Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Integrating Admission Hyperglycemia Into Multidisciplinary Risk Stratification for Sepsis in the ICU: A Retrospective Cohort Study
Authors Tambunan N, Priambodo AP ![]() , Nuraeni A
, Nuraeni A ![]() , Aziz MA
, Aziz MA
Received 7 March 2026
Accepted for publication 7 May 2026
Published 15 May 2026 Volume 2026:19 606688
DOI https://doi.org/10.2147/JMDH.S606688
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Brian Nyatanga
Natalia Tambunan,1,2 Ayu Prawesti Priambodo,3 Aan Nuraeni,3 Muhammad Afiif Aziz1
1Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Intensive Care Unit, Advent Hospital Bandung, Bandung, West Java, Indonesia; 3Department of Critical Care Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia
Correspondence: Natalia Tambunan, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia, Tel +6282214633347, Email [email protected]
Background: Hyperglycemia is a frequently observed metabolic derangement among critically ill patients in the intensive care unit (ICU). It is known to be associated with impaired immune responses and an elevated risk of severe infections, including sepsis. While this association has been extensively documented in high-income countries, evidence from developing nations such as Indonesia remains conspicuously limited, particularly regarding admission hyperglycemia as a prognostic indicator for sepsis. Managing this complex interaction requires a robust, multidisciplinary approach.
Purpose: To evaluate the independent association between admission hyperglycemia and the incidence of sepsis among critically ill ICU patients, adjusting for potential confounders including age, length of ICU stay, and comorbidities, in order to inform collaborative clinical pathways.
Methods: Using convenience sampling, this retrospective cohort study included 290 adult patients (≥ 18 years) admitted to the ICU between January 2021 and December 2025. Admission blood glucose levels were categorized into euglycemia (71– 140 mg/dL), mild hyperglycemia (141– 200 mg/dL), and severe hyperglycemia (> 200 mg/dL). The diagnosis of sepsis was determined based on the clinical assessment of the attending physicians. Data were analyzed using multivariable logistic regression.
Results: Of the 290 critically ill patients analyzed, 159 (54.8%) developed sepsis. Multivariable analysis demonstrated that severe admission hyperglycemia significantly amplified the risk of sepsis (adjusted Odds Ratio [aOR] = 2.54; 95% Confidence Interval [CI]: 1.33– 4.85; p = 0.005). Furthermore, advanced age (> 65 years) (aOR = 1.80; 95% CI: 1.10– 2.93; p = 0.019) and the presence of multiple comorbidities (≥ 2) (aOR = 2.16; 95% CI: 1.28– 3.67; p = 0.004) were identified as independent predictors. Mild hyperglycemia did not exhibit a statistically significant association with sepsis incidence.
Conclusion: Severe admission hyperglycemia (> 200 mg/dL) serves as a robust, independent predictor of sepsis in critically ill patients. Routine blood glucose screening at ICU admission is crucial for early risk stratification. Establishing a coordinated, multidisciplinary protocol integrating physicians, critical care nurses, clinical pharmacists, and dietitians is essential to optimize targeted metabolic interventions and effectively mitigate the sepsis burden.
Keywords: admission hyperglycemia, early medical intervention, intensive care units, patient care team, retrospective studies, sepsis
Introduction
Sepsis remains a leading cause of morbidity and mortality in intensive care units (ICUs) worldwide. According to the Global Burden of Disease Study 2017, the global incidence of sepsis is estimated at 43.7 million episodes annually, with a mortality rate of approximately 19.7%.1 In developing countries such as Indonesia, sepsis-related mortality remains significantly higher, often reaching 40–50% due to delayed diagnosis and limited healthcare resources.2
Hyperglycemia defined as blood glucose levels exceeding 140 mg/dL in non-diabetic patients or acutely elevated glucose in diabetic patients is frequently observed in critically ill ICU patients, irrespective of their prior diabetes history. Recent studies indicate that 30–50% of ICU patients experience hyperglycemia,3 representing one of the most common metabolic derangements in critical care. This metabolic disturbance has been consistently linked to impaired immune function, amplified inflammatory responses, and an elevated risk of nosocomial infections, including sepsis.4,5
The association between hyperglycemia and increased infection risk is mediated by complex, multifaceted biological mechanisms. First, hyperglycemia increases the production of Advanced Glycation End Products (AGEs), which can activate the NF-κB pathway, which in turn increases the production of proinflammatory cytokines and triggers a systemic inflammatory response that supports the development of sepsis. Hyperglycemia also increases the expression of adhesion molecules on endothelial cells that facilitate the migration of inflammatory cells to infected tissues, worsening the infection and increasing the risk of sepsis.6 Second, admission hyperglycemia triggers metabolic pathways, including the polyol pathway and protein kinase C (PKC) activation. This cascade results in the overproduction of reactive oxygen species (ROS) and pro-inflammatory cytokines (TNF-α, IL-6, IL-8).7 Furthermore, the formation of advanced glycation end-products (AGEs) activates the RAGE (receptor for AGEs) pathway, which exacerbates systemic inflammation and elevates sepsis risk.8
Third, hyperglycemia compromises vascular permeability by glycating endothelial tight junction proteins, thereby disrupting barrier integrity and facilitating bacterial translocation and invasive infections.9 Finally, acute hyperglycemia often leads to greater glycemic variability, an independent predictor of adverse clinical outcomes in septic patients compared to stable hyperglycemia.10
In addition to acute metabolic derangements, the susceptibility to sepsis in critically ill patients is significantly influenced by inherent demographic and clinical vulnerabilities. Advanced age is a well-established risk factor, as immunosenescence impairs both innate and adaptive immune responses, thereby reducing the patient’s physiological reserve and capacity to resolve infections.11 Similarly, biological sex has been implicated in varying immune responses, with literature suggesting potential sex-hormone-mediated differences in sepsis susceptibility. Furthermore, a high burden of comorbidities including hypertension, chronic kidney disease, and pre-existing diabetes mellitus contributes to a state of chronic systemic inflammation, rendering patients more susceptible to acute infectious insults.12 Clinical variables such as the ICU length of stay also influence the risk profile, as prolonged hospitalization often correlates with increased exposure to invasive procedures and nosocomial pathogens.2 Consequently, comprehensively explaining how these baseline variables including age, sex, comorbidities, and length of stay interact with acute stress hyperglycemia is essential to establish a robust risk stratification model for newly admitted ICU patients.
