Back to Journals » Journal of Inflammation Research » Volume 18
Integrating Pre- and Postoperative Systemic Inflammatory Markers for Acute Kidney Injury Prediction Following Radical Cystectomy: A Multi-Center Retrospective Study
Authors Liu Z, Fan P, Lu Y, Cao M, Yao W ![]() , Chen D, Ji F
, Chen D, Ji F
Received 10 April 2025
Accepted for publication 21 August 2025
Published 25 September 2025 Volume 2025:18 Pages 13335—13345
DOI https://doi.org/10.2147/JIR.S529335
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Wenjian Li
Zhongqi Liu,1,* Peng Fan,1,* Yanan Lu,1,* Minghui Cao,1 Weifeng Yao,2 Dongtai Chen,3 Fengtao Ji1
1Department of Anesthesiology, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 2Department of Anesthesiology, the Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, People’s Republic of China; 3Department of Anesthesiology, State Key Laboratory of Oncology in South China, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-Sen University Cancer Center, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dongtai Chen, Department of Anesthesiology, State Key Laboratory of Oncology in South China, Guangdong Provincial Clinical Research Center for Cancer, Sun Yat-Sen University Cancer Center, Guangzhou, People’s Republic of China, Email [email protected] Fengtao Ji, Department of Anesthesiology, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, People’s Republic of China, Email [email protected]
Purpose: The present study aimed to investigate the association of perioperative dynamic changes of systemic inflammation markers with AKI after radical cystectomy and their predictive value through machine learning algorithms.
Patients and Methods: Patients undergoing radical cystectomy with urinary diversion for bladder cancer from 2013 to 2022 at three university-affiliated tertiary hospitals were gathered. Perioperative dynamic changes of systemic inflammatory markers were calculated based on peripheral blood cell counts from pre- and post-operative values and categorized using restricted cubic splines (RCS). The number of positive changes in these markers was recorded as the perioperative inflammation index. Multivariable logistic regression was utilized to identify risk factors for AKI after radical cystectomy. AKI prediction models were constructed through various supervised machine learning algorithms and evaluated by the area under the receiver operating characteristic curve (AUROC).
Results: 727 patients were finally enrolled in the study, with 151 (20.8%) patients experiencing AKI following radical cystectomy. Postoperative hemoglobin (p = 0.003; OR, 0.977; 95% CI, 0.962– 0.992), albumin level (p = 0.007; OR, 0.906; 95% CI, 0.843– 0.974), intraoperative fluid infusion rate (p < 0.001; OR, 0.769; 95% CI, 0.665– 0.890) and the perioperative inflammation index (p < 0.001; OR, 1.507; 95% CI, 1.209– 1.877) were identified as independent risk factors with predictive value for AKI following radical cystectomy with urinary diversion. Among various machine learning models, XGBoost performed best (AUROC: 0.801; 95% CI: 0.735– 0.867) in AKI prediction.
Conclusion: The association between perioperative dynamic changes of inflammatory markers and AKI after radical cystectomy reinforced the necessity of perioperative inflammatory evaluation. AKI predictive models, integrating perioperative metrics, enable early identification and optimize perioperative management for AKI prevention.
Keywords: radical cystectomy, urinary diversion, perioperative systemic inflammation, acute kidney injury, machine learning algorithms
Introduction
Acute kidney injury (AKI) poses a significant risk following radical cystectomy and urinary diversion for bladder cancer, with incidence rates ranging from 10% to over 40%.1–3 Studies have indicated that individuals who experience AKI after surgery are more prone to developing chronic kidney disease and face heightened mortality rates.3,4 The occurrence of AKI after radical cystectomy for bladder cancer was reported to be influenced by various factors, including demographic indexes, preoperative evaluations, and surgical manipulation variables.1,2
Previous studies have demonstrated that the perioperative systemic inflammatory indexes, including the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), systemic inflammatory response index (SIRI), and systemic immune-inflammation index (SII), were associated with numerous postoperative adverse events, including AKI, and constituted an integral aspect of the perioperative evaluation.5–7 Elevated preoperative NLR, SII, and SIRI levels were reported to be related to AKI following percutaneous coronary intervention.8,9 In addition, perioperative dynamic changes of these inflammation markers were reported as risk factors for postoperative respiratory complications, prolonged pain, and mortality.10,11 Perioperative changes of NLR showed predictive value for AKI after Coronary Artery Bypass Grafting.12 However, in patients undergoing radical cystectomy and urinary diversion, the impact of perioperative dynamic changes of inflammation markers on the occurrence of postoperative AKI was not well defined.
The application of machine learning algorithms has become increasingly prevalent in assisting diagnosis and predictive modeling. In patients who had undergone cardiovascular surgery, gradient-boosted machine (GBM) models were developed to predict postoperative AKI.13,14 In addition, ensemble algorithms, including random forest (RF) and GBM, were employed to predict AKI in individuals who underwent liver resection or transplantation.15,16 However, insufficient external validation constrains the reliability and generalizability of these AKI predictive models, and predictive models for AKI following radical cystectomy and urinary diversion were infrequently reported.
Therefore, the present study aimed to verify the association between perioperative dynamic changes of systemic inflammation indexes and AKI after radical cystectomy with urinary diversion, and develop and validate the AKI machine learning predictive model based on perioperative evaluation and management metrics. We hypothesized that the perioperative dynamic changes of systemic inflammation indexes significantly affect the incidence of AKI, machine learning model incorporating perioperative metrics may offer a promising prediction for AKI after radical cystectomy.
