down and bottom-up perspectives.
The network currently gathers around 320 stakeholders from 46 countries and it includes several members from the EIP on AHA former AGs and RS, providing a continuum to the collaboration established from the core of the D4 AG on Age-friendly environments.
Conclusions
The growing complexity of current societal including demographic challenges reflects how health is cross-cutting across geography, organisational boundaries and cultural limits. Hence, collaborative efforts are pivotal to share experiences and resources to effectively and productively address such challenges. The challenges being faced across Europe in delivering safe, effective and sustainable healthcare services before the COVID pandemic are still with us. The exponential rise in the proportion of GDP being consumed through the delivery of modern healthcare, the demand and capacity challenges in parts of our systems and the ageing population and rise in long term conditions are all as real today as they were before. When you add to that the need to manage COVID, the increase in waiting times, the unmet demand from patients that have delayed presenting for care and the fact that service delivery is much less efficient due to the necessary additional infection control measures, there is a pressing need for us to transform how we are delivering healthcare. Innovation is going to be key the key enabler for Europe’s healthcare services to successfully remobilise and recover. To be successful and to de-risk this journey, the ecosystem created under the umbrella of the EIP on AHA could be a key enabler. The ongoing COVID-19 pandemic continues to teach us “the hard way” that we need to strengthen our efforts to increase capacity and to speed up the digital transformation of service provision towards a “one health” ecosystem in Europe. In fact, healthcare systems across Europe and elsewhere increasingly recognise the need to introduce new and innovative approaches, solutions, and technologies that will improve health and social care outcomes, clinical decision making, and organizational efficiency for citizens.
Health and social care transformation cannot progress unilaterally across different health and care providers within a region, nor can it be driven by researchers and industry shifting the paradigm of change to have it “supply” driven. The experiences represented in this article demonstrate that adopting a broad ecosystem taking a strategic approach facilitates the design of clinically effective health and social care pathways built around the individual patient or service user. Such pathways need to be evidence-based and clearly address the delivery of improved outcomes for patients and service users, whilst at the same time contributing to the sustainability of these systems. It is within these pathways that innovative solutions and digital technologies can become the enablers of change.
It is well recognised that one of the fundamental barriers to the adoption of innovative service change is cultural resistance. If a local or regional health system does not feel it has ownership of an innovation, it is highly likely it will be resisted and widespread adoption will prove elusive. Through the evolution of the Action Groups, involving all the key participants in the policy and delivery of healthcare services, the exchange of knowledge, experience and expertise took place in a supportive environment. Through the close engagement with Reference Sites, this allowed these hard won achievements to be taken back into local and regional systems and become embedded in local approaches to innovation and service transformation, accelerating there development, reducing risk and increasing the likelihood of successful adoption.
The EIP on AHA during its eight years demonstrated that developing effective and sustainable synergies with Action Groups offers greater support for Reference Sites in transferring innovations, because regional health and care priorities and challenges can be identified and advanced through AG commitments. The front-end identification of regional commitments based on real health and social care challenges and priorities can ensure at the back end of the process that recommendations from the AGs are finally implemented. As can be seen in this paper, the legacy of the EIP on AHA continues. While fragmented at times, largely due to the heterogeneity of the interventions and approaches to tackling similar issues, this report highlights that it is this very complexity that requires solutions such as the EIP on AHA. Similar collaborative, interdisciplinary and transnational initiatives should therefore be encourage to promote better integration in the EU and other European countries to deliver the ambitious targets of policy makers and to fulfil commitments made to all and especially older people.
In addressing regional challenges and priorities, it is important that the AGs that were created out of the EIP on AHA, which have now become self-sustaining groupings under the RSCN, develop synergies amongst themselves to ensure a holistic view is taken in the development of future recommendations and solutions. The collaboration between AGs and RSs has allowed cutting-edge technologies to be tested and monitored in real settings, and the results of the pilots provide real impact in the innovation and sustainability of health and care services. There remains a need to ensure that the EIP on AHA model is maintained and further developed and iteratively implemented after the EC mandate period ended in December 2020. The EIP on AHA RSCN has responded to this need by establishing a range of Thematic AGs that will bring together experts across Europe to address the key health and care challenges that have been highlighted by the EIP on AHA at regional, national and European level, and facilitate the transposition of change so that it delivers for those in need.
Through participation in new EC initiatives on digital health and health systems transformation, the RSCN will enable the community of experts (former AG members) and AHA regional innovation ecosystems (RSs), including the results of 8 years of activity, to be leveraged as a foundation for further development and implementation.
