Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Integrative Management of High-Risk Proliferative Diabetic Retinopathy: Precision Diagnostics via Ultra-Widefield Imaging and Therapeutic Strategies
Received 18 April 2025
Accepted for publication 6 September 2025
Published 12 October 2025 Volume 2025:18 Pages 3813—3832
DOI https://doi.org/10.2147/DMSO.S535338
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Zechen Liu, Jindong Han, Xiaorong Li
Tianjin Key Laboratory of Retinal Functions and Diseases, Tianjin Branch of National Clinical Research Center for Ocular Disease, Eye Institute and School of Optometry, Tianjin Medical University Eye Hospital, Tianjin, People’s Republic of China
Correspondence: Jindong Han, Tianjin Key Laboratory of Retinal Functions and Diseases, Tianjin Branch of National Clinical Research Center for Ocular Disease, Eye Institute and School of Optometry, Tianjin Medical University Eye Hospital, Tianjin, People’s Republic of China, Email [email protected] Xiaorong Li, Tianjin Key Laboratory of Retinal Functions and Diseases, Tianjin Branch of National Clinical Research Center for Ocular Disease, Eye Institute and School of Optometry, Tianjin Medical University Eye Hospital, Tianjin, People’s Republic of China, Email [email protected]
Abstract: Diabetic retinopathy (DR) is a leading cause of blindness worldwide. High-risk proliferative diabetic retinopathy (HR-PDR) is an advanced stage and carries a nearly 50% risk of severe vision loss within five years without intervention. Recent advances in ultra-widefield (UWF) imaging technologies enable comprehensive detection of peripheral lesions and facilitate more accurate diagnosis of disease severity, yet standardized quantitative biomarkers for predicting disease progression remain lacking. Current treatments, including pan-retinal photocoagulation (PRP), anti-vascular endothelial growth factor (anti-VEGF) agents, and pars plana vitrectomy (PPV), demonstrate varying levels of efficacy. There is currently no consensus on the optimal treatment regimen for HR-PDR. Therefore, this review analyzes the application value of UWF imaging in HR-PDR, compares the efficacy of different treatment regimens, and considers their cost-effectiveness and practical applicability meanwhile. Using UWF color fundus photography (CFP) combined with widefield swept-source optical coherence tomography angiography (WF-SS-OCTA) may enhance diagnostic and monitoring outcomes for HR-PDR. Anti-VEGF injections followed PRP could provide stable and sustained protective effects; early PPV may improve outcomes in select cases. Future research should prioritize addressing current research gaps, including the identification of optimal anti-VEGF/PRP protocols, strategies to overcome long-term adherence challenges, establishment of consistent retreatment criteria, clarification of surgical indications, and development of socioeconomic strategies.
Keywords: high-risk proliferative diabetic retinopathy, treatment methods, diagnostic techniques, review
Introduction
Diabetic retinopathy (DR), the primary microvascular complication of diabetes, is a leading cause of vision loss in middle-aged and elderly individuals. Globally, an estimated 160 million individuals were affected by DR in 2020, with projections indicating a rise to 242 million by 2045.1,2 As a progressive microvascular disease, DR is broadly classified into non-proliferative diabetic retinopathy (NPDR) and proliferative diabetic retinopathy (PDR), based on the presence of abnormal neovascularization. PDR is the most advanced stage, caused by severe retinal ischemia resulting from capillary closure. According to the Early Treatment Diabetic Retinopathy Study (ETDRS), high-risk proliferative diabetic retinopathy (HR-PDR) is defined as neovascularization of the disc (NVD) exceeding 1/4 disc area; vitreous or preretinal hemorrhage associated with any NVD; or neovascularization elsewhere (NVE) exceeding 1/2 disc area with vitreous or preretinal hemorrhage.3 Without intervention, nearly 25% of eyes with HR-PDR experience severe vision loss within two years, rising to 44% after four years.4,5 Vision-threatening complications, including vitreous hemorrhage (VH), tractional retinal detachment (TRD), and neovascular glaucoma (NVG), occur more frequently in HR-PDR eyes than in less severe PDR.6,7
Advances in retinal imaging modalities, such as ultra-widefield (UWF) color fundus photography (UWF CFP), UWF fluorescein angiography (UWFFA), and optical coherence tomography angiography (OCTA), have revolutionized HR-PDR diagnosis. UWF imaging captures approximately 110° to 220° of the retina, enabling more comprehensive peripheral lesion detection without pupillary dilation,8 while OCTA provides three-dimensional reconstructions of the microvasculature across all layers and enables quantitative assessment.9 Despite these innovations, their efficiency in diagnosing lesions in HR-PDR has not been reviewed or discussed in the past.
Treatment modalities for HR-PDR include pan-retinal photocoagulation (PRP), anti-vascular endothelial growth factor (anti-VEGF) agents, and pars plana vitrectomy (PPV). PRP is considered the gold-standard for reducing severe visual loss in patients with severe NPDR and PDR.10,11 Anti-VEGF therapy is the first-line option for cases with central-involved diabetic macular edema (CI-DME), while recent studies have confirmed its effects in inhibiting PDR progression and established it as a potential alternative.12 For eyes with significant complications like VH or TRD, PPV is essential but often associated with suboptimal visual outcomes.5,13 Approximately one-third of HR-PDR patients require additional surgery after initial therapy due to recurrent VH or fibrotic traction.14,15
This review is therefore the first to provide a comprehensive overview of the diagnosis and treatment of HR-PDR. The primary aim is to evaluate the diagnostic value of UWF imaging technology in identifying the pathological features of HR-PDR, and to compare the efficacy of current treatment methods based on anatomical and functional outcomes, taking into account treatment safety, cost-effectiveness, and clinical application. The review discusses current research gaps across multiple fields and provides guidance for future translational medicine and clinical research.
Wide-Field Imaging Modalities
UWF CFP
UWF CFP captures up to 200° of fundus in a single image, representing approximately 80% of the total retinal area (Figure 1).16 Previous studies have confirmed moderate to substantial consistency between ETDRS 7-field photographs and UWF CFP in DR severity grading.17,18 Notably, UWF CFP identifies additional peripheral lesions outside the ETDRS 7-field area in approximately one-third of patients, resulting in DR severity upgrades for 10–15% of eyes.19,20 The clinical significance of these peripheral lesions remains controversial in longitudinal studies. Predominantly peripheral lesions (PPLs) on UWF CFP may independently correlate with DR progression;21–23 however, larger prospective cohort studies are needed to validate this association.
 |
Figure 1 Representative 200°UWF CFP overlaid with simulated ETDRS 7-standard 30-degree field images (yellow circles shown). Microaneurysms (red arrow), NVs (red rectangle), and preretinal hemorrhage (red triangle) can be observed in the peripheral retina outside the 7-standard field of view. |
UWF CFP is the preferred imaging modality for rapid screening and diagnosis of HR-PDR. However, UWF CFP exhibits limitations including pseudocolor representation, peripheral distortion, and susceptibility to artifacts from eyelids and lashes that may compromise both image quality and field of view (FOV).16 In addition, it is challenging to differentiate intraretinal microvascular abnormalities (IRMAs) from retinal neovascularization (NVs), and almost impossible to identify retinal non-perfused areas (NPAs).24
UWFFA
Currently, fundus fluorescein angiography (FFA) is still considered the gold standard for detecting and monitoring NVs in retinal vascular diseases. Unlike conventional 30° to 55° FFA, UWFFA imaging system captures up to 200° retinal images in a single acquisition without requiring patient refixation.25 As an effective modality for visualizing subtle vascular pathology, UWFFA enhances dynamic assessment of microaneurysms (MAs), NPAs and leaking NVs (Figure 2). In a comparative analysis by Ying Cui et al, UWFFA demonstrated superior detection rates to UWF CFP for DR lesions, including MAs (97.9% vs 88.2%), IRMA (87.5% vs 44.1%) and NVs (NVE: 56.3% vs 28.9%; NVE+NVD: 75.0% vs 30.0%), although statistical values were not reported.24 The Diabetic Retinopathy Clinical Research (DRCR) Network Protocol AA study further supports UWFFA’s predictive utility for PDR progression through its enhanced identification of PPLs.21,26 Additionally, UWFFA helps to guide targeted laser therapy and personalized retreatment protocols in HR-PDR eyes.25,27
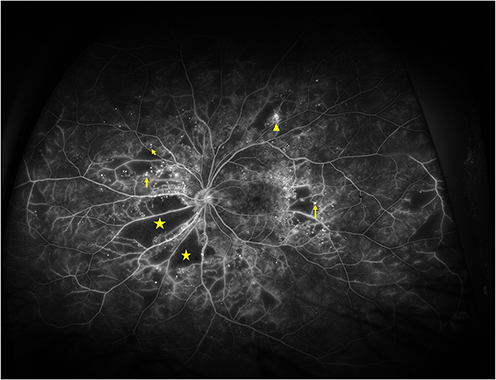 |
Figure 2 Representative UWFFA showing MAs (yellow arrows), leaking NVs (yellow triangle) and NPAs (pentagrams). |
Unfortunately, the invasive nature, prolonged duration, and risk of serious dye-related adverse events limit UWFFA’s adoption in clinical practice. In terms of distinguishing NVs from IRMAs, UWFFA offers no advantage due to its inability to provide depth-resolved retinal segmentation, particularly when compared to OCTA.28 Future studies should establish the correlation between UWFFA-derived quantitative metrics (eg, pan-retinal leakage index and ischemic index) and the risk of DR progression or visual prognosis.29
Wide-Field Swept-Source OCTA (WF-SS-OCTA)
As a noninvasive, safe, and repeatable retinal blood flow imaging system, WF-SS-OCTA has been extensively applied in the diagnosis, screening, and monitoring of HR-PDR. Unlike early OCTA systems limited to macular imaging, WF-SS-OCTA significantly increases the FOV to 50°to 80° or more. This allows visualization of retinal capillary perfusion at the posterior pole and mid-periphery in all retinal layers.30 WF-SS-OCTA has been shown to be superior to UWF CFP and non-inferior to UWFFA in detecting IRMAs, NVs and NPAs in PDR,30–33 even perform better in analyzing quantitative parameters,34 despite a relatively narrower FOV. Regarding MAs, while WF-SS-OCTA can locate their depth, it is less sensitive than FFA due to its relative insensitivity to the slow blood flow.35 In addition, WF-SS-OCTA can be used to evaluate the therapeutic response of PDR eyes to PRP and intravitreal injections of anti-VEGF agents.36
OCT B-scans with overlaid flow signals exhibit high sensitivity in detecting NVs, which can be observed as hyperreflective blood flow structures breaking through the internal limiting membrane (ILM) and projecting into the vitreous (Figure 3).37 The combined vitreoretinal interface (VRI) slab analysis enhances NVs detection rates to 99.1%.38 Meanwhile, the adhesion relationship between the posterior vitreous cortex (PVC) and the retina, known as the type of posterior vitreous detachment (PVD), can also be observed in the structural OCT B-scan (Figure 4).
