Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Integration of Traditional Chinese Medicine and Psychotherapy in Mental Health: A Narrative Review of Mechanisms, Clinical Evidence, and Future Directions
Received 6 March 2026
Accepted for publication 26 May 2026
Published 3 June 2026 Volume 2026:22 607443
DOI https://doi.org/10.2147/NDT.S607443
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Ji Du,1,2 Yong Tan2
1Department of Gynecology, Suzhou TCM Hospital Affiliated to Nanjing University of Chinese Medicine, Suzhou, Jiangsu, 215009, People’s Republic of China; 2The First Clinical Medical College, Nanjing University of Chinese Medicine, Nanjing, Jiangsu, 210023, People’s Republic of China
Correspondence: Yong Tan, Email [email protected]
Purpose: This narrative review critically evaluates the integration of Traditional Chinese Medicine (TCM) and Western psychotherapy in mental health care, identifying current evidence, methodological limitations, and future research priorities.
Methods: We narratively synthesized peer-reviewed literature focusing on clinical studies that combined TCM interventions (acupuncture, herbal medicine, TCM exercises such as Baduanjin and Tai Chi) with psychological or psychiatric approaches for mental disorders. Evidence was organized into three levels: clinical efficacy (human RCTs and meta-analyses), mechanistic studies (animal and biomarker research), and exploratory investigations (neuroimaging, omics, observational surveys).
Results: Key findings include: (1) TCM interventions combined with pharmacological or psychological treatments for depression showed a pooled standardized mean difference of − 2.05 (95% CI: − 2.74 to − 1.37) from 18 RCTs, indicating a large effect size but with high heterogeneity; (2) TCM exercises (Baduanjin, Tai Chi) improved attention and reduced mild anxiety (P=0.034), though evidence in clinical samples remains limited; (3) Mechanistic studies suggest potential regulation of the HPA axis, monoamine neurotransmitters, inflammation, and gut microbiota, but these findings are preliminary and derived mostly from animal models. Major barriers to integration include: lack of standardized TCM diagnostic criteria; few methodologically rigorous RCTs; high heterogeneity; insufficient cross-training of clinicians; and fundamental conceptual differences between TCM (holistic) and evidence-based psychotherapy (mechanistic).
Conclusion: While TCM-psychotherapy integration holds conceptual promise, current evidence is limited by substantial methodological weaknesses. The most robust evidence exists for acupuncture and TCM exercises for depression and anxiety over short-term follow-up (4– 12 weeks). Evidence for PTSD, severe mental illness, and long-term outcomes (≥ 6 months) remains preliminary. Future research should prioritize large, well-blinded RCTs with prespecified TCM syndrome criteria and longer follow-up periods.
Keywords: traditional Chinese medicine, psychotherapy, mental health, depression, acupuncture, integrated medicine, narrative review
Introduction
Background
Depression affects around 280 million people in the world, and it is one of the factors that increase the burden of mental health disorders. It has thus drawn increasing of attention to the treatment strategies that are comprehensive and focus on the whole patient, which are more than the standard pharmacological interventions and formal psychotherapeutic techniques.1 Traditional Chinese Medicine (TCM) has the basic theory of Yin-Yang balance, theory of Five Elements, and theory of mind body as one. Therefore, the theoretical system of TCM fits well with the modern biopsychosocial paradigm of health.2
There are many therapeutic practices that are applicable to mental well-being in TCM, such as the practice of acupuncture, use of medicinal herbs, nutritional advice, as well as contemplative physical exercises including Baduanjin and Tai Chi.3 In particular, the practice of Tai Chi has shown effectiveness in improving the mental health outcomes in diverse populations, including older adults and patients with chronic diseases.4,5 A common element of these approaches is the re-establishment of the smooth circulation of Qi and the regulation of the internal organ systems to globally manage the somatic and affective part of the diseases.6
Current Evidence and Its Limitations
The mechanistic investigations suggest that the approach of TCM might affect hypothalamic-pituitary-adrenal (HPA) axis and have antidepressant effects.7,8 However, most of these results are from animal studies and should be verified in human clinical situation.
There are a number of randomized controlled trials (RCTs) and meta-analyses that reported beneficial effects. However, this body of evidence is strongly constrained by (i) number of participants, (ii) the absence of sham control groups, (iii) the short observation period (usually 4–12 weeks long), (iv) the large amount of heterogeneity among the different studies, and (v) possible publication bias.9 For example, one meta-analysis of 18 RCTs reported a pooled standardized mean difference of −2.05 (95% CI from −2.74 to −1.37) for TCM wellness programs for depression.10 The authors pointed out the presence of large heterogeneity and the possible publication bias of the results.10
Gaps in Existing Reviews
So far, most reviews in the current literature have only looked at a specific TCM practice in separate, and not at the combination of all of them with psychotherapeutic practices. They have not critically discussed methodological errors and nor do they give systematic structures to classify different kinds of research results.11 Therefore, there is not much clear which parts of the current evidence are well supported, which findings are still explorative and what main problems are still blocking in this field.
Aims and Research Questions
This narrative review aims to answer three specific questions:
- What does the existing literature suggest about the combination of TCM treatment (acupuncture, herbal remedies, TCM exercises and so on) with some kind of psychological or psychiatric technique for the mental illness conditions?
- What methodological weaknesses and what theoretical problems are important enough that they limit the robustness of the conclusions that one can draw from the present investigations?
- What are the priorities for future research to advance the field of TCM-psychotherapy integration?
Evidence Organization
In order to address these issues, we perform a critical synthesis of peer-reviewed academic publications from 2012 to 2025. The body of evidence is divided in a three tiers hierarchical framework:
Level 1 (Clinical Effectiveness) – This level includes human randomized controlled trials (RCTs), systematic reviews and meta-analyses, that directly investigate the integration of the TCM intervention with some kind of psychological or psychiatric treatment. These investigations provide the most direct and relevant evidence for clinical practice. But they have in general problems of small number of participants, no blinding procedure, and short follow-up period.
Level 2 (Mechanistic Research) – this level comprises the studies with animal models, cellular experiments and human biomarker studies for investigating the possible underlying biological pathways. Most of the information obtained in this level is hypothesis forming and has not been used to produce any direct of clinical.
Level 3 (Exploratory and Observational Research)-Neuroimaging studies, omics analyses and cross-sectional surveys belong to this category. Such methodologies are useful to produce new hypotheses, and to find associations, but they are not amenable to provide evidence for the test of the effectiveness of particular interventions.
In this review, the clinical recommendations are mostly Level 1. The results of Levels 2 and 3 are discussed for their exploratory character and for the possible generation of new hypotheses.