Methods
Study Design and Setting
This retrospective, analytical cohort study was conducted at the Intensive Care Unit (ICU) of Advent Hospital Bandung, a 12-bed private referral hospital in West Java, Indonesia. The ICU at this facility operates under a collaborative care model involving intensivists, critical care nurses, clinical pharmacists, and dietitians, making it a highly relevant setting for evaluating complex clinical outcomes. Patient data were retrospectively analyzed from electronic medical records (EMR) for a five-year clinical period, encompassing ICU admissions from January 2021 to December 2025. The operational process of data extraction by the research team was subsequently conducted between December 2025 and January 2026. To ensure rigorous methodological transparency and high-quality reporting, this study was conducted and is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Population and Sampling
The study population comprised all adult patients admitted to the ICU during the study period. A convenience sampling method was employed, encompassing all accessible patients who met the predefined eligibility criteria during the five-year timeframe. In the context of this retrospective EMR-based study, this pragmatic sampling approach was deliberately chosen to capture a comprehensive, real-world representation of the critical care demographic, thereby reflecting the actual clinical burden and minimizing artificial selection bias.
The minimum sample size required for multivariable logistic regression was calculated using G*Power software (version 3.1.9.4). Assuming an expected Odds Ratio (OR) of 2.0, an alpha (α) error probability of 0.05, a statistical power (1-β) of 0.80, and adjusting for seven predictor variables, the minimum required sample size was determined to be approximately 92 patients. The final enrolled sample of 290 patients significantly exceeded this requirement, ensuring robust statistical power and reliability for the multivariable analysis.
Eligibility Criteria
Inclusion criteria were carefully defined to establish a robust and comparable baseline: age ≥18 years, documented availability of blood glucose measurements within the first 4 hours of ICU admission, and a minimum ICU length of stay of ≥24 hours to allow sufficient observation time for clinical outcomes.
To mitigate the influence of profound physiological or pharmacological confounders on both glycemic status and immune response, patients were systematically excluded if they met any of the following criteria: admission hypoglycemia (<70 mg/dL), pregnancy, documented history of chronic corticosteroid therapy prior to admission, or requiring major surgery during the ICU stay. Crucially, patients with an established diagnosis of sepsis prior to or upon ICU admission were excluded to ensure the analysis strictly captured incident (new-onset) sepsis acquired during critical care.
Variables and Operational Definitions
The primary dependent variable was the incidence of sepsis during the ICU stay, defined as a confirmed infection accompanied by evidence of a systemic inflammatory response. To reflect the collaborative nature of critical care, the onset of sepsis was identified through continuous clinical surveillance by critical care nurses and formally diagnosed by the attending physician, with final verification extracted from the patient’s electronic medical record (EMR). The primary independent variable was admission blood glucose, defined as the first glucose measurement obtained within 4 hours of ICU admission. For analytical purposes, glucose levels were stratified into three clinical categories: euglycemia (71–140 mg/dL), mild hyperglycemia (141–200 mg/dL), and severe hyperglycemia (>200 mg/dL). This categorization aligns with established critical care protocols and the Indonesian Society of Endocrinology (PERKENI) guidelines, which reflect American Diabetes Association (ADA) standards. These guidelines establish upper normal limits in the ICU as 140 mg/dL and identify levels >200 mg/dL as the threshold for severe stress hyperglycemia necessitating aggressive intervention.13 In this study, admission blood glucose was deliberately analyzed as a categorical, stratified variable rather than a continuous variable. This categorization was performed a priori based on these established clinical guidelines to ensure that the findings translate into immediate, actionable clinical thresholds for ICU nurses and intensivists, rather than generating a single, study-specific continuous cutoff that might lack external validity.
Potential confounders were systematically included in the analysis to ensure a robust evaluation of independent predictors. These clinical and demographic covariates comprised age (categorized as ≤65 vs. >65 years), ICU length of stay (≤5 vs. >5 days), and comorbidity burden (0–1 vs. ≥2 documented conditions). Specifically, the assessed comorbidities included pre-existing diabetes mellitus, chronic kidney disease, hypertension, chronic pulmonary disease, and cardiovascular disease.
Data Collection Instruments and Techniques
Data were systematically extracted from the EMR using a standardized, pre-tested data collection checklist designed specifically for the study’s variable components. Reflecting the collaborative documentation within the ICU, the extracted data encompassed a comprehensive clinical profile, including demographic information (age and sex), admission blood glucose levels (obtained via centralized laboratory testing or nurse-administered bedside point-of-care glucometers), documented comorbidities, physician-diagnosed sepsis, and ICU length of stay. To ensure high data integrity, all variables were meticulously recorded according to their established operational definitions and subsequently coded into categorical and numerical formats for robust statistical analysis.
Statistical Analysis
Data management and statistical analyses were performed using IBM SPSS Statistics, version 26.0 (IBM Corp., Armonk, NY, USA). In the descriptive (univariate) analysis, categorical variables were summarized as frequencies and percentages, whereas continuous variables were expressed as means and standard deviations (SD) following the assessment of data distribution. For the initial bivariate analysis, Pearson’s Chi-square tests were employed to evaluate the unadjusted associations between categorical independent variables and the incidence of sepsis. Crude Odds Ratios (OR) and their corresponding 95% Confidence Intervals (CI) were calculated to quantify these preliminary associations.
To identify robust, independent predictors of sepsis incidence (categorically coded as 1 = sepsis, 0 = no sepsis), a multivariable logistic regression model was constructed using the forced entry (“enter”) method. All predefined independent variables including admission glucose categories, age, comorbidities, and ICU length of stay were incorporated simultaneously into the model to definitively adjust for potential confounding effects. The overall adequacy and calibration of the final model were rigorously evaluated using the Hosmer-Lemeshow goodness-of-fit test, while potential multicollinearity among predictor variables was effectively ruled out by calculating Variance Inflation Factors (VIF). The VIF values for all independent variables ranged from 1.021 to 1.174, which are well below the conventional threshold of 5.0, confirming the absence of significant multicollinearity.
