Back to Journals » Nursing: Research and Reviews » Volume 15
Intensive Care Unit Nursing Stress: Measuring Heart Rate Variability and Workplace Trauma
Authors Levi P ![]() , Li P
, Li P ![]() , Nicholson WC, Heaton K
, Nicholson WC, Heaton K ![]() , Fazeli PL
, Fazeli PL ![]() , Watts PI, Moss J
, Watts PI, Moss J
Received 14 September 2024
Accepted for publication 15 June 2025
Published 25 July 2025 Volume 2025:15 Pages 91—109
DOI https://doi.org/10.2147/NRR.S473151
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ferry Efendi
Paula Levi,1 Peng Li,2 W Chance Nicholson,3 Karen Heaton,2 Pariya L Fazeli,2 Penni I Watts,2 Jacqueline Moss2
1College of Nursing, University of South Alabama, Mobile, AL, USA; 2School of Nursing, University of Alabama at Birmingham, Birmingham, AL, USA; 3Nell Hodgson Woodruff School of Nursing, Emory University, Atlanta, GA, USA
Correspondence: Paula Levi, College of Nursing, The University of South Alabama, 5721 USA Drive North, Office 2039A, Mobile, AL, USA, 36688, Tel +1.251.445.9400, Fax +1.251.445.9416, Email [email protected]
Purpose: Intensive care unit (ICU) nurses work in a demanding environment and face repeated encounters with traumatic and ethical issues, which may negatively impact their psychological and physical health, patient care, and hospitals’ bottom line. The purpose of this study was to investigate stress among ICU nurses performing workplace activities/events by measuring fluctuations in heart rate variability (HRV), a reliable indicator of stress-related physiological changes.
Methods: Real-time HRV was measured using a wearable, wireless electrocardiogram for 30 ICU nurses while at work in this cross sectional, observational study. Workplace events were categorized (Routine Care, Stat (urgent) Care, and Interpersonal) and assigned numerical code labels. HRV time- and frequency-domain indices of SDNN, RMSSD, HF, and LF were calculated and accurately linked to participants’ corresponding physiological HRV responses to workplace events on an observational data collection tool, accessed on a portable electronic tablet. The association of HRV with ICU workplace events and psychological and clinical outcomes was explored.
Results: Nurses’ HRV parameters of SDNN, RMSSD, and HF tended to have the greatest reduction to both Stat (urgent) and Routine care events. New nurses tended to have lower HRV than experienced nurses. We found high rates of perceived stress and peritraumatic dissociative experiences and low resilience in the ICU nurses.
Conclusion: HRV can be used as a contemporary index of workplace stress and trauma in ICU nurses. Study nurses were vulnerable to potential long-term physiological and psychological health issues. Understanding stress and trauma ICU nurses face at work will allow for strategies for interventions to reduce the development of post-traumatic stress disorder, peritraumatic dissociation, and other psychological outcomes.
Keywords: post-traumatic stress, PTSD, peritraumatic dissociative experiences, workplace stress
Introduction
Intensive care unit (ICU) nurses are repeatedly exposed to stressful and traumatic situations in the workplace including cardiopulmonary resuscitation of patients, violent patients or family members, witnessing patients suffer, and performing futile care.1–5 Due to the repetitive exposure to psychological stress and trauma, ICU nurses are at high risk for developing post-traumatic stress disorder (PTSD).6–9 PTSD may occur after nurses witness or experience a traumatic event(s) at their job with symptoms lasting longer than one month and is characterized using four symptom clusters: (a) reexperiencing intrusive memories of the traumatic event(s); (b) avoidance of similar situations or reminders of the traumatic event(s); (c) negative alterations in cognition and mood; and (d) hyperarousal symptoms.10
When ICU nurses suffer from symptoms of PTSD, it can adversely impact the nurse, patient care, and hospitals.2,5,8 Physiological consequences for ICU nurses with PTSD can include increased risk for the development of cardiovascular disease, diabetes, hypertension, cognitive dysfunction, and sleep disturbance.11–15 There is also increased risk for substance and alcohol abuse, anxiety, and depression.7,16–19 Recent literature revealed ICU nurses who cared for COVID-19 patients experienced unprecedented psychological stress, high rates of PTSD, suicidal thoughts, and in dire cases, even suicide.7,20–23 Stress is one of the major reasons contributing to nurses leaving their jobs.24,25 Shortages of ICU nurses have been a critical global problem, now intensified since the COVID-19 pandemic.24,25 In the US alone, there is a 10% shortage of registered nurses, equivalent to approximately 350,000 unoccupied positions, which has a direct impact on quality care and patient outcomes.25,26
The measure of heart rate variability (HRV) can offer an objective measure of stress and PTSD and is superior to using purely subjective measures, which are prone to response bias.27,28 The aim of this study was to investigate a major gap in the literature regarding fluctuations in HRV among ICU nurses while performing workplace activities/events and whether their HRV was associated with PTSD. This paper is based on the thesis of Paula Miller Levi. It has been published on the institutional research repository website: https://digitalcommons.library.uab.edu.
Heart Rate Variability as a Measure of Stress and PTSD
HRV, the variation in time intervals between adjacent heartbeats, is influenced by fluctuations of the sympathetic nervous system and the parasympathetic nervous system and reflects an individual’s ability to adapt to stress.27–30 Higher HRV can indicate better self-regulation and adaptation to stress, while reduced (or low) HRV can indicate poor ability to respond to stress and suggest health problems (eg, cardiovascular disease, PTSD, chronic stress).28–30 In other words, the quicker HRV returns to normal after a stressor (higher HRV), the better the adaptation to stress. Individuals with PTSD can have alterations in autonomic nervous system (ANS) function reflecting poor adaptation to stress.30–32
Methods
Recruitment and Sample
This observational study utilized a convenience sample of ICU nurses working in a large academic health science center. As this was a pilot study, the sample size was determined by the feasibility and precision of the estimates, rather than statistical power.33 Four ICUs were included: the Medical ICU, Medical Critical Care Unit, Cardiothoracic ICU, and Trauma Burn ICU. Female ICU nurses, 35 years old or younger, were eligible to ensure differences detected in HRV measurement of participants were not due to known differences between men and women or large differences in age.34,35 HRV, in general, decreases with age, and can be affected by age-related factors (eg, comorbidities, menopause). Further inclusion criteria included: (a) working at their jobs at least 6 months, for at least 24 hours/week; and (b) working strictly day shift. Exclusion criteria included conditions that may affect HRV, such as: traumatic brain injury, psychological trauma experienced outside of the ICU workplace lasting longer than one month, treatment for any psychiatric conditions, significant cardiovascular or respiratory comorbidities, diabetes, medications/drugs known to affect HRV (eg, beta blockers, anti-cholinergic agents, sedatives, antidepressants, illicit substances), working night shift, pregnancy, menopause, and post-menopause. Thirty eligible ICU nurses were included in this study. We think it is important to acknowledge that during the screening process, 27% (n = 8) of potential and willing participants were excluded due to drug treatment with antidepressant or antianxiety medications. The ethnic composition of the study sample was similar to that of the nursing population in the state of Alabama.36 A summary of participant characteristics can be found in Table 1.
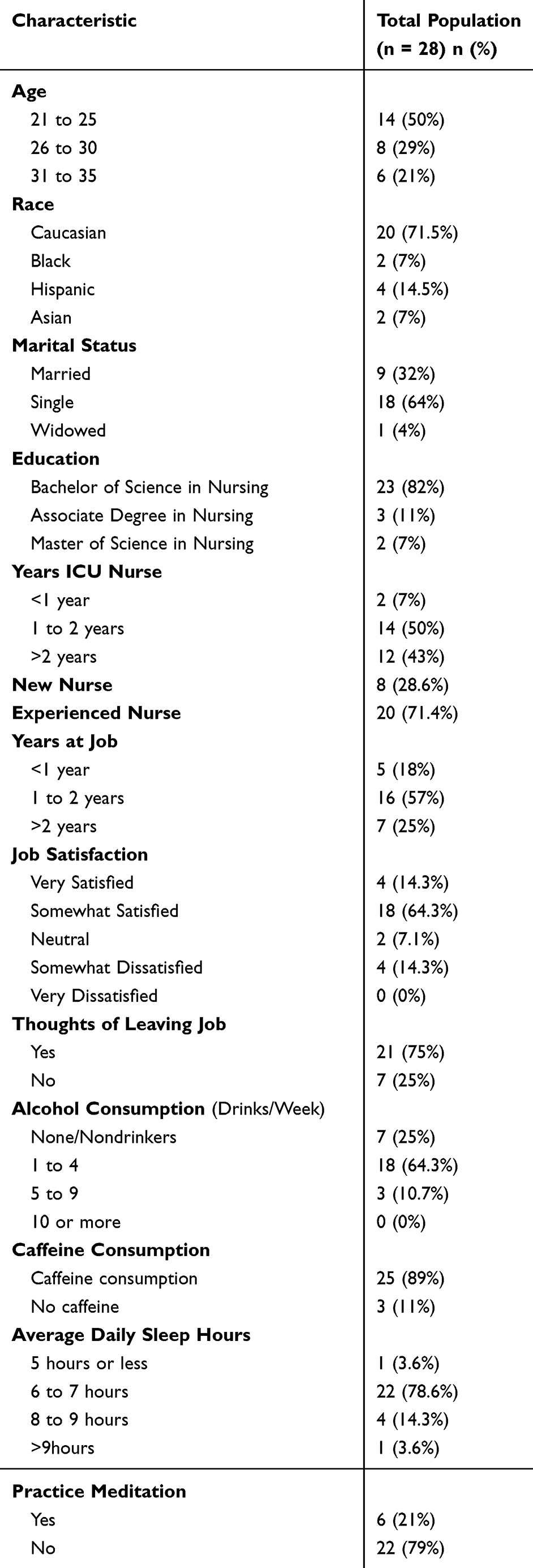 |
Table 1 Study Population Demographics and Lifestyle Characteristics |
Ethical Considerations
Ethical approval was obtained from the University of Alabama at Birmingham Institutional Review Board (IRB-300007663). All participants provided written informed consent. All procedures performed involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Measures and Instruments
The CamNtech Actiheart 5
The CamNtech Actiheart 5 (CamNtech Ltd., Cambridge, United Kingdom), a combined single-lead ECG and activity recorder, was used to collect HRV data. We analyzed the four most commonly used indices of HRV to examine PNS and SNS activation (see Table 2). Brage et al37 evaluated the accuracy between the Actiheart, ECG, and PolarTM measurements, as well as intra-instrument reliability and validity and concluded that the Actiheart was a reliable and valid tool for measuring HRV at rest, during walking, and running.
