Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 17
Integrated Endodontic and Restorative Management of C-Shaped Canals with Severe Coronal Loss in Mandibular Second Molar: A Case Report
Authors Nagadi E, Muryani A ![]() , Adang RAF
, Adang RAF
Received 16 November 2024
Accepted for publication 29 January 2025
Published 14 February 2025 Volume 2025:17 Pages 121—134
DOI https://doi.org/10.2147/CCIDE.S506763
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Eddie Nagadi, Anna Muryani, Rahmi Alma Farah Adang
Department of Conservative Dentistry, Faculty of Dentistry, Universitas Padjadjaran, Bandung, Indonesia
Correspondence: Anna Muryani, Department of Conservative Dentistry, Universitas Padjadjaran, Jl. Sekeloa Selatan 1, Bandung, Indonesia, Tel +62 896 19972132, Email [email protected]
Abstract: This case report describes the endodontic treatment of a lower right second molar with a C-shaped root canal in a 49-year-old woman exhibiting severe loss of coronal structure. Clinical examination revealed a cavity with temporary filling on tooth 47, which tested negative to cold stimuli but was positive to percussion and bite tests. Cone beam computed tomography (CBCT) scan revealed a C-shaped canal morphology with associated periapical radiolucency, graded as CBCT-PAI score 4. The canal was classified as C3 subdivision III (Melton et al), C3 type II (Fan et al), and 2 47 M2− 2D2− 1 (Ahmed et al’s). A non-surgical endodontic procedure was performed using metallurgically gold heat-treated files, passive ultrasonic irrigation, and warm hydraulic condensation obturation. Post-endodontic restoration included a post and core build-up with the wallpapering technique and a zirconia overlay. This case highlights the importance of CBCT imaging for diagnosis and treatment planning, careful selection of endodontic instruments and technique, and the use of advanced restoration methods to improve the outcome of challenging C-shaped canal treatments with extensive cavity involvement.
Keywords: endodontic, C-shaped canal, cone-beam computed tomography, wallpapering, zirconia, overlay
Introduction
The C-shaped canal is a morphological deviation of the root canal system predominantly observed in mandibular second molars. The C-shaped canal configuration was initially described in the field of endodontics by Cooke and Cox in 1979.1 This type of canal is named after its cross-sectional shape, which resembles a single ribbon-shaped orifice that forms a continuous arc. Typically, it begins at the mesiolingual line angle and extends buccally, ending at the distal aspect of the pulp chamber. The occurrence of C-shaped root canals varies considerably among different populations and types of teeth. The presence of these canals is predominantly observed in mandibular second molars (2.7–45.5%), with a larger occurrence in Asian populations in comparison to Europeans and Americans. Research suggests that there is a pattern of growing occurrence of this phenomenon from Northeast Africa to East Asian countries like China (0.6–41.27%) and Korea (31.3–45.5%), following a west-to-east gradient. Additionally, data indicates that C-shaped canals are not exclusive to mandibular second molars, but can also be observed in maxillary first molars (0.12%) and mandibular third molars (3.5–4.4%).2 The formation of the C-shaped root canal is attributed to the incomplete fusion of the Hertwig’s epithelial root sheath on either the buccal or lingual surface of the root. This failure leads to the development of a root that has a C-shaped structure, consistently including a C-shaped canal. In addition, the merging of roots caused by the accumulation of cementum over a period of time can also contribute to this particular form. The main anatomical characteristic of C-shaped canals is the existence of fin or web that connects the various root canals. Usually, teeth with this canal design have roots that are joined together on the outside or inner side, resulting in an intricate internal structure. The canal system, which is shaped like the letter C, can have various changes throughout the root, making it difficult to accurately determine its exact configuration based solely on its shape at the opening. C-shaped root canals often have a high likelihood of dividing into two or three canals in the lower part of the root.3–5
The categorization of C-shaped canals has undergone substantial changes since its initial proposal. Melton et al introduced a categorization system for C-shaped canals, which is determined by their cross-sectional configuration. Category I refers to a canal that is shaped like the letter C and runs continuously from the pulp chamber to the apex, without any separation (C1). Category II is characterized by a semicolon-shaped opening, where dentine divides a primary C-shaped canal from a separate mesial canal (C2). Category III consists of cases with two or more distinct canals, which can be further classified into three groups: subdivision I, where a C-shaped opening in the upper third of the tooth divides into separate canals that join together at the apex; subdivision II, where a C-shaped opening in the upper third of the tooth splits into separate canals from the middle of the root to the apex; and subdivision III, where a C-shaped opening divides into separate canals from the upper third of the tooth all the way to the apex (C3). In 2004, Fan et al enhanced and perfected Melton’s categorization by adopting a more comprehensive approach that incorporated both anatomical and radiographic characteristics, so overcoming the limitations of Melton’s system. The classification of Fan et al consists of five distinct types (Figures 1 and 2). Category I (C1) is characterized by a continuous “C” form without separation (Figure 1A). Category II (C2) is similar to a semicolon since it has a break in the contour of the letter “C” and the angles are at least 60° (Figures 1B and 2A). Category III (C3) comprises two or three distinct canals, each with angles that are both smaller than 60° (Figures 1C and 2B). Category IV (C4) is characterized by a solitary circular or oval passage in its cross-section, usually located close to the tip (Figure 1D). In contrast, Category V (C5) does not exhibit any discernible canal opening, frequently at the apex (Figure 1E).
