Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Intention and Practice on Personal Preventive Measures Against the COVID-19 Pandemic Among Adults with Chronic Conditions in Southern Ethiopia: A Survey Using the Theory of Planned Behavior
Authors Andarge E ![]() , Fikadu T
, Fikadu T ![]() , Temesgen R
, Temesgen R ![]() , Shegaze M
, Shegaze M ![]() , Feleke T, Haile F
, Feleke T, Haile F ![]() , Endashaw G, Boti N
, Endashaw G, Boti N ![]() , Bekele A
, Bekele A ![]() , Glagn M
, Glagn M ![]()
Received 30 September 2020
Accepted for publication 11 November 2020
Published 3 December 2020 Volume 2020:13 Pages 1863—1877
DOI https://doi.org/10.2147/JMDH.S284707
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Eshetu Andarge,1 Teshale Fikadu,1 Rodas Temesgen,2 Mulugeta Shegaze,1 Tesfaye Feleke,1 Firehiwot Haile,1 Gisila Endashaw,3 Negussie Boti,1 Alemayehu Bekele,4 Mustefa Glagn1
1School of Public Health, Arba Minch University, Arba Minch, Southern Nations Nationalities and Peoples Regional State, Ethiopia; 2Department of Internal Medicine, School of Medicine, Arba Minch University, Arba Minch, Southern Nations Nationalities and Peoples Regional State, Ethiopia; 3School of Nursing, Arba Minch University, Arba Minch, Southern Nations Nationalities and Peoples Regional State, Ethiopia; 4Center for Neglected Tropical Diseases, Arba Minch University, Arba Minch, Southern Nations Nationalities and Peoples Regional State, Ethiopia
Correspondence: Eshetu Andarge
School of Public Health, Arba Minch University, P.O. Box: 021, Arba Minch, Southern Nations Nationalities and Peoples Regional State, Ethiopia
Tel +251-9-45-89-59-37
Email [email protected]
Purpose: With prevention being the only and best available intervention, COVID-19 has recently become a global threat, having had and continuing to have enormous health, economic, and societal impacts. Evidence so far has documented a heightened risk of mortality to people with chronic conditions. There is a dearth of evidence regarding chronic disease patients’ intention and practice on the preventive measures. This study tried to fill this gap by assessing the intention to practice and practice on personal preventive measures (PPMs) among adults with chronic conditions.
Materials and Methods: A facility-based cross-sectional study was conducted in Southern Ethiopia among 806 adults with chronic conditions by employing a multistage sampling technique. Data were collected using a pre-tested and structured questionnaire. Statistical analysis was done using IBM SPSS software version 25. Binary logistic regression analysis was done to identify factors associated with intention and practice. Level of statistical significance was declared at a P-value of less than 0.05.
Results: The study showed that 52% (95% CI=47.61– 54.80) and 76.3% (95% CI=73.36– 79.24) of adults with chronic conditions were intending to practice and had ever practiced the personal preventive measures. Participants’ subjective norm (SN) (AOR=4.94; 95% CI=3.49– 6.96) and perceived behavioral control (PBC) (AOR=4.13; 95% CI=2.69– 6.34) were the factors associated with their intention. Good knowledge and a positive attitude were found to be significant factors associated with the participants’ actual practice of the PPMs among other independent factors.
Conclusion: Around half of the participants were intending to practice PPMs, and three-quarters had good practice on the PPMs against COVID-19. Interventions targeted to improve intention and practice on the PPMs need to take into account improving knowledge and attitude, and build positive subjective norms and heighten the confidence to control the preventive behaviors.
Keywords: intention, practice, theory of planned behavior, chronic conditions, South Ethiopia
Introduction
The WHO declared the outbreak of the novel coronavirus (2019-nCoV)-infected pneumonia as a Public Health Emergency of International Concern on January 30, 2020. Later, on February 11, 2020, the WHO announced a name for the new coronavirus disease: COVID-19, and on March 11, 2020 the outbreak was declared a global pandemic.1,2 It is an enveloped single-stranded RNA virus which has symptoms ranging from mild (similar to the common cold) to more severe respiratory, enteric hepatic, and neurological symptoms.3,4 As to current evidence, the primary transmission route for COVID-19 virus is through respiratory droplets and contact routes.5 COVID-19 can cause symptoms including fever, difficulty in breathing, cough (mostly dry), and invasive lesions on both lungs of the patients.6 There is a progressive increase in the number of cases of COVID-19 across the world, resulting in negatives outcomes to impacts from the macro-economic level to individual social protection, particularly in the context of low-income countries. A decline in GDP, a rise in inflation, and compromisation of quality healthcare services are a few to mention.7–10
The etiology of COVID-19 disease is that SARS-CoV-2 virus accesses host cells via the protein angiotensin-converting enzyme 2 (ACE2), which is particularly abundant in the lungs, explaining the predominant respiratory symptoms like cough, fever, and shortness of breath. The other major clinical events frequently observed in COVID-19 patients are related to its targeting of the endothelium, one of the largest organs in the human body. The attack by SARS-COV 2 subsequently leads to endothelial dysfunction which results in a loss in the endothelium’s capacity for vasodilation, fibrinolysis, anti-aggregation, and anti-thrombotic effects. The existing evidence generally suggests that patients with more comorbidities and chronic diseases could experience a worse prognosis as compared to healthy subjects. For instance, among COVID-19 patients with pre-existing diabetes, pneumonia evolves to a clinical stage more refractory to the usual therapies and was observed to demand ICU care.11
At present, ACE2 is at the center of a heated debate among the scientific community, and there are concerns that medical management of hypertension including the use of inhibitors of the renin-angiotensin-aldosterone system (RAAS) may contribute to the adverse health outcomes observed. Angiotensin converting enzyme inhibitors (ACEi) and/or angiotensin receptor blockers (ARBs) which are widely used for treatment of hypertension, interfere with ACE2 expression/activity. Thus, hypertensive patients undergoing ACEi and/or ARBs drug therapy may be at a higher risk of contracting a serious COVID-19 infection. But, according to Sardu et al,12,13 anti-hypertensive drugs like ACEI and ARB did not affect the prognosis in COVID-19 patients; patients with higher LVEF values had lowest risk of deaths. On the other hand, ACEi/ARBs have cardio-protective functions, and could improve LVEF by reduction of inflammation therefore not to stop taking ACEi/ARBs to control hypertension and to prevent more serious and dangerous complications in hypertensive patients with COVID-19 was suggested.