Research Ethics and Consent
This review does not use or reveal any personal or patient data.
Acknowledgments
The authors would like to thank Carina Dantas (Shine2Europe), Donna Henderson (Scottish Government), George Crooks (Digital Health and Care Innovation Centre, University of Strathclyde) and Rònàn O’Caoimh (Centre for Gerontology & Rehabilitation, University College Cork) for the valuable content they provided to the article and the role they played in the EIP on AHA. This article is based upon work from COST Action 19136 International Interdisciplinary Network on Smart Healthy Age-friendly Environments, supported by COST (European Cooperation in Science and Technology).
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bousquet J, Michel J, Standberg T, et al. The European innovation partnership on active and healthy ageing: the European Geriatric Medicine introduces the EIP on AHA column. Eur Geriatr Med. 2014;5(6):361–362. doi:10.1016/j.eurger.2014.09.010
2. Bousquet J, Illario M, Farrell J, et al. The reference site collaborative network of the European innovation partnership on active and healthy ageing. Transl Med UniSa. 2019;19:66–81.
3. Patella V, Florio G, Magliacane D, et al. Public prevention plans to manage climate change and respiratory allergic diseases. Innovative models used in Campania Region (Italy): the twinning aria implementation and the allergy safe tree decalogue. Transl Med UniSa. 2019;19:95–102.
4. Bousquet J, Bedbrook A, Czarlewski W, et al. Guidance to 2018 good practice: ARIA digitally-enabled, integrated, person-centred care for rhinitis and asthma. Clin Transl Allergy. 2019;9:16. doi:10.1186/s13601-019-0252-0
5. WE4AHA Project Consortium. 2018. Blueprint on digital transformation of health and care for the aging society. Available from: https://ec.europa.eu/digital-single-market/en/blueprint-digital-transformation-health-and-care-ageing-society.
6. European Commission. European scaling-up strategy in active and healthy ageing; 2015. Available from: https://ec.europa.eu/eip/ageing/library/European-scaling-strategy-active-and-healthy-ageing_en.html.
7. WE4AHA Project Consortium. Innovation to market plan; 2019. Available from: https://ec.europa.eu/eip/ageing/library/innovation-market-plan_en.
8. European Commission. Communication on enabling the digital transformation of health and care in the Digital Single Market; empowering citizens and building a healthier society; 2018. Available from: https://digital-strategy.ec.europa.eu/en/library/communication-enabling-digital-transformation-health-and-care-digital-single-market-empowering.
9. Boehler CE, de Graaf G, Steuten L, et al. Development of a web-based tool for the assessment of health and economic outcomes of the European Innovation Partnership on Active and Healthy Ageing (EIP on AHA). BMC Med Inform Decis Mak. 2015;15(Suppl 3):S4. doi:10.1186/1472-6947-15-S3-S4
10. Courbis AL, Murray RB, Arnavielhe S, et al. Electronic Clinical Decision Support System for allergic rhinitis management: MASK e-CDSS. Clin Exp Allergy. 2018;48(12):1640–1653. doi:10.1111/cea.13230
11. Bousquet J, Agache I, Aliberti MR, et al. Transfer of innovation on allergic rhinitis and asthma multimorbidity in the elderly (MACVIA-ARIA) - EIP on AHA Twinning Reference Site (GARD research demonstration project). Allergy. 2018;73(1):77–92. doi:10.1111/all.13218
12. Bousquet J, Hellings PW, Agache I, et al. ARIA 2016: care pathways implementing emerging technologies for predictive medicine in rhinitis and asthma across the life cycle. Clin Transl Allergy. 2016;6:47. doi:10.1186/s13601-016-0137-4
13. Bousquet J, Arnavielhe S, Bedbrook A, et al. MASK 2017: ARIA digitally-enabled, integrated, person-centred care for rhinitis and asthma multimorbidity using real-world-evidence. Clin Transl Allergy. 2018;8:45. doi:10.1186/s13601-018-0227-6
14. Bousquet J, Arnavielhe S, Bedbrook A, et al. The Allergic Rhinitis and its Impact on Asthma (ARIA) score of allergic rhinitis using mobile technology correlates with quality of life: the MASK study. Allergy. 2018;73(2):505–510. doi:10.1111/all.13307
15. Fonseca JA, Nogueira-Silva L, Morais-Almeida M, et al. Validation of a questionnaire (CARAT10) to assess rhinitis and asthma in patients with asthma. Allergy. 2010;65(8):1042–1048. doi:10.1111/j.1398-9995.2009.02310.x
16. Bousquet J, Anto JM, Annesi-Maesano I, et al. POLLAR: impact of air pollution on asthma and rhinitis; a European Institute of Innovation and Technology Health (EIT Health) project. Clin Transl Allergy. 2018;8:36. doi:10.1186/s13601-018-0221-z
17. O’Caoimh R, Molloy DW, Fitzgerald C, et al. ICT-supported interventions targeting pre-frailty: healthcare recommendations from the personalised ICT supported service for independent living and active ageing (PERSSILAA) study. Maciaszek L, O Donoghue J, Molloy W, Rocker C, Ziefle M, editors. Information and Communication Technologies for Ageing Well and e-Health: 3rd International Conference, ICT4AWE 2017, Revised Selected Papers. Springer; 2018:69–92. Communications in Computer and Information Science.
