Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Insulin Autoimmune Syndrome (Hirata Disease): A Comprehensive Review Fifty Years After Its First Description
Authors Cappellani D ![]() , Macchia E, Falorni A
, Macchia E, Falorni A ![]() , Marchetti P
, Marchetti P
Received 18 January 2020
Accepted for publication 13 March 2020
Published 1 April 2020 Volume 2020:13 Pages 963—978
DOI https://doi.org/10.2147/DMSO.S219438
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Daniele Cappellani,1 Enrico Macchia,1 Alberto Falorni,2 Piero Marchetti3
1Department of Clinical and Experimental Medicine, Unit of Endocrinology, University of Pisa, Pisa, Italy; 2Department of Medicine, Section of Internal Medicine and Endocrine and Metabolic Sciences, University of Perugia, Perugia, Italy; 3Department of Clinical and Experimental Medicine, Division of Metabolism and Cell Transplantation, University of Pisa, Pisa, Italy
Correspondence: Daniele Cappellani
Department of Clinical and Experimental Medicine, Unit of Endocrinology, University of Pisa, Ospedale Cisanello, via Paradisa 2, Pisa 56124, Italy
Tel +39 50 995001
Fax +39 50 578772
Email [email protected]
Abstract: Insulin autoimmune syndrome (IAS), also named Hirata’s disease, is a rare condition characterized by hypoglycemic episodes due to the presence of high titers of insulin autoantibodies (IAA). IAS is a form of immune-mediated hypoglycemia, which develops when a triggering factor (ie, a medication or a viral infection) acts on an underlying predisposing genetic background. IAS pathogenesis involves the formation of insulin-IAA complexes that induce glycemic alterations with a double-phase mechanism: IAA prevent insulin to bind its receptor in the postprandial phase, possibly resulting in mild hyperglycemia; thereafter, insulin is released from the complexes irrespective of blood glucose concentrations, thus inducing hypoglycemia. The diagnosis of IAS is challenging, requiring a careful workup aimed at excluding other causes of hyperinsulinemic hypoglycemia. The gold standard for the definitive diagnosis is the finding of IAA in a blood sample. Because IAS is frequently a self-remitting disease, its management mostly consists of supportive measures, such as dietary modifications, aimed at preventing the development of hypoglycemia. Pharmacological therapies may occasionally be necessary for patients presenting with severe manifestations of IAS. Available therapies may include drugs that reduce pancreatic insulin secretion (somatostatin analogues and diazoxide, for instance) and immunosuppressive agents (glucocorticoids, azathioprine and rituximab). The purpose of this review is to provide a comprehensive analysis of the disease, by describing the burden of knowledge that has been obtained in the 50 years following its first description, took in 1970, and by highlighting the points that are still unclear in its pathogenesis and management.
Keywords: insulin autoimmune syndrome, IAS, Hirata, hypoglycemia, autoimmunity
Introduction
Insulin autoimmune syndrome (IAS) is a rare condition, characterized by spontaneous episodes of hyperinsulinemic hypoglycemia due to the presence of high serum concentrations of insulin autoantibodies (IAA). IAS is also named Hirata’s disease, after the original description made in 1970 by Yukimasa Hirata and colleagues.1 IAS is one of the two types of autoimmune hypoglycemia, being the other type B insulin resistance, which is due to antibodies against the insulin receptor.2–4 According to its original definition, IAS develops in individuals who were not previously exposed to exogenous insulin and who do not present pathological abnormalities of the pancreatic islets; nevertheless, cases of glycemic instability were more recently reported in insulin-treated patients as a consequence of the development of insulin antibodies with biochemical and clinical features that were similar to those of IAA.5 The pathogenesis of IAS has been extensively investigated and the mechanisms underpinning the glycemic fluctuations described in IAS have been identified in a mismatch between plasma glucose and insulin concentrations, due to the presence of IAA. The diagnostic workup of IAS is complex and aims at a correct and complete differential diagnosis with other forms of hypoglycemic disorders.6 Despite being a condition that often undergoes self-remission, IAS management remains challenging, given the absence of committed specific therapies and the lack of comparison between the different therapeutic regimens that have been proposed. For the purposes of the present review, we performed a computer-aided literature search of the MEDLINE database; moreover, we examined the reference lists of the published articles, case reports and reviews. Studies that were published in languages other than English were excluded. The database was searched for articles published until September 2019.
Historic Perspectives
IAS was originally described in 1970 by Yukimasa Hirata and colleagues in a 47-year-old obese male with recurrent severe hypoglycemic episodes.1 For several years after the original Hirata’s description the reports of this condition were scanty and mostly, but not exclusively, from Japan.7–10 A subsequent milestone in the history of IAS includes the identification of the association with the exposure to sulphydryl medications in 1983.11 Many steps forward in the identification of the pathogenesis of IAS were taken during the 1990s: for instance, the association with specific immunogenic determinants was described in 1992,12 whereas the IAS was identified as a form of type VII hypersensitivity in 1995.13 In the last 20 years, many additional cases of IAS have been reported worldwide, deepening our knowledge on its pathogenesis and providing new tools for the diagnostic and therapeutic approaches to this disease.
Epidemiology
The exact incidence of IAS is still a matter of debate, being probably underestimated due to the difficulties in the diagnostic workup, the self-limiting nature of the disease, and the general unawareness of this disease until the last decade. A brief summary of the main epidemiological studies on IAS is reported in Table 1. Three hundred eighty cases of IAS were reported worldwide from 1970 to 2009.14 According to our knowledge, there is no published study that reported the exact worldwide incidence of IAS after 2009. On one hand, this may be due to the fact that newly found cases of IAS lacking of clinical novelty may have been considered unsuitable for publication by many Journals;15 on the other hand, many large retrospective cohort studies include patients that had already been described in single case reports or smaller series, thus making difficult the identification of the real incidence of the disease.
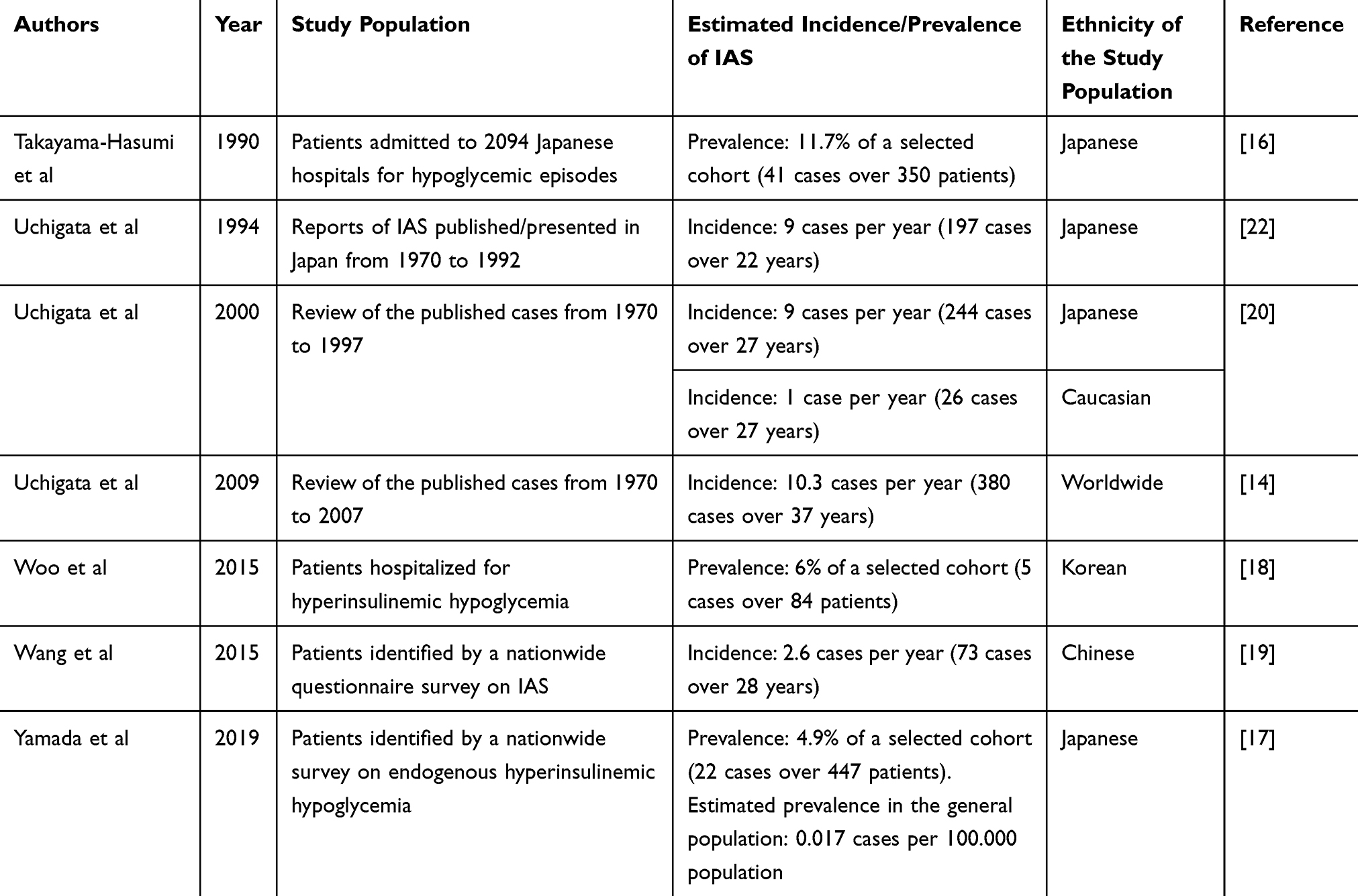 |
Table 1 Main Epidemiological Studies on Insulin Autoimmune Syndrome (IAS) |
IAS was originally described in Japan, and in 2009 over 90% of the published cases were reported in the Japanese population, where this disease was considered the third most common cause of hypoglycemia, after insulinoma and extrapancreatic neoplasias.15,16 The most recent study estimating the epidemiology of IAS in the Japanese population was conducted in 2019, and it reports an estimated prevalence of 0.017 cases per 100.000 in the general population.17 The prevalence of IAS in Korea was retrospectively estimated to be the 6% of a cohort of 84 patients undergoing a diagnostic workup for endogenous hyperinsulinemic hypoglycemia at a referral hospital.18 The prevalence of IAS in China was reported to be much lower, accounting for only 73 cases over a 30-years span.19 Although the first report of IAS in a Caucasian patient was published early in 1972,8 the disease has always been considered quite rare outside Asia. Yet, an increasing number of cases have been reported in the last decades in Caucasians.3
The uneven geographic distribution of IAS was primarily attributed to the evolutionary distribution of the HLA system alleles.20 However, this theory is counterbalanced by the observation that in more recent years the incidence of this disease has been increasing more evenly worldwide. Whether the reason for this epidemiological trend should be identified in the wider usage of medications and supplements that have been associated to IAS,4 or to the greater awareness for the disease and the wider availability of IAA assays is still a matter of debate.4
IAS seems to affect both sexes equally.3,21 The peak age at onset was originally reported in the seventh decade.22 However, it is nowadays known that the age at onset varies widely, and a temporal difference in its incidence among males and females was observed with an earlier incidence (fourth decade) for females and a later incidence (seventh decade) for males.19 IAS is rare in the pediatric population, even though there are scattered reports in children.23,24
Classification
Insulin autoimmune syndrome can be classified taking into account different perspectives. First of all, IAS can be classified on the basis of a previous exposure to exogenous insulin, which would determine a subdivision between patients who were previously exposed and patients who were not. This classification seems pleonastic, since IAS was originally defined as a syndrome developing in patients who were not previously exposed to exogenous insulin, as reported above. Nevertheless, given the presence of manuscripts describing IAS in diabetic patients who were previously treated with insulin therapy,25–27 we decided to include this introductory classification in order to provide a more complete overview of the disease.