Materials and Methods
Population
Patients who underwent radical cystectomy and urinary diversion for bladder cancer at Sun Yat-sen Memorial Hospital, Sun Yat-sen University Cancer Center, and the third affiliated hospital of Sun Yat-sen University between January 2013 and December 2022 were included in this study. Ethical approval was obtained from the institutional review boards of all participating centers (approval number: SYSKY-2023-165-01). The present study was followed in concordance with the Declaration of Helsinki. Patient consent was waived due to the retrospective nature of the study. The inclusion criteria were: (1) age ≥ 18 years; (2) underwent radical cystectomy and urinary diversion during the study period. Exclusion criteria included: (1) age < 18 years; (2) patients with non-bladder cancer; (3) patients with pre-existing chronic kidney disease or acute kidney injury before surgery; (4) patients with incomplete data.
Study Design
All surgeries were performed by chief surgeons, with anesthesia administered by senior attending anesthesiologists or those with higher qualifications. Patients underwent invasive arterial monitoring and central venous catheterization routinely. Induction of anesthesia was achieved using propofol (2–4 mg/kg) or etomidate (0.2–0.4 mg/kg), sufentanil (0.2–0.4 mg/kg), and muscle relaxant (cisatracurium [0.2–0.3 mg/kg] or rocuronium [0.8–1.0 mg/kg]). Maintenance of anesthesia during surgery was accomplished with inhalational anesthetics (sevoflurane or desflurane) (0.8–1 MAC) combined with opioids (sufentanil and remifentanil). Intermittent doses of muscle relaxants (cisatracurium [4–6 mg] or rocuronium [10–20 mg]) were used to maintain muscle relaxation. Additionally, a transversus abdominis plane (TAP) block with 0.25% ropivacaine was used for adjunctive analgesia.
Data Collection
Demographic information included sex, age, BMI, comorbidities (such as hypertension, diabetes, coronary heart disease (CHD), chronic obstructive pulmonary disease (COPD), etc)., ASA classification, and preoperative chemotherapy status.
Laboratory examination variables within 7 days preoperatively and up to 2 days postoperatively were collected, including hemoglobin, albumin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), total bilirubin, creatinine, and differential blood cell counts. The preoperative and postoperative systemic inflammatory markers (including NLR, PLR, LMR, SIRI, and SII) were calculated based on these blood cell counts. Specifically, the following formulas were applied: NLR = Neutrophil count / Lymphocyte count; PLR = Platelet count / Lymphocyte count; LMR = Lymphocyte count / Monocyte count; SIRI = (Neutrophil count × Monocyte count) / Lymphocyte count; SII = (Platelet count × Neutrophil count) / Lymphocyte count.
Surgical manipulation parameters included the duration of surgery, intraoperative blood loss, the type of urinary diversion (orthotopic neobladder, ileal conduit, and cutaneous ureterostomy), and surgical procedure (open, laparoscopy, or robot-assisted). The choice of urinary diversion and surgical procedure was determined by the surgeon based on the location and extent of the surgical site, patient condition, and patient preference.
Intraoperative management metrics were obtained, including the volume and type (crystalloids and colloids) of fluids infused, infusion rates, and details of red blood cell or plasma transfusions. The intraoperative fluid infusion rate was standardized to the patient’s body weight (mL/kg/ hr). Fluid infusion management was tailored by the anesthesiologist based on the patient’s blood pressure, urine output, hemodynamic monitoring, and central venous pressure (CVP) levels. For elderly patients (age > 65 years) or those with compromised function (cardiac or pulmonary), blood transfusions were initiated when the intraoperative hematocrit fell below 30%. In contrast, for other patients, blood transfusions were administered when the hematocrit dropped below 25%.
Outcome
The primary outcome was postoperative AKI, defined by the Acute Kidney Injury Network (AKIN) criteria as a serum creatinine increase of ≥ 26.5 μmol/l (≥ 0.3 mg/dl) or ≥ 1.5-fold from baseline within 48 hours postoperatively.17
Statistical Analysis
Continuous variables were presented as median with interquartile range (IQR) and were compared using the Mann–Whitney U-test. Categorical variables were expressed as frequencies and percentages (%) and were compared using the Chi-squared test or Fisher’s exact test.
Patients ultimately enrolled in this study were randomized in a 7:3 ratio into primary and validation cohorts, and Univariable comparisons were used to assess differences between the two cohorts. Restricted cubic splines (RCS) were employed to transform continuous systemic inflammatory markers into categorical variables based on their hazard ratio (HR) values in the primary cohort. Subsequently, Univariable comparisons were conducted in the primary cohort to identify potential risk factors for postoperative AKI. Variables with a p-value <0.10 in the Univariable comparisons were considered for inclusion in the multivariable logistic regression model to identify independent risk factors.
Supervised machine learning algorithms, including k-nearest neighbors (KNN), support vector machines (SVM), logistic regression, decision tree, RF, GBM, and XGBoost, were employed to develop prediction models for AKI. For the KNN, SVM, and logistic regression models, variables with a p-value less than 0.1 in the univariate analysis were selected to reduce dimensionality and avoid overfitting. For tree-based algorithms (including decision tree, RF, GBM, and XGBoost), all available variables were included in the initial model construction since these algorithms have internal mechanisms for handling multicollinearity, ranking feature importance, and performing implicit feature selection, which makes them suitable for high-dimensional data without requiring prior variable reduction. The z-score standardization was applied of continuous variables in KNN and SVM models. 5-fold cross-validation was utilized during model training and evaluation to prevent overfitting and provide a more robust estimate of model performance.
Model performance was evaluated in the validation cohort using the area under the receiver operating characteristic curve (AUROC), the area under the precision–recall curve (AUPRC), and the F1 score to comprehensively assess both overall discrimination and performance under class imbalance. The Shapley additive explanations (SHAP) values were utilized to demonstrate the variables with significant predictive value in the model with the highest AUROC, and the decision curve analysis (DCA) was employed to show the potential benefits of the model’s clinical application.
