Back to Journals » Advances in Medical Education and Practice » Volume 17
Integrating Health Communication into Basic Medical Courses: A Qualitative Study for Enhancing Professional Competencies in Undergraduate Medical Students
Authors Shi L, Yang K, Zeng J, Liu C, Zhao Y, Song H, Zhang Z, Lu L
Received 25 April 2026
Accepted for publication 13 June 2026
Published 21 June 2026 Volume 2026:17 619791
DOI https://doi.org/10.2147/AMEP.S619791
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sateesh Arja
Lihong Shi,1 Kun Yang,2 Junfeng Zeng,1 Chengfang Liu,1 Yunhe Zhao,1 Huifang Song,1 Zhong Zhang,1 Li Lu1,3
1School of Basic Medical Sciences, Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China; 2School of Clinical Medicine, Shanxi Medical University, Taiyuan, Shanxi, 030001, People’s Republic of China; 3Key Laboratory of Cellular Physiology of Chinese Ministry of Education, Shanxi Medical University, Taiyuan, Shanxi, People’s Republic of China
Correspondence: Li Lu, School of Basic Medical Sciences, Shanxi Medical University, Taiyuan, Shanxi, 030001, People’s Republic of China, Email [email protected]
Purpose: Medical students frequently undervalue basic medical courses prior to clinical training, resulting in learning difficulties. Current pedagogical approaches fail to integrate basic medical sciences with essential health communication skills. Consequently, strategies are needed to help students promptly recognize the value of basic courses while developing core communication competencies.
Methods: This qualitative study explored the integration of health communication activities into basic medical courses for 42 undergraduate medical students (Years 1– 3). Students engaged in structured communication tasks and composed reflections on the relationship between basic science and health communication. Additionally, semi-structured interviews with 15 community members were conducted to assess their perceptions of students’ communication. Applied thematic analysis was employed to analyze the reflective essays.
Results: The analysis identified 18 codes grouped into six themes: clinical health communication thinking, perception of scientific research, responsibility for health communication, communication of knowledge and skills, hands-on interaction, and knowledge system construction. Participants in the community interviews reported that students communicated clearly and professionally, with some indicating intentions to adjust health behaviors based on the information received.
Conclusion: In this exploratory qualitative study, the integration of health communication into basic medical courses was associated with enhanced students’ appreciation of foundational knowledge and improved self-perceived communication skills. These findings suggest a potential approach to curriculum reform. However, further quantitative research is required to assess broader educational and public health outcomes.
Keywords: health communication, undergraduate medical education, basic medical courses, adaptive expertise, professional identity formation, applied thematic analysis
Introduction
Health communication (HC) is a critical component of modern healthcare systems, playing a key role in disease prevention, health promotion, and chronic disease management.1–3 Effective HC aims to improve public health literacy, defined by the WHO as the ability to access, understand, and use health information to make informed health-related decisions.4 Achieving this objective fundamentally depends on healthcare professionals delivering accurate, accessible, and actionable health information.5,6
However, a significant gap persists between this ideal and current reality. Physicians, often considered the most trusted source of health information, frequently face overwhelming workloads that severely limit their capacity for effective HC.7,8 Recent evidence from China highlights the heavy burden on healthcare professionals. A national study of residents in standardized training found that 43% reported high perceived stress, 43% experienced burnout, and 27% had suicidal ideation.9 Another survey of Chinese clinicians showed that 43% experienced limited communication due to workload, and 37.2% identified insufficient communication skills as a major barrier to effective doctor–patient communication.10 Concurrently, medical education curricula—particularly during the foundational training phase—have largely neglected to build students’ ability to assess health literacy or translate complex science for diverse audiences.11–14 Consequently, despite the growing demand for skilled HC, systematic early training in this core competency remains inadequate.
This educational gap is particularly problematic because medical students often fail to recognize the importance of basic medical knowledge (BMK), including anatomy, physiology, and pathology, prior to clinical exposure.13,14 Despite advances such as problem-based learning (PBL) and case-based learning (CBL), many students continue to undervalue these foundational courses, resulting in low motivation and unclear learning objectives.15 This disconnect becomes particularly evident during clerkships, where students struggle to apply BMK to clinical practice, thereby impeding the development of adaptive expertise.13,14
While some interventions have integrated clinical sciences into clerkships,16 and more recently, biomedical sciences into clinical training,17–20 these curriculum reforms primarily target third-year and higher-year clinical rotation students rather than preclinical beginners. Consequently, there are scarce educational attempts focusing on early real-world biomedical knowledge (BMK) application for junior medical learners. Previous qualitative research has explored medical students’ perceptions of the practical value of preclinical biomedical science knowledge13 and how learners apply foundational science to actual patient management during family medicine clerkships,20 alongside barriers hindering cognitive integration between basic and clinical courses.14 In the field of clinical communication, Veazey et al conducted qualitative research to unpack multiple personal and contextual factors influencing doctor-patient communication. They emphasized that rigid, checklist-oriented communication training fails to meet actual clinical demands, noting that training focused on translating professional jargon into lay expressions is far more necessary.21 Similarly, Joann et al adopted Kolb’s experiential learning theory to explore preclinical students’ communication training within simulation centers, verifying that peer cooperation and iterative feedback can effectively enhance students’ communication proficiency.22 Nevertheless, none of the aforementioned studies incorporates structured, community-oriented health communication tasks into early basic medical teaching, nor do they combine student reflective writings with community member interviews for triangulated data analysis. Therefore, the present study addresses this gap by exploring whether the early integration of health communication activities, anchored in basic medical knowledge, can simultaneously enhance students’ appreciation of foundational science and their communication competencies — an area not previously examined qualitatively.
To address this gap, we designed an educational intervention informed by Kolb’s experiential learning theory23,24 that integrates HC activities, anchored in BMK, into the undergraduate medical curriculum. This study examines whether such integration can: (a) facilitate early student recognition of the value of BMK, rather than delaying this awareness until clinical clerkships; (b) simultaneously develop core HC competencies through structured training; and (c) provide the public with reliable health information disseminated by trained medical students. This study introduces a novel approach to bridging foundational science education with public health practice, offering valuable insights into curriculum design that can enhance both student learning and community health outcomes.
