")
Back to Journals » Clinical Interventions in Aging » Volume 13
Integrating participatory ergonomic management in non-weight-bearing exercise and progressive resistance exercise on self-care and functional ability in aged farmers with knee osteoarthritis: a clustered randomized controlled trial
Authors Isaramalai SA , Hounsri K , Kongkamol C, Wattanapisitkul P , Tangadulrat N, Kaewmanee T, Yuenyongviwat V
Received 19 June 2017
Accepted for publication 20 October 2017
Published 17 January 2018 Volume 2018:13 Pages 101—108
DOI https://doi.org/10.2147/CIA.S144288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Sang-arun Isaramalai,1 Kanokwan Hounsri,1 Chanon Kongkamol,2 Pornnit Wattanapisitkul,3 Napaporn Tangadulrat,3 Tippawan Kaewmanee,3 Varah Yuenyongviwat4
1Research Center for Caring System of Thai Elderly, Faculty of Nursing, 2Research Unit of Holistic Health and Safety Management in Community, Faculty of Medicine, 3Department of Physical Therapy, Faculty of Medicine, 4Department of Orthopaedic Surgery and Physical Medicine, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, Thailand
Background: Ergonomic hazards are the most important cause of knee osteoarthritis (OA) in aged para rubber farmers. Ergonomic management comprising improvement of working conditions and muscle-strengthening exercise has been well documented in terms of workers’ health benefit. However, those interventions were not adequate to sustain the advantage. Few studies have demonstrated the effect of integrating participatory ergonomic management (PEM) in non-weight-bearing exercise (NWE) and progressive resistance exercise (PRE), and none has focused on aged para rubber farmers with knee OA.
Purpose: This study investigated the effect of PEM-NWE, PEM-PRE, and standard treatment (ST) on self-care and functional ability in the aged population.
Materials and methods: A single-blinded, clustered randomized controlled trial was carried out. Participants (n=75) from three different communities in southern Thailand were randomly assigned to PEM-NWE, PEM-PRE, and ST. Self-care and functional ability (pain, stiffness, and physical function) were examined at baseline (B), during the intervention at Week 5 (W5), and after its completion at Week 9 (W9). Mean comparison of those outcomes over time was made using Generalized Linear Mixed Models (GLMMs).
Results: Compared to the standard treatment, the means of both groups, PEM-NWE and PEM-PRE, were significantly increased in self-care and functional ability. However, no significant difference between PEM-NWE and PEM-PRE was found.
Conclusion: Either or both interventions should be incorporated into nursing practice in order to promote occupational health and enhance quality of work life for Thai aged farmers. Further study on their cost-effectiveness is highly recommended.
Keywords: farmer, osteoarthritis, ergonomic, self-care, functional ability
Introduction
The rising prevalence of global disability with age increases the potential impact of knee osteoarthritis (OA) upon healthcare services.1 The association of knee OA with increasing obesity, sequelae of joint injury, loss of muscle strength, and occupational risk factors has been established.2,3 Briefly, a concomitant change in bone, muscle, and adipose tissue composition was explained as a consequence of deterioration in elder body composition, leading to decreased functionality.4
Aged para rubber farmers in Thailand habitually undertake tasks that involve high loading intensity on the knee from inappropriate postures and repetitive muscle work. Squatting or kneeling is usually done during low tapping, molding, or filtering latex, whereas knee bending is observed during knife sharpening. In addition, heavy lifting or carrying is found in the latex handling process.5 According to a problems survey of the population, ~38% of aged para rubber farmers reported knee pain related to occupational activities.6 Moreover, impacts of those hazards on their occupational activities are the leading cause for developing knee OA, functional impairment, and decreasing quality of life.3,7
To improve physical function and occupational performance, ergonomic management comprising joint protection strategies related to modified working conditions and muscle-strengthening exercise have been well documented with regard to workers’ health benefit, especially in persons with knee OA.8 However, ergonomic interventions focusing on the improvement of working conditions only may not be sufficient for these aged individuals in enhancing functional ability. Therefore, this measure needs to be combined with muscle-strengthening exercise.9
According to the Cochrane review on exercise for OA of the knee, both non-weight-bearing exercise (NWE) and progressive resistance exercise (PRE) reduce pain and increase functional ability in older individuals.10 Compared to PRE, NWE is more effective for short-term reduction of pain in people with knee OA, whereas PRE specifically improves physical functioning, strength, and performance of either simple or complex activities, and reduces adverse events – including muscle strain and joint pain – from excessive weight.11,12 However, the benefit of both exercise types on functional ability remains unclear.10
In addition, a systematic review found that participatory ergonomic approaches (PEAs) could significantly maximize workers’ health outcomes, such as musculoskeletal symptom relief and muscle injury prevention.13,14 The main concept of PEA is that self-care behavioral promotion requires strategies for enhancing ergonomic management and helps to overcome barriers to behavioral changes. PEA processes comprise raising risk awareness and attitudes toward ergonomic measures by problem-solving approaches. Consequently, solution implementation will be carried out for enhancing the ability to change behaviors.14 Thus, stages of self-care operations – estimative, transitive, and productive operations – were adopted to enhance PEA processes.