 |
Figure 1 The categorization of C-shaped canal configuration. (A) Continuous “C” shape without separation. (B) Semicolon-like shape with a break and angles ≥ 60°. (C) Two or three distinct canals with angles < 60°. (D) Single circular or oval passage near the tip. (E) No visible canal opening, often at the apex. Reprinted from J Endod. Volume 33(5), Jafarzadeh H, Wu YN. The C-shaped Root Canal Configuration: A Review. 517–23, Copyright 2007, with permission from Elsevier.3 |
 |
Figure 2 Angle measurement for the C2 canal (left) and C3 canal (right). (A) Angle β exceeds 60°, angle α smaller than 60°. (B) Both angle α and angle β are smaller than 60°. Reprinted from J Endod. Volume 33(5), Jafarzadeh H, Wu YN. The C-shaped Root Canal Configuration: A Review. 517–23, Copyright 2007, with permission from Elsevier.3 |
They highlighted that the C-shaped opening frequently links through a narrow passage and that the shape of the canal might differ along the root, rendering clinical crown morphology or orifice appearance ineffective indicators of the true canal structure. In their study, Fan et al used radiographic imaging to categorize C-shaped roots into three types: Type I (Figure 3A), where the mesial and distal canals merge before reaching the apical foramen; Type II (Figure 3B), where the canals maintain separate pathways to the apex; and Type III (Figure 3C), where one canal curves and overlaps with a longitudinal radiolucent line while the other canal continues independently to the apex. The historical development of classification in this field demonstrates a growing comprehension of the intricate anatomical features and the need for exact diagnostic criteria in endodontic treatment.3–5
 |
Figure 3 Classification of C-shaped roots using radiographic imaging. (A) Mesial and distal canals merge before the apical foramen. (B) Canals maintain separate pathways to the apex. (C) One canal curves and overlaps with a radiolucent line, while the other continues independently to the apex. Reprinted from J Endod. Volume 33(5), Jafarzadeh H, Wu YN. The C-shaped Root Canal Configuration: A Review. 517–23, Copyright 2007, with permission from Elsevier.3 |
In 2017, Ahmed et al introduced a new coding system aimed at offering a more precise and comprehensive classification of root canals. The updated system integrates comprehensive data on tooth notation, root count, and distinct characteristics of root canal designs into a unified code, thereby improving its usefulness in both clinical and research environments (Figure 4). The Ahmed et al system has shown to be superior to the Fan et al system in accurately categorizing single-rooted teeth with intricate canal structure, multi-rooted premolars, and molars. The integration of modern 3D imaging techniques, like as cone-beam computed tomography (CBCT) and micro-computed tomography (micro-CT), in this system enables more accurate and practical assessments of root and canal morphology.6
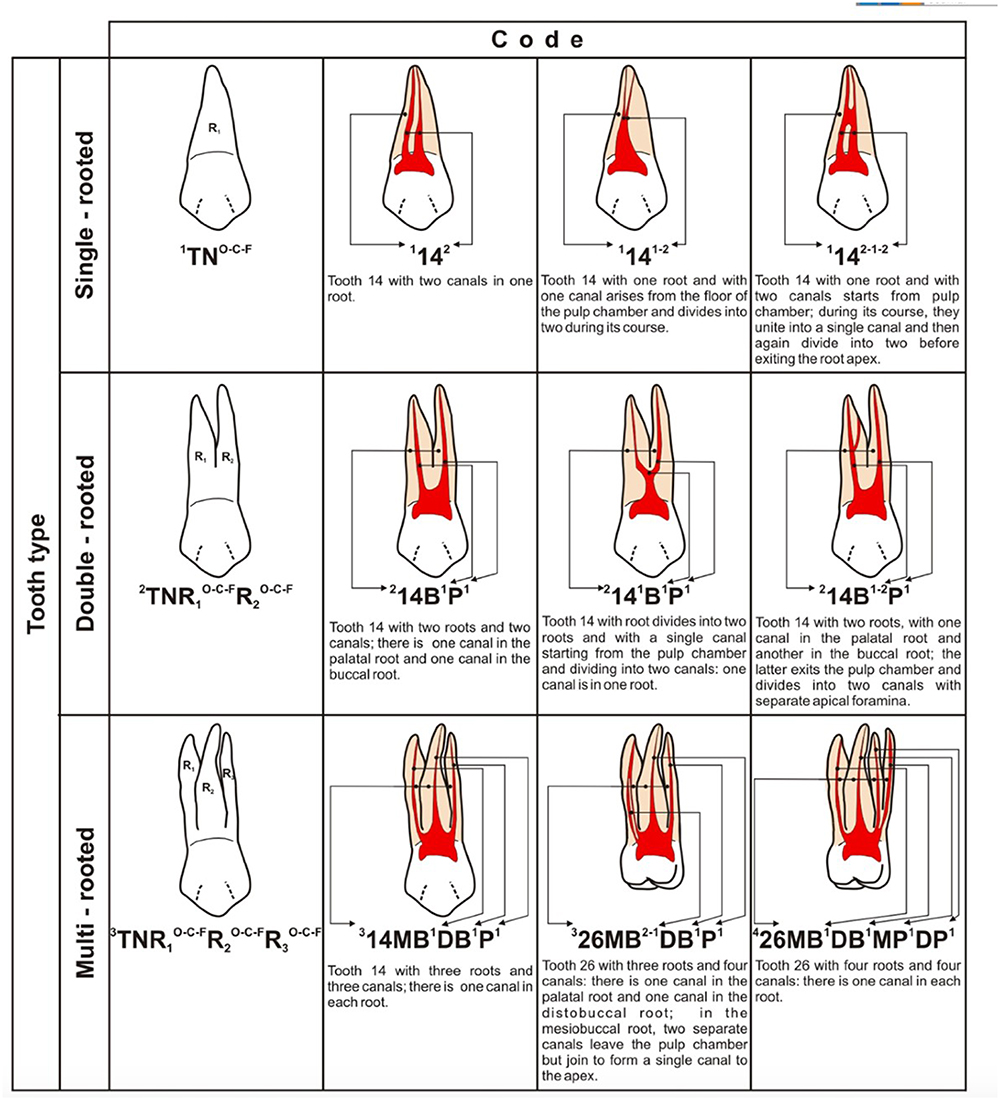 |
Figure 4 Application of Ahmed et al classification system. Reprinted from Ahmed HMA, Rossi-Fedele G, Dummer PMH. Critical analysis of a new system to classify root and canal morphology — a systematic review. Aust Endod J. 2023;49:750–768. © 2023 The Authors. Australian Endodontic Journal published by John Wiley & Sons Australia, Ltd on behalf of Australian Society of Endodontology Inc.6 |
Endodontic treatment of C-shaped canals is challenging due to their intricate anatomical structure. The complex architecture of the structure can ensnare residual soft tissue or contaminated material, so impeding the attainment of comprehensive cleansing and filling. In addition, the presence of fins and webs that connect the canals adds complexity to the processes of instrumentation and obturation. In order to properly deal with these intricacies, endodontists frequently have to adapt their methods and employ sophisticated imaging technologies. CBCT is essential in improving the handling of endodontic patients, especially those that involve intricate anatomical features like C-shaped canals. CBCT offers high-resolution, three-dimensional images that enable a thorough evaluation of the root canal system, making it easier to identify complex structures and variations that are sometimes overlooked with conventional radiography. This state-of-the-art imaging technology enhances the accuracy of diagnosing, planning treatment, and performing endodontic procedures by providing a good view of the canal structure, resulting in improved outcomes for endodontic treatments.5,7,8
