Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Integrating Artificial Intelligence into Clinical Care: A Cross-Sectional Study to Advance Healthcare in Saudi Arabia
Received 25 January 2026
Accepted for publication 15 April 2026
Published 25 April 2026 Volume 2026:19 598736
DOI https://doi.org/10.2147/JMDH.S598736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Linda Yoder
Maryam Allayl,1,2 Ghareeb Bahari3
1Jazan Health Cluster, Ministry of Health, Jazan, Saudi Arabia; 2Community, Psychiatric and Mental Health Nursing Department, College of Nursing, Riyadh, Saudi Arabia; 3Nursing Administration and Education Department, College of Nursing, King Saud University, Riyadh, Saudi Arabia
Correspondence: Ghareeb Bahari, Nursing Administration and Education Department, College of Nursing, King Saud University, Riyadh, Saudi Arabia, Tel +966118054381, Email [email protected]
Purpose: Mounting evidence suggests that artificial intelligence can support the self-management of chronic diseases, including skin conditions, insulin management, and blood pressure control. This study aimed to investigate the potential use of artificial intelligence (AI) in chronic condition management among patients in Saudi Arabia, where the prevalence of such diseases is increasing. Specifically, we assessed AI perception, self-efficacy, and cognitive symptom management; examined their associations with demographic variables, and evaluated the influence of AI perception and self-efficacy on cognitive symptom management.
Patients and Methods: This study employed a cross-sectional, descriptive-correlational design. Data were collected at a single time point to characterize the sample and explore relationships among variables. A convenience sample of 163 patients with chronic conditions was recruited. A structured questionnaire was used to assess AI perception, self-efficacy, cognitive symptom management, and demographic characteristics. Data were collected between December 2024 and March 2025 and were analyzed using descriptive statistics, Pearson’s correlation coefficient, one-way analysis of variance, and multiple regression analysis, as appropriate.
Results: The findings revealed that sex significantly influenced AI awareness, indicating a need for targeted outreach, particularly for women who demonstrated lower levels of AI awareness. Additionally, self-efficacy was a significant predictor of better cognitive symptom management (p < 0.01), as participants with higher self-efficacy reported significantly better management of cognitive symptoms and greater engagement in health-promoting behaviors compared to those with lower self-efficacy.
Conclusion: Our results highlight that self-efficacy is a key factor in managing cognitive symptoms associated with chronic conditions and underscore the importance of targeted interventions to enhance inclusivity and strengthen individuals’ confidence in managing their health. These findings can also inform the development of healthcare programs aimed at empowering patient self-management through AI-based tools.
Keywords: artificial intelligence, chronic conditions, self-efficacy, cognitive symptom management, healthcare technology
Introduction
The global incidence of chronic diseases continues to increase, affecting approximately 25% of the adults worldwide and posing significant challenges for individuals, families, and healthcare systems. Such conditions are associated with high morbidity and mortality rates and account for a substantial proportion of the global healthcare burden. As these conditions typically last over a year, require ongoing medical care, and potentially affect quality of life, patients with chronic diseases may face serious consequences, such as disease progression, functional impairment, reduced quality of life, hospitalization, and death if their conditions are not effectively managed.1 Thus, management of chronic conditions has become a priority, especially with an aging population.2
Common examples of chronic diseases including diabetes, hypertension, dyslexia, Alzheimer’s disease, and cancer are widely prevalent, affecting a substantial portion of the global population. Some of these diseases have been more extensively researched in terms of technological management solutions. However chronic diseases can be analyzed from various perspectives, and each viewpoint highlights specific features of a health condition and potential methods for its control, treatment, and management. Among the various perspectives, using artificial intelligence (AI) technologies in healthcare could help manage the condition and enhance the patients’ quality of life.3 Over the years, AI has evolved from early systems based on fixed medical rules to modern frameworks that use artificial neural networks and statistical methods for diagnosis and treatment planning.4 Notably, recent advancements in AI and digital healthcare technology have enhanced the self-management of serious chronic diseases, including skin conditions, insulin management, and blood pressure control.5 Thus, predictive modeling and AI offer significant opportunities to enhance care across various clinical areas, including diagnosis, risk assessment, lifestyle management, and home monitoring, which could lead to substantial improvements in the care of patients with prevalent chronic diseases with high rates of morbidity and mortality.6 For instance, AI-driven public healthcare systems can improve problem-solving capabilities and enhance the decision-making process.7
Currently, the healthcare system in Saudi Arabia is facing multiple challenges, including an aging population, increasing incidence of chronic diseases, and nurse shortage. Moreover, rising healthcare costs and the growing demand for long-term care services further strain the system. Therefore, the government is actively expanding healthcare infrastructure, encouraging the effective use of technology, enhancing the quality of healthcare services, and focusing on preventive care to address these challenges and make the healthcare system more efficient and effective. In this regard, the use of AI systems can be vital in transforming the healthcare system in Saudi Arabia by increasing efficiency, lowering costs, and improving the quality of care. Additionally, the Vision 2030 plan for Saudi Arabia features a detailed strategy to overhaul the healthcare system, aiming to develop a system that is more focused on patients, fosters innovation, and is accessible to all citizens.8 As Saudi Arabia aims to deliver high-quality healthcare services to its citizens, the use of the Internet and big data technologies can be invaluable in this regard in reducing various risks by enabling early predictions of chronic diseases on a large scale.9
Recently, a new method for developing predictive models for treatment outcomes of chronic diseases was introduced and shown to be more effective than traditional machine learning approaches. Additionally, the predictive models developed using the new method were successfully integrated with electronic health records using a SMART on FHIR clinical decision support system for Type 2 diabetes mellitus.10 Thus, Saudi Arabia can greatly enhance the management of chronic conditions by utilizing these technologies, resulting in improved health outcomes for its population. However, successfully implementing AI solutions in managing chronic diseases, particularly in Saudi Arabia, requires a thorough understanding of the healthcare environment, patient needs, and specific challenges in Saudi Arabia. Moreover, ethical and regulatory concerns associated with the deployment of AI systems in clinical practice must be addressed to ensure that AI technologies are applied responsibly and effectively.11
Furthermore, managing chronic conditions often requires patients to make lasting changes in their behavior, which may be influenced by several factors. One such factor is self-efficacy—the confidence a person has in their ability to take control of their health and follow through with necessary changes.11 Measurement of self-efficacy offers a simple way to evaluate how capable patients feel about managing their own care, and is often suggested as an important part of managing chronic diseases.11 Cognitive symptom management is another crucial aspect of care for patients with chronic conditions, which helps them cope with mental and emotional challenges such as stress, negative thinking, and fatigue that often accompany long-term illness.12 This approach empowers patients to become active participants in their care, challenge maladaptive thoughts, regulate emotions, and improve their overall quality of life by fostering resilience and effective coping mechanisms.
Impaired cognitive function can hinder a patient’s ability to monitor their own health and perform complex self-care tasks. In this regard, the self-efficacy theory by Bandura has been used to improve the management of chronic conditions by enhancing patients’ understanding of how they can use their ability to manage their health using AI.13 The primary principles of Bandura’s self-efficacy theory are mastery experiences, vicarious learning, social persuasion, and emotional states. These principles can influence self-belief in determining the behaviors chosen to achieve better outcomes. However, the correlation between AI use and self-efficacy and cognitive symptom management among patients with chronic conditions remains poorly understood, despite the growing use of digital tools in healthcare. Furthermore, evidence on these relationships—particularly within the Saudi context—is limited, resulting in a knowledge gap in understanding how AI may support the cognitive and self-management needs of patients.
Therefore, this study examined whether the use of AI was associated with better self-efficacy and cognitive symptom management among patients with chronic conditions in Saudi Arabia. In addition, we aimed to identify potential demographic factors that may be associated with these variables. We applied Bandura’s theory, particularly a mastery experience of using AI to influence patients’ self-confidence in using AI in chronic condition management among patients in Saudi Arabia. We hypothesized that the use of AI may support patients’ ability to take ownership of their care and enhance behavior change in cognitive symptoms management.