The level of statistical significance was set at p < 0.05 for all tests. All analyses were conducted using SPSS (version 26.0), R (version 4.0.2) with the “rms” package, and Python with the “numpy”, “pandas”, “sklearn”, and “shap” packages.
Results
Patient Selection
A total of 962 patients undergoing radical cystectomy and urinary diversion were included in this study. Among them, 14 patients were excluded due to pre-existing chronic kidney disease, 5 were excluded for undergoing surgery for non-tumor reasons, and 216 were excluded due to incomplete data. Ultimately, 727 patients were included in the final analysis. The median age of the patients was 64 years (IQR: 56–70 years), and the majority were male (86.5%). The median BMI of the subjects was 23.2 kg/m2 (IQR: 21.0–25.1 kg/m2). Postoperative AKI occurred in 151 patients (20.8%). The patients were divided into training and validation cohorts in a 7:3 ratio. Table 1 showed the comparison of demographic characteristics, perioperative laboratory examinations, Intraoperative management metrics, surgical manipulation parameters, and the AKI incidence between these groups.
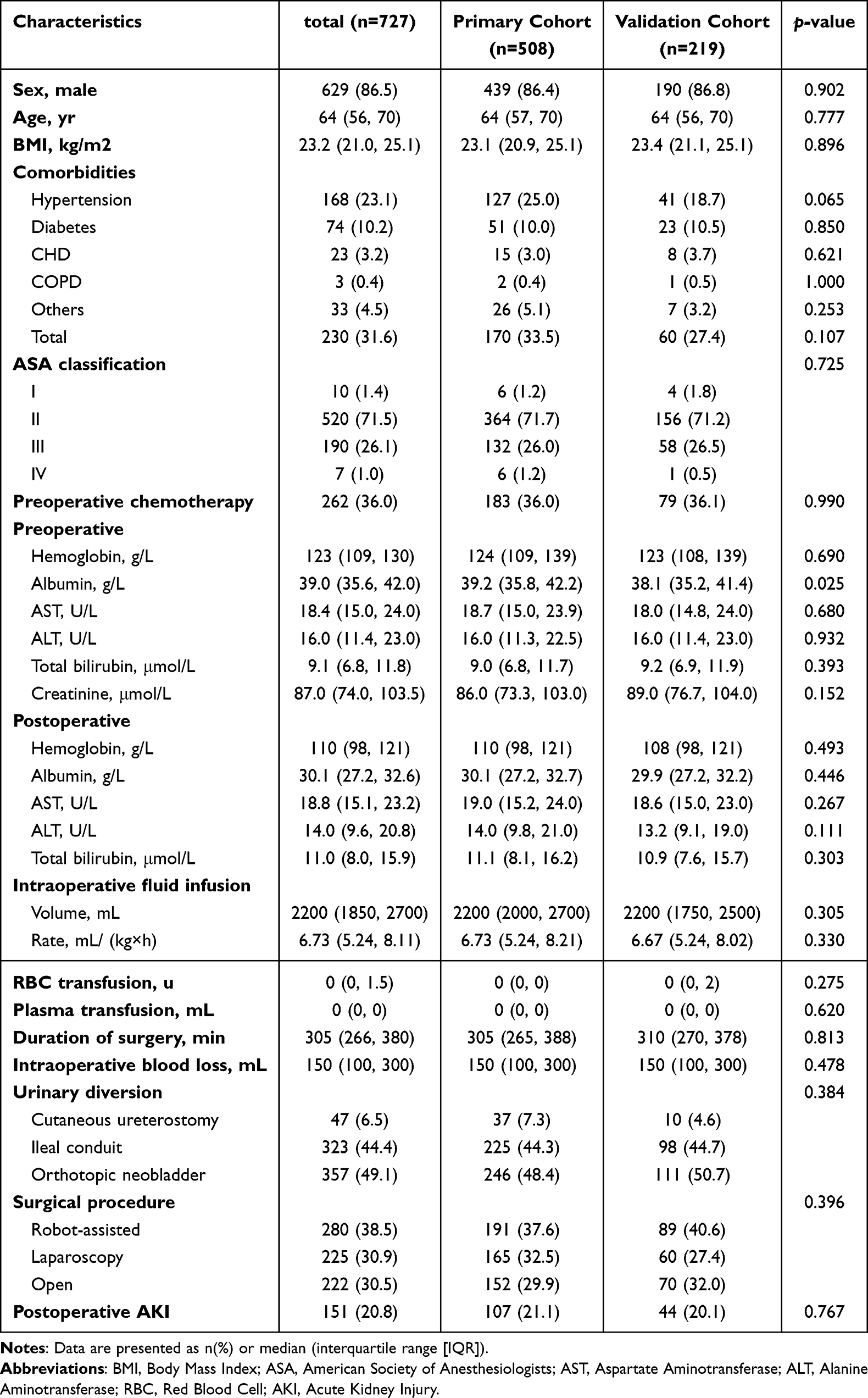 |
Table 1 Univariable Analysis Between the Primary and Validation Cohorts |
Univariable and Multivariable Analysis
Perioperative systemic inflammatory markers (including NLR, PLR, LMR, SIRI, and SII) were calculated based on differential blood cell counts. The postoperative systemic inflammation markers were divided by the preoperative corresponding markers to demonstrate the perioperative dynamic changes of these indexes. Based on the primary cohort, the dynamic changes of these systemic inflammatory markers were converted into categorical variables using RCS (Figure 1A–E). The perioperative dynamic changes of NLR, PLR, LMR, and SII had significant associations with postoperative AKI in Univariable comparisons (Table 2). Further, the number of positive dynamic changes of systemic inflammatory markers for each patient was recorded as a perioperative inflammation index to reveal the degree of inflammation activation during surgery. A positive association between the perioperative inflammation index and the incidence of AKI was found (Figure 1F).
