Back to Journals » Advances in Medical Education and Practice » Volume 16
Integrating Standardized Patient into Case-Based Learning in Posterior Fossa Meningioma Teaching: Evaluating the Added Value Beyond Case-Based Learning Alone
Authors Zhang S, Zhao C, Shen J ![]()
Received 18 August 2025
Accepted for publication 21 December 2025
Published 30 December 2025 Volume 2025:16 Pages 2463—2470
DOI https://doi.org/10.2147/AMEP.S556845
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Shaolin Zhang, Chenhui Zhao, Jun Shen
Department of Neurosurgery, The First Affiliated Hospital of Wannan Medical College (Yijishan Hospital of Wannan Medical College), Wuhu, Anhui, People’s Republic of China
Correspondence: Jun Shen, Email [email protected]
Purpose: To explore the effectiveness and pedagogical significance of a teaching model that integrates case-based learning (CBL) with standardized patient (SP) for posterior fossa meningiomas, compared to using CBL alone teaching.
Methods: In this randomized comparative study, we enrolled 72 interns and standardized residency trainees from the neurosurgery department of our hospital between July 2023 and September 2025. Participants were randomly divided into an experimental group (CBL+SP) and a control group (CBL-only), with 36 individuals in each group. After completing the study plans, teaching effectiveness was assessed through evaluations of theoretical knowledge and clinical skills, while participant satisfaction and teaching approach evaluation were measured using questionnaires. Furthermore, a survey was conducted among the CBL-only group to gather their opinions on the primary drawbacks of using this teaching approach exclusively.
Results: The experimental group demonstrated significantly higher theoretical test scores (88.71 ± 7.43 vs 79.47 ± 8.43, p < 0.001) and clinical skill scores (81.36 ± 5.68 vs 71.11 ± 7.22, p < 0.001) compared to the control group. Furthermore, the experimental group showed notable advantages over the control group in novelty, enhancing learning interest, self-study ability, integration of theory and practice, communication skills, clinical thinking, satisfaction rates, and teaching promotion (p < 0.05). The major drawback of the CBL-only teaching was the lack of clinical atmosphere and doctor-patient communication.
Conclusion: The SP-CBL integrated teaching model significantly improves clinical teaching outcomes compared to the CBL alone and is worthy of promotion in clinical education for posterior fossa meningiomas.
Keywords: case-based learning, standardized patient, combined teaching model, posterior fossa meningiomas, teaching effectiveness
Introduction
Posterior fossa meningiomas pose a significant challenge in neurosurgical education due to their complex anatomy, limited surgical space, and diverse clinical presentations.1,2 This complexity often leads to considerable difficulty for trainees in mastering their diagnosis and management.3
Our recent research has shown that traditional face-to-face teaching is superior to online teaching in neurosurgery clinical courses.4 However, traditional face-to-face teaching methods, while foundational, predominantly rely on didactic, “cramming-style” lectures that provide limited exposure to authentic clinical scenarios. Consequently, when confronted with real patients, trainees frequently demonstrate critical shortcomings, including incomplete history-taking, omission of key physical signs during physical examinations, an inability to link clinical findings to tumor localization, indecisiveness in formulating treatment plans, and inaccurate prognostic assessments.5,6
Case-based learning (CBL) has been introduced to bridge the theory-practice gap by using typical clinical cases to enhance memory retention, deepen disease understanding, improve clinical reasoning, and cultivate rigorous clinical thinking.7 However, CBL alone has inherent limitations: (1) Static case materials cannot simulate the informational uncertainty present in doctor-patient interactions, such as ambiguous complaints and disorganized medical histories; (2) There is a lack of real-time feedback, as seen in the failure to elicit pathological reflexes or deep/superficial reflexes during neurological examinations due to incorrect operational methods.
The use of Standardized Patients (SP)—trained individuals who simulate specific diseases—effectively addresses these limitations by accurately and vividly portraying disease-specific symptoms, signs, and histories.8 SP offer a safe platform for trainees to practice and receive immediate feedback, thereby cultivating practical skills and clinical confidence.9 While both CBL and SPs are valued in medical education, their synergistic potential in complex subspecialties such as neurosurgery remains underexplored.