Review Structure
After this brief introduction, we next describe the core TCM principles and the evidential framework (Core Concepts and Evidence Framework), the clinical evidence with critical appraisal (Clinical Evidence and Critical Evaluation), the mechanistic and diagnostic clues (Mechanistic and Diagnostic Insights), the controversies and methodological limitations (Controversies and Methodological Limitations), and the future directions with a layered conclusion (Future Directions and Conclusion).
Core Concepts and Evidence Framework
Core TCM Concepts in Mental Health
The principles of Traditional Chinese Medicine (TCM) are widely used for mental well-being evaluation and treatment. Zhang et al developed the TCM-50 survey, which is an instrument for the evaluation of health in physical, psychological, environment and social dimensions. It has a good measurement reliability: coefficient of Cronbach’s alpha is 0.927 and split-half coefficient is 0.876, which means that it gives a measurement possibility for the use of TCM ideas for the psychological assessment.12
A number of clinical investigations have looked at the use of the TCM based approaches for mental health results. For example, Fogarty et al carried out a randomized cross over study with 35 people which have been classified as overweight or obese, and they give acupuncture with advice on diet. The treatment was associated to better mental health indicators, but the number of people in the study (35) and the fact that the study is a cross over, without a washout phase, do not allow the generalizability of the conclusions.13
Li et al reported improvements in the attention in 222 university students after a 12 weeks Baduanjin training in,14 according to the Schultz Grid Test (192.4±47.14s instead 210.4±51.15s; P = 0.034). However, the use of a non-active comparison condition (no intervention) means that the found improvements could be due to the physical activity in a general way and not necessarily to the Baduanjin practice.
Theoretical context of Traditional Chinese Medicine (TCM) points out the fact that there is the relation intrinsically with the body and the psychological manifestations. For example, as Ling et al pointed out that the emotional disturbance is supposed to affect the flow of qi in the stomach and the physical complaint as vomiting will then go on. This is the example of the global vision of TCM in the mental health problem.15
In a cross-sectional investigation, that is considered Level 3 evidence, which is only good for generating hypotheses, Lv et al16 also investigated a cohort of 1421 university students. They found some correlations between a balanced physical constitution with a better overall health status. On the other side, people with imbalanced constitutions show higher percentages of depressive and anxiety-related symptoms. Again, we have to underline that in this research design no causal relationship can be established, and the results should not be interpreted as proof of therapeutical effectiveness. The results suggest that strategies for the maintenance of psychological health could be based on the types of traditional Chinese medicine constitution. But in this way, it should be confirmed with prospective studies.
Three-Level Evidence Framework
In the body of the literature, there is a big shortcoming, which is that there is not a clear distinction among the different kinds of evidence, that is, sometimes they are all confounded. In order to solve this problem, we have organized all the literature above in a three-levels hierarchical. Our criterions for the classification are based on the nature of the evidence and on the immediate use of this evidence in the clinical practice.
Level 1: Clinical Effectiveness-This category includes human RCTs, systematic reviews and meta-analyses that investigate the use of TCM modality, eg, acupuncture, herbal medicine and TCM exercise, in combination with psychological or psychiatrist treatment for mental disorders. These kinds of investigations provide the most directly and applicable evidence in the clinical setting. But they often have following limitations, eg, relatively small number of participants, difficulty of blinding procedure, and short time for follow-up. The representative studies in this tier are Ma et al17 and Ruan et al.10
Level 2: Mechanistic Investigations-This level includes the research done in animal models, in cellular system and in human biomarker studies that try to elucidate the possible biological mechanisms by which the TCM interventions may act. The areas of interest include the regulation of the hypothalamic-pituitary-adrenal (HPA) axis, the modulation of monoamine neurotransmitter, influences on inflammatory pathway, and alterations in gut microbiota composition. Such studies are useful for providing scientific hypothesis and understanding the possible ways, however, the results need to be interpreted with caution. The results of this level of evidence are not yet being directly translated to definitive clinical applications. Work at this level is given as, for instance, by Tian et al18,19 and Qu et al.20
Level 3: Exploratory and Observational Research – The studies in this item include, eg, neuroimaging (fMRI), omics analyses, and cross-sectional surveys. They are mainly hypothesis generating, and they were not set out to directly assess the effectiveness of the interventions. They can provide useful comments on the future studies, but their results should not be interpreted as evidence of the effectiveness of the treatment. For example, the work of Zhu et al21 for the retinal imaging in the schizophrenia, and the constitutional survey done by Lv et al.16
Application of the Framework
In the rest of this review, in the sections where we make clinical recommendations, the main stress will be on Level 1 evidence. The results of the Level 2 and Level 3 studies are given as exploratory or preliminary, as they are used to make hypothesis, and they are called by that name. This way the reader will see which conclusions are based on strong evidence and which are only in the very beginning of the investigate.
Table 1 provides a summary of the basic conceptual differences between the Traditional Chinese Medicine and the Western psychotherapeutic approaches, highlighting the points of difference (eg, theorization, ways of diagnosis, the type of support of the evidence) and possible areas of complementarity (eg, the regulation of the whole of the individual with systematic, evidence-informed therapeutic work).