Ensuring the long-term success of root canal therapy relies heavily on the proper restoration of endodontically treated teeth. Endodontically treated teeth are more prone to fractures as a result of the depletion of natural tooth structure and the inherent vulnerabilities that arise from the treatment procedure. Research has shown that the utilization of fiber-reinforced composites greatly improves the ability of these teeth to withstand fractures, resulting in improved support and distribution of biting forces. This strengthening is crucial for preserving the integrity of the remaining tooth structure and preventing severe failures. Furthermore, the implementation of modern methods like the wallpapering technique, which entails using polyethylene fiber tape to line the cavity walls, has demonstrated its capacity to enhance the bond strength and stress distribution. This, in turn, improves the overall durability and duration of the restoration, as supported by studies.9–11
Zirconia overlays are a cutting-edge option for repairing teeth that have undergone endodontic treatment. They provide notable benefits in terms of strength, minimal invasiveness, visual appeal, and long-lasting performance. Zirconia, a ceramic material known for its superior mechanical features such as high fracture toughness and flexural strength, is highly valued for its ability to withstand the occlusal stresses applied to posterior teeth. Utilizing zirconia in an overlay design is advantageous as it allows for the preservation of a greater portion of the original tooth structure when compared to conventional full-coverage crowns. This helps to retain the vitality of the tooth and minimizes the likelihood of additional structural damage. Zirconia overlays offer the advantage of superior marginal adaptation and seal, which is essential for minimizing microleakage and secondary caries. Moreover, the biocompatibility of zirconia guarantees that the restoration is easily accepted by the nearby gingival tissues, hence reducing the likelihood of any negative responses. Zirconia possesses esthetic qualities that closely resemble the translucency and color of natural teeth, making it a highly appealing choice for restorations in both the front and back areas of the mouth. In addition, the utilization of sophisticated adhesive techniques in combination with zirconia overlays amplifies the adhesive force between the restoration and the tooth, hence enhancing the overall durability and effectiveness of the restoration.12,13
Case Report
A 49-year-old woman visited the Dental Hospital of Universitas Padjadjaran due to a decaying tooth in the lower right back area, which was causing pain when chewing. Prior to this visit, the patient had sought treatment from a general dentist who applied a temporary filling to the afflicted tooth (Figure 5A). The patient was referred because of C-shaped appearance in the pulp chamber and significant structural damage to the crown. The clinical examination indicated a large cavity on tooth 47, characterized by the negativity to cold test but positivity to percussion and biting tests. The periapical radiographic imaging reveals a radiopaque appearance that resembles restorative material on the crown. There is also extensive radiolucency on the crown, which extends to the pulp and multiple roots. Additionally, there is disruption of the periodontal membrane and lamina dura. However, no abnormalities are observed at the alveolar crest and periapical area (Figure 5B).
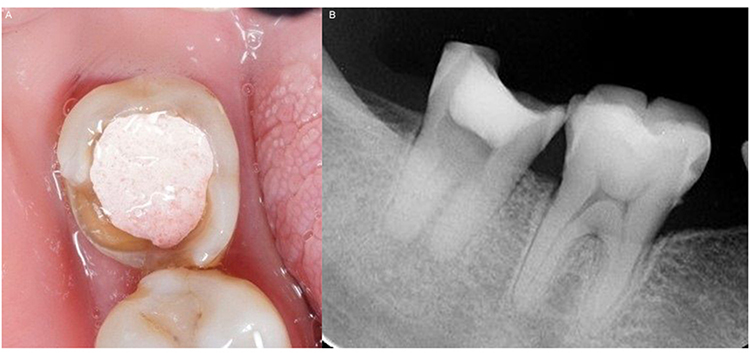 |
Figure 5 (A) A photograph depicting the clinical presentation during the initial examination; (B) Diagnostic periapical radiograph image. (Source: personal documentation). |
In addition, the CBCT examination provided detailed information about the structure of tooth 47, which consists of two roots and four root canals, arranged in a C-shaped configuration. The distal root contains two root canals, while the mesial root also contains two root canals. The distal root possesses a single apical foramen, whereas the mesial root contains two apical foramina (Figure 6A–D). The CBCT scan revealed a radiolucent area at the apex of the tooth, measuring 5.88 mm in diameter (Figure 7A). According to the interpretation of the CBCT, the classification of the C-shaped canal can be categorized as class C3 Subdivision III according to Melton et al and as C3 Type II according to Fan et al. According to Ahmed et al’s categorization, the root and canal morphology is categorized as 247 M2−2D2−1. The radiolucency has a periapical score of 4 as determined by the CBCT-PAI score (Figure 7B).