Materials and Methods
Study Design and Theoretical Framework
This exploratory qualitative study evaluated the learning outcomes of preclinical medical students following a basic medicine-oriented health communication (HC) intervention. The intervention design and subsequent data analysis were guided by Kolb’s experiential learning theory,23,24 which delineates learning into four cyclical phases: concrete experience, reflective observation, abstract conceptualization, and active experimentation. Two qualitative analytical approaches were employed: applied thematic analysis for student reflective essays and conventional content analysis for semi-structured interview transcripts from community participants.25,26
Participants
Medical Student Participants
Participants were recruited via voluntary response sampling between March and October 2024 at a Chinese medical university. Recruitment notices were posted on the university’s online learning platform and class WeChat groups. Eligibility criteria included full-time preclinical undergraduates (Years 1–3) without prior systematic health communication training who were willing to complete standardized reflective essays. No monetary incentives were provided. Ultimately, 42 eligible students (36 females, 6 males) across multiple majors were enrolled; detailed demographic information is listed in Appendix 1. Based on informational power theory and existing empirical evidence from qualitative studies focusing on medical students’ reflective narratives, the preliminary recruitment target was set at 35–45 participants. Thematic saturation was empirically verified after data collection and coding: no new codes emerged after analyzing the 35th essay, and analysis of the remaining seven essays further confirmed saturation, thereby justifying the final sample size. The distribution of participants by major was shown in Table 1.
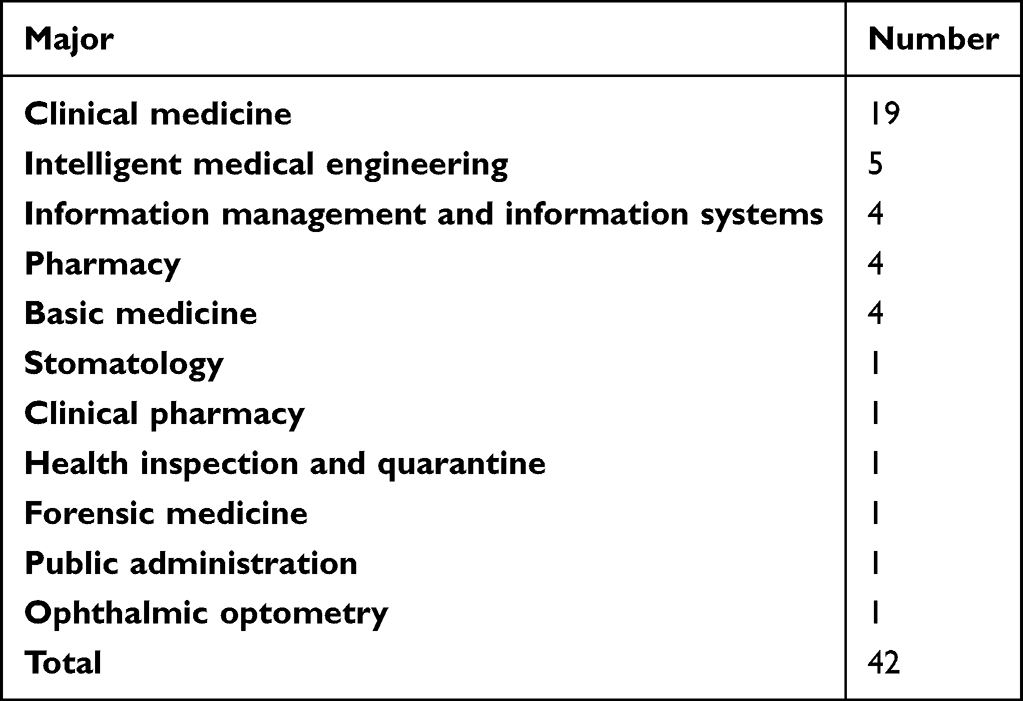 |
Table 1 Majors and Number of Participants in Health Communication Activities |
Community Interviewees
Purposive sampling was used to recruit community attendees who interacted with at least two participating students during the HC activity. A total of 15 community members (8 females, 7 males), aged 9–67 years, were interviewed. The sample covered diverse educational backgrounds, ranging from primary school to postgraduate level.
Intervention: Structured Health Communication Activity
The HC intervention was implemented during China’s National Science and Technology Activity Week in May 2024, adhering strictly to Kolb’s four-stage experiential learning framework:
- Concrete experience: Students delivered science popularization talks on specific medical topics (eg, cardiac anatomy, hepatic pathology, and the Heimlich maneuver) to onsite citizens, supported by anatomical models, microscopes, and illustrative charts;
- Reflective observation: Following onsite practice, students summarized communication barriers, reviewed relevant basic medical knowledge, viewed standardized HC demonstration videos, and discussed improvement strategies within peer groups;
- Abstract conceptualization: Based on reflection and group discussion, students formulated personalized, optimized frameworks for translating professional medical knowledge into lay-friendly explanations;
- Active experimentation: Revised communication schemes were applied in subsequent onsite science popularization activities, and participants recorded explanatory videos for follow-up assessment (see Appendix 2).
Data Collection
Data were collected from two independent sources to facilitate triangulation.
Reflective Essays
All 42 participants submitted anonymous reflective essays via an online form after the intervention to reduce response bias. Essay prompts were aligned with Kolb’s experiential learning cycle, guiding students to describe practical experiences, link communication practices to basic medical knowledge, and reflect on career implications; the detailed essay outline is presented in Appendix 3.
Semi-Structured Community Interviews
All interviews were conducted in a quiet onsite room following HC activities, with each session lasting 3–5 minutes. After obtaining oral informed consent, interviews were audio-recorded and transcribed verbatim in the original Chinese by a research assistant. The semi-structured interview protocol, which focused on information clarity, credibility, and behavioral intention, is documented in Appendix 4. All transcripts were anonymized by removing identifiable personal information prior to formal analysis.