Having implemented CBL, is it then necessary to incorporate SP into the course curriculum? Both educational scholars and students may be eager to learn the results of this study. Therefore, we innovatively integrated the SP methodology into the established CBL framework to create a closed-loop teaching system encompassing “three-dimensional case analysis, SP scenario simulation, and multi-faceted feedback.” As the first exploration of its application in clinical neurosurgical education for posterior fossa meningiomas, this approach can achieve comprehensive coverage of the continuum from “knowledge transmission” to “skill internalization” and “decision optimization” in posterior fossa tumor education, providing a replicable and innovative paradigm for neurosurgeon training. This study aimed to investigate the effectiveness, significance, and necessity of integrating SP into CBL in the teaching of posterior fossa meningiomas.
Materials and Methods
Population Characteristics
A total of 72 interns and standardized residency trainees (47.2% female) were enrolled from July 2023 to September 2025 and randomly divided into an experimental group (CBL+SP, n = 36) and a control group (CBL-only, n = 36) at the neurosurgery department, The First Affiliated Hospital of Wannan Medical College. In this study, the inclusion criteria were as follows: (1) participants must have received education in clinical and anatomical knowledge related to neurosurgery during their undergraduate studies; (2) participants must not have participated in any specialized training of CBL or SP. Participators were excluded if they: (1) study at neurosurgery department less than 2 weeks; (2) had prior experience in neurosurgery training.
The basic characteristics of the two group trainees are shown in Table 1. There were no significant differences in sex, age, trainee composition and pre-class assessment of basic knowledge. The study was approved by the ethics committee of the First Affiliated Hospital of Wannan Medical College (Yijishan Hospital of Wannan Medical College).
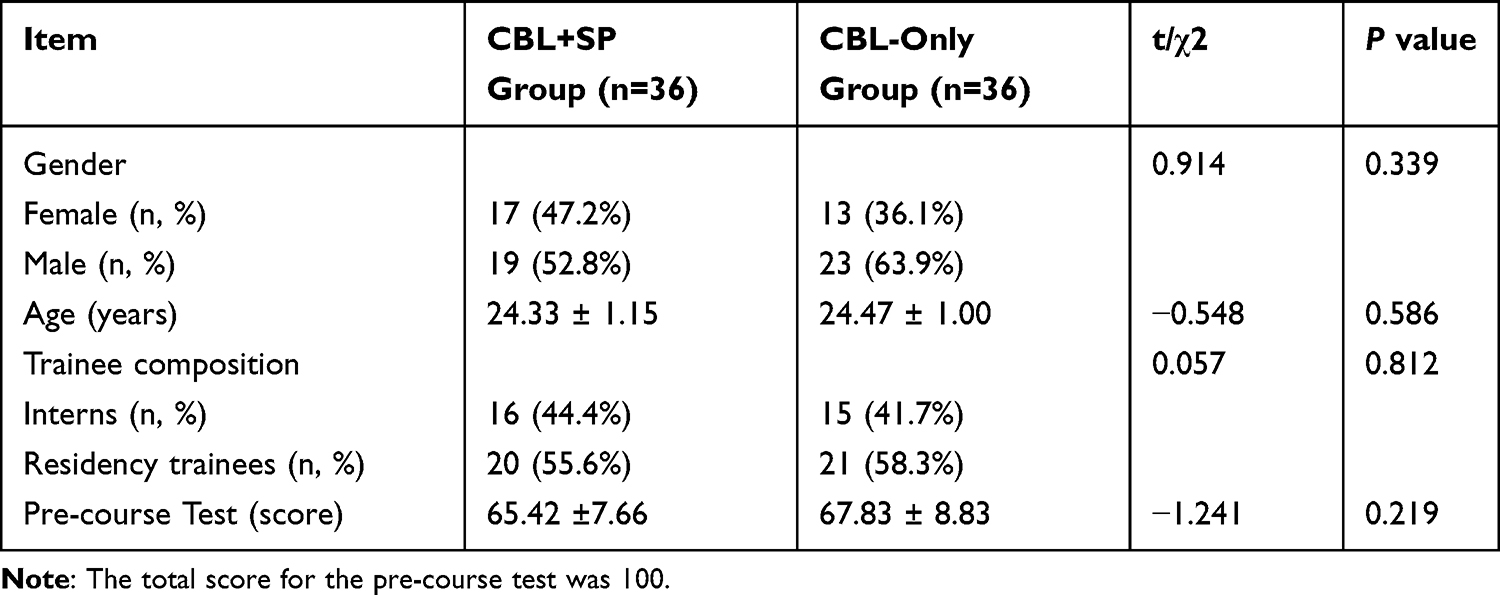 |
Table 1 Population Characteristics of the Two Groups |
Study Design
To evaluate the effectiveness and significance of the integrated CBL-SP teaching model for posterior fossa meningiomas, trainees were randomly divided into two groups: the experimental group (CBL+SP) and the control group (CBL-only).
