Back to Journals » OncoTargets and Therapy » Volume 9
Integrin and gene network analysis reveals that ITGA5 and ITGB1 are prognostic in non-small-cell lung cancer
Authors Zheng W, Jiang C, Li R
Received 4 July 2015
Accepted for publication 14 December 2015
Published 18 April 2016 Volume 2016:9 Pages 2317—2327
DOI https://doi.org/10.2147/OTT.S91796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr William C. Cho
Weiqi Zheng, Caihui Jiang, Ruifeng Li
Department of Radiation Oncology, Guangqian Hospital, Quanzhou, Fujian, People’s Republic of China
Background: Integrin expression has been identified as a prognostic factor in non-small-cell lung cancer (NSCLC). This study was aimed at determining the predictive ability of integrins and associated genes identified within the molecular network.
Patients and methods: A total of 959 patients with NSCLC from The Cancer Genome Atlas cohorts were enrolled in this study. The expression profile of integrins and related genes were obtained from The Cancer Genome Atlas RNAseq database. Clinicopathological characteristics, including age, sex, smoking history, stage, histological subtype, neoadjuvant therapy, radiation therapy, and overall survival (OS), were collected. Cox proportional hazards regression models as well as Kaplan–Meier curves were used to assess the relative factors.
Results: In the univariate Cox regression model, ITGA1, ITGA5, ITGA6, ITGB1, ITGB4, and ITGA11 were predictive of NSCLC prognosis. After adjusting for clinical factors, ITGA5 (odds ratio =1.17, 95% confidence interval: 1.05–1.31) and ITGB1 (odds ratio =1.31, 95% confidence interval: 1.10–1.55) remained statistically significant. In the gene cluster network analysis, PLAUR, ILK, SPP1, PXN, and CD9, all associated with ITGA5 and ITGB1, were identified as independent predictive factors of OS in NSCLC.
Conclusion: A set of genes was identified as independent prognostic factors of OS in NSCLC through gene cluster analysis. This method may act as a tool to reveal more prognostic-associated genes in NSCLC.
Keywords: integrin, prognosis, non-small-cell lung cancer, ITGA5, ITGB1
Introduction
Lung cancer, particularly non-small-cell lung cancer (NSCLC), is one of the most common malignancies and the most common cause of cancer-related mortality worldwide.1 The prognosis of patients with NSCLC, especially in an advanced stage, is generally poor where the 5-year survival rate is <10%.2
Integrins are heterodimeric cell-surface adhesion receptors generally consisting of noncovalently linked alpha and beta subunits. A total of 18 alpha and eight beta subunits with different functions are currently known.3 Integrin family members participate in a variety of processes influencing the cell’s biological behavior, including cell adhesion, recognition, immune response, metastasis of tumor cells as well as embryogenesis, hemostasis, and tissue repair.4 Alterations in integrin expression levels can influence cancer cell adhesion, polarity, and extracellular matrix assembly, which may result in tumor metastasis.5 Integrins can also interact with tyrosine kinase receptors, such as epidermal growth factor receptor (EGFR) and vascular EGFR (VEGFR), to promote cancer cell proliferation, survival, and differentiation.6 EGFR mutations frequently occur in patients with lung cancer, and these patients have been found to benefit from tyrosine kinase inhibitor-targeted therapy rather than first-line chemotherapy.7
There was a report that discussed the integrin profile and prognosis in NSCLC;8 however, external validation and interactions of integrins within the network of integrins were not determined. The Cancer Genome Atlas (TCGA) database has been developed in recent years using a large amount of NSCLC RNAseq data as well as detailed clinical data, and this has made bioinformatic data mining convenient and reliable.9 This study was aimed at determining the prognostic ability of integrins and associated genes identified through the molecular network using TCGA database analysis in NSCLC.
Materials and methods
Patients
Expression data of integrins and their associated genes and relative clinical data of patients with NSCLC were available in TCGA database provided on the website of the Cancer Genomics Browser of the University of California Santa Cruz (https://genome-cancer.ucsc.edu/). Thirty members of the integrin family were included in our study (Table S1). There were 1,092 patients with NSCLC enrolled in TCGA database (updated on February 24, 2015) according to the parameters defined in a previous study.10 Patients without fully characterized tumors, deficient overall survival (OS) data, or incomplete RNAseq information were excluded from the study. Clinicopathological characteristics, including age, sex, histology, TNM stage, American Joint Committee on Cancer stage, smoking status, and history of neoadjuvant and radiation therapy, were collected. Information on integrin family genes was also obtained from TCGA RNAseq database. Networks of integrin genes, which were independent prognostic predictors of NSCLC, were obtained from the cBioPortal website (http://www.cbioportal.org/public-portal/cgds_r.jsp). Network filters were set as “in the same complex” or “interacted with each other”, and threshold was set as >12% changes.
This study is based on publicly available data from TCGA database and did not involve interaction with human subjects or the use of personal identifying information. The study was approved by the Institutional Review Board of Guangqian Hospital, Quanzhou, Fujian, People’s Republic of China.