 |
Figure 3 Representative 24×20 mm UWF SS-OCTA image. (a) Retinal slab shows lesions including MAs (yellow arrows), intraretinal microvascular abnormalities (yellow triangles), NVs (red dashed lines), and NPAs (pentagrams). (b) VRI slab shows abnormal blood vessels growing into the vitreous and appearing above the retina (pink and green lines intersect at a cluster of neovascularization). (c) Corresponding B-scan of the horizontal retinal section shown by green line. NVs with blood flow signals (red) can be observed penetrating through the ILM and extending into the vitreous (pink lines in (b) and (c) corresponded to the same position). |
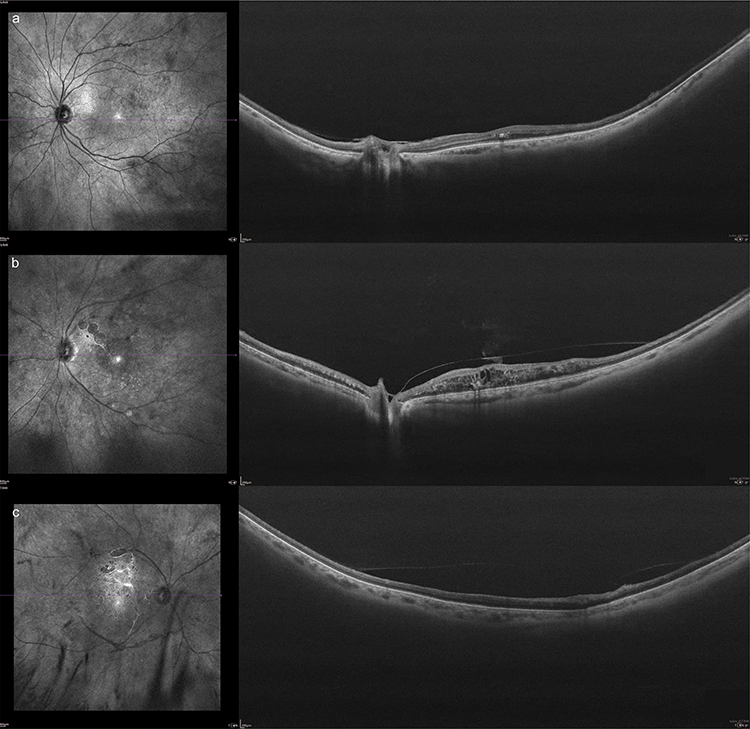 |
Figure 4 Structural OCT B-scan shows the adhesion relationship between the PVC and the retina, known as the type of PVD. Considering the status of the macular and optic disc regions, (a–c) show no PVD, partial PVD, and complete PVD, respectively. |
The currently available research suggests that WF-SS-OCTA could be an alternative to UWFFA (Table 1). Some studies propose that combining WF-SS-OCTA with UWF CFP offers a practical approach for DR diagnosis, monitoring and screening, as UWF CFP could somewhat compensate for the lack of a small FOV and increase the detection of DR lesions.24,39 However, it should be noted that SS-OCTA does not detect leakage, so it may miss some MAs and fibrotic retinal NVs.40 At the same time, a wider FOV means more susceptibility to imaging artifacts and segmentation errors. Quantitative OCTA metrics can vary significantly between different devices or image processing software, and these differences limit meaningful comparisons between studies (Table 2).
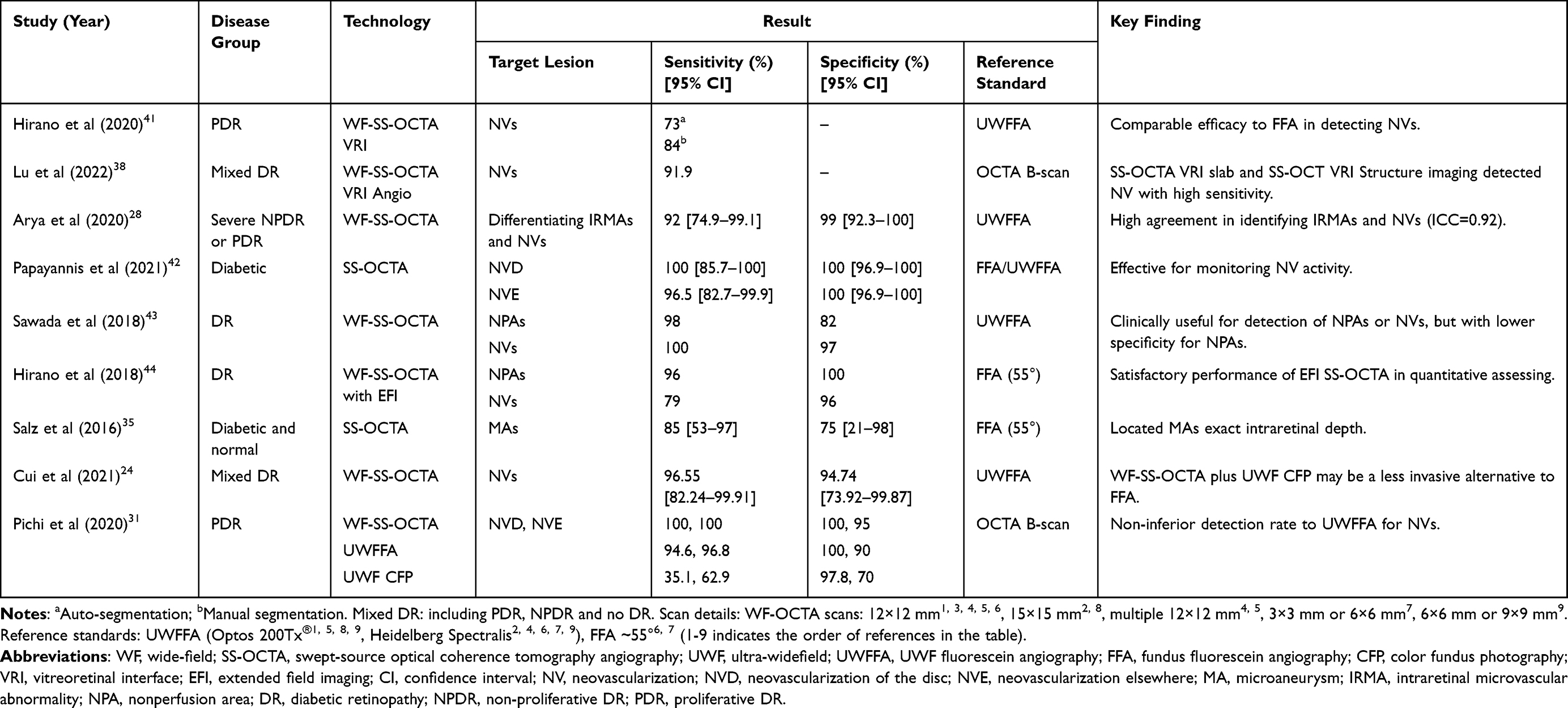 |
Table 1 Comparison of Wide-Field Optical Coherence Tomography Angiography (WF-OCTA) with Reference Standards for Detecting Diabetic Retinopathy Lesions: Sensitivity and Specificity Summary |
 |
Table 2 Summary of Advantages and Disadvantages of UWF CFP, UWF FA, and WF-SS-OCTA |
Treatment Strategies
Pan-Retinal Photocoagulation
Clinical Applications and Effects
Since its introduction in the 1960s, PRP has been considered the mainstay treatment for PDR, effectively preventing severe visual loss in patients with severe NPDR and PDR.10 The precise mechanism through which laser therapy improves retinal vascular disease remains incompletely understood. One possible therapeutic mechanism is that retinal laser permanently destroys retinal pigment epithelial cells and overlying tissue in the peripheral retina. This reduces overall retinal metabolic demand, thereby alleviating the level of retinal hypoxia and downregulating angiogenic factors like VEGF, ultimately mediating NVs regression.47
The Diabetic Retinopathy Study (DRS) demonstrated that without treatment, the risk of severe vision loss in HR-PDR patients within two years is about 25–30%, while prompt PRP treatment can reduce the risk by about 50–60%.48 The ETDRS further demonstrated that early PRP significantly reduces vitrectomy requirements compared to deferred treatment, using either full or mild scatter photocoagulation.49 Approximately 60% of treatment-naive patients exhibit rapid response of abnormal NVs regression, beginning as early as one week after the first PRP treatment and continuing for at least 3 months.50,51 PRP-induced NVs regression is usually stable and persistent, particularly in eyes with initial favorable responses.51 Long-term retrospective studies have confirmed that PRP can provide durable anatomical and visual outcomes for 10 years or even longer in HR-PDR patients.52 Early treatment is superior to delayed treatment. Ohlhausen et al reported that delaying PRP treatment for more than 31 days leads to poorer long-term visual acuity and extended treatment courses than earlier intervention.53 Their findings suggested that the optimal PRP treatment onset time is the day of diagnosis for HR-PDR patients, since these patients achieved superior vision outcomes compared to others at 2-year post-treatment follow-up. Given its definitive and enduring efficacy, PRP remains the cornerstone intervention for PDR.
However, lasers cannot stop the progression of DR completely. Even with adequate PRP treatment, patients remain at risk of vision deterioration, particularly in cases of HR-PDR. At two-year follow-up, approximately 34–37% of treated eyes still developed VH, 10% developed TRD, and 15% underwent PPV.51,54 Nearly one-third of PDR patients necessitate vitrectomy within 10 years post-PRP.55 OCTA follow-up also revealed a tendency of NVs recurrence after 6 months of PRP treatment.50 Trials show that a relatively large portion of PRP-treated eyes (approximately 50%) eventually require supplemental treatment.54,56
Factors associated with PDR worsening are investigated, and the severity of DR at baseline was found to be an independent risk factor.6,57 Ravi Parikh reported that 34.4% of PDR eyes with VH received PPV within two years of initial PRP treatment, which was 2.78 times higher than for PDR alone.58 In addition, eyes treated with pattern or mixed laser modalities exhibit higher progression risk than those receiving single-spot laser, potentially due to the longer stabilization time required.6,57 Consequently, HR-PDR patients require more intensive monitoring and consideration of supplemental laser therapy. No consensus exists, however, regarding optimal treatment initiation timing and interval protocols.
Side Effects and Limitations
Conventional retinal photocoagulation has several potential side effects and limitations. Of note, PRP generally preserves rather than improves vision, and may lead to permanent peripheral visual field loss or exacerbate DME.59 Another possible risk is that initiating PRP therapy may cause a transient angio-fibrotic switch, thereby increasing the likelihood of TRD progression, particularly in eyes with posterior hyaloid shrinkage and preretinal fibrosis.60 To mitigate adverse effects and patient discomfort, complete PRP should be divided into three or four sessions. However, the prolonged completion period increases the risk of hemorrhage during the treatment. If bleeding occurs, blood clots in the vitreous cavity can obstruct the retinal visual field, making adequate PRP more challenging and reducing the effectiveness of laser by absorbing its energy before it reaches the retina. In such cases, one option is to wait for the hemorrhage to resolve or, alternatively, to perform a vitrectomy.
Anti-Vascular Endothelial Growth Factor Injection
Clinical Applications and Effects
Intravitreal injections of anti-VEGF agents are emerging as an alternative therapy for PDR. Anti-VEGF therapy has traditionally been indicated for CI-DME, while recent studies have demonstrated its ability to slow the progression of DR and even improve retinopathy severity scores.61,62 Anti-VEGF drugs primarily exert anti-angiogenic and anti-edematous effects by binding to VEGF-A isoforms, which exhibit the strongest pro-angiogenic activity and increase vascular permeability.63 Rather than removing hemorrhages directly, anti-VEGF therapy targets the underlying pathophysiology, including neovascular regression while facilitating the absorption of accumulated hemorrhages through vascular stabilization, thereby preventing rebleeding.