Experimental Group (CBL-SP)
The teaching method consisted of three steps. Step 1 (Dual-Role Establishment): The SP-specific training was performed for teachers using typical clinical cases, allowing instructors to assume dual roles as both educators and SP. This approach enables them to fulfill the functions of “case simulator” and “teaching guide”. Step 2 (Pre-Class Preparation): Prior to the class sessions, instructors meticulously prepared comprehensive materials for a representative case. Key knowledge points were compiled into questions and provided to students. Students then looked up relevant knowledge to make thorough preparation before class. Step 3 (SP Scenario Simulation and Trainee Practice): During the class, the instructor, acting as the SP, simulated a patient with posterior fossa meningiomas, presenting typical patient history, symptoms, and signs. Students were required to complete the history taking, physical examination, and interpretation of auxiliary examinations within 20 minutes. Subsequently, they engaged in a discussion to answer questions posed before class and to formulate a detailed diagnosis and treatment plan. Finally, the instructor explained, analyzed, and summarized the key knowledge points. They also highlighted the students’ strengths and weaknesses and identified strategies for improvement.
Control Group (CBL-Only)
The teaching method was identical to that of the experimental group, excluding the SP teaching content.
Teaching Evaluation and Data Collection
After completing the teaching program, a comprehensive evaluation of teaching effectiveness will be conducted, encompassing four key dimensions: (1) theoretical knowledge assessment (total score: 100), which includes pathology, anatomical structures, clinical manifestations, diagnostic criteria, and treatment principles; (2) clinical skills (total score: 100), covering medical history taking, physical examination, interpretation of imaging, diagnosis and differential diagnosis, and the formulation of treatment plans; (3) teaching approach, including innovation, enhancement of learning initiative (learning interest and self-study ability), integration of theory and practice, communication skills, clinical thinking, and teaching promotion, with a maximum score of 10 points for each item; and (4) a satisfaction survey conducted through questionnaires.10 Students’ satisfaction is rated as very satisfied, satisfied, neutral, dissatisfied and very dissatisfied. Satisfaction was calculated using the formula: satisfaction = [(number of very satisfied students + number of satisfied students) / 36] * 100%. The number of neutral, dissatisfaction and very dissatisfaction were combined together and were not separately listed. In addition, questionnaires were distributed to the CBL-only group to gather their opinions on the primary drawbacks of using this teaching approach exclusively, including lack of quasi-realistic clinical scenarios, lack of physician-patient communication training, lack of connection between theory and practice, insufficient interaction with instructors, insufficient interaction with classmates and other reasons.
Data Analysis
Data were analyzed using SPSS Statistics software (version 22.0; IBM Corp). Categorical data were expressed as (n, %) and analyzed using Pearson’s chi-square test (χ2-test). Continuous data were presented as mean ± SD and analyzed using the independent t-test. A p-value of less than 0.05 indicated statistical significance.
Results
Comparison of Theoretical and Practical Scores Between the CBL+SP Group and the CBL-Only Group
To investigate whether the CBL+SP group was superior to the CBL-only group in enhancing the theoretical and practical abilities of the trainees, comparisons between the groups were conducted, and the results were listed in Table 2. We found that the experimental group outperformed the control group in theoretical knowledge (88.71± 7.43 vs 79.47±8.43, p < 0.001) and clinical skills (81.36 ± 5.68 vs 71.11 ± 7.22, p < 0.001), particularly in history taking, physical examination, diagnosis, and treatment planning. However, there was no significant difference in imaging interpretation (p = 0.305) (Table 2).