Statistical analysis
OS was defined as time from the date of diagnosis to the date of death or the last follow-up. Patients without an event of death were recorded as censored at the time of last follow-up. The R project (3.1.3) was used to perform statistical analysis. Survival curves were constructed using the Kaplan–Meier method, with log-rank tests used to assess differences between groups. Univariate and multivariate Cox proportional hazards models were used to analyze the relationship between integrin network expression and OS of patients with NSCLC in TCGA cohort. A two-sided P-value <0.05 was considered statistically significant. Odds ratios with 95% confidence intervals (CIs) were calculated.
Results
Clinical factors in TCGA cohorts
A total of 959 patients with NSCLC, including 576 men and 383 women, from TCGA cohort were enrolled in the current study. The median age of the cohort was 67. There were 485 patients diagnosed with adenocarcinoma and 474 patients diagnosed with squamous cell carcinoma (SCC). Detailed clinicopathological data are shown in Table 1. The median OS in this cohort was 16.7 months.
 | Table 1 Clinical characteristics of patients with NSCLC in TCGA cohort |
ITGA5 and ITGB1 expressions were independent prognostic factors for OS in TCGA cohort
In univariate Cox regression analysis, ITGA1, ITGA5, ITGA6, ITGB1, ITGB4, and ITGA11 were significantly associated with OS in patients with NSCLC (all P<0.05, Table 2). In multivariate models, after adjusting for age, sex, stage, histological subtype, smoking history, neoadjuvant therapy history, and radiation therapy history, ITGA5 (HR =1.17, 95% CI: 1.05–1.31) and ITGB1 (HR =1.31, 95% CI: 1.10–1.55) were independent predictors of prognosis (all P<0.01, Table 2).
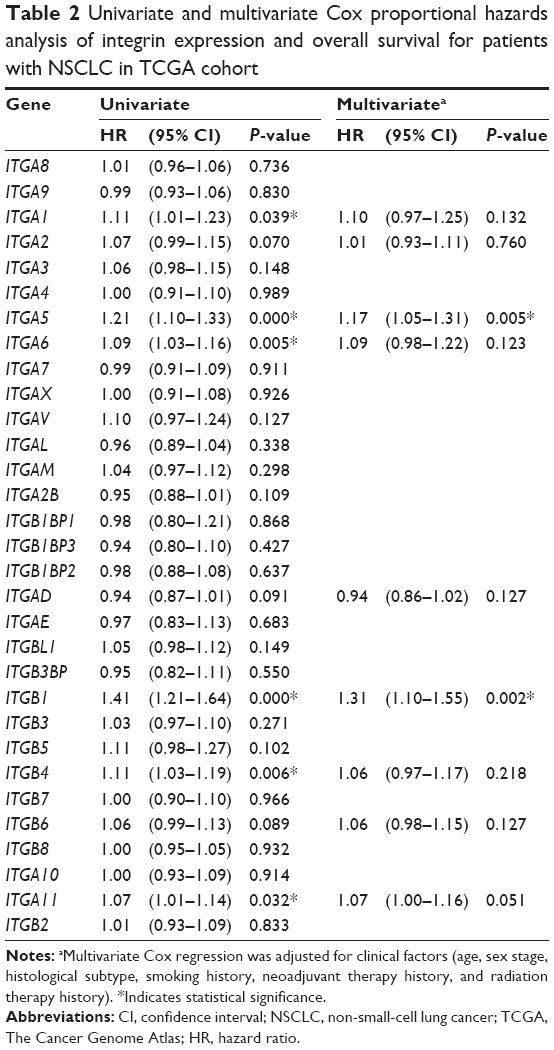 | Table 2 Univariate and multivariate Cox proportional hazards analysis of integrin expression and overall survival for patients with NSCLC in TCGA cohort |
We then divided TCGA cohort according to the histological subtype. In TCGA NSCLC cohort, large-cell carcinoma data were not available; therefore, we analyzed only two subgroups of adenocarcinoma and SCC. In 485 patients with adenocarcinoma, ITGA5 (HR =1.316, 95% CI: 1.135–1.525) and ITGB1 (HR =1.788, 95% CI: 1.399–2.286) were associated with OS in univariate analysis. However, in multivariate analysis, ITGA6 (HR =1.208, 95% CI: 1.014–1.439) was found to be the unique, independent prognostic factor. Also, ITGA5 (HR =1.142, 95% CI: 1.005–1.299) and ITGB1 (HR =1.231, 95% CI: 1.006–1.507) were prognostic factors of 474 patients with SCC with univariate analysis. After adjusting for clinical factors and other integrin family members, ITGA3 (HR =1.182, 95% CI: 1.002–1.394) was the only prognostic factor (Table 3).
