Back to Journals » Advances in Medical Education and Practice » Volume 16
Integrating Virtual Patients Into Preclinical Education to Enhance Early Clinical Exposure and Skill Acquisition in Medical Students
Authors Abuamara TMM ![]() , Abd-Elhay WM, AL-Ghamdi HS, Alghamdi MA, Baloush RAA, Mirdad DSA, Bawahab AA, Abd El Malik Hassan M
, Abd-Elhay WM, AL-Ghamdi HS, Alghamdi MA, Baloush RAA, Mirdad DSA, Bawahab AA, Abd El Malik Hassan M ![]() , Al-bawah N
, Al-bawah N
Received 4 May 2025
Accepted for publication 19 September 2025
Published 24 September 2025 Volume 2025:16 Pages 1705—1715
DOI https://doi.org/10.2147/AMEP.S538309
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Tamer MM Abuamara,1,2 Wagih M Abd-Elhay,2 Hasan S AL-Ghamdi,3 Mohammad A Alghamdi,3 Razan Abed A Baloush,4 Dahlia Soleman A Mirdad,4 Ahmed Abdulwahab Bawahab,4 Mohammed Abd El Malik Hassan,5 Naji Al-bawah6
1Center of Oral Diseases Studies, Faculty of Dentistry, Al-Ahliyya Amman University (AAU), Amman, Jordan; 2Histology Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt; 3Internal Medicine Department, Division of Dermatology, Faculty of Medicine, Al-Baha University, Al-Baha, Kingdom of Saudi Arabia; 4Department of Basic Medical Sciences, Pathology Division, College of Medicine, University of Jeddah, Jeddah, Saudi Arabia; 5Pediatrics Department, Faculty of Medicine, Al-Azhar University, Cairo, Egypt; 6Faculty of Medicine, Sana’a University, Sana’a, Yemen
Correspondence: Naji Al-bawah, Faculty of medicine, Sana’a University, Sana’a, 13078, Yemen, Email [email protected]
Background: Virtual patients (VPs) have traditionally been utilized in clinical education rather than in preclinical instruction. However, limited research has evaluated the effectiveness of VP-based sessions in enhancing early clinical exposure (ECE) during the preclinical years.
Aim: To assess the impact of VP-based tutorials in supplementing the Clinical Skills module for second-year medical students.
Methods: In this prospective study, the effectiveness of VP-based tutorials was compared to conventional lecture-based teaching within the Clinical Skills module. All second-year medical students enrolled during the 2022/2023 and 2023/2024 academic years were included. The 2022/2023 cohort (Group 1) received traditional lectures, while the 2023/2024 cohort (Group 2) participated in VP-based tutorials. Student performance was evaluated using pre- and post-module tests and formative Objective Structured Clinical Examination (OSCE) scores.
Results: Baseline performance showed no significant difference in pre-module test scores between Group 1 (26.55 ± 22.45%) and Group 2 (27.13 ± 26.21%) (p = 0.681). Both groups demonstrated significant improvements in post-module scores (Group 1: 73.88 ± 15.11%; Group 2: 75.01 ± 10.09%, p< 0.0001 for both), with no significant difference between the two (p = 0.129). However, Group 2 achieved significantly higher OSCE scores compared to Group 1 (82.62 ± 11.03% vs 75.80 ± 14.38%, p< 0.0001).
Conclusion: This study highlights the value of incorporating virtual patients into preclinical education. VP-based tutorials significantly enhance clinical skill development and facilitate early clinical exposure, offering a promising adjunct to traditional teaching methods in preclinical curricula.
Keywords: virtual patients, medical education, early clinical exposure, preclinical medical education, clinical skills
Introduction
Early clinical exposure (ECE) is a teaching and learning strategy that encourages medical students to interact with patients as early as their first year.1 Although the concept dates back to the late nineteenth century—when modern medical education began—its implementation has evolved considerably.2,3 Historically, medical education was predominantly lecture-based, with limited opportunities for hands-on experience.4 By the end of the nineteenth century, however, educators increasingly recognized the need for practical training to better prepare students for clinical practice.5–8
Numerous studies have shown that ECE motivates students and enhances academic performance, clinical competence, communication skills, and self-confidence.9–15 The evolution of ECE reflects ongoing efforts to develop innovative strategies that equip students with the knowledge, skills, and attitudes essential for becoming competent, empathetic physicians.10
Despite its advantages, ECE faces several challenges, including: (1) limited resources; (2) concerns about student and patient safety; (3) cultural barriers; and (4) the need for integration with both basic science and clinical curricula.5
To address these limitations, we advocate for the integration of virtual patients (VPs) into preclinical education. VPs are computer-based programs designed to simulate real-life clinical scenarios, facilitating learning in a safe and controlled environment.16,17 While VPs have traditionally been used in clinical phases of education, their application in the preclinical years remains underexplored.18 This study investigates the effectiveness of VP-based sessions in supplementing early clinical exposure within the Clinical Skills module during the preclinical phase of medical education. The term “virtual patients” in this study refers to structured, computer-assisted simulation scenarios delivered in the Clinical Skills Laboratory using high-fidelity mannequins with integrated physiological response systems. These scenarios were designed to replicate authentic patient encounters in a safe, controlled setting, allowing students to practice history-taking, physical examination, and clinical decision-making without risk to actual patients. Such simulation-based VP formats have been shown to bridge the gap between theoretical knowledge and clinical application by providing realistic, repeatable, and feedback-driven practice opportunities.