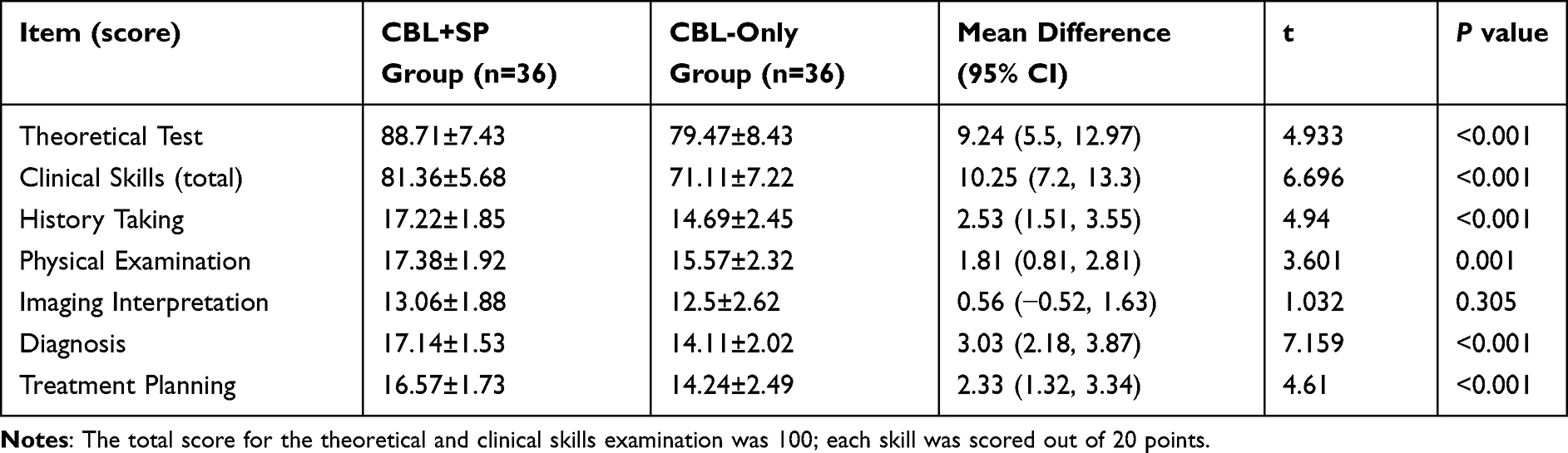 |
Table 2 Theory and Practical Skills Scores in the CBL+SP and CBL-Only Groups |
Teaching Method Evaluation
Upon completion of the course, questionnaires were distributed to participants for a comprehensive and objective evaluation to the teaching methods. The results showed that the CBL+SP group significantly outperformed the CBL-only group in novelty, enhancing learning interest, self-study ability, integration of theory and practice, communication skills, clinical thinking, and applicability for clinical teaching promotion. The detailed results are summarized in Table 3.