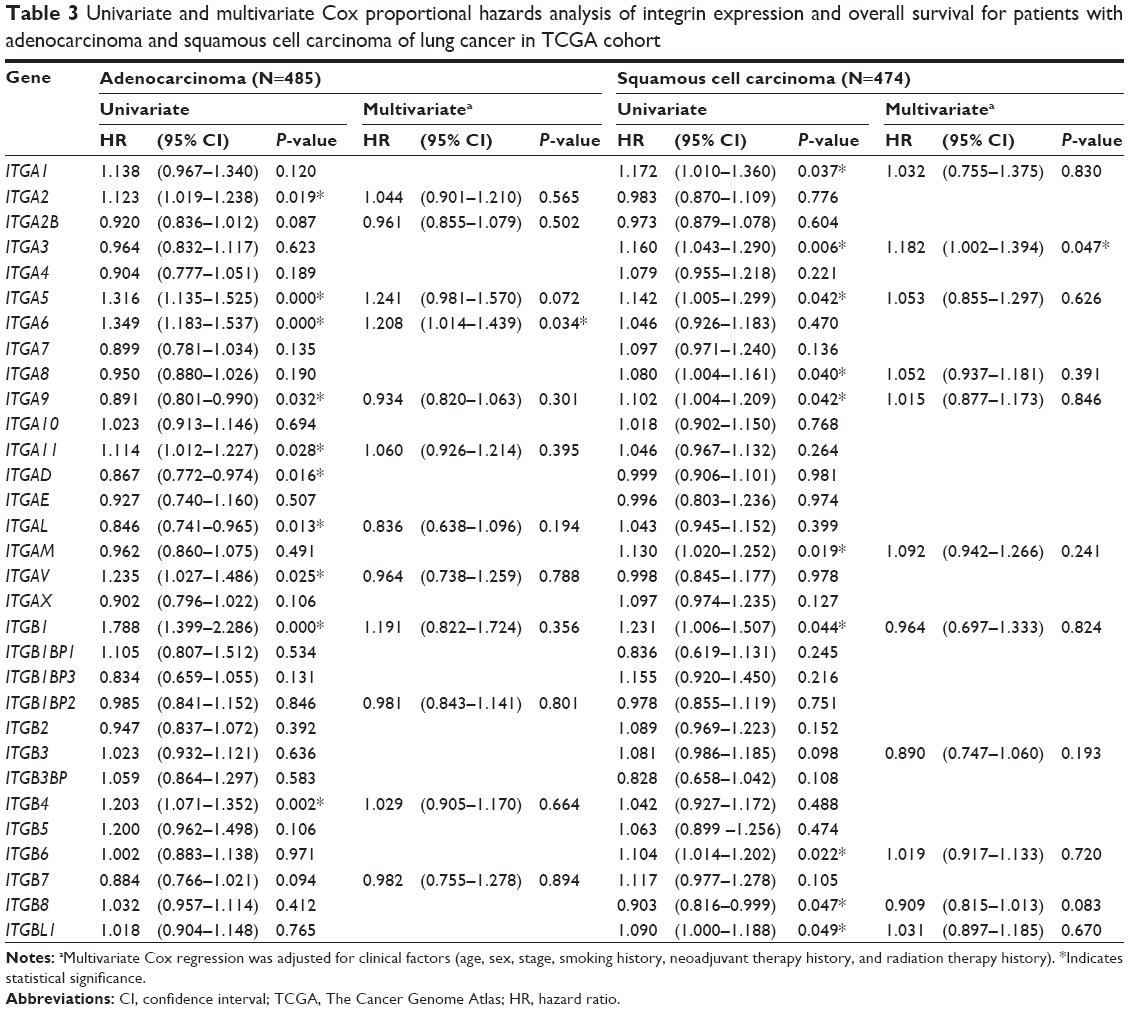 | Table 3 Univariate and multivariate Cox proportional hazards analysis of integrin expression and overall survival for patients with adenocarcinoma and squamous cell carcinoma of lung cancer in TCGA cohort |
Further studies of integrin and lymph node metastasis and distant metastasis were conducted with Spearman’s correlation analysis. ITGA3, ITGB5, ITGB6, and ITGB8 were associated with lymph node staging of SCC. ITGB1 was the only factor correlated with distant metastasis in SCC. The pattern was different in adenocarcinoma. ITGA5, ITGA7, ITGA9, ITGAD, ITGAL, and ITGAV were associated with N stage, and ITGA3, ITGB1BP3, ITGB5, and ITGBL1 were correlated with M stage (Table S2).
Expression levels of ITGA5 and ITGB1 in TCGA cohort showed nearly normal distribution (data not shown); therefore, we divided the cohort into low and high expressers according to the median expression levels of ITGA5 and ITGB1. Kaplan–Meier plots demonstrated that high expressers of ITGA5 or ITGB1 were associated with poor OS (all P<0.05, Figure 1A and B). Moreover, in subgroup analysis, ITGA5 and ITGB1 were associated with poor prognosis of adenocarcinoma as well as SCC (all P<0.05, Figure 2A–D).
 | Figure 1 Kaplan–Meier plots of survival are shown according to ITGA5 and ITGB1 expression. |
 | Figure 2 Kaplan–Meier estimates of overall survival according to ITGA5 expression, ITGB1 expression, and pathological histology. |
ITGA5 and ITGB1 gene cluster analysis and its association with prognosis
Although difference in integrin expression pattern existed between SCC and adenocarcinoma of lung cancer, ITGA5 and ITGB1 were more important genes because a selective inhibitor cilengitide has been developed.11 Therefore, the gene networks of ITGA5 and ITGB1 were studied. Three situations were selected for building the interaction network of ITGA5 and ITGB1 (Figure 3). They were stated as “react with”, “state change” (cut-point was set at 12%12), and “in same component”. A total of 33 genes were listed in the ITGA5 or ITGB1 gene networks (Table S3). In the univariate Cox regression model, PLAUR, PRKACA, ILK, YWHAZ, SPP1, PXN, LAMC1, TLN1, and CD9 expressions were indicated as predictive of prognosis in patients with NSCLC in TCGA cohort (P<0.05, Table 4). Multivariate analysis, after adjusting for all potential prognostic factors, indicated that PLAUR (HR =1.16, 95% CI: 1.04–1.30), ILK (HR =1.27, 95% CI: 1.00–1.60), SPP1 (HR =1.08, 95% CI: 1.02–1.15), PXN (HR =1.25, 95% CI: 1.06–1.48), and CD9 (HR =0.83, 95% CI: 0.74–0.94) were independent predictors of OS (all P<0.05, Table 4).