Qualitative Data Analysis
Applied Thematic Analysis of Student Reflective Writings
Data coding and theme extraction followed the six-phase thematic analysis protocol proposed by Braun and Clarke:
- Familiarization: Three independent coders (Y.Z., H.S., Z.Z.) repeatedly read all anonymized essays to achieve comprehensive data familiarity;
- Generating initial codes: Three researchers independently coded all essays using NVivo 12 to extract initial codes;
- Searching for themes: Extracted codes were aggregated and discussed by the team to preliminarily classify potential overarching themes;
- Reviewing themes: Preliminary themes were cross-checked against all coded extracts and full-text essays to ensure internal consistency;
- Defining and naming themes: The core connotation of each finalized theme was defined, and standardized names were assigned;
- Producing the analytical report: Representative original excerpts were selected to illustrate each theme in the results section.
Prior to formal coding, all three coders underwent a 4-hour standardized training session using five practice essays to standardize coding procedures. Weekly consensus meetings were held to resolve coding discrepancies; unresolved disagreements were arbitrated by the senior author (L.L)., and all codes and themes were finalized after three rounds of group discussions. The 18 discrete codes were synthesized into six core themes, with full code frequency statistics archived in Appendix 5.
Conventional Content Analysis of Community Interview Transcripts
Two researchers (J.Z., C.L.) independently coded all interview transcripts, extracted meaning units related to information comprehensibility, information credibility, and health behavioral willingness, and categorized the coded content through repeated group discussions to resolve divergent coding results. No new analytical categories emerged after the 12th interview, confirming data saturation for the community interview samples. Selected original quotations were translated into English for presentation in the manuscript.
Trustworthiness and Reflexivity
Multiple strategies were employed to ensure research trustworthiness:
Credibility: Data triangulation was achieved using dual data sources, including student essays and community interviews. Preliminary analytical findings were submitted to two external medical education researchers for peer debriefing and examination of alternative interpretations. Additionally, five randomly selected participating students completed member checking to verify the accuracy of the thematic interpretations.
Dependability: Complete audit trails, including original raw data, the formal codebook, team meeting records, and analytical decision logs, were maintained throughout the research process.