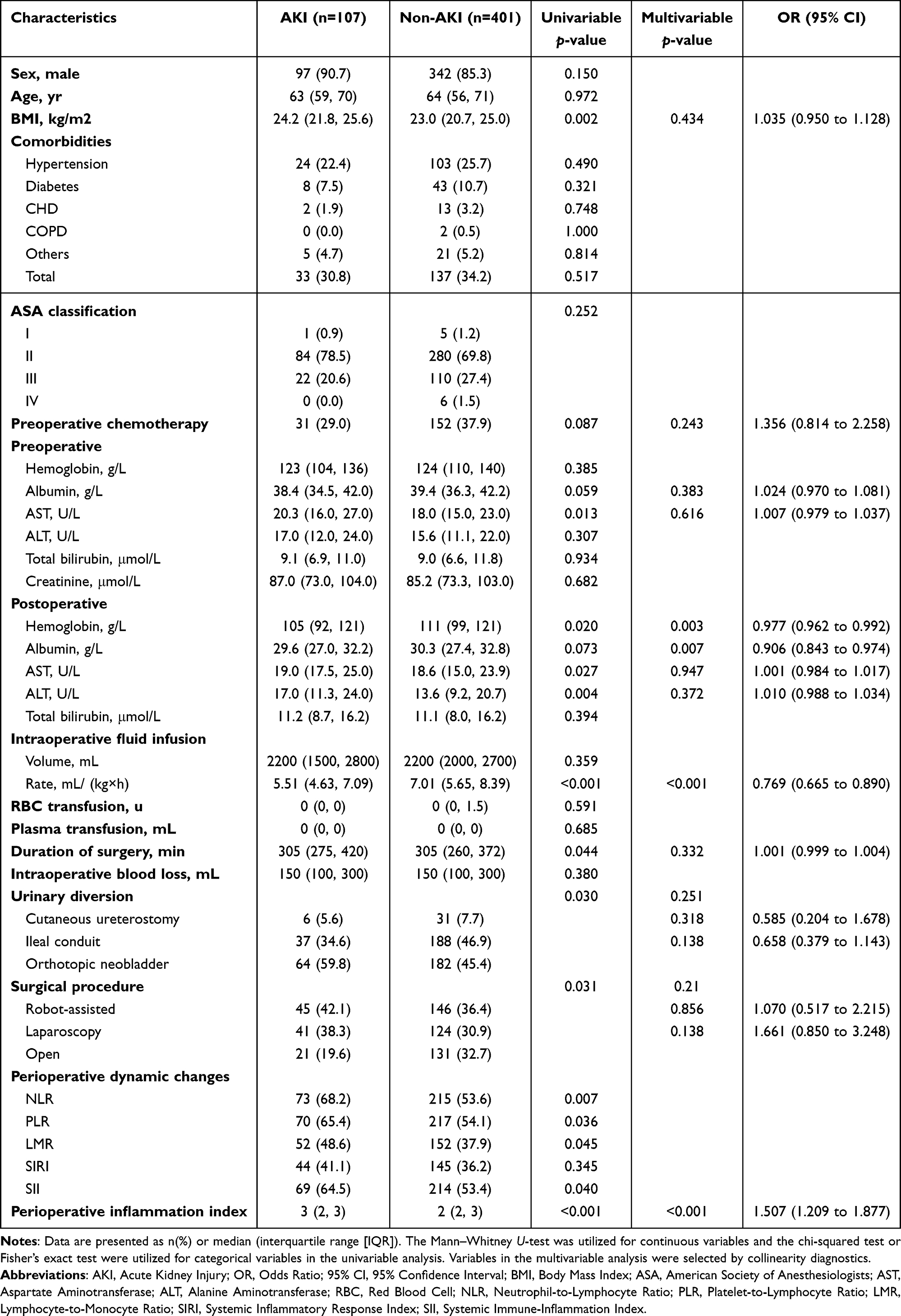 |
Table 2 Univariable and Multivariable Comparisons Between the AKI and Non-AKI Groups in the Primary Cohort |
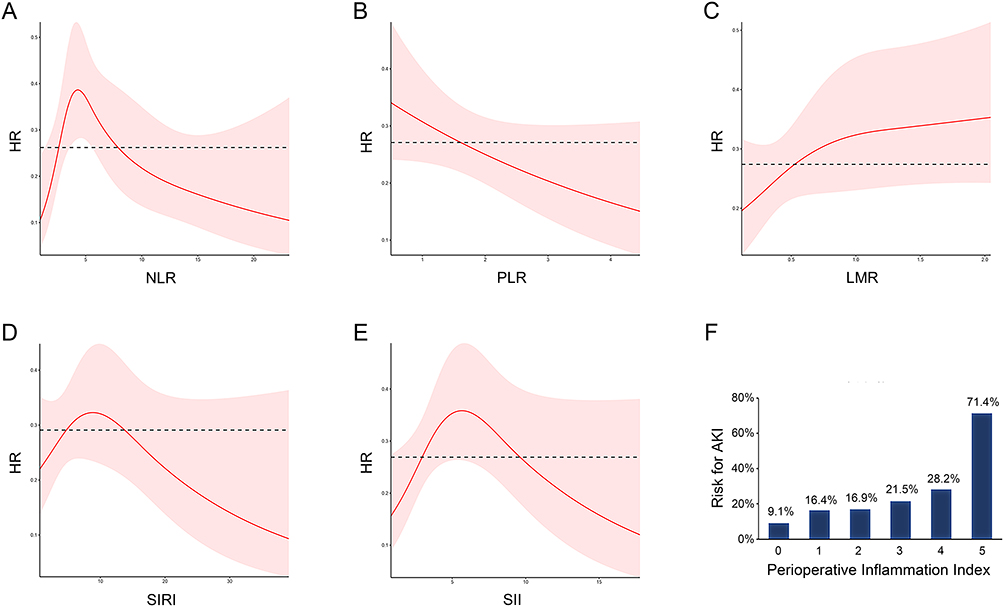 |
Figure 1 The associations of the dynamic changes of perioperative systemic inflammatory markers with AKI following radical cystectomy. (A) Restricted cubic spline of the HRs (95% CI) for AKI associated with the dynamic change of perioperative NLR. (B) Restricted cubic spline of the HRs (95% CI) for AKI associated with the dynamic change of perioperative PLR. (C) Restricted cubic spline of the HRs (95% CI) for AKI associated with the dynamic change of perioperative LMR. (D) Restricted cubic spline of the HRs (95% CI) for AKI associated with the dynamic change of perioperative SIRI. (E) Restricted cubic spline of the HRs (95% CI) for AKI associated with the dynamic change of perioperative SII. (F) A positive correlation was observed between the perioperative inflammation index (number of positive dynamic changes of systemic inflammatory markers) and the risk of AKI. |
In the primary cohort, Univariable comparisons indicated that BMI, preoperative AST, postoperative hemoglobin, AST and ALT levels, intraoperative fluid infusion rate, duration of surgery, the type of urinary diversion, surgical procedure and the perioperative inflammation index showed significant differences between the AKI and non-AKI groups (Table 2). Multivariable logistic regression identified postoperative hemoglobin (p = 0.003; OR, 0.977; 95% CI, 0.962 to 0.992), albumin level (p = 0.007; OR, 0.906; 95% CI, 0.843 to 0.974), intraoperative fluid infusion rate (p < 0.001; OR, 0.769; 95% CI, 0.665 to 0.890) and the perioperative inflammation index (p < 0.001; OR, 1.507; 95% CI, 1.209 to 1.877) as independent risk factors for the development of AKI (Table 2).
Development and Validation of Prediction Models
Various machine learning algorithms, including KNN, SVM, logistic regression, decision tree, RF, GBM, and XGBoost, were utilized to construct AKI prediction models in the primary group (Table S1). The ROC curves for these models in the validation cohort are shown in Figure 2. The AUROC values for the models in the validation cohort ranged from 0.658 to 0.801, with all models