 |
Table 2 Heart Rate Variability Indices Collected and Description |
Observational Data Collection Tool
An observational data collection tool, accessed on a portable electronic tablet, was utilized to document workplace events the ICU nurses experienced in real-time. The tool, originally developed for observation in a cardiovascular ICU,38 was modified to capture ICU workplace events (eg, communicating with provider, administering pain medication; see Table 3). The events were placed into categories (Routine Care, Stat Care, and Interpersonal), assigned numerical code labels, and programmed into a computerized template on Microsoft Access software for rapid documentation on the tablet. Observational data collected included: category of event, event, time of event, and duration of event. An important feature included the capability of activating the Start Time button first, and then the type of event, for rapid and precise timing of events, and accurately linking workplace events to participants’ corresponding physiological HRV response. For complete details on the modification of the tool, please visit the institutional research repository website: https://digitalcommons.library.uab.edu/etd-collection/185/
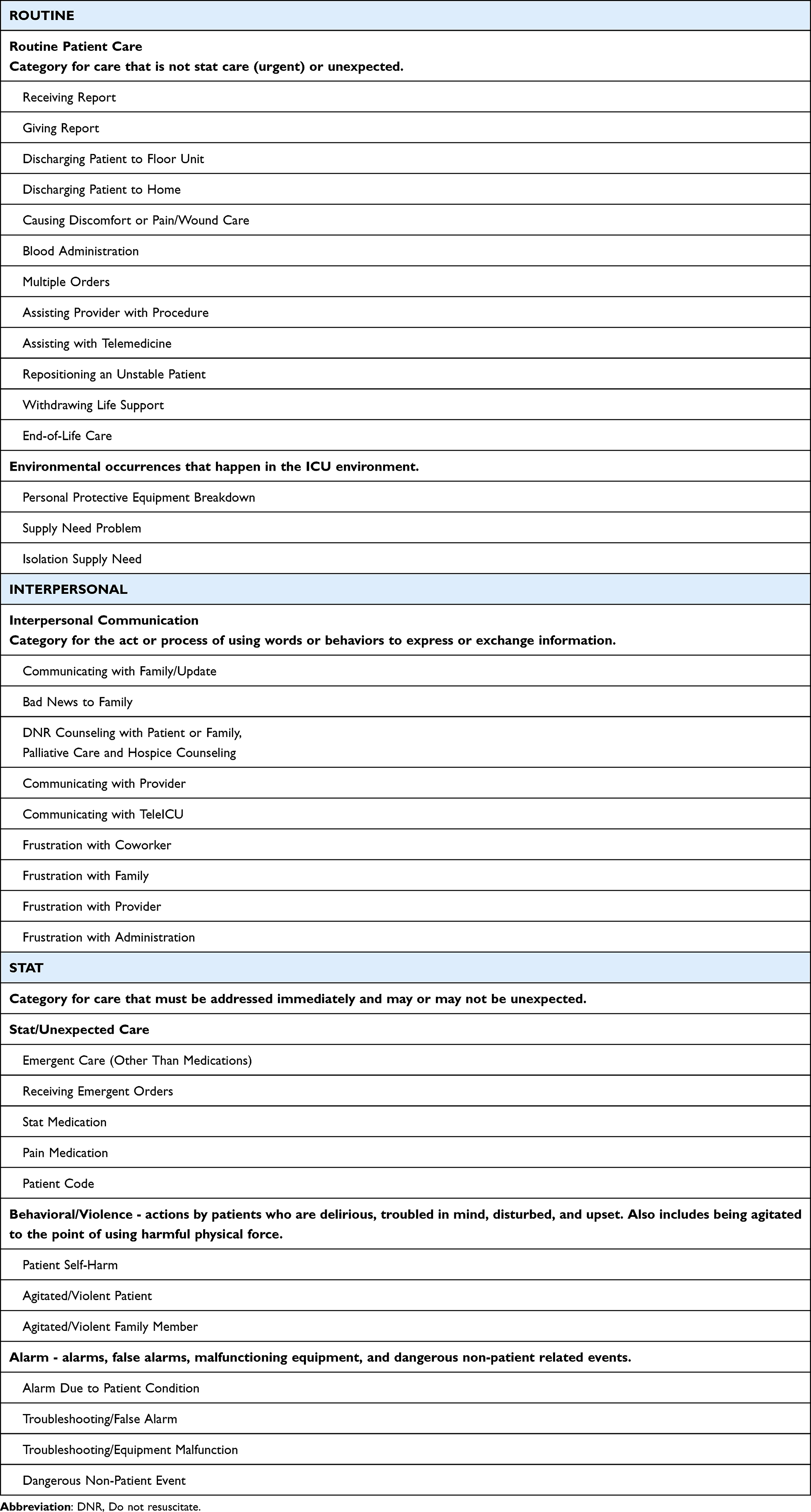 |
Table 3 Events and Their Categories |
The PTSD Checklist-5
The PTSD Checklist-5 (PCL-5) was used to assess PTSD symptoms. The PCL-5 contains 20 items in four subscales that correspond to the four symptom clusters of PTSD in DSM-5.39 Respondents rate how much they have been bothered by each item over the past month on a 5-point Likert scale ranging from 0 (not at all) to 4 (extremely). Total symptom severity scores can be obtained by summing the scores for each item (ranging from 0 to 80). A provisional diagnosis of PTSD can be made using a preliminary cutoff score of 31.40 Garcia et al41 demonstrated the PCL‐5 had strong internal consistency (α = 0.94) with a sample of 392 registered nurses. Cronbach’s alpha for the PCL-5 in this study ranged from 0.8 to 0.92.
Perceived Stress Scale 10-Item
The Perceived Stress Scale 10-item (PSS-10) measures stress perception, or the degree to which situations in an individual’s life are perceived as stressful.42 Participants rate each item using a 5‐point Likert scale. There are six negatively worded items which measure an individual’s feelings of a lack of control over their circumstances or their own emotions or reactions (Items 1, 2, 3, 6, 9, and 10); the four positively worded items (Items 4, 5, 7, and 8) measure an individual’s perceived inability to handle problems.43 Totals are achieved by reversing the scores on the four positive items and then summing all scale items. Scores range from 0 to 40. Internal consistency was found satisfactory (α = 0.82 and 0.72) in a population of 229 nurses working in hospitals.44 Cronbach’s alpha for the PSS-10 in this study was 0.83.
The Peritraumatic Dissociative Experiences Questionnaire
The Peritraumatic Dissociative Experiences Questionnaire (PDEQ) assesses retrospective reports of depersonalization, derealization, amnesia, out-of-body experience, and altered time perception at the time of the traumatic event.45 Peritraumatic dissociative experiences (PDEs) are believed to occur when an individual’s ability to cope with trauma is overwhelmed. Participants rate each item using a 5-point Likert-type scale. Higher scores indicate greater peritraumatic symptomatology. A cutoff score greater than 15 suggests significant peritraumatic dissociation. Van der Mei et al46 determined that the PDEQ demonstrated good test-retest reliability (r = 0.85, p <.01) and internal consistency (α = 0.81) in a sample of 647 trauma victims after emergency department admission. Cronbach’s alpha for the PDEQ in this study was 0.88.