The Diabetic Retinopathy Clinical Research Network (DRCR.net) Protocol S evaluated the effect of PRP versus intravitreal ranibizumab for PDR eyes (37% of whom were HR-PDR). Results demonstrated that ranibizumab therapy was noninferior to PRP in terms of change in visual acuity at 2 years, along with lower rates of vision-impairing DME, reduced peripheral visual field loss, and fewer vitrectomies.54 Further five-year follow-up maintained similar results and was accompanied by a lower incidence of TRD.64 However, visual field loss progressed in the anti-VEGF treated group, and nearly half of the affected eyes in both groups developed VH within follow-up.14 The PRIDE study confirmed that ranibizumab monotherapy is more effective than PRP alone at reducing NV leakage and area, and provides better visual acuity within 12 months.65 Similarly, the CLARITY trial showed that aflibercept achieved noninferior or superior best corrected visual acuity (BCVA) versus PRP alone at 52 weeks in PDR patients (25% of whom were HR-PDR).56 Moreover, the RECOVERY study reported statistically significant improvement in the progression of DR severity after aflibercept 1-year injection in PDR eyes without DME.61 The studies above seem to indicate that, at least in the short term, anti-VEGF therapy is noninferior to PRP for HR-PDR management.
Disadvantages and Limitations
Intravitreal injections require long-term follow-up, high patient compliance, and relatively high treatment costs. Anti-VEGF induced NVs regression can occur as early as 24 hours post-administration and persist for at least 4 weeks, but recurrence may develop subsequently.66,67 While previous studies indicated that PDR eyes require an average of 4–7 injections in the first year and typically fewer in subsequent years to maintain remission,54,56 no consensus exists regarding the optimal injection frequency and appropriate time to stop safely (if ever). Retrospective data from Wubben et al further indicates that anti-VEGF alone treated patients, particularly HR-PDR, who are unintentionally lost to follow-up (LTFU), face elevated risk of irreversible vision loss caused by NVG or TRD.68,69 This is a real concern, as approximately 25% of PDR patients will be LTFU within 4 years, whether received anti-VEGF or PRP treatment.70 By contrast, PRP generally provides longer-lasting effects with lower treatment burden and may offer an early protection against vision loss in high risk LTFU patients.69,71
The cost differential between anti-VEGF injections and PRP is substantial. Cost-effectiveness analysis indicates that when PRP served as the primary treatment, the 2-year cost per quality-adjusted life years (QALY) was $7988; while when intravitreal ranibizumab was primary treatment, the 2-year cost QALY was $19,150.72 Long-term analysis further confirmed markedly less favorable incremental cost-effectiveness ratios (ICERs) for ranibizumab versus PRP in patients without CI-DME at baseline: $552,268/QALY at 5 years and $742,202/QALY at 10 years. For patients with baseline CI-DME, ICERs were favorable $65,576/QALY at 5 years and $63,930/QALY at 10 years.73 Consequently, anti-VEGFs demonstrate significant cost-effectiveness potential in the treatment of PDR only under specific conditions.74,75 Using bevacizumab as an alternative to ranibizumab and aflibercept could reduce associated incremental costs.74 However, considering drug prices and medical insurance constraints in low- and middle-income countries, PRP retains a cost advantage in resource-limited settings.
Similar to PRP, anti-VEGF therapy cannot fundamentally reverse retinal ischemia or fully address the complex pathophysiology of DR. Anti-VEGF therapy appears to fail to consistently improve retinal perfusion,62 despite occasional reperfusion observations.76 Even with monthly injections, disease progression and visual deterioration remain possible.77,78 Additionally, it is important to be aware that anti-VEGF treatment may accelerate the transition from angiogenic dominance to fibrotic dominance in HR-PDR, contributing to TRD incidence rates ranging from 1.5% to 18.4%.79
Despite its demonstrated efficacy, anti-VEGF monotherapy is not currently recommended as an alternative to PRP for the treatment of PDR due to its uncertainty of long-term benefits compared to PRP, as well as the significant cost burden and elevated risks associated with LTFU. Instead, anti-VEGF therapy is recommended as a temporary adjunct therapy to PRP in PDR management or as a cost-effective intervention for patients with CI-DME requiring vision preservation.68,80 Further research should focus on long-term visual acuity outcomes under anti-VEGFs and PRP, the respective rates of vision-threatening complications, and the impact of nonadherence on final visual prognosis.
PRP Combined with Anti-VEGF Agent
Clinical Applications and Effects
Multiple studies have confirmed that combining PRP and anti-VEGF treatment has a synergistic effect, making it the preferred approach in clinical practice. Anti-VEGF injections reduce the necessary laser energy and volume, thereby alleviating adverse effects such as peripheral vision impairment and DME development. Meanwhile, PRP can have a longer-lasting effect on the regression of NVs, reducing the frequency of required injections and thus lowering long-term costs.
In the PROTEUS study, a 1-year randomized trial focusing exclusively on HR-PDR, Figueira et al demonstrated that PRP combined with ranibizumab three-needle basal therapy was more effective than PRP monotherapy in regressing the total NVs area, but no significant differences in BCVA were observed between two groups at any visits.81 Another 1-year retrospective study reported that three-needle basal conbercept plus PRP therapy achieved a higher rate of NVs resolution, greater BCVA improvement, and lower average central macular thickness (CMT). It also reduced the need for vitrectomy in HR-PDR patients compared to PRP alone.82 Similar results have also been confirmed in PRP combined with other anti-VEGF drugs, such as aflibercept and bevacizumab, in the short-term follow-up of 6 months to 1 year.83,84 Pretreatment with a single anti-VEGF injection before PRP enhances treatment completion rates and patient satisfaction by reducing the incidence of VH, especially in baseline HR-PDR patients.85 Notably, combination therapy achieved the greatest reduction in disease severity grade among HR-PDR patients compared with either anti-VEGF or PRP monotherapy.65 While current evidence consistently supports combination therapy for accelerating NVs regression and improving short-term anatomical structures, its impact on sustained visual acuity gains remains inconsistent.81,86–89 Long-term benefits of combination therapy for HR-PDR beyond one to two years require validation through extended trials.
Recommend Combination Therapy Strategies
The recommended combination regimen prioritizes intravitreal anti-VEGF administration before PRP. The sequence leverages differential therapeutic timelines. As mentioned above, PRP initiates NVs regression as early as 1 week but requires more than 3 weeks for maximal effect, whereas anti-VEGF therapy acts rapidly.67,89 Patients receiving anti-VEGF followed by PRP exhibit lower 5-year rates of PDR complications and PPV requirements compared to those treated with PRP-first sequencing.90 For HR-PDR patients, preemptive anti-VEGF is critical to mitigate VH risk during PRP. Evidence-based protocols recommend administering anti-VEGF injections 1 week prior to PRP and completing in 3–4 sessions over 2 months (2-week intervals each time).84,85 Increasing the loading doses may function in improving retinal structure, but no further visual function enhancement was achieved.84 For patients with DME at baseline, three monthly anti-VEGF loading doses during PRP are strongly recommended.81,91 Economically, single-dose is much more acceptable than triple-dose in clinical practice. Significant knowledge gaps remain regarding the optimal anti-VEGF dosage during PRP treatment and personalized maintenance strategies for HR-PDR patients with different clinical phenotypes.
Pars Plana Vitrectomy
Clinical Applications and Effects
The traditional indications for PPV in eyes with PDR include non-resolving or recurrent visually impairing VH and/or tractional retinal complications threatening or involving the macula.92 By mechanically removing vitreous opacities, fibrovascular membranes, and PVCs, vitrectomy achieves earlier visual benefits and effectively releases macula-threatening traction factors by reducing both tangential and antero-posterior traction forces.93 Successful vitrectomy also induces a long-term reduction in VEGF levels, shifting the intraocular environment towards an anti-angiogenic state and partially alleviating the progression of retinopathy.94,95
Recent advances in surgical instrumentation and vitrectomy techniques have expanded the indications for PPV, prompting retinal specialists to intervene earlier in the disease course. In eyes with advanced PDR, postoperative anatomical success rates reached 87% to 98%; however, visual acuity improvement remained limited (ranging from approximately 0.68logMAR to 1.4logMAR), with an elevated risk of adverse events including visual instability and recurrent retinal detachment.96–99 Several studies suggest that early surgical intervention for HR-PDR patients, with or without VH, is a potential option to improve long-term visual outcomes and minimize treatment burden. The landmark Diabetic Retinopathy Vitrectomy Study (DRVS) first demonstrated this benefit in PDR eyes with useful vision (BCVA≥10/200) and active, extensive NVs or fibrovascular proliferations. Within 4 years, the early vitrectomy group achieved superior visual outcomes compared to conventional management, with no increased risk of complications.13 Similarly, a recent study found that pre-emptive vitrectomy was safe and effective in eyes with extensive, persistent, non-fibrotic retinal neovascularization and good baseline vision (BCVA≥20/50). These eyes maintained stable visual outcomes at approximately 0.15logMAR through the 12-month follow-up period.100 This result significantly outperforms visual outcomes typically achieved with PPV for advanced PDR, where postoperative vision is frequently compromised by fibrotic complications and macular edema. However, the benefits of early vitrectomy appear to increase with greater baseline neovascular severity and poorer baseline visual acuity.101 An eight-year real-world study demonstrated the advantages of PPV over conventional treatment in terms of long-term visual improvement and reduced reoperation rates, particularly in patients under the age of 50, although the study included eyes with complications.102 In addition, Elhamid103 and Antoszyk104 confirmed that early vitrectomy accelerates visual recovery and reduces the likelihood of recurrent VH and TRD compared to anti-VEGF monotherapy or anti-VEGF/PRP combination therapy. This therapeutic advantage may stem from the fact that PPV can directly remove tractional forces on residual neovascular complexes.
The economic benefits of early PPV are also noteworthy. Cost-utility analyses from Protocol S demonstrated that early PPV was as cost-effective as PRP for treating PDR eyes without DME, both within the initial 2 years and over a lifetime. In contrast, the cost-effectiveness gap between anti-VEGF therapy and early PPV widened significantly over time, from 2.4 to 3 times in the first 2 years, to 5.3 to 10.8 times cost/QALY in lifetime.105 Cost-analysis from Protocol AB revealed that PPV plus PRP-first strategy saves approximately half therapeutic cost compared to aflibercept-first strategy for managing non-clearing VH in PDR patients over 104 weeks.106
Effects of Posterior Vitreous Detachment and Age
Evidence indicates that the progression of DR is influenced by the status of the PVD. Vitreoretinal adhesion constitutes a crucial factor mediating the development of retinal NVs.107 Current consensus states that partial PVD is a characteristic vitreous alteration in PDR and a predisposing factor for disease progression, whereas complete PVD represents a strong negative risk factor.107–109 A retrospective study of 403 eyes with DR found that eyes with partial PVD or no PVD exhibited significantly higher progression rates over 3 years compared to those with complete PVD. Notably, eyes exhibiting partial PVD with thickened PVC approached a progression rate of nearly 100%.107 Additionally, studies have reported that younger PDR patients present with more severe disease manifestations, including a heightened risk of visual loss and TRD, compared to older patients, irrespective of prior PRP therapy.102,110 This disparity may be attributed to the prevalence of firm peripheral vitreoretinal adhesion and active, extensive fibrovascular proliferation at the vitreoretinal interface in younger PDR cohorts.