Secondly, IAS can be classified according to the association with other autoimmune diseases: on the one hand, it can be a solitary manifestation of autoimmunity, whereas on the other hand it can be associated with other autoimmune diseases, being included in type 3A or in type 4 autoimmune polyendocrine syndrome.28 The linkage between IAS and Graves’ disease that was originally identified9 has been subsequently clarified:11,29 these two different autoimmune diseases may be associated not as independent manifestations of a common autoimmune condition, but because IAS may be the consequence of the exposure to antithyroid drugs administered to the patient for the cure of the hyperthyroidism. The association of IAS with other forms of autoimmunity was described more frequently in Caucasian than in Asian patients.3
Moreover, IAS can be classified by distinguishing between drug-induced forms and apparently-spontaneous ones.14 The list of medications associated with IAS is long, and includes the medications reported below and summarized in Table 2. The prevalence of drug-induced forms was estimated to be 43% in a Japanese series of 197 IAS patients diagnosed from 1970 to 1991.22 Similarly, in 2009 it was estimated that drug-induced IAS accounted for about the 50% of the total in the Caucasian population.3 Given the progressive extension of the list of medications that have been associated to the development of the syndrome, more recent studies hypothesized that the above-mentioned estimates of drug-induced IAS were underestimating the problem, being the actual prevalence above eighty percent.19
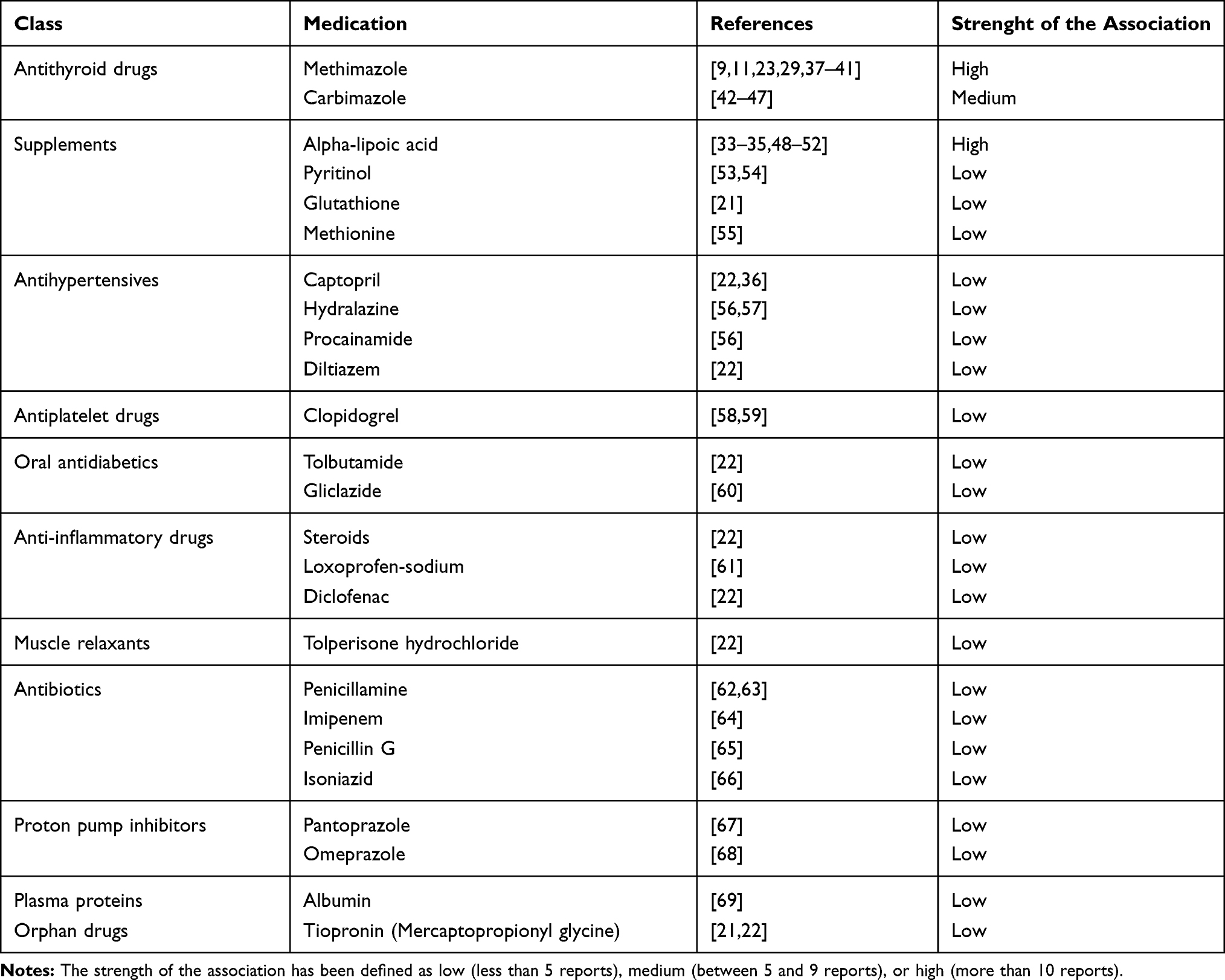 |
Table 2 List of Medications Associated with the Development of Insulin Autoimmune Syndrome |
Etiology
The etiopathogenesis of IAS has not been fully understood. The most widely accepted theory is that IAS results from the interaction of a genetic predisposition with environmental triggers, thus leading to the production of insulin autoantibodies which have a pathogenic role.15
The genetic background of the syndrome was extensively investigated from the early 1990s. The immunogenetic determinants for the IAS were identified in the genes of the class II Human Leukocyte Antigen (HLA) system: the disease resulted strongly associated with HLA-DR4 and specifically with the DRB1*0406 and, although less significantly, DRB1*0403 and DRB1*0407.12,30,31 The higher prevalence of HLA-DRB1*0406 in Asian populations was advocated as the determinant of the higher incidence of IAS in Japan compared to the western countries.20 Furthermore, a correlation between the genetic background and the risk of developing a particular form of drug-induced IAS (ie methimazole-induced IAS in patients with Graves’ disease) was also postulated: the incidence of methimazole-induced IAS is particularly high in Japan compared to other countries, and the patients who develop IAS following methimazole exposure invariably carry the DRB1*0406 allele.32 As a consequence, the lower incidence of methimazole-induced IAS outside Japan was supposed to be due to the lower prevalence of the HLA-DRB1*0406 in the general population.20 HLA-DRB1*0406 was originally supposed to be also associated with the alpha-lipoic acid-induced IAS in Japanese patients,33 but this finding was not confirmed nor in Caucasians,34 nor in other Asian populations.35 More recent papers describing case reports of IAS outside Asia did not uniformly confirm the linkage of the IAS with the above-mentioned immunodeterminants, suggesting that the genetic spectrum of the syndrome may be broader (especially outside Asia), and thus indicating the need of further studies to understand more deeply the genetic background of the syndrome.24,36
Many different triggers have been advocated to induce the development of IAS when acting on an underlying predisposing background: among them, in order of importance, there are medications, viruses and hematological diseases.
The list of medications that have been suspected as possible triggers for the development of IAS is reported in Table 2.