Brief Trauma Questionnaire
The Brief Trauma Questionnaire (BTQ) was used to determine whether participants had experienced a traumatic event that met the DSM-5 Criterion A for PTSD. Questions asked about possible traumatic events (eg, serving in a war zone, having witnessed someone being seriously injured or killed). Respondents report whether traumatic events occurred, whether they felt their life was in danger, or if they were seriously injured from the event. Scores range from 0 to 10. The BTQ is considered a reliable and valid measure of trauma exposure.47 McCanlies et al48 determined the BTQ had excellent internal consistency (α = 0.89) with a sample of 328 police officers.
Connor-Davidson Resilience Scale-10 Item (CD-RISC-10)
The Connor-Davidson Resilience Scale-10 item (CD-RISC-10) short form was used to measure resilience over the past 30 days.49 The CD-RISC-10 consists of 10 items structured on a 5-point Likert-type scale. Scores range from 0 to 40, with higher scores indicating higher levels of resilience.49 Kim et al50 found the CD-RISC-10 demonstrated good internal consistency (α = 0.86) with a sample of 320 nurses. Cronbach’s alpha for the CD-RISC-10 in this study was 0.89.
Patient-Reported Outcomes Measurement Information System (PROMIS) on Sleep Disturbance 4-Item
Dimensions of the PROMIS Sleep Disturbance (SD) 4-item short form include perceived sleep quality, depth, and difficulties falling asleep over the past 7 days.51 Participants complete the scale using a 5-point Likert-type scale, with higher scores reflecting greater sleep disturbance. PROMIS measures generate T-scores that can be compared to the US general population. A T-score of 50 is the average, with a standard deviation of 10; higher T-scores represent greater sleep disturbance.52 Satisfactory internal consistency (α =0.85) was found by Green et al53 in a sample of 121 law enforcement officers. Cronbach’s alpha for the PROMIS-SD 4-item in this study was 0.89.
PROMIS Emotional Distress-Anxiety and -Depression 4-Item Short Forms
The PROMIS Emotional Distress-Anxiety (ED-A) and -Depression (ED-D) 4-item short forms were used to measure symptoms of anxiety and depression in the past 7 days. Participants completed the scales using a 5-point Likert-type scale of “never”, “rarely”, “sometimes”, “often”, and “always”. Higher T-scores indicated greater anxiety and depression severity. Cronbach’s alpha for PROMIS-ED-A was high (α = 0.97) in a sample of 402 frontline healthcare providers.54 Cronbach’s alpha for PROMIS-ED-D in a predominantly veteran sample (n = 651) ranged from 0.89 to 0.95.55 Cronbach’s alpha for the PROMIS-ED-A and -ED-D 4-item in this study was 0.85 and 0.92, respectively.
Procedures
To minimize participant burden at work, participants completed demographic information, a health information questionnaire, questions on job satisfaction, and the majority of surveys (PCL-5, BTQ, CD-RISC-10, and three PROMIS measures) on Qualtrics, an online survey platform, one to two days before on-unit participation (see Table 4). Participants were contacted before their day of on-unit participation and reminded to prepare for the study by abstaining from alcohol use and extreme physical exercise for a minimum of 24 hours, getting a good night’s sleep, limiting caffeine intake to 12 ounces (or 80 mg) that morning, and to arrive 40 minutes before the start of their 12-hour shift (6:30 am) for application of the heart rate variability monitor and baseline measurement. All participants reported that they complied with the pre-study instructions before baseline HRV was taken.
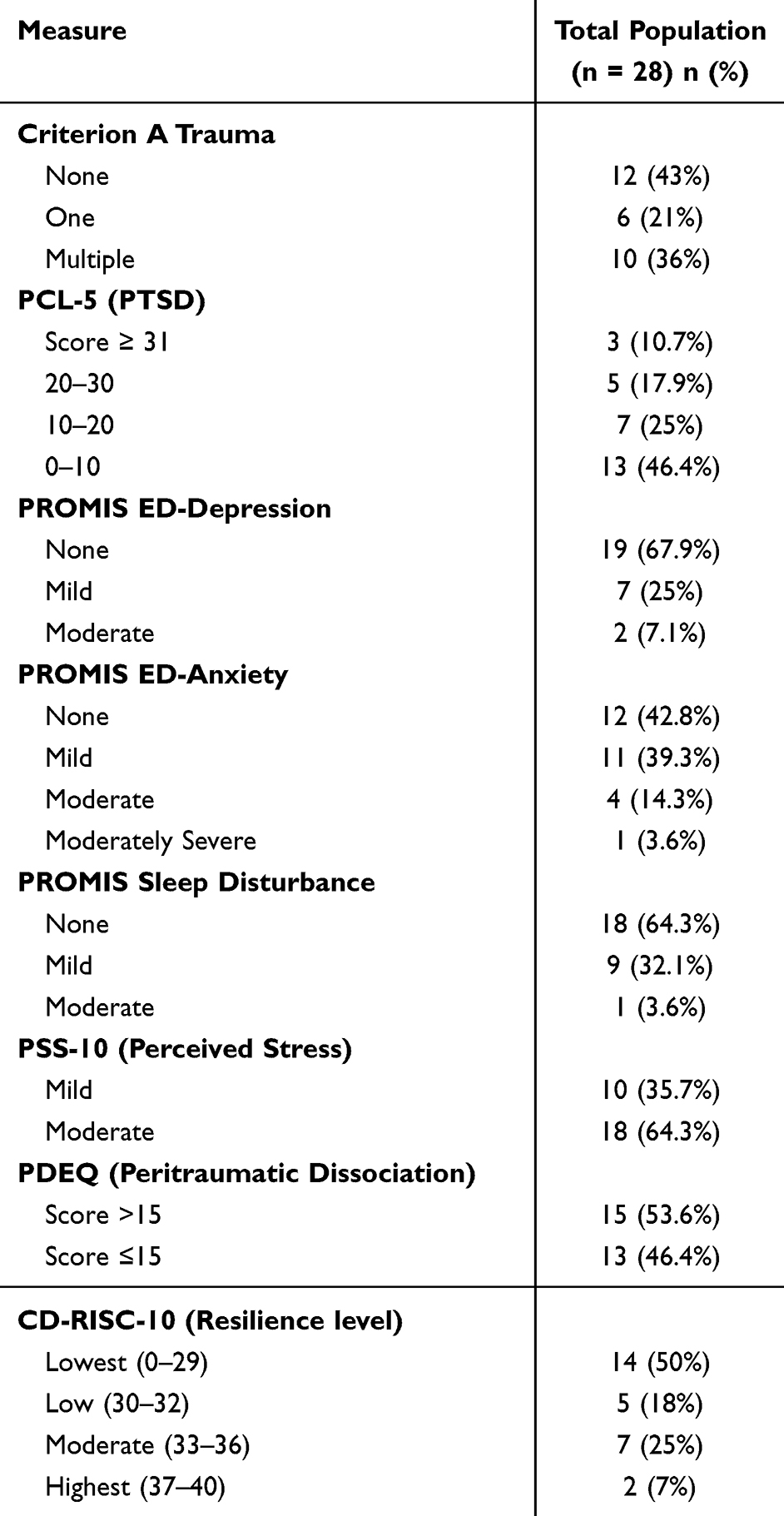 |
Table 4 Measure and Instrument Scores |
The PI placed the Actiheart on each participant per CamNtech guidelines.56 Baseline measurement (5 minutes acclimatization/10-minute measurement) was taken after placement of the Actiheart. Baseline measurement included participants’ pre-study activity (before 6:30 am) of sitting, standing, and walking, limited to non-engagement with unit-specific activities (eg, sitting in a chair, walking to nurses’ station). Each participant was observed between 6:30 and 10:30 am. The PI was the sole observer; only one nurse participated on any given day. At the end of the study period, participants completed two questionnaires in a private setting to obtain information on perceived stress (PSS-10) and peritraumatic dissociative experiences (PDEQ) related to their encounters that morning.
Data Analysis
Many participants experienced numerous consecutive events with little to no time for recovery. We created a new category, “Combined Events”, to accommodate these rapid, short-timed events (eg, addressing an alarm repeatedly going off) and evaluated HRV parameters from the start time of the first event until the end time of the last event that allowed enough time to evaluate the recovery period (5 minutes).