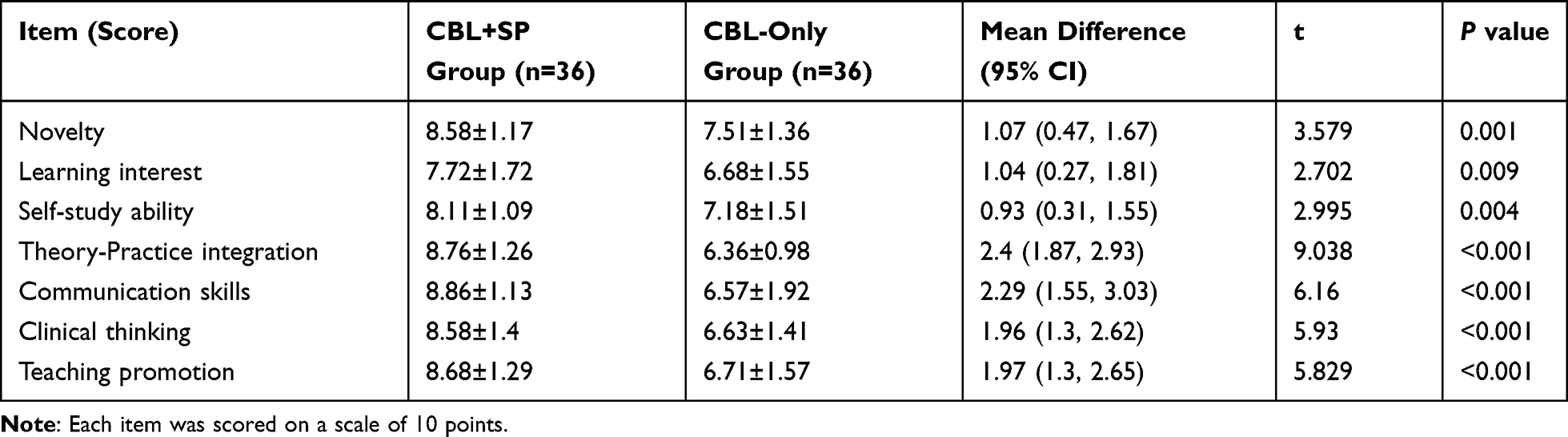 |
Table 3 Evaluation of Teaching Methods |
Comparison of Student’s Satisfaction Survey
Furthermore, a comparative analysis of teaching satisfaction between the two groups revealed the following results. In the CBL+SP group, 19 students were very satisfied (52.78%), 11 cases satisfied (30.55%), and 6 cases neutral or dissatisfied (16.67%). In contrast, the CBL-only group reported only 8 students as very satisfied (22.22%), 14 cases satisfied (38.89%), and 14 cases as neutral or dissatisfied (38.89%), respectively. Consequently, the CBL+SP group presented significantly higher satisfaction compared to the CBL-only group (83.33% versus 61.11%, p = 0.035). The results are demonstrated in Figure 1.
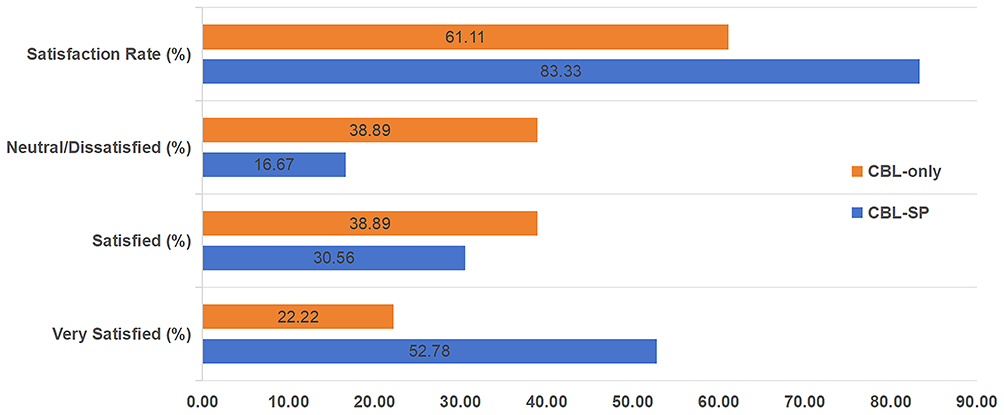 |
Figure 1 Comparison of students’ satisfaction between the two groups (61.11%: 83.33%, p = 0.035). |
Shortcomings of The CBL Alone Teaching
Since the research results indicated that the CBL-SP group significantly outperforms the CBL-only group, we conducted a further exploration to identify the shortcomings of the CBL-only group. As shown in Figure 2, students identified the primary disadvantage of the CBL-only teaching as the lack of quasi-realistic clinical scenarios (33.33%), followed by the lack of physician-patient communication training (25%) and a weak connection between theory and practice (16.67%). Other disadvantages included insufficient interaction with instructors (11.11%), limited interaction with classmates (8.33%), and various other reasons (5.56%).