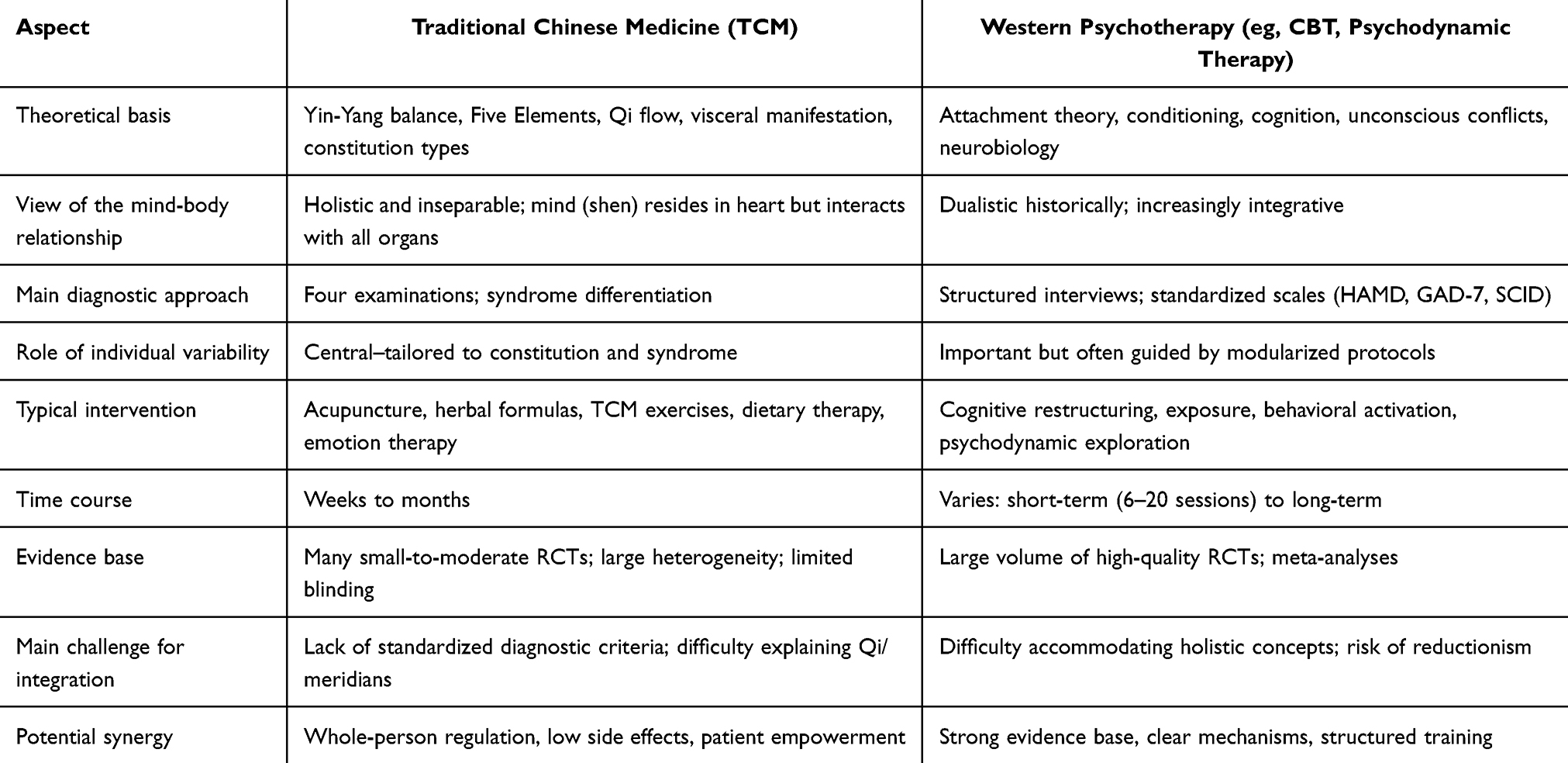 |
Table 1 Comparison of Core Concepts Between Traditional Chinese Medicine (TCM) and Western Psychotherapy in Mental Health Care |
Clinical Evidence and Critical Evaluation
The Use of Acupuncture and Traditional Chinese Medicine Exercises for Depression and Anxiety
The increasing volume of research shows that acupuncture and practices from TCM could be of some therapeutic benefit for people with mild-to-moderate level of depression and of anxiety. But because of the constraints in the study methodology, these results must be interpreted with caution and measured.
Ma et al in a study on the role of acupuncture in the treatment of the depression they did a randomized controlled experiment with 157 subjects suffering from the depression. They compared the combination of electroacupuncture with paroxetine to the paroxetine by itself. After the six weeks intervention, the acupuncture groups showed greater improvement in the quality of life (measured with the WHOQOL-68 scale) than the group with the paroxetine only.17 But these results suggest that the acupuncture could lead to better therapeutic result for the people that suffering from the depression. Nevertheless, because of the methodological limitations of this study (the lack of a sham acupuncture control group and the short follow-up period (only six weeks), we can not draw the causal conclusion.
A systematic review and meta-analysis by Ruan et al, which used data from 18 randomized controlled trials with 1451 participants, showed that whole wellness interventions based on the principle of TCM significantly improved the depressive symptoms. The pooled effect size as a standardized mean difference was −2.05 (95% CI −2.74 to −1.37; P value less than 0.00001).10 However, the authors mentioned that there was a considerable statistical heterogeneity between the included studies, with I2 statistic bigger than 90%. Also, an examination of funnel plots showed an asymmetry, suggesting the presence of publication bias. The methodological rigor of the trials was also limited as there were not enough details about the way the randomization and the blinding protocols were implemented.
Exercises of Traditional Chinese Medicine for improving focus and reducing mild anxiety. In the study by Li and colleagues, 222 healthy university students did Baduanjin practice for 12 weeks and their attention was significantly enhanced (data: 192.4 47.14 sec vs. 210.4 51.15 sec; P = 0.034).14 These results give some first experimental proof of the results; however, the design of the study use an inactive comparison condition (no treatment), therefore is impossible to know if we obtain the benefit because we did Baduanjin or because of the physical exercise in general. In the future they should include active control conditions to support these results.
Integrated Treatment for Post-Stroke Depression
Xie and colleagues compared 163 people with post-stroke depression, a treatment with Five Element theory-based psychotherapy in addition to standard care versus standard care by itself. At both the four-and eight-week times, the group which received the combined intervention showed significantly better results on measures of depressive symptoms, anxiety and sleep.22 While these results are promising, this study did not have a group that was getting some other active psychological therapy as a control, and the observation was only out to eight weeks without a follow-up. Therefore, at this time we cannot make any definite conclusions about the long-term effect and specificity of the treatment effect.
Auricular Acupuncture for Post-Breast Cancer Depression
In a randomized controlled trial with three parallel groups (N = 90), lv et al have studied therapies of the depression after the surgery of the breast. They compared the followed interventions: auricular acupuncture with TCM psychotherapy, auricular acupuncture alone and the western-pharmaceutical (dianxit). After the treatment course of four weeks, the group of the combined therapy showed the better clinical response rate (60.0%) than that of the auricular acupuncture only group (40.0%) and the group of the medication only (36.7%), (P < 0.05).23
However, there are some limitations to be taken into account: the number of participants was small (30 in each group), there was no sham acupuncture control condition, it is not reported if outcome assessors were blinded and the observation was only up to 4 weeks after the intervention. There is definitely a need for larger confirmatory studies, blinded rigorously, to confirm these first results.
Acupuncture for COVID-19 Convalescent Patients
In a randomized controlled trial involving 136 participants, Liang et al studied the application of pressing needle acupuncture in the recovery of patients with COVID-19. After the treatment, there were significant decreases on the scores on the PHQ-9, GAD-7 and ISI scales (P < 0.05) and these beneficial effects were kept at the one month follow up.24 This research was conducted at a single site. The control group (sham acupuncture or no acupuncture) was not clearly described, and outcomes beyond one month were not evaluated.
Evidence for PTSD and Severe Mental Illness
Research on how to combine traditional Chinese medicine with the psychotherapy for disorders, such as post-traumatic stress disorder (PTSD), serious psychiatric disorders such as the bipolar disorder and schizophrenia and the persistent sleep difficulty etc, is very scarce and not methodologically adequate. In their study on the symptoms of PTSD after the Wenchuan earthquake, Hong, and others mentioned that there are not too many studies to use TCM herbal remedy or acupuncture for PTSD.25 The early results are suggested that there might be some therapeutic effect, but the data at present are all from the small-scale observation research. More large-scale randomized controlled trials are required before the clinical guidelines could be set.