Materials and Methods
Study Design
This study had a cross-sectional, descriptive-correlational design. Data were collected at a single time point to describe the sample characteristics and variables and determine the relationships between them. This design was also completed within a specific timeframe to determine the patterns among variables, contributing to a better understanding of the variables.14
Study Setting
The study was conducted at the Primary Healthcare Centers (PHCs) in Saudi Arabia, which are managed by the Ministry of Health to provide essential healthcare services to citizens and residents. Vision 2030 by Saudi Arabia seeks to achieve its healthcare sector goals, including improving the quality of care services, increasing life expectancy, and reducing the burden on secondary and tertiary hospitals.15 The government aims to promote a healthy quality of life for people and provide resources for an effective healthcare system focusing on preventive and primary healthcare services, which aligns with the objectives of the Vision.
Sampling Process
This study employed a convenience sampling method. The required sample size was calculated using the Soper online formula [https://www.danielsoper.com/statcalc/calculator.aspx?id=1], with an anticipated effect size of 0.15, a desired statistical power level of 0.80, a number of 12 factors, and a probability level of 0.05. These parameters indicated that a minimum sample size of 127 participants was required. Considering an additional 10% to account for potential missing data, the estimated sample size was calculated to be a minimum of 140 participants.
The inclusion criteria were as follows: 1) adult patients aged ≥ 18 years; and 2) diagnosed with one or more chronic illnesses and receiving treatment at a PHC in Saudi Arabia. The exclusion criteria were as follows: patients 1) with acute medical conditions or those requiring immediate medical intervention unrelated to their chronic illness; 2) with cognitive impairments, including conditions such as dementia or severe mental health disorders, that prevent them from comprehending the study requirements or participating effectively; and 3) who do not speak or understand the Arabic language, as this would hinder their ability to complete surveys accurately and provide meaningful responses.
Instrumentation
Data were collected using a structured questionnaire consisting of four sections. The instrument was translated into Arabic using a forward–backward translation process to ensure understanding for Arabic-speaking participants and was pilot tested to confirm clarity and cultural appropriateness. The first and second sections of the questionnaire included questions on demographics and 12 items related to AI, respectively. The third and fourth sections of the questionnaire covered self-efficacy and cognitive symptom management, respectively, with six items each.
Artificial Intelligence Scale
In this study, the assessment focused on participants’ perceptions, familiarity, and readiness to engage with AI-enabled healthcare tools, rather than on the technical performance of specific AI algorithms. Therefore, the AI scale was used to assess the attitudes, understanding, and engagement of using technologies to manage healthcare conditions.16 This scale includes 12 items which measure an individual’s trust in AI tools to complete tasks and evaluates the perceived use, accuracy, and usefulness of the tool. Scores range from 1 (strongly disagree) to 5 (strongly agree), with higher scores indicating better perceived use of AI in healthcare. The items assess multiple aspects of AI perception, such as its potential to reduce errors in medical practice, facilitate patients’ access to services, and enable healthcare professionals to make more accurate decisions. Additionally, the scale explores concerns related to privacy, data security, and the reliability of AI technologies. The AI scale also provides insight into psychological and contextual factors that may influence user acceptance of AI-supported clinical care. Assessing these dimensions allows for more understanding of the facilitators and barriers to AI adoption in chronic conditions self-care. In this study, the scale demonstrated acceptable internal consistency (Cronbach’s α = 0.74).
Self-Confidence Scale
The Self-confidence scale comprises six items which measure an individual’s belief in their ability to perform specific tasks and achieve goals.17 Each of these items typically assesses different aspects of self-efficacy, such as confidence in overcoming challenges, persistence, and the ability to manage difficult situations. Respondents rate their agreement with statements on a scale from 10 (totally confident) to 1 (not at all confident) to quantify self-efficacy levels. In this study, the scale had Cronbach’s alpha 0.94, indicating excellent internal consistency of the scale.
Cognitive Symptom Management Scale
Chronic conditions often impact physical health and cognitive functions such as memory, concentration, and problem-solving abilities. Therefore, the Cognitive Symptom Management scale, a 6-item behavior change tool that determines whether people are practicing any cognitive stress reduction techniques for healthier behaviors, was also administered in this study.18 The scale scores range from 0–5, with a higher score indicating more practice of these techniques. The reliability of this scale was determined to be 0.87.
Data Collection Procedures
Data were collected using an online questionnaire designed using Google Forms and distributed to eligible patients with chronic conditions through commonly used social media platforms. The use of an online survey facilitated broader access to respondents and ensured efficient data collection within the study period. Participation was voluntary, and responses were collected anonymously. Research assistants were also asked to facilitate data collection to maintain consistency in data collection procedures and improve the efficiency of the study process. Data were collected between December 2024 and March 2025.
Data Analysis
All data analyses were performed using the Statistical Package for the Social Sciences (SPSS) Version 31 (IBM Corp., Armonk, NY, USA). Prior to this, data management was conducted to ensure data quality, security, accessibility, and compliance, ultimately enhancing the reliability and effectiveness of the research outcomes. Missing data were minimal and were addressed using mean or mode imputation, depending on the variable type. Outliers were evaluated using statistical and visual methods, however, none required action as no concerning values were identified. Continuous variables are presented as measures of central tendency (Means and Standard Deviation measures), whereas categorical variables are presented as frequencies and percentages.
The independent sample t-test was used to evaluate the difference between the mean scores of the two groups, providing insights into the influence of different demographic factors on self-efficacy and cognitive symptoms levels. In addition to p-values, effect sizes (Cohen’s d) and 95% confidence intervals were estimated to determine the magnitude and precision of group differences. Pearson’s correlation coefficient was used to assess the strength and direction of linear relationships between continuous variables.19 The effect size was reported based on the magnitude and the strength of the association between the variables. The 95% confidence intervals were estimated using bias-corrected and accelerated (BCa) bootstrapping to enhance the robustness of the Pearson’s findings.
A one-way analysis of variance (ANOVA) was used to assess the difference in the means of the dependent variable among three or more independent groups,19 providing insights into how different factors influence self-efficacy and cognitive symptom management. Multiple linear regression was used to examine the relationships among AI perception, self-efficacy, and cognitive symptom management while controlling for other covariates, which were selected based on theoretical relevance and their potential to confound the variables’ associations. Standardized regression coefficients (β) were reported as measures of effect size, along with unstandardized coefficients and 95% confidence intervals. Bootstrapped BCa confidence intervals were used where appropriate to improve estimation accuracy. This analytical method helped identify the relative contributions of multiple predictors to the outcome variable, providing a more comprehensive understanding of the dynamics involved.
Ethical Considerations
This study was approved by the Institutional Review Board at King Saud University Medical City and was performed in accordance with the ethical standards and guidelines of the Declaration of Helsinki. All included participants provided written informed consent prior to study participation.
Results
Univariate Analyses
Table 1 summarizes the demographic and background characteristics of 163 participants. The majority of them were Saudi nationals (95.7%), with women comprising 73% of the cohort. Most participants were married (75.5%) and had attained university-level education (68.7%). Approximately, more than half (55.2%) of the participants reported an income above 7000 SAR, and 60.7% of them lived in urban areas. Among the study cohort, 46% participants had been diagnosed with a chronic illness for more than five years. Additionally, 65.6% participants had a household member with a chronic illness, and one-third (33.7%) had previously used AI tools.