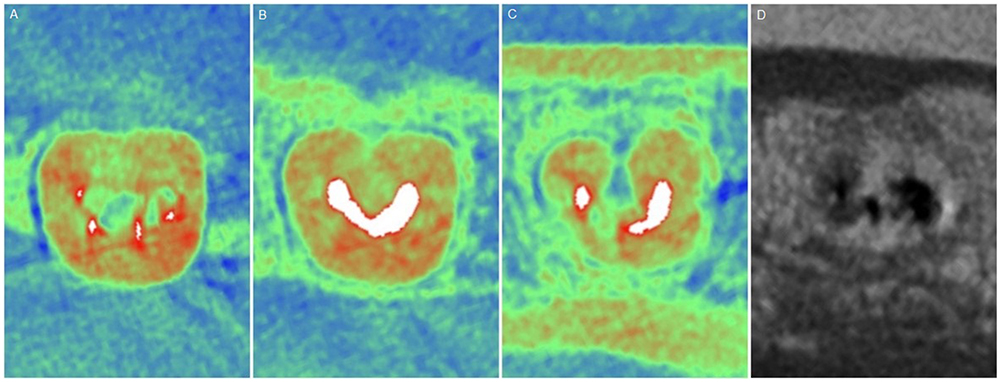 |
Figure 6 Axial view of the CBCT examination of tooth 47. (A) Cross-section at the Cementoenamel Junction (CEJ) shows 4 root canal orifices; (B) cervical third shows a continuous C-shaped canal; (C) middle third shows a semicolon shape; (D) apical section shows 2 apical foramina in the mesial root and 1 apical foramen in the distal root. (Source: personal documentation). |
 |
Figure 7 Pre-operative CBCT radiolucency image at the apex of tooth 47. (A) The coronal view shows a radiolucency diameter at the apex of tooth 47 measuring 5.88 mm; (B) The axial view of the periapical lesion on the CBCT shows no evidence of bone expansion or destruction. (Source: personal documentation). |
According to the diagnostic criteria of the American Association of Endodontists (AAE), the diagnosis for this case is previously initiated therapy with symptomatic apical periodontitis of tooth 47, based on the clinical and radiographic examination data. Non-surgical root canal treatment was performed at tooth 47, which involved removing decay and accessing the cavity (Figure 8A), determining the length of the root canal with an electronic apex locator (Figure 8B), cleaning and shaping the root canal (Figure 8C–E), applying medication within the canal, and obturating the root canal (Figures 8F and 9).
 |
Figure 8 The endodontic treatment process for tooth 47 involves the following steps: (A) Isolation of the tooth using a rubber dam, removal of decay, and gaining access to the cavity; (B) Negotiating the canals using #6 #8 #10 K-files and determining the working length using an Electronic Apex Locator (EAL); (C) Preparing the root canal using the crown-down technique with specially designed files (Protaper Ultimate, Dentsply Sirona, USA) that have a regressive taper and are heat-treated with gold metallurgy, up to size #30; (D) Cleaning the canal using irrigation solutions of 3% NaOCl, 17% EDTA, and 2% CHX, which are activated using the passive ultrasonic irrigation technique; (E) Drying and examining the root canal morphology after chemomechanical preparation; (F) Placing calcium hydroxide medication inside the canal for a period of 3 weeks. Upon examination, the patient’s symptoms were completely disappeared, and tests involving percussion and biting showed no abnormalities. The obturation procedure utilized the warm hydraulic condensation approach, employing bioceramic sealer (AH Plus Bioceramic Sealer, Dentsply Sirona, USA). (Source: personal documentation). |
 |
Figure 9 Periapical X-ray during the obturation phase of root canal treatment for tooth 47. (A) Master cone fit; (B) Immediate post-obturation; (C) Post-obturation at 1-month recall. (Source: personal documentation). |
After the obturation procedure, the patient was then scheduled for a follow-up assessment one month later. During this evaluation, the root canal filling was examined utilizing CBCT imaging (Figure 10).
 |
Figure 10 Axial CBCT slices to evaluate the hermetic integrity of the root canal filling in a C-shaped canal. (Source: personal documentation). |
Post-endodontic restoration was conducted one month following the follow-up for obturation. The choice of the post was based on the residual wall thickness, which measured only 2 mm in the non-vital tooth. A glass fiber post and polyethylene fiber tape was inserted into the distobuccal root canal. The core build-up was performed utilizing the wallpapering technique, which involved the application of polyethylene fiber tape and short fiber reinforced composite. Following the core build-up, crown preparation was performed with an overlay design using the morphologically driven preparation technique. This involved creating a box-shaped structure on the proximal and part of the buccal surface that had previously been impacted by caries (Figure 11A and B). An intraoral scanner was used to capture an impression, which was then digitally designed utilizing zirconia material for the restoration (Figure 11C).