Data processing of HRV parameters followed recommendations of the Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology.27 Kubios Premium software 3.5.057 was utilized for analyzing HRV data. HRV data were first visually inspected and low-quality data were manually removed. Data were inspected manually using a piecewise cubic spline interpolation method to identify and correct missed beats, extra and misaligned beats, and real artifact. The approach demonstrated 96.9% accuracy in detecting real artifact and 99.9% accuracy in identifying normal beats.58 Artifact correction was performed with an artifact identification threshold of 0.35s to minimize overcorrection.27,59 Data were pre-processed using a smoothness priors method for detrending RR intervals (Lambda = 500, fc = 0.035 hz), eliminating very low frequency components.60 Variations of autoregressive integrated moving average (ARIMA; vector, exogenous, etc). modeling was used to validate baseline (sitting/standing/mobile), events, and stress-recovery of dynamic HRV output data. The ARIMA modeling was used to detrend select time intervals until non-stationary trends were absent from the final time series (confirmed with Augmented Dickey-Fuller test) and supported use of “best” analysis windows, fit, and suitability (of residuals and autocorrelations) within selected time intervals.61 A Fast Fourier algorithm was used to compute power in the LF and HF spectra using Welch’s (1967) periodogram method (150 s Hanning window and overlapping segments at 50%). Because HF HRV data is influenced by breathing, these data were analyzed taking breathing frequency into account in accordance with previous studies to provide more comparable data.62
Demographic descriptive statistics, health information, and survey measure scores were summarized using frequency, proportion, mean, and standard deviation, where appropriate. General linear mixed models (GLMM) were used to examine associations between HRV parameters (SDNN, RMSSD, HF, and LF) and types of events (Interpersonal, Routine Care, Stat, and Combined Events). GLMM were also used to examine associations between HRV parameters and experience of the nurse (new nurse [<2 years], experienced nurse [≥2 years]). Spearman correlation coefficients were used to determine correlations between HRV outcomes and survey scores. Survey scores were also dichotomized according to the criteria of symptom severity for subgroup comparison. The Wilcoxon rank sum test was used to compare HRV between nurses in different groups, such as work experience (≥2 years vs <2 years), with and without PTSD, etc. All analyses were performed using R Software version 4.1.0.63 All tests were two-sided and employed a significance level of .05.
Results
HRV data were collected from 30 participants; however, data from two participants were excluded due to an unacceptable amount of artifact (defined in the data analysis section). Regarding job satisfaction, 64% (n = 18) reported being merely “somewhat satisfied” with their job, with only 14% (n = 4) “very satisfied”. Reflecting retention problems in the US, 75% (n = 21) of the nurses in this sample thought of leaving their job in the past 6 months. See Table 1 for demographic and lifestyle characteristics.
The majority of participants in this sample (78.5%; n = 22) reported a mean sleeping time of 6 to 7 hours per night; 18% (n = 5) more than 7 hours; one nurse (3.5%) reported less than 6 hours sleep per night. In this sample, 64% (n = 18) of participants scored within normal limits, whereas 18% (n = 5) reported mild sleep disturbance, and 5 (18%) described moderate sleep disturbance. A complete list of survey measure scores can be found in Table 4.
More than half of participants (57%; n = 16) reported experiencing a previous trauma, with 36% (n = 10) having experienced multiple traumas. Based PCL-5 score ≥31, 3 (11%) participants were identified as having probable PTSD. Nearly two-thirds of participants (64%; n = 18) reported moderate stress (PSS-10), with 36% (n = 10) answering positively to mild stress. Perhaps one of the most insightful findings was that of the PDEQ, in that 54% (n = 15) of participants had previous peritraumatic dissociative experiences, or experiences where “what was happening seemed unreal to me, like I was in a dream, or watching a movie or play”.
For anxiety, one participant (3.5%) scored as having moderately severe anxiety, 29% (n = 8) moderate anxiety, and 25% (n = 7) mild anxiety. Depression scores indicated 7% (n = 2) had moderate depression and 25% (n = 7) mild depression. Resilience scores using CD-RISC-10 resulted in a mean score of 30.11 (SD 5.08) indicating low overall resilience for the sample. Lastly, 21% (n = 6) of the ICU nurses in this sample practiced some type of meditation.
Workplace Events and HRV Parameters
In total, there were 111 events recorded for the 28 participants after merging combined events into the Combined Events category. HRV parameters in RMSSD, HF (reflecting parasympathetic activity), and SDNN (demonstrating overall HRV) tended to have the greatest reduction from Baseline to Stat or Routine events (see Table 5 and Figure 1). Trends of less decrease in RMSSD and HF to Interpersonal or Combined Events, with an increase in SDNN were observed. For LF (reflecting both sympathetic and parasympathetic activity), the largest increase from Baseline tended to be seen for Interpersonal Events, with a lesser increase for Routine and Stat events.
 |
Table 5 Change in ICU Nurses’ HRV Parameters from Baseline to Events |
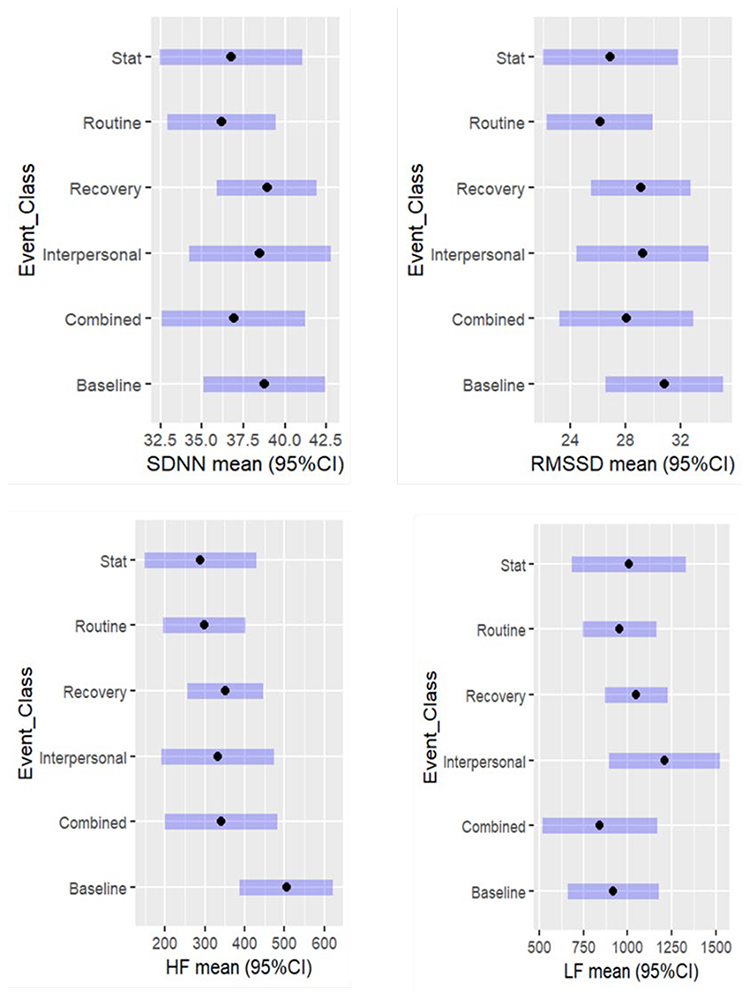 |
Figure 1 Change in HRV Parameters From Baseline to Events and Recovery. |
When differentiating HRV parameters between new and experienced nurses, new nurses tended to have reduced Baseline HRV compared to experienced nurses. New nurses also had reduced RMSSD, SDNN, and HF and greater increases in LF to events and recovery than experienced nurses (see Figure 2 and Table 6). Experienced nurses appeared to have a larger reduction to events from Baseline than new nurses in SDNN (2.51 vs 0.81, respectively) and HF (220.1 vs 143.1, respectively); however, this was largely due to new nurses reduced Baseline HRV. In LF, a greater increase tended to be seen in new nurses vs experienced nurses (88.5 vs 56.5, respectively). Regarding recovery from the events, experienced nurses tended to recover closer to Baseline post event than new nurses for SDNN (2.46 vs 0.97, respectively) and RMSSD (2.31 vs 0.86, respectively). In HF, a slight beneficial recovery post event tended to be seen in new nurses (35.9 vs 66.6, respectively). An even greater increase in LF was seen post event in both groups, with a tendency for experienced nurses to have a lesser increase post event (42.1 vs 131.6, respectively). None of the above comparisons were statistically significant, possibly due to the small sample size. No significant association of HRV and psychometric study variables was found by subgroup comparisons using Wilcoxon Rank Sum Test (see Table 7) or Spearman correlation analysis (see Table 8).