Confirmability: All research team members maintained continuous reflexive journals to record personal presuppositions regarding health communication education. Regular team discussions were organized to monitor how the researchers’ occupational backgrounds as basic medical educators might influence data coding and theme formation, thereby minimizing subjective analytical bias.
Ethical Considerations
The study complied with the ethical requirements of the Declaration of Helsinki. An exemption from full ethical approval was granted by the Institutional Review Board of the Shanxi Medical University. Written informed consent was obtained from all participating medical students and community members prior to data collection.
Results
Thematic Analysis Results of Coded Student Reflections
Following the health communication intervention, all 42 participants submitted reflective essays to explore connections between basic medical knowledge and practical health communication. Thematic analysis yielded 18 individual codes clustered into six overarching themes (Tables 2 and 3), with full code frequency data archived in Appendix 5. The six themes include clinical health communication thinking, perception of scientific research, responsibility for health communication, communication of knowledge and skills, hands-on interaction, and knowledge system construction.
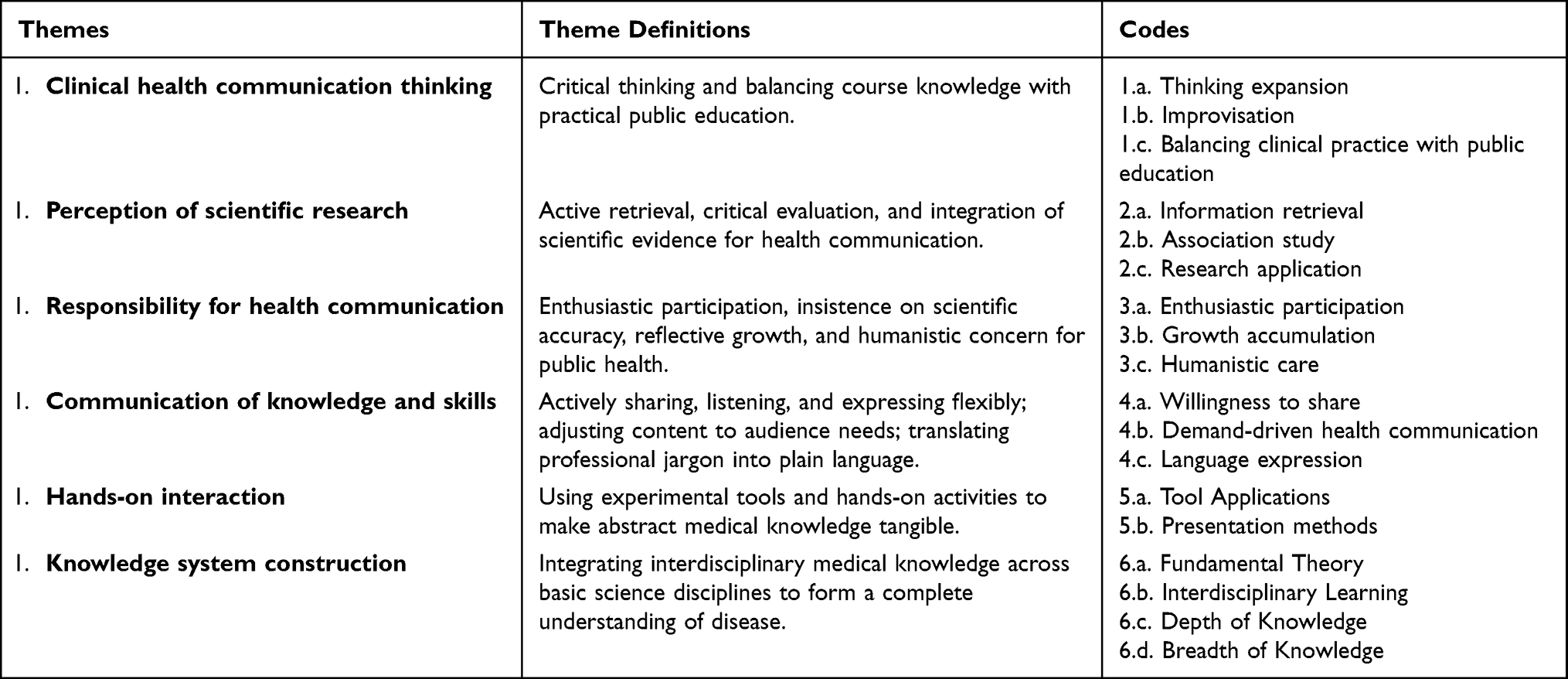 |
Table 2 Themes, Theme Definitions, and Codes of Participants’ Essays |
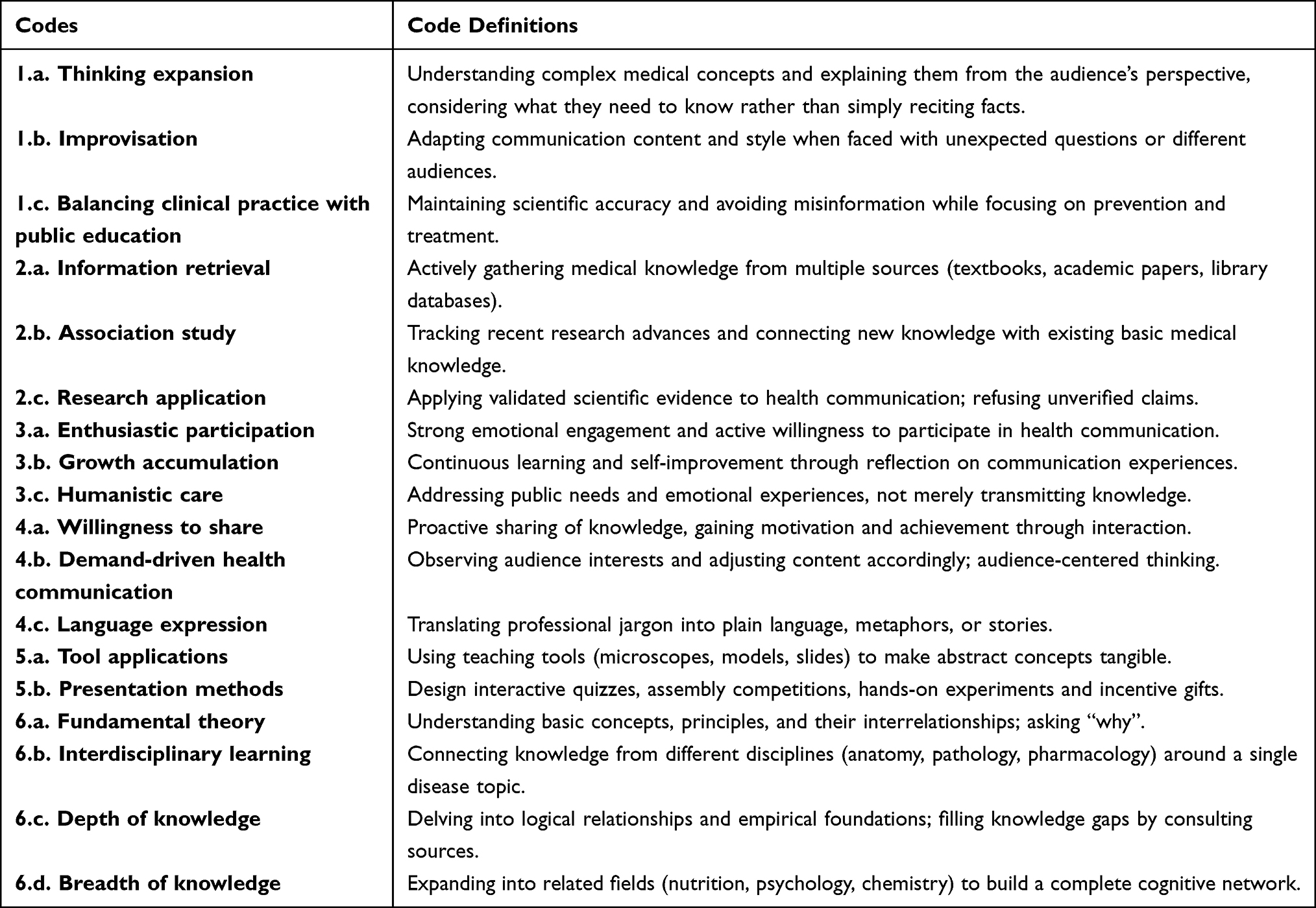 |
Table 3 Codes and Code Definitions |
Theme 1: Clinical Health Communication Thinking
This theme captured students’ ability to think critically and balance biomedical knowledge with the practical demands of public education. Rather than simply reciting textbook facts, students learned to restructure their understanding, adapt to unexpected situations, and ensure that the information delivered was both accurate and accessible to lay audiences.
Code 1.a. Thinking expansion — Students broadened their perspectives by connecting complex medical concepts to real-world communication, considering public informational needs and how to explain variations across different populations.
One student wrote:
As a medical student and a science communicator, the knowledge we receive must be accurate and logically coherent. But the next step is ‘output’: after mastering a rich body of knowledge, how do we tell visitors what they want to know in an appropriate and understandable way? What must be told, and what can be omitted? This requires us not to see problems from our own perspective, but to think more from the visitor’s or patient’s point of view – this is difficult, but also crucial. (Participant 1)
Code 1.b. Improvisation— Students developed the ability to adjust their communication content and style in real time when faced with unexpected questions or diverse audiences.