Materials and Methods
Study Design and Ethics
This prospective, comparative study was conducted at the Faculty of Medicine, Al-Azhar University (Cairo, Egypt) from September 2022 to September 2024, in collaboration with the University of Jeddah and Al-Baha University (KSA). Ethical approval was obtained from the Al-Azhar University Ethics Committee, and written informed consent was obtained from all participants. The required sample size was calculated using GPower version 3.1.9.7, assuming a medium effect size (Cohen’s d = 0.5), α = 0.05, and power = 80%, which indicated that at least 1,200 participants (600 per group) were needed. Our study cohorts met this requirement, with 599 students in Group 1 and 597 students in Group 2.
Participants
Second-year medical students enrolled in the Clinical Skills module during the 2022/2023 and 2023/2024 academic years were included. Foreign students and repeaters were excluded. Group 1 (2022/2023) comprised 599 students; Group 2 (2023/2024) comprised 597 students.
Module Structure and Cohorts
The Clinical Skills module ran over 15 weeks, with seven lecture topics delivered in the first seven weeks alongside eight weekly real-patient clinical sessions. In 2022/2023 (Group 1), the seven topics were taught as traditional lectures; in 2023/2024 (Group 2), these lectures were replaced by virtual patient (VP)–based tutorials conducted in the on-campus skills laboratory using computer-based scenarios integrated with mannequins. Both groups received the same eight clinical sessions in identical sequence and content, in groups of approximately 25 students.
Intervention Virtual Patient Tutorials
In the intervention cohort (Group 2), teaching was delivered using interactive computer-based virtual patient (VP) cases as the core instructional method. Each VP case simulated a realistic clinical encounter, guiding students through sequential history-taking, examination findings, investigations, and clinical reasoning steps in a branching format. These cases were designed to align with the module’s learning objectives and mapped to the blueprint for assessments.
To complement the VP cases, selected procedural skills were demonstrated using mannequins (eg, cardiovascular and respiratory examination) within the same tutorial session. The mannequin component was used solely to illustrate and reinforce key examination techniques presented in the VP scenario; it did not constitute an independent simulation module. This ensured that the VP remained the primary educational strategy while providing students with relevant hands-on reinforcement.
Seven Lecture Topics and Learning Objectives
Each topic was linked to specific learning objectives (LOs) across cognitive, psychomotor, and affective domains. The wording below follows the original module blueprint, with only essential grammar corrections:
- General medical history – define components (personal history, presenting complaints, past history, family history) [Remember]; explain their significance [Understand]; differentiate subjective from objective data [Analyse]; take a complete history [Apply]; prioritize presenting complaints [Evaluate]; demonstrate empathy, confidentiality, and cultural sensitivity [Affective].
- General medical examination – list the main steps (inspection, palpation, percussion, auscultation) [Remember]; describe normal findings [Understand]; identify abnormal signs [Analyse]; perform systematic examination [Apply]; integrate findings with history to reach a diagnosis [Evaluate]; respect patient privacy and dignity [Affective].
- Neurological disorders – enumerate history components [Remember]; describe the neurological examination (mental status, cranial nerves, motor, sensory, coordination, reflexes) [Understand]; differentiate upper from lower motor neuron lesions [Analyse]; perform neurological examination [Apply]; localize lesions based on findings [Evaluate]; maintain empathy and professionalism [Affective].
- Abdominal disorders – list history elements [Remember]; explain the significance of symptoms [Understand]; describe the examination sequence [Understand]; perform complete abdominal examination [Apply]; differentiate between acute and chronic abdominal conditions [Analyse]; integrate findings into differential diagnosis [Evaluate]; uphold patient dignity [Affective].
- Cardiovascular disorders – list targeted history components [Remember]; explain symptom–pathophysiology relationships [Understand]; describe cardiovascular examination [Understand]; perform focused examination [Apply]; differentiate normal and abnormal signs (heart sounds, jugular venous pressure) [Analyse]; integrate findings into a working diagnosis [Evaluate]; ensure patient comfort [Affective].
- Chest disorders – list history elements (cough, dyspnea, chest pain, hemoptysis) [Remember]; explain symptom significance [Understand]; describe respiratory examination [Understand]; perform systematic chest examination [Apply]; differentiate abnormal respiratory signs [Analyse]; integrate findings into diagnosis [Evaluate]; demonstrate cultural sensitivity [Affective].
- Differences between adult and pediatric history/examination – list differences [Remember]; explain developmental influences [Understand]; describe modifications for children [Understand]; perform pediatric examination with caregiver engagement [Apply]; differentiate normal developmental variations from pathology [Analyse]; integrate findings into pediatric impressions [Evaluate]; communicate effectively and patiently [Affective].
VP-Based Tutorial Format
Each VP tutorial lasted 55 minutes and followed a standard format: Introduction (5 min) – review objectives and session plan; Main activity (40 min) – group discussion of computer-based clinical scenarios with integrated mannequin demonstrations, guided by open-ended questions to stimulate reasoning; Wrap-up (10 min) – summarize key points, address misconceptions, and provide feedback. Facilitators emphasized active participation, equitable discussion, respect for peers, and safe learning environments. Mini-assessments (short quizzes, one-minute papers) and verbal feedback were used to reinforce learning.