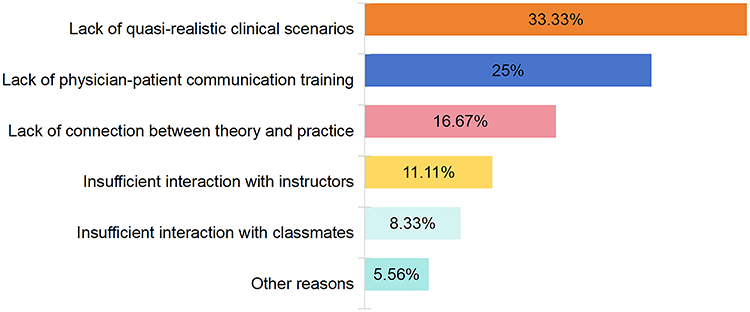 |
Figure 2 Shortcomings of the CBL-only teaching. |
Discussion
With ongoing advancements in medical education, traditional teaching methods are increasingly inadequate for meeting the demands of modern medical talent development. Contemporary pedagogy is shifting toward a competency-based approach focused on clinical skills. Notably, medical students who rely solely on traditional didactic instruction exhibit higher rates of clinical misdiagnosis during their initial patient encounters, which can lead to preventable disputes between physicians and patients due to insufficient communication skills. Research indicates that, compared to conventional teaching models, CBL approach significantly enhances the effectiveness of clinical teaching while reducing medical errors and lowering patient complaint rates.11,12
As innovative teaching approaches in contemporary medical education, CBL and SP are increasingly being implemented across various clinical disciplines.7,13–17 They each have their own advantages. CBL is a case-centered learning approach that enables learners to actively acquire knowledge about diseases while developing clinical reasoning and critical thinking skills through the analysis and discussion of specific clinical cases while simulating diagnostic decision-making processes.12 However, its limitations primarily lie in the inability to simulate the actual clinical scenarios and the lack of physician-patient communication training. In this study, we found that the teaching effectiveness and satisfaction in the CBL+SP group were significantly better than those in the CBL group, which the CBL+SP teaching had significantly higher theoretical test scores and clinical skill scores. These findings are consistent with our excepted outcomes and the conclusions of other study.18 However, studies on the combined CBL+SP teaching method remain limited, particularly regarding whether the combined CBL+SP approach is superior to CBL-only teaching. Further investigated why the performance of the CBL+SP group was significantly better than that of the group using only CBL teaching. We found that the primary limitation of using CBL alone is its inability to simulate clinical scenarios, doctor-patient communication, and the integration of theory with practice. Therefore, many scholars began to focus on combining CBL with other teaching methods, resulting in a significant improvement in teaching effectiveness.19–21 In contrast, the SP is an individual trained to consistently portray specific medical conditions, symptoms, some physical signs, and psychosocial characteristics in simulated clinical encounters. This methodology provides learners with authentic, replicable interactions in a controlled educational setting, and quasi-realistic clinical scenarios that can help students improve their communication skills with patients and clinical operational skills, effectively addressing the limitations of CBL. However, the primary limitation of SP is its inability to simulate objective pathological signs. Therefore, integrating CBL with SP is expected to further enhance educational outcomes in clinical medical education. To date, there remains a paucity of research on integrated CBL+SP teaching methodologies in the literature. This gap may be attributed to the substantial human resource investment required. In this study, the students pointed out that the CBL+SP teaching model demands a significant investment of their time and effort. The deep integration of CBL and SP essentially establishes an educational closed-loop system encompassing case cognition, contextual interaction, and structured feedback.