Another student reflected:
People did not always ask questions according to our prepared script, which meant we had to expand our knowledge base. We summarized their questions, looked for answers, and if we really could not answer, we asked the teachers for help. (Participant 18)
Code 1.c. Balancing clinical practice with public education — Students recognized the need to maintain scientific accuracy and avoid misinformation while focusing on what the public truly needed to know about prevention and treatment.
A student explained:
We analyzed the audience and used plain language to describe medical knowledge. For different groups we explained the knowledge they were interested in. The key was to clearly communicate how to prevent and treat the disease – the things the public really cared about. (Participant 23)
Another student emphasized:
The information we provide must be correct. I would not guess or spread unverified claims. (Participant 5)
Theme 2: Perception of Scientific Research
This theme captured students’ recognition that effective health communication requires active retrieval, critical evaluation, and integration of scientific evidence from both classic textbooks and cutting-edge research. Students learned to consult academic literature, use library resources, track recent advances, and translate this evidence into language that the public can understand. This theme reflected a shift from passively accepting knowledge to actively verifying and applying it.
Code 2.a. Information retrieval — Students proactively gathered medical knowledge from multiple sources (textbooks, academic papers, health communication platforms, library databases) rather than relying on a single source or fragmented memory.
One student wrote:
I first carefully read posts on domestic social media and lifestyle platforms, which covered the basic introduction, causes, and correction methods of hyperopia. In addition, I fully used the university library resources, searched the official website, and integrated the relevant health communication knowledge. (Participant 2)
Code 2.b. Association study — Students actively tracked and read recent research advances, understood cutting‑edge scientific findings, and connected this new knowledge with their existing basic medical knowledge so that they could provide the most up‑to‑date and accurate information in their health communication.
Another student reflected:
By consulting authoritative sources and the latest research findings, we deeply investigated the pathological mechanisms underlying the early symptoms of fatty liver disease. (Participant 27)
Code 2.c. Research application — Students applied validated scientific evidence to their communication practice, ensuring that the information they delivered was well–supported and reliable. They refused to use unverified claims and insisted on grounding their explanations in scientific evidence.
A student emphasized:
Health communication must be based on rigorous scientific theory … such knowledge must be found in relevant literature, not simply obtained from general online search engines. (Participant 7)
Theme 3: Responsibility for Health Communication
This theme captured students’ awareness that, as medical students and future doctors, they have a responsibility to deliver accurate and scientific health information to the public. This sense of responsibility is reflected not only in their enthusiastic participation but also in their insistence on scientific accuracy, their reflective growth, and their humanistic concern for public health. They no longer regard health communication as a routine task, but embrace it as a mission—taking responsibility for both the information they convey and the well-being of their audience.
Code 3.a. Enthusiastic participation — Students showed strong emotional engagement and active willingness to participate in health communication. They volunteered, prepared diligently, explained passionately, and experienced a sense of achievement and value through interaction. This enthusiasm stemmed from their love of medicine and recognition of social responsibility.
One student wrote:
I am very happy and honoured to share the first aid methods and bleeding control techniques with everyone. I hope you will never need to use this knowledge, but I also worry that if you do need it, you might not know how to apply it. (Participant 28)
Code 3.b. Growth accumulation — Students continuously learned and accumulated knowledge during the health communication process, and they grew by reflecting on their own limitations. They realized that health communication is not only outward delivery but also inward improvement – each explanation and each answer to a question deepened and systematised their understanding of medical knowledge.
Another student reflected:
This health communication activity opened a new world for me and made me deeply realise the responsibility of medical students in health communication. (Participant 15)
Code 3.c. Humanistic care — Students prioritized the real needs and emotional experiences of the public, rather than merely transmitting knowledge. They listened to the audience’s experiences, understood patients’ suffering, and offered empathetic responses. Such care reflected the humanistic dimension of medicine; health communication is not cold lecturing but a process of understanding and support between individuals.
A student described:
A gentleman in his sixties … said, ‘I have already had a stent placed.’ … At the end of our explanation, we became students listening to his story. His calm expression deeply impressed me. (Participant 18)
Theme 4: Communication of Knowledge and Skills
This theme reflected students’ recognition that health communication involves more than simply “telling what they know”. Rather, it requires active sharing, careful listening, and flexible expression. Students progressed from initial hesitation and stiffness to a willingness to speak and interact. They learned to adjust their content according to the audience’s needs rather than simply lecturing. Most importantly, they developed the ability to translate professional jargon into plain language. This theme captured students’ growth in two dimensions: “how to say” and “what to say”.
Code 4.a. Willingness to share — Students transformed from being hesitant and lacking confidence to proactively sharing knowledge. They recognized that health communication provides a unique opportunity to share what they have learned, and through this sharing, they gained a sense of achievement and motivation. This willingness is a prerequisite for effective communication.
One student wrote:
I decided to join this health communication activity for medical students … I felt that this was a novel and completely new experience, one that I would never have again if I missed it. (Participant 1)
Code 4.b. Demand-driven health communication — Students no longer focused solely on their prepared material. Instead, they first observed and understood the audience’s interests, age characteristics, and knowledge background, then adjusted their content accordingly. They realized that the purpose of health communication is to be understood and useful to the audience, not merely to complete a presentation task. This audience-centered approach is key to effective communication.
Another student explained:
Children were more interested in assembling models, adolescents were mainly interested in the causes and prevention of diseases, while parents were more interested in treatment. Therefore, we needed to prepare diverse content. (Participant 4)
Code 4.c. Language expression — Students learned to transform obscure medical terminology into spoken language, metaphors, or stories that the public could understand. They recognized that professional jargon is a barrier to communication, whereas plain language serves as a bridge. This ability requires not only knowledge but also repeated practice and perspective-taking.