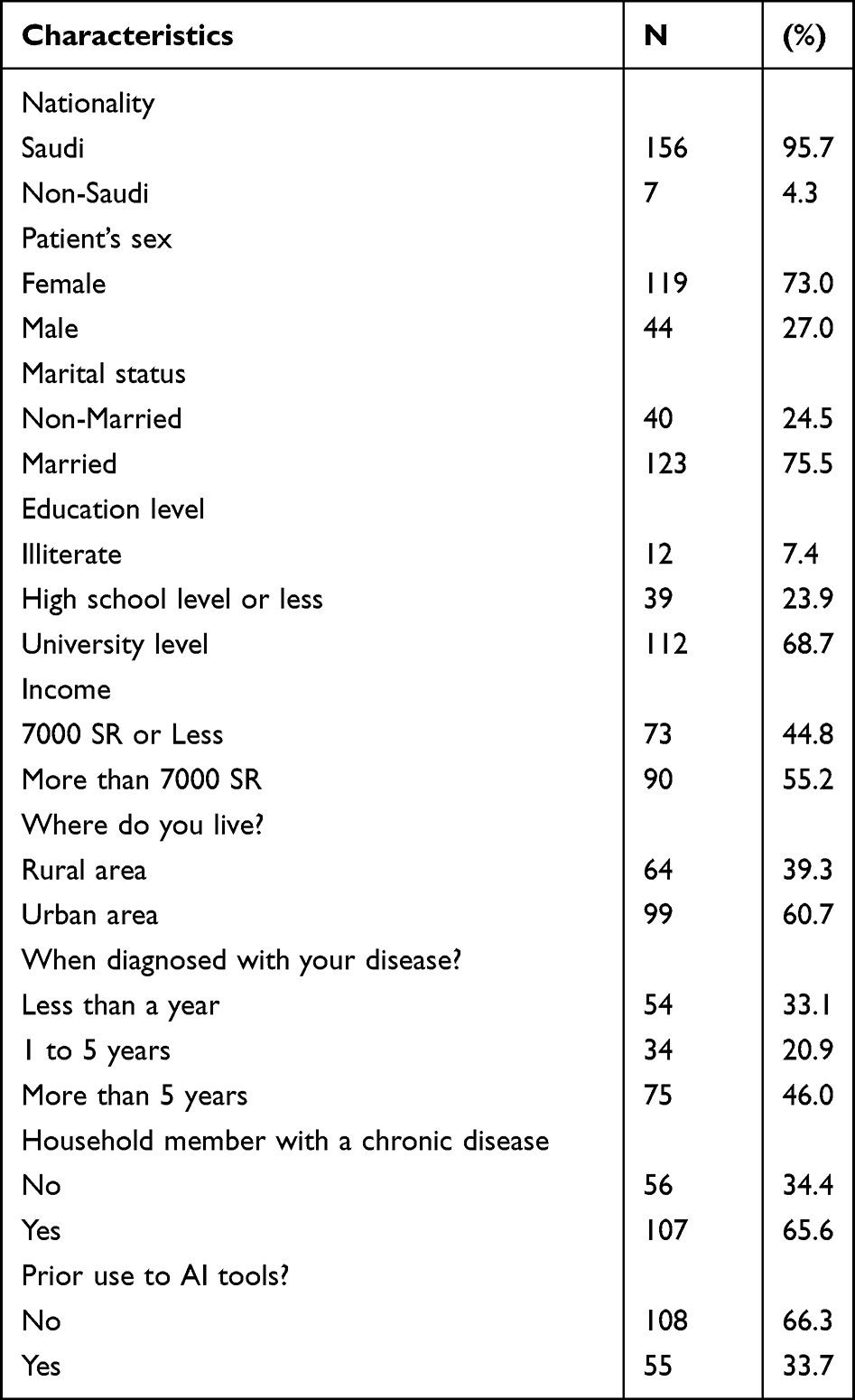 |
Table 1 Sample Characteristics (N= 163) |
Bivariate Analyses
Tables 2–4 present the mean differences in AI perception, self-efficacy, and cognitive symptoms management, respectively, across key binary demographic variables, analyzed using independent sample t-tests. No statistically significant differences were observed in the demographic variables (p > 0.05). While some trends suggested variations (eg, higher self-efficacy among those with previous AI use), most comparisons did not reach statistical significance. These results suggest that the selected demographic variables have limited influence on the studied psychological variables.
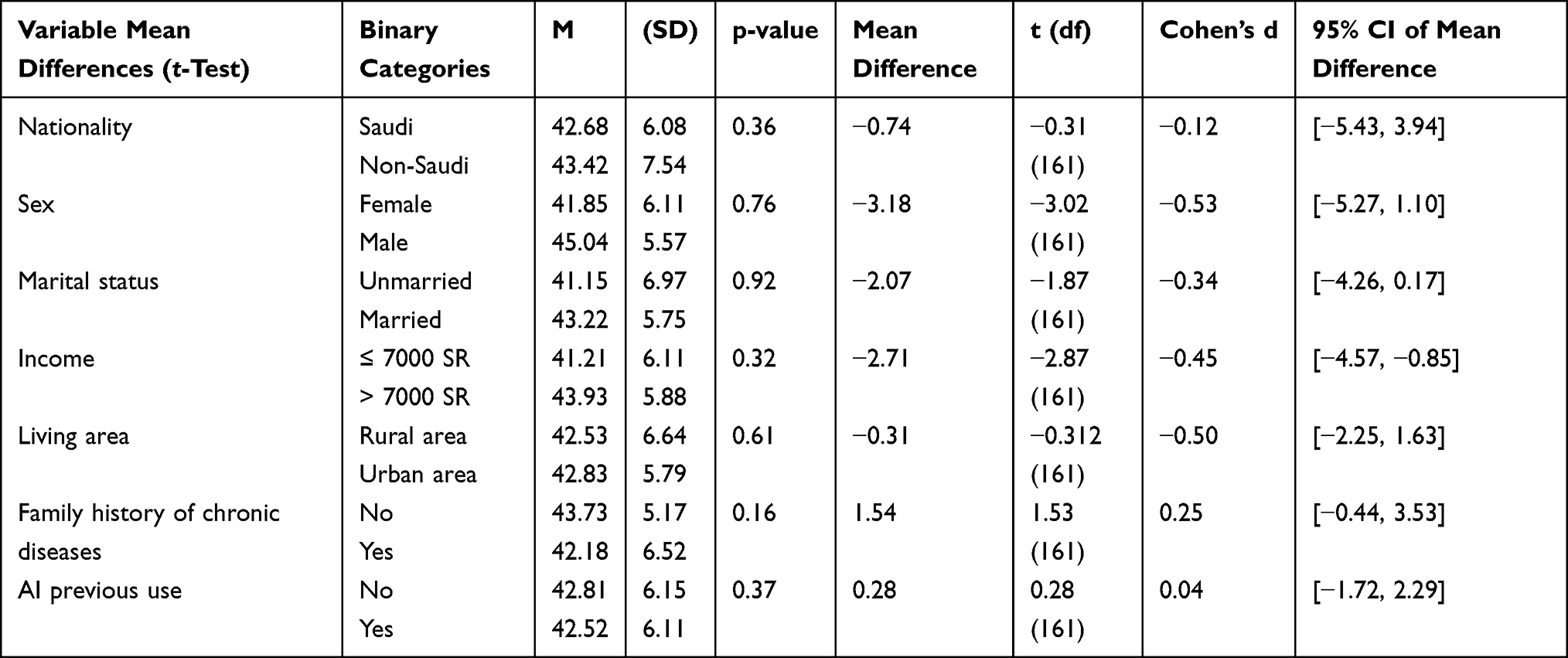 |
Table 2 Mean Differences Between AI Perception and Some Demographic Variables |
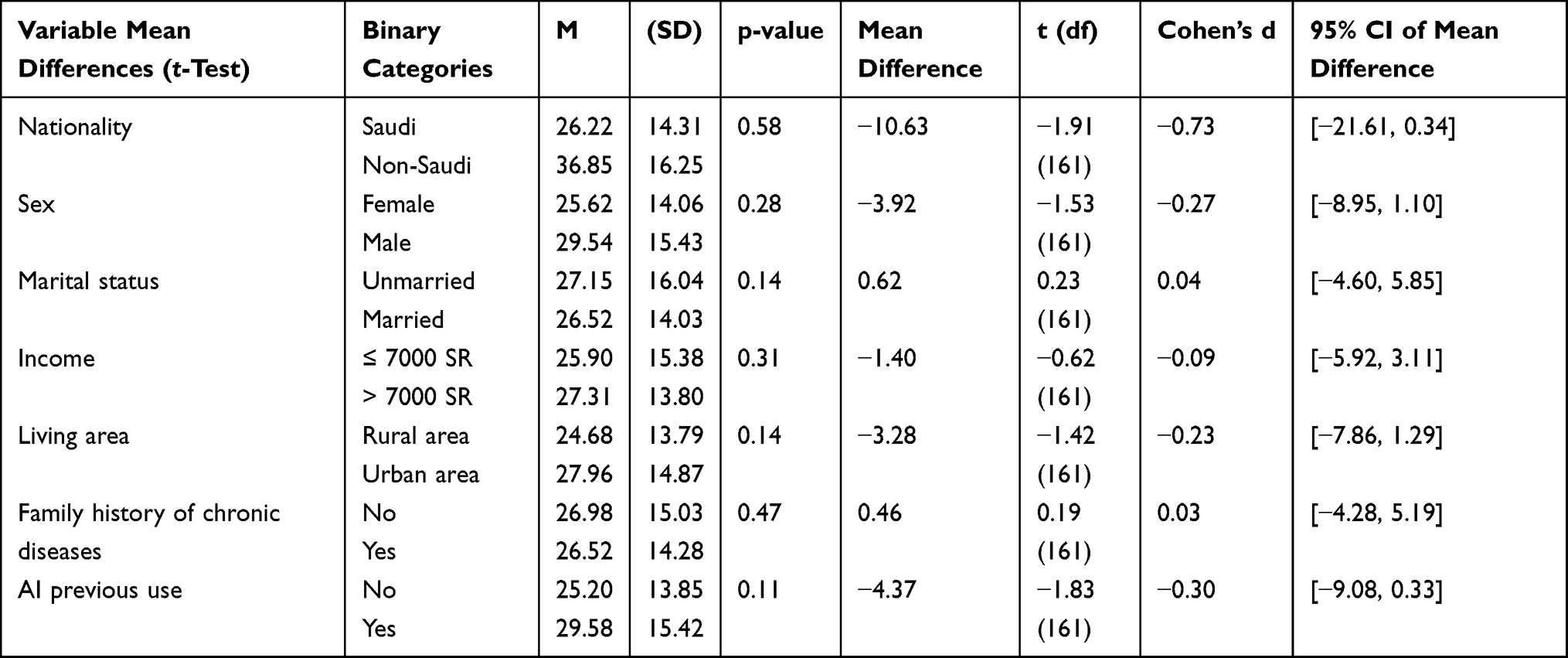 |
Table 3 Mean Differences Between Self-Efficacy and Some Demographic Variables |
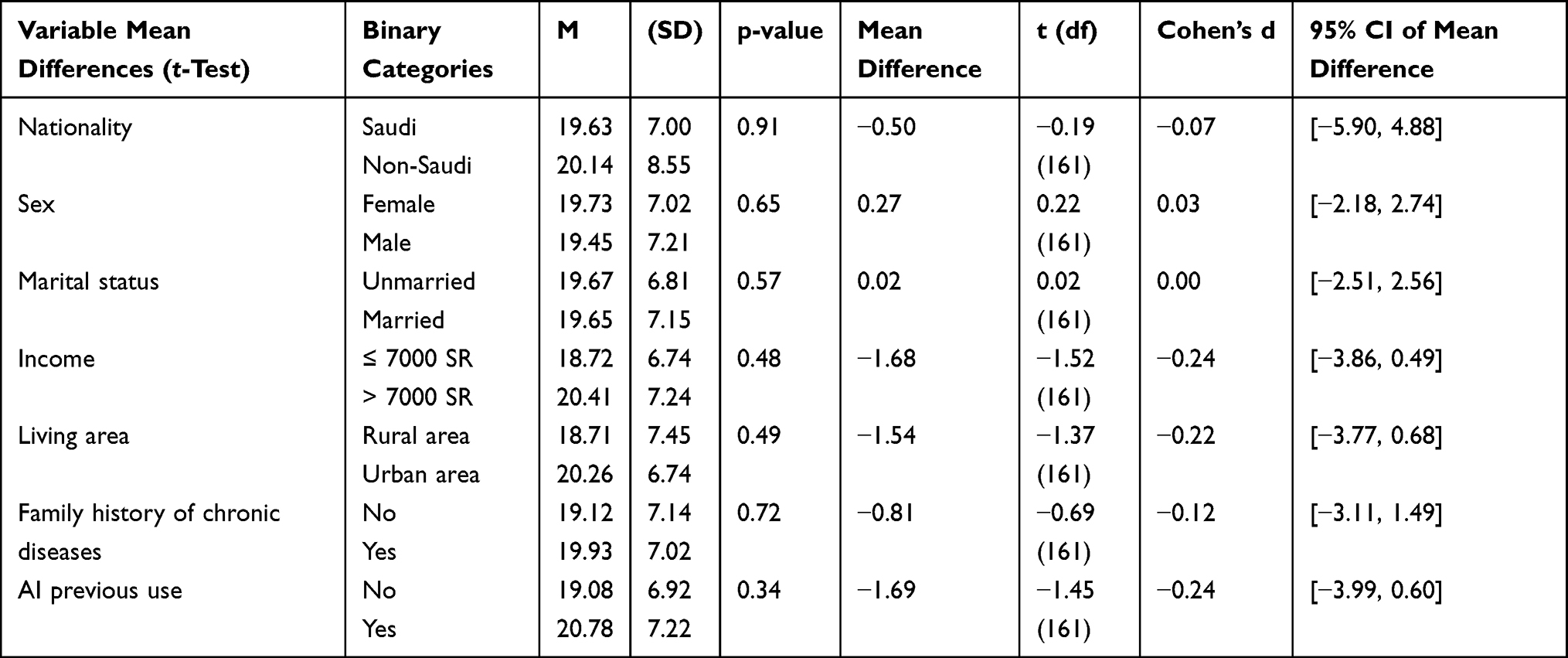 |
Table 4 Mean Differences Between Cognitive Symptoms Management and Some Demographic Variables |
Subsequently, we analyzed the correlation among the continuous variables age, AI perception, self-efficacy, and cognitive symptom management using Pearson’s correlation coefficient. A significant correlation observed was between self-efficacy and cognitive symptom management (r = 0.543, p < 0.05), which indicated that higher self-efficacy may be associated with higher cognitive symptom management. However, other correlations were weak and not statistically significant, suggesting minimal direct relationships between the other variables (see Table 5 for further details). Additionally, one-way ANOVA revealed no statistically significant differences in AI perception, self-efficacy, or cognitive symptom management across demographic groups (p > 0.05).
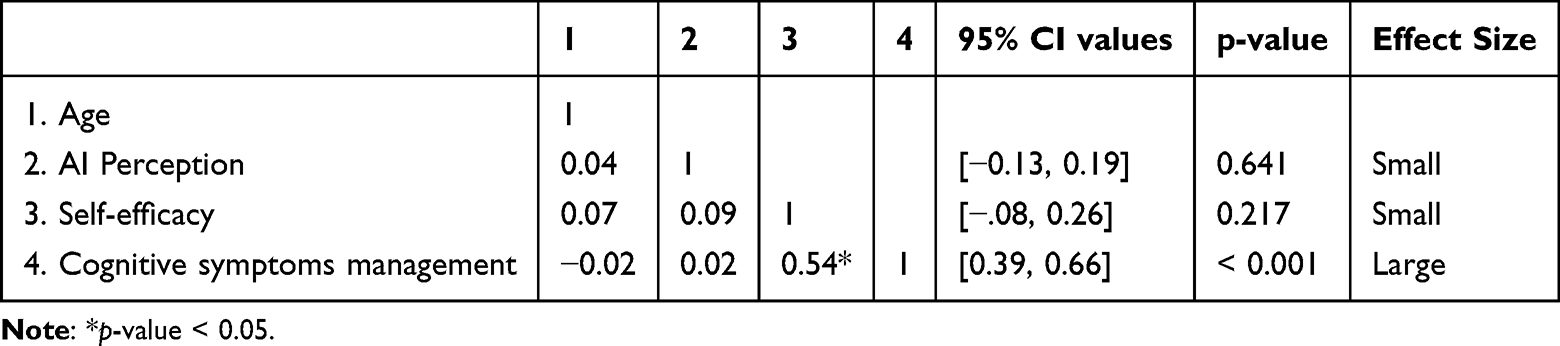 |
Table 5 Correlations Between Continuous Variables |
Multivariate Analyses
Different regression models were used to examine the relationships between key variables from multiple perspectives, allowing for a comprehensive understanding of their effects. The final model was specifically designed to address the third objective of this study, ensuring that the most relevant predictors were accurately assessed.
The first regression model examined predictors of AI perception (Table 6). The model was statistically significant (R2 = 0.123, p = 0.025), explaining 12.3% of the variance in AI perception. In this model, sex emerged as a significant predictor of AI perception (β = 0.19, p = 0.02), with men having more positive perceptions than women. Other variables did not significantly predict AI perception, suggesting limited demographic influence.