Communication of Learning Objectives
At module commencement, LOs were presented verbally, displayed on initial slides, and included in the course handbook. Facilitators related objectives to clinical relevance, broke complex objectives into measurable tasks, and explicitly linked them to assessment formats (SBA and OSCE).
Assessments
Written test – 50 single-best-answer (SBA) questions mapped to the LOs and module blueprint, reviewed by senior faculty for content validity. The same questions, in a different order, were administered pre- and post-module to allow direct comparison without difficulty variation.Example SBA: “A 35-year-old man presents with fatigue. The physician asks about occupation, lifestyle, and marital status. Which history component is this?”
Formative OSCE – Ten stations: four history-taking, four examination, two differential diagnosis, using real patients where possible and mannequins when required. Pathologies, station scripts, and marking criteria were identical for both cohorts. Example OSCE station: Focused history for chest complaints (8 min) with a 20-mark checklist covering history of present illness, risk factors, past/family history, and social history.
Study Flow and Timing
Week 1: introduction to LOs and pre-test SBA. Weeks 2–7: lectures (Group 1) or VP tutorials (Group 2). Weeks 8–15: clinical sessions. Week 15: post-test SBA and OSCE. The sequence of activities for both cohorts is illustrated in Figure 1.
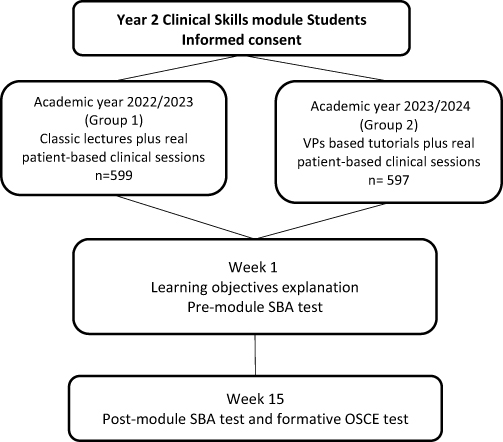 |
Figure 1 Schematic illustration of the study design. |
Statistical Analysis
Data were analyzed using SPSS for Windows, version 22.0 (IBM, Armonk, NY, USA). An independent t-test was used to compare the mean scores of pre- and post-module assessments within and between groups. A p-value of <0.05 was considered statistically significant.
Results
A total of 1,196 students participated in the study, with 599 in Group 1 and 597 in Group 2. Both groups were comparable at baseline, as indicated by pre-module test scores: Group 1 scored 26.55 ± 22.45% and Group 2 scored 27.13 ± 26.21% (p = 0.681).
After completion of the 15-week module, post-module test scores improved significantly within each group. Group 1 improved from 26.55 ± 22.45% to 73.88 ± 15.11% (p < 0.0001), and Group 2 from 27.13 ± 26.21% to 75.01 ± 10.09% (p < 0.0001). There was no statistically significant difference between groups in post-module test scores (p = 0.129).
When assessing performance in the formative OSCE, Group 2 achieved significantly higher scores compared to Group 1 (82.62 ± 11.03% vs 75.80 ± 14.38%, p < 0.0001).
Performance by Cognitive Domain
Analysis by cognitive level (based on 50 SBA items) showed significant gains across all domains — Remembering, Understanding, and Applying/Higher-order thinking — in both groups (all p < 0.0001). For example, in Group 1, “Remembering” scores increased from 6.28 ± 2.7 to 18.98 ± 4.2, and in Group 2 from 6.41 ± 0.3 to 19.38 ± 4.4. The “Applying and higher” domain showed the greatest relative improvement, particularly in Group 2 (2.15 ± 0.2 to 7.28 ± 1.3).
Comparisons between groups at baseline revealed no significant differences in any cognitive domain. However, in the post-module assessment, Group 2 scored significantly higher in the “Applying and higher” category (p < 0.0001).
OSCE Skills Performance
The OSCE consisted of 10 stations assessing procedural and clinical skills mapped to module objectives. Both groups showed strong performance across domains, but Group 2 consistently scored higher in stations targeting application and integration of skills, in line with the enhanced virtual patient component.
Lecture Topics and Learning Objectives
The module comprised seven lecture topics, each designed with explicit learning objectives to ensure constructive alignment with assessments:
- Basic life support – Perform CPR and use an automated external defibrillator according to current guidelines (Applying).
- History taking – Elicit a complete, focused medical history tailored to the presenting complaint (Understanding/Applying).
- Physical examination – Perform systematic examination of the cardiovascular, respiratory, and abdominal systems (Applying).
- Vital signs measurement – Accurately measure and interpret temperature, pulse, blood pressure, and respiratory rate (Remembering/Applying).
- Venipuncture and injection techniques – Demonstrate correct procedures for intravenous access and intramuscular injection (Applying).
- Urinary catheterization – Insert and manage a urinary catheter in male and female models, respecting aseptic technique (Applying).
- Basic wound care – Clean, dress, and suture simple wounds in simulation models (Applying).
These objectives were explicitly linked to the MCQ blueprint and OSCE checklists to ensure consistency between teaching, learning, and assessment.