A student reflected:
Translating complex medical knowledge into simple and understandable language … through continuous communication and discussion, I not only enriched my knowledge base but also learned many practical skills for health communication. (Participant 2)
Theme 5: Hands-on Interaction
This theme reflected students’ recognition that verbal explanation alone often fails to capture the audience’s attention, especially among children and non-professionals. By allowing the audience to manipulate models, participate in experiments, or assemble teaching aids, students found that hands-on activities greatly stimulated interest and deepened understanding. This “learning by doing” approach not only made health communication more vivid and engaging but also rendered abstract basic medical knowledge intuitive and tangible. Through this process, students learned how to design and use tools and how to organize interactive sessions, thereby enhancing audience participation and the overall effectiveness of their communication.
Code 5.a. Tool applications — Students learned to use various teaching tools such as microscopes, anatomical models, pathology slides, and laboratory equipment. With visual and tactile aids, they helped the audience understand abstract medical concepts. The use of tools transformed health communication from “hearing about it” to “seeing and touching”, significantly lowering the barrier to understanding.
One student wrote:
We held the heart model … and let children open the heart model to see its internal structure. (Participant 23)
Code 5.b. Presentation methods — Students designed a variety of presentation formats, including interactive quizzes, assembly competitions, hands-on experiments, and small gifts as incentives. They recognized that health communication is not one-way lecturing but two-way interaction. Effective presentation methods can motivate the audience and make knowledge more memorable.
Another student explained:
We designed an interactive quiz game where participants could win small gifts by answering questions. This approach greatly stimulated everyone’s enthusiasm to participate. … We also invited participants to assemble models. (Participant 4)
Theme 6: Knowledge System Construction
This theme captured students’ recognition that the various basic medical disciplines (anatomy, pathology, pharmacology, etc.) are not isolated but form an integrated whole. Through health communication, students were prompted to connect knowledge from different courses around a single disease or topic, building a complete chain from structure and function to pathological mechanisms and treatment principles. This interdisciplinary integration not only deepened their understanding but also helped them develop a systematic framework for clinical thinking. Students realized that only by weaving fragmented knowledge into a network can one truly achieve mastery and flexible application.
Code 6.a. Fundamental theory — Students valued the understanding of basic concepts, principles, and their interrelationships. They moved beyond rote memorization to ask “why” – exploring the mechanisms of disease, the principles of drug action, and the logical relationships of human structure. A solid grasp of fundamental theory is the cornerstone of constructing a knowledge system.
One student wrote:
Myocardial infarction is caused by acute blockage of the coronary artery leading to insufficient blood supply to the corresponding myocardial area. It results from coronary atherosclerosis, arrhythmia, respiratory failure, and other causes – insufficient blood supply, myocardial hypoxia, and excessive oxygen consumption. (Participant 23)
Code 6.b. Interdisciplinary learning — Students actively connected knowledge from different disciplines, for example, integrating anatomical structure, pathological mechanisms, and pharmacological treatment principles around the same disease topic. They recognized that clinical problems are rarely solvable by a single discipline; interdisciplinary integration is an essential mode of thinking for physicians.
Another student explained:
Health communication can link together the various pieces of knowledge about the same disease found in different basic medicine subjects, forming a complete large system – from the structure of the heart (anatomy), the branch blood supply areas of the coronary arteries, sympathetic nerve activity, the triggers (the formation of atherosclerosis and thrombosis in pathology), to the use of medications (pharmacology). (Participant 23)
Code 6.c. Depth of knowledge — Students were not satisfied with surface-level information but delved into the logical relationships and empirical foundations behind the facts. They asked “why this happens” and filled their knowledge gaps by consulting sources or asking teachers, ensuring that their explanations were accurate and thorough.
A student reflected:
We summarized their questions, looked for answers, and if we really could not answer, we asked the teachers for help. (Participant 18)
Code 6.d. Breadth of knowledge — Students recognized that medical knowledge should not be limited to textbooks and classrooms; they actively expanded into related fields such as nutrition, psychology, chemistry, and physics. A broad knowledge base helped them build a more complete cognitive network and enabled them to respond to a wider variety of questions during health communication.
A student stated:
I also paid attention to other areas closely related to eye health, such as nutrition and psychology. I learned that proper diet and mental health also play crucial roles in eye health. (Participant 2)
Semi-Structured Interviews with General Community Members
During and after the health communication event, brief semi-structured interviews and informal conversations were conducted with several community members. The following representative quotations were recorded verbatim by student interviewers.
A male participant with a cardiac stent stated:
I already had a stent. I had experienced everything you explained. The squeezing chest pain and shortness of breath were truly unbearable. Hearing you explain the mechanism of myocardial infarction helped me better understand what happened to me. (CM02)
A middle-aged woman with fatty liver disease remarked:
I have fatty liver disease. I had heard about fatty liver, cirrhosis, and liver cancer, but I never truly understood them. Seeing the cellular changes through the microscope was shocking. I would definitely adjust my diet to prevent my fatty liver from progressing. (CM03)
A woman who learned the Heimlich maneuver commented:
I had only heard about the Heimlich maneuver before. Today, I finally learned it systematically. If my child chokes in the future, I will know what to do. (CM05)
A young man stated:
I do not know anatomy, but I could actually feel the arteries you pointed to. Thus, emergency bleeding control has precise locations. (CM06)
Most community interviewees noted that the information delivered by students was easier to understand and more trustworthy than informal online health content. Several participants also indicated tentative plans to adjust their personal health-related behaviours accordingly.
Discussion
Thematic analysis of the reflective essays revealed that participants developed a deeper appreciation for basic science subjects and improved their health communication skills through this educational intervention. These findings aligned with Kolb’s experiential learning theory,23,24 demonstrating that engagement in concrete health communication (HC) experiences, followed by reflective observation and active experimentation, enabled students to recognize the clinical relevance of their basic medical knowledge (BMK) while developing essential communication competencies.