This list has been progressively extended to include new medications, most of which have been added during the last ten years. However, many of the drugs that have been proposed as potential triggers for the development of IAS have been merely reported by one single paper. This point claims that more solid confirmatory evidences are required for most of the cited drugs. At present, methimazole9,11,37,38 and alpha-lipoic acid33–35,48 remain the only medications whose exposure has been more commonly linked to the development of IAS. It is noteworthy that the association between alpha-lipoic acid and IAS has been increasing during the last decade.14 Alpha-lipoic acid is a compound that is widely prescribed in many medical fields, mainly due to its antioxidative properties:70 as a consequence, it has been proposed as an adjuvant therapy for instance in diabetic neuropathy,71,72 polycystic ovary syndrome,73 central nervous system related diseases74 and as a supplement for dieting and anti-aging.14 To date, alpha-lipoic acid-induced IAS seems more common than methimazole-induced IAS.34
Importantly, the medications associated with IAS are mostly sulphydryl and reducing compounds, providing a clue regarding a possible pathogenesis of the disease. The proposed mechanism is that these drugs would bind and cleave the sulphydryl bonds between the insulin chains A and B, thus leading to a conformational change in its molecular structure that makes the endogenous insulin more immunogenic:75 as a matter of fact, following the cleavage of the bonds between the insulin chains, the antigen-presenting cells may bind much more of the linear fragment of the insulin A chain, thus leading to the activation of self-directed insulin-specific T-helper cells.76 However, IAS has also been reported in patients that were taking medications that do not contain sulphydryl bounds, such as albumin.69 The onset timing of drug-induced IAS varies widely: as a matter of fact, while some authors report the onset of the first IAS manifestations few days after the first administration of the responsible medication,35,49 others identify a longer onset time, up to many months.34,37 The mean onset time was estimated to be four to six weeks following the beginning of the offending medication.22 Yet, there are reports of drug-induced IAS developing years after the first administration of the offending medication, due to an additional and subsequent cycle of the medical therapy.39
Many viral infections have been reported to be triggers for the development of IAS: measles virus, mumps virus, rubella virus, varicella zoster virus, coxsackie B virus and hepatitis C virus.77 The supposed mechanism is that the viral infection acts as a super-antigen, thus triggering the production of the IAA that cause the syndrome.78
The association with hematological disorders, such as multiple myeloma or monoclonal gammopathy of undetermined significance has been described in Caucasians.79
There are many reported cases of patients who develop IAS without a previous history of exposure to known triggering factors. This spontaneously-onset IAS has been mostly reported in Japan, whereas it seems a quite rare phenomenon in western countries. It has been proposed that the cases that were reported as spontaneously-onset were actually determined by triggers that underwent misrecognized.19
Pathogenesis
IAS has been described as a form of type VII hypersensitivity, characterized by the presence of autoantibodies against a circulating antigen.13 The cornerstone of the IAS is the appearance of circulating insulin autoantibodies (IAA), which have a pathogenic role in the development of the syndrome, and play also a central diagnostic role in this disease. IAA are immunoglobulins (Ig) directed against the native endogenous insulin molecule. They may belong to different Ig classes, although they are more commonly IgG;4 IAA belonging to IgA and IgM are definitely rare, although described.77,80 Due to their high binding capacity, IAA are able of binding several molecules of insulin, resulting in the formation of large antigens-antibodies complexes. On the other hand, the low affinity for insulin is responsible for a significant spontaneous dissociation rate, which inappropriately raises unbound insulin concentrations, thus resulting in hypoglycemic episodes, as reported below. High binding capacity and low affinity are the specific features of the IAA that are capable of inducing IAS.81 As a matter of fact, even though modern insulin analogs have a low immunogenicity, insulin antibodies may sometimes be detected in patients receiving insulin therapy, but these antibodies are rarely capable of causing hyperglycemia or hypoglycemia.25 This is because the insulin antibodies that develop following exposure to exogenous insulin are more often characterized by a higher affinity and a lower binding capacity against insulin compared to IAA. As a consequence, they mostly result in smaller antigen-antibody complexes which have a lower spontaneous dissociation rate, thus they are unable to produce significant glycemic fluctuations.5 Nevertheless, insulin antibodies developing after the administration of exogenous insulin may seldom present with features similar to those of IAA, such as a high binding capacity and low affinity, thus resulting in glycemic instability.5,82,83
IAA have no pathological effects when present at small titers: up to 2% of a cohort of healthy blood donors presented small titers of IAA, without any previous or current manifestation of IAS.84
The presence of the IAA induces IAS with a double-phase mechanism, which is constantly underpinned by a mismatch between blood glucose concentrations and free insulin concentrations,15,85 as reported in Figure 1. The first phase takes place when insulin normally secreted by the pancreatic beta-cells in response to rising plasma glucose concentrations binds to autoantibodies, becoming unable to exert its physiological effects. In other terms, in this first phase, insulin-IAA complexes hinder the physiological mechanisms of insulin action,86 thus resulting in low unbound insulin concentrations and consequent transient hyperglycemia. Early postprandial hyperglycemia is a further stimulus for the secretion of insulin molecules that are partly bound to circulating insulin-IAA complexes and partly unbound and free to exert its physiological action. Spontaneous dissociation of insulin from the complexes does not cease when plasma glucose concentrations lower, thus resulting in a relative excess of unbound insulin, which evokes hypoglycemia.15,86
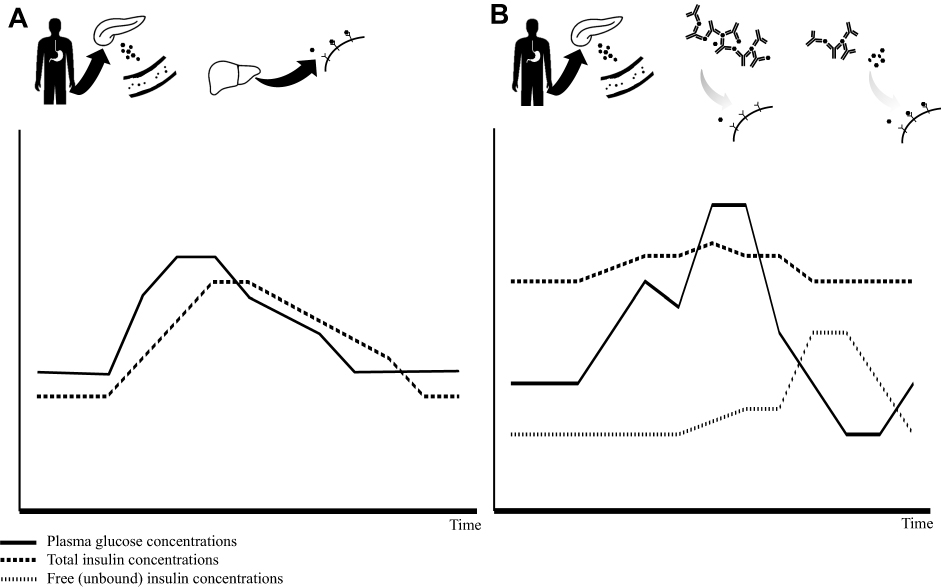 |
Figure 1 The insulin autoimmune syndrome pathogenesis. Notes: Panel (A) schematic overview of the physiologic insulin secretion and action: following glucose intake, pancreatic beta-cells secrete insulin which enters into the bloodstream, getting to peripheral tissues when it exerts its physiological functions in order to maintain glucose homeostasis. Panel (B) schematic overview of the double-phase mechanism of the insulin autoimmune syndrome. Following glucose intake, pancreatic beta-cells secrete insulin which enters into the blood stream getting included in the insulin-IAA macro-complexes. In the early postprandial phase, inclusion intro macro-complexes prevents insulin to act on its receptors in peripheral tissues, thus inducing hyperglycemia (phase 1). Due to the relatively low affinity for insulin, IAA subsequently release insulin molecules irrespective of plasma glucose concentrations, thus inducing hypoglycemic episodes (phase 2). Below both panels is reported a schematic representation of glucose and insulin concentrations over time: the continuous line represents plasma glucose concentrations, dotted line represents total insulin, pointed line represents free unbound insulin. |
A few reports show the pathological examinations of IAS patients who underwent invasive procedures due to an initial mistake in differential diagnosis with insulinoma: the changes reported were consistent with pancreatic islets hyperplasia in one case87 and nesidioblastosis in another case.18
Clinical Presentation
The clinical manifestations of IAS vary widely in terms of severity, duration and remission rates.15 The clinical hallmark of IAS is hypoglycemia, which manifests with autonomic (hunger, seating, tremor, anxiety) and neuroglycopenic (irritability, behavioral changes, confusion, amnesia, seizures, loss of consciousness) symptoms.88 Importantly, the cut-off to elicit hypoglycemic symptoms is much lower in patients who suffer from recurrent hypoglycemia compared to healthy patients.89 IAS-induced hypoglycemia is usually mild, even though cases presenting with severe manifestations (up to seizures and coma) have been reported.37,57,66,90
An important point is the timing of hypoglycemia in relation to meals: most patients present postprandial hypoglycemia,3 which is consistent with the pathogenic mechanism described above. However, there are reports of patients presenting with fasting hypoglycemia or even unpredictable hypoglycemic episodes.
In line with the supposed pathogenic mechanism86 described above, patients may present with swings from hyperglycemia to hypoglycemia. In such circumstances, the typical presentation consists in early postprandial hyperglycemia and subsequent reactive hypoglycemia, as described in the earliest report of IAS in a Caucasian patient.8 Glycated hemoglobin concentrations may vary according to the frequency and severity of hypoglycemic attacks and to the presence of glucose concentrations swings, so normal or even increased HbA1c concentrations can be found.36,86 An increase in body weight has been reported, especially in patients presenting with long-lasting misrecognized IAS.36 Whether this point could be due to the increased food intake as a corrective mechanism for hypoglycemia, or to the anabolic effects exerted by hyperinsulinemia, has not been investigated.
Finally, for patients presenting IAS as a manifestation of a wider autoimmune movement, hypoglycemia can be preceded, accompanied or followed by other autoimmune manifestations, involving other endocrine glands, or other organs and systems.28
Diagnosis
When approaching a patient affected by hypoglycemia, the differential diagnosis between the different possible causes is mandatory, although challenging.6 As a matter of fact, the therapeutic approach to hypoglycemia is strictly dependent on its cause. Although rare, IAS should be suspected in any patient presenting with hypoglycemia, in order to avoid any unnecessary diagnostic and therapeutic procedure.91 A flow-chart of the diagnostic work-up of IAS is shown in Figure 2.