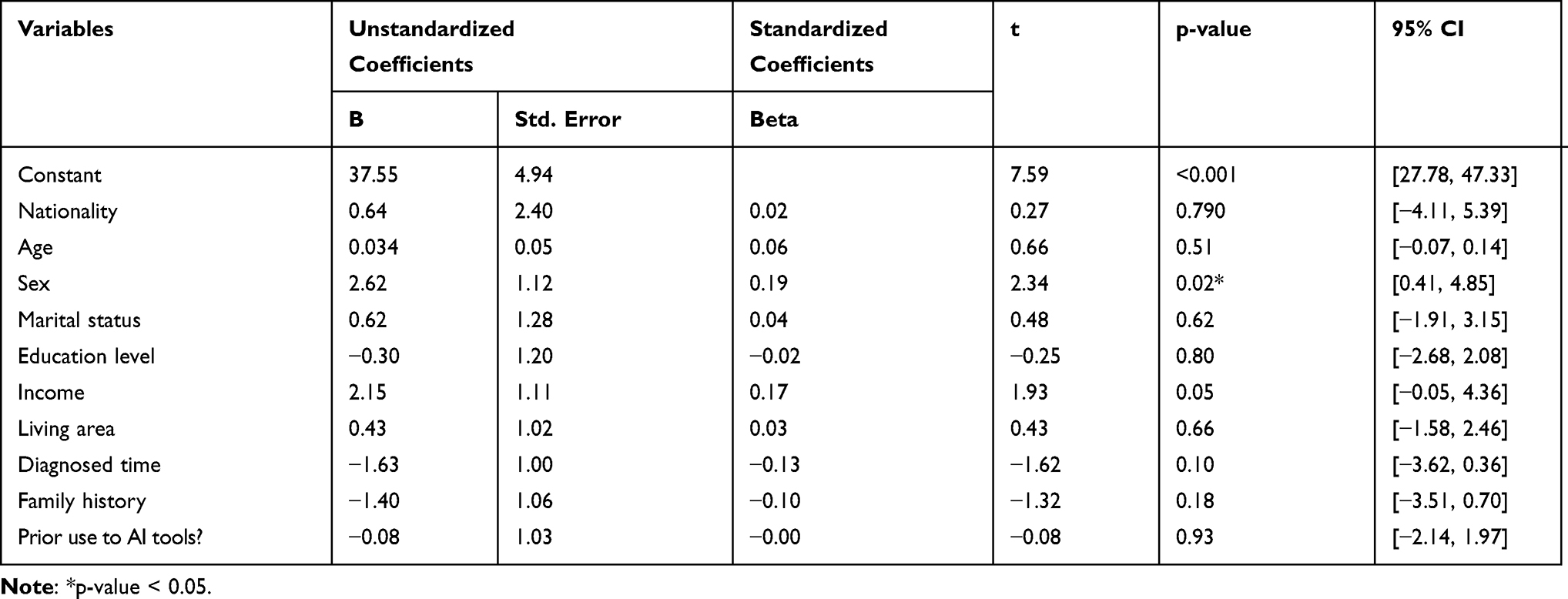 |
Table 6 Multiple Regression Analysis for the AI Perception Variable |
The second model aimed to identify factors predicting self-efficacy (Table 7). Although the model was not statistically significant overall (R2 = 0.089, p = 0.148), these findings warrant further investigation in future studies with larger samples or more targeted variables.
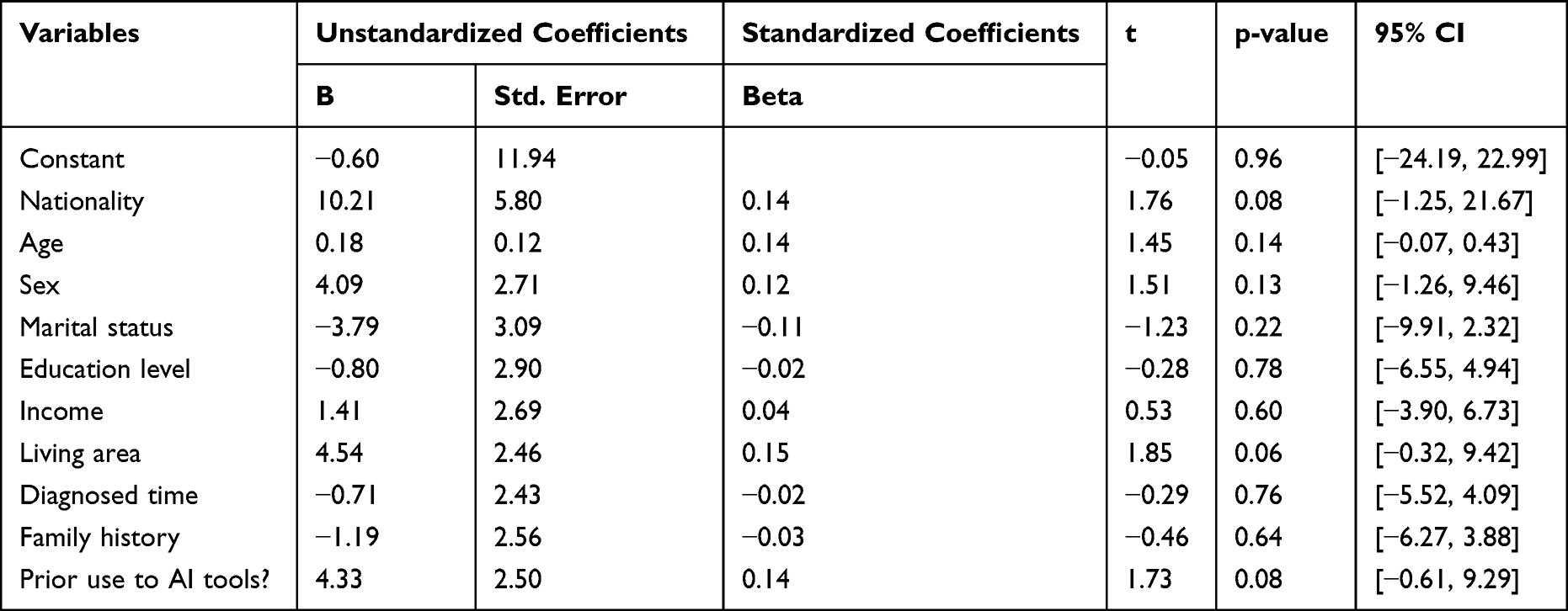 |
Table 7 Multiple Regression Analysis for Self-Efficacy |
Table 8 summarizes the results of the third regression model, which assessed predictors of cognitive symptom management. The model was not statistically significant (R2 = 0.039, p = 0.789), and none of the variables significantly predicted cognitive symptom management. These results suggest that cognitive symptom management in this cohort may be influenced by factors beyond the measured demographics.