except KNN and SVM achieving an AUROC above 0.7. In addition, the XGBoost model achieved the highest AUROC of 0.801 (95% CI: 0.735 to 0.867) with a sensitivity of 84.1% and a specificity of 64.6% (Table 3). Furthermore, XGBoost also demonstrated the highest AUPRC of 0.503 (95% CI: 0.352 to 0.637) and the best F1 score of 0.522, indicating superior performance in identifying positive cases under class imbalance (Table 3).
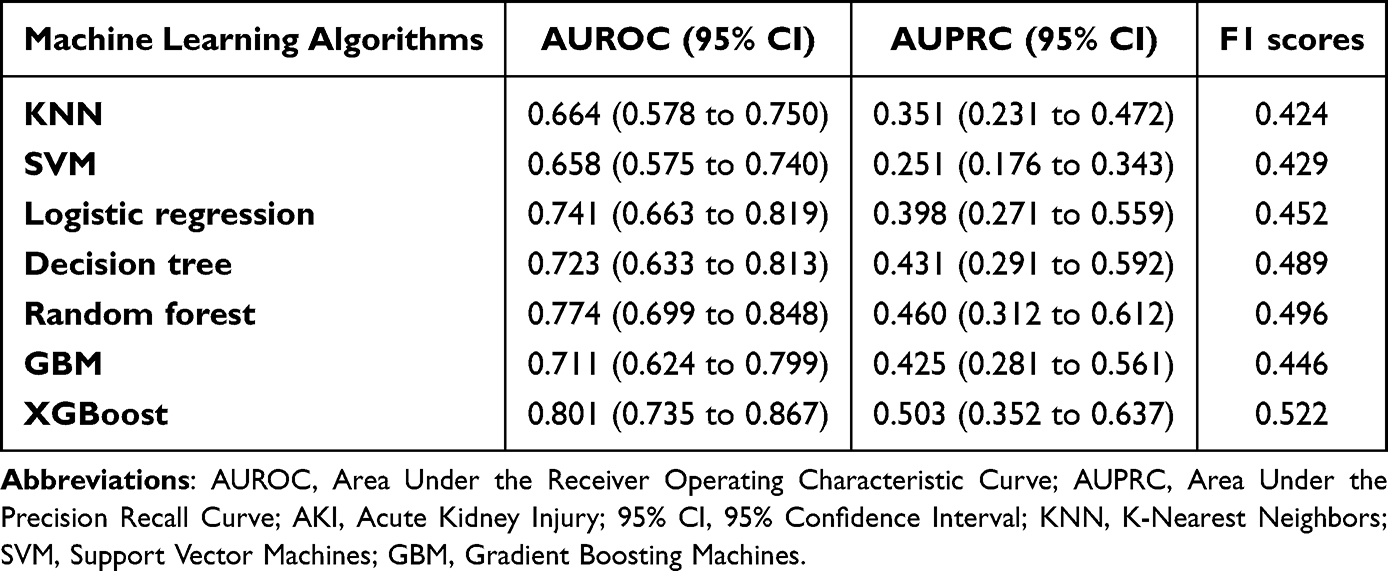 |
Table 3 The AUROC of AKI Prediction Models Developed Based on Machine Learning Algorithm |
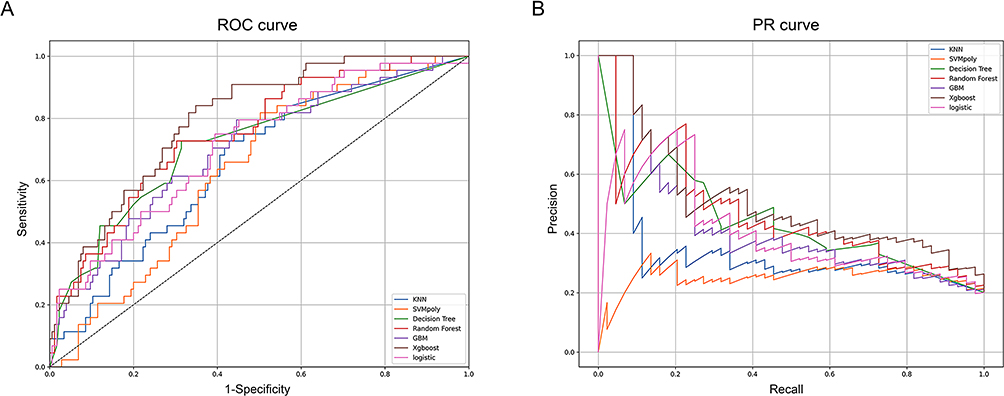 |
Figure 2 The receiver operating characteristic (ROC) and precision–recall (PR) curves of machine learning models in the validation cohort. The ROC curves (A) and PR curves (B) illustrate the predictive performance of different machine learning models for AKI in the validation cohort. The XGBoost model achieved the highest AUROC (brown curve) and AUPRC (brown curve) for AKI prediction. |
Model Interpretation and Clinical Application
SHAP analysis showed that intraoperative fluid infusion rate, postoperative hemoglobin, albumin, ALT and total bilirubin levels, preoperative hemoglobin, ALT and total bilirubin levels, BMI, and the perioperative inflammation index were important predictors in the XGBoost model. (Figure 3). The DCA demonstrated the standardized net benefit of the XGBoost model (Figure 4). Based on the DCA, the XGBoost model provided potential clinical benefit when the threshold probability was set between 0.1 and 0.7.
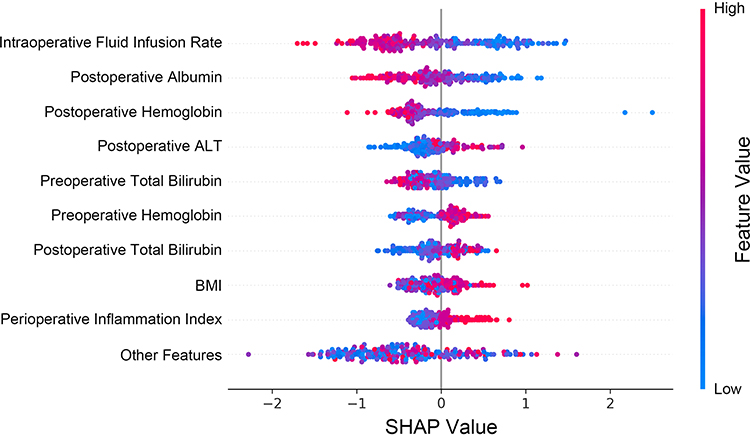 |
Figure 3 The SHAP values of the top 10 important features for the XGBoost AKI prediction model. The red and blue points indicate nodules having high to low values of the specific feature. The SHAP value in the x-axis indicates the impact of each variable on the model. |
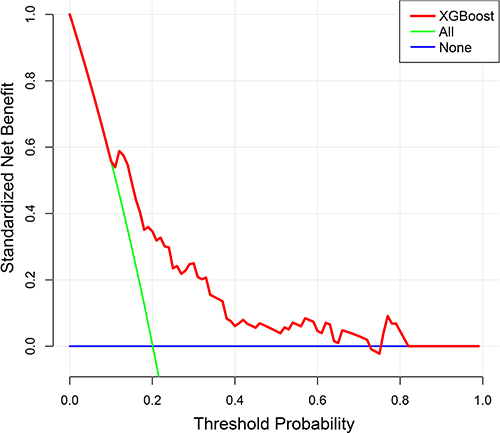 |
Figure 4 The Decision Curves of the XGBoost model. The y-axis measures the standardized net benefit. The threshold probability is presented on the x-axis. The green line represents the assumption that all patients experienced AKI after radical cystectomy. The black line represents the assumption that no postoperative AKI has occurred. Based on the red line (represents the XGBoost model), the threshold probability could be set between 10% and almost 70% when the benefit of the XGBoost model was more than either the treat-all or treat-none scheme. |