Self-care operations are important to develop a nursing program aiming to improve the workers’ capabilities on responding to their self-care needs. A supportive–educative system promoting the clients’ knowledge, motivation, and practice skills was designed by using four helping methods, such as teaching, guiding, supporting, and providing environment.15 The program would enable aged rubber farmers with knee OA to gain knowledge and skills that lead them to care for themselves.
However, the existing knowledge of the integrating effect of participatory ergonomic management (PEM) and strengthening exercises (NWE and PRE) is limited. This study developed those strategies in ergonomic management for investigating the effect of PEM-NWE, PEM-PRE, and standard treatment on self-care and functional ability in aged para rubber farmers with knee OA. It might be worthwhile in terms of cost-effectiveness and efficacy of the intervention to promote self-care and functional ability for the population.
Materials and methods
Study design
Three primary care units (PCUs) were randomly allocated to one of three intervention arms, comprising PEM-NWE, PEM-PRE, and standard treatment (ST), conducted over an 8-week period, during January to March 2015 after approval by the Research Ethics Committee, Faculty of Medicine, Prince of Songkhla University (Thai Clinical Trial Number TCTR20160219001).
Subjects and eligibility
Para rubber farmers aged ≥60 years who currently had symptomatic knee OA, as determined by the clinical and radiographic criteria of the American College of Rheumatology16 and the Kellgren–Lawrence radiographic grading scale (<4), were selected from each of three PCUs. Patients with a history of major knee injury, knee surgery, or steroid injection, as well as those having a contraindication to strengthening exercise such as uncontrolled hypertension, inflamed knee during exercise, cognitive dysfunction, or planning for knee surgery, were excluded.
Clustered randomization procedure
A random number sequence was generated by package integrated computing environment, R. Clusters. The sample size was calculated based on our pilot study17 using the command “lmmpower” in package “longpower”; the R program yielded a sample size of 25 participants in each group (PEM-NWE, PEM-PRE, and ST). Because we expected that more aged workers would withdraw from the ergonomic management and strengthening exercise intervention, we added 20% participants to protect against dropout. In the trial, CK prepared the allocation sequence list, and KH carried out the allocation through identification of home and working areas of the volunteers. All potential participants were informed about the study purpose; what their participation would involve; confidentiality and autonomy issues; and the right to withdraw at any time. Those who agreed to participate were asked to sign a written informed consent form at the first visit. All participants completed the study program to which they were allocated (Figure 1).