People with underlying health conditions and older adults are at greatest risk for severe infection and death due to COVID-19.14 This adds to the worst situation that non-communicable diseases (NCDs) are the leading causes of mortality, equivalent to 71% of all deaths globally. Each year, 15 million people die from a NCD between the ages of 30 and 69 years; over 85% of these “premature” deaths occur in low- and middle-income countries.15 Even though strong evidence is yet to come, the highest toll of mortality and complications from COVID-19 is among people with pre-existing chronic conditions including cardio-vascular illness, diabetes, hypertension, liver and kidney problem, chronic respiratory diseases, and cancer and the elderly (≥65) adding to the invariably higher global mortality of 71% from non-communicable diseases.14,16 Patients with type 2 diabetes mellitus (T2DM) frequently report respiratory symptoms and are at increased risk of several pulmonary diseases. Few available studies showed that a possible association existed between T2DM and COVID-19 infection. Patients with T2DM exhibited high prevalence, severity of disease, and mortality with Covid-19 infection when compared to non-diabetics. In addition, T2DM patients have higher rates of need for Intensive Care Unit and hospitalization. Indeed, over-glycemia is a negative factor to influence clinical outcomes and to reduce the effects of anti-viral drugs and drugs leading to the best prognosis among diabetic patients.17–19
Given all these impacts to the macro and micro-economy, the healthcare system, and individual vulnerabilities, to date, there is no specific medicine recommended to prevent or treat the new coronavirus (2019-nCoV). Preventive measures ranging from individuals to large scale societal level practices are the only available means to control the spread of the virus and minimize its impacts.10,20
Behavioral scientists suggest the importance of behavioral interventions in averting the impacts of pandemics. They claim that the unfolding COVID-19 pandemic can only be brought under control by massive and rapid behavior change as human behavior will determine how quickly COVID-19 spreads and the mortality in the time of the current absence of medical treatment and vaccination.21,22 An approach to behavioral studies using a theory is a possible solution for exploring determinants of different public health protective and professional behaviors.23–27 One of such theories commonly and successfully used in social behavioral studies and public health is the theory of planned behavior (TPB).28,29 Applying the TPB to identify which theoretical constructs predict intention to practice in the time of public health emergency, as has been done in studies among communities in China,30,31 is advisable since intention seems to be a valid proxy measure for behavior.32 Intentions are self-instructions to perform particular behaviors or to obtain certain outcomes.33 Strong prior evidences showed a good degree of consistence between intention and action (behavior), as intentions explain 28% of the variance of behavior even though the inconsistency between the two is not negligible.32,34
Even though the course of COVID-19 cases seems slower in the African region, the continent was told to prepare for the worst in the time to come indicating the urgency of the preventive measures.35,36 Ethiopia is the third highest hit country in Africa by the COVID-19 infection recently. The high risk to people with co-morbidity of chronic conditions like diabetes, hypertension, chronic cardiac, respiratory, liver and kidney diseases, and cancer, as well as the elderly, suggests for a special focus to these groups and, therefore, there is a need to investigate how they are intending to practice the recommended PPMs, the magnitude of practice on the personal preventive measures, and factors affecting these issues. Besides, the preventive measures are not common practices which need behavioral change in the routine disease prevention which makes investigation to their intention since intention leads to action.
Thus, what proportion of adults with chronic conditions are intending or practicing the PPMs and factors associated with their intention or practice needs to be investigated. Therefore, this study is aimed to assess intention to practice and practical behavior of these preventive measures among people with chronic conditions in Gamo and Konso zones, Southern Ethiopia. The study would assist in providing explicit information on the attitude, subjective norm, and perceived control for PPMs, intentions, and actual practices among the target groups, and could suggest solutions to improve the preventive behaviors among the high risk groups for mortality and complications from COVID-19.
Patients and Methods
Study Setting
The study was conducted in two zones (Gamo and Konso) in the Southern Nations, Nationalities and Peoples regional state. The two zones were selected because of the high legal and illegal people movement through trade and tourism in the areas, so the inhabitants might have a higher chance of exposure to COVID 19. Gamo zone was administratively divided into 14 districts and four town administrations, with a total population of 1,544,753 (780,101 females and 764,652 males) projected for the year 2019/20 from the 2007 national census. Arba Minch is the main town of Gamo zone, which is located 454 km South of Addis Ababa, the capital city of Ethiopia. With the main town, Karat, located 521 km south of Addis Ababa, Konso zone is the second zone of the study. The zone was administratively divided into four districts and two town administrations with a total population of 306,000 (154,530 female and 151,470 male) projected for the same year. The study was conducted in public hospitals of Gamo and Konso zones. There are five hospitals currently serving the Gamo zone population: four of them are district hospitals (Chencha, Geresse, Kemba, and Selamber hospitals) and one is a general hospital (Arba Minch General hospital). In Konso zone, there are two district hospitals (Karat and Segen hospital). Currently a zonal level task-force established in collaboration with Arba Minch University and Arba Minch college of health sciences are providing awareness creation, surveillance, and screening services in the prevention and control of the COVID-19 pandemic (Gamo and Konso zone health department, Arba Minch and Karat, Ethiopia).
Study Design
A hospital-based cross-sectional study was conducted among adults with chronic conditions from June 18 to August 30, 2020. The theory of planned behavior is used to examine the intentions and practical behaviors of the study participants.
Population of the Study
The source populations of this study were adults with chronic conditions (hypertension, diabetes mellitus, chronic kidney, heart and liver diseases, HIV/AIDS, Asthma, TB, and cancer) who were on follow-up in public hospitals of Gamo and Konso zones. The study populations were adults with chronic conditions who were on follow-up in the four randomly selected hospitals of Gamo and Konso zones. All adults (18 and above) with chronic conditions were eligible for inclusion in the study, except for those who were unable to communicate and/or admitted patients.
Sample Size Determination and Sampling Procedure
The sample size was determined using Open-Epi software by following single population proportion assumptions of 95% confidence level, expected prevalence of intention to practice PPMs of 50% (absence of estimates from a related study), and 5% degree of precision. The sample size calculated using these assumptions was 384. With additional consideration of a design effect of two (for use of multi-stage cluster sampling) and a 10% potential non-response rate, the final sample size was estimated to be 845.