The comparable baseline and overall post-module scores between the two groups reflect that both cohorts were drawn from the same academic year, had undergone identical preclinical training prior to the intervention, and were taught the same core content and learning objectives during the module, with variations primarily influencing higher-order cognitive domains and OSCE performance.
Figures and Tables
The detailed results are summarized in Tables 1–5 and illustrated in Figures 2–4, which show the magnitude of improvement in both groups and the differences in OSCE outcomes.
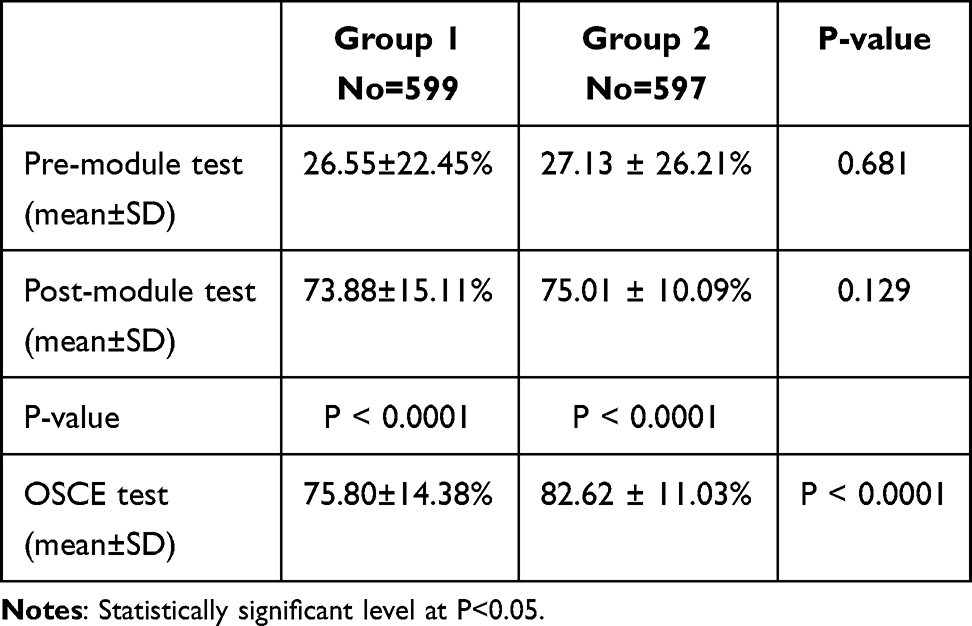 |
Table 1 Comparison Between Pre- and Post-Module Test Scores Among Both Groups |
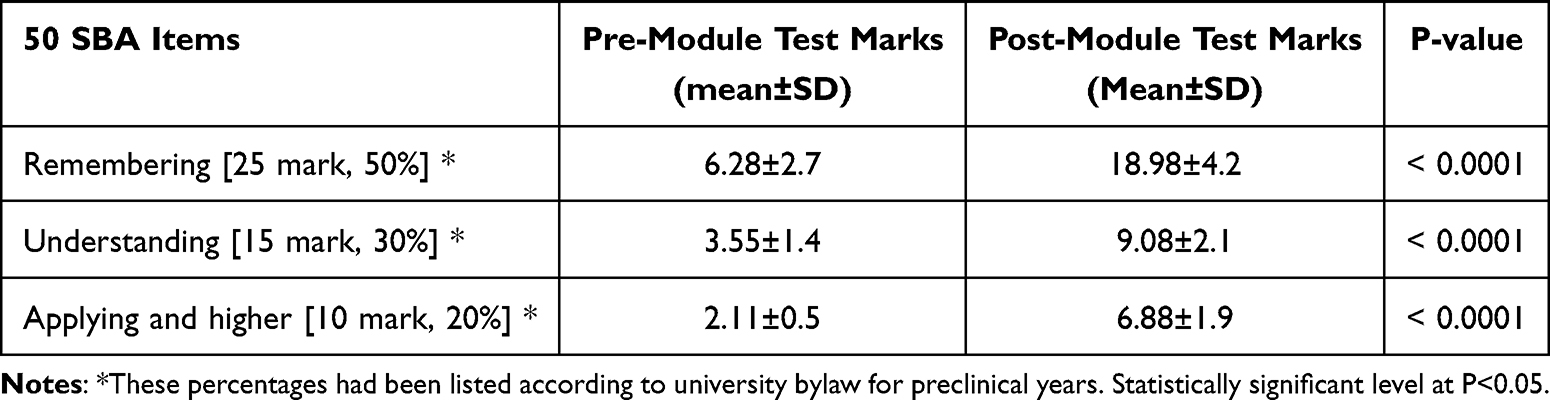 |
Table 2 Comparison Between Pre- and Post-Module Test Scores Among Group 1 According to Their Cognitive Level |
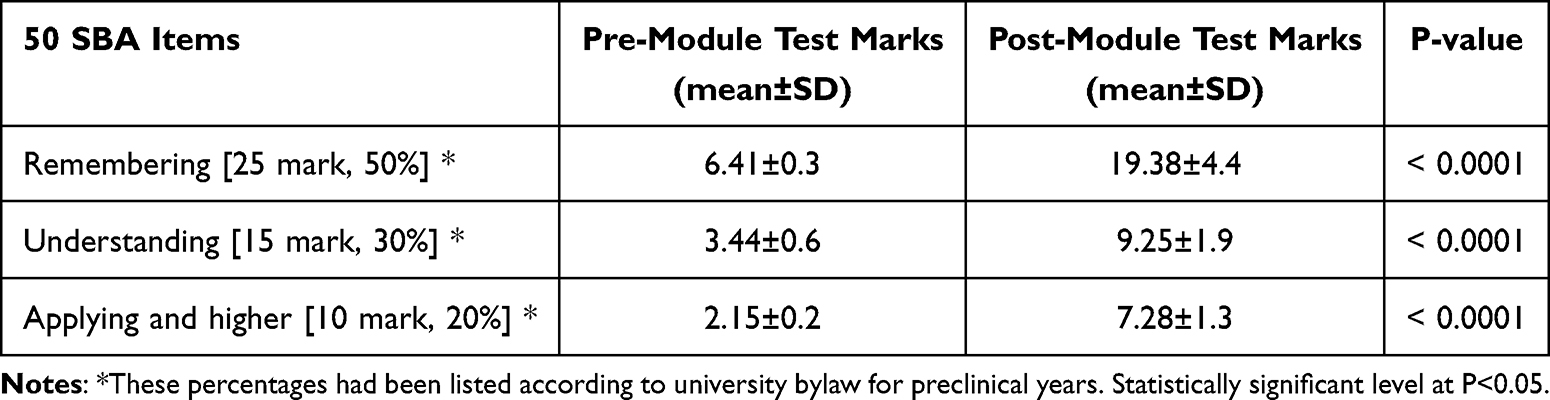 |
Table 3 Comparison Between Pre- and Post-Module Test Scores Among Group 2 According to Their Cognitive Level |
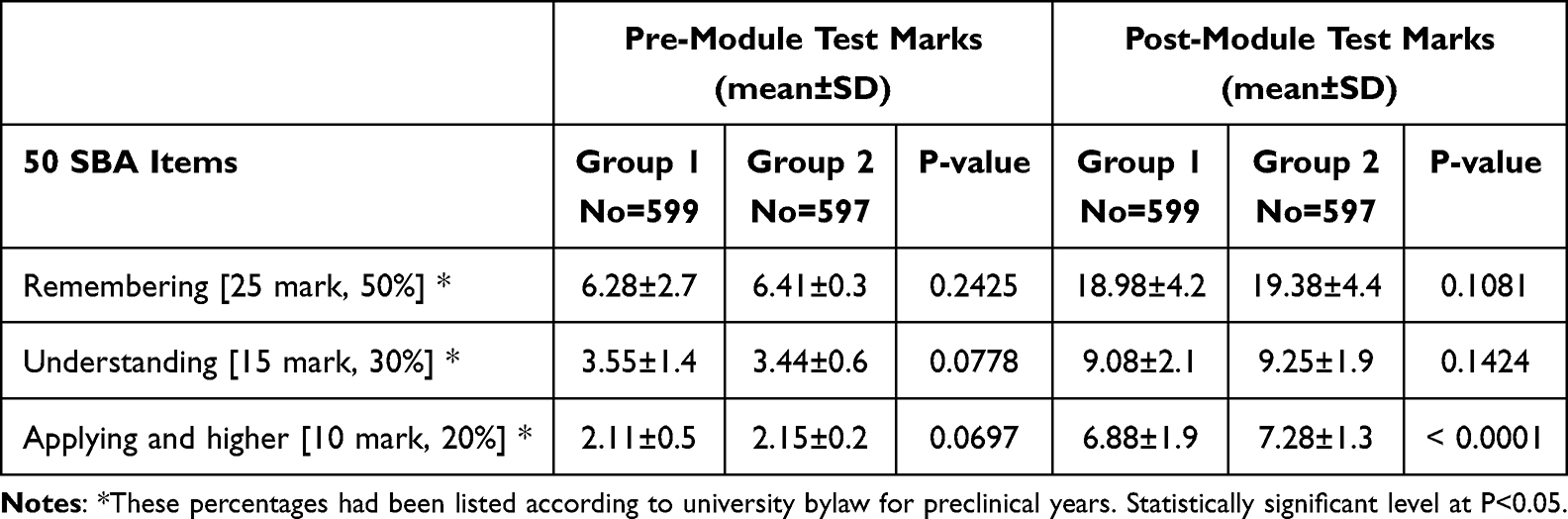 |