Also, Rometsch-Ogioun et al reported that TCM interventions improved both the chronic pain and the PTSD symptoms of the disaster survivors.26 As we have seen for the other case, these are only first observations of small non-randomized studies, which will have to be confirmed by well-designed clinical trials.26
Summary of Key Clinical Evidence
Table 2 gives a summary of the important clinical research that considered the use of TCM and psychotherapeutic approaches together for the mental disorder of interest. For each included study, the table gives the patients characteristics, what integrated intervention was applied, what was the control or comparison treatment, what was the main outcome measures, what the main results were and, as be important, an evaluation of the main methodological flaws that this analysis found in.
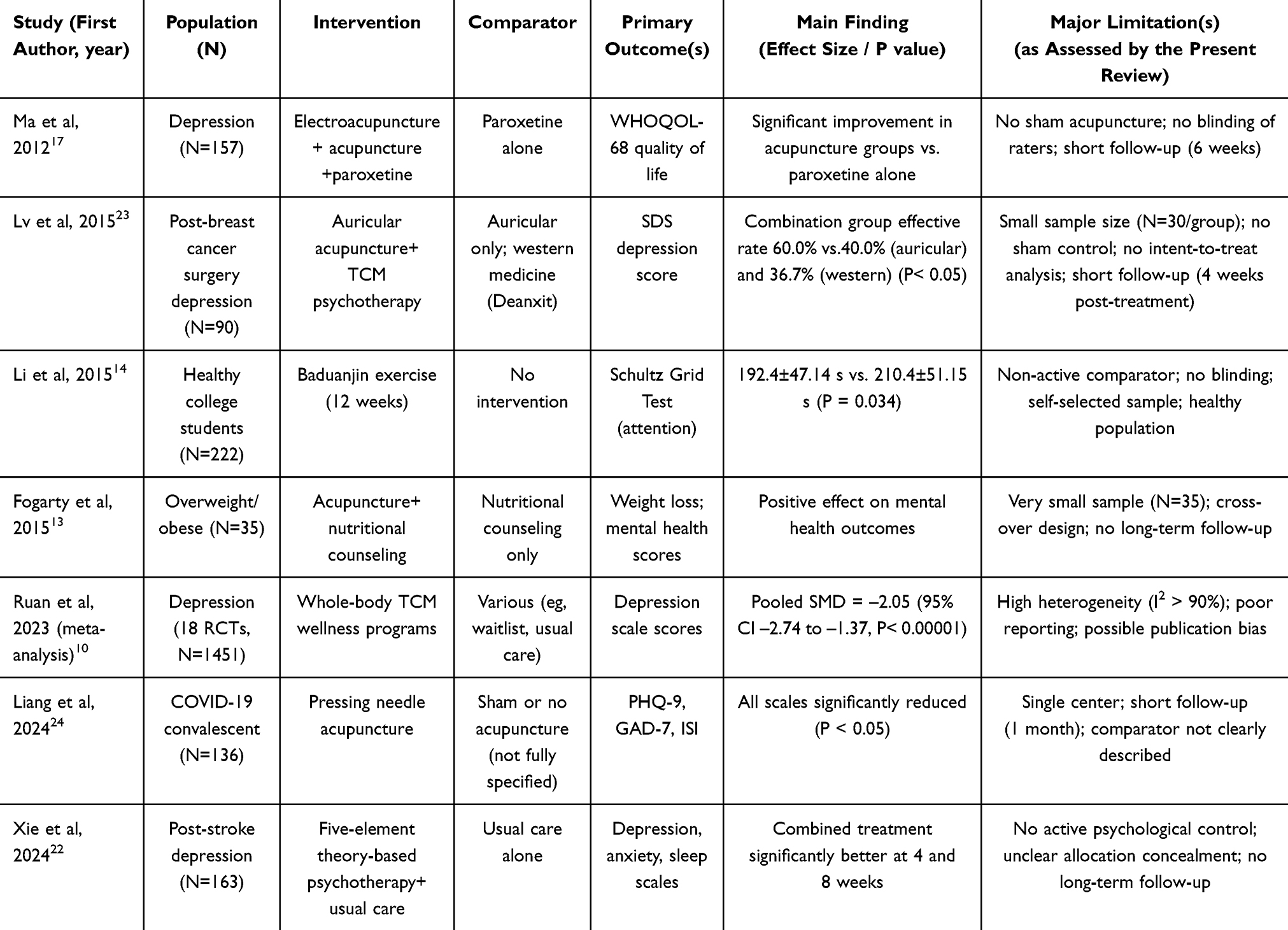 |
Table 2 Summary of Representative Clinical Studies on TCM Combined with Psychological Interventions for Mental Disorders, with Critical Appraisal of Limitations |
Stepped Model for Integration
On the basis of the evidence we have reviewed, Figure 1 shows a proposed tiered structure for the use of TCM and Western psychotherapy in the clinical practice. It goes from the first screening and evaluation (Tier 0), to low intensity preventive (Tier 1), then to a combined approach for the treatment of moderate symptom (Tier 2), and finally to the augmentation approach for severe or refractory (Tier 3). The two-way arrows in tier 2 indicates the possibility of a synergistic effect between the interventions that are specific of TCM and to the psychotherapies with empirical evidence.