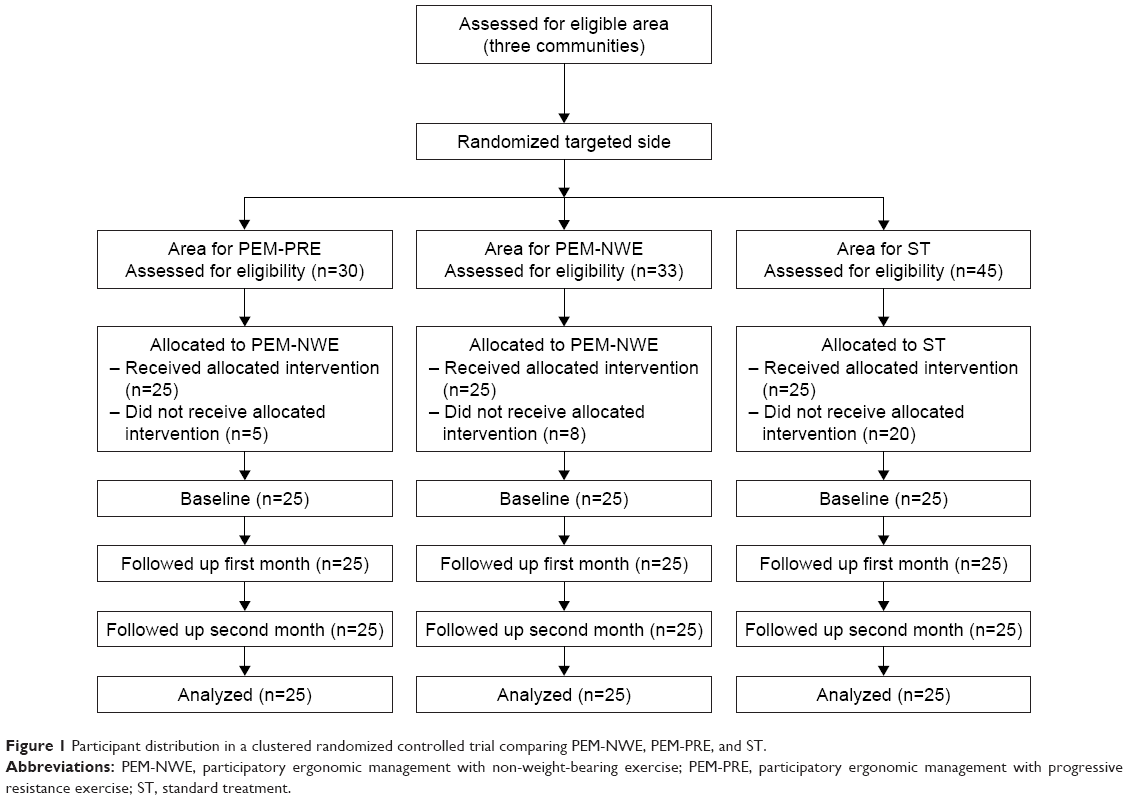 | Figure 1 Participant distribution in a clustered randomized controlled trial comparing PEM-NWE, PEM-PRE, and ST. |
Interventions
A pretest of participants’ demographics, self-care behaviors, and functional ability was conducted in the PEM-NWE, PEM-PRE, and ST groups. ST received usual care services, based on standard protocols, coupled with a 2-hour boosted educational session, whereas PEM-NWE and PEM-PRE received both center-based and home-based activities as follows.
Center-based interventions were held at community centers.
- Twenty-minute job hazard analysis: group discussion using flip chart on ergonomic risk factors in working process that increase the severity of knee OA, such as low-level tapping, knife sharpening, and latex manual handling, and their self-care management was undertaken.
- One-hour health education session: A 20-minute teaching and a 40-minute exercise demonstration on ergonomic management (working conditions and muscle-strengthening exercise) through participatory group discussion.
- Thirty-minute mutual goal setting: The identified risks factors from job hazard analysis and actions that needed to be carried out were analyzed. Individual goals and action plans were designed into daily living activities under the supervision of ergonomists, physical therapists, and nurse practitioners. Ten-minute guiding for self-monitoring record on ergonomic management using logbook was provided.
Home-based interventions were conducted every other week.
Thirty-minute home visits were carried out for providing guidance and support. Participants’ barriers to ergonomic management were analyzed and alternatives were suggested; moreover, participants were encouraged to implement them in their daily life.
Exercise procedures
With regard to the procedures of both exercise programs, all participants were required to complete their own exercise programs at least 3 days per week for 8 weeks. Both exercise programs were designed to increase lower extremity muscle strength bilaterally around the hip and knee joints (Table 1).