Table 4 Comparison Between Pre- and Post-Module Test Scores Among Both Groups According to Their Cognitive Level |
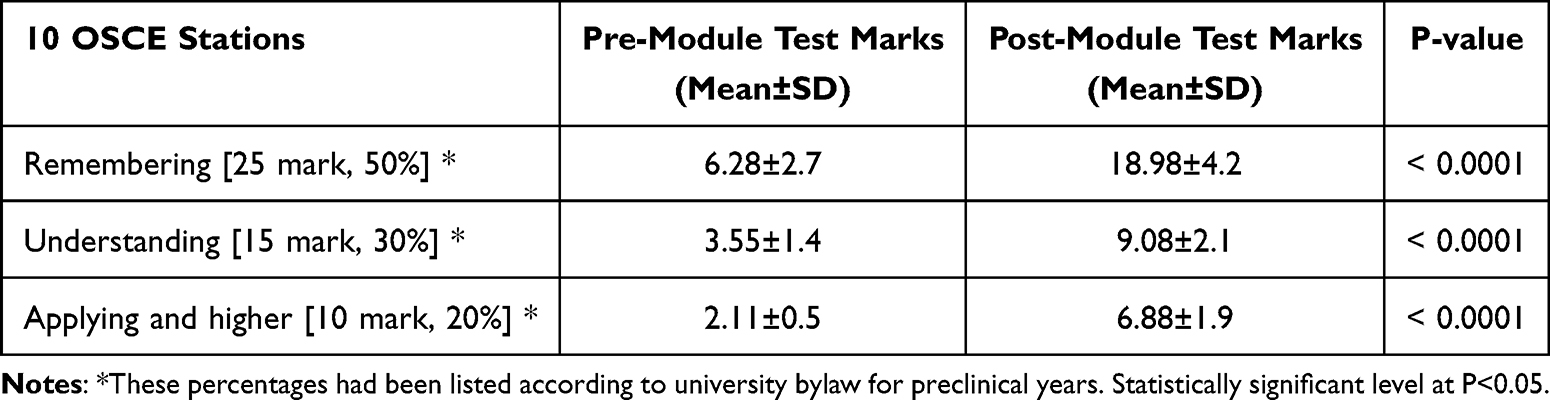 |
Table 5 Comparison Between OSCE Test Scores Among Both Groups According to Their Targeted Skills |
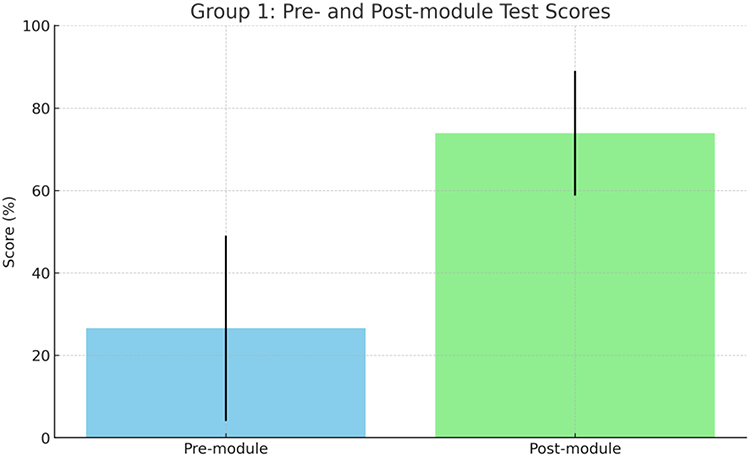 |
Figure 2 Group 1: Pre- and Post-module Test Scores. |
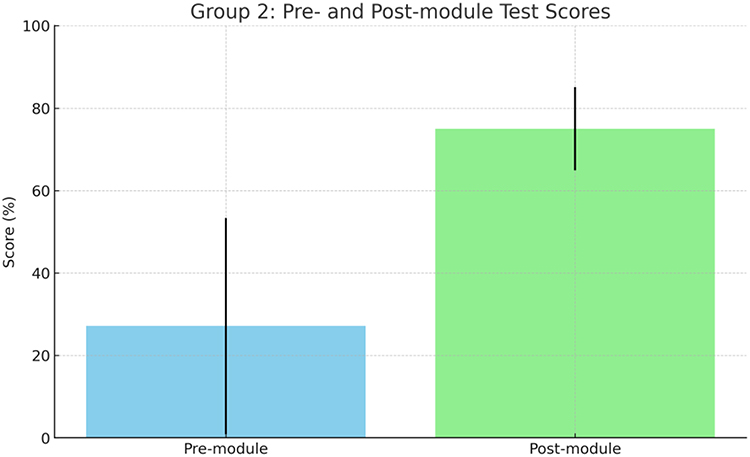 |
Figure 3 Group 2: Pre- and Post-module Test Scores. |
 |
Figure 4 OSCE Test Scores Comparison. |
Discussion
Simulation-based training is a cornerstone in modern medical education. Elendu et al (2024) confirmed that simulation methodologies, including VPs lead to superior clinical skills, improved patient safety behavior, and better learning outcomes compared to lecture-only formats.19
Recent evidence underscores the effectiveness of VPs in supporting clinical reasoning early in medical education. A systematic review found that computer-based VP tools significantly improved students’ diagnostic and reasoning abilities across a variety of preclinical subjects, demonstrating both feasibility and learning gains in such cohorts.20 Moreover, García-Torres et al (2024) reported that interactive, conversational virtual patients enhanced clinical competencies, especially in history-taking and reasoning, while achieving high learner satisfaction, reinforcing how VPs can supplement traditional instruction effectively.21
The improvement in OSCE performance observed in the second group of this study may be attributed to the integration of virtual patient scenarios within the module, which offered more opportunities for case-based application of knowledge, enhanced clinical reasoning, and improved readiness for procedural tasks, thereby increasing both competence and confidence during the assessment.22
The Year 2 Clinical Skills module, part of the Al-Azhar MBBS program, spans 15 weeks (one session per week) and accounts for 1 credit hour. The module integrates various teaching methodologies, including seven traditional lectures and eight real patient-based clinical sessions. This study aimed to assess the efficacy of VP-based tutorials in enhancing early clinical exposure (ECE) in the preclinical years.