Results
Study Population and Baseline Characteristics
During the study period, a total of 650 critically ill patients were initially assessed for eligibility. After excluding 360 patients based on predefined criteria (eg., age <18 years, ICU length of stay <24 hours, primary diagnosis of sepsis at admission, and incomplete medical records), a final cohort of 290 ICU patients was included in the multivariable analysis (Figure 1). Of these 290 patients analyzed, a substantial proportion (n = 159; 54.8%) developed sepsis during hospitalization. The cohort presented with a mean age of 62.3 ± 15.2 years, with a slight demographic skew towards the elderly, as 158 patients (54.5%) were aged >65 years. The sex composition demonstrated a relatively balanced distribution, comprising 167 males (57.6%) and 123 females (42.4%).
 |
Figure 1 STROBE flow diagram of the study cohort selection process. |
Reflecting a high burden of clinical complexity typical of critical care settings, the vast majority of patients (n = 265; 91.4%) were admitted with at least one documented comorbidity. The most prevalent underlying conditions were hypertension (21.8%), chronic kidney disease (17.0%), diabetes mellitus (16.3%), and a history of stroke (16.0%). Upon ICU admission, the distribution of blood glucose levels revealed that over half of the cohort experienced acute metabolic derangement: 84 patients (29.0%) presented with mild hyperglycemia and 83 patients (28.6%) with severe hyperglycemia, whereas 123 patients (42.4%) remained euglycemic. Consequent to their critical illness, approximately 60.0% of the patients (n = 174) required a prolonged ICU length of stay exceeding 5 days, while 116 patients (40.0%) were hospitalized for ≤5 days. The complete demographic and clinical profiles of the participants are detailed in Table 1.
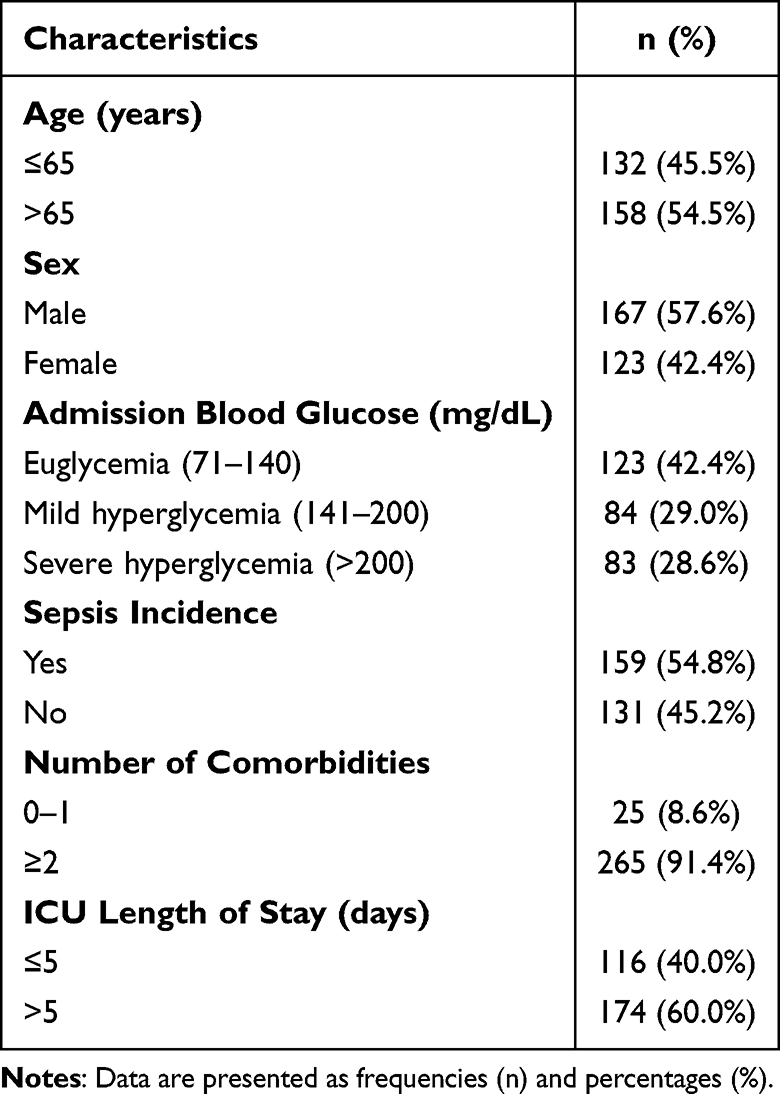 |
Table 1 Demographic and Clinical Characteristics of the Study Participants (n = 290) |
Association Between Admission Blood Glucose and Sepsis Incidence
Initial bivariate analysis demonstrated a robust, statistically significant association between admission blood glucose categories and the subsequent development of sepsis (χ2 = 34.634; p < 0.001). A compelling clinical trend was observed, wherein the incidence of sepsis escalated progressively across the metabolic profiles. Specifically, while 46.3% (57/123) of euglycemic patients experienced sepsis, this proportion rose notably to 63.1% (53/84) in the mild hyperglycemia cohort (Crude OR = 1.98; 95% CI: 1.17–3.37), and peaked at 69.9% (58/83) among those presenting with severe hyperglycemia (Crude OR = 2.71; 95% CI: 1.53–4.80). The comprehensive bivariate results, detailed in Table 2, underscore a definitive upward trajectory in sepsis risk that corresponds directly with higher admission blood glucose levels.