The samples of the study were obtained using multi-stage sampling. Initially, three hospitals from the five hospitals in Gamo zone and one hospital from the two hospitals in Konso were selected using a lottery method. The list of patients with chronic conditions was obtained from each hospital’s registry. The sample size was allocated in proportion to the number of patients in each hospital. Second, the required numbers of individuals allocated to each hospital were selected using a systematic random sampling after calculating the sampling interval (K) by dividing the total number of adults with chronic conditions in each hospital by the required sample from each hospital. The first participant was selected randomly from the k participants appointed on the date of data collection based on the medical registration number. Then, every kth participant was included for each hospital till the required samples were obtained. The patients randomly selected were interviewed on the date of their follow-up.
Data Collection Methods, Instrument, and Procedures
A total of 15 trained data collectors having a bachelor degree in public health and nursing, and five healthcare professionals having a master’s degree in the health discipline collected the data and supervised the data collection, respectively. A pre-tested, structured, interviewer-administered questionnaire which addresses socio-demographic factors, knowledge, and attitude on the PPMs and the constructs of theory of planned behavior was used to collect the data. The questionnaire was adapted from the WHO Survey tool and Guidance on COVID-19 and a related literature.30,37 Data were collected digitally using an Open Data Kit (ODK) mobile phone-based application in a face-to-face interview. The ODK is a user-friendly open source android mobile application which works well without a network connectivity. It replaces the paper form questionnaire used in survey data gathering. A template of questions was prepared in a computer database and transferred to the cell phones of data collectors, especially trained on how to use it for data collection. An exit interview was made with the clients on the date of their follow-up after they have received the necessary care for their follow-up. In order to protect the data collection team and the patients from getting COVID-19 infection, the data collection was strictly adhered to the recommendation on physical distancing, respiratory etiquette, and other PPMs.38
Variables of the Study
The study has two related dependent variables: One aspect of it assesses the intention to comply with the PPMs and the other aspect looks into the practice of the PPMs. Various socio-demographic variables (age, sex, marital status, educational status, economic status, having children at minor age, having disability for self and any family member), perception towards community emergency services and resources, perceived agreement with local leaders and trust in their work, comprehensive knowledge about COVID-19, attitude towards the PPMs, subjective norm, and perceived behavioral control were considered as explanatory variables of the study.
Definitions and Measurements
Definitions
A restriction or inability to perform an activity in the manner or within the range considered normal for a human being, mostly resulting from impairment.39
Personal preventive measures (PPMs) against COVID-19: methods of personal prevention like hand-washing with soap and water/alcohol rub for 20 seconds, avoiding touching one’s eyes, nose, and mouth with unwashed hands, staying home when one is sick or when had a cold, covering ones mouth and nose when he/she coughs or sneezes, keeping physical distancing, use of face mask when going out and self-isolation.
Illnesses which expose individuals to a heightened risk of mortality from COVID-19, which include cardiovascular diseases, diabetes, chronic respiratory disease, hypertension, cancer, chronic liver disease, and chronic kidney disease.14
It is not seeing family and friends during the pandemic.30
Measurements
The intention to practice PPMs was measured using seven questions which assessed whether the participants intended to practice the six PPMs mentioned above after being recommended to by a health department or by any mass media. The questions are given responses on a 5-point Likert scale, and mean scores were computed for each participant. Those who score the mean and above were considered as having a good intention to practice the PPMs; otherwise they were considered as not having a good intention to practice the PPMs. Practice of PPMs was measured using the seven questions on the PPMs which ask whether the participants practice the PPMs or not.37 Eleven items were used to measure the three constructs of the TPB based on a 4–5-point Likert scale. Attitude towards PPMS was measured by six items. Subjective norm (SN) was measured by two items, and perceived behavioral control (PBC) on PPMs was measured by three items.30 The attitude was dichotomized into favorable and unfavorable based on participants score of the mean and above or below the mean, respectively. Similarly, respondents who scored the mean and above of the subjective norm value were considered to have positive subjective norms, otherwise they were regarded as having negative subjective norm on PPMs. Respondents who scored the mean and above PBC value were considered to have higher PBC, otherwise they were regarded as having a lower PBC on PPMs. Knowledge about COVID-19 was assessed using a comprehensive questionnaire adapted from the WHO survey tool consisting of aspects of sign and symptoms, the PPMs and incubation period of COVID-19 using 17 questions on PPMs with (Yes/No/I do not know) options.37 The responses were scored as having awareness (1=yes) and having no awareness (2=No or 3=I do not know). The responses “No” and “I do not know” were recoded as (0=no awareness) and yes=1, with the maximum score of 14 and minimum score of 0. Based on Bloom’s cut-off point for knowledge, participants who scored less than 60% were regarded as having “poor knowledge”, 60–79% was regarded as “moderate knowledge”, and greater than or equal to 80% as having “good knowledge”. Similarly, practice on PPMs was also dichotomized into “good practice” when participants scored 80% and above, and “not good” practice when they scored less than 80%.
Data Processing and Analysis
Data was checked for completeness, edited, coded, and entered into Epi-data version 3.1 and exported to SPSS 25.0 statistical software for analysis. After cleaning data for inconsistencies and missing values, descriptive statistics such as mean, frequency, and percentages were computed. The participants’ socioeconomic status was set from permanent household assets by using a questionnaire adapted from the EDHS household wealth index questionnaire. Exploratory factor analysis using the principal components analysis (PCA) method and reliability analysis was conducted to determine dimension and internal consistency, respectively, among the multiple items used to make a composite score for intention, practice, attitude, knowledge, subjective norm (SN), and perceived behavioral control (PBC). Accordingly, use of a face mask and self-isolation when going out were removed for having unsatisfactory communality of less than 0.5 (0.35 for face mask use and 0.23 for self-isolation) from items assessing intention and practice of the PPMs, respectively. The PCA produced a single component which explained 84.64% and 61.74% total variance by the six remaining variables for intention and for practice, respectively. Reliability analysis showed an acceptable consistency among the remaining six variables (Cronbach’s Alpha=0.96 for intention and 0.87 for practice). In a similar fashion items were also reduced from the knowledge questions (signs and symptoms like sore throat, runny nose, headache, and the incubation period for COVID-19) for low communalities. The remaining 13 items, with acceptable internal consistency (Cronbach’s Alpha=0.91), were used to score the knowledge of the participants. The PCA produced a single component explaining 81.97%, 79.16%, and 75.63% for attitude, SN, and PBC items, respectively, with no item reduced in the analysis. Reliability analysis also gave an acceptable internal consistency in all cases (Cronbach’s Alpha=0.96, 0.74, and 0.84 for attitude, SN, and PBC items, respectively). The wealth index of the participants was also ranked into quintiles after reduction of items using PCA and based on factor score of the first component, which explained the maximum variance.