Complications
The primary concern regarding early vitrectomy is the high incidence of postoperative complications. Previous studies have established postoperative vitreous cavity hemorrhage (POVCH) as a well-recognized complication, with reported incidence rates ranging from 12% to 40%.100,103,111,112 Elevated VEGF levels at the time of initial vitrectomy constitute an independent risk factor for POVCH development.111,112 Early POVCH (<4 weeks) is primarily associated with lysis of residual blood clots in the peripheral vitreous skirt, persistent hemorrhage from fragile vessels transected during surgery, and incomplete removal of fibrovascular tissue.113 Conversely, late POVCH (>4 weeks) is predominantly caused by neovascularization growth at the entry sites and recurrence on the retinal surface, driven by sustained intraocular VEGF overproduction following surgery.112 Therefore, meticulous surgical technique is important, emphasizing the complete removal of vitreous surrounding the entry sites, fibrovascular membranes and vitreous cortex. Furthermore, patients need to be counseled preoperatively regarding the risk of transient visual impairment in the early postoperative period and the potential necessity for secondary surgery before long-term visual stability is achieved.100
Cataract formation is another highly prevalent complication following vitrectomy. A large retrospective study reported that nearly 50% of phakic eyes undergoing PPV alone developed cataracts within 6 months postoperatively.114 Similarly, Ben et al demonstrated that all phakic eyes developed cataracts requiring surgery at 4-year follow-up after comparing PPV alone and PPV combined with phacoemulsification for the treatment of PDR eyes.115 While combined surgery significantly enhances intraoperative visualization of anterior vitreous structures, facilitating more thorough PRP and vitreous removal, it also prolongs the operative duration and increases the risk of anterior chamber instability, corneal edema, and postoperative NVG. Therefore, although combined surgery may be a suitable approach for PDR patients with significant pre-existing cataracts, the substantial risk of NVG development necessitates careful consideration.
NVG following vitrectomy in PDR patients is the most severe complication, portending a poor visual prognosis, with reported incidence rates ranging from approximately 2% to 15%.110,116 Main risk factors identified include younger age, elevated preoperative intraocular pressure, uncontrolled diabetes mellitus, absence of prior PRP, postoperative VH, and undergoing combined cataract extraction with vitrectomy.116–118 Postoperative anti-VEGF injections appear to protect against NVG occurrence.119
Summary and Limitations
Overall, vitrectomy is considered to be a cost-effective and durable therapeutic approach for PDR. When considering early PPV for eyes with HR-PDR, critical issues to focus on include whether to combine cataract surgery and how to reduce perioperative complications. The status of the PVD and patients’ age are essential considerations in the decision-making process. Eyes exhibiting partial or absent PVD, particularly in younger individuals with advanced disease, may derive significant benefit from early vitrectomy with complete hyaloid removal, coupled with extensive intraoperative anti-proliferative photocoagulation.102
However, a standardized definition of “early” intervention and the optimal time to perform vitrectomy remain undefined. Current available studies predominantly use BCVA, fundus lesion characteristics, or duration of VH as indicators for early surgical intervention. Some authors propose performing vitrectomy if persistent VH shows inadequate absorption after 4–6 weeks; nevertheless, there is no standardized consensus. Current recommendations for early vitrectomy are largely based on retrospective studies with low levels of evidence. Further prospective, high-quality research is imperative to establish definitive surgical timing criteria and evaluate long-term prognosis.
PPV Combined with Anti-VEGF Agents and/or PRP
PPV Combined with PRP
Preoperative or intraoperative PRP reduces the incidence of POVCH in eyes with PDR, potentially mediated by decreased vitreous VEGF concentration and accelerated regression of NVs.15,120,121 Intraoperative PRP can be delivered more anteriorly than that performed with a slit lamp. The DRCR.net Protocol AB study demonstrated that PPV combined with intraoperative PRP achieved superior early visual acuity gains compared to anti-VEGF monotherapy, although long-term benefits at 24 weeks were not significant.104 For HR-PDR patients presenting with VH, combined vitrectomy and concurrent intraoperative laser may obviate the need for preoperative PRP, potentially reducing surgical waiting times, follow-up burden, and low-vision related costs.122 Notably, the DRVS group did not advocate vitrectomy as an alternative to photocoagulation, but rather as an adjunctive intervention for severe complications following PRP or when preoperative PRP is unfeasible.13
PPV Combined with Anti-VEGF Agents
Perioperative injection of anti-VEGF is widely considered as a necessary adjunctive therapy to minimize intraoperative and postoperative complications and maximize surgical outcomes. By effectively reducing intravitreal VEGF levels, preoperative anti-VEGF injections induce NVs regression and facilitate surgical procedures such as the dissection of fibrovascular membranes.123 Meta-analyses confirm that preoperative anti-VEGF treatment reduces intraoperative bleeding, shortens surgery duration, and decreases complication rates, including intraoperative iatrogenic retinal breaks and POVCH.124–126 Reinjection at PPV conclusion replenishes the drug eliminated during vitrectomy, mitigates pharmacokinetic-related efficacy loss, and further reduces the likelihood of POVCH associated with postoperative VEGF surge.112,127,128 Further, perioperative anti-VEGF injection is associated with a slight improvement in postoperative BCVA.125–127,129 Given the transient intravitreal VEGF suppression achieved (approximately 4 weeks) with current anti-VEGF agents,130 adequate preoperative or intraoperative PRP remains crucial to prevent NVs recurrence and ensure long-term stability.
However, the optimal interval between preoperative intravitreal anti-VEGF injection and vitrectomy remains contentious. Theoretically, vitrectomy should be performed after significant NVs regression but before fibrovascular complex constriction exacerbates the progression of TRD.113 Russo et al reported that longer injection-to-surgery intervals significantly increased the risk of macular traction, and it is relatively safe to perform surgery within 10 days after injection.131 EI-Sabagh et al found that the pan-endothelial marker CD34, expressed in neovascular vessels, showed no significant decrease until day 5 post-injection, indicating that too early surgical intervention may be insufficient for NVs regression.132 Their findings also revealed marked reduction in the proliferative vascular component without significant contractile component accumulation around day 10, potentially defining an optimal window. Additional evidence suggests that a preoperative interval of 6 to 14 days may maximize efficacy in improving postoperative BCVA, reducing surgery time, and minimizing recurrent VH incidence.126 While higher anti-VEGF doses may reduce the severity and incidence of early POVCH without increasing the risk of other complications, supporting evidence is limited.133 Further randomized prospective trials are needed to explore the optimal timing and dosing regimens for specific anti-VEGF agents.
Barriers to Clinical Application in Real-World
Early detection of microvascular abnormalities and prompt intervention can prevent severe visual impairment in DR. However, patients often present with poor vision and already meet the diagnostic criteria for HR-PDR at their initial visit. Large-scale systematic DR screening programs for all diabetes patients enable earlier detection and intervention, but significant infrastructure investment and time requirements limit implementation, particularly in middle- and low-income regions.134,135 Vacancies and uneven distribution of experts hinder the application of techniques. While UWF imaging technology offers potential advantages in DR screening and management, it may be costly and unsuitable for remote areas. Advances in artificial intelligence (AI), deep learning algorithms, and telemedicine are expected to enable personalized, automated real-time medicine, potentially bridging the current gap.135–137
The relatively low cost and long-term efficacy of PRP contribute to its accessibility. Conversely, the extensive application of anti-VEGF therapy in PDR patients without CI-DME is constrained by frequent administration, intensive follow-up, suboptimal cost-effectiveness, uncertain long-term effectiveness, and potential ocular or systemic adverse events.138,139 Although evidence suggests comparable effectiveness among different anti-VEGF agents, real-world variations in individual patient sensitivity exist. Additionally, extended and uncertain treatment regimens can lead to patient fatigue. When combined with treatment non-compliance due to regulatory hurdles (eg, reimbursement limitations), the risk of vision-threatening complications increases, often leading to unsatisfactory long-term outcomes. In addition, early surgical intervention is often poorly accepted for specific high-risk patients despite good baseline vision. Supporting evidence is currently insufficient, and further exploratory studies focusing on long-term visual acuity and complication risks are required.
While emerging novel imaging and treatment modalities hold significant potential to improve DR clinical outcomes, equitable global implementation of these advances across both high- and low-resource settings is imperative.
Current Limitations and Future Perspectives
Application of UWF Imaging Technology
UWF imaging can detect a great number of PPLs in patients with DR. However, its impact on predicting visual impairment and disease progression remains insufficiently characterized. While the assessment of quantitative metrics derived from multimodal UWF imaging, particularly OCTA parameters, has been extensively investigated, data comparability across different devices is limited by the absence of standardized acquisition and analysis protocols established by international consensus.45 Furthermore, reliable evidence linking these imaging biomarkers to DR progression and long-term visual outcomes is currently lacking. Future research should prioritize establishing the sensitivity and specificity of quantitative UWF and OCTA metrics for predicting visual decline and disease progression. Additionally, the significant biases introduced by imaging artifacts highlight the critical need for research dedicated to optimizing image acquisition techniques and developing advanced artifact correction algorithms.140
Research Limitations and Gaps
The current body of evidence is constrained by several limitations, including short study durations, small sample sizes, significant LTFU, and inconsistent inclusion criteria. Most existing studies are retrospective, with follow-up periods typically limited to 6–12 months, and often fail to report crucial details regarding DM duration and systemic control, which are factors known to profoundly influence treatment efficacy and disease prognosis. To address these limitations, prospective, large-scale, randomized controlled trials (RCTs) with extended follow-up periods (>5 years) and rigorous documentation of baseline DM characteristics are essential for generating reliable comparative prognostic data.
Diabetic patients frequently experience high LTFU rates due to barriers in accessing ophthalmic care. Reported LTFU rates in RCTs range from 15% over 2 years to 45% over 5 years, with real-world data suggesting even higher rates in clinical practice.141 Potential adverse consequences of inadequate follow-up, especially for patients with HR-PDR, remain poorly understood. Moreover, cost-effectiveness analyses of different treatments often fail to incorporate the significant impact of poor patient adherence. Future high-quality studies should focus on identifying patients at high risk for LTFU using predictive models and developing targeted interventions (eg, telemedicine monitoring, patient education programs, integrated care pathways) to improve retention and reduce vision loss. Although challenging to obtain, incorporating real-world adherence data and LTFU outcomes is essential for improving the practical applicability of research findings.
Treatment Strategies and Options
A definitive consensus on the optimal management strategy for HR-PDR patients is currently lacking. Prompt PRP remains the standard initial intervention for HR-PDR patients with a clear fundus view;10,11 however, the timing and efficacy of supplemental laser is inconclusive. When anti-VEGF agents serve as the primary therapy, a regimen of three initial loading doses followed by a pro re nata (PRN) approach is commonly employed. Nevertheless, evidence supporting individualized dosing strategies, criteria for treatment cessation, and long-term outcomes with anti-VEGF monotherapy requires further clarification. Similarly, when anti-VEGF agents are used alongside vitrectomy to reduce perioperative complications, standardized protocols regarding agent selection, dosage, optimal timing, and postoperative regimen are yet to be firmly established.