Notably, students shifted from a disease-centered perspective to a more holistic understanding of health, recognizing the practical applicability of their foundational knowledge. This transformation is reflected in the development of clinical health communication thinking (Theme 1) and responsibility for health communication (Theme 3), which directly enhanced students’ adaptability as future healthcare providers. These competencies enabled students to bridge the gap between theoretical knowledge and real-world application, addressing the well-documented challenge medical students face in connecting basic science to clinical practice.13,14
This approach effectively alleviated student confusion by transforming basic science education from abstract theoretical content into actionable knowledge for health promotion. The improvements in knowledge communication and skill application (Theme 4), as well as hands-on interaction (Theme 5), indicate the development of practical HC competencies that are often overlooked in traditional curricula.11,12 Through autonomous information retrieval (Code 2a), association studies (Code 2b), and the design of explanatory tools (Code 5a), students cultivated a stronger sense of competence and relevance, thereby reshaping their perception of BMK.
Our findings particularly highlight how HC activities based on BMK cultivated intrinsic motivation among students — a crucial factor in medical education.27,28 This shift in motivation is particularly valuable during the early stages of medical education when students often encounter confusion and a decline in motivation.29
Furthermore, this approach appeared to support aspects of cognitive integration and professional identity formation, which are essential outcomes in medical education.11,26 The processes of scientific research perception (Theme 2) and knowledge system construction (Theme 6) enabled students to progress from simply acquiring facts to applying knowledge in real-world contexts.30,31 The social learning environment created through HC activities further supported professional identity formation, as students began to “think, act, and feel like physicians” through their interactions with the public.32
An equally significant finding highlights the enhancement of health literacy among medical undergraduates. Although the importance of health literacy training for healthcare providers is widely acknowledged,11,12 its systematic integration into basic medical education remains a novel approach. Our intervention enabled students to recognize the depth and breadth of BMK (Codes 6c, 6d) and its crucial role in fostering personal health literacy. The observed changes in communication methods—from hesitancy to willingness to engage (Code 4a), from monologue to audience-responsive HC (Code 4b), and adaptation to public language styles (Code 4c)—demonstrate the development of practical health literacy communication skills.
This educational model provides a promising strategy for curriculum reform in life sciences education. Community feedback indicated that student-delivered HC was perceived as more professional and trustworthy than online health information, particularly in explaining pathological mechanisms rather than providing superficial recommendations. Community members also reported intentions to adjust health behaviors, such as improving diet or learning first-aid techniques.
Implications for Educational Practice
This study offers a practical framework for curriculum reform that enhances both educational and public health outcomes. Integrating HC activities based on BMK provides an effective model for increasing the relevance of basic medical sciences while simultaneously developing communication competencies. Educators should incorporate such experiential learning opportunities early in medical training to help students appreciate the value of foundational knowledge and cultivate adaptive expertise prior to clinical clerkships. Furthermore, the communication skills honed through these public-facing activities—such as simplifying complex terminology, adapting to diverse audiences, and building trust—are likely to transfer to clinical practice, thereby enabling students to explain diagnoses and treatment plans more effectively.
Implications for Low-Resource Settings
The intervention utilized only basic, low-cost resources, including anatomical models, microscopes, posters, and common laboratory materials. Neither expensive simulation equipment nor standardized patients were required, rendering the model highly transferable to resource-limited medical schools. Educators can adopt similar strategies by using existing teaching models and recycled materials for hands-on activities; organizing peer role-play sessions instead of hiring simulated patients; leveraging free online videos and infographics for preparatory learning; and partnering with local community spaces (eg, schools, community centers) to host pop-up health communication booths. These low-cost approaches enabled institutions with limited budgets to implement early health communication training without compromising educational quality.
Limitations
This study has several limitations. First, data were collected from a single university, which restricted the external generalizability of the results. Second, all evidence was derived from self-reported student reflections and community interviews; despite anonymous submission and voluntary recruitment, these sources were susceptible to social desirability bias. Third, the absence of long-term follow-up precludes confirmation of whether the observed improvements persist over time. Fourth, community participants were recruited from a one-off health communication activity with a limited sample size (n = 15), potentially limiting the representativeness of public feedback. To mitigate researcher bias during analysis, the research team maintained reflexive logs and held regular group discussions to monitor the influence of professional backgrounds and preset viewpoints on result interpretation. Future research should employ multi-center designs combined with quantitative tools and mixed-method evaluations to strengthen the robustness of the evidence.
Conclusion
In this exploratory qualitative study, integrating health communication activities into basic medical courses was associated with students’ increased appreciation of foundational knowledge and self-perceived communication skills. This approach appears to address the challenge of students undervaluing basic science courses prior to clinical exposure. Furthermore, it may contribute to public health literacy by helping students translate complex medical concepts into language understandable to lay audiences. This educational model represents a potential strategy for curriculum reform in life sciences education, providing a meaningful bridge between basic science instruction and real-world health application. Further quantitative research is needed to assess broader educational and public health outcomes.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
The study was performed in accordance with the Declaration of Helsinki. The Institutional Review Board of Shanxi Medical University confirmed that no ethical approval is required.
Acknowledgments
The health communication activities for medical students were greatly facilitated by the strong support from the Shanxi Provincial Science and Technology Department.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by 2024 Shanxi Higher Education Reform and Innovation Project (Grant/Award Number: J20240533) and 2023 Shanxi Province Health Communication Special Project (Grant/Award Number: 3F082023122).
Disclosure
The author(s) reported no conflicts of interest in this work.
References
1. Schillinger D, Baron RJ. Health communication science in the balance. JAMA. 2023;330(9):803. doi:10.1001/jama.2023.14763
2. Suka M. Public health communication studies in Japan. Nihon Eiseigaku Zasshi. 2021;76. doi:10.1265/jjh.21006
3. Qiu J. Science communication in China: a critical component of the global science powerhouse. Natl Sci Rev. 2020;7(4):824–14. doi:10.1093/nsr/nwaa035
4. World Health Organization. Health promotion glossary of terms 2021. World Health Organization. 2021. Available from: https://www.who.int/publications/i/item/9789240038349.