Bivariate analysis was done and all explanatory variables which have an association with the outcome variable at a P-value less than 0.25 were included in the multivariable analysis model. Then multivariable analyses was done using a backward stepwise selection method (backward LR) to determine independent factors of intention and practice on PPMs. Model fitness was checked using Hosmer and Lemeshow goodness of fitness test. Multicollinearity among explanatory variables was checked using variance inflation factor (VIF>10). OR with its 95% CI was used to show the degree of association between the explanatory variable and the outcome variable. Level of statistical significance was declared at a P-value of less than or equal to 0.05.
Data Quality Assurance
The questionnaire was translated to Amharic and back translation will be done by another person to check for the original meaning. Data collectors and supervisors were trained for 3 days about the objectives of the study, skipping pattern, interview, and context of the questionnaire with strict adherence to physical distancing. The questionnaire was pre-tested on 5% of the sample to modify any difficult items and to estimate the survey time. Data completeness and consistency was checked by supervisors during the data collection time.
Ethical Consideration
Ethical approval and clearance was obtained from the institutional ethical review board of Arba Minch University. The study was conducted in accordance with the Declaration of Helsinki. A letter of cooperation was written to the respective district and town administration health offices. Written informed consent was obtained from the study participants after informing them about the purpose of the study. Data privacy and confidentiality of information of individuals was assured. The right to participate or not in the study was granted to the participants. Ethical recommendations for COVID-19 research were strictly followed during the face-to-face survey. The data collectors and patients wore face masks while collecting data, and physical distancing was maintained during the interview.
Results
Socio-Demographic and Related Characteristics of the Study Participants
A total of 806 participants were included in the study, with a response rate of 95.4%. The mean age was 42.67 (±13.4). The majority of the respondents were under 60 years old (89.2%), living in urban areas (78.3%), married (76.7%), did not have any disability among themselves and any family member (89.8% and 87.5%), and had harmony with the local leaders (83.7%) (Table 1).
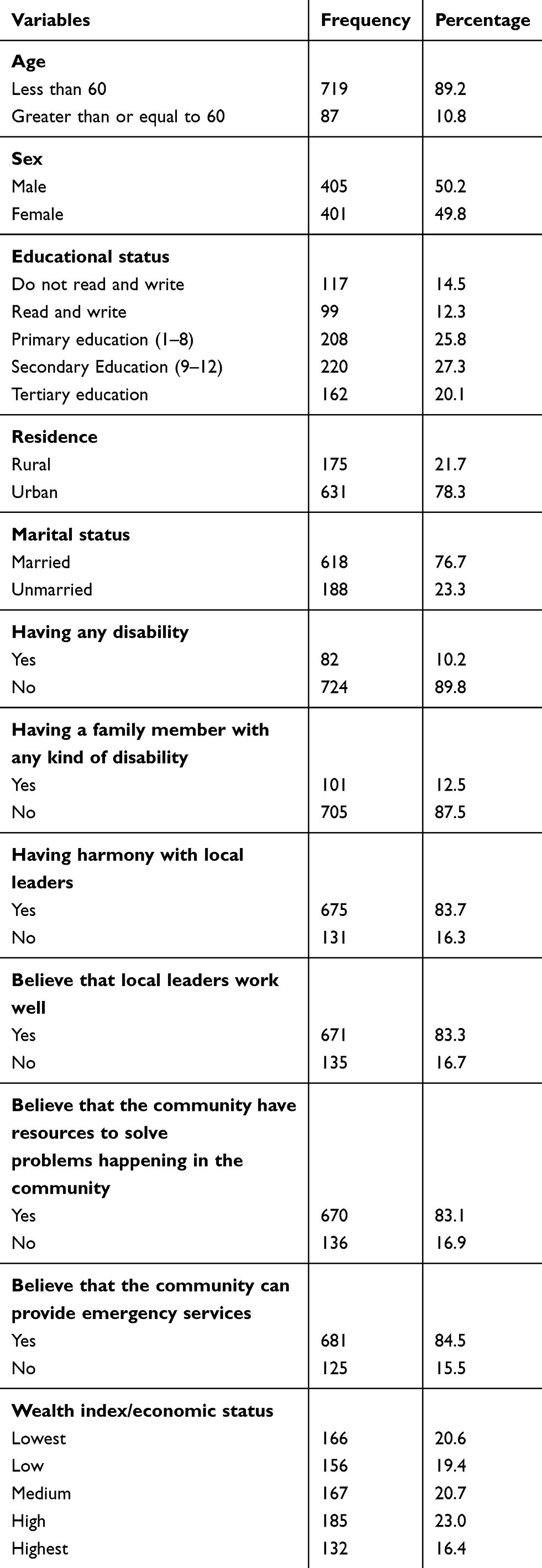 |
Table 1 Socio-Demographic and Related Characteristics of Adults with Chronic Conditions on Follow-Up in Public Hospitals of Gamo and Konso Zones, Southern Ethiopia, June 2020 |
Subjective Norm and Perceived Behavioral Control and Attitude Among the Study Participants
Three hundred and eighty (47%; 95% CI=43.4–50.7) of the participants had a positive subjective norm, while 589 (73.1%; 95% CI=69.9–76.2) perceived that they had higher control in their behavior. The proportion of participants having a favorable attitude towards personal protective measures for COVID 19 was 33.5% (95% CI=30.23, –36.76). About 30% of the participants strongly agreed that they believed in the prevention capability of the PPMs towards COVID-19 (Table 2).
 |
Table 2 Attitude Towards the PPMs of COVID-19 Among Adults with Chronic Conditions Follow-Up in Public Hospitals of Gamo and Konso Zones, Southern Ethiopia, June 2020 |
Knowledge of Respondents on COVID-19
The proportion of participants who had good knowledge towards personal preventive measures for COVID 19 was 44.7% (95% CI=41.23–348.10). Half of the study participant did not know that muscle or body aches could be a possible symptom of COVID 19. However, the majority of the participants (80.0%) and (72.8%) did not known that diarrhea and loss of taste and smell were likely symptoms of COVID 19 (Table 3).