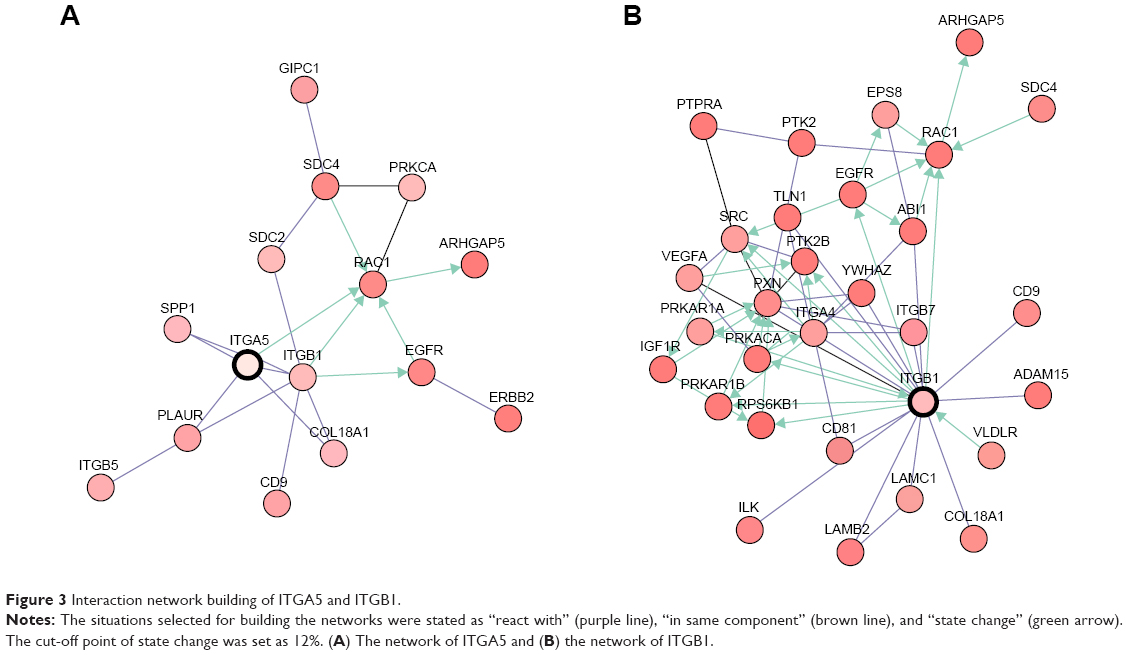 | Figure 3 Interaction network building of ITGA5 and ITGB1. |
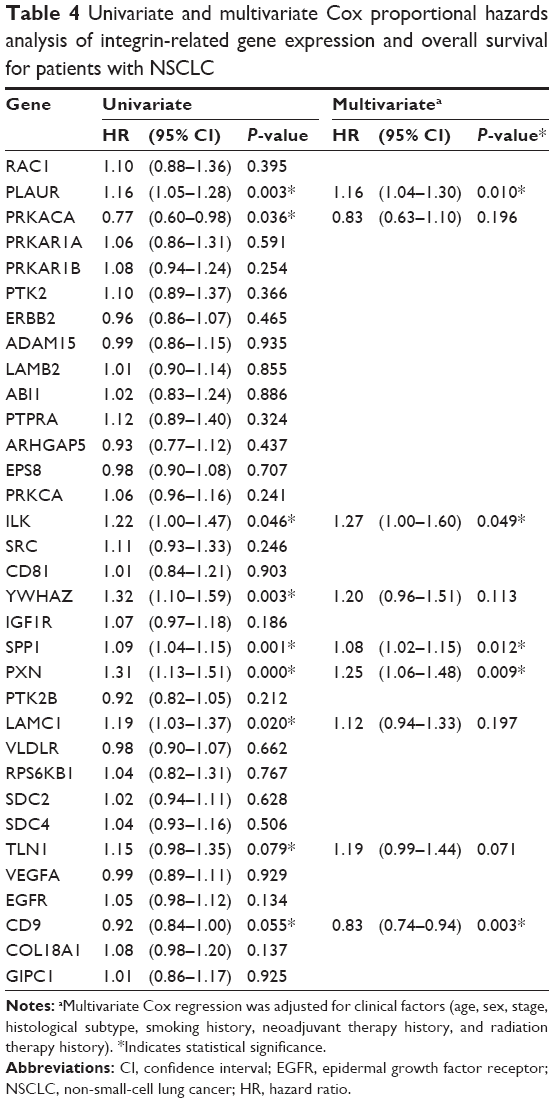 | Table 4 Univariate and multivariate Cox proportional hazards analysis of integrin-related gene expression and overall survival for patients with NSCLC |
Discussion
Dingemans et al had reported that ITGA5 and ITGB1 were prognostic factors in the early stage of NSCLC.8 We validated their findings in a large cohort from TCGA database. Aside from ITGA5 and ITGB1, PLAUR, ILK, SPP1, PXN, and CD9 were identified as independent predictors of OS in patients with NSCLC using gene network analysis.