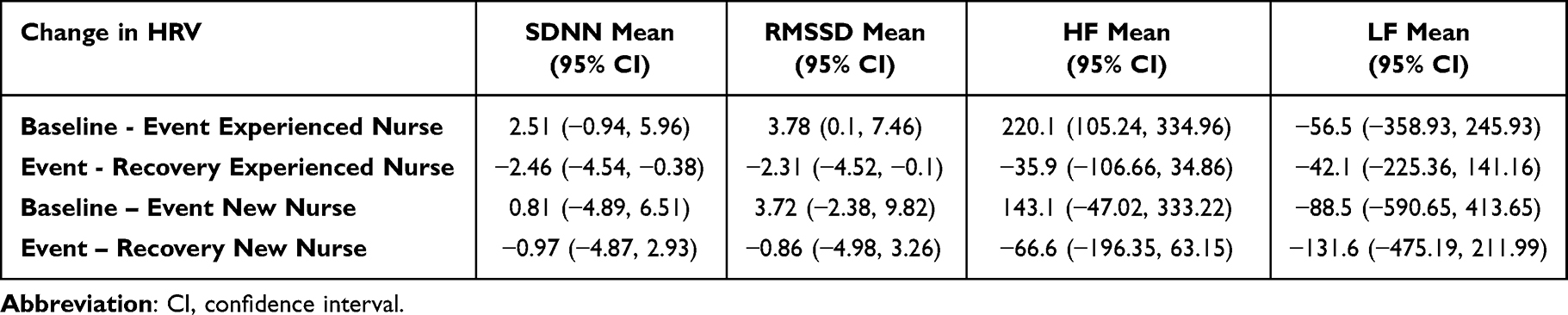 |
Table 6 Change in HRV Parameters in ICU Nurses by Work Experience |
 |
Table 7 Heart Rate Variability Parameters and Psychometric Measures by Subgroup |
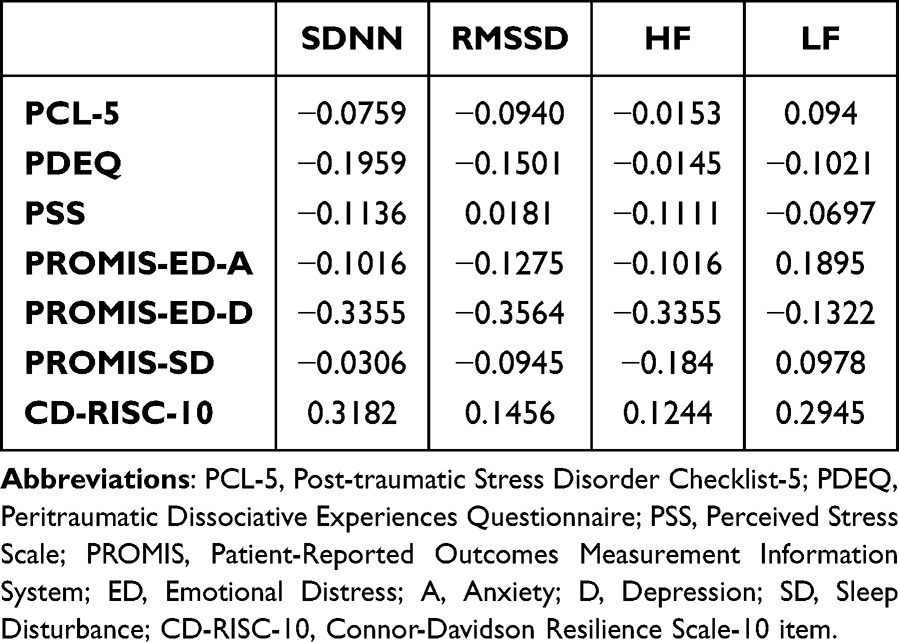 |
Table 8 Spearman Correlations Between Heart Rate Variability Parameters and Psychometric Measures |
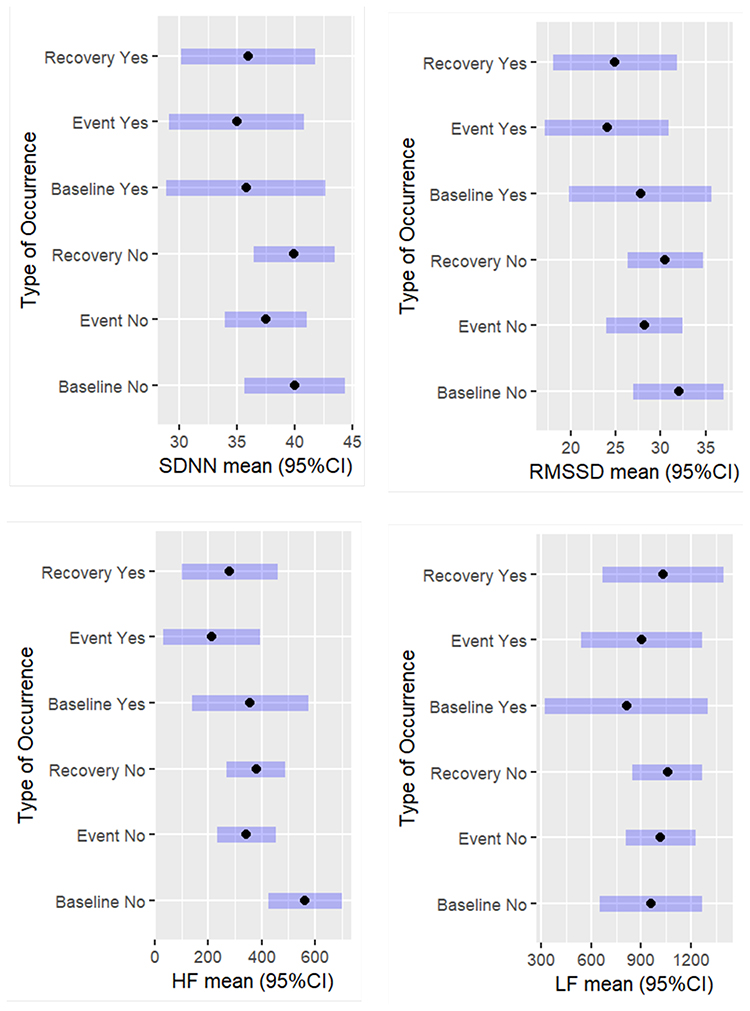 |
Figure 2 Differences in Change in HRV Parameters Between New Nurses and Experienced Nurses. Notes: New Nurses = Yes; Experienced Nurses = No. |
Discussion
The main objectives of this study were twofold: to investigate and quantify the association of HRV to workplace events ICU nurses experience, as well as to examine the association between HRV and PTSD and associated measures of psychological stress.
HRV and Workplace Events
We found ICU nurses’ HRV parameters of SDNN, RMSSD, and HF tended to have the greatest reduction from Baseline to Stat and Routine Events. Greater reduction from Baseline to these events suggests that, overall, these were more stressful for the ICU nurses. An increase in LF to events was also observed. Increases in the HRV parameter of LF can reflect an increase in SNS activity. The reduction of HRV from Baseline to Stat events was expected. These are the events that require prompt attention, and include urgent care (ie, if care were not given, would likely result in physical danger or grave disability) or unexpected care events (eg, an unexpected drop in blood pressure requiring an immediate intravenous vasopressor). What was not expected was that even though reductions in HRV parameters were observed with Combined Events (those that occurred in rapid succession, allowing little to no time for recovery), Routine events tended to cause more of a reduction in HRV parameters. Therefore, routine events were stressful for the ICU nurses, not just urgent or multiple events in succession. This suggests that even though routine in this environment, job actions causing moral distress, performing care that causes discomfort or pain, withdrawing life-support, repositioning an unstable patient, or providing end-of-life care, can be as stressful for nurses as responding to a Stat or urgent event.64,65 The day–to–day workplace environment (eg, poor control over workload, excessive electronic record charting) can also induce significant stress.66
Our HRV findings are in accordance with others in the scientific literature. Kim et al67 meta-analysis and review also found psychological stress caused a decrease in the HF band and increase in the LF band, and further noted that these were the most frequently reported factors in their review. Järvelin-Pasanen et al68 study with a sample of female nurses, which investigated the differences between and within normal and extended work shifts, also determined lower mean RMSSD and HF, and higher LF values of HRV. Goffeng et al69 study used similar time-domain HRV as this study and found a reduction in SDNN and RMSSD parameters in a sample of health care workers during extended work shifts. Li et al70 study investigated workplace stress in nurses using HRV parameters of RMSSD and LF. They, too, found reductions in RMSSD and increases in LF during the nurses’ work shift.
New Nurses Versus More Experienced Nurses
Of particular interest, we found new ICU nurses tended to have lower Baseline HRV and reduced HRV to events and recovery than experienced ICU nurses. One explanation is that new nurses’ HRV parameters may be more reduced because the work environment is more unpredictable for them, and they may possibly have been thinking harder about the uncertainty of their workday. Previous literature has determined that increased mental tasks can result in reduced HRV.71 The American Nurses Foundation 2023 Pulse on the Nation’s Nurses Survey found that a significant relationship exists between younger age and emotional health. Younger nurses, and those with less experience, were disproportionally impacted by workplace stress factors than those with more experience.66 Mentorship programs with experienced nurses on the unit, peer support groups, and access to good communication with leadership are strategies administration and nurse managers should support to provide a solid foundation for new nurses.72,73
Psychometric Findings
This sample of ICU nurses reported symptoms of PTSD (mean PCL-5 score 14.25, SD 11.97), with 3 (11%) participants meeting the threshold for a provisional diagnosis of PTSD. Schuster and Dwyer’s74 pre-COVID-19 pandemic integrative review of PTSD prevalence in nurses reported 8.5–20.8% of registered nurses and 18.2–24% of ICU nurses met criteria for PTSD. Of consideration, in our study approximately 25% of potential participants were excluded due to use of antianxiety or antidepressant agents, perhaps reducing the number of participants potentially reporting symptoms of PTSD.