18. O’Caoimh R, Molly D, Fitzgerald C, et al. Healthcare recommendations from the personalised ICT supported service for independent living and active ageing (PERSSILAA) study. In
19. Jansen-Kosterink S, Van Velsen L, Frazer S, Dekker-van Weering M, O’Caoimh R, Vollenbroek-Hutten M. Identification of community-dwelling older adults at risk of frailty using the PERSSILAA screening pathway: a methodological guide and results of a large-scale deployment in the Netherlands. BMC Public Health. 2019;19(1):1–9. doi:10.1186/s12889-019-6876-0
20. Illario M, De Luca V, Tramontano G, et al. The Italian reference sites of the European innovation partnership on active and healthy ageing: progetto mattone internazionale as an enabling factor. Annali dell’Istituto Superiore di Sanità. 2017;53:60–69. doi:10.4415/ANN_17_01_12
21. Liotta G, Ussai S, Illario M, et al. Frailty as the future core business of public health: report of the activities of the A3 action group of the European Innovation Partnership on active and healthy ageing (EIP on AHA). Int J Environ Res Public Health. 2018;15(12):2843. doi:10.3390/ijerph15122843
22. Iavarone A, Carpinelli Mazzi M, Russo G, et al. The Italian version of the quick mild cognitive impairment (Qmci-I) screen: normative study on 307 healthy subjects. Aging Clin Exp Res. 2019;31(3):353–360. doi:10.1007/s40520-018-0981-2
23. Carpinelli Mazzi M, Iavarone A, Russo G, et al. Mini-mental state examination: new normative values on subjects in Southern Italy. Aging Clin Exp Res. 2020;32(4):699–702. doi:10.1007/s40520-019-01250-2
24. Dos santos PM, O’Caoimh R, Svendrovski A, et al. The RAPid COmmunity COGnitive screening Programme (RAPCOG): developing the Portuguese version of the quick mild cognitive impairment (Qmci-P) screen as part of the EIP on AHA twinning scheme. Transl Med. 2019;19:82.
25. O’Caoimh R, Sweeney C, Hynes H, et al. COLLaboration on AGEing-COLLAGE: Ireland’s three star reference site for the European Innovation Partnership on Active and Healthy Ageing (EIP on AHA). Eur Geriatr Med. 2015;5(6):505–511. doi:10.1016/j.eurger.2015.04.009
26. Brouns B, van Bodegom-vos L, de Kloet AJ, et al. Effect of a comprehensive eRehabilitation intervention alongside conventional stroke rehabilitation on disability and health-related quality of life: a pre-post comparison. J Rehabil Med. 2021;53(3):jrm00161. doi:10.2340/16501977-2785
27. Illario M, Maione A, Rusciano M, et al. NutriLive: an integrated nutritional approach as a sustainable tool to prevent malnutrition in older people and promote active and healthy ageing—the EIP-AHA nutrition action group. Adv Public Health. 2016;2016:1–9. doi:10.1155/2016/5678782
28. Maggio M, Barbolini M, Longobucco Y, et al. A novel tool for the early identification of frailty in elderly people: the application in primary care settings. J Frailty Aging. 2020;9(2):101–106. doi:10.14283/jfa.2019.41
29. Tziraki-Segal C, De Luca V, Santana S, et al. Creating a culture of health in planning and implementing innovative strategies addressing non-communicable chronic diseases. Front Sociol. 2019;4:9. doi:10.3389/fsoc.2019.00009