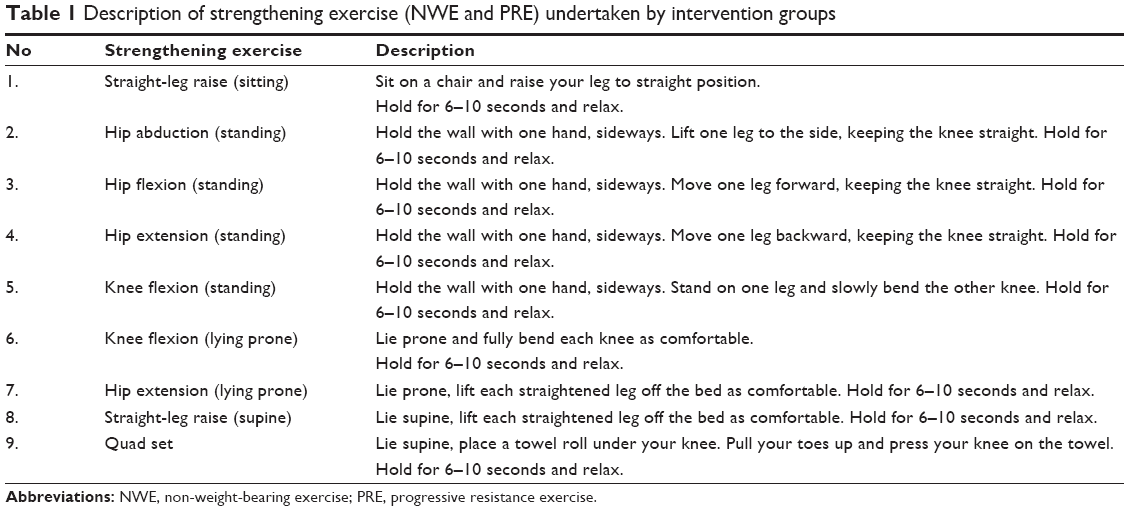 | Table 1 Description of strengthening exercise (NWE and PRE) undertaken by intervention groups |
The exercise sessions included at least three sets of ten repetitions of nine exercises. Each exercise started with dynamic movement through the full range of motion and continued to a 10-second hold static movement at the end of the range of movement. The repetitions and durations of exercises were self-prescribed by participants based on PEM.
In the PRE group, intensity was based on participants’ ability to execute a maximum of 10 repetitions (10 RM). Sandbags were used for the weight increments, starting from 50% of 10 RM in the first to second week, increasing to 75% of 10 RM in the third to fourth week, and reaching 100% of 10 RM in the fifth to eighth week. The load adjustment took place under the supervision of an experienced physical therapist to yield a gradual progression of training.
Furthermore, a muscle-strengthening training booklet was given to each exercise group. The NWE booklet explained nine exercises of unweighted leg movement, whereas the PRE booklet described nine sandbag exercises. All exercise sessions were self-conducted and took place at home. Home visitation by a physical therapist and nurse practitioner was conducted every 2 weeks to enhance participant compliance and exercise.
Instruments
The Demographic and Health Information Form (DHFF), developed by KH, consists of close-ended checklists of participants’ general data such as gender, age, and education level; work characteristics such as working areas – flat, slope, and hillside – tapping level; and extra work, including health status indicators such as waist circumference, symptoms, and pain onset.
The Thai version of Self-Care Questionnaires (Thai-SCQ), modified from Boonsrichan,18 comprises three phases of self-care (estimative, transitive, and productive). A total of 15 items were scored on the 5-point Likert scale, with a higher score indicating higher self-care. Its Cronbach’s alpha coefficient was 0.82.
The modified Thai version of Western Ontario and McMaster Universities Osteoarthritis (WOMAC) comprises 24 self-report items with numeric rating scale categorized into pain (5 items), stiffness (2 items), and physical function (17 items). A higher score indicates a lower functional ability. Reliability evaluation using the test–retest method yielded 86% agreement.
Data analysis
Data analyses were conducted with R 3.2.5. One-way ANOVA, Kruskal–Wallis test, and chi-square test were used to compare data of three randomized groups at baseline. Means of self-care and functional ability were compared between PEM-NWE versus ST and PEM-PRE versus ST on the Generalized Linear Mixed Model (GLMM) using package “nlme”, and additional p-values were calculated based on Satterthwaite’s approximations using “lmerTest”. Stepwise regressions were conducted considering Akaike Information Criterion or log-likelihood, depending on their intraclass correlation of variances. The significance level was set at 0.05 (two-tailed).
Results
Participant characteristics at baseline
The majority of the study population was female, and the mean age (±SD) was 66.9±4.5 years for PEM-NWE, 68±5.8 years for PEM-PRE, and 63.7±4.3 years for ST, which was significantly different between the three groups. In addition, significant differences in their working areas (flat and hillside), tapping level (upper knee to below waist), extra work (gardener and farmers), and waist circumference existed (p<0.01). However, no significant difference was observed in gender, years of working, working hours, and body mass index (BMI) (p>0.05; Table 2).