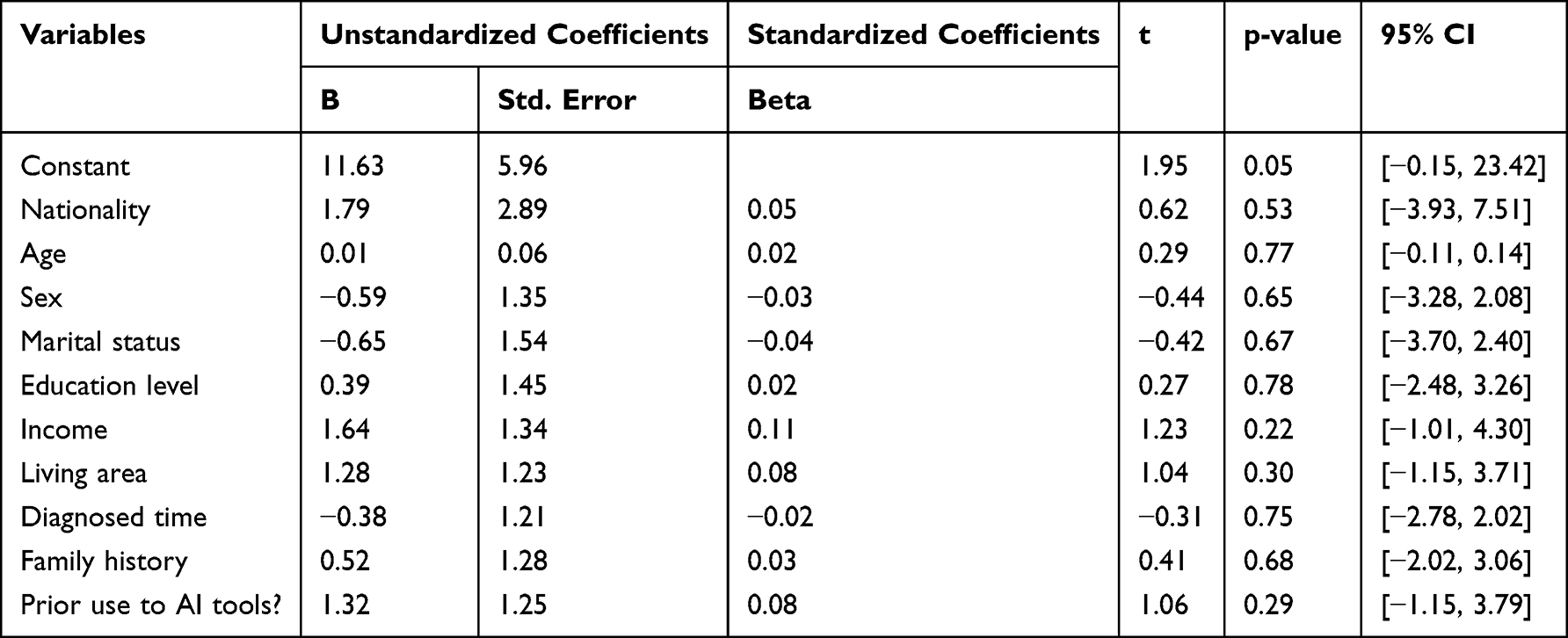 |
Table 8 Multiple Regression Analysis for Cognitive Symptoms Management |
The fourth regression model examined AI perception and self-efficacy and other demographics as predictors of cognitive symptom management. The model was statistically significant (R2 = 0.32, p < 0.001), explaining 32% of the variance. Notably, self-efficacy was a strong and significant predictor of cognitive symptom management (β =0.56, p <0.001), while AI perception was not. This suggests that cognitive symptom management is more strongly related to how confident individuals feel about managing their condition (self-efficacy) rather than to their perceptions of AI (see Table 9).
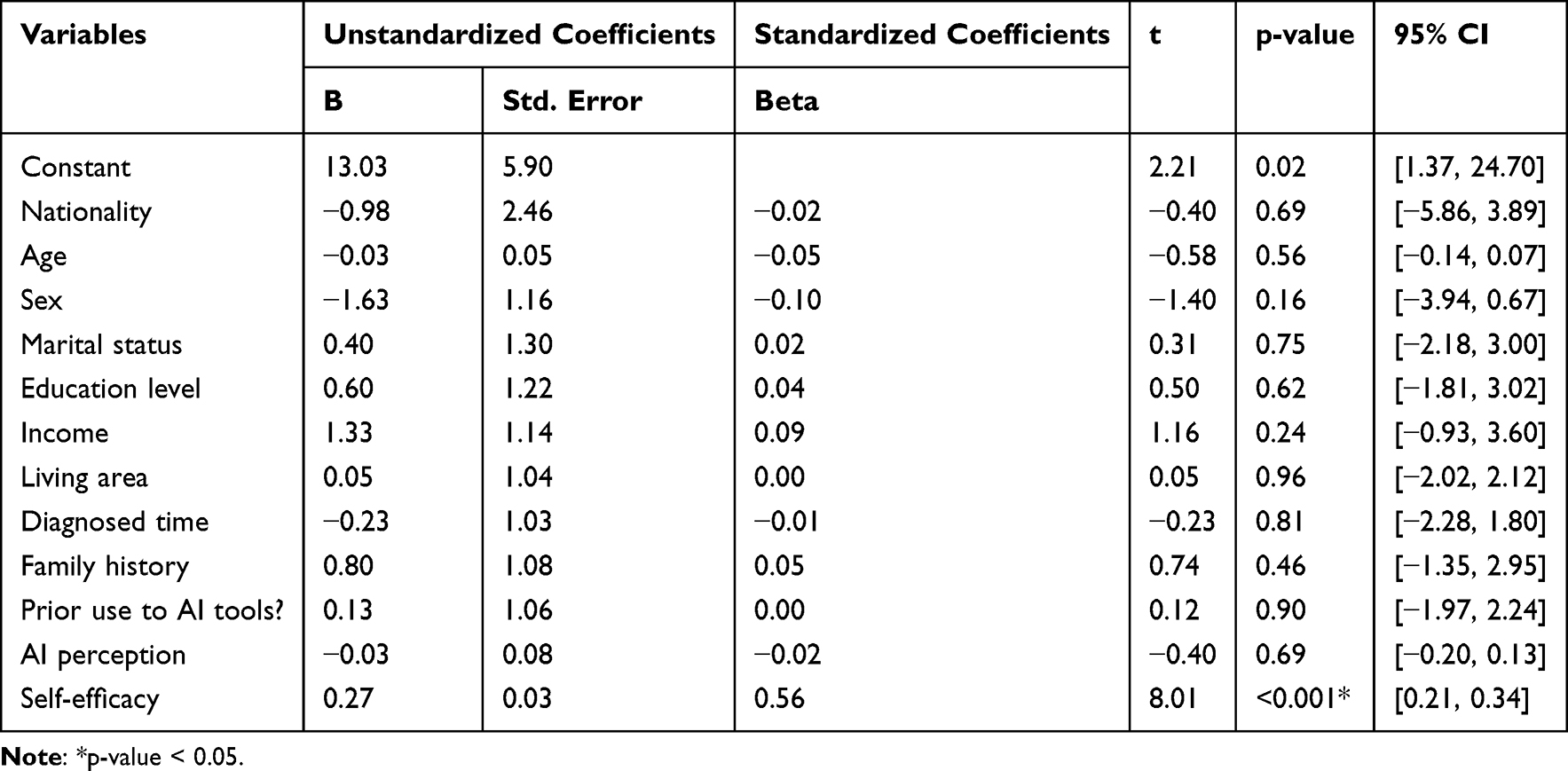 |
Table 9 Multiple Regression Analysis for AI Perception, Self-Efficacy, and Cognitive Symptoms Management |
Discussion
The results of this study showed a strong positive correlation between self-efficacy and cognitive management outcomes. This suggests that an increase in self-efficacy can significantly improve cognitive management outcomes. Additionally, the magnitude of this association indicates that self-efficacy is statistically significant and practically meaningful in influencing cognitive symptom management. Thus, this study underscores the significant relationship between self-efficacy and cognitive performance in patients with chronic conditions. This finding is consistent with that of a previous study which reported that improved health education for individuals with a single chronic condition is associated with better adherence to self-management practices and medication routines in their daily lives.20 These findings suggest that self-efficacy may function as an essential psychological mechanism through which individuals effectively manage cognitive challenges associated with chronic conditions. Additionally, our findings highlight the importance of fostering self-efficacy in individuals, as it may lead to better cognitive performance. Notably, this relationship remained strong even after considering relevant sociodemographic and clinical factors, reinforcing the stability of the observed association. Consequently, effective interventions should be implemented to enhance self-efficacy, especially in contexts where cognitive functioning is critical to success, as they may yield meaningful improvements in cognitive symptom management and overall patient functioning.
In this study, Saudi participants scored lower than non-Saudi participants in terms of AI perception. Although this difference was small, it highlights potential contextual disparities in exposure to and familiarity with AI-enabled healthcare tools. This discrepancy can be attributed to differences in familiarity with technology, where non-Saudis participants may have had more exposure to AI tools than Saudi participants. Therefore, such differences should be interpreted with caution, given the relatively small number of non-Saudi participants in the sample. Additionally, this may reflect broader socio-cultural factors in Saudi Arabia, where rapid digital transformation is still evolving across sectors and individuals may vary in their opportunities and readiness to adopt emerging technologies. Variability in digital literacy and access may shape the perceptions of AI more strongly than nationality alone.