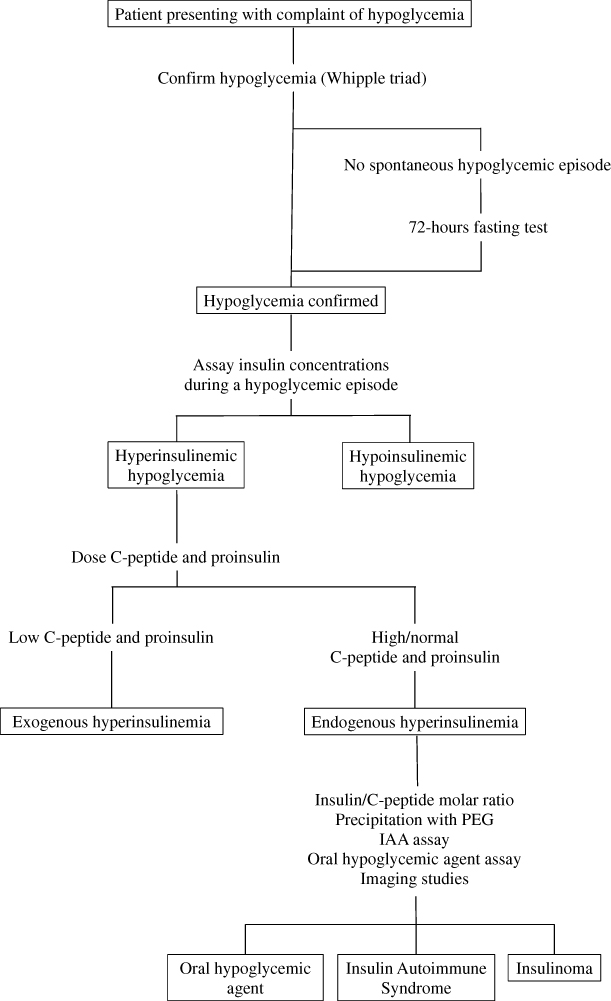 |
Figure 2 Flowchart for the diagnosis of insulin autoimmune syndrome. Abbreviations: PEG, polyethylene glycol; IAA, insulin autoantibodies. |
The first step in the approach to IAS is confirming the diagnosis of hypoglycemia, which can be proved by the presence of the Whipple triad: symptoms or signs of hypoglycemia associated with low plasma glucose concentrations (≤ 70 mg/dL),92,93 and resolution of those symptoms or signs after the plasma glucose concentration is raised by glucose administration. The documentation of the hypoglycemic episode is mandatory, since the nature of the hypoglycemia-related symptoms is not pathognomonic. If hypoglycemia does not appear spontaneously it should be investigated, even with the use of a fasting evaluation (up to 72 hours fast) with repeated measures of plasma glucose concentrations.6 The oral glucose tolerance test is not routinely suggested in the work-up of the patient presenting for hypoglycemia.6 In the specific case of IAS, the individual responses to the oral glucose administration show a wide variability,94 and different glycemic responses to the oral glucose load were identified in the same patient when tested at different IAA titers.95
The second step consists in assaying serum insulin concentrations during a hypoglycemic episode.
Usually patients affected by insulin autoimmune syndrome present with extremely high insulin concentrations, often above 1000 pmol/L,42 which is a rare finding in other forms of hyperinsulinemic hypoglycemia.85 Interestingly, insulin concentrations can vary widely when assayed with different kits. The immunoradiometric assay (IRMA) is far more accurate for the dosage of unbound insulin compared to immunochemiluminometric assays (ICMA).35 Hypoglycemia factitia due to exogenous insulin administration is another possible cause of hyperinsulinemic hypoglycemia. Because different insulin assays may exhibit variable cross-reactivity with insulin analogues,96 it is not possible to differentiate hypoglycemia factitia from IAS by these insulin assays. However, once hyperinsulinemic hypoglycemia has been confirmed, C-peptide and proinsulin are useful for differentiating between endogenous and exogenous forms of hyperinsulinemia.6 Low C-peptide and proinsulin are suspicious for exogenous insulin administration. On the contrary, high or inappropriately normal C-peptide and proinsulin concentrations are found in endogenous hyperinsulinemia, such as insulinoma or IAS.
A possible caveat of relying on C-peptide and proinsulin testing is that they do not allow the exclusion of other forms of hypoglycemia factitia, such as those due to oral hypoglycemic agents, such as sulfonylureas. The administration of these drugs can be excluded by dosing their presence in a blood sample.97
Insulin to C-peptide molar ratio has been proposed as a diagnostic tool for IAS.98 Pancreatic beta-cells secrete insulin and C-peptide in equimolar proportions, however these molecules have different half-lives, being 5–10 mins for insulin and 30–35 mins for C-peptide. As a consequence, the physiologic insulin to C-peptide molar ratio is lower than 1. The insulin to C-peptide molar ratio may be theoretically reversed to higher than 1 in IAS (due to the substantially higher insulin concentrations as a consequence of the prolonged half-live on the insulin molecules that are bound in the insulin-IAA complexes) and in exogenous insulin administration (due to the hypoglycemia-driven suppression of endogenous insulin secretion, which is responsible for the lower C-peptide concentrations).91,98 However, the use of insulin to C-peptide molar ratio in the diagnosis of IAS has been strongly criticized, given that C-peptide and proinsulin concentrations may vary widely in this condition, depending on the IAA capacity of binding these molecules as well, or to their ability to interfere with the available immunoassays.4
Precipitation with polyethylene glycol (PEG), followed by insulin assay in the supernatant has been proposed as a method for detecting the IAA.34 The recovery of insulin following PEG precipitation results substantially lower in the sera of patients affected by IAS compared to healthy controls. However, proven that gel filtration chromatography with the addition of exogenous insulin may enhance the sensitivity for the identification of insulin immunocomplexes,78 precipitation with PEG should be used cautiously when searching insulin-IAA complexes.36
The measurement of IAA titer is mandatory for the diagnosis of IAS99 since it is the only lab test that allows a reliable diagnosis of IAS.4 However, the availability of IAA assay is not widespread and the results of this test are obtained with delay, therefore preliminary confirmatory tests are performed. A possible pitfall in the measurement of IAA is that most of commercially-available assays are able to identify only IgG class of IAA, thus producing false negative results in the rare patients who present other classes of IAA.4 In this context, the PEG precipitation can be considered a preliminary test, given its ability to precipitate IAA of any class.
Antibodies directed towards insulin may be detected in insulin-treated patients and even in healthy donors.84 In this context, a Scatchard analysis100 may be used with the aim to characterize the antibodies’ features, such as their affinity for the antigen and their binding capacity.81,101 The typical antibodies detected in the IAS present high binding capacity and low affinity for the endogenous insulin molecule.5,101
Imaging studies are obviously useless in the diagnosis of IAS. However, given the difficulties in the differential diagnosis with other forms of endogenous hyperinsulinemic hypoglycemia, IAS patients often undergo inappropriate and expensive imaging studies in their diagnostic workup. The incidental finding of a lesion at imaging studies may induce the execution of further examinations or even invasive procedures.
It is still a matter of debate whether a thorough screening aimed at excluding any associated autoimmune disease in the context of a PGA may be cost-effective, once the diagnosis of IAS is made.
A scheme for the differential diagnosis with other forms of hypoglycemia is reported in Table 3. Briefly, due to its higher prevalence102 and the underlying similarities, insulinoma is the disease that enters more often in differential diagnosis with IAS. As a matter of fact, insulinoma is another form of endogenous hyperinsulinemic hypoglycemia, just like IAS. However, IAS-induced hypoglycemia is more often milder compared to insulinoma and, on the contrary, IAS-induced hyperinsulinemia is much higher compared to insulinoma.42,85 Given the possibility that insulinomas may not be detected at conventional imaging studies,103,104 the only reliable tool for the differential diagnosis is the assay for IAA, that are present in IAS but absent in insulinomas. Nesidioblastosis may result in the noninsulinoma pancreatogenous hypoglycemia syndrome (NIPHS), another cause of endogenous hyperinsulinemic hypoglycemia that appears more often after a meal.105,106 This condition is much rarer than insulinoma. Furthermore, the development of NIPHS may be preceded by a history of gastric surgery and dumping syndrome.107,108 The presence of the latter points in the patient’s past clinical history may be useful in the diagnostic work-up, even though the ultimate tools used for differentiating nesidioblastosis from IAS are the same available for the differential diagnosis with insulinoma.6 The results of a recent Korean study prove that the differential diagnosis between IAS and other forms of endogenous hyperinsulinemic hypoglycemia is impossible without the availability of the IAA assay: the incidence of nesidioblastosis at a tertiary-level hospital declined after IAA assays were introduced as a routine test for patients presenting for hyperinsulinemic hypoglycemia.18 Hypoglycemia due to exogenous insulin administration (in the set of psychiatric conditions or surreptitious usage) is a form of hyperinsulinemic hypoglycemia associated with low C-peptide and proinsulin concentrations97,109 and, obviously, not associated with IAA.110 More complex is the differential diagnosis with other forms of drug-induced hypoglycemia, such as those due to the administration of oral hypoglycemic agents: the definitive diagnosis of sulfonylurea-induced hypoglycemia can be obtained by assaying for the presence of these medications in a blood sample.6 Type B insulin resistance is another form of autoimmune hypoglycemia,3 which is due to the presence of autoantibodies which bind to the insulin receptor exerting agonistic effects, thus resulting in insulin resistance and paradoxical hypoglycemia.4 Patients affected by type B insulin resistance often display features of severe insulin resistance, such as severe diabetes mellitus poorly responsive to insulin therapy and acanthosis nigricans,111 which are usually not present in patients affected by IAS. Despite this clinical difference, the only reliable method for the differential diagnosis between these two forms of autoimmune hypoglycemia is the characterization of the autoantibodies: as a matter of fact, IAA are present in IAS, whereas anti-receptor insulin antibodies are present in type B insulin resistance.112
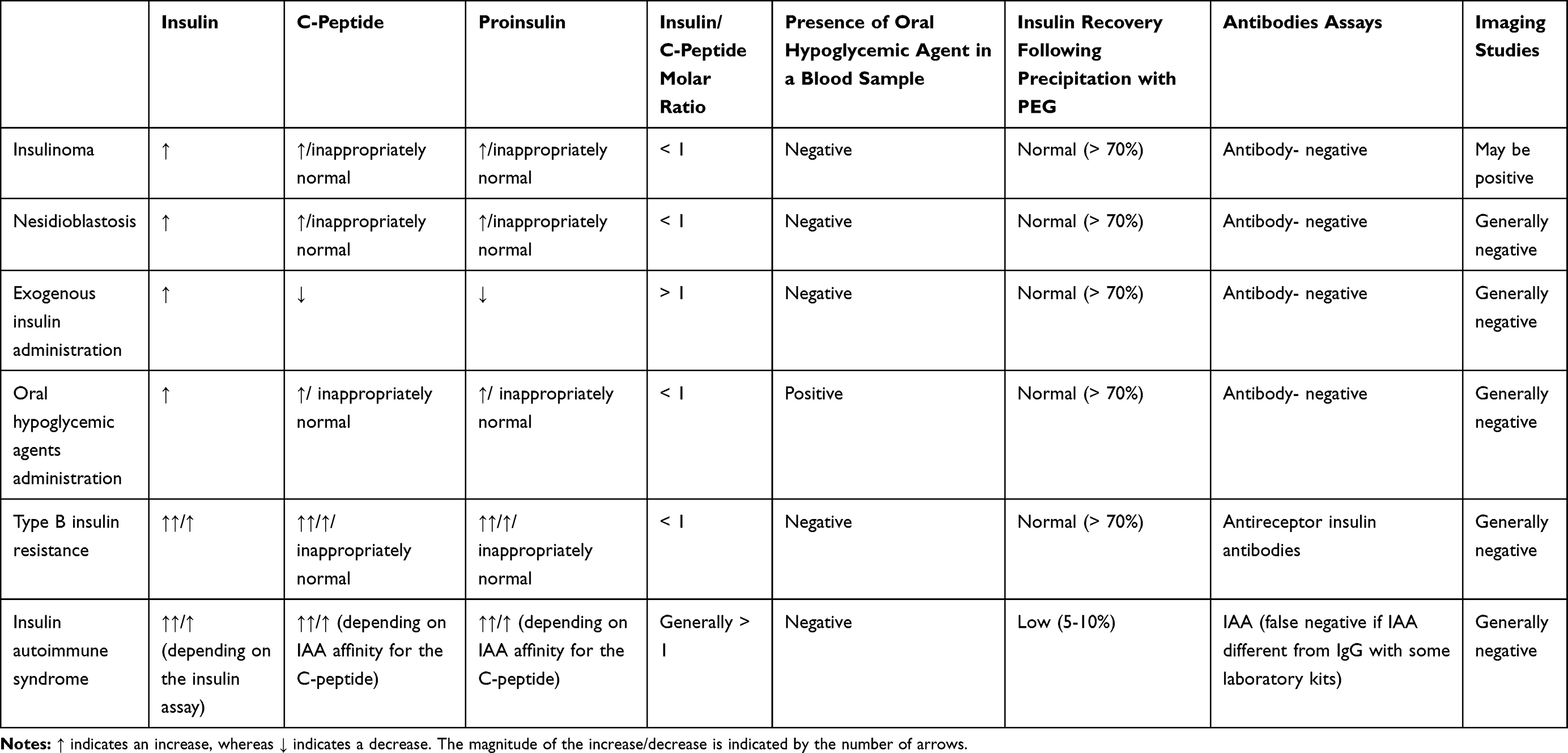 |
Table 3 Diagnostic Tools for the Differential Diagnosis Between Hypoglycemias of Different Origins |
Therapy
The medical treatment of autoimmune hypoglycaemia is problematic for the following reasons: (i) it is not clear whether pharmacologic treatment can be avoided, given the high rates of spontaneous remission; (ii) the whole literature describing the therapeutic approaches consists in scattered case reports or small case series, and no comparison study among the proposed treatment regimens has ever been performed; (iii) predicting factors that allow the identification of patients who benefit most from active treatment have never been searched. The pharmacological options that are currently available include glucocorticoids, somatostatin analogues, diazoxide, azathioprine, rituximab.