As cell adhesion proteins, integrins play an important role in the cellular and extracellular environment to regulate attachment, survival, and motility.13 Integrins are communicators between the cell and the extracellular environment.5 Integrins can activate growth receptors and downstream cellular signals,6 leading to cancer growth, metastasis, tumor angiogenesis, and resistance to radiotherapy and chemotherapy.14,15 Integrin expression levels have been reported to correlate with prognosis in glioblastoma, cervical squamous cell cancer, ovarian cancer, gastric cancer, and melanoma.13,16–23 As drug targets, integrin inhibition enhances the cytotoxic efficacy of radiation and chemotherapy.24,25 Several integrin inhibitors have entered clinical trials as cancer therapy agents.26
Previous studies have reported an association between increased integrin alpha 5 expression and poor outcome in NSCLC.8,27 More specifically, Adachi et al found that in lymph-node-negative patients with NSCLC, high ITGA5 expressers had a significantly worse 5-year survival. It was suggested that tumors that express high levels of ITGA5 were more prone to metastasis or had undetectable micrometastases at the time of surgery.27 Other studies have also pointed to a relationship between ITGA5 and tumor metastasis. Valastyan et al reported that the downregulation of ITGA5 by miR-31 decreased breast cancer metastasis in vivo.28 MiR-148b-mediated ITGA5 inhibition could also decrease lung metastasis formation.29
The prognostic value of ITGB1 in NSCLC has been reported,30 and it was shown to be correlated with lymph node metastasis.31 ITGB1 inhibition has been shown to decrease lung cancer invasion and metastasis in vitro and in vivo.32 Our work indicates a certain correlation between NSCLC outcome and the integrin gene family; however, the mechanism, which is likely to be complex, remains unclear. Further study is required.
Our study tried to answer several questions left unanswered in previous studies. We found that integrins were differently expressed in SCC and adenocarcinoma of lung cancer. The independent factors were different as well. They were ITGA6 in adenocarcinoma and ITGA3 in SCC. The diversity of independent prognostic factors of NSCLC was possible due to different expression patterns of SCC and adenocarcinoma. A previous study had shown that ITGA3 was upregulated in adenocarcinoma but not in SCC;33 however, we found that the upregulation of ITGA3 in SCC indicated poor prognosis. In adenocarcinoma, the ITGA3 levels were relatively high with minor diversity. Another controversial topic is integrin and the metastatic potential of NSCLC. In our study, different subtypes of NSCLC demonstrated diverse integrins that were associated with metastasis. Only ITGA3 and ITGA5 were associated with NSCLC metastasis. ITGA5 was associated with lymph node metastasis of adenocarcinoma, which was possibly due to the role of ITGA5 in activating endothelial cells during tumor angiogenesis.8 Furthermore, our study identified a new set of genes as NSCLC biomarkers or even therapeutic targets through ITGA5 and ITGB1 network analysis. Suppression PLAUR expression could decrease lung cancer lymph node metastasis.34 ILK binds the cytoplasmic domain of beta integrins and regulates the integrin-mediated signal transduction. Its activity is important in epithelial-to-mesenchymal transition, and the overexpression of ILK has been implicated in tumor growth and metastasis via nuclear factor-κB signaling.35 SPP1 encodes for the protein osteopontin, which is principally expressed in NSCLC tissues. SPP1 may be tightly regulated by the Ras oncogene36 and is important in VEGF-mediated tumor angiogenesis.37 PXN, which encodes for the protein paxillin, has been shown to be regulated by miR-21838 and could make EGFR-mutant lung cancers resistant to tyrosine kinase inhibitor via modulating the stability of BIM and Mcl-1 proteins.39
Different from the above four genes, CD9 was a favorable factor in NSCLC outcome. This is supported by previous studies that showed that the low expression of CD9 may contribute to the early recurrence of NSCLC.40 These studies suggested that the influence of integrins on the outcome of NSCLC might be via the regulation of epithelial-to-mesenchymal transition, tumor invasion, angiogenesis, and metastasis. These consistent results demonstrated that our method was applicable for detecting new prognostic indicators or even therapeutic targets.
In the study, all information was obtained from a large population with long-time follow-up and standard specimen collection and sequencing. The results were open-access, repeatable, and with high statistical power. However, there were certain limitations to our study. Although there was external validation previously,8 we analyzed the correlation among integrins and network gene expression and NSCLC OS only in TCGA cohort. The prognosis of NSCLC is affected by many factors, such as comorbidity, tumor stage, surgical performance, and response to radiation therapy and chemotherapy, so a single biomarker is not enough. In addition, information on ethnicity was not available in TCGA database. In conclusion, further mechanistic research will be required to understand in more detail the integrin family and its role in patients with NSCLC.
Conclusion
ITGA5 and ITGB1 were identified as independent prognostic integrin markers associated with OS in NSCLC, and several outcome-related genes were determined through gene cluster analysis. This method could act as a tool to uncover more prognostic-associated genes and therapeutic targets in NSCLC.
Acknowledgment
The authors sincerely thank Dr Wan Fangning, Fudan University Shanghai Cancer Center, for providing bioinformatics support for this article.