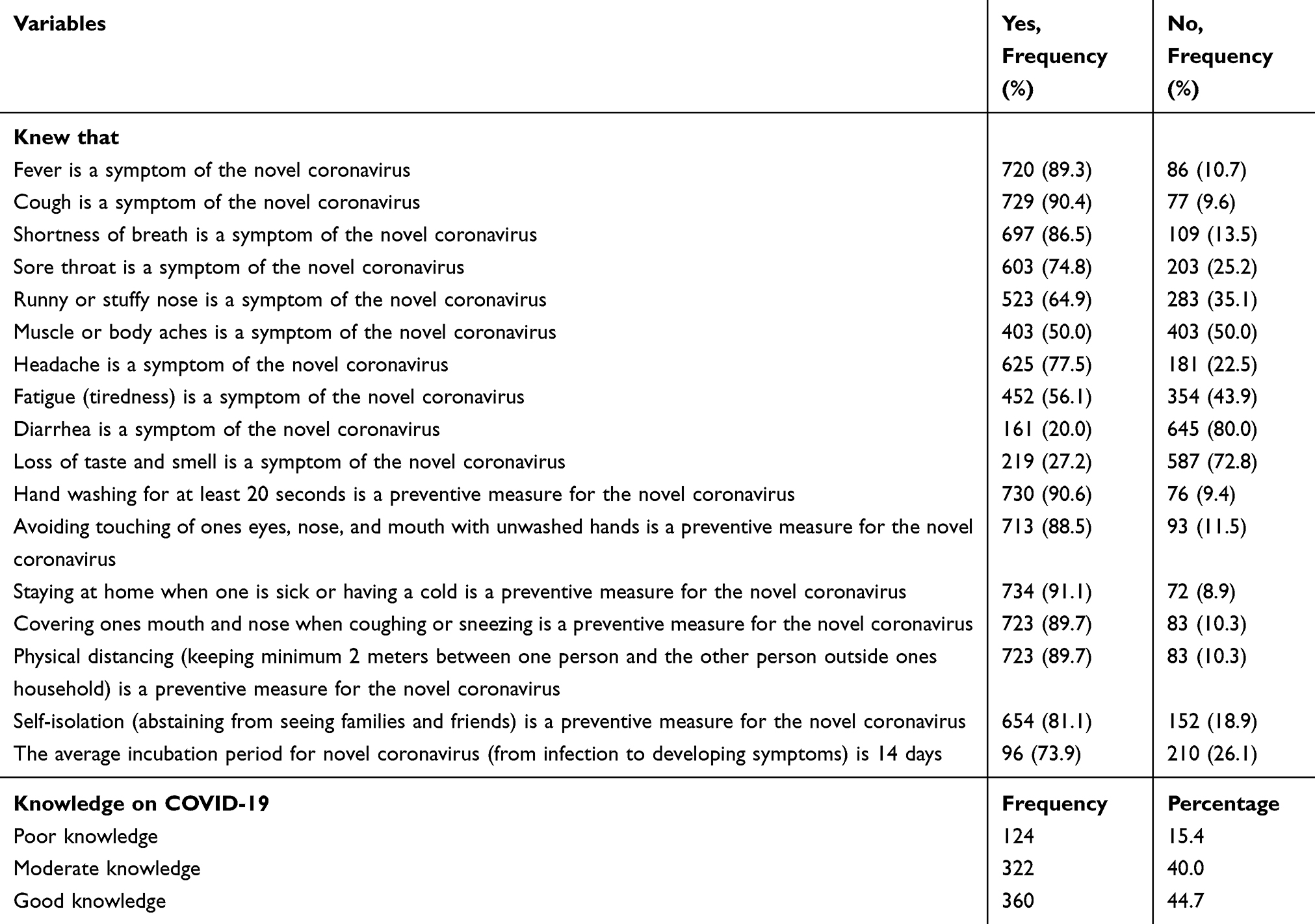 |
Table 3 Knowledge on COVID-19 Among Adults with Chronic Conditions on Follow-Up in Public Hospitals of Gamo and Konso Zones, Southern Ethiopia, June 2020 |
Intention and Practice on Personal Preventive Measures
The study showed that more than half of participants (52%; 95% CI=47.61–54.80) were intending to practice personal preventive measures. Likewise, along the range of 5 degrees of intention, around half (49–52.7%) absolutely intended to practice most of the PPMs, apart from the use of a face mask, which was the least (41.3%) absolutely intended PPM. A few of the participants (5.3%) were absolutely not intending to practice using a face mask when going outside of their household. The proportion of participants who practiced personal preventive measures towards COVID 19 was 76.3% (95% CI=73.36–79.24). The majority of the participants practiced hand washing and covering of the mouth and nose during coughing or sneezing (90.8% and 90.6%, respectively). However, only one third of the participants practiced self-isolation (Table 4).
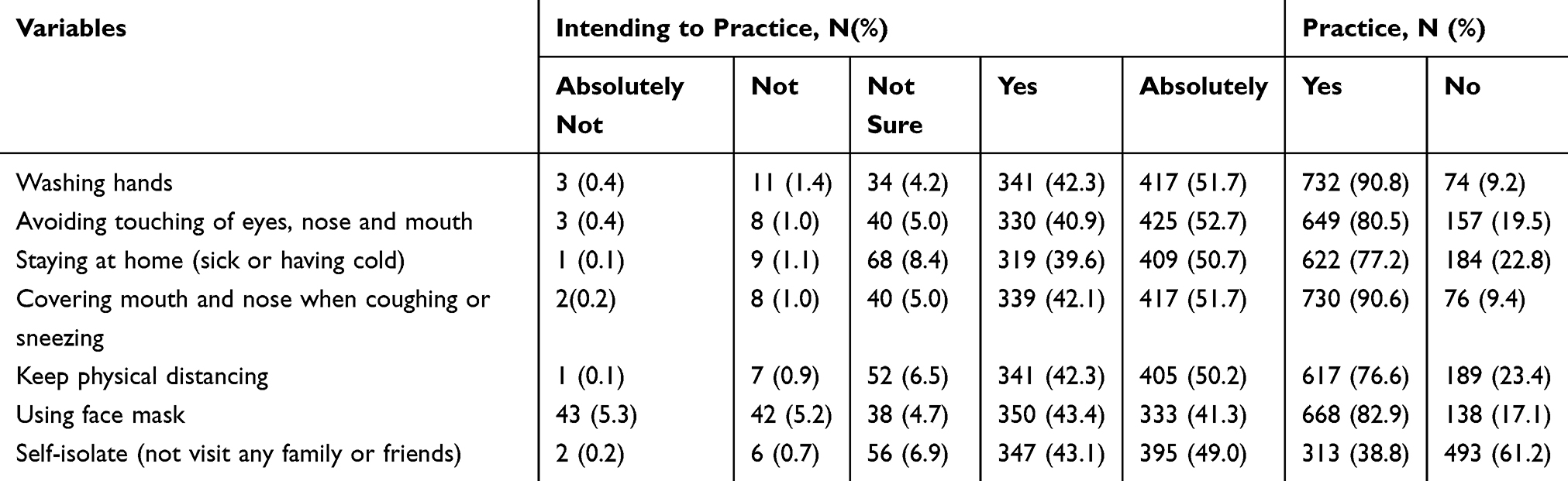 |
Table 4 Intention and Practice on PPMs Among Adults with Chronic Conditions Follow-Up in Public Hospitals of Gamo and Konso Zones, Southern Ethiopia |
Factors Associated with Intention to Practic Personal Preventive Measures
Among 13 variables selected as candidates for multivariable analysis, participant’s subjective norm and perceived behavioral control showed a significant association with their intention to practice PPMs.