Clinical guidelines recommend early PPV for PDR patients with dense, non-clearing VH.11,142,143 However, the definitions of “early” versus “late” intervention remain ambiguous. Performing vitrectomy too early carries a risk of overtreatment in patients with potential for spontaneous hemorrhage resolution, while delaying surgery risks irreversible complications like TRD. Key unresolved questions include: 1) Which patient subgroups benefit most from early PPV? 2) How should postoperative complications, such as POVCH, be managed – with observation, injection of anti-VEGF, or prompt secondary surgery? Future research must address these critical knowledge gaps through well-designed comparative studies and the development of evidence-based algorithms.
Summary and Conclusion
In summary, this review summarizes the diagnostic utility of UWF imaging in HR-PDR and analyzes comparative treatment outcomes, emphasizing the influence of patient adherence and cost-effectiveness on therapeutic selection. Unlike existing literature focused on isolated treatment modalities or imaging techniques, this review distinctively bridges the gap between technological innovation, clinical decision-making, and healthcare system implementation in managing HR-PDR. Key limitations include its limited focus on DME management, exclusion of anti-inflammatory treatment modalities, and potential selection bias caused by variable inclusion criteria across referenced studies (eg, incorporation of NPDR cases or concomitant TRD).
UWF imaging has great potential to reshape HR-PDR screening and management. The noninvasive, rapid, and reproducible nature of combined UWF CFP and WF-SS-OCTA supports their utility in HR-PDR diagnosis and monitoring (GRADE 2C: low-quality evidence, weak recommendation).30,39,144 While conventional and ultra-widefield FFA remain indispensable for detecting vascular leakage, their invasive nature and potential adverse effects necessitate judicious clinical application.
Timely intervention is imperative for HR-PDR due to the high risk of vision-threatening complications associated with delayed treatment. Although anti-VEGF monotherapy can effectively induce neovascular regression and improve visual and anatomical outcomes, the necessity of PRP should be emphasized, particularly for patients with high LTFU risk or limited financial resources.145 Anti-VEGF therapy and PRP can be performed concurrently in HR-PDR, but long-term visual benefits require further validation in RCTs.11 For individuals with persistent VH, early vitrectomy with intraoperative PRP is recommended (GRADE 1B: moderate-quality evidence, strong recommendation),13,100,103,142–144 and perioperative injection of anti-VEGF can reduce the incidence of intraoperative bleeding and early postoperative VH (GRADE 1B: moderate-quality evidence, strong recommendation).125,129,144 Blood glucose control is the cornerstone of managing all patients with HR-PDR, and is crucial for the success of any ocular intervention and the prevention of further progression or recurrence. Strict adherence to diabetes management guidelines, including medication, diet, and lifestyle modifications, is essential to stabilize retinal vascular structure and reduce systemic factors that drive neovascularization. Real-world treatment selection should balance issues of efficacy, safety, cost, adherence, ocular and systemic factors, with the understanding that poor metabolic control can undermine the effectiveness of local therapies.
Abbreviations
DR, diabetic retinopathy; HR-PDR, high-risk proliferative diabetic retinopathy; PRP, pan-retinal photocoagulation; VEGF, vascular endothelial growth factor; PPV, pars plana vitrectomy; NVD, neovascularization of the disc; NVE, neovascularization elsewhere; UWF CFP, ultra-widefield color fundus photography; UWFFA, ultra-widefield fluorescein angiography; FFA, fundus fluorescein angiography; WF-SS-OCTA, wide-field swept-source optical coherence tomography angiography; CI-DME, central-involved diabetic macular edema; VH, vitreous hemorrhage; TRD, tractional retinal detachment; IRMA, intraretinal microvascular abnormalities; NPAs, non-perfused areas; VRI, vitreoretinal interface; ILM, internal limiting membrane; PVC, posterior vitreous cortex; PVD, posterior vitreous detachment; BCVA, best corrected visual acuity; POVCH, post-operative vitreous cavity hemorrhage; GRADE, Grading of Recommendations Assessment, Development and Evaluation.
Informed Consent
There are no human participants in this article and informed consent is not required.
Funding
Funded by Tianjin Key Medical Discipline Construction Project (TJYXZDXK-3-004A-2).
Disclosure
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Teo ZL, Tham YC, Yu M, et al. Global prevalence of diabetic retinopathy and projection of burden through 2045: systematic review and meta-analysis. Ophthalmology. 2021;128(11):1580–1591. doi:10.1016/j.ophtha.2021.04.027
2. Burton MJ, Ramke J, Marques AP, et al. The lancet global health commission on global eye health: vision beyond 2020. Lancet Glob Health. 2021;9(4):e489–e551. doi:10.1016/S2214-109X(20)30488-5
3. Early Treatment Diabetic Retinopathy Study Research Group. Fundus photographic risk factors for progression of diabetic retinopathy: ETDRS report number 12. Ophthalmology. 1991;98(5 Suppl):823–833.
4. Diabetic Retinopathy Study Research Group. Preliminary report on effects of photocoagulation therapy. Am J Ophthalmol. 2018;185:14–24. doi:10.1016/j.ajo.2017.11.010
5. Indications for photocoagulation treatment of diabetic retinopathy: diabetic Retinopathy Study Report no. 14. The Diabetic Retinopathy Study Research Group - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/2447027/.
6. Bressler SB, Beaulieu WT, Glassman AR, et al. Factors associated with worsening proliferative diabetic retinopathy in eyes treated with panretinal photocoagulation or ranibizumab. Ophthalmology. 2017;124(4):431–439. doi:10.1016/j.ophtha.2016.12.005
7. Baek SU, Park MS, Cho BJ, Park IW, Kwon S. Risk factors associated with progression of diabetic retinopathy in eyes treated with panretinal photocoagulation. Sci Rep. 2021;11(1):13850. doi:10.1038/s41598-021-93384-5
8. Patel SN, Shi A, Wibbelsman TD, Klufas MA. Ultra-widefield retinal imaging: an update on recent advances. Ther Adv Ophthalmol. 2020;12:2515841419899495. doi:10.1177/2515841419899495
9. Waheed NK, Rosen RB, Jia Y, et al. Optical coherence tomography angiography in diabetic retinopathy. Prog Retin Eye Res. 2023;97:101206. doi:10.1016/j.preteyeres.2023.101206
10. Chinese Medical Association Ophthalmology Branch Retinal Disease Group, Chinese Medical Doctor Association Ophthalmology Branch Retinal Disease Group. Clinical diagnosis and treatment guidelines for diabetic retinopathy in China (2022). Chin J Retinal Dis. 2023;39(02):99–124. doi:10.3760/cma.j.cn511434-20230110-00018
11. Flaxel CJ, Adelman RA, Bailey ST, et al. Diabetic retinopathy preferred practice pattern®. Ophthalmology. 2020;127(1):P66–P145. doi:10.1016/j.ophtha.2019.09.025
12. Gunasekaran T, Gunasekaran Y, Tze Hui P. Review of studies comparing panretinal photocoagulation and anti-vascular endothelial growth factor therapy in the treatment of proliferative diabetic retinopathy. Cureus. 2022;14(2):e22471. doi:10.7759/cureus.22471
13. The Diabetic Retinopathy Vitrectomy Study Research Group. Early vitrectomy for severe proliferative diabetic retinopathy in eyes with useful vision: results of a randomized trial--diabetic retinopathy vitrectomy study report 3. Ophthalmology. 1988;95(10):1307–1320. doi:10.1016/s0161-6420(88)33015-0
14. Gross JG, Glassman AR, Liu D, et al. Five-year outcomes of panretinal photocoagulation vs intravitreous ranibizumab for proliferative diabetic retinopathy: a randomized clinical trial. JAMA Ophthalmol. 2018;136(10):1138–1148. doi:10.1001/jamaophthalmol.2018.3255
15. Baget-Bernaldiz M, Romero-Aroca P, Mira-Puerto A, et al. Risk factors for recurrent vitreous hemorrhage in type 2 diabetes mellitus patients after posterior vitrectomy. J Clin Med. 2023;12(8):2989. doi:10.3390/jcm12082989
16. Byberg S, Vistisen D, Diaz L, et al. Optos wide-field imaging versus conventional camera imaging in Danish patients with type 2 diabetes. Acta Ophthalmol. 2019;97(8):815–820. doi:10.1111/aos.14118
17. Aiello LP, Blodi B, Gao X, et al. Ultra-widefield and early treatment diabetic retinopathy study 7-field grading of diabetic retinopathy. JAMA Ophthalmol. 2024;142(9):856–863. doi:10.1001/jamaophthalmol.2024.2890
18. Aiello LP, Odia I, Glassman AR, et al. Comparison of Early Treatment Diabetic Retinopathy Study Standard 7-Field Imaging With Ultrawide-Field Imaging for Determining Severity of Diabetic Retinopathy. JAMA Ophthalmol. 2019;137(1):65–73. doi:10.1001/jamaophthalmol.2018.4982
19. Price LD, Au S, Chong NV. Optomap ultrawide field imaging identifies additional retinal abnormalities in patients with diabetic retinopathy. Clin Ophthalmol. 2015;9:527–531. doi:10.2147/OPTH.S79448
20. Silva PS, Cavallerano JD, Sun JK, Soliman AZ, Aiello LM, Aiello LP. Peripheral lesions identified by mydriatic ultrawide field imaging: distribution and potential impact on diabetic retinopathy severity. Ophthalmology. 2013;120(12):2587–2595. doi:10.1016/j.ophtha.2013.05.004
21. Marcus DM, Silva PS, Liu D, et al. Association of predominantly peripheral lesions on ultra-widefield imaging and the risk of diabetic retinopathy worsening over time. JAMA Ophthalmol. 2022;140(10):946–954. doi:10.1001/jamaophthalmol.2022.3131
22. Silva PS, Cavallerano JD, Haddad NMN, et al. Peripheral lesions identified on ultrawide field imaging predict increased risk of diabetic retinopathy progression over 4 years. Ophthalmology. 2015;122(5):949–956. doi:10.1016/j.ophtha.2015.01.008
23. Sadda SR, Nittala MG, Taweebanjongsin W, et al. Quantitative assessment of the severity of diabetic retinopathy. Am J Ophthalmol. 2020;218:342–352. doi:10.1016/j.ajo.2020.05.021
24. Cui Y, Zhu Y, Wang JC, et al. Comparison of widefield swept-source optical coherence tomography angiography with ultra-widefield colour fundus photography and fluorescein angiography for detection of lesions in diabetic retinopathy. Br J Ophthalmol. 2021;105(4):577–581. doi:10.1136/bjophthalmol-2020-316245
25. Wessel MM, Aaker GD, Parlitsis G, Cho M, D’Amico DJ, Kiss S. Ultra-wide-field angiography improves the detection and classification of diabetic retinopathy. Retina. 2012;32(4):785–791. doi:10.1097/IAE.0b013e3182278b64
26. Silva PS, Marcus DM, Liu D, et al. Association of ultra-widefield fluorescein angiography-identified retinal nonperfusion and the risk of diabetic retinopathy worsening over time. JAMA Ophthalmol. 2022;140(10):936–945. doi:10.1001/jamaophthalmol.2022.3130
27. Cai S, Liu TYA. The role of ultra-widefield fundus imaging and fluorescein angiography in diagnosis and treatment of diabetic retinopathy. Curr Diab Rep. 2021;21(9):30. doi:10.1007/s11892-021-01398-0
28. Arya M, Sorour O, Chaudhri J, et al. Distinguishing intraretinal microvascular abnormalities from retinal neovascularization using optical coherence tomography angiography. Retina. 2020;40(9):1686–1695. doi:10.1097/IAE.0000000000002671
29. Ehlers JP, Jiang AC, Boss JD, et al. Quantitative ultra-widefield angiography and diabetic retinopathy severity: an assessment of panretinal leakage index, ischemic index and microaneurysm count. Ophthalmology. 2019;126(11):1527–1532. doi:10.1016/j.ophtha.2019.05.034
30. Wang M, Garg I, Miller JB. Wide field swept source optical coherence tomography angiography for the evaluation of proliferative diabetic retinopathy and associated lesions: a review. Semin Ophthalmol. 2021;36(4):162–167. doi:10.1080/08820538.2021.1887901
31. Pichi F, Smith SD, Abboud EB, et al. Wide-field optical coherence tomography angiography for the detection of proliferative diabetic retinopathy. Graefes Arch Clin Exp Ophthalmol. 2020;258(9):1901–1909. doi:10.1007/s00417-020-04773-x
32. Khalid H, Schwartz R, Nicholson L, et al. Widefield optical coherence tomography angiography for early detection and objective evaluation of proliferative diabetic retinopathy. Br J Ophthalmol. 2021;105(1):118–123. doi:10.1136/bjophthalmol-2019-315365
33. Parameswarappa DC, Langstang AJ, Kavya S, Mohamed A, Stewart MW, Rani PK. The role of widefield optical coherence tomography angiography in assessing the severity of diabetic retinopathy. Ophthalmol Ther. 2024;13(9):2369–2380. doi:10.1007/s40123-024-00995-y
34. Shah PN, Mishra DK, Falahat P, et al. Inter-rater reliability of proliferative diabetic retinopathy assessment on wide-field OCT-angiography and fluorescein angiography. Transl Vis Sci Technol. 2023;12(7):13. doi:10.1167/tvst.12.7.13
35. Salz DA, de Carlo TE, Adhi M, et al. Select features of diabetic retinopathy on swept-source optical coherence tomographic angiography compared with fluorescein angiography and normal eyes. JAMA Ophthalmol. 2016;134(6):644–650. doi:10.1001/jamaophthalmol.2016.0600
36. Couturier A, Rey PA, Erginay A, et al. Widefield OCT-angiography and fluorescein angiography assessments of nonperfusion in diabetic retinopathy and edema treated with anti-vascular endothelial growth factor. Ophthalmology. 2019;126(12):1685–1694. doi:10.1016/j.ophtha.2019.06.022
37. Early sign of retinal neovascularization evolution in diabetic retinopathy: a longitudinal OCT angiography study - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/37868804/.