Moreover, sex was significantly correlated with AI perception; men generally exhibited a stronger perception of AI than women. This association was remained significant even after controlling for other sociodemographic variables, suggesting a stable relationship between sex and AI perception. This difference could stem from societal expectations that encourage men to engage more with technology, while women may face barriers. In this regard, a previous study21 revealed that sex plays an important role in how students use AI-based tools in education, with boys demonstrating a greater intention to engage with AI than girls. The study also highlighted notable differences in how innovation characteristics are perceived based on sex. These findings align with broader literature indicating that gendered access and confidence in technology may influence attitudes toward AI adoption. Furthermore, married individuals might utilize AI more because they often share responsibilities at home, making technology a valuable resource for managing daily tasks. However, this association was not statistically significant in the analyses and should be interpreted as exploratory. A previous study found that AI usage has a positive influence on managing household responsibilities and improving communication within relationships.22,23 Collectively, these observations suggest that personal and social contexts may shape AI adoption, even when direct effects are modest.
In this study, non-Saudi patients appeared to have better self-efficacy in managing chronic diseases compared to their Saudi counterparts, although this difference was not statistically significant. This finding suggests that nationality alone may not be a decisive determinant of self-efficacy when other contextual and individual factors are considered. Factors such as access to healthcare and educational resources may influence these outcomes, thereby alleviating challenges related to access to care.24 These factors may interact with individual experiences and health literacy rather than operate independently. Additionally, patients living in urban areas tended to report higher self-efficacy than those in rural settings, likely reflecting greater access to healthcare resources, health information, and support systems in Saudi Arabia. Although this was observed, the association was not significant in adjusted analyses and should therefore be applied carefully. While some studies showed that patients in urban areas reported higher self-efficacy due to better access to healthcare and support systems, other studies presented contrasting findings. For example, Miller et al25 examined self-management of rural adults with multimorbidity and found that the participants reported high levels of self-efficacy, patient activation, and social support compared to urban adults. Moreover, a study comparing patients with cancer in rural and urban settings revealed that rural patients had significantly greater knowledge, skills, and confidence in managing their health than their urban counterparts.26 These findings suggest that self-efficacy may be shaped by social cohesion, community engagement, and family support networks rather than geographic location does. Community involvement and the preference for more isolated living in rural areas may also enhance health behaviors and self-management capabilities. However, urban patients often have better access to healthcare facilities and support systems, which can also empower them to manage their health more effectively. Taken together, the findings highlight the complex and context-dependent nature of self-efficacy in chronic disease care.
Cognitive symptom management also interacts with family dynamics. Patients who have a family member with a chronic disease may benefit from shared emotional support and practical guidance. Such shared experiences may facilitate adaptive coping strategies and knowledge exchange, which can support cognitive symptom management. In the Saudi context, strong family cohesion enhances this effect, providing reassurance and shared assistance for managing chronic conditions. Family-centered support structures may serve as an important contextual factor in patient self-management. However, Silva, et al26 explored the relationship between family dynamics and cognitive decline in older adults and reported that approximately 10% of the participants experienced family dysfunction, although this was not linked to declines in cognitive performance measured. Ultimately, the study concluded that family functioning does not significantly impact cognitive decline among older individuals living in the community. These findings suggest that while family support may influence subjective management experiences, its direct effect on cognitive outcomes may be limited.
Furthermore, prior experience with AI tools can aid in managing cognitive symptoms. Familiarity with digital technologies may increase confidence and reduce uncertainty when engaging with AI tools. Thus, in Saudi Arabia, expanding digital health initiatives and increasing tech adoption may enhance individuals’ confidence and willingness to use such tools effectively. Nevertheless, the potential benefits of AI familiarity should also be considered alongside its limitations. For example, Gerlich27 investigated the connection between AI usage and cognitive skills, raising several important concerns. Their findings indicated a negative correlation between frequent use of AI tools and critical thinking abilities, implying that individuals who depend heavily on automation may face challenges in exercising independent reasoning. This highlights the importance of balanced AI integration that supports, rather than replaces, human cognitive engagement. Nevertheless, familiarity with technology can offer patients strategies and resources that enhance their ability to overcome cognitive difficulties, making them feel more confident and capable in managing their conditions. Accordingly, AI-enabled tools should be designed to support cognitive self-management while preserving active patient involvement.
In the regression analyses, although some models explained only a limited proportion of the variance, this was expected given the multifactorial nature of the outcomes. Cognitive symptom management and technology perception are influenced by a complex interplay of psychological, social, and contextual factors that extend beyond sociodemographic characteristics alone. The AI perception model was significant, indicating that at least one predictor had a meaningful impact on AI perception. Notably, sex emerged as the only significant predictor within this model, suggesting that men may perceive AI more positively than women. This is consistent with Russo et al28 who found that women experience significantly higher levels of anxiety regarding AI compared to men, which negatively affects their willingness to use these technologies. Moreover, while men generally have more positive attitudes toward AI, women often feel less knowledgeable, contributing to their reluctance to engage with AI tools. These differences may reflect broader gender disparities in access to technological training and confidence rather than intrinsic differences in capability.
In the regression analysis model for cognitive symptom management using all demographic variables, AI perception, and self-efficacy were significant; however, self-efficacy emerged as the only significant predictor of cognitive symptom management, underscoring its central role in influencing outcomes. The absence of a direct effect of AI perception after adjustment suggests that technology attitudes alone may be insufficient to support cognitive outcomes without adequate personal capability and confidence. Strong cultural emphasis on personal responsibility and family expectations may further reinforce the impact of self-efficacy on how individuals’ approach and manage their symptoms. This highlights self-efficacy as a potentially modifiable target for interventions aimed at improving cognitive symptom management. This is consistent with the results of Simone et al,29 who explored the connections between motivation for lifestyle changes aimed at reducing dementia risk and participation in health behaviors. The results revealed that higher self-efficacy significantly predicted increased physical and cognitive activity, as well as improved sleep quality. Additionally, Miao et al30 found that self-efficacy was a significant predictor of academic success. Collectively, these findings support the main role of self-efficacy across diverse domains of performance and well-being. They also underscore the importance of understanding sex dynamics in technology perception and the vital impact of self-efficacy on cognitive functioning.
Study Implications
The findings of this study have significant implications in research and clinical practice. For instance, understanding the role of sex in AI perception can inform targeted educational and outreach programs that aim to increase technology acceptance among underrepresented groups, particularly women. Stakeholders can enhance engagement with AI technologies by addressing the specific barriers they face, ultimately fostering a more inclusive technological landscape. Additionally, the strong link between self-efficacy and cognitive outcomes suggests that interventions aimed at enhancing self-efficacy could lead to improved cognitive performance, especially in managing chronic diseases.
Furthermore, the insights gained from this study can guide healthcare providers and policymakers in designing programs that power AI tools to support patient self-management. Healthcare initiatives can focus on equipping patients with the skills and confidence needed to utilize these technologies effectively recognizing the importance of self-efficacy. This could lead to better health outcomes and improved quality of life for individuals, particularly those living with chronic conditions. Overall, the study highlights the need for continued exploration of the factors influencing AI perception and self-efficacy, paving the way for future research.
Limitations of the Study
Despite its positive outcomes, this study has some limitations. First, convenience sampling from PHCs or the disproportion representation of women in the sample may limit the generalizability of the findings. Therefore, future studies should consider employing broader, probability-based sampling approaches to enhance representativeness.31,32 Second, the reliance on self-reported measures may have introduced potential bias, as participants may overestimate or underestimate their experiences and abilities.33 Third, the cross-sectional design limited the ability to draw causal inferences, highlighting the need for longitudinal studies to better understand the relationships over time.34 Fourth, the study did not account for other factors that could influence AI perception and self-efficacy, such as socioeconomic status or educational background, which might provide a more comprehensive understanding of the outcomes. Although the sample exhibited a sex imbalance, supplemental analyses confirmed that this did not meaningfully affect the statistical inferences. Given the cultural context of the participants, the findings may not apply to populations from different cultural backgrounds, potentially limiting the study’s relevance in a global context. Finally, the study conceptualized AI as a supportive digital health tool, and the findings should be applied in the context of user perception and self-efficacy rather than as an evaluation of AI system performance.
Conclusion
This study explored how AI use relates to self-efficacy and cognitive symptom management in Saudi patients with chronic conditions, along with demographic factors that may influence these associations. Men may engage with AI technologies more positively than women, indicating the need for targeted interventions to foster greater inclusivity in technology adoption among women. Additionally, the strong relationship between self-efficacy and cognitive symptom management emphasizes the importance of enhancing individuals’ confidence in managing their chronic conditions. Consequently, future research should explore the underlying factors shaping these insights and support strategies to improve engagement with AI-supported health tools.