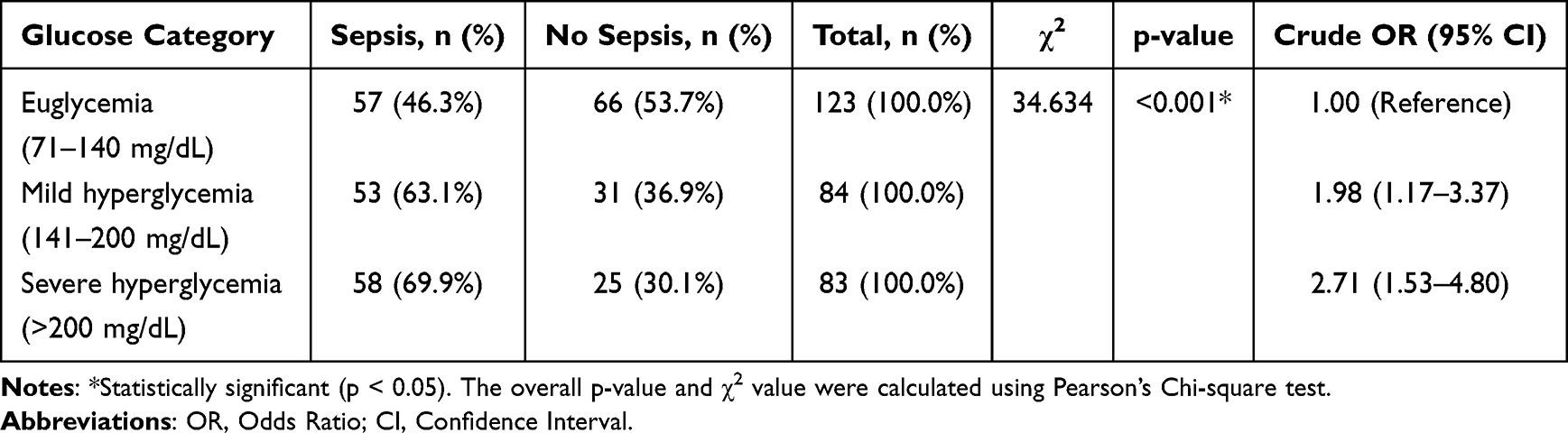 |
Table 2 Bivariate Analysis: Association Between Admission Blood Glucose and Sepsis Incidence |
Clinical Characteristics Based on Sepsis Status
To further elucidate the distinct clinical profiles of patients who developed sepsis versus those who did not, a comprehensive comparative analysis was performed. The sepsis cohort presented with significantly advanced age (mean: 64.8 ± 14.5 years) compared to the non-sepsis group (59.4 ± 15.8 years; p = 0.008). This demographic vulnerability was compounded by a notably higher prevalence of multiple comorbidities (≥2 conditions) among septic patients (95.6% vs. 86.3%; p = 0.008).
Crucially, absolute admission blood glucose levels were profoundly elevated in the sepsis cohort, averaging 178.4 ± 65.3 mg/dL against 138.2 ± 52.1 mg/dL in non-septic patients (p < 0.001). Consistent with this pronounced metabolic instability, a pre-existing diagnosis of diabetes mellitus was more than twice as frequent in the sepsis group (22.0% vs. 9.2%; p = 0.002). Consequently, the compounding clinical burden of sepsis and baseline vulnerabilities translated into a significantly prolonged ICU length of stay, with a median of 6 (IQR: 4–11) days compared to a median of 6 (IQR: 4–10) days for those who remained free of sepsis (p < 0.001). Conversely, there was no statistically significant difference in the distribution of patient sex between the sepsis and non-sepsis groups (57.9% male vs. 57.3% male; p = 0.910), indicating that biological sex did not directly influence the incidence of sepsis in this cohort. A comprehensive comparison of these variables is detailed in Table 3.
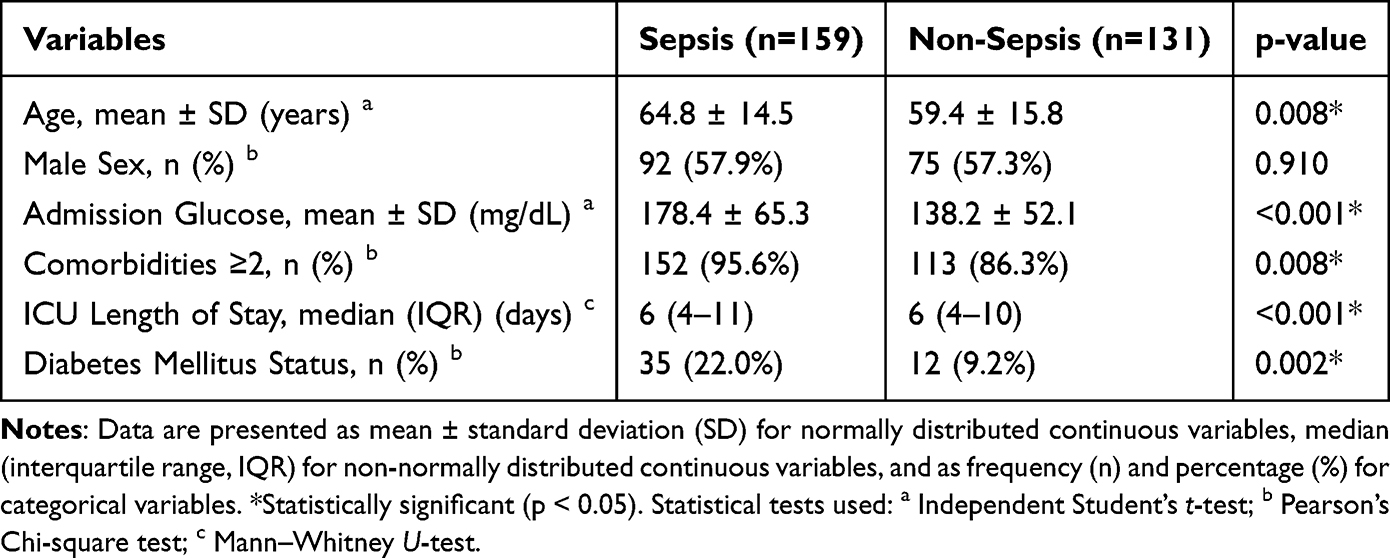 |
Table 3 Comparison of Clinical Characteristics Between Sepsis and Non-Sepsis Groups |
Multivariable Logistic Regression Analysis
In the final multivariable regression model, which systematically adjusted for age, comorbidities, ICU length of stay, baseline diabetes mellitus status, and admission blood glucose categories, severe hyperglycemia emerged as a robust and independent predictor of sepsis. Strikingly, patients presenting with severe admission hyperglycemia (>200 mg/dL) exhibited a 2.54-fold amplified risk of developing sepsis compared to their euglycemic counterparts (Adjusted Odds Ratio [aOR] = 2.54; 95% CI: 1.33–4.85; p = 0.005).
Beyond this acute metabolic derangement, underlying systemic vulnerabilities also significantly compounded the risk profile. Advanced age (>65 years) (aOR = 1.80; 95% CI: 1.10–2.93; p = 0.019) and the concurrent presence of multiple comorbidities (≥2) (aOR = 2.16; 95% CI: 1.28–3.67; p = 0.004) were both identified as significant independent predictors of sepsis incidence.