38. Lu ES, Cui Y, Le R, et al. Detection of neovascularisation in the vitreoretinal interface slab using widefield swept-source optical coherence tomography angiography in diabetic retinopathy. Br J Ophthalmol. 2022;106(4):534–539. doi:10.1136/bjophthalmol-2020-317983
39. Ultra-widefield color fundus photography combined with high-speed ultra-widefield swept-source optical coherence tomography angiography for non-invasive detection of lesions in diabetic retinopathy - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/36408020/.
40. Nouri H, Abtahi SH, Mazloumi M, Samadikhadem S, Arevalo JF, Ahmadieh H. Optical coherence tomography angiography in diabetic retinopathy: a major review. Surv Ophthalmol. 2024;69(4):558–574. doi:10.1016/j.survophthal.2024.03.004
41. Hirano T, Hoshiyama K, Hirabayashi K, et al. Vitreoretinal interface slab in OCT angiography for detecting diabetic retinal neovascularization. Ophthalmol Retina. 2020;4(6):588–594. doi:10.1016/j.oret.2020.01.004
42. Papayannis A, Tsamis E, Stringa F, Iacono P, Battaglia Parodi M, Stanga PE. Swept-source optical coherence tomography angiography vitreo-retinal segmentation in proliferative diabetic retinopathy. Eur J Ophthalmol. 2021;31(4):1925–1932. doi:10.1177/1120672120944028
43. Sawada O, Ichiyama Y, Obata S, et al. Comparison between wide-angle OCT angiography and ultra-wide field fluorescein angiography for detecting non-perfusion areas and retinal neovascularization in eyes with diabetic retinopathy. Graefes Arch Clin Exp Ophthalmol. 2018;256(7):1275–1280. doi:10.1007/s00417-018-3992-y
44. Hirano T, Kakihara S, Toriyama Y, Nittala MG, Murata T, Sadda S. Wide-field en face swept-source optical coherence tomography angiography using extended field imaging in diabetic retinopathy. Br J Ophthalmol. 2018;102(9):1199–1203. doi:10.1136/bjophthalmol-2017-311358
45. Quantitative approaches in multimodal fundus imaging: state of the art and future perspectives - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/35933313/.
46. Tan B, Lim NA, Tan R, et al. Combining retinal and choroidal microvascular metrics improves discriminative power for diabetic retinopathy. Br J Ophthalmol. 2023;107(7):993–999. doi:10.1136/bjophthalmol-2021-319739
47. Everett LA, Paulus YM. Laser therapy in the treatment of diabetic retinopathy and diabetic macular edema. Curr Diab Rep. 2021;21(9):35. doi:10.1007/s11892-021-01403-6
48. The Diabetic Retinopathy Study Research Group. Photocoagulation treatment of proliferative diabetic retinopathy: clinical application of Diabetic Retinopathy Study (DRS) findings, DRS Report Number 8. Ophthalmology. 1981;88(7):583–600.
49. Flynn HW, Chew EY, Simons BD, Barton FB, Remaley NA, Ferris FL; The Early Treatment Diabetic Retinopathy Study Research Group. Pars plana vitrectomy in the Early Treatment Diabetic Retinopathy Study: ETDRS report number 17. Ophthalmology. 1992;99(9):1351–1357. doi:10.1016/s0161-6420(92)31779-8
50. Feng HE, Weihong YU, Dong F. Observation of retinal neovascularization using optical coherence tomography angiography after panretinal photocoagulation for proliferative diabetic retinopathy. BMC Ophthalmol. 2021;21(1):252. doi:10.1186/s12886-021-01964-w
51. Vander JF, Duker JS, Benson WE, Brown GC, McNamara JA, Rosenstein RB. Long-term stability and visual outcome after favorable initial response of proliferative diabetic retinopathy to panretinal photocoagulation. Ophthalmology. 1991;98(10):1575–1579. doi:10.1016/s0161-6420(91)32085-2
52. Long-term visual outcome in proliferative diabetic retinopathy patients after panretinal photocoagulation - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/10413257/.
53. Ohlhausen M, Payne C, Greenlee T, Chen AX, Conti T, Singh RP. Impact and characterization of delayed pan-retinal photocoagulation in proliferative diabetic retinopathy. Am J Ophthalmol. 2021;223:267–274. doi:10.1016/j.ajo.2020.09.051
54. Gross JG, Glassman AR, Jampol LM, et al. Panretinal photocoagulation vs intravitreous ranibizumab for proliferative diabetic retinopathy: a randomized clinical trial. JAMA. 2015;314(20):2137–2146. doi:10.1001/jama.2015.15217
55. Khan R, Surya J, Rajalakshmi R, et al. Need for vitreous surgeries in proliferative diabetic retinopathy in 10-year follow-up: India retinal disease study group report no. 2. Ophthalmic Res. 2021;64(3):432–439. doi:10.1159/000512767
56. Sivaprasad S, Prevost AT, Vasconcelos JC, et al. Clinical efficacy of intravitreal aflibercept versus panretinal photocoagulation for best corrected visual acuity in patients with proliferative diabetic retinopathy at 52 weeks (CLARITY): a multicentre, single-blinded, randomised, controlled, phase 2b, non-inferiority trial. Lancet. 2017;389(10085):2193–2203. doi:10.1016/S0140-6736(17)31193-5
57. Perais JA, McCullough PG, McLaughlin GA, et al. Predictive factors associated with anatomical and functional outcomes after panretinal photocoagulation in people with proliferative diabetic retinopathy. Retina. 2022;42(8):1536–1544. doi:10.1097/IAE.0000000000003510
58. Parikh R, Shah RJ, VanHouten JP, Cherney EF. Ocular findings at initial pan retinal photocoagulation for proliferative diabetic retinopathy predict the need for future pars plana vitrectomy. Retina. 2014;34(10):1997–2002. doi:10.1097/IAE.0000000000000192
59. Perais J, Agarwal R, Evans JR, et al. Prognostic factors for the development and progression of proliferative diabetic retinopathy in people with diabetic retinopathy. Cochrane Database Syst Rev. 2023;2(2):CD013775. doi:10.1002/14651858.CD013775.pub2
60. Kuiper EJ, Van Nieuwenhoven FA, de Smet MD, et al. The angio-fibrotic switch of VEGF and CTGF in proliferative diabetic retinopathy. PLoS One. 2008;3(7):e2675. doi:10.1371/journal.pone.0002675
61. Alagorie AR, Velaga S, Nittala MG, Yu HJ, Wykoff CC, Sadda SR. Effect of aflibercept on diabetic retinopathy severity and visual function in the RECOVERY study for proliferative diabetic retinopathy. Ophthalmol Retina. 2021;5(5):409–419. doi:10.1016/j.oret.2020.08.018
62. Bonnin S, Dupas B, Lavia C, et al. Anti-vascular endothelial growth factor therapy can improve diabetic retinopathy score without change in retinal perfusion. Retina. 2019;39(3):426–434. doi:10.1097/IAE.0000000000002422
63. Arrigo A, Aragona E, Bandello F. VEGF-targeting drugs for the treatment of retinal neovascularization in diabetic retinopathy. Ann Med. 2022;54(1):1089–1111. doi:10.1080/07853890.2022.2064541
64. Alsoudi AF, Wai KM, Koo E, Parikh R, Mruthyunjaya P, Rahimy E. Progression to pars plana vitrectomy in patients with proliferative diabetic retinopathy. JAMA Ophthalmol. 2024;142(7):662–668. doi:10.1001/jamaophthalmol.2024.1844
65. Lang GE, Stahl A, Voegeler J, et al. Efficacy and safety of ranibizumab with or without panretinal laser photocoagulation versus laser photocoagulation alone in proliferative diabetic retinopathy - the PRIDE study. Acta Ophthalmol. 2020;98(5):e530–e539. doi:10.1111/aos.14312
66. Falavarjani KG, Habibi A, Khorasani MA, Anvari P, Sadda SR. Time course of changes in optic disk neovascularization after a single intravitreal bevacizumab injection. Retina. 2019;39(6):1149–1153. doi:10.1097/IAE.0000000000002107
67. Hu Z, Su Y, Xie P, et al. OCT angiography-based monitoring of neovascular regression on fibrovascular membrane after preoperative intravitreal conbercept injection. Graefes Arch Clin Exp Ophthalmol. 2019;257(8):1611–1619. doi:10.1007/s00417-019-04315-0
68. Wubben TJ, Johnson MW, Sohn EH, et al. Anti–vascular endothelial growth factor therapy for diabetic retinopathy: consequences of inadvertent treatment interruptions. Am J Ophthalmol. 2019;204:13–18. doi:10.1016/j.ajo.2019.03.005
69. Obeid A, Su D, Patel SN, et al. Outcomes of eyes lost to follow-up with proliferative diabetic retinopathy that received panretinal photocoagulation versus intravitreal anti-vascular endothelial growth factor. Ophthalmology. 2019;126(3):407–413. doi:10.1016/j.ophtha.2018.07.027
70. Obeid A, Gao X, Ali FS, et al. Loss to follow-up in patients with proliferative diabetic retinopathy after panretinal photocoagulation or intravitreal anti-VEGF injections. Ophthalmology. 2018;125(9):1386–1392. doi:10.1016/j.ophtha.2018.02.034
71. Walton M, Bojke L, Simmonds M, et al. Anti-vascular endothelial growth factor drugs compared with panretinal photocoagulation for the treatment of proliferative diabetic retinopathy: a cost-effectiveness analysis. Value Health. 2024;27(7):907–917. doi:10.1016/j.jval.2024.03.007
72. Lin J, Chang JS, Smiddy WE. Cost evaluation of panretinal photocoagulation versus intravitreal ranibizumab for proliferative diabetic retinopathy. Ophthalmology. 2016;123(9):1912–1918. doi:10.1016/j.ophtha.2016.05.037
73. Hutton DW, Stein JD, Glassman AR, et al. Five-year cost-effectiveness of intravitreous ranibizumab therapy vs panretinal photocoagulation for treating proliferative diabetic retinopathy: a secondary analysis of a randomized clinical trial. JAMA Ophthalmol. 2019;137(12):1424–1432. doi:10.1001/jamaophthalmol.2019.4284