Posterior cranial fossa meningiomas, which occur in the cerebellopontine angle, petroclival region, and clivus region, present complex and diverse clinical manifestations due to the narrow space, intricate anatomical structures, and adjacent to the brainstem and cranial nerves. Trainees often find it challenging to master this content, as diagnosis and treatment require the integration of multidisciplinary knowledge, including neurosurgery, imaging, anatomy, and pathology. Consequently, the requirements for the trainees’ comprehensive abilities are quite high. Traditional medical education predominantly relies on classroom and didactic lectures, textbook-based learning, and theoretical instruction. While this approach helps students build a solid theoretical foundation, purely theoretical knowledge often proves insufficient for transforming into clinical practice skills when confronting complex, challenging, and individualized diseases. Enhancing students’ comprehensive clinical diagnostic and therapeutic abilities—particularly in clinical decision-making and operative skills—has long been a major challenge in neurosurgical medical education.22–24 The new teaching method integrates CBL and SP, combining theoretical learning, case-based analysis, and hands-on clinical practice. However, this approach has not yet been widely adopted in current clinical education, particularly in neurosurgery. Through CBL, students deepen their understanding of diseases by analyzing typical cases, while SP allows them to simulate real clinical scenarios, enhance communication skills, and further consolidate theoretical knowledge. These two methods complement and reinforce each other. In this study, a multi-dimensional comparative analysis demonstrated that the CBL+SP group significantly outperformed the CBL-only group in mastering theoretical knowledge, clinical practical skills, communication abilities, teaching evaluations, and overall satisfaction. Furthermore, from the students’ perspective, they prefer the combined CBL-SP teaching method. Although the CBL+SP integrated teaching model requires more time from both instructors and learners, it proves to be an effective pedagogical approach for complex diseases.
Limitations
Several limitations should be taken into consideration. First, the sample size is relatively small, which may limit the generalizability of the results. Second, the data were collected from a single medical center; therefore, a future multicenter study might yield different conclusions. Finally, the teaching time in the CBL+SP group may have been longer than in the CBL group. If the teaching time had been equal between the two groups, the results could have been affected.
Conclusion
Our study revealed that the combined CBL-SP teaching model establishes a tight connection between theoretical learning and clinical practice, providing an innovative approach for clinical education in complex diseases, especially in posterior fossa meningiomas. Compared to CBL alone, the combination of CBL and SP significantly enhances teaching effectiveness and student satisfaction. Therefore, although CBL alone improves teaching effectiveness, integration with SP remains necessary and is worthy of promoting in clinical education.
Statements and Declarations
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the First Affiliated Hospital of Wannan Medical College (Yijishan Hospital of Wannan Medical College). All subjects provided informed consent for the study.
Acknowledgments
We appreciate the support and assistance provided by other students and teachers.
Funding
Funding support of the study was provided by Teaching Research Project of Anhui Provincial Department of Education (2021jyxm1636) and Special Research Start-up Foundation for Introduced Talents (YR20230138).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kurucz P, Ganslandt O, Buchfelder M, et al. Microsurgical anatomy and pathoanatomy of the outer arachnoid membranes in the cerebellopontine angle: cadaveric and intraoperative observations. Acta Neurochir. 2023;165(7):1791–1805. doi:10.1007/s00701-023-05601-x
2. Ceccato GHW, da Trindade ÉSGG, Foltran RS, et al. Microsurgical resection of giant petroclival meningioma via the posteriorpetrosal approach: 2-dimensional operative video. World Neurosurg. 2022;166:191–200. doi:10.1016/j.wneu.2022.08.008
3. Shao X, Yuan Q, Qian D, et al. Virtual reality technology for teaching neurosurgery of skull base tumor. BMC Med Educ. 2020;20(1):3. doi:10.1186/s12909-019-1911-5
4. Shen J, Zhang S, Sun D, et al. Comparison of face-to-face teaching and online teaching in neurosurgery education for medical students. BMC Med Educ. 2025;25(1):232–240. doi:10.1186/s12909-025-06817-4