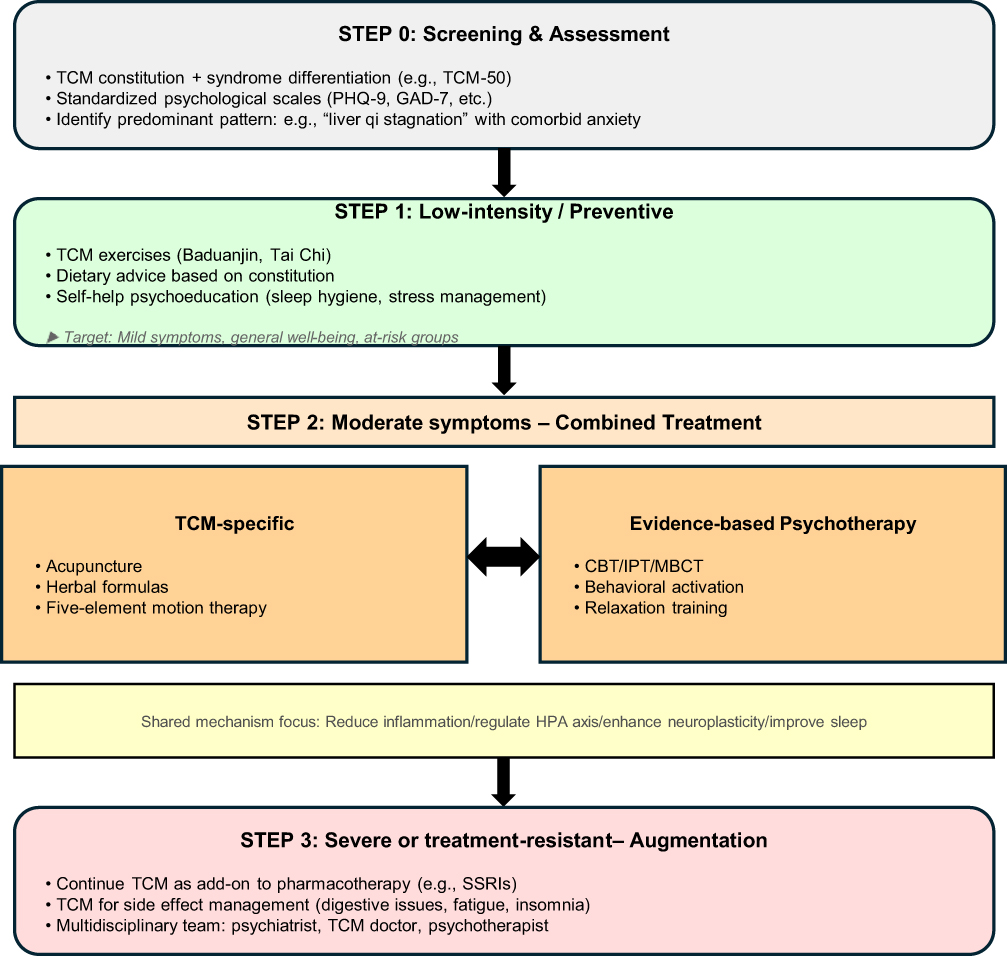 |
Figure 1 A proposed stepped model for integrating TCM and Western psychotherapy in mental health care. |
Mechanistic and Diagnostic Insights
Pathological Mechanisms (Level 2 Evidence)
Traditional Chinese Medicine (TCM) provides a paradigm to think about mental disorders in which the mind and the body are in a union. Mechanistically, there are a number of research efforts trying to look for some possible biological mechanism by which the approaches of TCM might work in the context of mental. We need to point out that the evidences below are mostly from animal studies, and they should be verified in the human population first before any clinical use.
Concerning neuroinflammatory mechanisms, Fang and others showed that the Xiaoyao Pill reduced the inflammation and protected the neuronal cell death of hippocampal neurons induced by lipopolysaccharide. The herbal preparation was able to reduce the expression of the pro-inflammatory cytokines IL-6 and TNF-α and to increase the concentrations of brain derived neurotrophic factor (BDNF).27 These observations agree with the TCM that suppose that some emotional dysregulation can cause the stagnation of the liver qi and can produce the internal heat and phlegm-dampness and can cause the mental disease.
Neurogenesis and signaling mechanisms. For instance, in a rodent model of post-stroke depression, Tian et al found that treating YNJYP increased the neuronal regeneration by modulating the Notch signaling cascade and decreased the behaviors of depression.19 These information about the underlying mechanisms suggests the possible convergences between the conception of the traditional Chinese medicine and the recent neurobiological research, but it has to be verified by clinical trials in human.
Gut-brain axis regulation. Qu et al investigated the effect of a Chinese herbal formulation in rats exposed to chronic unpredictable mild stress. The intervention was able to correct the stress-induced disruption of the gut microbiota composition and ameliorate the depressive-like symptoms of the animals, in particular, by changing the proportions of the Firmicutes and Bacteroidetes, which are the bacterial phyla involved in the regulation of the emotions.20 This is a new perspective on the possible ways by which TCM could influence the psychiatric conditions working on the gut microbiome, but still it is necessary to see this from the studies performed on humans.
Constitutional predispositions. Yap et al found in a sample of university students in Malaysia a relation between a Qi-stagnation constitutional type and depressive symptoms (B = 0.089, P = 0.011).28 This suggests that some constitutional patterns could be predispositions for some psychological condition. Since in that work, the methodological approach was cross-sectional (this gives level 3 of evidence), it is not possible to say about causation.
Diagnostic Approaches (Level 3 Evidence)
The basis of the Traditional Chinese Medicine diagnosis is the four diagnostic methods: observation, auscultation and olfaction, questioning, and palpation. The classical TCM diagnosis intend to collect the data of the patient, but they are usually full of subjectivity and the variation of interpretation. The development of nowadays is to combine the basic thoughts of TCM diagnosis with the modern technology tools.
Standardized Assessment Instruments
The survey tool of the TCM-50, based on TCM health preservation in general, presents good measurement characteristics (Cronbach’s alpha coefficient 0.927). The TCM-50 provides a systematic way for assessing the full wellness, including the aspect of the psychological health.12 Zhou et al constructed another questionnaire based on TCM theory. It also demonstrated good internal consistency (α=0.83). Authors found ten separate components that are related with different mental health indicators.29
Neuroimaging and Ocular Assessment
As a preliminary study (Level 3 evidence), Zhu and others have studied the retinal characteristics in 29 people with schizophrenia and 25 people without the disorder. They have described a thinning of the central retinal region which is inversely related to the degree of the negative symptoms.21 In TCM, the eyes are linked to internal organs by the meridian way. This means that the eyes could provide us some information of the assessment about both the physical and the psychological well-being. However, these results are only suggestive and need to be confirmed by more extensive, prospective work.
Artificial Intelligence and Machine Learning
Guo et al discussed the possible uses of large language model in the situation of the intelligent diagnostics and therapy in the TCM.30 They found that the artificial intelligence can help to analyze the symptoms reported by the patients and find the relationship of the minds and the body.30 Tian et al built an online system for the assessment of the risk of the psychological distress of the people with the lung cancer. The machine learning models they used showed the powerful ability to differentiate the different level of risk.31 Such technological approaches are possible to make more standard mental health evaluation based on TCM, but at present, it is still in the preliminary stages of research and development.
Summary of Mechanistic and Diagnostic Evidence
In summary, for the research of mechanisms (Level 2 evidence) it is suggested that TCM approaches could possibly influence processes such as the neuroinflammation, the generation of new neurons, and the composition of the bacteria in the gut. Although, in general, this is based on studies performed with animals and it needs to be confirmed in human trials. For diagnostic methods (Level 3 evidence), the field is using the standardized tools of assessment and some new technologies, such as brain imaging and artificial intelligence. It must be underlined that these are only first, exploratory studies, and so they cannot be considered as a proof of working of the therapy. Each of these domain needs more investigations with more robust and methodologically solid research design.