74. Simmonds M, Llewellyn A, Walker R, et al. Anti-VEGF drugs compared with laser photocoagulation for the treatment of proliferative diabetic retinopathy: a systematic review and individual participant data meta-analysis. Health Technol Assess. 2025;29(23):1–75. doi:10.3310/MJYP6578
75. Luckham K, Tebbs H, Claxton L, et al. A Markov model assessing the cost-effectiveness of various anti-vascular endothelial growth factor drugs and panretinal photocoagulation for the treatment of proliferative diabetic retinopathy. Eye. 2025;39(7):1364–1372. doi:10.1038/s41433-025-03641-4
76. Tao Y, Jiang P, Zhao Y, et al. Retrospective study of aflibercept in combination therapy for high-risk proliferative diabetic retinopathy and diabetic maculopathy. Int Ophthalmol. 2021;41(6):2157–2165. doi:10.1007/s10792-021-01773-6
77. Brown DM, Nguyen QD, Marcus DM, et al. Long-term outcomes of ranibizumab therapy for diabetic macular edema: the 36-month results from two Phase III trials: RISE and RIDE. Ophthalmology. 2013;120(10):2013–2022. doi:10.1016/j.ophtha.2013.02.034
78. Boyer DS, Nguyen QD, Brown DM, Basu K, Ehrlich JS; RIDE and RISE Research Group. Outcomes with as-needed ranibizumab after initial monthly therapy: long-term outcomes of the phase III RIDE and RISE trials. Ophthalmology. 2015;122(12):2504–2513.e1. doi:10.1016/j.ophtha.2015.08.006
79. Tan Y, Fukutomi A, Sun MT, Durkin S, Gilhotra J, Chan WO. Anti-VEGF crunch syndrome in proliferative diabetic retinopathy: a review. Surv Ophthalmol. 2021;66(6):926–932. doi:10.1016/j.survophthal.2021.03.001
80. Hutton DW, Stein JD, Bressler NM, et al. Cost-effectiveness of intravitreous ranibizumab compared with panretinal photocoagulation for proliferative diabetic retinopathy: secondary analysis from a diabetic retinopathy clinical research network randomized clinical trial. JAMA Ophthalmol. 2017;135(6):576–584. doi:10.1001/jamaophthalmol.2017.0837
81. Figueira J, Fletcher E, Massin P, et al. Ranibizumab plus panretinal photocoagulation versus panretinal photocoagulation alone for high-risk proliferative diabetic retinopathy (PROTEUS Study). Ophthalmology. 2018;125(5):691–700. doi:10.1016/j.ophtha.2017.12.008
82. Sun Y, Qi H. A comparison between the therapeutic effects of Conbercept combined with panretinal photocoagulation and panretinal photocoagulation monotherapy for high-risk proliferative diabetic retinopathy. Front Endocrinol. 2022;13:1038757. doi:10.3389/fendo.2022.1038757
83. Rebecca, Shaikh FF, Jatoi SM. Comparison of efficacy of combination therapy of an Intravitreal injection of bevacizumab and photocoagulation versus pan retinal photocoagulation alone in high risk proliferative diabetic retinopathy. Pak J Med Sci. 2021;37(1):157–161. doi:10.12669/pjms.37.1.3141
84. Li S, Tao Y, Yang M, et al. Aflibercept 5+PRN with retinal laser photocoagulation is more effective than retinal laser photocoagulation alone and aflibercept 3+PRN with retinal laser photocoagulation in patients with high-risk proliferative diabetic retinopathy and diabetic macular edema: a 12-month clinical trial. Front Endocrinol. 2024;15:1286736. doi:10.3389/fendo.2024.1286736
85. Zhang Q, Zhang T, Zhuang H, Sun Z, Qin Y. Single-dose intravitreal conbercept before panretinal photocoagulation as an effective adjunctive treatment in Chinese proliferative diabetic retinopathy. Ophthalmologica. 2019;242(2):59–68. doi:10.1159/000495423
86. Tonello M, Costa RA, Almeida FPP, Barbosa JC, Scott IU, Jorge R. Panretinal photocoagulation versus PRP plus intravitreal bevacizumab for high-risk proliferative diabetic retinopathy (IBeHi study). Acta Ophthalmol. 2008;86(4):385–389. doi:10.1111/j.1600-0420.2007.01056.x
87. Zhou AY, Zhou CJ, Yao J, Quan YL, Ren BC, Wang JM. Panretinal photocoagulation versus panretinal photocoagulation plus intravitreal bevacizumab for high-risk proliferative diabetic retinopathy. Int J Ophthalmol. 2016;9(12):1772–1778. doi:10.18240/ijo.2016.12.12
88. Fu P, Huang Y, Wan X, et al. Efficacy and safety of pan retinal photocoagulation combined with intravitreal anti-VEGF agents for high-risk proliferative diabetic retinopathy: a systematic review and meta-analysis. Medicine. 2023;102(39):e34856. doi:10.1097/MD.0000000000034856
89. He F, Yu W. Longitudinal neovascular changes on optical coherence tomography angiography in proliferative diabetic retinopathy treated with panretinal photocoagulation alone versus with intravitreal conbercept plus panretinal photocoagulation: a pilot study. Eye. 2020;34(8):1413–1418. doi:10.1038/s41433-019-0628-3
90. Alsoudi AF, Wai KM, Koo E, Parikh R, Mruthyunjaya P, Rahimy E. Initial therapy of panretinal photocoagulation vs anti-VEGF injection for proliferative diabetic retinopathy. JAMA Ophthalmol. 2024;142(10):972–975. doi:10.1001/jamaophthalmol.2024.3283
91. Schmidt-Erfurth U, Garcia-Arumi J, Bandello F, et al. Guidelines for the management of diabetic macular edema by the European Society of Retina Specialists (EURETINA). Ophthalmologica. 2017;237(4):185–222. doi:10.1159/000458539
92. Machemer R, Blankenship G. Vitrectomy for proliferative diabetic retinopathy associated with vitreous hemorrhage. Ophthalmology. 1981;88(7):643–646. doi:10.1016/s0161-6420(81)34972-0
93. Berrocal MH, Acaba-Berrocal L. Early pars plana vitrectomy for proliferative diabetic retinopathy: update and review of current literature. Curr Opin Ophthalmol. 2021;32(3):203–208. doi:10.1097/ICU.0000000000000760
94. Yoshida S, Nakama T, Ishikawa K, et al. Antiangiogenic shift in vitreous after vitrectomy in patients with proliferative diabetic retinopathy. Invest Ophthalmol Vis Sci. 2012;53(11):6997–7003. doi:10.1167/iovs.12-9671
95. Chen HJ, Ma ZZ, Li Y, Wang CG. Change of vascular endothelial growth factor levels following vitrectomy in eyes with proliferative diabetic retinopathy. J Ophthalmol. 2019;2019:6764932. doi:10.1155/2019/6764932
96. Gupta B, Sivaprasad S, Wong R, et al. Visual and anatomical outcomes following vitrectomy for complications of diabetic retinopathy: the DRIVE UK study. Eye. 2012;26(4):510–516. doi:10.1038/eye.2011.321
97. Storey PP, Ter-Zakarian A, Philander SA, et al. Visual and anatomical outcomes after diabetic traction and traction-rhegmatogenous retinal detachment repair. Retina. 2018;38(10):1913–1919. doi:10.1097/IAE.0000000000001793
98. Mikhail M, Ali-Ridha A, Chorfi S, Kapusta MA. Long-term outcomes of sutureless 25-G+ pars-plana vitrectomy for the management of diabetic tractional retinal detachment. Graefes Arch Clin Exp Ophthalmol. 2017;255(2):255–261. doi:10.1007/s00417-016-3442-7
99. Sokol JT, Schechet SA, Rosen DT, Ferenchak K, Dawood S, Skondra D. Outcomes of vitrectomy for diabetic tractional retinal detachment in Chicago’s county health system. PLoS One. 2019;14(8):e0220726. doi:10.1371/journal.pone.0220726
100. Tan SZ, Steel DH, Stanzel BV, et al. Safety and effectiveness of pre-emptive diabetic vitrectomy in patients with severe, non-fibrotic retinal neovascularisation despite panretinal photocoagulation. Eye. 2023;37(8):1553–1557. doi:10.1038/s41433-022-02167-3
101. Glassman AR, Beaulieu WT, Maguire MG, et al. Visual acuity, vitreous hemorrhage, and other ocular outcomes after vitrectomy vs aflibercept for vitreous hemorrhage due to diabetic retinopathy: a secondary analysis of a randomized clinical trial. JAMA Ophthalmol. 2021;139(7):725–733. doi:10.1001/jamaophthalmol.2021.1110
102. Berrocal MH, Acaba-Berrocal L, Acaba AM. Long-term outcomes of same patient eyes treated with pars plana vitrectomy in one eye and conventional treatment in the other for complications of proliferative diabetic retinopathy. J Clin Med. 2022;11(18):5399. doi:10.3390/jcm11185399
103. Abd Elhamid AH, Mohamed AAEA, Khattab AM. Intravitreal Aflibercept injection with Panretinal photocoagulation versus early Vitrectomy for diabetic vitreous hemorrhage: randomized clinical trial. BMC Ophthalmol. 2020;20(1):130. doi:10.1186/s12886-020-01401-4
104. Antoszyk AN, Glassman AR, Beaulieu WT, et al. Effect of intravitreous aflibercept vs vitrectomy with panretinal photocoagulation on visual acuity in patients with vitreous hemorrhage from proliferative diabetic retinopathy: a randomized clinical trial. JAMA. 2020;324(23):2383–2395. doi:10.1001/jama.2020.23027
105. Lin J, Chang JS, Yannuzzi NA, Smiddy WE. Cost evaluation of early vitrectomy versus panretinal photocoagulation and intravitreal ranibizumab for proliferative diabetic retinopathy. Ophthalmology. 2018;125(9):1393–1400. doi:10.1016/j.ophtha.2018.02.038
106. Young BK, Johnson MW, Wubben TJ. Cost analysis of intravitreal aflibercept vs vitrectomy with panretinal photocoagulation for vitreous hemorrhage from proliferative diabetic retinopathy. JAMA Ophthalmol. 2021;139(7):804–805. doi:10.1001/jamaophthalmol.2021.1565
107. Ono R, Kakehashi A, Yamagami H, et al. Prospective assessment of proliferative diabetic retinopathy with observations of posterior vitreous detachment. Int Ophthalmol. 2005;26(1–2):15–19. doi:10.1007/s10792-005-5389-2
108. Kakehashi A, Kado M, Akiba J, Hirokawa H. Variations of posterior vitreous detachment. Br J Ophthalmol. 1997;81(7):527–532. doi:10.1136/bjo.81.7.527