However, the indication to a first-line interventional approach for every IAS patient has been questioned, given that the syndrome is mainly a spontaneously-remitting disease.35 As a matter of fact, approximately 82% of the IAS patients underwent spontaneous remission in a revision of 197 patients diagnosed with IAS from 1970 to 1992:22 the duration of hypoglycemic episodes was between one and three months in this cohort, without differences according to sex.22
Withdrawal of the medication identified as the trigger for the development of IAS seems rational. Nevertheless, the real advantages of the drug discontinuation is unclear provided that no study has ever evaluated the remission rates for patients who withdraw the trigger medication compared to patients who do not.
Besides pharmacological therapies, dietary modifications have been proposed in order to counterbalance the development of hypoglycemic episodes. A rational approach consists in small frequent meals with low carbohydrate content aimed at reducing early postprandial hyperglycaemia and the consequent stimulus to insulin secretion, and at preventing hypoglycemic attacks.85,91 Treatment with uncooked cornstarch has been successfully applied in the setting of IAS, after originally resulting effective in the setting of glycogen storage diseases.55 Cornstarch is a glucose polymer slowly absorbed by the gut and able to avoid postprandial glycemic peaks, so the purposes of its administration are somehow overlapped with the suggested dietary regimen consisting in small and frequent meals. Similarly, treatment with alpha-glucosidase inhibitors (acarbose), prevents postprandial hyperglycemia, thus displaying different degrees of benefit in reducing glycemic excursions in IAS.113,114 In case of severe hypoglycemic episodes, intravenous glucose administration may be necessary, especially in order to prevent nightly glycemic fluctuations.88
Among the strategies aimed at reducing insulin release, somatostatin analogues,40,115 diazoxide41,115,116 and even pancreatectomy18,79 have been proposed, with variable results.
Scattered cases have proposed metformin in a combined therapeutic approach to IAS, with the aim to reduce insulin resistance (especially in patients affected by metabolic syndrome) and thus reducing insulin secretion and the consequent formation of insulin-IAA complexes.36,117 The results of this treatment have not been evaluated systematically.
Given the autoimmune nature of the IAS, this condition has been treated with high-dose corticosteroids, with overall good results.3,22,34,115 Other immunosuppressive agents, such as azathioprine, have been proposed in case of persistency of the disease despite high-dose systemic corticosteroids.118 Rituximab is an anti-CD20 monoclonal antibody that has been used for the treatment of severe refractory IAS both alone119,120 and following immunoadsorption with an adsorber system containing sheep antigens directed against human immunoglobulins.121 The rational for its use in the setting of IAS comes from the type 1 diabetes immunological intervention trial “TrialNet”, which demonstrated that a single course of rituximab produced a complete disappearance of IAA in 40% of patients that were previously IAA-positive, with an effect lasting up to three years.122
Plasmapheresis has been used in more severe cases, with the aim to lower IAA titer rapidly, thus preventing hypoglycemia.113,123,124
Independently from the kind of therapeutic approach adopted, frequent glucose monitoring during the follow-up seems advisable. Continuous glucose monitoring (CGM) allows glucose measurement in the interstitial fluid with a frequency up to 5 mins, with the possibility of high and low glucose levels alarms and glucose trend information, that has been proven efficacious in diabetic patients in helping reducing HbA1c concentrations.125 The same tool was successfully applied in IAS,36,119 given its characteristics that allow a prompter recognition of hypoglycemic episodes and enhance patient’s compliance to self-monitoring. However, CGM suffers of a certain delay in reporting glycemic variations when compared to the direct measurement in the capillary blood through finger-sticks, and this is due to the lag time necessary to equilibrate blood and interstitial glucose concentrations. Flash glucose monitoring (FGM) is another monitoring tool that was applied successfully in the management of IAS.35 FGM is an intermittently-scanned continuous monitoring system. As a consequence, FGM is a low-cost non-invasive tool, useful for frequent monitoring of glucose concentrations, that enhances the patient self-monitoring by reducing the burden of finger-sticks. Compared to CGM, the pros of the FGM consist in its increased simplicity and lower cost, whereas its cons consist in the absence of an acoustic alarm for hypoglycaemic episodes. On the other hand, the tendency arrows provided by this system may help the patient in preventing downward glycemic fluctuations.126
The prognosis of the disease has not been investigated systematically, so no data regarding its survival rate are currently available. The recurrence rate of IAS following its full resolution is low: in the above-mentioned revision of 197 Japanese patients, only nine over 197 patients experienced recurrence of the hypoglycemic episodes, which accounts for a recurrence rate lower than 5%.22 Recurrence followed re-administration of the triggering drug only in a minority of patients, whereas the majority developed recurrence of the disease without any known triggering factor.22 Given that recurrence of the disease reappeared even one year following the last hypoglycemic episode, the timing of the correct follow-up is not clear.
Conclusion
Fifty years following its first description, IAS has been extensively reported and many important results have been accomplished in the research regarding this condition. Indeed, nowadays IAS is no longer considered a curious and rare disease mainly originating in Asian patients but has had a worldwide spread and its incidence seems definitely increasing, especially in western countries. This may be due to the wide diffusion of medications and substances that are well-known triggering factors in the pathogenesis of the disease, or to the larger awareness for this condition compared to the past decades. As a consequence, considering IAS in the differential diagnosis of hypoglycemia is nowadays mandatory, even outside the setting of patients of Asian ancestry. The diagnostic approach to IAS is complex, and the gold standard for the differential diagnosis with other forms of hypoglycemia consists in the measurement of insulin autoantibodies. As a consequence, a blood sample for the IAA assay should always be obtained in the suspect of IAS, even before proceeding to potentially useless and costly imaging examinations. If IAA assay is not available, the sample should be preliminarily tested with PEG precipitation, and then eventually sent to a lab that owns the kit for measuring the IAA. Once the diagnosis of IAS has been confirmed, the patients should be evaluated carefully in order to assess the indication to pharmacologic therapy, always taking into account that no study have currently compared different treatment regimens. IAS patients should be monitored thoroughly, both during the active phase of the disease and following its remission. To date, even though the research in this field has accomplished astonishing results, there are still some missing points, especially regarding the pathogenesis of the disease and its management. The need for medical trials that compare different treatment modalities is urgent, even though the recruitment of a sufficient amount of IAS patients is difficult, due to the rarity of the condition.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hirata Y, Ishizu H, Ouchi N. Insulin autoimmunity in a case of spontaneous hypoglycemia. J Jpn Diabetes Soc. 1970;13:312–320.