More than half (54%) of the ICU nurses described having substantial dissociative symptoms. For example, some ICU nurses answered positively to questions such as, “I had moments of losing track of what was going on”, or “Things seemed to be happening in slow motion”, or “ I felt as though I were spectator watching what was happening to me, as if I were floating above the scene or observing it as an outsider”. Individuals who experience dissociation at the time of the traumatic event, or soon after, report alterations in time, place, person, and a sense of unreality to the event.45 It is thought that dissociation functions as a protective mechanism for the individual, reducing conscious awareness of the traumatic event, and ultimately blocking painful emotions.75 Repetitive exposure to witnessing pain, suffering, and traumatic incidents places ICU nurses at high risk for peritraumatic dissociative states.76 Prior research has identified peritraumatic dissociation as a significant antecedent or predictor of PTSD.77,78
Perceived stress of the ICU nurses was measured by the PSS-10, with nearly two-thirds (n = 18; 64.3%) reporting moderate stress and approximately one-third (n = 10; 35.7%) having low stress. Mean score for the group was 15.57 (SD 5.56). Higher levels as measured by the PSS-10 have been associated with increased cortisol levels and suppressed immune function.79 The high levels of stress reported in this group could lead to multiple physiological and psychological issues long-term.
Our sample of ICU nurses reported mostly mild symptoms of sleep disturbance, (n = 9; 30%), with only 1 (3%) nurse reporting moderate sleep disturbance. The pooled prevalence of sleep disturbance among “frontline” nurses (comprising 18 studies) in Al Maqbali et al16 systematic review and meta-analysis was 43%. Our sample of ICU nurses reported mostly mild anxiety symptoms (n = 11; 39.3%), with 4 (14.3%) participants having moderate anxiety symptoms, and only 1 (3.6%) answering positively for severe anxiety symptoms. For depression, 7 (25%) ICU nurses reported mild symptoms, while 2 (7.1%) had moderate symptoms. These values are much reduced from the peak of the COVID-19 pandemic, when nearly a third of ICU nurses (31.1%) in Guttormson et al1 study met the criteria for moderate to severe anxiety, while 44.6% met the criteria for moderate to severe depression. Our study’s lower depression finding may likely be due to study exclusion criterion excluding ICU nurses with a diagnosis of depression and/or taking antidepressants. The pooled prevalence of anxiety and depression among “frontline” nurses in Al Maqbali et al16 systematic review and meta-analysis was 37% and 35%, respectively.
In this sample of ICU nurses, the total mean CD-RISC-10 score was 30.11, which, according to the suggested interquartile cut-off points,80 is the lowest point in the second quartile of the average score distribution. Half of the ICU nurses’ (50%) total score was ≤29, which falls in the lowest quartile, meaning lowest resilience, and suggests difficulties in coping with stress. Similar results using the CD-RISC-10 were found with a sample of US nurses working during the COVID-19 pandemic,81 with nearly half of the respondents’ (46.4%) total score ≤29.
No significant association of HRV and psychometric study variables (PTSD, PDEs, perceived stress, anxiety, depression, sleep, and resilience) was found. Possible explanations for the absence of a relationship between psychometric study variables and HRV could be due to limitations of self-report measures. Also, most study findings relating to PTSD and HRV have been conducted among participants with an associated chronic condition, whereas our sample was comprised of healthy, young females. Nurses in this study showed low HRV (higher stress) in response to performing not only stat events, but routine events for nurses in an ICU (but not routine in most environments), and many were experiencing dissociative experiences. All this combined could be responsible for the low resiliency reported in these nurses, leaving them even more vulnerable for stress-related issues in the future. In our sample of nurses, only 78% reported being “somewhat” to “very satisfied” with their job, which reflects broader trends in hospital-based nursing. Job satisfaction data from the National Sample Survey of Registered Nurses (NSSRN) found that job satisfaction among hospital-based registered nurses declined by 11.8%, from 89.0% to 77.2%, since the previous NSSRN survey in 2017.82 This trend emphasizes the need for addressing workplace factors (eg, inadequate staffing, stressful work environment, burnout, and unsatisfactory management or leadership) that contribute to job dissatisfaction in hospital settings. Given that 75% of study nurses had thoughts of leaving their job, and that job dissatisfaction is a key factor in hospital nurses deciding to leave their jobs,83 significant and relentless policy interventions are called for to create healthy work environments and foster a more resilient nurse workforce.
Limitations
The nature of the cross-sectional design of this study means we cannot infer causality. Also, the cross-sectional nature of our study may not reflect the true direction of relationships between survey measures, as symptoms and/or responses may be transient. This was a convenience sample, so there may be selection bias. Furthermore, we had a small sample size in this pilot study, limiting detection of true relationships. Our sample was comprised of young, healthy female participants; therefore, our results may not generalize to other populations. One possible explanation of new nurses having lower HRV than experienced nurses we cannot rule out, is that nurses who had experienced increased workplace stress left their job and more resilient experienced nurses in our study site remained. Lastly, approximately 25% of potential participants were excluded from participation due to antidepressant or antianxiety medication use; this could have skewed our results toward a less stress-affected population of ICU nurses.
Conclusion
Study nurses showed high levels of dissociative symptoms, perceived stress, and anxiety, low resilience, and moderate levels of depression, regardless of excluding those known (>25%) to having medication for these issues. Despite the lack of association to other study variables, the ICU nurses experienced reductions in HRV to events at work and are vulnerable to potential related long-term physiological and psychological health issues. Stress is regulated by the ANS, increasing sympathetic modulation and the fight-or-flight response to stressors. It is important to identify ICU nurses with symptoms of PTSD, perceived stress, and PDEs, as individuals with chronic stress (and PTSD) have been observed as having alterations in ANS function.30 Chronic stress can lead to adaptations (allostasis) and pathophysiology due to allostatic load or overload.84 These adaptations to stress over time can result in a blunted response to stress and adverse long-term pathophysiology.84 Screening nurses for psychological stress early, including dissociative experiences could lead to a change in practice toward the initiation of interventions to mitigate potential issues that lead to health, patient care, and institutional staffing problems.
The findings from our study have several potential clinical implications. Indicators of stress and recovery of ICU nurses at work, such as HRV parameters, are useful for early identification and prevention of stress. Information on types of work-related events that reduce HRV (cause stress) can help identify strategies to reduce stress, which is beneficial for health promotion at work. The PDEQ may be a useful early indicator of PTSD and demonstrates the need for intervention in this population. Future prospective, longitudinal designs, measuring HRV over at least 24 hours, and with a large sample size are needed to evaluate the relationship between HRV and both workplace stress and PTSD in ICU nurses. Furthermore, research with ICU nurses given a diagnosis of depression and/or taking medications versus those with no depression is needed. Lastly, more research is needed to investigate HRV and stress differences in new nurses versus experienced nurses.
Acknowledgments
The authors thank the ICU nurses who participated in this study. This paper is based on the thesis of Paula Miller Levi. It has been published on the institutional research repository website: https://digitalcommons.library.uab.edu/cgi/viewcontent.cgi?params=%2Fcontext%2Fetd-collection%2Farticle%2F1180%2F&path_info=Levi_uab_0005D_13524.pdf
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Deep South Center for Occupational Health and Safety and the National Institute of Occupational Safety and Health (Grant #T42OH008436).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Guttormson JL, Calkins K, McAndrew N, Fitzgerald J, Losurdo H, Loonsfoot D. Critical care nurses’ experiences during the COVID-19 pandemic: a US national survey. Am J Crit Care. 2022;31(2):96–103. doi:10.4037/ajcc2022312
2. Quesada-Puga C, Izquierdo-Espin FJ, Membrive-Jiménez MJ, et al. Job satisfaction and burnout syndrome among intensive-care unit nurses: a systematic review and meta-analysis. Int Crit Care Nurs. 2024;82:103660. doi:10.1016/j.iccn.2024.103660