The odds of intention for practicing personal preventive measures were 4.94-times higher among those having a positive subjective norm than those having a negative subjective norm. Similarly, the odds of intention were 4.13-times higher among those participants with a higher perceived behavioral control than those with a lower perceived behavioral control (Table 5).
 |
Table 5 Factors Associated with Intention in Practicing Personal Preventive Measures Among Adults with Chronic Medical Condition from Public Hospitals of Gamo and Konso Zones, Southern Ethiopia, June 2020 |
Factors Associated with Practice of Personal Preventive Measures Against COVID-19
The odds of practicing PPMs against COVID-19 was 2.4-times higher among those less than 60 years oldcompared with those greater than or equal to 60 years (AOR= 2.42; 95% CI=1.31–4.47). Likewise, the odds of practicing the PPMs was 2.10, 2.52, 4.56, and 8.44-times higher for those from households with low, medium, high, and highest wealth quintiles compared with those from the least wealth quintile (AOR=2.10; 95% CI=1.14–3.87), (AOR=2.52; 95% CI=1.18–5.39), (AOR=4.56; 95% CI=1.96–10.56), and [AOR=8.44; 95% CI=2.32–30.76), respectively.
Educational status has also shown an association with PPMs against COVID-19. The odds of practicing personal preventive measures towards COVID-19 was about 2-, 4-, and 7-times higher among participants who attended primary (1–8) (AOR=1.98; 95% CI=1.02–3.91), secondary (9–12) (AOR=3.89; 95% CI=1.77–8.55), and tertiary educations (AOR=6.97; 95% CI=2.16–22.48), compared with those who were not able to read and write, respectively.
Compared with rural residence, being in an urban area has increased the odds of practicing PPMs by 3.71 (AOR=3.21; 95% CI=1.90–5.41), while having a good knowledge increased it by 3.71 (AOR=3.71; 95% CI=1.97–7.00) among people with chronic medical conditions.
The study participants’ attitude and perception that their community would have a solution to its problems also showed a significant association with their practice of the PPMs. Those who had a favorable attitude towards PPMs and those who perceived that their community had a resource to solve its problem had 2.01 (AOR=2.01; 95% CI=1.17–3.48) and 2.65 (AOR=2.65; 95% CI=1.48–4.74) times higher odds of practicing the measures compared with their counterparts, respectively (Table 6).
 |
Table 6 Factors Associated with Practice Among Adults with Chronic Medical Conditions from Public Hospitals of Gamo and Konso Zones, Southern Ethiopia |
Discussion
People with chronic conditions are at particularly risk for mortality from COVID-19. Hence, there is a need for studies investigating their intention and practices on PPMs in order to get informative evidence that would protect them from acquiring COVID-19 infection. Therefore, this study was aimed to examine this among adults with chronic conditions, and factors associated with their intention and practical behavior. The study provided important information regarding intention and practice towards PPMs among people with one or more chronic conditions that were on follow-up at public hospitals from two zones in Southern Ethiopia.
In the study, slightly more than half of the participants intended to practice the PPMs. Absolute intent to practice the specific PPMs was also low, at around half of the participants. Scholarly or scientific literature dealing with the intention to comply with PPMs are scanty among the same population. A large survey among American general populations showed a higher national average intention to most certainly comply (over 80%) for four common recommendations (wash hands, social distancing, stay home, and cough etiquette).40 The discrepancy might be related to public awareness and fatality rate differences among populations in the two countries, which might have been the reason for the higher intention among the study participants in America. In this study, the least proportion of participants were absolutely intending to use a face mask while going out of the home, while the highest were absolutely not intending to practice it, on the contrary. Although a relatively higher proportion of the participants intend to stay at home, the lower intention to use a face mask is against the recommendation to vulnerable individuals to use a face mask rationally when exposed to high-risk areas since COVID-19 could be transmitted before symptom onset. If people who have been infected but who are contagious and asymptomatic wear face masks, community transmission might be reduced.41 As uptake and adherence to health behaviors are highly dependent on individuals’ intention and motivation,42 it is quite important to improve chronic disease patients’ intention and motivation to practice the PPMs which are the only available solutions to keep them from acquiring COVID-19 infection, morbidity and mortality. As a central factor of performing a behavior, a strong intention leads to a better realization of a given behavior.28,29
Regarding the factors significantly associated with the participant’s intention to comply with the PPMs, two of the latent components which determine an individual’s intention to practice (attitude, subjective norm and perceived behavioral control) showed a significant association in the present study. Those having a positive subjective norm and with a higher perceived behavioral control had higher odds of intention to practice the PPMs. This means that those who perceived a social pressure positively and had a positive normative belief had higher odds of intention to practice the PPMs. Similarly, those participants who perceived they had a higher behavioral control had higher odds of intention to practice the PPMs. This implies that the participants’ perceived social pressure and normative belief (SN) and their perceived ease or difficulty of performing the PPMs (PBC) affected their intention. This is consistent with studies in a pandemic setting and as it is constructed in the TPB.28–30,43 In the present study, attitude did not show an association with intention of the participants to practice the PPMS, but it has shown a significant association with their practice. The findings suggest that intention to practice can be improved through developing positive subjective norms and enhancing their perception towards behavioral control among chronic disease patients in the study area. An actual practice of the PPMs can be improved by enhancing measures which would bring about a favorable attitude among other factors which showed an independent association with practice of the PPMs.