Disclosure
The authors declare no conflicts of interest in this work.
References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. | ||
Yang P. Epidemiology of lung cancer prognosis: quantity and quality of life. Methods Mol Biol. 2009;471:469–486. | ||
Desgrosellier JS, Cheresh DA. Integrins in cancer: biological implications and therapeutic opportunities. Nat Rev Cancer. 2010;10(1):9–22. | ||
Schwartz MA, Ginsberg MH. Networks and crosstalk: integrin signalling spreads. Nat Cell Biol. 2002;4(4):E65–E68. | ||
Hynes RO. Integrins: bidirectional, allosteric signaling machines. Cell. 2002;110(6):673–687. | ||
Hehlgans S, Haase M, Cordes N. Signalling via integrins: implications for cell survival and anticancer strategies. Biochim Biophys Acta. 2007;1775(1):163–180. | ||
Steuer CE, Ramalingam SS. Targeting EGFR in lung cancer: lessons learned and future perspectives. Mol Aspects Med. 2015;45:67–73. | ||
Dingemans AM, van den Boogaart V, Vosse BA, van Suylen RJ, Griffioen AW, Thijssen VL. Integrin expression profiling identifies integrin alpha5 and beta1 as prognostic factors in early stage non-small cell lung cancer. Mol Cancer. 2010;9:152. | ||
Zhao Q, Shi X, Xie Y, Huang J, Shia B, Ma S. Combining multidimensional genomic measurements for predicting cancer prognosis: observations from TCGA. Brief Bioinform. 2015;16(2):291–303. | ||
Cancer Genome Atlas Research Network. Comprehensive molecular profiling of lung adenocarcinoma. Nature. 2014;511(7511):543–550. | ||
Albert JM, Cao C, Geng L, Leavitt L, Hallahan DE, Lu B. Integrin alpha v beta 3 antagonist Cilengitide enhances efficacy of radiotherapy in endothelial cell and non-small-cell lung cancer models. Int J Radiat Oncol Biol Phys. 2006;65(5):1536–1543. | ||
Zhang YM, Dai BL, Zheng L, et al. A novel angiogenesis inhibitor impairs lovo cell survival via targeting against human VEGFR and its signaling pathway of phosphorylation. Cell Death Dis. 2012;3:e406. | ||
Zhang ZY, Xu KS, Wang JS, et al. Integrin alphanvbeta6 acts as a prognostic indicator in gastric carcinoma. Clin Oncol (R Coll Radiol). 2008;20(1):61–66. | ||
Tchaicha JH, Mobley AK, Hossain MG, Aldape KD, McCarty JH. A mosaic mouse model of astrocytoma identifies alphavbeta8 integrin as a negative regulator of tumor angiogenesis. Oncogene. 2010;29(31):4460–4472. | ||
Zutter MM. Integrin-mediated adhesion: tipping the balance between chemosensitivity and chemoresistance. Adv Exp Med Biol. 2007;608:87–100. | ||
Ahmed N, Riley C, Rice GE, Quinn MA, Baker MS. Alpha(v)beta(6) integrin-A marker for the malignant potential of epithelial ovarian cancer. J Histochem Cytochem. 2002;50(10):1371–1380. | ||