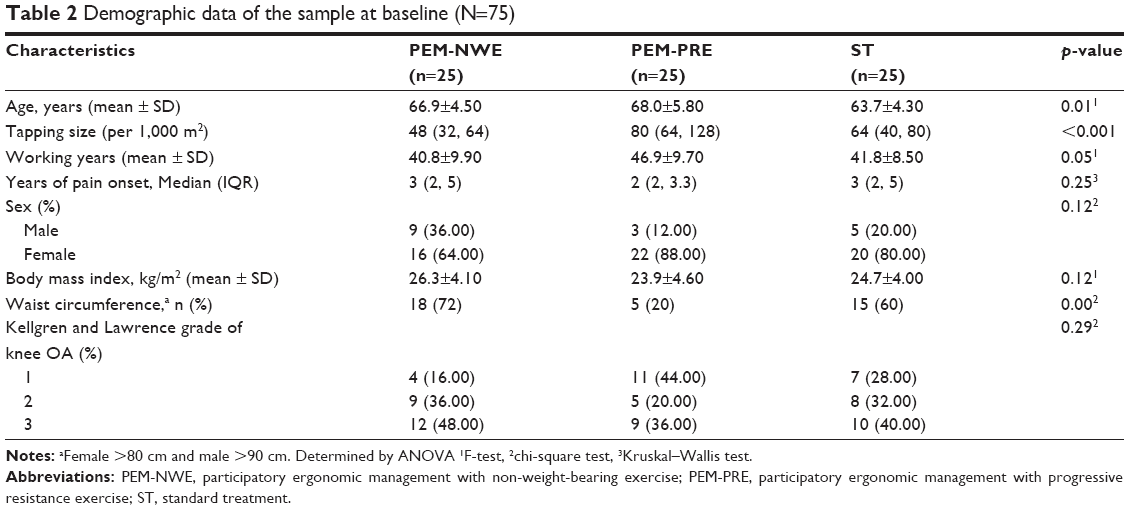 | Table 2 Demographic data of the sample at baseline (N=75) |
Self-care
At the end of the trial, GLMM analyses revealed statistically significant differences in self-care between groups in the mixed-effect model in which all time points were included (p<0.001; R2GLMM(c) =0.59). Both PEM-NWE and PEM-PRE showed a significant difference in the total mean score of self-care (p<0.05; Table 3).
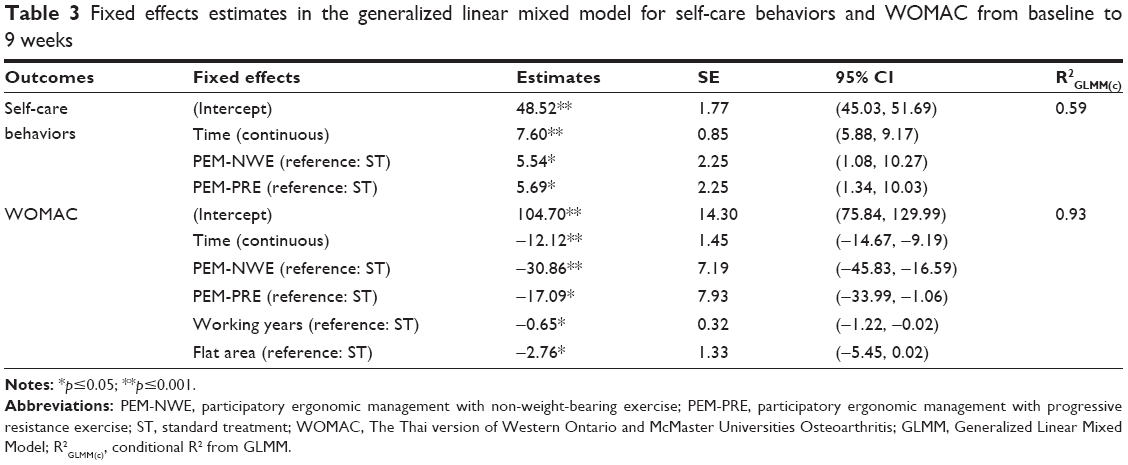 | Table 3 Fixed effects estimates in the generalized linear mixed model for self-care behaviors and WOMAC from baseline to 9 weeks |
The total self-care mean score of the PEM-NWE considerably increased from 49.60±14.87 at baseline (B) to 67.40±10.86 at W5, and slightly increased to 68.52±10.99 at W9. Similarly, the total mean scores of the PEM-PRE increased from 51.96±9.21 at B to 65.92±10.64 at W5 and slightly increased to 67.6±12.35 at W9. The total mean scores of the ST increased from 48.48±9.68 at B to 59.76±8.78 at W5 and to 59.52±7.57 at W9 (Table 4).