Controversies and Methodological Limitations
Scientific Validity of TCM Psychotherapy
The scientific credibility of psychological treatments based on Traditional Chinese Medicine remains debated. Indeed, the skeptics claim that some basic TCM concepts such as the balance of Yin and Yang, the theory of the Five elements, the notion of Qi and the meridian system, lack a clear basis in current biomedical research and are hard to bring in line with known psychology.32 The difference of the founding concepts is a problem for the discussion between different disciplines. It is also a problem for the research that is to be done in order to follow the methodological strictness necessary in the medical practice of the evidence-based, but at the same time, to keep the integrative and holistic that is at the heart of TCM.
Meanwhile, advocates point to the increasing preclinical and clinical data that show the way of TCM could have some quantifiable biological effect. For example, the plant-based compounds that can be extracted from TCM herbs have effects like antidepressants via some way, eg, modulating neurotransmitters, regulating hypothalamic-pituitary-adrenal (HPA) axis, showing anti-inflammation, and stimulating neurogenesis.33 The results are consistent with a holistic view, but the majority are from preclinical. To see whether the mechanism knowledge would bring important clinical benefit for patients, well-done clinical trials are needed.
Challenges in Integration
A number of practical and conceptual obstacles hinder the combination of TCM with clinical psychology.
Philosophical Distinctions
TCM adopts a holistic and energy-based view of the functions of the body and the process of the disease. Clinical psychology, on the other hand, is based on Western empirical traditions, which focus on systematic observation, exact measurement and a detailed analysis of the different psychological events. These “foundational differences” put difficulties in the direct mapping of TCM constructs, like meridians and Qi, to the terminology used in the clinical psychology.32
Absence of Uniform Diagnostic Standards
The fact that TCM is in the focus of syndrome differentiation. Syndrome differentiation is a process that naturally deals with important individual variability. Different TCM practitioners may diagnose the same individual with different syndromes, and there are not uniform, recognized criteria to define the syndromes (eg. liver qi stagnation or heart-spleen deficiency) in the framework of the RCT methodologies.34 This diminishes the comparability between different research efforts and it adds to the complexity of the meta-analytic reviews.
Methodological Quality of Current Research
Most of the published investigations of the integration of traditional Chinese medicine and psychotherapy are with small number of participants, inadequate blinding procedures and not optimal study designs. For these reasons, it is difficult to make definite judgments on treatment effectiveness or safety.34 The lack of such scientific data is a big obstacle for the wider implementation in the clinical practice.
Insufficient Interdisciplinary Training
There is a shortage of health-care professionals that are qualified in both TCM and psychotherapy. This is a problem not only for the practical provision of co-treatments, but also for the creation of methodologically solid interdisciplinary research projects.
Recurring Methodological Limitations
A careful review of the literature examined above shows a number of still present methodological weaknesses. These are enough to strongly diminish the reliability and the force of any inferences that can be made about the possible integration of TCM with psychotherapeutic approaches.
Sample Size and Statistical Power
As shown in Table 2, most of the randomized controlled trials (RCTs) have less than 100 sample in each treatment group, and many of them have less than 50. The small sample reduces the statistical power to identify the moderate treatment effect and increase the probability to get the false-positive result. For example, in the study reported by Fogarty et al, there are only 35 subjects in the crossover trial,13 and in the study reported by Lv et al, there are 30 individuals in each arm.23 The report rarely has post-hoc analyses of the statistical power.
Blinding and Sham Controls
The extent to which blinding can be implemented for acupuncture and the exercise therapy of Traditional Chinese Medicine (TCM) is generally considered as a big problem. A small number of studies used the sham acupuncture device or plausible placebo herbal preparation. In the case of no proper blinding, the magnitude of the treatment effect that is observed might be inflated because of the expectation of participants and researchers. This inflation is in particular likely for subjective measures, for instance, scores on inventories of depression and anxiety.9
Variability in TCM Diagnostic Standards
As we mentioned above, the lack of homogeneous criteria for the differentiation of the syndrome complicates the comparison of the different studies and the meta-analysis is more difficult. If the same clinical conditions are addressed by the different investigations, they may have the different choices of the acupuncture points, herbal prescriptions or exercise.
Bias in Publication
The studies that have a good result are published more than the studies with no or bad result. This is particularly the case for the field of complementary medicine where the literature is full of small studies with a good effect. In their meta-analysis, Ruan et al have seen a sum of the SMD of the −2.05; but they said that the asymmetry of the funnel plot shows that there could be some publication bias.10
Limited Duration of Follow-Up
Most of the studies only follow-ups their participants for 4 to 12 weeks after the intervention. It is still not clear whether the combination of TCM and psychotherapy would provide benefits that is longer than six months.
Implications for the Field
The fact that there are these methodological constraints does not mean that it is not possible to see the value of the use of traditional Chinese medicine together with psychotherapy. However, it does mean that the field needs:
Control groups that are standardized (eg. sham acupuncture or convincing placebo interventions) to distinguish specific therapeutic effects from general or contextual effects.
In the studies looking at the practice of TCM exercise, we found that some included an active control condition (eg. stretching routine, or light walking) to see whether the observed benefit is specifically due to the mind-body aspect.
Studies involving larger participant numbers, with sample size calculations determined and registered prior to commencement.
Extended observation periods (six months or more) to evaluate the persistence of any benefits.
Prospective registration of clinical trials to reduce publication bias and enhance research transparency.
Checking of the results that were first reported by the single teams of the research, independently, in the best case also in different geographical and cultural contexts.
Without these methodological improvements, the discipline is at the risk of overestimating the perceived impacts of the treatments and to get conclusions of the effectiveness of the integration of TCM-psychotherapy that are not well supported.
Future Directions and Conclusion
Future Research Priorities
Based on the evidence synthesized and on the methodological problems mentioned, a number of important issues for future research emerge.
First of all, large, well-blinded randomized controlled trials are urgently needed. In subsequent RCTs, sham acupuncture or convincing placebos comparators should be included, pre-specified TCM syndrome classification standards should be used, and sufficient numbers of participants should be determined by preliminary statistical power analyses. Using multi-center study designs would also make the findings more applicable to other populations.
Furthermore, we need to develop and verify outcome assessment tools for TCM principles. Currently, we still do not have validated instruments that can measure the overall, constitution-oriented concepts that are at the core of TCM. The establishment of such measurement tools will allow the investigators to measure results that are meaningful for both TCM and conventional biomedical view point.
Third, longer follow-up periods should be implemented. In the present work, most of the results are reported just after the end of the interventions, from four to twelve weeks. It is not verified that the therapeutic benefit persists after six months. Future experiments should include the evaluation at six and one year.