Elayadi AN, Samli KN, Prudkin L, et al. A peptide selected by biopanning identifies the integrin alphavbeta6 as a prognostic biomarker for nonsmall cell lung cancer. Cancer Res. 2007;67(12):5889–5895. | ||
Goldberg I, Davidson B, Reich R, et al. Alphav integrin expression is a novel marker of poor prognosis in advanced-stage ovarian carcinoma. Clin Cancer Res. 2001;7(12):4073–4079. | ||
Kageshita T, Hamby CV, Hirai S, Kimura T, Ono T, Ferrone S. Alpha(v)beta3 expression on blood vessels and melanoma cells in primary lesions: differential association with tumor progression and clinical prognosis. Cancer Immunol Immunother. 2000;49(6):314–318. | ||
Hazelbag S, Kenter GG, Gorter A, et al. Overexpression of the alpha v beta 6 integrin in cervical squamous cell carcinoma is a prognostic factor for decreased survival. J Pathol. 2007;212(3):316–324. | ||
Nikkola J, Vihinen P, Vlaykova T, Hahka-Kemppinen M, Heino J, Pyrhonen S. Integrin chains beta1 and alphav as prognostic factors in human metastatic melanoma. Melanoma Res. 2004;14(1):29–37. | ||
Schittenhelm J, Schwab EI, Sperveslage J, et al. Longitudinal expression analysis of alphav integrins in human gliomas reveals upregulation of integrin alphavbeta3 as a negative prognostic factor. J Neuropathol Exp Neurol. 2013;72(3):194–210. | ||
Vellon L, Menendez JA, Lupu R. AlphaVbeta3 integrin regulates heregulin (HRG)-induced cell proliferation and survival in breast cancer. Oncogene. 2005;24(23):3759–3773. | ||
Mikkelsen T, Brodie C, Finniss S, et al. Radiation sensitization of glioblastoma by cilengitide has unanticipated schedule-dependency. Int J Cancer. 2009;124(11):2719–2727. | ||
Albert JM, Cao C, Ling G, Leavitt L, Hallahan DE, Bo L. Integrin alpha(V)beta(3) antagonist Cilengitide enhances efficacy of radiotherapy in endothelial cell and non-small-cell lung cancer models. Int J Radiat Oncol. 2006;65(5):1536–1543. | ||
Goodman SL, Picard M. Integrins as therapeutic targets. Trends Pharmacol Sci. 2012;33(7):405–412. | ||
Adachi M, Taki T, Higashiyama M, Kohno N, Inufusa H, Miyake M. Significance of integrin alpha5 gene expression as a prognostic factor in node-negative non-small cell lung cancer. Clin Cancer Res. 2000;6(1):96–101. | ||
Valastyan S, Chang A, Benaich N, Reinhardt F, Weinberg RA. Concurrent suppression of integrin alpha5, radixin, and RhoA phenocopies the effects of miR-31 on metastasis. Cancer Res. 2010;70(12):5147–5154. | ||
Cimino D, De Pitta C, Orso F, et al. miR148b is a major coordinator of breast cancer progression in a relapse-associated microRNA signature by targeting ITGA5, ROCK1, PIK3CA, NRAS, and CSF1. FASEB J. 2013;27(3):1223–1235. | ||