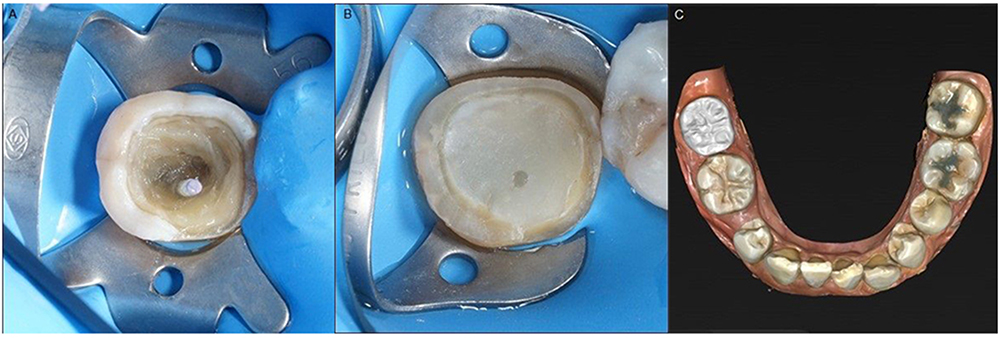 |
Figure 11 Post and Core Buildup Protocol: (A) placement of a glass fiber post into the distobuccal canal (Dentoclic, Itena, France), application of polyethylene fiber tape to the floor and cavity walls using the wallpapering technique. (B) A core buildup with short fiber reinforced composite (Ever X Posterior, GC, Japan) was done, followed by the morphologically driven preparation technique in overlay, including a proximal and buccal box. (C) Digital scanning and designing of the overlay using zirconia material. (Source: personal documentation). |
The cementation process of the zirconia commenced with an intraoral try-in. Subsequently, the zirconia overlay was cleansed using a universal cleaning material. Afterward, the zirconia overlay was subjected to air-particle abrasion and priming methods (Figure 12A–D).
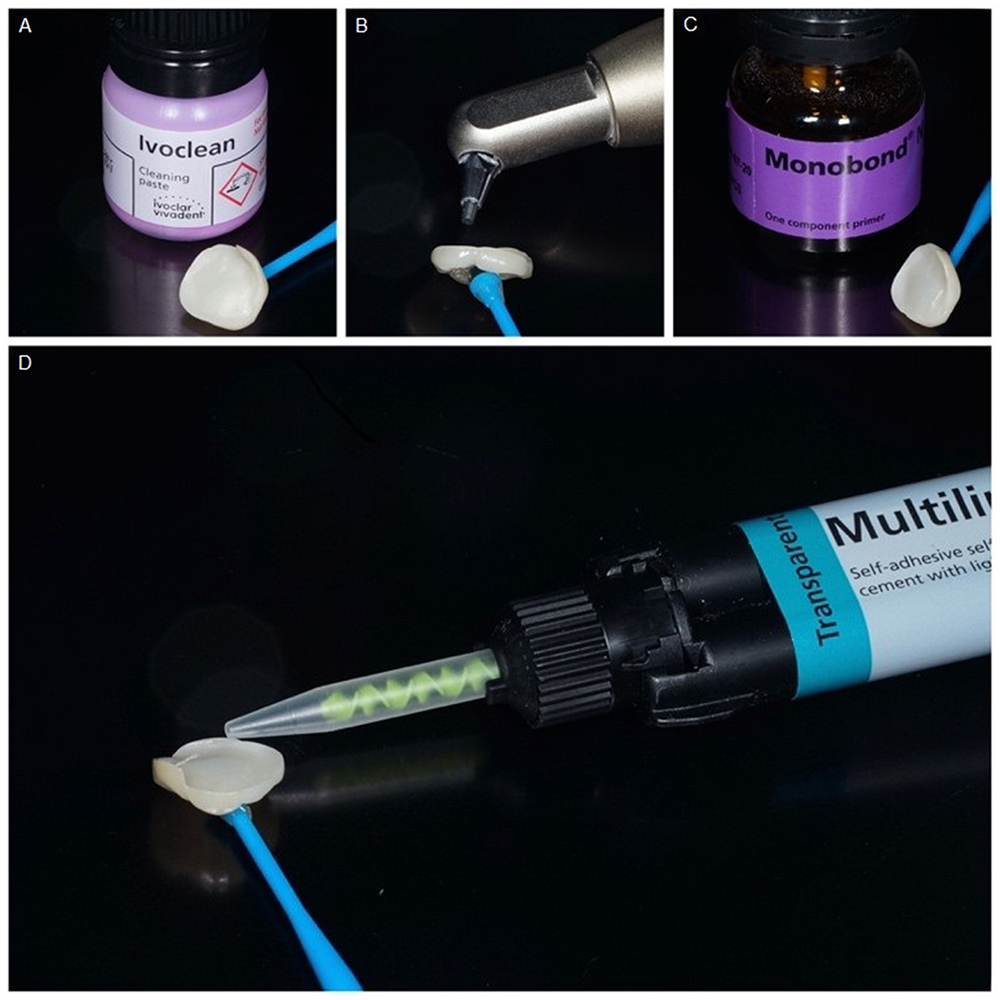 |
Figure 12 Preparation of the Restoration: (A) An intraoral try-in of the zirconia overlay was performed, followed by cleaning with a universal cleaning paste (Ivoclean, Ivoclar Vivadent, Liechtenstein); (B) The bonding surface was sandblasted using air-particle abrasion with 50 µm aluminum oxide and thoroughly rinsed with water spray and dried with oil-free air; (C) A thin coat of primer was applied to the pretreated surfaces with a micro brush for 60 seconds, then any remaining excess was dispersed with a strong stream of air (Monobond N, Ivoclar Vivadent, Liechtenstein); (D) The zirconia overlay was ready to be luted with self-adhesive resin cement (Multilink Speed, Ivoclar Vivadent, Liechtenstein). (Source: personal documentation). |
Tooth 47 was isolated with a rubber dam and cleaned with pumice to eliminate any remaining temporary crown cement. The tooth surface preparation involved three steps: etching with 37% phosphoric acid, followed by applying a primer and adhesive utilizing a two-bottle multimode bonding system (Figure 13A–D). Subsequently, the process of cementation was performed utilizing a self-adhesive resin cement (Figures 12D and 13E). The excess cement was removed, and the occlusion was examined and modified as needed (Figure 13F).