5. Mor-Anavy S, Lev-Ari S, Levin-Zamir D. Health literacy, primary care health care providers, and communication. Health Lit Res Pract. 2021;5(3):e194–e200. doi:10.3928/24748307-20210529-01
6. Gonçalves-Bradley DC, J Maria AR, Ricci-Cabello I, et al. Mobile technologies to support healthcare provider to healthcare provider communication and management of care. Cochrane Database Syst Rev. 2020;8(8):CD012927. doi:10.1002/14651858.CD012927.pub2
7. Kang G. Two months, eight Chinese physicians suffered sudden death. Am J Med. 2021;134(6):e398–e399. doi:10.1016/j.amjmed.2019.08.018
8. Song XN, Shen J, Ling W, et al. Sudden deaths among Chinese physicians. Chin Med J. 2015;128(23):3251–3253. doi:10.4103/0366-6999.170263
9. Li Z, Wu M, Zhang X, et al. Interrelationships of stress, burnout, anxiety, depression, quality of life and suicidality among Chinese residents unDer standardized residency training: a network analysis. Ann Med. 2024;56(1):2433030. doi:10.1080/07853890.2024.2433030
10. Liang Y, Zhang H, Li S, Ma Q. Shared decision-making on life-sustaining treatment: a survey of current barriers in practice among clinicians across China. Healthcare. 2025;13(5):547. doi:10.3390/healthcare13050547
11. Sullivan GM. The growing health literacy gap and graduate medical education. J Grad Med Educ. 2017;9(3):275–277. doi:10.4300/JGME-D-17-00216.1
12. Ye R, Wu Y, Sun C, et al. Health communication patterns and adherence to a micronutrient home fortification program in rural China. J Nutr Educ Behav. 2022;54(1):36–45. doi:10.1016/j.jneb.2021.07.014
13. Dickinson BL, Gibson K, VanDerKolk K, et al. “It is this very knowledge that makes us doctors”: an applied thematic analysis of how medical students perceive the relevance of biomedical science knowledge to clinical medicine. BMC Med Educ. 2020;20(1):356. doi:10.1186/s12909-020-02251-w
14. Kercheval JB, Mott NM, Kim EK, et al. Students’ perspectives on basic and clinical science integration when step 1 is administered after the core clerkships. Teach Learn Med. 2023;35(2):117–127. doi:10.1080/10401334.2022.2030235
15. Zhao W, He L, Deng W, Zhu J, Su A, Zhang Y. The effectiveness of the combined problem-based learning (PBL) and case-based learning (CBL) teaching method in the clinical practical teaching of thyroid disease. BMC Med Educ. 2020;20(1):381. doi:10.1186/s12909-020-02306-y
16. Fanwei QU, Jin HE, Hua MA, et al. A comparative analysis of medical education models and curriculums of a medical university and a medical education center. JNMA J Nepal Med Assoc. 2019;57(215):45–49. doi:10.31729/jnma.4107
17. Dahlman KB, Weinger MB, Lomis KD, et al. Integrating foundational sciences in a clinical context in the post-clerkship curriculum. Med Sci Educ. 2018;28(1):145–154. doi:10.1007/s40670-017-0522-1
18. Daniel M, Morrison G, Hauer KE, et al. Strategies from 11 US medical schools for integrating basic science into core clerkships. Acad Med. 2021;96(8):1125–1130. doi:10.1097/ACM.0000000000003908
19. Emanuel EJ. Reforming American medical education. Milbank Q. 2017;95(4):692–697. doi:10.1111/1468-0009.12291
20. Porter-Stransky KA, Gibson K, VanDerKolk K, et al. How medical students apply their biomedical science knowledge to patient care in the family medicine clerkship. Med Sci Educ. 2023;33(1):63–72. doi:10.1007/s40670-022-01697-5
21. Veazey K, Notebaert A, Robertson EM. Medical student perceptions of establishing effective clinical communication: a qualitative study. Adv in Health Sci Educ. 2026;31(2):653–681. doi:10.1007/s10459-025-10468-x
22. Sam CP, Nathan JL, Aroksamy JA, Ramasamy N, Mamat NHB, Nadarajah VD. A qualitative study on the experiences of preclinical students in learning clinical and communication skills at a simulation centre. Med Sci Educ. 2023;33(5):1127–1137. doi:10.1007/s40670-023-01851-7
23. Yardley S, Teunissen PW, Dornan T. Experiential learning: AMEE Guide No. 63. Med Teach. 2012;34(2):e102–115. doi:10.3109/0142159X.2012.650741
24. Kolb DA. Experiential Learning: Experience as the Source of Learning and Development. Prentice Hall; 1984.
25. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
26. Guest G, MacQueen K, Namey E. Applied Thematic Analysis. SAGE Publications, Inc.; 2012. doi:10.4135/9781483384436
27. Kusurkar RA, Ten Cate TJ, van Asperen M, Croiset G. Motivation as an independent and a dependent variable in medical education: a review of the literature. Med Teach. 2011;33(5):e242–262. doi:10.3109/0142159X.2011.558539
28. Tokumasu K, Obika M, Obara H, Kikukawa M, Nishimura Y, Otsuka F. Processes of increasing medical residents’ intrinsic motivation: a qualitative study. Int J Med Educ. 2022;13:115–123. doi:10.5116/ijme.6250.1017
29. Karim MY. Using clinical cases to restore basic science immunology knowledge in physicians and senior medical students. Front Immunol. 2020;11:1756. doi:10.3389/fimmu.2020.01756
30. Pusic MV, Hall E, Billings H, et al. Educating for adaptive expertise: case examples along the medical education continuum. Adv Health Sci Educ Theory Pract. 2022;27(5):1383–1400. doi:10.1007/s10459-022-10165-z
31. Steenhof N. Adaptive expertise in continuing pharmacy professional development. Pharmacy. 2020;8(1):21. doi:10.3390/pharmacy8010021
32. Cruess RL, Cruess SR, Boudreau JD, Snell L, Steinert Y. Reframing medical education to support professional identity formation. Acad Med. 2014;89(11):1446–1451. doi:10.1097/ACM.0000000000000427
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.