Conversely, mild hyperglycemia (aOR = 1.37; p = 0.291) and a prolonged ICU stay (>5 days) (aOR = 1.36; 95% CI: 0.81–2.28; p = 0.246) did not reach statistical significance in this rigorously adjusted model. Notably, a pre-existing diagnosis of diabetes mellitus (aOR = 1.52; p = 0.153) also failed to demonstrate an independent predictive effect, underscoring a critical clinical nuance: the acute stress response manifested as severe admission hyperglycemia is a far more critical prognostic indicator for sepsis than chronic glycemic status alone. The comprehensive results of the multivariable analysis are detailed in Table 4.
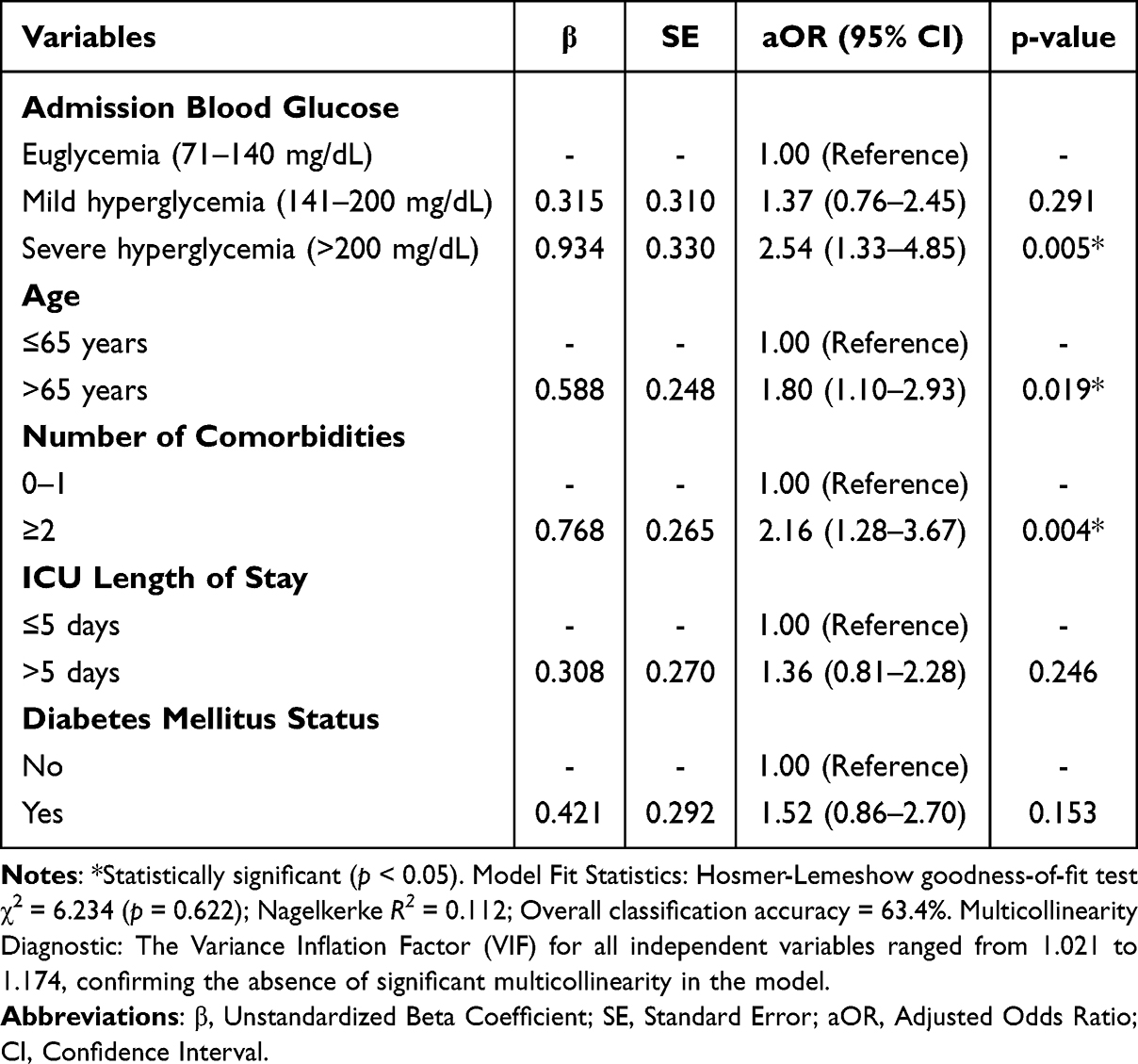 |
Table 4 Multivariable Logistic Regression Analysis for Predictors of Sepsis (n = 290) |
Discussion
Principal Findings
This retrospective cohort study demonstrates that severe admission hyperglycemia is a robust and independent prognostic indicator for sepsis incidence among critically ill ICU patients. Specifically, individuals presenting with severe hyperglycemia (>200 mg/dL) faced a 2.54-fold amplified risk of developing sepsis compared to their euglycemic counterparts. While this magnitude of risk aligns with previously established cohorts in developed nations,10,14 our findings provide crucial, previously scarce empirical evidence from an Indonesian critical care setting. This contextual data is highly valuable, as it underscores the urgent need to establish localized, multidisciplinary critical care pathways adapted to resource-limited environments.
The high overall prevalence of sepsis in our cohort (54.8%) closely mirrors global epidemiological trends, reinforcing that sepsis remains a pervasive and life-threatening complication within the ICU. More strikingly, the incidence of sepsis among patients with severe admission hyperglycemia (69.9%) was starkly elevated compared to those maintaining euglycemia (46.3%). This dramatic disparity highlights the profound clinical impact of acute metabolic derangement on a patient’s susceptibility to severe infections. Consequently, it emphasizes that early metabolic stabilization cannot be viewed in isolation; rather, it requires an integrated approach combining vigilant nursing surveillance, precise medical diagnostics, and prompt nutritional and pharmacological management to mitigate infection risks.