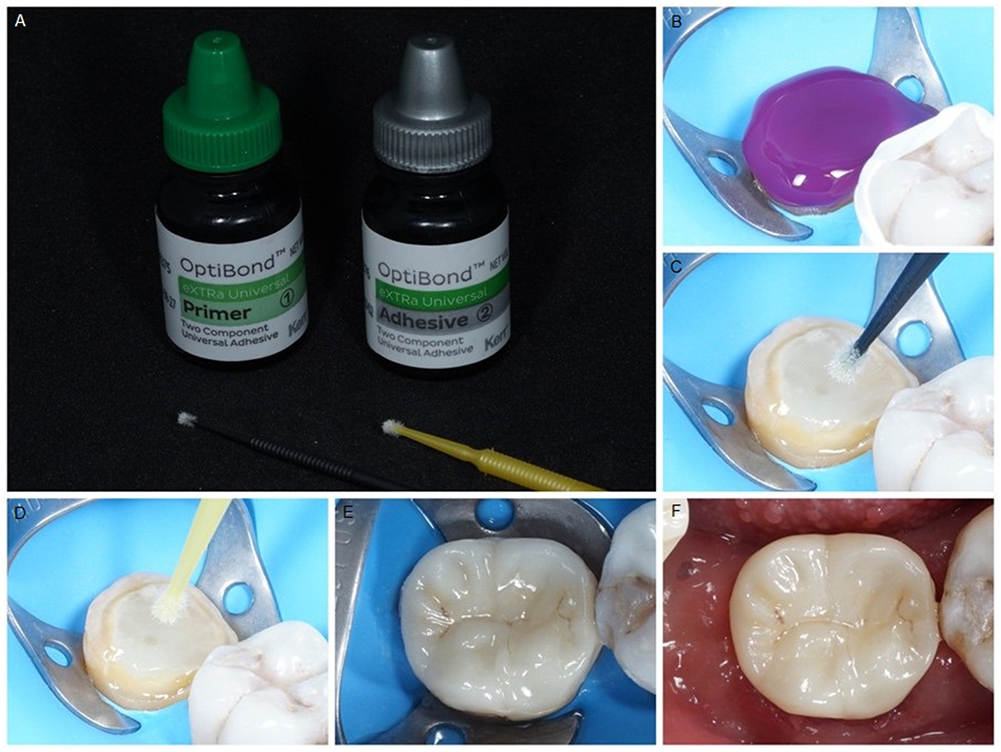 |
Figure 13 Tooth surface preparation using a two-bottle multimode bonding system (Optibond exTRa Universal, Kerr, USA). (A) Primer and adhesive bottles, each with a separate micro brush; (B–D) Tooth 47 was etched with 37% phosphoric acid for 15 seconds, then thoroughly washed and air-dried (Gel Etchant, Kerr, USA). The primer (first bottle) was applied using a micro brush with a scrubbing motion for 20 seconds, followed by air thinning for 5 seconds. The adhesive (second bottle) was then applied with a light brushing motion for 15 seconds, air-thinned for 5 seconds with strong air to prevent adhesive pooling, and light-cured for 10 seconds; (E) The zirconia overlay was cemented using self-adhesive resin cement (Multilink Speed, Ivoclar Vivadent, Liechtenstein); (F) Excess cement was cleaned, and occlusion was checked, with no adjustments needed. (Source: personal documentation). |
After the restoration was cemented, the patient was later asked to come back for a follow-up session. An intraoral radiograph known as a bitewing was obtained to assess the efficacy of the treatment (Figure 14).
 |
Figure 14 Post-restoration bitewing radiograph. (Source: personal documentation). |
The patient conveyed contentment and stated the absence of any grievances. The percussion and biting tests yielded negative results, indicating no inflammation of the gingival tissue. Afterward, the patient received dental health education to guarantee the proper maintenance of oral hygiene.
Discussion
The main objective of root canal therapy is to meticulously shape and cleanse the whole root canal system, followed by the complete filling of the canal with an inert substance.14,15 Failure to address any portion of the canal space can result in ineffective endodontic results. A C-shaped canal is a type of canal that has a continuous slit linking some or all canals in teeth with fused roots. It is defined by its characteristic C-shaped cross-sectional appearance. The primary obstacle associated with C-shaped canals is the existence of an isthmus that connects the different canals, rendering them arduous to thoroughly clean and fully fill.1,5
Identifying C-shaped canals requires the use of both radiographic and clinical assessments. A C-shaped root can be observed in mandibular second molars on radiographs, either as a single fused root or as two separate roots with a connection between them. CBCT is a highly valuable tool for precisely identifying the shape and structure of roots and canals, greatly improving the diagnosis of C-shaped canals.5–8 Research has shown that CBCT offers superior imaging capabilities, which assist in the thorough evaluation and treatment of intricate root canal systems, including C-shaped canals. According to Wang et al, the use of radiography and clinical examination under a microscope together resulted in a higher detection rate (41.27%) of C-shaped canals compared to using radiography alone (34.64%) or clinical examination alone (39.18%).16 The design of the access cavity for teeth with C-shaped root canal systems can vary greatly depending on the pulp morphology of the tooth. In order to avoid any oversight of anomalies, it is advisable to carry out root canal negotiation using small endodontic files, specifically K-files with sizes 6, 8, and 10.
This instance involved identifying the presence of C-shaped canal morphology by examining the square form of the root in the pre-operative periapical radiograph. Previous observations have indicated that roots with a C-shaped canal usually have a conical or square shape.2,5 A cone beam computed tomography (CBCT) scan was arranged, and the findings showed that there were two roots with four root canals, and three apical foramina. Cone beam computed tomography (CBCT) enables the detection of intricate features that are frequently overlooked by conventional radiography, including the presence of apical foramina and periapical lesions. To get optimal results, it is crucial to have a comprehensive comprehension of the CBCT findings. This will enable the precise execution of chemomechanical instrumentation and cleaning of the root canals, enabling thorough access and obturation of all areas inside the root canal system.