2. De Pirro R, Roth RA, Rossetti L, Goldfine ID. Characterization of the serum from a patient with insulin resistance and hypoglycemia. Evidence for multiple populations of insulin receptor antibodies with different receptor binding and insulin-mimicking activities. Diabetes. 1984;33(3):301–304. doi:10.2337/diab.33.3.301
3. Lupsa BC, Chong AY, Cochran EK, Soos MA, Semple RK, Gorden P. Autoimmune forms of hypoglycemia. Medicine (Baltimore). 2009;88(3):141–153. doi:10.1097/MD.0b013e3181a5b42e
4. Censi S, Mian C, Betterle C. Insulin autoimmune syndrome: from diagnosis to clinical management. Ann Transl Med. 2018;6(17):335. doi:10.21037/atm
5. Ishizuka T, Ogawa S, Mori T, et al. Characteristics of the antibodies of two patients who developed daytime hyperglycemia and morning hypoglycemia because of insulin antibodies. Diabetes Res Clin Pract. 2009;84(2):e21–e23. doi:10.1016/j.diabres.2009.02.007
6. Cryer PE, Axelrod L, Grossman AB, et al. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2009;94(3):709–728. doi:10.1210/jc.2008-1410
7. Hirata Y. Insulin Autoimmune Syndrome - the second case. J Jpn Diabetes Soc. 1972;15:187–192.
8. Folling I, Norman N. Hyperglycemia, hypoglycemic attacks, and production of anti-insulin antibodies without previous known immunization. Immunological and functional studies in a patient. Diabetes. 1972;21(7):814–826. doi:10.2337/diab.21.7.814
9. Hirata Y, Tominaga M, Ito JI, Noguchi A. Spontaneous hypoglycemia with insulin autoimmunity in Graves’ disease. Ann Intern Med. 1974;81(2):214–218. doi:10.7326/0003-4819-81-2-214
10. Oneda A, Matsuda K, Sato M, Yamagata S, Sato T. Hypoglycemia due to apparent autoantibodies to insulin. Characterization of insulin-binding protein. Diabetes. 1974;23(1):41–50. doi:10.2337/diab.23.1.41
11. Hirata Y. Methimazole and insulin autoimmune syndrome with hypoglycemia. Lancet (London, England). 1983;2(8357):1037–1038. doi:10.1016/S0140-6736(83)91031-0
12. Uchigata Y, Kuwata S, Tokunaga K, et al. Strong association of insulin autoimmune syndrome with HLA-DR4. Lancet (London, England). 1992;339(8790):393–394. doi:10.1016/0140-6736(92)90080-M
13. Uchigata Y, Hirata Y, Omori Y. A novel concept of type VII hypersensitivity introduced by insulin autoimmune syndrome (Hirata’s disease). Autoimmunity. 1995;20(3):207–208. doi:10.3109/08916939508993352
14. Uchigata Y, Hirata Y, Iwamoto Y. Drug-induced insulin autoimmune syndrome. Diabetes Res Clin Pract. 2009;83(1):e19–e20. doi:10.1016/j.diabres.2008.10.015
15. Ismail AA. The insulin autoimmune syndrome (IAS) as a cause of hypoglycaemia: an update on the pathophysiology, biochemical investigations and diagnosis. Clin Chem Lab Med. 2016;54(11):1715–1724. doi:10.1515/cclm-2015-1255
16. Takayama-Hasumi S, Eguchi Y, Sato A, Morita C, Hirata Y. Insulin autoimmune syndrome is the third leading cause of spontaneous hypoglycemic attacks in Japan. Diabetes Res Clin Pract. 1990;10(3):211–214. doi:10.1016/0168-8227(90)90063-Y
17. Yamada Y, Kitayama K, Oyachi M, et al. Nationwide survey of endogenous hyperinsulinemic hypoglycemia in Japan (2017-2018): congenital hyperinsulinism, insulinoma, non-insulinoma pancreatogenous hypoglycemia syndrome and insulin autoimmune syndrome (Hirata’s disease). J Diabetes Investig. 2019. doi:10.1111/jdi.13180
18. Woo CY, Jeong JY, Jang JE, et al. Clinical features and causes of endogenous hyperinsulinemic hypoglycemia in Korea. Diabetes Metab J. 2015;39(2):126–131. doi:10.4093/dmj.2015.39.2.126
19. Wang YL, Yao PW, Zhang XT, Luo ZZ, Wu PQ, Xiao F. Insulin autoimmune syndrome: 73 cases of clinical analysis. Chin Med J (Engl). 2015;128(17):2408–2409. doi:10.4103/0366-6999.163376
20. Uchigata Y, Hirata Y, Omori Y, Iwamoto Y, Tokunaga K. Worldwide differences in the incidence of insulin autoimmune syndrome (Hirata disease) with respect to the evolution of HLA-DR4 alleles. Hum Immunol. 2000;61(2):154–157. doi:10.1016/S0198-8859(99)00144-5
21. Hirata Y, Uchigata Y. Insulin autoimmune syndrome in Japan. Diabetes Res Clin Pract. 1994;24(Suppl):S153–S157. doi:10.1016/0168-8227(94)90243-7
22. Uchigata Y, Eguchi Y, Takayama-Hasumi S, Omori Y. Insulin autoimmune syndrome (Hirata disease): clinical features and epidemiology in Japan. Diabetes Res Clin Pract. 1994;22(2–3):89–94. doi:10.1016/0168-8227(94)90040-X
23. Lee SH, Oh SH, Chung WY. Insulin autoimmune syndrome induced by methimazole in a Korean girl with Graves’ disease. Ann Pediatr Endocrinol Metab. 2013;18(1):32–35. doi:10.6065/apem.2013.18.1.32
24. Alves C, Constanca J, De Leon DD, Snider K, Stanley C. A novel atypical presentation of insulin autoimmune syndrome (Hirata’s disease) in a child. J Pediatr Endocrinol Metab. 2013;26(11–12):1163–1166. doi:10.1515/jpem-2013-0215
25. Su CT, Lin YC. Hyperinsulinemic hypoglycemia associated with insulin antibodies caused by exogenous insulin analog. Endocrinol Diabetes Metab Case Rep. 2016;2016:16–0079.
26. Kobayashi S, Amano H, Kawaguchi Y, Yokoo T. A novel treatment of hyperinsulinemic hypoglycemia induced by insulin antibodies with alkali administration: a case report. J Med Case Rep. 2019;13(1):79. doi:10.1186/s13256-019-1989-8
27. Chen F, Yang J, Liu Y, et al. Insulin autoimmune syndrome: three case reports. Medicine (Baltimore). 2018;97(51):e13486. doi:10.1097/MD.0000000000013486
28. Betterle C, Zanchetta R. Update on autoimmune polyendocrine syndromes (APS). Acta Biomed. 2003;74(1):9–33.
29. Takei M. Insulin auto-antibodies produced by methimazole treatment in the patients with the Graves’ disease. J Tokyo Women’s Med Coll. 1980;50:54.
30. Uchigata Y, Omori Y, Nieda M, Kuwata S, Tokunaga K, Juji T. HLA-DR4 genotype and insulin-processing in insulin autoimmune syndrome. Lancet (London, England). 1992;340(8833):1467. doi:10.1016/0140-6736(92)92654-X
31. Uchigata Y, Tokunaga K, Nepom G, et al. Differential immunogenetic determinants of polyclonal insulin autoimmune syndrome (Hirata’s disease) and monoclonal insulin autoimmune syndrome. Diabetes. 1995;44(10):1227–1232. doi:10.2337/diab.44.10.1227
32. Uchigata Y, Kuwata S, Tsushima T, et al. Patients with Graves’ disease who developed insulin autoimmune syndrome (Hirata disease) possess HLA-Bw62/Cw4/DR4 carrying DRB1*0406. J Clin Endocrinol Metab. 1993;77(1):249–254. doi:10.1210/jcem.77.1.8325948
33. Uchigata Y. The novel agent, alpha lipoic acid, can cause the development of insulin autoimmune syndrome. Intern Med. 2007;46(17):1321–1322. doi:10.2169/internalmedicine.46.0221
34. Gullo D, Evans JL, Sortino G, Goldfine ID, Vigneri R. Insulin autoimmune syndrome (Hirata Disease) in European Caucasians taking alpha-lipoic acid. Clin Endocrinol (Oxf). 2014;81(2):204–209. doi:10.1111/cen.12334
35. Cappellani D, Sardella C, Campopiano MC, Falorni A, Marchetti P, Macchia E. Spontaneously remitting insulin autoimmune syndrome in a patient taking alpha-lipoic acid. Endocrinol Diabetes Metab Case Rep. 2018;2018:18–0122.
36. Reis MZR, Fernandes VO, Fontenele EGP, et al. Insulin autoimmune syndrome in an occidental woman: a case report and literature review. Arch Endocrinol Metab. 2018;62(5):566–570. doi:10.20945/2359-3997000000078
37. Zhang Y, Zhao T. Hypoglycemic coma due to insulin autoimmune syndrome induced by methimazole: a rare case report. Exp Ther Med. 2014;8(5):1581–1584. doi:10.3892/etm.2014.1964
38. Basu A, Service FJ, Yu L, Heser D, Ferries LM, Eisenbarth G. Insulin autoimmunity and hypoglycemia in seven white patients. Endocr Pract. 2005;11(2):97–103. doi:10.4158/EP.11.2.97
39. Hakamata M, Itoh M, Sudo Y, Miyata N. Insulin autoimmune syndrome after the third therapy with methimazole. Intern Med. 1995;34(5):410–412. doi:10.2169/internalmedicine.34.410
40. Jain N, Savani M, Agarwal M, Kadaria D. Methimazole-induced insulin autoimmune syndrome. Ther Adv Endocrinol Metab. 2016;7(4):178–181. doi:10.1177/2042018816658396
41. Gomez Cruz MJ, Jabbar M, Saini N, et al. Severe hypoglycemia secondary to methimazole-induced insulin autoimmune syndrome in a 16 year old African-American male. Pediatr Diabetes. 2012;13(8):652–655. doi:10.1111/pedi.2012.13.issue-8
42. Virally ML, Timsit J, Chanson P, Warnet A, Guillausseau PJ. Insulin autoimmune syndrome: a rare cause of hypoglycaemia not to be overlooked. Diabetes Metab. 1999;25(5):429–431.
43. Mettananda C, de Silva HJ, Fernando R. Hypoglycaemia and fits in a thyrotoxic man. BMJ Case Rep. 2009;2009. doi:10.1136/bcr.07.2008.0448
44. Wong ST, Ng WY, Thai AC. Case report: autoimmune insulin syndrome in a Chinese female with Graves’ disease. Ann Acad Med Singapore. 1996;25(6):882–885.
45. Lu CC, Lee JK, Lam HC, Yang CY, Han TM. Insulin autoimmune syndrome in a patient with methimazole and carbimazole-treated Graves’ disease: a case report. Zhonghua Yi Xue Za Zhi (Taipei). 1994;54(5):353–358.