Okamura M, Yamaji S, Nagashima Y, et al. Prognostic value of integrin beta1-ILK-pAkt signaling pathway in non-small cell lung cancer. Hum Pathol. 2007;38(7):1081–1091. | ||
Han JY, Kim HS, Lee SH, Park WS, Lee JY, Yoo NJ. Immunohistochemical expression of integrins and extracellular matrix proteins in non-small cell lung cancer: correlation with lymph node metastasis. Lung Cancer. 2003;41(1):65–70. | ||
Wang XM, Li J, Yan MX, et al. Integrative analyses identify osteopontin, LAMB3 and ITGB1 as critical pro-metastatic genes for lung cancer. PLoS One. 2013;8(2):e55714. | ||
Boelens MC, van den Berg A, Vogelzang I, et al. Differential expression and distribution of epithelial adhesion molecules in non-small cell lung cancer and normal bronchus. J Clin Pathol. 2007;60(6):608–614. | ||
Ichiki K, Mitani N, Doki Y, Hara H, Misaki T, Saiki I. Regulation of activator protein-1 activity in the mediastinal lymph node metastasis of lung cancer. Clin Exp Metastasis. 2000;18(7):539–545. | ||
Yan Z, Yin H, Wang R, et al. Overexpression of integrin-linked kinase (ILK) promotes migration and invasion of colorectal cancer cells by inducing epithelial-mesenchymal transition via NF-kappaB signaling. Acta Histochem. 2014;116(3):527–533. | ||
Zhang J, Takahashi K, Takahashi F, et al. Differential osteopontin expression in lung cancer. Cancer Lett. 2001;171(2):215–222. | ||
Shijubo N, Uede T, Kon S, et al. Vascular endothelial growth factor and osteopontin in stage I lung adenocarcinoma. Am J Respir Crit Care Med. 1999;160(4):1269–1273. | ||
Wu DW, Cheng YW, Wang J, Chen CY, Lee H. Paxillin predicts survival and relapse in non-small cell lung cancer by microRNA-218 targeting. Cancer Res. 2010;70(24):10392–10401. | ||
Wu DW, Chen CY, Chu CL, Lee H. Paxillin confers resistance to tyrosine kinase inhibitors in EGFR-mutant lung cancers via modulating BIM and Mcl-1 protein stability. Oncogene. Epub April 27, 2015. | ||
Higashiyama M, Taki T, Ieki Y, et al. Reduced motility related protein-1 (MRP-1/CD9) gene expression as a factor of poor prognosis in non-small cell lung cancer. Cancer Res. 1995;55(24):6040–6044. |
Supplementary materials
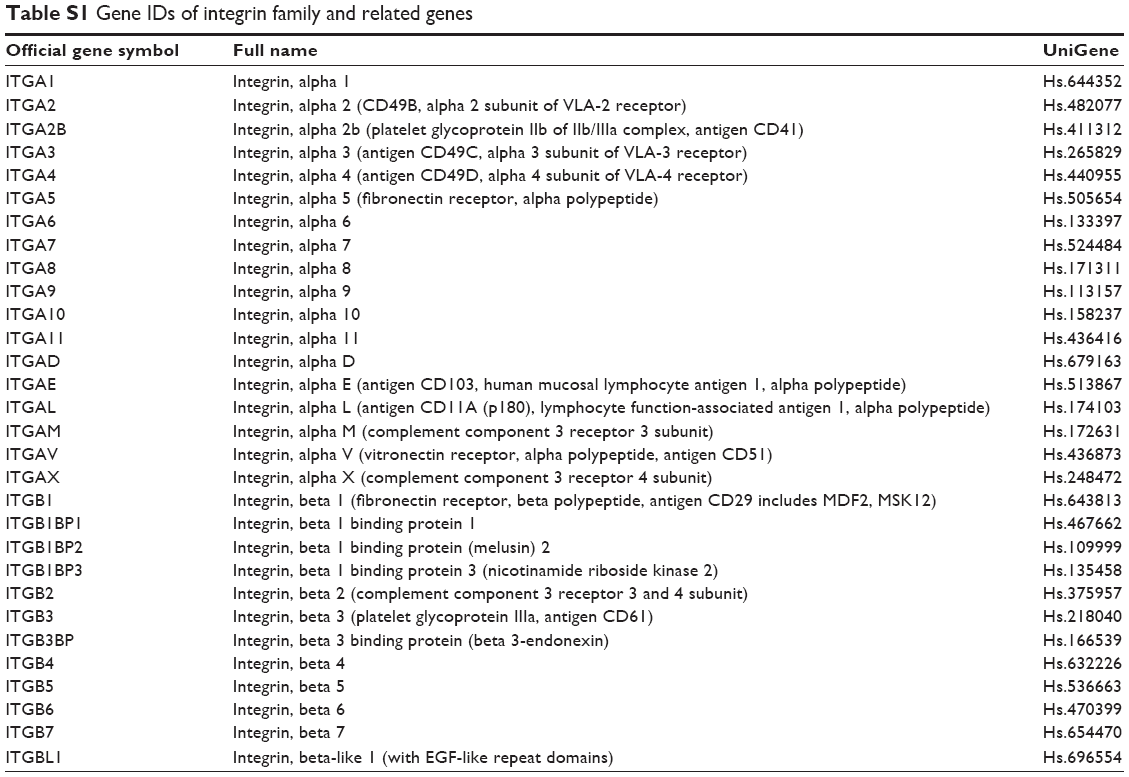 | Table S1 Gene IDs of integrin family and related genes |
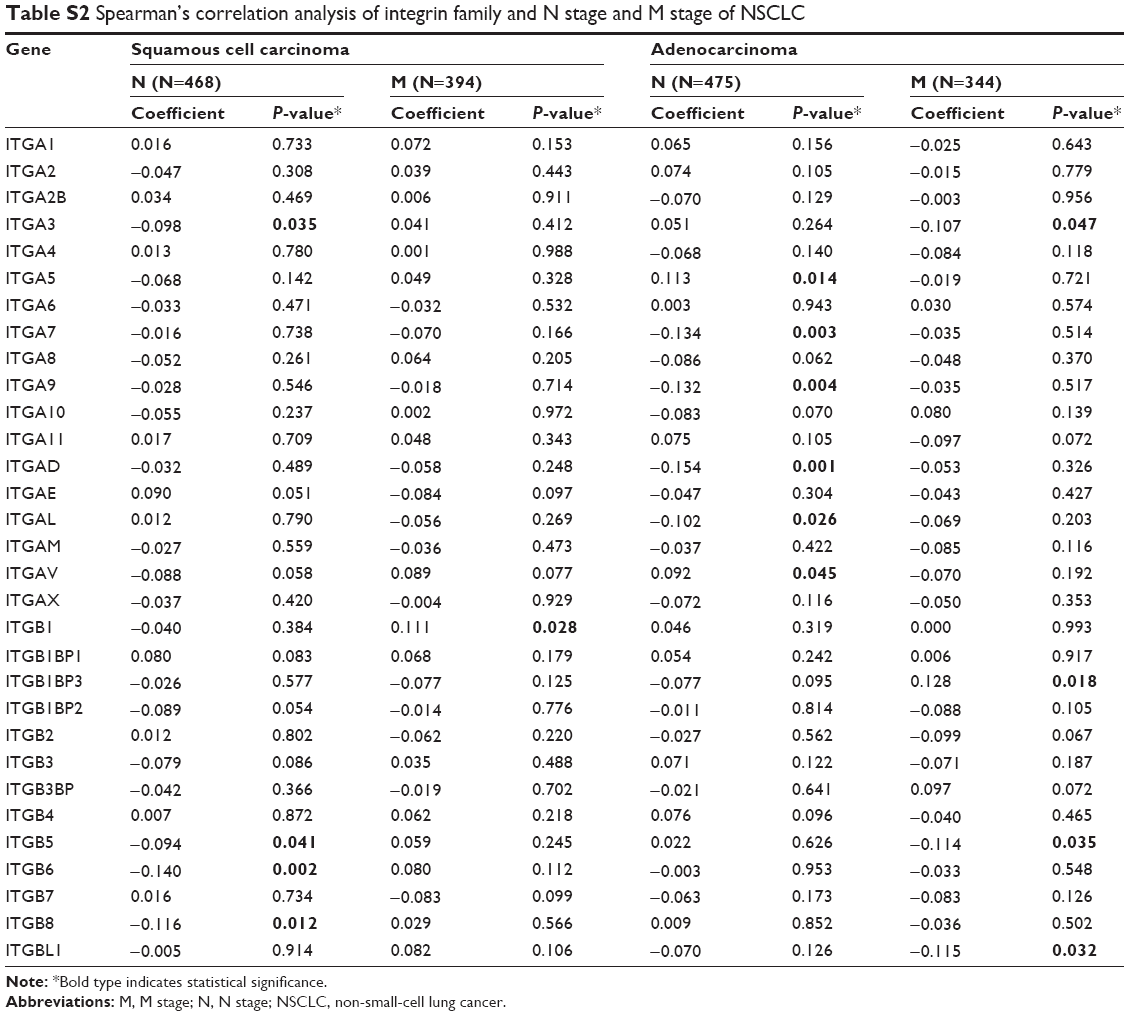 | Table S2 Spearman’s correlation analysis of integrin family and N stage and M stage of NSCLC |
 | Table S3 Gene IDs of ITGA5 and ITGB1 network genes |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.