Comparison with Previous Literature
The observed adjusted odds ratio (aOR) of 2.54 for severe hyperglycemia is highly consistent with similar studies conducted across diverse populations. For instance, Goyal et al14 reported a comparable OR of 2.8 in a multicenter Indian cohort, while Chao et al10 identified an OR of 2.35 within an Asian ICU setting. The consistency of this association across different geographic regions and healthcare infrastructures provides compelling evidence that severe hyperglycemia represents a true pathophysiological risk factor for sepsis, rather than merely acting as a surrogate marker for disease severity.15
Conversely, our results indicated that mild hyperglycemia (141–200 mg/dL) lacked a statistically significant independent association with sepsis following rigorous multivariable adjustment. This finding diverges from certain reports in the literature that suggest a linear risk continuum with rising glucose levels. This discrepancy is clinically intriguing and may reflect a specific biological threshold; it implies that admission glucose levels must exceed the 200 mg/dL nadir to induce clinically significant alterations in the host immune response and substantially increase infection susceptibility. Mechanistically, mild elevations in glucose may not be profound enough to overwhelm the host’s endogenous antioxidant defenses or to trigger the massive NF-κB and RAGE pathway activation required to precipitate widespread immune dysfunction. Additionally, while our study utilized guideline-based glycemic stratification for immediate clinical utility, future studies could evaluate admission glucose as a continuous variable using Receiver Operating Characteristic (ROC) curve analysis to identify highly specific, population-based cutoff values and Area Under the Curve (AUC) metrics for sepsis prediction.
Underlying Pathophysiological Mechanisms
The robust association between severe admission hyperglycemia and sepsis observed in our cohort is supported by well-established pathophysiological mechanisms from previous literature. Acute hyperglycemia induces profound immune dysfunction by impairing neutrophil chemotaxis, phagocytosis, and the respiratory burst, thereby diminishing the host’s ability to control bacterial proliferation.16 Furthermore, elevated glucose accelerates the formation of advanced glycation end-products (AGEs), which activates the RAGE pathway and triggers intracellular cascades such as NF-κB. This generates a paradoxical pro-inflammatory milieu characterized by excessive reactive oxygen species (ROS) and cytokines, compounding overall immune exhaustion.8 Concurrently, hyperglycemia-induced protein glycation disrupts endothelial tight junctions, increasing vascular permeability and facilitating bacterial translocation from mucosal barriers.9 These structural alterations are particularly critical during the early phases of ICU admission when patients are most vulnerable to rapid clinical deterioration. Additionally, hyperglycemia shifts the hemostatic balance by increasing von Willebrand factor and depleting protein.17
The Role of Confounding Factors
Our multivariable analysis confirmed that advanced age and the presence of multiple comorbidities are significant independent predictors of sepsis incidence, corroborating established critical care literature. Specifically, age greater than 65 years demonstrated independent prognostic significance (aOR = 1.80, 95% CI: 1.10–2.93, p = 0.019). This aligns seamlessly with the immunosenescence model, wherein elderly populations experience a progressive, age-related decline in the functional capacity of both adaptive and innate immune system components.2,11
This demographic vulnerability is further compounded by a severe clinical burden; notably, 91.4% of the ICU cohort presented with at least one comorbid condition. The accumulation of these underlying diseases (≥2 comorbidities) independently amplified the risk of sepsis (aOR = 2.16, 95% CI: 1.28–3.67, p = 0.004). This finding reinforces the evidence that a high comorbidity burden particularly involving diabetes, hypertension, chronic kidney disease, and cerebrovascular disease diminishes physiological reserve and significantly heightens the patient’s susceptibility to stress-induced infections.12
Interestingly, while a prolonged ICU length of stay (>5 days) is conventionally associated with increased nosocomial infection risk, it did not exhibit a significant independent effect in our rigorously adjusted model. This nuanced finding suggests that the relationship between extended hospitalization and sepsis is likely not strictly causal in this cohort. Rather, it may be mediated by other overarching variables, such as the initial severity of the patient’s critical illness or unobserved cumulative exposures within the ICU environment.
Furthermore, a pre-existing diagnosis of diabetes mellitus did not emerge as an independent predictor of sepsis in our multivariable model. A plausible mechanistic explanation is that patients with known diabetes routinely receive antidiabetic therapies and dietary management, which may precondition their metabolic response and blunt acute, severe glycemic fluctuations under stress.16 This physiological adaptation suggests that the acute stress response manifesting as severe admission hyperglycemia is a far more potent catalyst for immune dysfunction than the chronic glycemic status itself. Additionally, biological sex did not significantly affect sepsis incidence, indicating that the overwhelming systemic inflammation characteristic of critical illness likely overrides potential sex-hormone-mediated immune differences.
Clinical Implications
The findings of this study provide a compelling rationale for integrating routine blood glucose screening into standard ICU triage and admission protocols for all patients, irrespective of their prior diabetic status. Identifying severe admission hyperglycemia (>200 mg/dL) as a high-risk marker allows for the immediate activation of a multidisciplinary clinical pathway aimed at early sepsis prevention. In this collaborative model, the role of critical care nurses is pivotal; they serve as the first line of surveillance, identifying metabolic triggers and escalating clinical vigilance through rigorous temperature monitoring and the meticulous inspection of invasive sites. This early warning system enables physicians to initiate targeted empirical antimicrobial therapy more promptly when sepsis is suspected, thereby reducing the risk of clinical deterioration.
Optimizing clinical outcomes in these high-risk patients further necessitates a coordinated interdisciplinary approach to glycemic management. Effective care coordination between intensivists, clinical pharmacists, and dietitians is essential to maintain blood glucose within the evidence-based target range of 140–180 mg/dL.18 Within this team-based framework, clinical pharmacists play a critical role in the precise titration of insulin protocols to avoid the paradoxical risks of severe hypoglycemia, while dietitians ensure that nutritional support is tailored to minimize glycemic excursions. As demonstrated by Gunst et al, the timing and method of metabolic intervention are critical components of ICU care.19 By shifting from fragmented care to an integrated multidisciplinary strategy, healthcare teams can more effectively address the biological complexities of hyperglycemia-induced immune dysfunction.