Disclosure of AI Use
AI tool was used to help improve language and readability of some sentences, with caution. The content has been reviewed and approved for publication.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the institutional review board of King Saud University (Reference #: E-24-9265), dated 20 November 2024. Informed consent was obtained from all participants.
Acknowledgments
Both Maryam Allayl and Ghareeb Bahari contributed equally as first-joint authors for this study. The authors extend their appreciation to the Ongoing Research Funding program, (ORF-2026-438) at King Saud University, Riyadh, Saudi Arabia.
Funding
This work was supported by the Ongoing Research Funding program, (ORF-2026-438) at King Saud University, Riyadh, Saudi Arabia.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Alharbi R, Qadri A, Mahnashi M, et al. Utilization of health applications among patients diagnosed with chronic diseases in Jazan, Saudi Arabia during the COVID-19 pandemic. Patient Prefer Adherence. 2021;15:2063–14. doi:10.2147/PPA.S329891
2. Xie Y, Lu L, Gao F, et al. Integration of artificial intelligence, blockchain, and wearable technology for chronic disease management: a new paradigm in smart healthcare. Curr Med Sci. 2021;41(6):1123–1133. doi:10.1007/s11596-021-2485-0
3. Ayesh A. User-Centric A.I. Analytics for chronic health conditions management [Internet]. arXiv; 2024. Available from: http://arxiv.org/abs/2402.01652.
4. Aamir A, Iqbal A, Jawed F, et al. Exploring the current and prospective role of artificial intelligence in disease diagnosis. Ann Med Surg. 2024;86(2):943–949. doi:10.1097/MS9.0000000000001700
5. Alotaibi M. Intelligent Eczema management and awareness system for Saudi Arabia System Architecture. In:
6. Tarumi S, Takeuchi W, Chalkidis G, et al. Leveraging artificial intelligence to improve chronic disease care: methods and application to pharmacotherapy decision support for type-2 diabetes mellitus. Methods Inf Med. 2021;60(S 01):e32–e43. doi:10.1055/s-0041-1728757
7. Omar AN, Baabdullah AM, Alalwan AA, Lal B, Dwivedi YK. Artificial intelligence-based public healthcare systems: G2G knowledge-based exchange to enhance the decision-making process. Gov Inf Q. 2022;39(4):101618. doi:10.1016/j.giq.2021.101618
8. Saeed A, Bin Saeed A, AlAhmri FA. Saudi Arabia health systems: challenging and future transformations with artificial intelligence. Cureus. 2023;15(4):e37826. doi:10.7759/cureus.37826
9. Qaffas AA, Hoque R, Almazmomi N. The Internet of things and big data analytics for chronic disease monitoring in Saudi Arabia. Telemed J E Health. 2021;27(1):74–81. doi:10.1089/tmj.2019.0289
10. Mennella C, Maniscalco U, De Pietro G, Esposito M. Ethical and regulatory challenges of AI technologies in healthcare: a narrative review. Heliyon. 2024;10(4):e26297. doi:10.1016/j.heliyon.2024.e26297
11. Chan SWC. Chronic disease management, self-efficacy and quality of life. J Nurs Res. 2021;29(1):e129. doi:10.1097/JNR.0000000000000422
12. Gkintoni E, Vassilopoulos SP, Nikolaou G. Mindfulness-based cognitive therapy in clinical practice: a systematic review of neurocognitive outcomes and applications for mental health and well-being. J Clin Med. 2025;14(5):1703. doi:10.3390/jcm14051703
13. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037//0033-295x.84.2.191
14. Lau F. Methods for correlational studies. In: Handbook of EHealth Evaluation: An Evidence-Based Approach. Victoria (BC): University of Victoria; 2017.
15. Alasiri AA, Mohammed V. Healthcare transformation in Saudi Arabia: an overview since the launch of vision 2030. Health Serv Insights. 2022;15:11786329221121214. doi:10.1177/11786329221121214
16. Syed W, Basil A, Al-Rawi M. Assessment of awareness, perceptions, and opinions towards artificial intelligence among healthcare students in Riyadh, Saudi Arabia. Medicina. 2023;59(5):828. doi:10.3390/medicina59050828
17. Lorig KR, Sobel DS, Ritter PL, Laurent D, Hobbs M. Effect of a self-management program on patients with chronic disease. Effective Clin Pract ECP. 2001;4(6):256–262.
18. Scott F. Outcome measures for health education and other health care interventions. Am J Health Syst Pharm. 1997;54(8):1002. doi:10.1093/ajhp/54.8.1002
19. Rao JS. Statistical Methods in Health Disparity Research. New York: Chapman & Hall/CRC; 2023:298.
20. Chen J, Tian Y, Yin M, et al. Relationship between self-efficacy and adherence to self-management and medication among patients with chronic diseases in China: a multicentre cross-sectional study. J Psychosom Res. 2023;164:111105. doi:10.1016/j.jpsychores.2022.111105
21. Ofosu-Ampong K. Gender differences in perception of artificial intelligence-based tools. J Digit Art Humanit. 2023;4(2):52–56. doi:10.33847/2712-8149.4.2_6
22. Nkurunziza A, Munganyinka C. Exploring the impact of artificial intelligence (AI) technology on communication, intimacy, and relationship satisfaction among married couples. Int J Home Sci. 2024;10(3):127–132. doi:10.22271/23957476.2024.v10.i3c.1686
23. Li DM, Parikh S, Costa A. A critical look into artificial intelligence and healthcare disparities. Front Artif Intell. 2025;8:1545869. doi:10.3389/frai.2025.1545869
24. Miller JJ, Barnason SA, Schmaderer M, et al. Self-management of rural adults with multimorbidity: a cross-sectional descriptive study. Online J Rural Nurs Health Care. 2024;24(1):29–51. doi:10.14574/ojrnhc.v24i1.748
25. Nelson D, McGonagle I, Jackson C, Gussy M, Kane R. A rural-urban comparison of self-management in people living with cancer following primary treatment: a mixed methods study. Psychooncology. 2022;31(10):1660–1670. doi:10.1002/pon.6011
26. Silva DF, Souza-Talarico JN, Santos JL, Duarte YA. Family dysfunction and cognitive decline in aging: the “Health, wellbeing, and Aging” (SABE) longitudinal population-based study. Dement Neuropsychol. 2023;17:e20220109. doi:10.1590/1980-5764-dn-2022-0109
27. Gerlich M. AI tools in society: impacts on cognitive offloading and the future of critical thinking. Societies. 2025;15(1):6. doi:10.3390/soc15010006
28. Russo C, Romano L, Clemente D, Iacovone L, Gladwin TE, Panno A. Gender differences in artificial intelligence: the role of artificial intelligence anxiety. Front Psychol. 2025;16:1559457. doi:10.3389/fpsyg.2025.1559457
29. Simone SM, Kaplan M, Giovannetti T. Self-efficacy is key: examining the role of motivation to engage in healthy lifestyle behaviors for dementia prevention in midlife. J Appl Gerontol. 2025;7334648251345191. doi:10.1177/07334648251345191
30. Miao H, Guo R, Li M. The influence of research self-efficacy and learning engagement on Ed.D students’ academic achievement. Front Psychol. 2025;16:1562354. doi:10.3389/fpsyg.2025.1562354
31. Bauer PJ. Recognizing limits on the generalizability of findings of psychological science research. J Appl Res Mem Cogn. 2023;12(2):199–202. doi:10.1037/mac0000125
32. Yarkoni T. The generalizability crisis. Behav Brain Sci. 2020;45e1. doi:10.1017/S0140525X20001685
33. Bauhoff S. Self-report bias in estimating cross-sectional and treatment effects. In: Maggino F, editor. Encyclopedia of Quality of Life and Well-Being Research. Cham: Springer International Publishing; 2023:6277–6279.
34. Figueiredo RG, Patino CM, Ferreira JC. Cross-sectional studies: understanding applications, methodological issues, and valuable insights. J Bras Pneumol. 2025;51e20250047. doi:10.36416/1806-3756/e20250047
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.