Based on Bloom’s cut-off point of 80% as a good practice, about three-quarters of chronic disease patients in this study reported that they had ever practiced the PPMs consistently. With regard to the specific preventive measures, the majority of the participants practiced hand washing and covering mouth and nose during coughing or sneezing. Since no case of corona was reported in the area during the data collection, only one third of the participants practiced self-isolation in the present study. This is much higher than the findings from the Gondar study where only one quarter of the participants had good practice towards the preventive measures. The specific preventive measures practice (hand washing with soap and water, physical distancing, etc) was also higher in this study compared with the Gondar study.41 The discrepancy could be related to the reason that a higher proportion of the participants in this study were from an urban area and bigger towns compared with the participants in the Gondar study. Urban residence showed an independent positive association with good practice of the PPMs in this study. Urban dwellers do have the opportunity to get up to date information and develop positive attitude towards the prevention as they have better access to the mass media, digital media, and electric power supply.44,45
Likewise, in the study a higher level education also showed an independent significant association with practice of the PPMs in the study. This is also consistent with the study from Gondar.44,46 Education is one of the strongest factors ever reported to positively affect healthy behaviors in the scientific literature.53−55 This is for the fact that it enables one to get information, able to consume the obtained information, comprehend, analyze, and understand it and take action.
Household socio-economic condition (wealth status) of the participants was another independent factor which showed association with chronic disease patients practice on PPMs. Those from low, medium, high, and highest had a higher odds of practicing the PPMs compared with those from the lowest wealth quintile. This is plausible in the spirit that a better wealth status enables people to own a better position in the community, a better access to education and information as well as a better health seeking behavior.47 Even though improving socio-economic status of peoples is not an overnight intervention, the finding could suggest a focused approach to those patients with an economic disadvantage in the efforts of COVID-19 prevention and control among the stakeholders.
Unlike the “high risk” of mortality and morbidly from COVID-19 among the elderly, those younger than 60 years were having higher odds of practicing the PPMs compared with those 60 and above in the current study. This finding alerts for a special focus on the promotion of COVID-19 preventive measures among the elderly so that they can have a better awareness and positive attitude.
Having a good comprehensive knowledge and about COVID-19 was the other factor independently and positively associated with good practice on the PPMs. This is consistent with the study from Gondar and China.44,48 Patients with a good knowledge on the dangers, symptoms, and signs as well as the preventive measures of COVID-19 would develop a positive attitude and might have practiced the PPMs against COVID-19. The finding suggests that awareness creation and improvement of knowledge need to be strengthened among the patients by healthcare professionals who particularly care to these clients on a follow-up basis.
The last but not the least association was seen between the participants’ perception that their community would have a resource to solve to its problems and their practice of the PPMs. Those who had such a perception had higher odds of good practice on the PPMs as compared with their counterparts. Communities with adequate resources (man power, technology, and food) will be more resilient,30 and people in the community will be encouraged to practice the PPMs in the hope that the community will address the risk of COVID-19.
To the best of our knowledge, this is the first study dealing on intention to practice PPMs among people with chronic conditions in Ethiopia as well as Sub-Saharan Africa. Despite its strength in providing the above discussed information for practical considerations, it has few limitations to consider. Owing to resource constraints, the scope of the study was limited at two zones in Southern Ethiopia, hindering its generalizability to all chronic disease patients in the country. Ideally the study would have been more inclusive of patients with chronic disease, had it been conducted among patients with chronic disease in a community set-up. This was not possible for the absence of a reliable community level registry of people with chronic conditions in the set-up. Even though the questionnaire used in this study was from a suggested source for a survey on COVID-19, it is not rigorously validated for the specific population of the study, though reliability analysis was done and acceptable for composite variables in the study.
Conclusion
Based on mean score for intention and Bloom’s cut-off for practice measurements, around half of the participants were intending to practice PPMs and three-quarters had good practice on the PPMs against COVID-19. Participants’ PBC and SN were found to be significant factors associated with their intention to practice the PPMs, while age, socioeconomic condition, educational status, knowledge on COVID-19, and attitude towards COVID-19 PPMs showed an association with their practice on the PPMs. Interventions targeting to improve intention and practice on the personal preventive measures need to address their perception towards behavioral control and positively influence their subjective norms, knowledge, and attitude among others.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Surveillances V. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19)—China, 2020. China CDC Weekly. 2020;2(8):113–122. doi:10.46234/ccdcw2020.032
2. World Health Organization. 2019-nCoV outbreak is an emergency of international concern. 2020. Available from: http://www.euro.who.int/en/health-topics/emergencies/pages/news/new.
3. Zhu N, Zhang D, Wang W, China Novel Coronavirus Investigating and Research Team. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020.
4. WHO. Coronavirus. 2020. Available from: https://www.who.int/health-topics/coronavirus.
5. WHO. Scientific brief on modes of transmission of virus causing COVID-19: implications for IPC precaution recommendations. Available from: https://www.who.int/news-room/commentaries/detail/modes-of-transmission-of-virus-causing-covid-19-implications-for-ipc-precaution-recommendations.
6. Song F, Shi N, Shan F, et al. Emerging 2019 novel coronavirus (2019-nCoV) pneumonia. Radiology. 2020;295(1):210–217. doi:10.1148/radiol.2020200274
7. WHO. Coronavirus disease (COVID-19) pandemic. 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus.
8. World Bank. Draft analysis - COVID-19: potential poverty and social impacts in Ethiopia and policy responses. This note was prepared by the Ethiopia team of the Poverty and Equity Global Practice. 2019.
9. Chan JF, Yuan S, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet. 2020;395(10223):514–523. doi:10.1016/S0140-6736(20)30154-9
10. Wang Z, He T, Zhu L, Sheng H, Huang S, Hu J. Active quarantine measures are the primary means to reduce the fatality rate of COVID-19. Bull World Health Organ. 2020. doi:10.2471/BLT.20.255844
11. Sardu C, Gambardella J, Morelli MB, Wang X, Marfella R, Santulli G. Hypertension, thrombosis, kidney failure, and diabetes: is COVID-19 an endothelial disease? A comprehensive evaluation of clinical and basic evidence. J Clin Med. 2020;9(5):1417. doi:10.3390/jcm9051417
12. Sardu C, Maggi P, Messina V, et al. Could anti‐hypertensive drug therapy affect the clinical prognosis of hypertensive patients with COVID‐19 infection? Data from centers of southern Italy. J Am Heart Assoc. 2020;9(17):e016948. doi:10.1161/JAHA.120.016948
13. Sardu C, Marfella R, Maggi P, et al. Implications of AB0 blood group in hypertensive patients with covid-19. BMC Cardiovasc Disord. 2020;20(1):1.