30. En Buena Edad Platform. Available from: www.enbuenaedad.es/en.
31. Birov S, Lavin C, Stroetmann V. Scaling-up of ICT solutions in active and healthy ageing through twinning actions. In:
32. Pinzón S, Padial M, Navarro B, et al. Identifying needs and expectations of potential users of the virtual platform to foster healthy and active ageing in Andalusia. Nurs Fam Health Care. 2018;1:1–3. doi:10.15761/NFHC.1000102
33. Pinzón-Pulido S, Padial-Espinosa M, López-Samaniego L, et al. Creation process of the digital platform to foster healthy and active aging: enbuenaedad. Front Public Health. 2019;7:22. doi:10.3389/fpubh.2019.00022
34. Borrmann M, Lindner S, Hofer-Fischanger K, et al. Strategy for deployment of integrated healthy aging regions based upon an evidence-based regional ecosystem-the styria model. Front Med. 2020;7:510475. doi:10.3389/fmed.2020.510475
35. Berger S, Eglseer D, Eisenberger A, Wirnsberger GH, Roller-Wirnsberger RE. Development of a nutritional documentation tool: a Delphi study. Br J Nutr. 2019;121(6):662–669. doi:10.1017/S0007114518003781
36. Alpe Adria Gesundheits-konferenz. [Alpe Adria Health Conference]. Available from: https://www.healthconference.eu/.
37. Malva JO, Amado A, Rodrigues A, et al. The quadruple helix-based innovation model of reference sites for active and healthy ageing in Europe: the ageing@Coimbra case study. Front Med. 2018;5:132. doi:10.3389/fmed.2018.00132
38. Mair A, Fernandez-Llimos F. Polypharmacy management programmes: the SIMPATHY project. Eur J Hosp Pharm. 2017;24:5–6. doi:10.1136/ejhpharm-2016-001044
39. Wynne R. FitWork good practice guide 2018. ENWP; 2018. Available from: https://ec.europa.eu/programmes/erasmus-plus/project-result-content/8aba5051-b3e0-4e01-861a-a9fd9765f569/D4.2%20Good%20practices%20to%20develop%20physical%20activity%20programs%20at%20work_Revised%20(3).pdf.
40. Cano A, Kurpas D, Bujnowska-Fedak M, et al. FOCUS: frailty management optimisation through EIPAHA commitments and utilisation of stakeholders’ input – an innovative European project in elderly care. Fam Med Prim Care Rev. 2016;18(3):373–376. doi:10.5114/fmpcr/63234
41. Apóstolo J, Couto F, Bobrowicz-Campos E, et al. An interregional, transdisciplinary and good practice-based approach for frailty: the mind&gait project. Transl Med UniSa. 2019;19:11–16.
42. Apóstolo J, Bobrowicz-Campos E, Moreno-Casbas T, et al. A study protocol for development and validation of a clinical prediction model for frailty (ModulEn): a new European Commitment to Tackling Frailty. Transl Med UniSa. 2019;19:36–41.
43. Martins G, Santos L, Dias J. Towards a context-aware adaptable services framework with applications in elderly care.
44. Uusi-Rasi K, Karinkanta S, Kannus P, et al. Does long-term recreational gymnastics prevent injurious falls in older women? BMC Geriatr. 2020;20:37. doi:10.1186/s12877-020-1428-0
45. KaatumisSeula, Self-rated fall risk screening tool. Available from: https://www.ukkinstituutti.fi/kaatumisseula.
46. AFFINITY national falls and bone health project 2018–2023. Available from: https://www.hse.ie/eng/services/list/4/olderpeople/falls-prevention-and-bone-health/.
47. HSE’s health service change guide. Available from: https://www.hse.ie/eng/staff/resources/changeguide/resources/change-guide.pdf.
48. European Commission. European Injury Data Base (IDB) purpose and methods. Available from: https://ec.europa.eu/health/indicators_data/idb/purpose_methods_en.
49. Oinas-Kukkonen H, Harjumaa M. Persuasive systems design: key issues, process model, and system features. Commun Assoc Inf Syst. 2009;24:28.
50. Senior Group. MAMA-OK Functionning model. Available from: http://senior-group.fr/.
51. Profiling Motivation Application (PMA). Available from: https://ec.europa.eu/eip/ageing/library/eip-aha-profiling-motivation-application-prototype-creating_en.
52. Grooten L, Fabbricotti IN, Devroey D, Vrijhoef HJM. Assessment of the implementation fidelity of a strategy to scale up integrated care in five European regions: a multimethod study. BMJ Open. 2020;10(3):e035002. doi:10.1136/bmjopen-2019-035002
53. Dantas C, van Staalduinen W, Jegundo A, et al. Smart healthy age-friendly environments - policy recommendations of the thematic network SHAFE. Transl Med UniSa. 2019;19:103–108.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.