46. Armitage M, Franklyn J, Scott-Morgan L, et al. Insulin autoantibodies in Graves’ disease–before and after carbimazole therapy. Diabetes Res Clin Pract. 1990;8(3):169–176. doi:10.1016/0168-8227(90)90113-8
47. Lin HD, Chen HD, Chang PY, Lin CY, Ching KN. Insulin autoimmune syndrome in methimazole or carbimazole treated Chinese patients of Graves’ disease. Zhonghua Yi Xue Za Zhi (Taipei). 1988;42(3):163–168.
48. Furukawa N, Miyamura N, Nishida K, Motoshima H, Taketa K, Araki E. Possible relevance of alpha lipoic acid contained in a health supplement in a case of insulin autoimmune syndrome. Diabetes Res Clin Pract. 2007;75(3):366–367. doi:10.1016/j.diabres.2006.07.005
49. Takeuchi Y, Miyamoto T, Kakizawa T, Shigematsu S, Hashizume K. Insulin Autoimmune Syndrome possibly caused by alpha lipoic acid. Intern Med. 2007;46(5):237–239. doi:10.2169/internalmedicine.46.1893
50. Izzo V, Greco C, Corradini D, et al. Insulin autoimmune syndrome in an Argentine woman taking alpha-lipoic acid: A case report and review of the literature. SAGE Open Med Case Rep. 2018;6:2050313X18819601.
51. Bresciani E, Bussi A, Bazzigaluppi E, Balestrieri G. Insulin autoimmune syndrome induced by alpha-lipoic acid in a Caucasian woman: case report. Diabetes Care. 2011;34(9):e146. doi:10.2337/dc11-0600
52. Ishida Y, Ohara T, Okuno Y, et al. Alpha-lipoic acid and insulin autoimmune syndrome. Diabetes Care. 2007;30(9):2240–2241. doi:10.2337/dc07-0689
53. Archambeaud-Mouveroux F, Canivet B, Fressinaud C, de Buhan B, Treves R, Laubie B. Autoimmune hypoglycemia: the fault of pyritinol? Presse Med. 1988;17(34):1733–1736.
54. Canivet B, Archambeaud F. Pyrithioxine and hypoglycemic autoimmune syndrome. Autoimmunity. 1988;1(4):321–322. doi:10.3109/08916938809010686
55. Deguchi A, Okauchi Y, Suehara S, Mineo I. Insulin autoimmune syndrome in a health supplement user: the effectiveness of cornstarch therapy for treating hypoglycemia. Intern Med. 2013;52(3):369–372. doi:10.2169/internalmedicine.52.7844
56. Blackshear PJ, Rotner HE, Kriauciunas KA, Kahn CR. Reactive hypoglycemia and insulin autoantibodies in drug-induced lupus erythematosus. Ann Intern Med. 1983;99(2):182–184. doi:10.7326/0003-4819-99-2-182
57. Burch HB, Clement S, Sokol MS, Landry F. Reactive hypoglycemic coma due to insulin autoimmune syndrome: case report and literature review. Am J Med. 1992;92(6):681–685. doi:10.1016/0002-9343(92)90787-C
58. Yamada E, Okada S, Saito T, Osaki A, Ozawa A, Yamada M. Insulin autoimmune syndrome during the administration of clopidogrel. J Diabetes. 2016;8(4):588–589. doi:10.1111/1753-0407.12385
59. Rajpal A, Kassem LS, Moscoso-Cordero M, Arafah BM. Clopidogrel-induced insulin autoimmune syndrome: a newly recognized cause of hypoglycemia in a patient without diabetes. J Endocr Soc. 2017;1(9):1217–1223. doi:10.1210/js.2017-00316
60. Feng X, Yuan L, Hu Y, et al. Gliclazide-induced insulin autoimmune syndrome: a rare case report and review on literature. Endocr Metab Immune Disord Drug Targets. 2016;16(4):230–234. doi:10.2174/1871530316666161223144558
61. Okazaki-Sakai S, Yoshimoto S, Yagi K, Wakasugi T, Takeda Y, Yamagishi M. Insulin autoimmune syndrome caused by an adhesive skin patch containing loxoprofen-sodium. Intern Med. 2013;52(21):2447–2451. doi:10.2169/internalmedicine.52.0570
62. Benson EA, Ho P, Wang C, Wu PC, Fredlund PN, Yueng RT. Insulin autoimmunity as a cause of hypoglycemia. Arch Intern Med. 1984;144(12):2351–2354. doi:10.1001/archinte.1984.00350220067015
63. Herranz L, Rovira A, Grande C, et al. Autoimmune insulin syndrome in a patient with progressive systemic sclerosis receiving penicillamine. Horm Res. 1992;37(1–2):78–80. doi:10.1159/000182286
64. Lidar M, Rachmani R, Half E, Ravid M. Insulin autoimmune syndrome after therapy with imipenem. Diabetes Care. 1999;22(3):524–525. doi:10.2337/diacare.22.3.524a
65. Cavaco B, Uchigata Y, Porto T, Amparo-Santos M, Sobrinho L, Leite V. Hypoglycaemia due to insulin autoimmune syndrome: report of two cases with characterisation of HLA alleles and insulin autoantibodies. Eur J Endocrinol. 2001;145(3):311–316. doi:10.1530/eje.0.1450311
66. Ma WY, Won JG, Tang KT, Lin HD. Severe hypoglycemic coma due to insulin autoimmune syndrome. J Chin Med Assoc. 2005;68(2):82–86. doi:10.1016/S1726-4901(09)70140-6
67. Gopal K, Priya G, Gupta N, Praveen EP, Khadgawat R. A case of autoimmune hypoglycemia outside Japan: rare, but in the era of expanding drug-list, important to suspect. Indian J Endocrinol Metab. 2013;17(6):1117–1119. doi:10.4103/2230-8210.122644
68. Sahni P, Trivedi N, Omer A. Insulin Autoimmune Syndrome: a rare cause of postprandial hypoglycemia. Endocrinol Diabetes Metab Case Rep. 2016;2016:16–0064.
69. Kamei S, Kaneto H, Shigemoto R, et al. Human serum albumin: possible cause of insulin autoimmune syndrome. J Diabetes Investig. 2016;7(6):919–920. doi:10.1111/jdi.2016.7.issue-6
70. Papanas N, Ziegler D. Efficacy of alpha-lipoic acid in diabetic neuropathy. Expert Opin Pharmacother. 2014;15(18):2721–2731. doi:10.1517/14656566.2014.972935
71. Vallianou N, Evangelopoulos A, Koutalas P. Alpha-lipoic acid and diabetic neuropathy. Rev Diabet Stud. 2009;6(4):230–236. doi:10.1900/RDS.2009.6.230
72. Pieralice S, Vari R, Minutolo A, et al. Biomarkers of response to alpha-lipoic acid ± palmitoiletanolamide treatment in patients with diabetes and symptoms of peripheral neuropathy. Endocrine. 2019;66(2):178–184. doi:10.1007/s12020-019-01917-w
73. Fruzzetti F, Fidecicchi T, Palla G, Gambacciani M. Long-term treatment with alpha-lipoic acid and myo-inositol positively affects clinical and metabolic features of polycystic ovary syndrome. Gynecol Endocrinol. 2020;36(2):152–155. doi:10.1080/09513590.2019.1640673
74. Holmquist L, Stuchbury G, Berbaum K, et al. Lipoic acid as a novel treatment for Alzheimer’s disease and related dementias. Pharmacol Ther. 2007;113(1):154–164. doi:10.1016/j.pharmthera.2006.07.001
75. Hattori N, Duhita MR, Mukai A, Matsueda M, Shimatsu A. Development of insulin antibodies and changes in titers over a long-term period in patients with type 2 diabetes. Clin Chim Acta. 2014;433:135–138. doi:10.1016/j.cca.2014.03.008
76. Matsushita S, Takahashi K, Motoki M, Komoriya K, Ikagawa S, Nishimura Y. Allele specificity of structural requirement for peptides bound to HLA-DRB1*0405 and -DRB1*0406 complexes: implication for the HLA-associated susceptibility to methimazole-induced insulin autoimmune syndrome. J Exp Med. 1994;180(3):873–883. doi:10.1084/jem.180.3.873
77. Halsall DJ, Mangi M, Soos M, et al. Hypoglycemia due to an insulin binding antibody in a patient with an IgA-kappa myeloma. J Clin Endocrinol Metab. 2007;92(6):2013–2016. doi:10.1210/jc.2007-0075
78. Church D, Cardoso L, Bradbury S, et al. Diagnosis of insulin autoimmune syndrome using polyethylene glycol precipitation and gel filtration chromatography with ex vivo insulin exchange. Clin Endocrinol (Oxf). 2017;86(3):347–353. doi:10.1111/cen.2017.86.issue-3
79. Moreira RO, Lima GA, Peixoto PC, Farias ML, Vaisman M. Insulin autoimmune syndrome: case report. Sao Paulo Med J. 2004;122(4):178–180. doi:10.1590/S1516-31802004000400010
80. Elias D, Cohen IR, Schechter Y, Spirer Z, Golander A. Antibodies to insulin receptor followed by anti-idiotype. Antibodies to insulin in child with hypoglycemia. Diabetes. 1987;36(3):348–354. doi:10.2337/diab.36.3.348
81. Eguchi Y. Scatchard analysis of insulin autoantibodies in the insulin autoimmune syndrome. J Tokyo Women’s Med Coll. 1989;59:1286–1305.
82. Iizuka K, Tomita R, Horikawa Y, Takeda J. A case of glycemic instability and insulin allergy due to anti-insulin antibodies in a patient with type 2 diabetes. Diabetol Int. 2012;3(4):233–238. doi:10.1007/s13340-012-0077-8
83. Tamura Y, Kimbara Y, Funatsuki S, et al. A case of insulin antibody-induced glucose instability in an elderly woman with type 2 diabetes on hemodialysis, successfully ameliorated with liraglutide. Diabetol Int. 2013;4(1):71–75. doi:10.1007/s13340-012-0100-0
84. Sodoyez JC, Sodoyez-Goffaux F, Koch M, et al. Clonally restricted insulin autoantibodies in a cohort of 2200 healthy blood donors. Diabetologia. 1990;33(12):719–725. doi:10.1007/BF00400341
85. Redmon JB, Nuttall FQ. Autoimmune hypoglycemia. Endocrinol Metab Clin North Am. 1999;28(3):603–618, vii. doi:10.1016/S0889-8529(05)70090-6
86. Ismail AA. The double whammy of endogenous insulin antibodies in non-diabetic subjects. Clin Chem Lab Med. 2008;46(2):153–156. doi:10.1515/CCLM.2008.031
87. Uchigata Y, Hirata Y. Insulin autoimmune syndrome (IAS, Hirata disease). Ann Med Interne (Paris). 1999;150(3):245–253.