3. Levi P, Moss J. Intensive care unit nurses’ lived experiences of psychological stress and trauma caring for COVID-19 patients. Workplace Health Saf. 2022;70(8):358–367. doi:10.1177/21650799211064262
4. Ramírez-Elvira S, Romero-Béjar JL, Suleiman-Martos N, et al. Prevalence, risk factors and burnout levels in intensive care unit nurses: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(21):11432. doi:10.3390/ijerph182111432
5. Salmon G, Morehead A. Posttraumatic stress syndrome and implications for practice in critical care nurses. Crit Care Nurs Clin North Am. 2019;31(4):517–526. doi:10.1016/j.cnc.2019.07.007
6. Mokaya PO, Ntinyari N, Limungi G, Kasmai EK, Gabriella HF. Assessing the impact of the coronavirus pandemic on the mental health status of intensive care unit nurses: a systematic review. BMC Nurs. 2025;24(1):487. doi:10.1186/s12912-025-03117-6
7. Greenberg N, Weston D, Hall C, Caulfield T, Williamson V, Fong K. Mental health of staff working in intensive care during COVID-19. Occup Med. 2021;71(2):62–67. doi:10.1093/occmed/kqaa220
8. Levi P, Patrician PA, Vance DE, Montgomery AP, Moss J Post-traumatic stress disorder in intensive care unit nurses: a concept analysis. Workplace Health Saf. 2021;69(5):224–234. doi:10.1177/2165079920971999
9. Rodríguez-Rey R, Palacios A, Alonso-Tapia J, et al. Are pediatric critical personnel satisfied with their lives? prediction of satisfaction with life from burnout, posttraumatic stress, and posttraumatic growth, and comparison with noncritical pediatric staff. Pediatr Crit Care Med. 2019;20(3):e160–e169. doi:10.1097/PCC.0000000000001861
10. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
11. Meinhausen C, Prather AA, Sumner JA. Posttraumatic stress disorder (PTSD), sleep, and cardiovascular disease risk: a mechanism-focused narrative review. Health Psychol. 2022;41(10):663–673. doi:10.1037/hea0001143
12. Bustamante-Sánchez Á, Tornero-Aguilera JF, Fernández-Elías VE, Hormeño-Holgado AJ, Dalamitros AA, Clemente-Suárez VJ. Effect of stress on autonomic and cardiovascular systems in military population: a systematic review. Cardiol Res Pract. 2020;2020:7986249. doi:10.1155/2020/7986249
13. Dyball D, Evans S, Boos CJ, Stevelink SAM, Fear NT. The association between PTSD and cardiovascular disease and its risk factors in male veterans of the Iraq/Afghanistan conflicts: a systematic review. Int Rev Psychiatry. 2019;31(1):34–48. doi:10.1080/09540261.2019.1580686
14. Hoerster KD, Campbell S, Dolan M, et al. PTSD is associated with poor health behavior and greater body mass index through depression, increasing cardiovascular disease and diabetes risk among U.S. veterans. Prev Med Rep. 2019;15:100930. doi:10.1016/j.pmedr.2019.100930
15. Roberts AL, Liu J, Lawn RB, et al. Association of posttraumatic stress disorder with accelerated cognitive decline in middle-aged women. JAMA Network Open. 2022;5(6):e2217698. doi:10.1001/jamanetworkopen.2022.17698
16. Al Maqbali M, Al Sinani M, Al-Lenjawi B. Prevalence of stress, depression, anxiety and sleep disturbance among nurses during the COVID-19 pandemic: a systematic review and meta-analysis. J Psychosom Res. 2021;141:110343. doi:10.1016/j.jpsychores.2020.110343
17. Luciano MT, Acuff SF, Olin CC, et al. Posttraumatic stress disorder, drinking to cope, and harmful alcohol use: a multivariate meta-analysis of the self-medication hypothesis. J Psychopathol Clin Sci. 2022;131(5):447–456. doi:10.1037/abn0000764
18. Krishnamoorthy Y, Nagarajan R, Saya GK, Menon V. Prevalence of psychological morbidities among general population, healthcare workers and COVID-19 patients amidst the COVID-19 pandemic: a systematic review and meta-analysis. Psychiatry Res. 2020;293:113382. doi:10.1016/j.psychres.2020.113382
19. Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. 2020;88:901–907. doi:10.1016/j.bbi.2020.05.026
20. Ariapooran S, Ahadi B, Khezeli M. Depression, anxiety, and suicidal ideation in nurses with and without symptoms of secondary traumatic stress during the COVID-19 outbreak. Arch Psychiatr Nurs. 2022;37:76–81. doi:10.1016/j.apnu.2021.05.005
21. Feingold JH, Peccoralo L, Chan CC, et al. Psychological impact of the COVID-19 pandemic on frontline health care workers during the pandemic surge in New York City. Chronic Stress. 2021;5:2470547020977891. doi:10.1177/2470547020977891
22. Hong S, Ai M, Xu X, et al. Immediate psychological impact on nurses working at 42 government-designated hospitals during COVID-19 outbreak in China: a cross-sectional study. Nurs Outlook. 2021;69(1):6–12. doi:10.1016/j.outlook.2020.07.007
23. Shen X, Zou X, Zhong X, Yan J, Li L. Psychological stress of ICU nurses in the time of COVID-19. Crit Care. 2020;24(1):200. doi:10.1186/s13054-020-02926-2
24. American Hospital Association. AHA letter re: challenges facing America’s health care workforce as the U.S. enters third year of COVID-19 pandemic. 2022. Available from: https://www.aha.org/lettercomment/2022-03-01-aha-provides-information-congress-re-challenges-facing-americas-health.
25. Shah MK, Gandrakota N, Cimiotti JP, Ghose N, Moore M, Ali MK. Prevalence of and factors associated with nurse burnout in the US. JAMA Network Open. 2021;4(3):e215373. doi:10.1001/jamanetworkopen.2020.36469
26. Nursing Solutions, Incorporated. Retention & RN staffing report. 2023. Available from: https://www.nsinursingsolutions.com/Documents/Library/NSI_National_Health_Care_Retention_Report.pdf.
27. Malik M. Heart rate variability: standards of measurement, physiological interpretation, and clinical use: task force of the European society of cardiology and the North American society for pacing and electrophysiology. Ann Noninvasive Electrocardiol. 1996;1(2):151–181. doi:10.1111/j.1542-474X.1996.tb00275.x
28. Ge F, Yuan M, Li Y, Zhang W. Posttraumatic stress disorder and alterations in resting heart rate variability: a systematic review and meta-analysis. Psychiatry Invest. 2020;17(1):9–20. doi:10.30773/pi.2019.0112
29. Correia ATL, Lipinska G, Rauch HGL, Forshaw PE, Roden LC, Rae DE. Associations between sleep-related heart rate variability and both sleep and symptoms of depression and anxiety: a systematic review. Sleep Med. 2023;101:106–117. doi:10.1016/j.sleep.2022.10.018
30. Schneider M, Schwerdtfeger A. Autonomic dysfunction in posttraumatic stress disorder indexed by heart rate variability: a meta-analysis. Psychol Med. 2020;50(12):1937–1948. doi:10.1017/S003329172000207X
31. Corrigan SL, Roberts S, Warmington S, Drain J, Main LC. Monitoring stress and allostatic load in first responders and tactical operators using heart rate variability: a systematic review. BMC Public Health. 2021;21(1):1701. doi:10.1186/s12889-021-11595-x
32. Powers A, Mekawi Y, Fickenwirth M, et al. Emotion dysregulation and dissociation contribute to decreased heart rate variability to an acute psychosocial stressor in trauma-exposed Black women. J Psychiatr Res. 2021;142:125–131. doi:10.1016/j.jpsychires.2021.07.032
33. Moore CG, Carter RE, Nietert PJ, Stewart PW. Recommendations for planning pilot studies in clinical and translational research. Clin Transl Sci. 2011;4(5):332–337. doi:10.1111/j.1752-8062.2011.00347.x
34. Geovanini GR, Vasques ER, de Oliveira Alvim R, et al. Age and sex differences in heart rate variability and vagal specific patterns - Baependi Heart Study. Glob Heart. 2020;15(1):71. doi:10.5334/gh.873
35. Spina GD, Gonze BB, Barbosa ACB, Sperandio EF, Dourado VZ. Presence of age- and sex-related differences in heart rate variability despite the maintenance of a suitable level of accelerometer-based physical activity. Braz J Med Biol Res. 2019;52(8):e8088. doi:10.1590/1414-431X20198088
36. Alabama Board of Nursing. Analysis of Alabama Board of Nursing 2021 and 2022 Workforce Survey. 2022. Available from: https://www.abn.alabama.gov/wp-content/uploads/2023/09/2021-2022-ABN-Workforce-Survey-Executive-Summary_9.13.2023.pdf.
37. Brage S, Brage N, Franks PW, Ekelund U, Wareham NJ. Reliability and validity of the combined heart rate and movement sensor Actiheart. Eur J Clin Nutr. 2005;59(4):561–570. doi:10.1038/sj.ejcn.1602118
38. Moss J, Berner ES, Savell K. A mobile data collection tool for workflow analysis. Stud Health Technol Inform. 2007;129(Pt 1):48–52.
39. National Center for PTSD. PTSD checklist for DSM-5 (PCL-5). U.S. Department of Veterans Affairs. Available from: https://www.ptsd.va.gov/professional/assessment/documents/using-pcl5.pdf.
40. Blevins CA, Weathers FW, Davis MT, Witte TK, Domino JL. The posttraumatic stress disorder checklist for DSM-5 (PCL-5): development and initial psychometric evaluation. J Trauma Stress. 2015;28(6):489–498. doi:10.1002/jts.22059
41. Garcia O, Slavish DC, Dietch JR, et al. What goes around comes around: nightmares and daily stress are bidirectionally associated in nurses. Stress Health. 2021;37(5):1035–1042. doi:10.1002/smi.3048
42. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi:10.2307/2136404
43. Taylor JM. Psychometric analysis of the ten-item perceived stress scale. Psychol Assess. 2015;27(1):90–101. doi:10.1037/a0038100
44. Sandhu SS, Ismail NH, Rampal KG. The Malay version of the perceived stress scale (PSS)-10 is a reliable and valid measure for stress among nurses in Malaysia. Malays J Med Sci. 2015;22(6):26–31. doi:10.1136/oem.59.1.67
45. Marmar CR, Weiss DS, Metzler TJ. The Peritraumatic Dissociative Experiences Questionnaire. In: Wilson JP, Keane TM, editors. Assessing Psychological Trauma and PTSD. New York: Guildford Press; 1997:412–428.