Although VPs have traditionally been used in clinical teaching, the results of this study demonstrate that they are highly effective tools for preclinical education. The use of VPs significantly improved students’ clinical skills and facilitated ECE.
The findings of this study indicate that VPs positively impact the application of clinical knowledge, as evidenced by improved performance on the Objective Structured Clinical Examination (OSCE) in Group 2, compared to Group 1. Furthermore, both classic lectures and VP-based tutorials equally enhanced students’ understanding of basic clinical concepts, as shown by the comparison of pre- and post-module examination performance in both groups.
Several studies have highlighted the benefits of VP-based sessions in clinical disciplines. For instance, Leung and colleagues found that final-year medical students who were exposed to branched VPs performed significantly better on end-module multiple-choice questions (MCQs), essay questions, and the final surgery written exam in an anesthesia module compared to those exposed to storyline-based VPs.23 Similarly, a study in the United States showed that medical students who used VPs during clinical courses in surgery and urology had higher exam results than those who underwent standard ward education.24
However, it is important to note that some studies have shown limited benefits of VPs. For example, a study comparing VPs with no intervention during a four-year surgical clerkship found improvements in history-taking skills, but no significant differences in diagnostic investigations, differential diagnosis, or treatment planning, as assessed by paper-based exams.25 Despite this, meta-analyses and systematic reviews consistently indicate that VPs generally lead to favorable outcomes.26,27
When considering the efficacy of VPs in preclinical education, there is a noticeable gap in the literature. A study by Makransky et al demonstrated that first-year undergraduates who received a VP tutorial following a didactic lecture showed better understanding of medical genetics counseling, as measured by pre- and post-tests.28 However, this study focused on a single case and lacked a comparison group, making it difficult to compare VP-based education to traditional methods. The current study, with its longer duration and dual assessments (written and OSCE), provides evidence that VP-based tutorials positively influence practical outcomes, even when traditional lectures and VP-based tutorials yield similar results in theoretical knowledge. Another study by Nicolaou et al also concluded that VPs can be effectively implemented in preclinical pharmacology teaching, leading to enhanced knowledge and boosted learning outcomes.18
Our results align with recent findings showing that VPs enhance clinical reasoning when implemented in preclinical curricula.21,29 Coupled with broader evidence that simulation-based formats improve skill acquisition and patient safety,19,30 our study supports extending VP use as a complementary instructional modality. Notably, systematic reviews highlight VP feasibility in preclinical contexts and the adaptability of VR-enhanced cases to support self-directed learning and competency alignment.20
Limitations
This study was conducted at a single institution with a single undergraduate course. Student motivation for VP-based sessions may have been influenced by their interest in a new learning method. Therefore, further research using a cross-over design may be needed to confirm these results and assess the broader applicability of VP-based tutorials.
Conclusion
The effectiveness of VPs in preclinical education remains an open question, particularly regarding the specific learners and stages of education that benefit the most from this method. This study offers important insights into the use of VPs at the preclinical stage, demonstrating statistically significant improvements in clinical skills acquisition and facilitation of early clinical exposure.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Written informed consent was obtained from each study participant. We received ethical approval from Faculty of Medicine, Al-Azhar University Ethics Research Committee, reference number: MEU._101Med.Research_ 0000102.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tayade MC, Latti RG. Effectiveness of early clinical exposure in medical education: settings and scientific theories. J Educ Health Promot. 2021;10(1):117. doi:10.4103/jehp.jehp_988_20
2. Kolb DA. Learning styles and disciplinary differences. Modern Amer College. 1981;232–255.
3. Kolb DA. Experiential Learning: Experience as the Source of Learning and Development Vol 1. Englewood Cliffs, NJ: Prentice-Hall; 1984.
4. Dornan T, Littlewood S, Margolis SA, Scherpbier A, Spencer J, Ypinazar V. How can experience in clinical and community settings contribute to early medical education? Med Teach. 2006;28(1):3–18. doi:10.1080/01421590500410971
5. Ingale MH, Tayade MC, Bhamare S. Early clinical exposure: dynamics, opportunities, and challenges in modern medical education. J Educ Health Promot. 2023;12(1:295. doi:10.4103/jehp.jehp_237_23.
6. Jayaraj YM, Tayade MC. Ethical dilemma in medical professionals in COVID-19 pandemics and pravara initiatives. Pravara Med Rev. 2020;12(4):2–7.
7. Sawant SP, Rizvi S. Importance of early clinical exposure in learning anatomy. Scholars J Appl Med Sci. 2015;3:1035–1038.
8. Kar M, Kar C, Roy H, Goyal P. Early clinical exposure as a learning tool to teach neuroanatomy for first year MBBS students. Int J Appl Basic Med Res. 2017;7(Suppl 1):S38–41. doi:10.4103/ijabmr.IJABMR_143_17
9. Tayade MC, Giri PA, Latti RG. Effectiveness of early clinical exposure in improving attitude and professional skills of medical students in current Indian medical education set up. J Family Med Prim Care. 2021;10(2):681–685. doi:10.4103/jfmpc.jfmpc_1765_20
10. Tayade MC, Latti RG. Attitude of medical students towards early clinical exposure and integrated teaching in Western Maharashtra. Indian J Basic Appl Med Res. 2016;5:261–266.