88. Martens P, Tits J. Approach to the patient with spontaneous hypoglycemia. Eur J Intern Med. 2014;25(5):415–421. doi:10.1016/j.ejim.2014.02.011
89. Cryer PE. Hypoglycemia, functional brain failure, and brain death. J Clin Invest. 2007;117(4):868–870. doi:10.1172/JCI31669
90. Vogeser M, Parhofer KG, Furst H, Jacob K, Brodl UC, Seidel D. Autoimmune hypoglycemia presenting as seizure one week after surgery. Clin Chem. 2001;47(4):795–796. doi:10.1093/clinchem/47.4.795
91. Wong SL, Priestman A, Holmes DT. Recurrent hypoglycemia from insulin autoimmune syndrome. J Gen Intern Med. 2014;29(1):250–254. doi:10.1007/s11606-013-2588-9
92. International Hypoglycaemia Study G. Glucose concentrations of less than 3.0 mmol/L (54 mg/dL) should be reported in clinical trials: a joint position statement of the american diabetes association and the european association for the study of diabetes. Diabetes Care. 2017;40(1):155–157. doi:10.2337/dc16-2215
93. Ratner RE. Hypoglycemia: new Definitions and Regulatory Implications. Diabetes Technol Ther. 2018;20(S2):S250–S253. doi:10.1089/dia.2018.0113
94. Yuan T, Li J, Li M, et al. Insulin autoimmune syndrome diagnosis and therapy in a single chinese center. Clin Ther. 2019;41(5):920–928. doi:10.1016/j.clinthera.2019.03.009
95. Censi S, Albergoni MP, Gallo N, Plebani M, Boscaro M, Betterle C. Insulin autoimmune syndrome (Hirata’s disease) in an Italian patient: a case report and review of the literature. Clin Chem Lab Med. 2018;56(6):889–895. doi:10.1515/cclm-2017-0392
96. Owen WE, Roberts WL. Cross-reactivity of three recombinant insulin analogs with five commercial insulin immunoassays. Clin Chem. 2004;50(1):257–259. doi:10.1373/clinchem.2003.026625
97. Marks V, Teale JD. Drug-induced hypoglycemia. Endocrinol Metab Clin North Am. 1999;28(3):555–577. doi:10.1016/S0889-8529(05)70088-8
98. Lebowitz MR, Blumenthal SA. The molar ratio of insulin to C-peptide. An aid to the diagnosis of hypoglycemia due to surreptitious (or inadvertent) insulin administration. Arch Intern Med. 1993;153(5):650–655. doi:10.1001/archinte.1993.00410050082011
99. Ismail AA. Testing for insulin antibodies is mandatory in the differential diagnosis of hypoglycaemia in nondiabetic subjects. Clin Endocrinol (Oxf). 2012;76(4):603–604. doi:10.1111/cen.2012.76.issue-4
100. Scatchard G. The attractions of proteins for small molecules and ions. Ann N Y Acad Sci. 1949;51(4):660–672. doi:10.1111/nyas.1949.51.issue-4
101. Eguchi Y, Uchigata Y, Yao K, Yokoyama H, Hirata Y, Omori Y. Longitudinal changes of serum insulin concentration and insulin antibody features in persistent insulin autoimmune syndrome (Hirata’s disease). Autoimmunity. 1994;19(4):279–284. doi:10.3109/08916939409071354
102. Service FJ, McMahon MM, O’Brien PC, Ballard DJ. Functioning insulinoma–incidence, recurrence, and long-term survival of patients: a 60-year study. Mayo Clin Proc. 1991;66(7):711–719. doi:10.1016/S0025-6196(12)62083-7
103. Grimaldi F, Fazio N, Attanasio R, et al. Italian Association of Clinical Endocrinologists (AME) position statement: a stepwise clinical approach to the diagnosis of gastroenteropancreatic neuroendocrine neoplasms. J Endocrinol Invest. 2014;37(9):875–909. doi:10.1007/s40618-014-0119-0
104. Mehrabi A, Fischer L, Hafezi M, et al. A systematic review of localization, surgical treatment options, and outcome of insulinoma. Pancreas. 2014;43(5):675–686. doi:10.1097/MPA.0000000000000110
105. Service FJ, Natt N, Thompson GB, et al. Noninsulinoma pancreatogenous hypoglycemia: a novel syndrome of hyperinsulinemic hypoglycemia in adults independent of mutations in Kir6.2 and SUR1 genes. J Clin Endocrinol Metab. 1999;84(5):1582–1589. doi:10.1210/jcem.84.5.5645
106. Thompson GB, Service FJ, Andrews JC, et al. Noninsulinoma pancreatogenous hypoglycemia syndrome: an update in 10 surgically treated patients. Surgery. 2000;128(6):
107. Malik S, Mitchell JE, Steffen K, et al. Recognition and management of hyperinsulinemic hypoglycemia after bariatric surgery. Obes Res Clin Pract. 2016;10(1):1–14. doi:10.1016/j.orcp.2015.07.003
108. Ritz P, Hanaire H. Post-bypass hypoglycaemia: a review of current findings. Diabetes Metab. 2011;37(4):274–281. doi:10.1016/j.diabet.2011.04.003
109. Marks V, Teale JD. Hypoglycemia: factitious and felonious. Endocrinol Metab Clin North Am. 1999;28(3):579–601. doi:10.1016/S0889-8529(05)70089-X
110. Service FJ, Palumbo PJ. Factitial hypoglycemia. Three cases diagnosed on the basis of insulin antibodies. Arch Intern Med. 1974;134(2):336–340. doi:10.1001/archinte.1974.00320200146022
111. Arioglu E, Andewelt A, Diabo C, Bell M, Taylor SI, Gorden P. Clinical course of the syndrome of autoantibodies to the insulin receptor (type B insulin resistance): a 28-year perspective. Medicine (Baltimore). 2002;81(2):87–100. doi:10.1097/00005792-200203000-00001
112. Chu JP, Zheng XW, Lu J, et al. Insulin-induced autoimmune syndrome: A case report. Exp Ther Med. 2016;12(5):3359–3362. doi:10.3892/etm.2016.3767
113. Philippon M, Sejil S, Mugnier M, et al. Use of the continuous glucose monitoring system to treat insulin autoimmune syndrome: quantification of glucose excursions and evaluation of treatment efficacy. Diabet Med. 2014;31(7):e20–e24. doi:10.1111/dme.2014.31.issue-7
114. Savas-Erdeve S, Yilmaz Agladioglu S, Onder A, et al. An uncommon cause of hypoglycemia: insulin autoimmune syndrome. Horm Res Paediatr. 2014;82(4):278–282. doi:10.1159/000362758
115. Schlemper RJ, Uchigata Y, Frolich M, Vingerhoeds AC, Meinders AE. Recurrent hypoglycaemia caused by the insulin autoimmune syndrome: the first Dutch case. Neth J Med. 1996;48(5):188–192. doi:10.1016/0300-2977(95)00085-2
116. Church D, Cardoso L, Kay RG, et al. Assessment and management of anti-insulin autoantibodies in varying presentations of insulin autoimmune syndrome. J Clin Endocrinol Metab. 2018;103(10):3845–3855. doi:10.1210/jc.2018-00972
117. Paiva ES, Pereira AE, Lombardi MT, et al. Insulin autoimmune syndrome (Hirata disease) as differential diagnosis in patients with hyperinsulinemic hypoglycemia. Pancreas. 2006;32(4):431–432. doi:10.1097/01.mpa.0000220872.18153.72
118. Panikar V, Joshi S, Vadgama J, et al. Autoimmune hypoglycemia relapse on glucocorticoids, effectively treated with azathioprine. J Assoc Physicians India. 2018;66(12):78–79.
119. Saxon DR, McDermott MT, Michels AW. Novel management of insulin autoimmune syndrome with rituximab and continuous glucose monitoring. J Clin Endocrinol Metab. 2016;101(5):1931–1934. doi:10.1210/jc.2016-1097
120. Church D, Hunter RW, Lyall M, et al. Resolution of Hypoglycemia and Cardiovascular Dysfunction After Rituximab Treatment of Insulin Autoimmune Syndrome. Diabetes Care. 2017;40(7):e80–e82. doi:10.2337/dc17-0264
121. Kroemer TM, Erler A, Tsourdi E, et al. Immunoadsorption followed by rituximab as a definitive treatment for insulin autoimmune syndrome (Hirata Syndrome): a case report. Diabetes Care. 2018;41(3):e23–e24. doi:10.2337/dc17-1974
122. Yu L, Herold K, Krause-Steinrauf H, et al. Rituximab selectively suppresses specific islet antibodies. Diabetes. 2011;60(10):2560–2565. doi:10.2337/db11-0674
123. Dozio N, Scavini M, Beretta A, et al. Imaging of the buffering effect of insulin antibodies in the autoimmune hypoglycemic syndrome. J Clin Endocrinol Metab. 1998;83(2):643–648. doi:10.1210/jcem.83.2.4599
124. Yaturu S, DePrisco C, Lurie A. Severe autoimmune hypoglycemia with insulin antibodies necessitating plasmapheresis. Endocr Pract. 2004;10(1):49–54. doi:10.4158/EP.10.1.49
125. Beck RW, Riddlesworth T, Ruedy K, et al. Effect of continuous glucose monitoring on glycemic control in adults with type 1 diabetes using insulin injections: the DIAMOND randomized clinical trial. JAMA. 2017;317(4):371–378. doi:10.1001/jama.2016.19975
126. Kudva YC, Ahmann AJ, Bergenstal RM, et al. Approach to using trend arrows in the freestyle libre flash glucose monitoring systems in adults. J Endocr Soc. 2018;2(12):1320–1337. doi:10.1210/js.2018-00294
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.