46. van der Mei WF, Barbano AC, Ratanatharathorn A, et al. Evaluating a screener to quantify PTSD risk using emergency care information: a proof of concept study. BMC Emerg Med. 2020;20(1):16. doi:10.1186/s12873-020-00308-z
47. Schnurr P, Vielhauer M, Weathers F, Findler M. Brief trauma questionnaire. APA PsycTests. 1999. doi:10.1037/t07488-000
48. McCanlies EC, Sarkisian K, Andrew ME, Burchfiel CM, Violanti JM. Association of peritraumatic dissociation with symptoms of depression and posttraumatic stress disorder. Psychol Trauma. 2017;9(4):479–484. doi:10.1037/tra0000215
49. Campbell-Sills L, Stein MB. Psychometric analysis and refinement of the Connor-Davidson resilience scale (CD-RISC): validation of a 10-item measure of resilience. J Trauma Stress. 2007;20(6):1019–1028. doi:10.1002/jts.20271
50. Kim SC, Quiban C, Sloan C, Montejano A. Predictors of poor mental health among nurses during COVID-19 pandemic. Nurs Open. 2021;8(2):900–907. doi:10.1002/nop2.697
51. Buysse DJ, Yu L, Moul DE, et al. Development and validation of patient-reported outcome measures for sleep disturbance and sleep-related impairments. Sleep. 2010;33(6):781–792. doi:10.1093/sleep/33.6.781
52. HealthMeasures. PROMIS: measure development & research. 2022. Available from: https://www.healthmeasures.net/explore-measurement-systems/promis/measure-development-research.
53. Green K, Eddy A, Flowers J, Christopher M. A confirmatory factor analysis of the PROMIS sleep disturbance among law enforcement officers. J Police Crim Psychol. 2022;37(1):141–145. doi:10.1007/s11896-021-09471-w
54. Reitz KM, Terhorst L, Smith CN, et al. Healthcare providers’ perceived support from their organization is associated with lower burnout and anxiety amid the COVID-19 pandemic. PLoS One. 2021;16(11):e0259858. doi:10.1371/journal.pone.0259858
55. Kroenke K, Stump TE, Chen CX, et al. Minimally important differences and severity thresholds are estimated for the PROMIS depression scales from three randomized clinical trials. J Affect Disord. 2020;266:100–108. doi:10.1016/j.jad.2020.01.101
56. CamNtech L. The Actiheart guide to getting started. 2022. Available from: https://www.camntech.com/Products/Actiheart/The%20Actiheart%20Guide%20to%20Getting%20Started.pdf.
57. Tarvainen MP, Niskanen JP, Lipponen JA, Ranta-Aho PO, Karjalainen PA. Kubios HRV-heart rate variability analysis software. Comput Methods Programs Biomed. 2014;113(1):210–220. doi:10.1016/j.cmpb.2013.07.024
58. Lipponen JA, Tarvainen MP. A robust algorithm for heart rate variability time series artefact correction using novel beat classification. J Med Eng Technol. 2019;43(3):173–181. doi:10.1080/03091902.2019.1640306
59. Laborde S, Mosley E, Thayer JF. Heart rate variability and cardiac vagal tone in psychophysiological research - recommendations for experiment planning, data analysis, and data reporting. Front Psychol. 2017;8:213. doi:10.3389/fpsyg.2017.00213
60. Tarvainen MP, Georgiadis SD, Ranta-Aho PO, Karjalainen PA. Time-varying analysis of heart rate variability signals with a Kalman smoother algorithm. Physiol Meas. 2006;27(3):225–239. doi:10.1088/0967-3334/27/3/002
61. Gujral H, Kushwaha AK, Khurana S. Utilization of time series tools in life-sciences and neuroscience. Neurosci Insights. 2020;15:2633105520963045. doi:10.1177/2633105520963045
62. Shaffer F, Meehan ZM. A practical guide to resonance frequency assessment for heart rate variability biofeedback. Front Neurosci. 2020;14:570400. doi:10.3389/fnins.2020.570400
63. R Core Team. R: a language and environment for statistical computing. R foundation for statistical computing. 2022. Available from: https://www.R-project.org/.
64. Salari N, Shohaimi S, Khaledi-Paveh B, Kazeminia M, Bazrafshan MR, Mohammadi M. The severity of moral distress in nurses: a systematic review and meta-analysis. Philos Ethics Humanit Med. 2022;17(1):13. doi:10.1186/s13010-022-00126-0
65. American Nurses Foundation. Pulse on the nation’s nurses survey series: mental health and wellness survey 4, 2023. https://www.nursingworld.org/practice-policy/work-environment/health-safety/disaster-preparedness/coronavirus/what-you-need-to-know/survey-4/.
66. American Nurses Foundation. COVID-19 two-year impact assessment. 2022. Available from: https://www.nursingworld.org/practice-policy/work-environment/health-safety/disaster-preparedness/coronavirus/what-you-need-to-know/covid-19-impact-assessment-survey-the-second-year/contentassets/covid-19-two-year-impact-assessment-written-report-final.pdf.
67. Kim HG, Cheon EJ, Bai DS, Lee YH, Koo BH. Stress and heart rate variability: a meta-analysis and review of the literature. Psychiatry Invest. 2018;15(3):235–245. doi:10.30773/pi.2017.08.17
68. Järvelin-Pasanen S, Ropponen A, Tarvainen MP, Karjalainen PA, Louhevaara V. Differences in heart rate variability of female nurses between and within normal and extended work shifts. Ind Health. 2013;51(2):154–164. doi:10.2486/indhealth.ms1368
69. Goffeng EM, Nordby KC, Tarvainen MP, et al. Fluctuations in heart rate variability of health care workers during four consecutive extended work shifts and recovery during rest and sleep. Ind Health. 2018;56(2):122–131. doi:10.2486/indhealth.2017-0100
70. Li X, Zhu W, Sui X, Zhang A, Chi L, Lv L. Assessing workplace stress among nurses using heart rate variability analysis with wearable ECG device-a pilot study. Front Public Health. 2022;9:810577. doi:10.3389/fpubh.2021.810577
71. Arutyunova KR, Bakhchina AV, Konovalov DI, Margaryan M, Filimonov AV, Shishalov IS. Heart rate dynamics for cognitive load estimation in a driving simulation task. Sci Rep. 2024;14(1):31656. doi:10.1038/s41598-024-79728-x
72. Mínguez Moreno I, González de la Cuesta D, Barrado Narvión MJ, Arnaldos Esteban M, González Cantalejo M. Nurse mentoring: a scoping review. Healthcare. 2023;11(16):2302. doi:10.3390/healthcare11162302
73. Watson AL, Young C, Whitham A, Prescott S, Flynn EJ. Enhancing nursing practice through peer support: strategies for engagement in the nursing workforce. J Radiol Nurs. 2025;44(1):31–35. doi:10.1016/j.jradnu.2024.06.003
74. Schuster M, Dwyer PA. Post-traumatic stress disorder in nurses: an integrative review. J Clin Nurs. 2020;29(15–16):2769–2787. doi:10.1111/jocn.15288
75. Atchison M, McFarlane AC. A review of dissociation and dissociative disorders. Aust N Z J Psychiatry. 1994;28(4):591–599. doi:10.1080/00048679409080782
76. Geuzinge R, Visse M, Duyndam J, Vermetten E. Social embeddedness of firefighters, paramedics, specialized nurses, police officers, and military personnel: systematic review in relation to the risk of traumatization. Front Psychiatry. 2020;11:496663. doi:10.3389/fpsyt.2020.496663
77. Memarzia J, Walker J, Meiser-Stedman R. Psychological peritraumatic risk factors for post-traumatic stress disorder in children and adolescents: a meta-analytic review. J Affect Disord. 2021;282:1036–1047. doi:10.1016/j.jad.2021.01.016
78. Thompson-Hollands J, Jun JJ, Sloan DM. The association between peritraumatic dissociation and PTSD symptoms: the mediating role of negative beliefs about the self. J Trauma Stress. 2017;30(2):190–194. doi:10.1002/jts.22179
79. Cohen S, Janicki-Deverts D. Who’s stressed? Distributions of psychological stress in the United States in probability samples from 1983, 2006, and 2009. J Appl Soc Psychol. 2012;42(6):1320–1334. doi:10.1111/j.1559-1816.2012.00900.x
80. Davidson JRT. Connor-Davidson resilience scale (CDRISC) manual. 2018. Available from: http://www.connordavidson-resiliencescale.com/CD-RISC%20Manual%2008-19-18.pdf.
81. Petzel J. Resilience of regional hospital nursing staff working during the COVID-19 pandemic measured by the Connor-Davidson resilience scale. Maine Med Center. 2021;2021:2187.
82. Health Resources and Services Administration. National sample survey of registered nurses (NSSRN). 2022.
83. Enea M, Maniscalco L, de Vries N, et al. Exploring the reasons behind nurses’ intentions to leave their hospital or profession: a cross-sectional survey. Int J Nurs Stud Adv. 2024;7:100232. doi:10.1016/j.ijnsa.2024.100232
84. McEwen BS. Protective and damaging effects of stress mediators. N Engl J Med. 1998;338(3):171–179. doi:10.1056/NEJM199801153380307
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.