Fourth, we need to improve the quality of reporting. The investigators need to report according to the CONSORT standards for trials of non-pharmacological measures that we should account for the way in which randomization was performed, the way in which the assignment of group was concealed, and the way in which those who assess the outcome of the patients are blinding, and that the analyses are done according to the intention-to-treat.
Fifth, the setting up of cross disciplines educational programs are proposed as well. So far, only few practitioners have the formal training in both TCM and psychotherapy based on the empirical evidence. Educational tracks that train for both domains would help the rigorous scientific work and the provision of unified patient care.
Sixth, the trial pre-registration should be implemented. The prospective registration of the clinical studies should be required, because this would lead to less publication bias and to better research transparency. Readers would be able to distinguish between the outcomes that were pre-specified in the study protocol and the ones that have been found with post-hoc analyses.
Conclusion
The present narrative review has been a critical review of the evidence for the inclusion of TCM in combination with Western psychotherapeutic approaches in mental health care. Based on the literature synthesized we can give the following tiered conclusions.
Evidence That is Relatively Well-Established by Existing Research
Several small-to-moderate randomized controlled trials and meta-analytic reviews have indicated that the use of the acupuncture in addition to the drug-based or psychotherapeutic standard of care interventional might be able to ameliorate the manifestations of mild-to-moderate depression and anxiety at a short term of observation, for a few weeks for up to twelve weeks. One of the meta-analyses that include 18 randomized controlled trials has calculated the combined effect size of −2.05 with 95% confidence interval of −2.74 to −1.37 concerning for comprehensive TCM wellness programs targeting depressive symptoms.10 The practices of TCM, in particular of Baduanjin and Tai Chi, have reliable positive effects on the attentional capacity, the perceived life satisfaction and the low level of anxiety for the community living non clinical groups. For example, one particular randomized controlled trial reported statistically significant differences between the intervention and the control arms (P = 0.034).14 Systematic reviews confirm these findings, but the methodological rigor of the original research underlying is often limited.
Preliminary Nature of the Existing Evidence
The combination of TCM with psychotherapy for, for example, post-traumatic stress disorder, for serious psychiatric disorders (bipolar disorder and schizophrenia etc), and for persistent insomnias, is so far not well researched and is not free of methodological drawbacks. The investigations done are to a large extent small scale, not done with blinding, and mostly do not have placebo or active controls.22,23,25,26 Exploratory work of mechanisms, for example, with gut microbiome alteration, neuroimaging finding and inflammatory pathways, etc. is promising but at the preliminary state. These findings have not yet become to be known as established clinical biomarkers or submitted to the treatment protocol.18–21 Data from animals cannot be transferred to the human clinical population. Information of long term-effects (six months or longer) is almost missing, as most trials assessed outcomes immediately post-treatment.
Major Obstacles Hindering Progress in This Area
First, since there is no yet an established and validated way of implementing the TCM syndrome differentiation in RCTs, there is a lot of variability and low reproducibility between the different researchers’ efforts.34 Second, most of the investigations are characterized by small number of participants (usually less than 50 in each treatment group), not enough use (if any) of sham acupuncture or placebo comparison condition, not enough blinding of those that assess the outcomes, and possible publication bias, as shown by the asymmetrical funnel plots in some of the key meta-analytic reviews.9,10 Third, there are deep theoretical differences (TCM is holistic and energy based, while Western psychotherapy is in a mechanism based and empirically driven way) which are strong barriers to a good Dialogue and Synthesis.32,34 Fourth, there is a lack of practitioners who are good in both TCM and in the evidence based psychotherapeutic methods that can use the researches insights in the real clinical work. Fifth, there is not yet a validated outcome measure for TCM in the specific context of mental health studies, so the researchers have to rely on the assessment tools that have been developed for the Western models of psychopathology.
The combination of traditional Chinese medicine with psychotherapy represents a conceptually attractive and patient-oriented model for mental healthcare. However, the current work is limited by important methodological shortcomings. The most supportive is for acupuncture and TCM based physical exercises for the treatment of depression and anxiety. The benefit is seen in the short time of follow-up, from 4 to 12 weeks. For other disorders, eg. post-traumatic stress disorder and severe mental illness and for the outcomes for six months or more the evidence base is still emerging and is preliminary.
The field is still at an early stage, and shows potential but needs to be developed with care. There is an urgent requirement for well-designed and robust research before such integrated approaches can be recommended for standard clinical use. If there is no improvement in methodological rigor, in the choice of the comparator conditions, in the number of participants, in the length of the follow up and in the transparency of the way the reporting is done, there is a risk of inflating the perceived therapeutic benefits and to reach premature judgments. On the contrary, should these improvements be done, the combination of traditional Chinese medicine and psychotherapy could become a possible supplement of the field of mental health treatments. It would be interesting for those who are looking for more comprehensiveness of care with not too much adverse effects.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ilbay G, Dogan ZI, Balıkcı A, Erdogan S, Karaoglan Kahilogulları A. Effects of postnatal caffeine exposure on absence epilepsy and comorbid depression: results of a study in WAG/Rij rats. Brain Sci. 2022;12(3):361. doi:10.3390/brainsci12030361
2. Lai NS, Lu MC, Chang HH, et al. Association of Traditional Chinese medicine body constitution and health-related quality of life in female patients with systemic lupus erythematosus: a cross-sectional study. Evid Based Complement Alternat Med. 2021;2021:5568219. doi:10.1155/2021/5568219
3. Dong S, Wang Y, Wei H, et al. Effects of baduanjin exercise on rehabilitation of patients with mild to moderate Parkinson’s disease. Front Neurosci. 2022;15:827180. doi:10.3389/fnins.2021.827180