Another difficulty in preparing C-shaped root canal systems is the danger areas within these canals. Chai and Thong analyzed and quantified the most constricted areas of the buccal and lingual canal walls in C-shaped mandibular second molars. Researchers found that the average minimum width of the walls of the buccal canal was much larger than that of the lingual canal walls, which are located near the furcation area. In addition, the buccal and lingual walls were shown to be narrowest at the apical and mesial areas. Research has shown that C-shaped root canal systems with thinner lingual walls are more likely to be damaged during shaping and post-canal preparation procedures.17 Therefore, using regressive taper files (Protaper Ultimate, Dentsply Sirona, USA) in this case has several advantages, especially in reducing the risk of unintentional damage in these vulnerable areas. The design of regressive taper files, which gradually reduce in size towards the crown, helps to preserve more dentin and decrease the likelihood of perforation in the thinner canal walls. This design improves the file’s flexibility and responsiveness to the natural anatomy of the canal, making it easier and more efficient to clean and shape the canal more safely. In addition, the gradual decrease in taper helps preserve the strength and stability of the tooth, reducing the chances of developing weak areas that may result in fractures.18
The task of thoroughly cleansing root canals poses considerable difficulty in endodontic therapy, mostly due to the intricate anatomical variances found in C-shaped canals. Hence, it is vital to choose a suitable irrigation method to ensure thorough cleaning and disinfection of all parts of the intricate root canals. This will minimize the chances of reinfection and enhance the overall effectiveness of endodontic treatment. The utilization of passive ultrasonic irrigation (PUI) with NaOCl 3%, EDTA 17%, and CHX 2% in this particular scenario is quite beneficial because of its exceptional cleansing and disinfecting characteristics.19–21 Zou et al have reached an agreement that PUI (passive ultrasonic irrigation) greatly improves the effectiveness of irrigants by creating powerful acoustic streaming and cavitation effects. These effects accelerate the elimination of debris, necrotic tissue, and bacteria from intricate canal structures. Sodium hypochlorite (NaOCl) at a concentration of 3% is effective for disinfection and tissue dissolution. Ethylenediaminetetraacetic acid (EDTA) at a concentration of 17% aids in the process of chelating calcium ions to eliminate the smear layer. Chlorhexidine (CHX) at a concentration of 2% gives long-lasting antibacterial properties. When activated by PUI, this combination effectively cleans and disinfects C-shaped root canals, minimizing the chance of reinfection and enhancing the overall outcome of endodontic therapy.22
The utilization of the warm hydraulic condensation approach in conjunction with a bioceramic sealer offers significant benefits in attaining ideal three-dimensional filling in intricate scenarios, such as C-shaped root canals. This procedure improves the ability of the sealer to conform to the canal walls and the complex anatomy, resulting in a uniform and completely filled space without any gaps. Bioceramic sealers are recognized for their exceptional biocompatibility, antibacterial characteristics, and capacity to adhere to dentin, hence enhancing the long-term efficacy of the treatment.23,24 Applying heat to the hydraulic condensation process ensures that the gutta-percha and sealer spread evenly into all the imperfections in the canal, resulting in a better seal and minimizing the likelihood of microleakage.25,26
Utilizing glass fiber and polyethylene fiber for post-placement in conjunction with the wallpapering approach for core build-up in cases of significant loss of tooth structure on mandibular molars provides numerous benefits, especially when combined with zirconia overlays. The use of fiber-reinforced composites in this circumstance is justified since they improve stress distribution and provide structural reinforcement. Based on the research conducted by Neri et al and Rahmayanti et al, the finite element analysis shows that the utilization of fiber-reinforced composites, particularly through the application of the wallpapering approach, leads to a substantial enhancement in the distribution of stress throughout the tooth structure. This technique decreases the level of tension in susceptible regions, thereby reducing the likelihood of fractures. The use of polyethylene and glass fibers enhances the overall fracture resistance of the repair, hence guaranteeing superior long-term stability and durability.9,10
In addition, the utilization of zirconia overlays enhances this method because zirconia possesses exceptional mechanical characteristics, including high fracture toughness and strength, along with its biocompatibility. Zirconia is not only visually appealing but also offers a resilient repair that can endure the forces exerted during chewing. Utilizing fiber-reinforced composites for the core construction and zirconia for the final restoration offers a strong and dependable alternative for treating teeth with significant loss of the crown.13,27
Conclusion
The case report demonstrates the successful treatment of a challenging C-shaped mandibular second molar with significant coronal loss through advanced endodontic and restorative techniques. Cone-beam computed tomography enabled proper diagnosis and adequate planning for treatment, while the appropriate procedure of cleaning, shaping, and obturation of the complex root canal system was carried out using the modern endodontic techniques. Advanced restoration treatment further strengthened the tooth structure using the wallpapering technique, followed by zirconia overlay. The good clinical outcomes, which include symptom removal and the return of function to normalcy, underscore even more how important advanced endodontic technology is in treating such complex canal configurations. It can safely be inferred from these results that clinicians should incorporate these advanced endodontic treatment modalities for better success of treatment in demanding cases and to ensure long-term durability and better patient outcomes.
Consent Statement
Institutional approval was not required to publish the case report for this retrospective single case report as it did not involve experimental research or animal subjects. Written informed consent for publication of the case details and accompanying images was obtained from the patient.