Discussion
The present study employed the RCS to transform the levels of perioperative dynamic changes of different systemic inflammatory metrics (NLR, PLR, LMR, SIRI, and SII) into categorical variables, which were then integrated as the Perioperative Inflammation Index. Furthermore, the perioperative inflammatory index, in conjunction with intraoperative fluid infusion rate and postoperative Hb and Alb levels, were identified as independent risk factors with significant predictive value for AKI after radical cystectomy. Among the multitude of machine learning AKI prediction models, the XGBoost model exhibited the most promising performance. The DCA suggested a potential clinical benefit when the XGBoost model was employed with positive decision thresholds set between 0.1 and 0.7.
The current study integrated the perioperative dynamic changes of various inflammatory markers (NLR, PLR, LMR, SIRI, and SII) into the perioperative inflammation index, thereby identifying a robust association between it and AKI after radical cystectomy. These inflammation markers are derived from routine blood tests and reflect the balance between different types of immune cells, providing insights into the body’s inflammatory state.18 Perioperative changes in these markers reflect an imbalance in the immune response and the development of systemic inflammatory response syndrome (SIRS), which can lead to tissue damage and impaired organ function.8,19 Previous studies have demonstrated that perioperative changes in NLR and PLR were valuable predictors of postoperative AKI in colorectal cancer patients,20 which was consistent with our results. The perioperative dynamic changes of these inflammatory indexes were reported to be influenced by intraoperative fluid management strategies,20 surgical manipulation stimuli,21 and anti-inflammatory drug administration.22 Therefore, the robust correlation between these inflammation metrics and AKI underscores their potential for personalized postoperative risk assessment and the tailoring of anesthetic intervention strategies.