4. You Y, Min L, Tang M, Chen Y, Ma X. Tai Chi research from 1980 to 2020: a bibliometric analysis of global scientific outputs and research trends. Int J Environ Res Public Health. 2021;18(11):6150. doi:10.3390/ijerph18116150
5. You Y, Liu J, Tang M, Wang D, Ma X. Effects of Tai Chi exercise on improving walking function and posture control in elderly patients with knee osteoarthritis: a systematic review and meta-analysis. Medicine. 2021;100(16):e25655. doi:10.1097/MD.0000000000025655
6. Li X, Wang X, Song L, et al. Effects of Qigong, Tai Chi, acupuncture, and Tuina on cancer-related fatigue for breast cancer patients: a protocol of systematic review and meta-analysis. Medicine. 2020;99(45):e23016. doi:10.1097/MD.0000000000023016
7. Deng C, Chen H, Meng Z, Meng S. Roles of traditional Chinese medicine regulating neuroendocrinology on AD treatment. Front Endocrinol. 2022;13:955618. doi:10.3389/fendo.2022.955618
8. Zhang X, Wang M, Qiao Y, et al. Exploring the mechanisms of action of Cordyceps sinensis for the treatment of depression using network pharmacology and molecular docking. Ann Transl Med. 2022;10(6):282. doi:10.21037/atm-22-762
9. Yang L, Zhang Q, Wen M, et al. Clinical evidence for acupuncture-assisted treatment of depression: a systematic review and meta-analysis with meta-regression. Gen Hosp Psychiatry. 2025;97:64–14. doi:10.1016/j.genhosppsych.2025.09.002
10. Ruan J, Chen S, Liang J, et al. TCM-based integrated health interventions for depression: a systematic review and meta-analysis. J Clin Nurs. 2023;32(17–18):5632–5651. doi:10.1111/jocn.16666
11. Wu Y, Huang J, Guo J, Lian W, Suo M. Drug repurposing in traditional Chinese medicine: from empirical wisdom to modern therapeutic strategies. Front Pharmacol. 2025;16:1631727. doi:10.3389/fphar.2025.1631727
12. Zhang H-M, Bai M-H, Wang Q. Development, reliability and validity of TCM health self-evaluation scale (TCM-50). Chin J Integr Med. 2017;23(5):350–356. doi:10.1007/s11655-014-1853-z
13. Fogarty S, Stojanovska L, Harris D, et al. A randomised cross-over pilot study investigating the use of acupuncture to promote weight loss and mental health in overweight and obese individuals participating in a weight loss program. Eat Weight Disord. 2015;20(3):379–387. doi:10.1007/s40519-014-0175-7
14. Li M, Fang Q, Li J, et al. The effect of Chinese traditional exercise-baduanjin on physical and psychological well-being of college students: a randomized controlled trial. PLoS One. 2015;10(7):e0130544. doi:10.1371/journal.pone.0130544
15. Ling Y, Yang D, Shao W. Understanding vomiting from the perspective of TCM. Ann Palliat Med. 2012;1(2):143–160. doi:10.3978/j.issn.2224-5820.2012.07.03
16. Lv H, Zhu L, Chen Z, et al. Physical and mental health conditions of young college students with different TCM constitutions in zhejiang province of China. J Tradit Chin Med = Chung Tsa Chih Ying Wen Pan. 2015;35(6):703–708.
17. Ma S, Qu S, Huang Y, et al. Improvement in quality of life in depressed patients following verum acupuncture or electroacupuncture plus paroxetine: a randomized controlled study of 157 cases. Neural Regener Res. 2012;7(27):2123–2129.
18. Tian J, Liu C, Xiang H, et al. Investigation on the antidepressant effect of sea buckthorn seed oil through the GC-MS-based metabolomics approach coupled with multivariate analysis. Food Funct. 2015;6(11):3585–3592. doi:10.1039/C5FO00695C
19. Tian H, Li X, Tang Q, et al. Yi-nao-jie-yu prescription exerts a positive effect on neurogenesis by regulating notch signals in the hippocampus of post-stroke depression rats. Front Psychiatry. 2018;9:483. doi:10.3389/fpsyt.2018.00483
20. Qu W, Liu S, Zhang W, et al. Impact of TCM treatment on chronic unpredictable mild stress-induced depression-like behaviors: intestinal microbiota and gut microbiome function. Food Funct. 2019;10(9):5886–5897. doi:10.1039/C9FO00399A
21. Zhu J, Wang Z, Chen T, et al. Thinning of central foveal thickness in the retina of patients with schizophrenia. Eur Arch Psychiatry Clin Neurosci. 2025;275(3):839–849. doi:10.1007/s00406-024-01943-4
22. Xie L, Zi Y. Application of psychotherapy based on five-element theory in TCM in improving the mental states of patients with post-stroke depression. Actas Esp Psiquiatr. 2024;52(4):542–548. doi:10.62641/aep.v52i4.1801
23. Lv X, Wang B, Chen Jianbin N, et al. clinical observation of depression after breast cancer operation treated with aurieular point sticking therapy. Zhongguo Zhen Jiu. 2015;35(5):447–450.
24. Liang R, Tang L, Li L, et al. The effect of pressing needle therapy on depression, anxiety, and sleep for patients in convalescence from COVID-19. Front Neurol. 2024;15:1481557. doi:10.3389/fneur.2024.1481557
25. Hong C, Efferth T. Systematic review on post-traumatic stress disorder among survivors of the wenchuan earthquake. Trauma Violence Abuse. 2016;17(5):542–561. doi:10.1177/1524838015585313
26. C R-OES, Windthorst P, Denkinger J, et al. Chronic pain in refugees with posttraumatic stress disorder (PTSD): a systematic review on patients’ characteristics and specific interventions. J Psychosom Res. 2019;118:83–97. doi:10.1016/j.jpsychores.2018.07.014
27. Fang Y, Shi B, Liu X, et al. Xiaoyao pills attenuate inflammation and nerve injury induced by lipopolysaccharide in hippocampal neurons In vitro. Neural Plast. 2020;2020:8841332. doi:10.1155/2020/8841332
28. Yap SY, Foo CN, Lim YM, et al. TCM body constitutions and psychological determinants of depression among university students in Malaysia: a pilot study. Int J Environ Res Public Health. 2021;18(10):5366. doi:10.3390/ijerph18105366
29. Zhou X, Xu F, Gao J, et al. Development and preliminary validation of the questionnaire (the first edition) based on TCM for detecting health status in China. Evid-Based Complement Altern Med: eCAM. 2015;2015:863685. doi:10.1155/2015/863685
30. Guo Y, Wang H, Ren X, et al. Can GPTs accelerate the development of intelligent diagnosis and treatment in TCM? A survey and empirical analysis. J Evidence Based Med. 2025;18(1):e70004. doi:10.1111/jebm.70004
31. Tian X, Li H, Li F, et al. Development and validation of a web-based calculator for determining the risk of psychological distress based on machine learning algorithms: a cross-sectional study of 342 lung cancer patients. Support Care Cancer. 2024;33(1):63.
32. Aung SKH, Fay H, Hobbs RF. TCM as a basis for treating psychiatric disorders: a review of theory with illustrative cases. Med Acupunct. 2013;25(6):398–406. doi:10.1089/acu.2013.1007
33. Zhao R, Wang J, Chung SK, et al. New insights into anti-depression effects of bioactive phytochemicals. Pharmacol Res. 2025;212:107566. doi:10.1016/j.phrs.2024.107566
34. Chen Q, Wang Q, Ding S, et al. Problems lowering the study quality in traditional medicine, introspection from an example of meta-analysis of acupuncture. BMC Complementary Med Ther. 2020;20(1):41. doi:10.1186/s12906-019-2806-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.