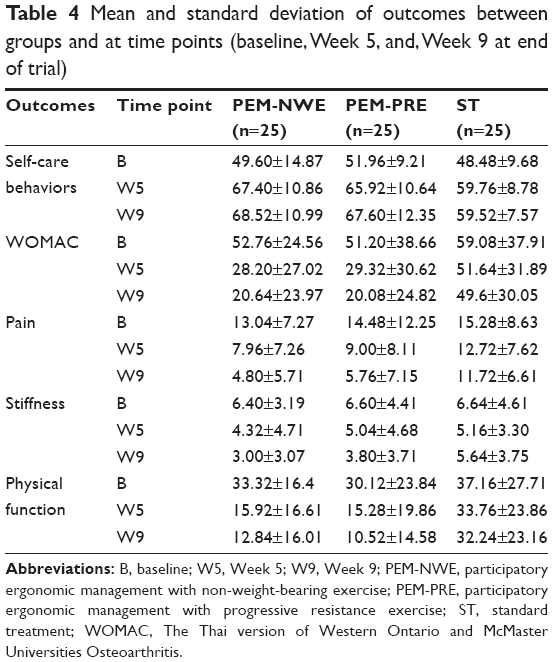 | Table 4 Mean and standard deviation of outcomes between groups and at time points (baseline, Week 5, and, Week 9 at end of trial) |
Functional ability
At the end of the trial, GLMM analyses revealed statistically significant differences in functional ability between groups in the mixed-effect model wherein all time points were included (p<0.001; R2GLMM(c) =0.93). Both PEM-NWE and PEM-PRE showed a significant difference from the ST in the total mean score of functional ability (p<0.05; Table 3).
The total mean scores of functional ability in the PEM-NWE considerably decreased from 52.76±24.56 at B to 28.20±27.02 at W5 and slightly increased to 20.64±23.97 at W9. Similarly, the total mean scores of the PEM-PRE decreased from 51.20+38.66 at B to 29.32+30.62 at W5, and slightly increased to 20.08+20.08 at W9. The total mean scores of the ST decreased from 59.08±37.91 at B to 51.64±31.89 at W5 and to 49.60±30.05 at W9 (Table 4).
Moreover, pain was significantly correlated after adjusting working experience, working area (slope), and Kellgren–Lawrence grade 3 (p<0.05). There was a significant time-by-group and age interaction for physical abilities (p<0.01). In contrast, the improvement in the stiffness subdomain was not significantly greater in the PEM-NWE and PEM-PRE compared with the ST (p>0.05).
Discussion
Results of this study showed that the effect of integrating PEM in NWE and PRE could improve self-care and functional ability in aged para rubber farmers with knee OA as compared with those who received booster educational information. Both intervention groups spectacularly enhanced self-care and functional ability during 1 month and showed slight improvement after completing the program (2 months). Findings imply that PEM based on the process of self-care operation was effective in increasing self-care by the aged para rubber farmers and eventually improved functional ability.
The increasing self-care in the aged para rubber farmers resulted from a combination of participatory ergonomic education through group discussion with mutual goal setting and home visits. Understanding ergonomic risk factors threatening knee OA through group discussion leads to recognition of their care demands. Self-care actions need to be undertaken for controlling knee OA severity such as avoiding or arranging risky postures and organizing workstation. The educational strategy is based on the experiential learning theory that helps in developing self-care ability through learning through direct experiences and communication with others.19 This finding is consistent with those from previous studies, demonstrating that implementation of PEM can be effective in reducing pain and work disability.20,21
Home visitation is another important part of enhancing self-care behaviors. The process was linked to better implementation of ergonomic self-care confidence because of guidance, self-evaluation, and self-refection by an aged working population. Moreover, motivation related to provision of continuous positive feedback supports elder workers to reach clear destinations. Previous studies found that home visitation was a significant predictor of life-quality improvement for knee OA.22,23
Mutual goal setting is a core strategy used in both group discussions and home visits. Individual action planning in daily work of elderly workers helped maximize practicability of performance. These procedures enable each aged participant to choose an appropriate strategy for considering the possibility in self-care operations. The process helps participants gain more confidence before practice because of continuous self-evaluation of their health status and support by healthcare providers. Results were supported by evidences that self-judgment and self-reaction are strategies to enhance self-management in diminishing the severity of knee OA.22,24
Muscle-strengthening exercise is a key component of conservative treatment that significantly improves functional ability among aged workers with knee OA. This exercise substantially increases the function of the quadriceps, hip abductors, hip extensors, hamstrings, and calf muscles, all of which should be particularly targeted in individuals with knee OA.9 Stronger quadriceps can absorb shock of movement and reduce ground reaction forces to minimize pain in individuals with knee OA during weight-bearing activities.25
This finding was consistent with those of Tanaka et al,11 who mentioned that NWE is the most effective exercise for pain relief in the short term, compared with PRE and aerobic exercise. A significant improvement in WOMAC scores in terms of significant pain reduction, joint stiffness, and physical function was confirmed, compared to minimal clinically important improvement (MCII). PEM-NWE had exactly the same efficacy as PEM-PRE in reducing pain and increasing physical function when assessed using MCII(pain) =−40.8% and MCII(function) =−26.0%.26 With an important difference in regard to pain and physical function, PEM-NWE achieves considerably more pain reduction than does PEM-PRE (MCII(pain) =−63.19% and −60.22%, respectively), whereas PEM-PRE achieves greater increase in physical function than does PEM-NWE (MCII(function) =−65.07% and −61.46%, respectively).