Funding
This research received no external funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Cooke HG, Cox FL. C-shaped canal configurations in mandibular molars. J Am Dent Assoc. 1979;99(5):836–839. doi:10.14219/jada.archive.1979.0402
2. Seo MS, Park DS. C‐shaped root canals of mandibular second molars in a Korean population: clinical observation and in vitro analysis. Int Endod J. 2004;37(2):139–144. doi:10.1111/j.0143-2885.2004.00772.x
3. Jafarzadeh H, Wu YN. The C-shaped root canal configuration: a review. J Endod. 2007;33(5):517–523. doi:10.1016/j.joen.2007.01.005
4. Fan B, Cheung GSP, Fan M, Gutmann JL, Bian Z. Case report/clinical techniques C-shaped canal system in mandibular second molars: part I-anatomical features. 2004.
5. Kato A, Ziegler A, Higuchi N, Nakata K, Nakamura H, Ohno N. Aetiology, incidence and morphology of the C-shaped root canal system and its impact on clinical endodontics. Int Endodontic J. 2014;47:1012–1033. doi:10.1111/iej.12256
6. Ahmed HMA, Rossi-Fedele G, Dummer PMH. Critical analysis of a new system to classify root and canal morphology — a systematic review. Aust Endod J. 2023;49:750–768. doi:10.1111/aej.12780
7. Kolarkodi SH. The importance of cone-beam computed tomography in endodontic therapy: a review. Saudi Dent J. 2023;35(7):780–784. doi:10.1016/j.sdentj.2023.07.005
8. Lo Giudice R, Nicita F, Puleio F, et al. Accuracy of periapical radiography and CBCT in endodontic evaluation. Int J Dent. 2018;2018:1–7. doi:10.1155/2018/2514243
9. Neri H, Aripin D, Muryani A, Yolanda Y, Mahyuddin AI, Dharsono HDA. Stress analysis on mesiolingual cavity of endodontically treated molar restored using bidirectional fiber-reinforced composite (Wallpapering Technique). Clin Cosmet Investig Dent. 2024;16:75–89. doi:10.2147/CCIDE.S450325
10. Rahmayanti ZA, Aripin D, Muryani A, et al. Stress distribution of endodontically treated tooth MOD cavity restored with ribbon fiber-reinforced composite (Wallpapering Technique) using finite element method. Clin Cosmet Investig Dent. 2024;16:91–99. doi:10.2147/CCIDE.S450458
11. Sengun A, Cobankara FK, Orucoglu H. Effect of a new restoration technique on fracture resistance of endodontically treated teeth. Dent Traumatol. 2008;24(2):214–219. doi:10.1111/j.1600-9657.2007.00538.x
12. Sultan S, Al Garni H, Al Onazi M, et al. Minimally invasive posterior full crown competitors: onlays, occlusal veneers, vonlays and endocrowns: a review and proposed classification. J Int Dent Med Res. 2021;14(4):1617–1622.
13. Özkurt Z, Kazazoĝlu E. Clinical success of zirconia in dental applications. J Prosthodontics. 2010;19(1):64–68. doi:10.1111/j.1532-849X.2009.00513.x
14. Berman LH, Hargreaves KM, editors.. Cohen’s Pathways of the Pulp.
15. Rotstein I, Ingle JI. Ingle’s Endodontics.
16. Wang Y, Guo J, Yang HB, Han X, Yu Y. Incidence of C-shaped root canal systems in mandibular second molars in the native Chinese population by analysis of clinical methods. Int J Oral Sci. 2012;4(3):161–165. doi:10.1038/ijos.2012.42
17. Chai W, Thong Y. Cross-sectional morphology and minimum canal wall widths in C-shaped roots of mandibular molars. J Endod. 2004;30(7):509–512. doi:10.1097/00004770-200407000-00012
18. Singh S, Attur K, Oak A, Mustafa M, Bagda KK, Kathiria N. An appraisal on newer endodontic file systems: a narrative review. J Contemp Dent Pract. 2023;23(9):944–952. doi:10.5005/jp-journals-10024-3398
19. Plotino G, Grande NM, Mercade M, et al. Efficacy of sonic and ultrasonic irrigation devices in the removal of debris from canal irregularities in artificial root canals. J Appl Oral Sci. 2019;27.
20. Rodríguez-Figueroa C, McClanahan SB, Bowles WR. Spectrophotometric determination of irrigant extrusion using passive ultrasonic irrigation, endoactivator, or syringe irrigation. J Endod. 2014;40(10):1622–1626. doi:10.1016/j.joen.2014.03.017
21. Boutsioukis C, Psimma Z, Van der Sluis LWM. Factors affecting irrigant extrusion during root canal irrigation: a systematic review. Int Endodontic J. 2013;46:599–618. doi:10.1111/iej.12038
22. Zou X, Zheng X, Liang Y, et al. Expert Consensus on Irrigation and Intracanal Medication in Root Canal Therapy. Vol. 16. International Journal of Oral Science. Springer Nature; 2024.
23. Geogi CC, Dubey S, Singh P, Rajkumar B. Bioceramic in Endodontics. Book Rivers; 2022.
24. Drukteinis S, Camilleri J. Bioceramic Materials in Clinical Endodontics. Springer; 2021.
25. Lin PH, Lin DJ, Huang HL, Hsu JT, Tu MG. Comparison sealing ability in three bioceramic sealers applied in hydraulic condensation technique by using micro-computed tomography. J Dent Sci. 2023;18(3):1258–1263. doi:10.1016/j.jds.2023.02.016
26. Jaha HS. Hydraulic (Single Cone) versus thermogenic (Warm Vertical Compaction) obturation techniques: a systematic review. Cureus. 2024;16(6):e62925. doi:10.7759/cureus.62925
27. Kontonasaki E, Rigos AE, Ilia C, Istantsos T. Monolithic zirconia: an update to current knowledge. Optical properties, wear, and clinical performance. Dent J. 2019;7:90. doi:10.3390/dj7030090
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.