5. Tabuñar SMS, Parreño Sacdalan MD. Attrition in the training programs of the University of the Philippines-Philippine General Hospital (UP-PGH): a 5-year review of trends and reasons from 2018–2022. Acta Med Philipp. 2025;59(6):85–98. doi:10.47895/amp.vi0.9376
6. Seehra JK, Doleman B, Lund J. Progression of academic surgical residents to higher academic training and associations with protected characteristics: a UK Cohort Study. J Surg Educ. 2025;82(8):103552. doi:10.1016/j.jsurg.2025.103552
7. Bruen C, Illing J, Daly R, et al. Medical student experiences of Case-Based Learning (CBL) at a multicultural medical school. BMC Med Educ. 2025;25(1):152–162. doi:10.1186/s12909-024-06585-7
8. Hartmann L, Kaden JJ, Strohmer R. Authentic SP-based teaching in spite of COVID-19 - is that possible? GMS J Med Educ. 2021;38(1):Doc21. doi:10.3205/zma001417
9. Malik TG, Mahboob U, Khan RA, et al. Virtual patients versus standardized patients for improving clinical reasoning skills in ophthalmology residents. A randomized controlled trial. BMC Med Educ. 2024;24(1):429. doi:10.1186/s12909-024-05241-4
10. Shen J, Yuan L, Ge R, et al. Improving medical student recruitment into neurosurgery through teaching reform. BMC Med Educ. 2022;22(1):656. doi:10.1186/s12909-022-03722-y
11. Wang X, Che X, Tang X, et al. Application of combined teaching method of case-based-learning and clinical pathway in practical gynecological teaching. PeerJ. 2024;12:e17813. doi:10.7717/peerj.17813
12. Zhu Y, Zhang J, Fei J, et al. Problem-based learning and case-based learning in clinical practical teaching for gynecology residents: a narrative review. Adv Med Educ Pract. 2025;16:1269–1279. doi:10.2147/AMEP.S534053
13. Alizadeh M, Saramad A, Rafiepoor H, et al. Effect of virtual case-based learning (CBL) using the flipped class and peer instruction on the motivation to learn basic sciences. BMC Med Educ. 2024;24(1):1230–1238. doi:10.1186/s12909-024-06229-w
14. Zhao W, He L, Deng W, et al. The effectiveness of the combined problem-based learning (PBL) and case-based learning (CBL) teaching method in the clinical practical teaching of thyroid disease. BMC Med Educ. 2020;20(1):381–390. doi:10.1186/s12909-020-02306-y
15. Ricchi A, Martelli E, Molinazzi MT, et al. Survey of students of the degree course in obstetrics, on learning using case based learning (cbl) method in the area of professional teachings. Clin Ther. 2018;169(5):e213–e216. doi:10.7417/CT.2018.2081
16. Shang Y, Cao KF, Yue JY, et al. Comparative effectiveness of various teaching modes, including PBL, CBL, and CTTM in paediatric medical education with combined online and offline approaches. BMC Med Educ. 2025;25(1):8–15. doi:10.1186/s12909-024-06267-4
17. Calik A, Kapucu S. Comparative effectiveness of developed serious game versus standardized patients’ simulation in nursing education. Games Health J. 2024;13(6):466–476. doi:10.1089/g4h.2024.0037
18. Yu Z, Zhao Z, Chen X, et al. Effects of standardised patients (SP) combined with case-based learning (CBL) in Chinese clinical education: a systematic review and meta-analysis. BMJ Open. 2025;15(9):e095705. doi:10.1136/bmjopen-2024-095705
19. Lu J, Wu R, Zhu L, et al. Application of the BOPPPS combined with CBL method in clinical clerkship of pediatric dentistry. BMC Med Educ. 2025;25(1):1348. doi:10.1186/s12909-025-07967-1
20. Liu R, Li L, Zhou Y, et al. The application of CBL and mind mapping combined with Mini-CEX teaching mode in the cultivation of clinical competence of ultrasound residents. PLoS One. 2025;20(7):e0327739. doi:10.1371/journal.pone.0327739
21. Zhao W, He L, Deng W, et al. The effectiveness of the combined problem-based learning (PBL) and case-based learning (CBL) teaching method in the clinical practical teaching of thyroid disease. BMC Med Educ. 2020;20(1):381. doi:10.1186/s12909-020-02306-y
22. Lee JJ, Klepcha M, Wong M, et al. The first pilot study of an interactive, 360° augmented reality visualization platform for neurosurgical patient education: a case series. Oper Neurosurg. 2022;23(1):53–59. doi:10.1227/ons.0000000000000186
23. Colombo E, Regli L, Esposito G, et al. Mixed reality for cranial neurosurgical planning: a single-center applicability study with the first 107 subsequent holograms. Oper Neurosurg. 2023;26(5):551–558. doi:10.1227/ons.0000000000001033
24. Jain S, Timofeev I, Kirollos RW, et al. Use of mixed reality in neurosurgery training: a single centre experience. World Neurosurg. 2023;176:e68–e76. doi:10.1016/j.wneu.2023.04.107
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.