In addition to perioperative inflammatory response, intraoperative fluid infusion rate and postoperative Hb and Alb levels were identified as independent risk factors for AKI after radical cystectomy and contributed significantly to the prediction model construction. Previous studies indicated that lower intraoperative infusion rates are associated with an increased risk of AKI due to mechanisms involving inadequate tissue perfusion, compensatory vasoconstriction, and impaired waste clearance.23,24 Considering the findings of this study, and those of previous investigations, excessively low intraoperative infusion rates should be eschewed to minimize the risk of AKI after radical cystectomy. On the other side, postoperative anemia was found to double the risk of AKI in patients undergoing total hip replacement arthroplasty,25 and postoperative hypoalbuminemia has been identified as an independent risk factor for AKI in critically ill patients.26 The findings of this study further clarify the association between intraoperative fluid infusion strategy and postoperative anemia and nutritional status with AKI after radical cystectomy, providing evidence for optimizing intraoperative management.
By leveraging large datasets that include perioperative and intraoperative variables, machine learning models offer a means to improve early detection and intervention strategies for at-risk patients for postoperative adverse events.27,28 Among the various machine learning techniques applied, ensemble algorithms like RF and XGBoost showed substantial potential in predicting postoperative AKI.29 However, specific studies directly addressing AKI prediction after radical cystectomy are limited. Therefore, this study constructed postoperative AKI prediction models for patients undergoing radical cystectomy for bladder cancer. In a manner consistent with previous studies, the predictive model with the ensemble algorithm, XGBoost, demonstrated the highest performance. This may be attributed to the advanced gradient-boosting framework of XGBoost. Furthermore, the DCA plot showed that the clinical benefit curve of the XGBoost model was higher than both the “All” and “None” strategies for thresholds between 0.1 and 0.7. The DCA result enables the evaluation of clinical relevance without the requirement for additional validation data in a traditional decision-analytic approach, justifying that the presented XGBoost model holds great potential for clinical application for predicting AKI following radical cystectomy.30
Limitations exist in the present study. Firstly, selection bias was inevitable, and establishing causation was challenging due to the observational nature of the retrospective study. Secondly, unmeasured surgical manipulation or perioperative management variables (such as the existence of intraoperative hypotension) may diminish predictive models’ performance. Thirdly, the final analysis was conducted on a relatively small sample size. Therefore, multicenter prospective large-sample studies should be conducted to verify the causal association between perioperative data and AKI after radical cystectomy for bladder cancer.
Conclusion
This study revealed an intimate association between a group of perioperative evaluation and management variables, including the degree of perioperative inflammatory response activation, and AKI after radical cystectomy. AKI predictions of machine learning models developed in this study enabled early interventions, such as medication adjustments and optimized fluid management, tailored to individual patient risk profiles. This personalized approach not only improves patient outcomes but also aids in efficient resource allocation, ensuring high-risk patients receive the necessary care and monitoring.
Ethics Approval and Informed Consent
Ethical approval was obtained from the institutional review boards of all participating centers (approval number: SYSKY-2023-165-01). The present study was followed in concordance with the Declaration of Helsinki. Patient consent was waived due to the retrospective nature of the study. All patient data were anonymized and handled in accordance with relevant data protection regulations to ensure confidentiality.
Funding
This study was supported by the Science and Technology Projects in Guangzhou [grant number 2023A04J2102]. The funding organizations had no role in the conceptualization, design, data collection, analysis, decision to publish, or preparation of the paper.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Joung KW, Choi SS, Kong YG, et al. Incidence and risk factors of acute kidney injury after radical cystectomy: importance of preoperative serum uric acid level. Int J Med Sci. 2015;12(7):599–604. doi:10.7150/ijms.12106
2. Hanna PT, Peterson M, Albersheim J, et al. Acute kidney injury following enhanced recovery after surgery in patients undergoing radical cystectomy. J Urol. 2020;204(5):982–988. doi:10.1097/JU.0000000000001153
3. Kwon T, Jeong IG, Lee C, et al. Acute kidney injury after radical cystectomy for bladder cancer is associated with chronic kidney disease and mortality. Ann Surg Oncol. 2016;23(2):686–693. doi:10.1245/s10434-015-4886-4
4. Ikehata Y, Tanaka T, Ichihara K, et al. Incidence and risk factors for acute kidney injury after radical cystectomy. Int J Urol. 2016;23(7):558–563. doi:10.1111/iju.13104
5. watt DG, McSorley ST, Park JH, Horgan PG, McMillan DC. A postoperative systemic inflammation score predicts short- and long-term outcomes in patients undergoing surgery for colorectal cancer. Ann Surg Oncol. 2017;24(4):1100–1109. doi:10.1245/s10434-016-5659-4
6. Bain CR, Myles PS, Corcoran T, Dieleman JM. Postoperative systemic inflammatory dysregulation and corticosteroids: a narrative review. Anaesthesia. 2023;78(3):356–370. doi:10.1111/anae.15896
7. Liu Z, Wu H, Liufu N, et al. Development and validation of a nomogram incorporating selected systemic inflammation-based prognostic marker for complication prediction after vascularized fibula flap reconstruction. Oral Oncol. 2019;99:104467. doi:10.1016/j.oraloncology.2019.104467
8. Yang Z, Qiao Y, Wang D, Yan G, Tang C. Association between inflammatory biomarkers and contrast-induced acute kidney injury in ACS patients undergoing percutaneous coronary intervention: a cross-sectional study. Angiology. 2023;75(9):831–40.