A specified success factor in the study intervention comes from incorporating a mixed-skill health team, consisting of the ergonomist, physical therapist, and nurse practitioner to enhance self-care behaviors. The ergonomist analyzed ergonomic risks and advised on appropriate practical ergonomic self-care. The physical therapist designed and demonstrated the exercise techniques. The nurse practitioner guided and directed the course of ergonomic self-care, and provided physical or psychological support continuously. A mixed team of qualified personnel with specialty certifications helped to improve self-care behaviors and achieve better clinical outcomes because of team coordination.27
The findings of this study in aged para rubber farmers in Thailand may not be generalizable to other countries. In addition, almost all of the aged farmers with knee OA involved in the trial were women. The applicability of these findings to aged males, therefore, may be limited. This study examined the effects of PEM with muscle-strengthening exercise only upon trial completion. As a result, no determination was undertaken with regard to long-term effects. Furthermore, postural and workplace environmental modifications were difficult for informal workers in natural environments. However, nurse practitioners and healthcare providers can adopt PEA incorporated into home visits.
These findings are important – both for policymakers aiming to ensure care for older workers with chronic disease and community healthcare providers, to expand their roles in the health of the aged population. An approach is needed to consider the participation of policymakers and healthcare providers for promoting sustainable development in communities. A longitudinal study needs to be conducted for the purpose of determining whether the trial provides positive, long-term effects on improving self-care and functional ability among aged para rubber farmers with knee OA. Moreover, in regard to its effect on functional mobility of older individuals, future study needs to consider its outcome evaluation using physical performance tests.
Conclusion
Findings from this study support the hypothesis that integrating the PEM in NWE and PRE based on the theory of self-care operations contributes to positive effects of self-care and functional ability for aged para rubber farmers with knee OA in 2 months. The program may be a beneficial intervention that could be used for improving health and work capability in informal aged workers with chronic health conditions, as previously mentioned in the literature.
Acknowledgments
This work was supported by the Higher Education Research Promotion and National Research University Project of Thailand, Office of the Higher Education Commission. The authors thank the three PCUs and their health volunteers.
Disclosure
The authors report no conflicts of interest in this work.
References
Cross M, Smith E, Hoy D, et al. The global burden of hip and knee osteoarthritis: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(7):1323–1330. | ||
Silverwood V, Blagojevic-Bucknall M, Jinks C, Jordan JL, Protheroe J, Jordan KP. Current evidence on risk factors for knee osteoarthritis in older adults: a systematic review and meta-analysis. Osteoarthr Cart. 2015;23(4):507–515. | ||
Ezzat AM, Li LC. Occupational physical loading tasks and knee osteoarthritis: a review of the evidence. Physiother Can. 2014;66(1): 91–107. | ||
Jafarinasabian P, Inglis JE, Reilly W, Kelly OJ, Ilich JZ. Aging human body: changes in bone, muscle and body fat with consequent changes in nutrient intake. J Endocrinol. 2017;234(1):R37–R51. | ||
Bensa-ard N. Work Condition and Musculoskeletal Pain Among Para Rubber Planters: A Case Study in Tambon Nakleua Kantang, Changwat Trang [dissertation]. Songkhla: Prince of Songkla University; 2002. Thai. | ||
Teerachitkul J, Naka K, Boonphadh P. Management of muscular aches and pains in old-age rubber tappers. Thai J Nurs Council. 2012;27(2):134–147. | ||