14. Yang J, Zheng Y, Gou X, et al. Prevalence of comorbidities in the novel Wuhan coronavirus (COVID-19) infection: a systematic review and meta-analysis. Int J Infect Dis. 2020. doi:10.1016/j.ijid.2020.03.017
15. WHO. Non Communicable Diseases. Geneva, Switzerland; 2016. Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases.
16. Bigna JJ, Noubiap JJ. The rising burden of non-communicable diseases in sub-Saharan Africa. Lancet Glob Health. 2019;7(10):e1295–e1296. doi:10.1016/S2214-109X(19)30370-5
17. Sardu C, Gargiulo G, Esposito G, Paolisso G, Marfella R. Impact of diabetes mellitus on clinical outcomes in patients affected by Covid-19. Cardiovasc Diabetol. 2020;19(1):1–4. doi:10.1186/s12933-020-01047-y
18. Sardu C, D’Onofrio N, Balestrieri ML, et al. Outcomes in patients with hyperglycemia affected by Covid-19: can we do more on glycemic control? Diabetes Care. 2020. doi:10.2337/dc20-0723
19. Marfella R, Paolisso P, Sardu C, et al. Negative impact of hyperglycaemia on tocilizumab therapy in Covid-19 patients. Diabetes Metab. 2020;46(5):403–405. doi:10.1016/j.diabet.2020.05.005
20. WHO. Coronavirus (COVID-19) African region updates. Available from: https://www.afro.who.int/health-topics/coronavirus-covid-19.
21. Betsch C. How behavioural science data helps mitigate the COVID-19 crisis. Nat Hum Behav. 2020;4(5):438. doi:10.1038/s41562-020-0866-1
22. Michie S, Rubin GJ, Amlot R. Behavioural science must be at the heart of the public health response to covid-19. BMJ Opin. 2020.
23. Grimshaw JM, Eccles MP, Walker AE, Thomas RE. Changing physicians’ behavior: what works and thoughts on getting more things to work. J Contin Educ Health Prof. 2002;22(4):237–243.
24. Grol RP, Bosch MC, Hulscher ME, Eccles MP, Wensing M. Planning and studying improvement in patient care: the use of theoretical perspectives. Milbank Q. 2007;85(1):93–138.
25. Raissian KM, Su JH. The best of intentions: prenatal breastfeeding intentions and infant health. SSM Popul Health. 2018;5:86–100. doi:10.1016/j.ssmph.2018.05.002
26. Semungus A, Tafese Z, Semella T. Application of the theory of planned behavior to assess the determinants of HIV/AIDS risk among high school students in Hawassa City, Ethiopia. J Community Public Health Nurs. 2017;3(1):1–9. doi:10.4172/2471-9846.1000151
27. Kortteisto T, Kaila M, Komulainen J, Mäntyranta T, Rissanen P. Healthcare professionals’ intentions to use clinical guidelines: a survey using the theory of planned behaviour. Implement Sci. 2010;5(1):51. doi:10.1186/1748-5908-5-51
28. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50:179–211. doi:10.1016/0749-5978(91)90020-T
29. Conner M, Armitage CJ. Extending the theory of planned behavior: a review and avenues for further research. J Appl Soc Psychol. 1998;28:1429–1464. doi:10.1111/j.1559-1816.1998.tb01685.x
30. Zhang X, Wang F, Changwen Z, Wang Z. Willingness to self-isolate when facing a pandemic risk: model, empirical test, and policy recommendations. Int J Environ Res Public Health. 2020;17:197. doi:10.3390/ijerph17010197
31. Zhang Y, Yang H, Cheng P, Luqman A. Predicting consumers’ intention to consume poultry during an H7N9 emergency: an extension of the theory of planned behavior model. Hum Ecol Risk Assess. 2019.
32. Sheeran P. Intention - behavior relations: a conceptual and empirical review. Eur Rev Soc Psychol. 2002;1:1–36. doi:10.1080/14792772143000003
33. Triandis HC. Values, attitudes, and interpersonal behavior. In: Howe HE
34. Webb TL, Sheeran P. Does changing behavioral intentions engender behavior change? A meta-analysis of the experimental evidence. Psychol Bull. 2006;132(2):249–268. doi:10.1037/0033-2909.132.2.249
35. Aljeezeera news. Available from: https://www.aljazeera.com/news/2020/03/covid-19-africa-told-prepare-worst-response-200319085112877.html.
36. WHO region office for Africa. WHO concerned as COVID-19 cases accelerate in Africa. April, 2020. Available from: http://whotogowhoafroccmaster.newsweaver.com/JournalEnglishNewsletter/1x9518utfz7y48iiujdam4?lang=en&a=6&p=56762267&t=31103673.
37. WHO. Survey tool and guidance. Rapid, simple, flexible behavioural insights on COVID-19. Monitoring knowledge, risk perceptions, preventive behaviours and trust to inform pandemic outbreak response. 2020.
38. WHO. Research ethics practice during COVID-19.Specific considerations during health emergencies. 2020. Available from: https://www.idrc.ca/en/research-ethics-practices-during-covid-19.
39. Barbotte E, Guillemin F, NearkasenChau, and the Lorhandicap. Prevalence of impairments, disabilities, handicaps and quality of life in the general population: a review of recent literature. Bull World Health Organ. 2001;79:1047–1055.
40. Lennon RP, Sakya SM, Miller EL, et al. Public intent to comply with COVID-19 public health recommendations. HLRP. 2020;4(3):e161–e165.
41. Feng S, Shen C, Xia N, Song W, Fan M, Cowling BJ. Rational use of face masks in the COVID-19 pandemic. Lancet Respir Med. 2020;8(5):434–436. doi:10.1016/S2213-2600(20)30134
42. Chan DKC, Yang SX, Mullan B, et al. Preventing the spread of H1N1 influenza infection during a pandemic: autonomy-supportive advice versus controlling instruction. J Behav Med. 2015;38:416–426. doi:10.1007/s10865-014-9616-z
43. Zhang Y, Yang H, Cheng P, Luqman A. Predicting consumers’ intention to consume poultry during an H7N9 emergency: an extension of the theory of planned behavior model. Hum Ecol Risk Assess. 2020;26(1):1503931. doi:10.1080/10807039.2018.1503931
44. Akalu Y, Ayelign B, Derbew M. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13:1949–1960. doi:10.2147/IDR.S258736
45. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016.
46. Erfani A, Shahriarirad R, Ranjbar K. Knowledge, attitude and practice toward the novel coronavirus (COVID-19) outbreak: a population-based survey in Iran. Bull World Health Organ. 2020;3.
47. Latunji OO, Akinyemi OO. Factors influencing health-seeking behavior among civil Servants in Ibadan, Nigeria. Ann Ib Postgrad Med. 2018;16(1):52–60.
48. Zhong B, Luo W, Li H, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.