109. Kakehashi A, Takezawa M, Akiba J. Classification of posterior vitreous detachment. Clin Ophthalmol. 2014;8:1–10. doi:10.2147/OPTH.S54021
110. Liao M, Wang X, Yu J, et al. Characteristics and outcomes of vitrectomy for proliferative diabetic retinopathy in young versus senior patients. BMC Ophthalmol. 2020;20(1):416. doi:10.1186/s12886-020-01688-3
111. Wakabayashi Y, Usui Y, Okunuki Y, et al. Intraocular VEGF level as a risk factor for postoperative complications after vitrectomy for proliferative diabetic retinopathy. Invest Ophthalmol Vis Sci. 2012;53(10):6403–6410. doi:10.1167/iovs.12-10367
112. Wakabayashi Y, Usui Y, Tsubota K, et al. Persistent overproduction of intraocular vascular endothelial growth factor as a cause of late vitreous hemorrhage after vitrectomy for proliferative diabetic retinopathy. Retina. 2017;37(12):2317–2325. doi:10.1097/IAE.0000000000001490
113. Yeung L, Liu L, Wu WC, et al. Reducing the incidence of early postoperative vitreous haemorrhage by preoperative intravitreal bevacizumab in vitrectomy for diabetic tractional retinal detachment. Acta Ophthalmol. 2010;88(6):635–640. doi:10.1111/j.1755-3768.2008.01498.x
114. Alshaikhsalama AM, Thompson KN, Patrick H, Lee J, Voor TA, Wang AL. Clinical characteristics and surgical outcomes of patients undergoing pars plana vitrectomy for proliferative diabetic retinopathy. Ophthalmol Retina. 2024;8(8):823–831. doi:10.1016/j.oret.2024.02.015
115. Ben Addou Idrissi S, Bengebara O, Filali Sadouk M, et al. Comparison of pars plana vitrectomy and combined pars plana vitrectomy with phacoemulsification for proliferative diabetic retinopathy: a retrospective study about 120 eyes. Indian J Ophthalmol. 2024;72(Suppl 2):S287–S292. doi:10.4103/IJO.IJO_1976_23
116. Hwang S, Kim JH, Choi YH, et al. Incidence and risk factor analysis of neovascular glaucoma following vitrectomy in patients with proliferative diabetic retinopathy. Sci Rep. 2024;14(1):22490. doi:10.1038/s41598-024-73395-8
117. Takayama K, Someya H, Yokoyama H, et al. Risk factors of neovascular glaucoma after 25-gauge vitrectomy for proliferative diabetic retinopathy with vitreous hemorrhage: a retrospective multicenter study. Sci Rep. 2019;9(1):14858. doi:10.1038/s41598-019-51411-6
118. The incidence and risk factors of neovascular glaucoma secondary to proliferative diabetic retinopathy after vitrectomy - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/33334171/.
119. Hwang S, Hong EH, Kang MH, Shin YU. Early postoperative bevacizumab for preventing neovascular glaucoma in phacovitrectomy for proliferative diabetic retinopathy. Sci Rep. 2025;15(1):1231. doi:10.1038/s41598-025-85667-y
120. Liggett PE, Lean JS, Barlow WE, Ryan SJ. Intraoperative argon endophotocoagulation for recurrent vitreous hemorrhage after vitrectomy for diabetic retinopathy. Am J Ophthalmol. 1987;103(2):146–149. doi:10.1016/s0002-9394(14)74219-9
121. Patel V, Rohowetz LJ, Pakravan P, Kalavar M, Yannuzzi NA, Sridhar J. Outcomes of pars plana vitrectomy with panretinal photocoagulation for treatment of proliferative diabetic retinopathy without retinal detachment: a seven-year retrospective study. Clin Ophthalmol. 2023;17:471–478. doi:10.2147/OPTH.S400474
122. Fassbender JM, Ozkok A, Canter H, Schaal S. A comparison of immediate and delayed vitrectomy for the management of vitreous hemorrhage due to proliferative diabetic retinopathy. Ophthalmic Surg Lasers Imaging Retina. 2016;47(1):35–41. doi:10.3928/23258160-20151214-05
123. Li S, Yang Y, Zou J, Zeng J, Ding C. The efficacy and safety of intravitreal injection of Ranibizumab as pre-treatment for vitrectomy in proliferative diabetic retinopathy with vitreous hemorrhage. BMC Ophthalmol. 2022;22(1):63. doi:10.1186/s12886-022-02303-3
124. Zhao XY, Xia S, Chen YX. Antivascular endothelial growth factor agents pretreatment before vitrectomy for complicated proliferative diabetic retinopathy: a meta-analysis of randomised controlled trials. Br J Ophthalmol. 2018;102(8):1077–1085. doi:10.1136/bjophthalmol-2017-311344
125. Martinez-Zapata MJ, Salvador I, Martí-Carvajal AJ, et al. Anti-vascular endothelial growth factor for proliferative diabetic retinopathy. Cochrane Database Syst Rev. 2023;3(3):CD008721. doi:10.1002/14651858.CD008721.pub3
126. Wang DY, Zhao XY, Zhang WF, Meng LH, Chen YX. Perioperative anti-vascular endothelial growth factor agents treatment in patients undergoing vitrectomy for complicated proliferative diabetic retinopathy: a network meta-analysis. Sci Rep. 2020;10(1):18880. doi:10.1038/s41598-020-75896-8
127. Sun X, Wang X, Guo X, Wang M, Liu H. Combined use of anti-VEGF drugs before and during pars plana vitrectomy for severe proliferative diabetic retinopathy. Ophthalmol Ther. 2023;12(6):3133–3142. doi:10.1007/s40123-023-00803-z
128. Pharmacokinetics of intravitreal anti-VEGF drugs in vitrectomized versus non-vitrectomized eyes - PubMed. 2017. Available from: https://pubmed.ncbi.nlm.nih.gov/29134820/.
129. Dervenis P, Dervenis N, Smith JM, Steel DH. Anti-vascular endothelial growth factors in combination with vitrectomy for complications of proliferative diabetic retinopathy. Cochrane Database Syst Rev. 2023;5(5):CD008214. doi:10.1002/14651858.CD008214.pub4
130. Beer PM, Wong SJ, Hammad AM, Falk NS, O’Malley MR, Khan S. Vitreous levels of unbound bevacizumab and unbound vascular endothelial growth factor in two patients. Retina. 2006;26(8):871–876. doi:10.1097/01.iae.0000233327.68433.02
131. Russo A, Longo A, Avitabile T, et al. Incidence and risk factors for tractional macular detachment after anti-vascular endothelial growth factor agent pretreatment before vitrectomy for complicated proliferative diabetic retinopathy. J Clin Med. 2019;8(11):1960. doi:10.3390/jcm8111960
132. Preoperative intravitreal bevacizumab use as an adjuvant to diabetic vitrectomy: histopathologic findings and clinical implications - PubMed. 2011. Available from: https://pubmed.ncbi.nlm.nih.gov/21055812/.
133. Su T, Lai D, Wu Y, et al. Comparison of the efficacy and safety of ranibizumab 0.5 mg versus 1.0 mg with pars plana vitrectomy for the treatment of proliferative diabetic retinopathy: a Randomized Controlled Trial. Retina. 2024;44(4):680–688. doi:10.1097/IAE.0000000000003998
134. Kousha O, Gil LC, Panggalo I, Blaikie A, Ellis J. Methods of assessment of diabetic retinopathy in low- and middle-income countries: a protocol for scoping review. BMJ Open. 2025;15(7):e095892. doi:10.1136/bmjopen-2024-095892
135. Vujosevic S, Aldington SJ, Silva P, et al. Screening for diabetic retinopathy: new perspectives and challenges. Lancet Diabetes Endocrinol. 2020;8(4):337–347. doi:10.1016/S2213-8587(19)30411-5
136. Tang F, Luenam P, Ran AR, et al. Detection of diabetic retinopathy from ultra-widefield scanning laser ophthalmoscope images: a multicenter deep learning analysis. Ophthalmol Retina. 2021;5(11):1097–1106. doi:10.1016/j.oret.2021.01.013
137. Liu J, Gibson E, Ramchal S, et al. Diabetic retinopathy screening with automated retinal image analysis in a primary care setting improves adherence to ophthalmic care. Ophthalmol Retina. 2021;5(1):71–77. doi:10.1016/j.oret.2020.06.016
138. Ntjam NN, Thulliez M, Paintaud G, et al. Cardiovascular adverse events with intravitreal anti-vascular endothelial growth factor drugs: a systematic review and meta-analysis of randomized clinical trials. JAMA Ophthalmol. 2021;139(6):610–619. doi:10.1001/jamaophthalmol.2021.0640
139. Zehden JA, Mortensen XM, Reddy A, Zhang AY. Systemic and ocular adverse events with intravitreal anti-VEGF therapy used in the treatment of diabetic retinopathy: a review. Curr Diab Rep. 2022;22(10):525–536. doi:10.1007/s11892-022-01491-y
140. Wang XN, Li S, Cai X, Li T, Long D, Wu Q. Imaging artifacts and quality evaluation with ultrawide-field swept-source OCTA in diabetic retinopathy. Curr Eye Res. 2024;49(4):410–416. doi:10.1080/02713683.2023.2296362
141. Suresh R, Yu HJ, Thoveson A, et al. Loss to follow-up among patients with proliferative diabetic retinopathy in clinical practice. Am J Ophthalmol. 2020;215:66–71. doi:10.1016/j.ajo.2020.03.011
142. Confalonieri F, Barone G, Ferraro V, et al. Early versus Late Pars Plana Vitrectomy in Vitreous Hemorrhage: a Systematic Review. J Clin Med. 2023;12(20):6652. doi:10.3390/jcm12206652
143. Chinese Medical Association Ophthalmology Branch Retinal Disease Subcommittee, Chinese Medical Doctor Association Ophthalmology Branch Retinal Disease Specialized Committee, Expert Group on the Expert Consensus on Vitrectomy Surgery for the Treatment of Type 2 Diabetic Retinopathy. Expert consensus on vitrectomy surgery for the treatment of type 2 diabetic retinopathy. Chin J Retinal Dis. 2024;40(09):663–686. doi:10.3760/cma.j.cn511434-20240729-00286
144. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ. 2008;336(7650):924–926. doi:10.1136/bmj.39489.470347.AD
145. Wong TY, Sun J, Kawasaki R, et al. Guidelines on diabetic eye care: the international council of ophthalmology recommendations for screening, follow-up, referral, and treatment based on resource settings. Ophthalmology. 2018;125(10):1608–1622. doi:10.1016/j.ophtha.2018.04.007
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.