Verbeek J, Mischke C, Robinson R, et al. Occupational exposure to knee loading and the risk of osteoarthritis of the knee: a systematic review and a dose-response meta-analysis. Saf Health Work. 2017;8(2):130–142. | ||
Yuenyongviwat V. Knee osteoarthritis. In: Kongkamol P, Siriruk T, Ngamchaliew T, editors. Common Problems in Family Practice. Songkhla: Chanmueng Press; 2012. | ||
Bennell KL, Hinman RS. A review of the clinical evidence for exercise in osteoarthritis of the hip and knee. J Sci Med Sport. 2011;14(1):4–9. | ||
Fransen M, McConnell S, Harmer AR, Van der Esch M, Simic M, Bennell KL. Exercise for osteoarthritis of the knee: a Cochrane systematic review. Br J Sports Med. 2015;49(24):1554–1557. | ||
Tanaka R, Ozawa J, Kito N, Moriyama H. Efficacy of strengthening or aerobic exercise on pain relief in people with knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Clin Rehabil. 2013;27(12):1059–1071. | ||
Liu CJ, Latham NK. Progressive resistance strength training for improving physical function in older adults. Cochrane Database Syst Rev. 2009;(3):CD002759. | ||
Cantley LF, Taiwo OA, Galusha D, et al. Effect of systematic ergonomic hazard identification and control implementation on musculoskeletal disorder and injury risk. Scand J Work Environ Health. 2014;40(1):57–65. | ||
Rivilis I, Van Eerd D, Cullen K, et al. Effectiveness of participatory ergonomic interventions on health outcomes: a systematic review. Appl Ergon. 2008;39(3):342–358. | ||
Orem DE. Nursing: Concepts of Practice. St. Louis, MO: Mosby; 2001. | ||
Altman R, Asch E, Bloch D, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986;29(8):1039–1049. | ||
Hounsri K. Effect of Ergonomic Self-Care Promoting Program on Self-Care and Severity of Knee Osteoarthritis in Aged Para Rubber Farmers [dissertation]. Songkhla: Prince of Songkla University; 2015. Thai. | ||
Boonsrichan B. Selected Basic Conditioning Factors, Self-Care Agency, and Self-Care for Symptom Control of Low Back Pain among Tapping Workers in Para Rubber Plantation [dissertation]. Songkhla: Prince of Songkla University; 2006. Thai. | ||
Heinrich W, Rivera JE. A framework for PLA in traditional higher education: experiential learning assessment for embedded outcomes. PLA Inside Out. 2016;(5):1–16. | ||
Cloostermans L, Bekkers MB, Uiters E, Proper KI. The effectiveness of interventions for ageing workers on (early) retirement, work ability and productivity: a systematic review. Int Arch Occup Environ Health. 2015;88(5):521–532. | ||
Sundstrup E, Jakobsen MD, Andersen CH, et al. Participatory ergonomic intervention versus strength training on chronic pain and work disability in slaughterhouse workers: study protocol for a single-blind, randomized controlled trial. BMC Musculoskelet Disord. 2013;14:67. | ||
Kao MH, Tsai YF, Chang TK, Wang JS, Chen CP, Chang YC. The effects of self-management intervention among middle-age adults with knee osteoarthritis. J Adv Nurs. 2016;72(8):1825–1837. | ||
Saraboon Y, Aree-Ue S, Maruo SJ. The effect of multifactorial intervention programs on health behavior and symptom control among community-dwelling overweight older adults with knee osteoarthritis. Orthop Nurs. 2015;34(5):296–308. | ||
Nochit W, Kaewthummanukul T, Srisuphan W, Senaratana W. Effects of working behavior modification program on low back pain prevention behaviors and back muscle endurance among Thai farmers. Pac Rim Int J Nurs Res Thail. 2014;18(4):305–319. | ||
Lim BW, Hinman RS, Wrigley TV, Sharma L, Bennell KL. Does knee malalignment mediate the effects of quadriceps strengthening on knee adduction moment, pain, and function in medial knee osteoarthritis? A randomized controlled trial. Arthritis Rheum. 2008;59(7):943–951. | ||
Tubach F, Ravaud P, Baron G, et al. Evaluation of clinically relevant changes in patient reported outcomes in knee and hip osteoarthritis: the minimal clinically important improvement. Ann Rheum Dis. 2005;64(1):29–33. | ||
Dubois CA, Singh D. From staff-mix to skill-mix and beyond: towards a systemic approach to health workforce management. Hum Resour Health. 2009;7:87. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.