11. Wenrich MD, Jackson MB, Wolfhagen I, Ramsey PG, Scherpbier AJJ. What are the benefits of early patient contact?--? – a comparison of three preclinical patient contact settings. BMC Med Educ. 2013;13(1):80. doi:10.1186/1472-6920-13-80
12. Khabaz Mafinejad M, Mirzazadeh A, Peiman S, et al. Medical students’ attitudes towards early clinical exposure in Iran. Int J Med Educ. 2016;7:195–199. doi:10.5116/ijme.5749.78af
13. Peacock JG, Grande JP. Patient exposure in the basic science classroom enhances differential diagnosis formation and clinical decision-making. PeerJ. 2015;3:e809. doi:10.7717/peerj.809
14. Windish DM, Paulman PM, Goroll AH, Bass EB. Do clerkship directors think medical students are prepared for the clerkship years? Acad Med. 2004;79(1):56–61. doi:10.1097/00001888-200401000-00013
15. von Below B, Hellquist G, Rödjer S, Gunnarsson R, Björkelund C, Wahlqvist M. Medical students’ and facilitators’ experiences of an early professional contact course: active and motivated students, strained facilitators. BMC Med Educ. 2008;8(1:56. doi:10.1186/1472-6920-8-56.
16. Dafli E, Fountoukidis I, Hatzisevastou-Loukidou C, D Bamidis P. Curricular integration of virtual patients: a unifying perspective of medical teachers and students. BMC Med Educ. 2019;19(1):416. doi:10.1186/s12909-019-1849-7
17. Manesh R, Dhaliwal G. Digital tools to enhance clinical reasoning. Med Clin North Am. 2018;102(3):559–565. doi:10.1016/j.mcna.2017.12.015
18. Nicolaou PA, El Saifi M. The impact of using virtual patients in preclinical pharmacology teaching. Adv Physiol Educ. 2020;44(3):363–369. doi:10.1152/advan.00009.2020
19. Elendu C, Amaechi DC, Okatta AU. The impact of simulation-based training in medical education: a review. Medicine. 2024;103(27):e38813. doi:10.1097/MD.0000000000038813
20. Torosian S, Mousakhani V, Wehsener, Wehsener S, Ramnauth V, Walcott-Bedeau G. S. et al. Virtual reality and preclinical medical education: a systematic review of its application and effectiveness. Discov Educ. 2025;4(191). doi:10.1007/s44217-025-00628-x
21. García-Torres D, Vicente Ripoll MA, Fernández Peris C, Mira Solves JJ. Enhancing clinical reasoning with virtual patients: a hybrid systematic review combining human reviewers and ChatGPT. Healthcare. 2024;12(22):2241. doi:10.3390/healthcare12222241
22. Phanudulkitti C, Puengrung S, Meepong R, Vanderboll K, Farris KB, Vordenberg SE. A systematic review on the use of virtual patient and computer-based simulation for experiential pharmacy education. Explor Res Clin Soc Pharm. 2023;11:100316. doi:10.1016/j.rcsop.2023.100316
23. Leung JY, Critchley LA, Yung AL, Kumta SM. Evidence of virtual patients as a facilitative learning tool on an anesthesia course. Adv Health Sci Educ Theory Pract. 2015;20(4):885–901. doi:10.1007/s10459-014-9570-0
24. Kerfoot BP, Baker H, Jackson TL, et al. A multi-institutional randomized controlled trial of adjuvant Web-based teaching to medical students. Acad Med. 2006;81(3):224–230. doi:10.1097/00001888-200603000-00004
25. Vash JH, Yunesian M, Shariati M, Keshvari A, Harirchi I. Virtual patients in undergraduate surgery education: a randomized controlled study. ANZ J Surg. 2007;77(1–2):54–59. doi:10.1111/j.1445-2197.2006.03978.x
26. Consorti F, Mancuso R, Nocioni M, Piccolo A. Efficacy of virtual patients in medical education: a meta-analysis of randomized studies. Comput Educ. 2012;59(3):1001–1008. doi:10.1016/j.compedu.2012.04.017
27. Cook DA, Erwin PJ, Triola MM. Computerized virtual patients in health professions education: a systematic review and meta-analysis. Acad Med. 2010;85(10):1589–1602. doi:10.1097/ACM.0b013e3181edfe13
28. Makransky G, Bonde MT, Wulff JS, et al. Simulation based virtual learning environment in medical genetics counseling: an example of bridging the gap between theory and practice in medical education. BMC Med Educ. 2016;16(1):98. doi:10.1186/s12909-016-0620-6.
29. Plackett R, Kassianos AP, Mylan S, Kambouri M, Raine R, Sheringham J. The effectiveness of using virtual patient educational tools to improve medical students’ clinical reasoning skills: a systematic review. BMC Med Educ. 2022;22(1):365. doi:10.1186/s12909-022-03410-x
30. Malik TG, Mahboob U, Khan RA, Alam R. Virtual patients versus standardized patients for improving clinical reasoning skills in ophthalmology residents. A randomized controlled trial. BMC Med Educ. 2024;24(1):429. doi:10.1186/s12909-024-05241-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Holographic Imaging Combined with VR Simulation in Obstetrics and Gynecology Resident Training: A Review on Skill Development and Patient Privacy Protection
Yi L, Dong Z, Zeng J, Ou J, Zhao E
International Journal of Women's Health 2026, 18:590972
Published Date: 21 April 2026