From a public health and policy perspective, utilizing admission hyperglycemia as a prognostic tool is particularly pragmatic for healthcare systems in developing nations like Indonesia. In resource-constrained environments where advanced biomarker diagnostics may be unavailable, blood glucose screening offers a simple, cost-effective, and highly feasible method for early risk stratification.20 Implementing standardized protocols that combine initial glucose monitoring with a comprehensive assessment of age and comorbidity burden allows clinicians to allocate limited critical care resources more efficiently. Ultimately, fostering an interdisciplinary culture that prioritizes early metabolic stabilization and coordinated infection surveillance is a scalable strategy to reduce the sepsis burden and enhance patient survival rates across diverse clinical settings.13
Study Limitations
Several limitations should be considered when interpreting these findings. Primarily, the retrospective, single-center design derived from a 12-bed ICU at Advent Hospital Bandung inherently limits the generalizability of our results to other institutions or diverse geographic regions with differing healthcare infrastructures.21 Furthermore, the reliance on secondary data necessitated the exclusion of patients with incomplete medical records, which carries an inherent risk of selection bias, particularly if missing documentation correlated with the patients’ clinical outcomes. Diagnostically, sepsis was determined through the subjective clinical assessments of attending physicians rather than standardized, objective criteria such as the Sepsis-3 SOFA score. Furthermore, we were unable to retrospectively calculate simplified physiological alternatives, such as the quick SOFA (qSOFA) score. This limitation arose because the routine secondary EMR data lacked consistent, time-stamped documentation of specific physiological parameters (such as the exact Glasgow Coma Scale and respiratory rate) at the precise moment of suspected sepsis onset. Consequently, this reliance on clinical judgment potentially introduces diagnostic variability and misclassification bias.22
Regarding clinical and metabolic measurements, blood glucose levels were solely assessed at admission, precluding the evaluation of intra-hospital glycemic variability, which is well-documented to correlate strongly with adverse critical care outcomes. Additionally, our institutional EMR documentation practices did not systematically capture specific inflammatory biomarkers (eg., procalcitonin or serial lactate), validated illness severity scores (such as APACHE II), or baseline nutritional indicators like albumin levels.23 Moreover, from an analytical perspective, the multivariable logistic regression model yielded a relatively low Nagelkerke R2 value (0.112). This indicates that while admission hyperglycemia and multiple comorbidities are significant predictors, sepsis remains a highly complex, multifactorial syndrome, and our model does not capture all potential contributing variables (eg., specific pathogenic strains or exact timing of initial interventions). Finally, although we adjusted for a prior history of diabetes in our model, we did not perform a detailed subgroup analysis stratified by diabetes status. This omission was due to sample size constraints within the diabetic subgroup, which would have limited the statistical power to detect distinct prognostic differences. Nevertheless, to rigorously mitigate these methodological constraints, our multivariable analysis successfully incorporated robust, widely accepted proxy indicators for clinical severity namely advanced age, multiple comorbidities, and prolonged ICU length of stay. The inclusion of these comprehensive covariates ensures the reliability and validity of our adjusted prognostic findings.
Multidisciplinary Applicability
The findings of this study possess direct clinical relevance for healthcare professionals across a multidisciplinary critical care team. To effectively translate these findings into clinical practice and mitigate sepsis risk, a structured approach with a clear division of responsibilities is essential. Intensivists and endocrinologists are responsible for establishing individualized glycemic targets and prescribing dynamic, protocol-driven insulin therapies based on admission glucose levels. ICU nurses play a pivotal role in the continuous, real-time monitoring of blood glucose levels, administering timely insulin corrections, and acting as the primary observers for early clinical signs of systemic deterioration. Simultaneously, clinical pharmacists are tasked with meticulously reviewing medication regimens to prevent drug-induced dysglycemia and optimizing antimicrobial dosages based on the patient’s metabolic state. Finally, clinical dietitians must design highly calibrated enteral or parenteral nutrition plans that synchronize precisely with insulin administration to avoid both severe glycemic spikes and iatrogenic hypoglycemia. This synergistic division of labor ensures comprehensive, round-the-clock metabolic control. While this study successfully establishes admission hyperglycemia as a significant predictor for the incidence of sepsis, its direct impact on definitive prognostic outcomes remains an area for further exploration. Although our data indicates a significant association with prolonged ICU length of stay a recognized proxy for clinical burden future longitudinal studies are highly warranted to investigate whether early dysglycemia directly correlates with harder prognostic endpoints in septic patients, such as 28-day mortality, the requirement for mechanical ventilation, or the progression of multi-organ failure.
Conclusion
In conclusion, this study demonstrates that severe admission hyperglycemia (>200 mg/dL) serves as a robust and independent prognostic indicator of sepsis incidence in critically ill patients. The observed 2.54-fold increased risk which persists after rigorous adjustment for age, comorbidity burden, and baseline diabetes status highlights that acute metabolic derangement is a critical, modifiable clinical marker. These findings underscore that the early identification of admission hyperglycemia provides a vital window for risk-stratified interventions, potentially mitigating the sepsis burden and improving clinical outcomes within the intensive care environment.
Consequently, routine blood glucose screening should be integrated into standardized ICU triage protocols to facilitate rapid clinical decision-making. The implementation of a coordinated, multidisciplinary management strategy integrating the specialized roles of physicians, critical care nurses, clinical pharmacists, and dietitians is essential to optimize glycemic control and enhance patient survival, particularly in resource-limited settings. Future prospective, multicenter research utilizing standardized Sepsis-3 criteria is warranted to validate these findings and inform the development of national guidelines for integrated metabolic and infectious disease surveillance in Indonesia. Furthermore, while these findings provide a foundational framework for critical care management, it is necessary for future prospective studies to evaluate these conclusions across various clinical subgroups. Specifically, targeted analyses evaluating patients with highly severe baseline conditions stratified by validated illness severity scores are imperative to tailor and individualize metabolic interventions more precisely. Additionally, future prospective studies should incorporate easily accessible hematological inflammatory markers derived from routine blood tests, such as the Neutrophil-to-Lymphocyte Ratio (NLR), to further correlate admission glycemic status with the magnitude of the systemic inflammatory response.
Ethics Statement
This study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Ethical approval for this retrospective study was granted by the Health Research Ethics Committee of Universitas Advent Indonesia (Approval Number: 543/KEPK-FIK.UNAI/EC/XII/25; Date of Approval: December 4, 2025). Furthermore, we confirm that all data were extracted after ethical approval was officially granted. Institutional permission to access and utilize the patient medical records was formally granted by the dataset owner, the Administrative Committee of Advent Hospital Bandung (Decision No. 2025-1059), where the first author is concurrently employed as clinical staff. The requirement for written informed consent was formally waived by the Ethics Committee. This exemption was granted because the study involved the secondary analysis of pre-existing medical records, posed no more than minimal risk to participants, and did not adversely affect patient rights or clinical care. To ensure strict confidentiality and comply with institutional privacy policies, all patient data were meticulously anonymized and de-identified prior to analysis.