9. Ma K, Qiu H, Zhu Y, Lu Y, Li W. Preprocedural SII combined with high-sensitivity c-reactive protein predicts the risk of contrast-induced acute kidney injury in stemi patients undergoing percutaneous coronary intervention. J Inflamm Res. 2022;15:3677–3687. doi:10.2147/JIR.S370085
10. Shu B, Xu F, Zheng X, et al. Change in perioperative neutrophil-lymphocyte ratio as a potential predictive biomarker for chronic postsurgical pain and quality of life: an ambispective observational cohort study. Front Immunol. 2023;14:1177285. doi:10.3389/fimmu.2023.1177285
11. Bae MI, Shim J-K, Song JW, Ko SH, Choi YS, Kwak Y-L. Predictive value of the changes in neutrophil-lymphocyte ratio for outcomes after off-pump coronary surgery. J Inflamm Res. 2023;16:2375–2385. doi:10.2147/JIR.S411057
12. Parlar H, Arıkan AA, Önmez A. Dynamic changes in perioperative cellular inflammation and acute kidney injury after coronary artery bypass grafting. Braz J Cardiovasc Surg. 2021;36(3):354–364. doi:10.21470/1678-9741-2020-0163
13. Penny-Dimri JC, Bergmeir C, Reid CM, Williams-Spence J, Cochrane AD, Smith JA. Machine learning algorithms for predicting and risk profiling of cardiac surgery-associated acute kidney injury. Semin Thorac Cardiovasc Surg. 2021;33(3):735–745. doi:10.1053/j.semtcvs.2020.09.028
14. Lei G, Wang G, Zhang C, Chen Y, Yang X. Using machine learning to predict acute kidney injury after aortic arch surgery. J Cardiothorac Vasc Anesth. 2020;34(12):3321–3328. doi:10.1053/j.jvca.2020.06.007
15. He ZL, Zhou JB, Liu ZK, et al. Application of machine learning models for predicting acute kidney injury following donation after cardiac death liver transplantation. Hepatobiliary Pancreat Dis Int. 2021;20(3):222–231. doi:10.1016/j.hbpd.2021.02.001
16. Lei L, Wang Y, Xue Q, Tong J, Zhou CM, Yang JJ. A comparative study of machine learning algorithms for predicting acute kidney injury after liver cancer resection. PeerJ. 2020;8:e8583.
17. Mehta RL, Kellum JA, Shah SV, et al. Acute kidney injury network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11(2):R31. doi:10.1186/cc5713
18. Aringer M. Inflammatory markers in systemic lupus erythematosus. J Autoimmun. 2020;110:102374. doi:10.1016/j.jaut.2019.102374
19. Peng C, Li J, Xu G, Jin J, Chen J, Pan S. Significance of preoperative systemic immune-inflammation (SII) in predicting postoperative systemic inflammatory response syndrome after percutaneous nephrolithotomy. Urolithiasis. 2021;49(6):513–519. doi:10.1007/s00240-021-01266-2
20. Chan JCY, Diakos CI, Chan DLH, et al. A longitudinal investigation of inflammatory markers in colorectal cancer patients perioperatively demonstrates benefit in serial remeasurement. Ann Surg. 2018;267(6):1119–1125. doi:10.1097/SLA.0000000000002251
21. Rossaint J, Zarbock A. Perioperative inflammation and its modulation by anesthetics. Anesth Analg. 2018;126(3):1058–1067. doi:10.1213/ANE.0000000000002484
22. Lin JX, Wang ZK, Huang YQ, et al. Dynamic changes in pre- and postoperative levels of inflammatory markers and their effects on the prognosis of patients with gastric cancer. J Gastrointest Surg. 2021;25(2):387–396. doi:10.1007/s11605-020-04523-8
23. Ma AEA, Grass F, Calini G, et al. Intraoperative fluid management a modifiable risk factor for surgical quality - improving standardized practice. Ann Surg. 2022;275(5):891–896. doi:10.1097/SLA.0000000000005384
24. Burkhard FC, Studer UE, Wuethrich PY. Superior functional outcome after radical cystectomy and orthotopic bladder substitution with restrictive intraoperative fluid management: a followup study of a randomized clinical trial. J Urol. 2015;193(1):173–178. doi:10.1016/j.juro.2014.07.109
25. Choi YJ, Kim SO, Sim JH, Hahm KD. Postoperative anemia is associated with acute kidney injury in patients undergoing total hip replacement arthroplasty: a retrospective study. Anesth Analg. 2016;122(6):1923–1928. doi:10.1213/ANE.0000000000001003
26. Yoon HJ, Kim TH, Ko DE, Song JW, Min N, Ham SY. Postoperative hypoalbuminemia as a predictor of acute kidney injury after open repair of ruptured abdominal aortic aneurysm. World J Surg. 2023;47(12):3382–3393. doi:10.1007/s00268-023-07178-z
27. Mahajan A, Esper S, Oo TH, et al. Development and validation of a machine learning model to identify patients before surgery at high risk for postoperative adverse events. JAMA Netw Open. 2023;6(7):e2322285. doi:10.1001/jamanetworkopen.2023.22285
28. Wu X, Hu J, Zhang J. Machine learning-based model for predicting major adverse cardiovascular and cerebrovascular events in patients aged 65 years and older undergoing noncardiac surgery. BMC Geriatr. 2023;23(1):819. doi:10.1186/s12877-023-04509-6
29. Tseng PY, Chen YT, Wang CH, et al. Prediction of the development of acute kidney injury following cardiac surgery by machine learning. Crit Care. 2020;24(1):478. doi:10.1186/s13054-020-03179-9
30. Vickers AJ, Elkin EB. Decision curve analysis: a novel method for evaluating prediction models. Med Decis Making. 2006;26(6):565–574. doi:10.1177/0272989X06295361
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.