Acknowledgments
The authors would like to express their sincere gratitude to Advent Hospital Bandung for granting permission to conduct this research and providing access to patient data. We also thank all the ICU clinical staff who assisted in the data collection process. This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6.RKT/HK.07.00/2025).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The conduct of this research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors, as the study was conducted as part of a master’s thesis program in Critical Care Nursing at Universitas Padjadjaran. The Article Processing Charge (APC) for publication was supported by the institutional grant detailed in the Acknowledgments section.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the global burden of disease study. Lancet. 2020;395(10219):200–12. doi:10.1016/S0140-6736(19)32989-7
2. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi:10.1007/s00134-021-06506-y
3. Lu Z, Tao G, Sun X, et al. Association of blood glucose level and glycemic variability with mortality in sepsis patients during icu hospitalization. Front Public Health. 2022;10:857368. doi:10.3389/fpubh.2022.857368
4. Charoenngam N, Alexanian SM, Apovian CM, Holick MF. Association between hyperglycemia at hospital presentation and hospital outcomes in covid-19 patients with and without type 2 diabetes: a retrospective cohort study of hospitalized inner-city covid-19 patients. Nutrients. 2021;13(7):2199. doi:10.3390/nu13072199
5. Mondal S, DasGupta R, Lodh M, et al. Stress hyperglycemia ratio, rather than admission blood glucose, predicts in-hospital mortality and adverse outcomes in moderate-to severe COVID-19 patients, irrespective of pre-existing glycemic status. Diabet Res Clin Pract. 2022;190(April):109974. doi:10.1016/j.diabres.2022.109974
6. Krinsley JS, Maurer P, Holewinski S, et al. Glucose control, diabetes status, and mortality in critically ill patients: the continuum from intensive care unit admission to hospital discharge. Mayo Clin Proc. 2017;92(7):1019–1029. doi:10.1016/j.mayocp.2017.04.015
7. Marik P, Bellomo R, Marik PE. (2013). Stress hyperglycemia: an essential survival response. Critical Care. 2013;17:305
8. Hadzi-Petrushev N, Angelovski M, Mladenov M. Advanced glycation end products and diabetes. Contemp Endocrinol. 2023. doi:10.1007/978-3-031-39721-9_5
9. Ince C, Mayeux PR, Nguyen T, et al. The endothelium in sepsis. Shock. 2016;45(3):259–270. doi:10.1097/SHK.0000000000000473
10. Chao WC, Tseng CH, Wu CL, Shih SJ, Yi CY, Chan MC. Higher glycemic variability within the first day of ICU admission is associated with increased 30-day mortality in ICU patients with sepsis. Ann Intensive Care. 2020;10(1):17. doi:10.1186/S13613-020-0635-3
11. Agorastos A, Chrousos GP. The neuroendocrinology of stress: the stress-related continuum of chronic disease development. Mol Psychiatry. 2022;27(1):502–513. doi:10.1038/s41380-021-01224-9
12. Akinosoglou K, Kapsokosta G, Mouktaroudi M, et al. Diabetes on sepsis outcomes in non-ICU patients: a cohort study and review of the literature. J Diabetes Complications. 2021;35(1):107765.
13. PERKENI. Tatalaksana Pasien Dengan Hiperglikemia Di Rumah Sakit. 2022;37.
14. Goyal A, Gupta S, Gupta Y, Tandon N. Proposed guidelines for screening of hyperglycemia in patients hospitalized with COVID-19 in low resource settings. Diabetes Metab Syndr Clin Res Rev. 2020;14(5):753–756. doi:10.1016/j.dsx.2020.05.039
15. Song G, Liu X, Lu Z, et al. Relationship between stress hyperglycaemic ratio (SHR) and critical illness: a systematic review. Cardiovasc Diabetol. 2025;24(1). doi:10.1186/s12933-025-02751-3
16. van Vught LA, Scicluna BP, Hoogendijk AJ, et al. Association of diabetes and diabetes treatment with the host response in critically ill sepsis patients. Crit Care. 2016;20(1):1–15. doi:10.1186/s13054-016-1429-8
17. Ma H, Qian X, Song X, et al. Identifying early blood glucose trajectories in sepsis linked to distinct long-term outcomes: a K-means clustering study with external validation. Front Immunol. 2025;16:1610519. doi:10.3389/fimmu.2025.1610519
18. Singer P, Blaser AR, Berger MM, et al. ESPEN practical and partially revised guideline: clinical nutrition in the intensive care unit. Clin Nutr. 2023;42(9):1671–1689. doi:10.1016/j.clnu.2023.07.011
19. Gunst J, Debaveye Y, Güiza F, et al. Tight blood-glucose control without early parenteral nutrition in the ICU. N Engl J Med. 2023;389(13):1180–1190. doi:10.1056/nejmoa2304855
20. Purba AKR, Mariana N, Aliska G, et al. The burden and costs of sepsis and reimbursement of its treatment in a developing country: an observational study on focal infections in Indonesia. Int J Infect Dis. 2020;96:211–218. doi:10.1016/j.ijid.2020.04.075
21. Andriani IJS. The blood glucose regulation in Intensive Care Unit (ICU). J Komplikasi Anestesi. 2023;10(3):82–103. doi:10.22146/jka.v10i3.12390
22. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
23. Jiang N, Xie W, Wang D, Wang W. Early appropriate therapy with polymyxin B reduces the mortality in burn sepsis caused by carbapenem-resistant gram-negative bacteria: a retrospective analysis. Eur J Clin Microbiol Infect Dis. 2025;1–10.
24. Rhodes A, Evans L, Alhazzani W. Guía internacional para el manejo de la sepsis y el shock séptico. Care Med. 2017;45(3):486–552.
25. Plummer MP, Finnis ME, Phillips LK, et al. Stress induced hyperglycemia and the subsequent risk of type 2 diabetes in survivors of critical illness. PLoS One. 2016;11(11):1–12. doi:10.1371/journal.pone.0165923
26. Singh M, Upreti V, Singh Y, Kannapur AS, Nakra M, Kotwal N. Effect of glycemic variability on mortality in ICU settings: a prospective observational study. Indian J Endocrinol Metab. 2018;22(5):632–635. doi:10.4103/ijem.IJEM_11_18
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nonlinear Association Between Calculated Globulin Levels and 28-Day Mortality in Patients with Sepsis: A Retrospective Cohort Study
She X, Zhao X, Yang H, Cui X
Risk Management and Healthcare Policy 2025, 18:2743-2757
Published Date: 20 August 2025