Back to Journals » International Journal of Women's Health » Volume 14
Insecticide-Treated Nets Utilization and Associated Factors Among Pregnant Women in Miesso Woreda, Eastern Ethiopia: Observational Study
Authors Tesfaye T, Mengistie B ![]() , Egata G, Bekele H
, Egata G, Bekele H ![]() , BT Merga
, BT Merga ![]() , Eshetu B, Balis B
, Eshetu B, Balis B ![]()
Received 11 January 2022
Accepted for publication 18 March 2022
Published 31 March 2022 Volume 2022:14 Pages 445—453
DOI https://doi.org/10.2147/IJWH.S357942
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Tigist Tesfaye,1 Bezatu Mengistie Alemu,2 Gudina Egata,2 Habtamu Bekele,3 Bedasa Taye Merga,2 Bajrond Eshetu,3 Bikila Balis3
1Department of Public Health, Oromia Regional Health Bureau, Addis Ababa, Ethiopia; 2School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 3Department of Midwifery, School of Nursing and Midwifery, College of Health and Medical Science, Haramaya University, Harar, Ethiopia
Correspondence: Bikila Balis, School of Nursing, College of Health and Medical Science, Haramaya University, P.O. Box: 235, Harar, Ethiopia, Tel +251921788619, Email [email protected]
Background: Even though most sub-Saharan Africa adopted the World Health organization guidelines for malaria prevention, the coverage of insecticide-treated nets by pregnant women is low, where 28 million pregnant women did not receive insecticide-treated nets services. Likewise, only 13– 51.4% of pregnant women utilize insecticide-treated nets in Ethiopia.
Methods: A community-based cross-sectional study was conducted in Miesso woreda from April 01 to 30, 2017, among 424 pregnant women. A multi-stage cluster sampling technique was used to select the study participants. A structured interviewer-based administered questionnaire and observational checklist were used to collect the data. The collected data were entered into Epi data version 3.1 and exported to SPSS version 23 for analysis. Multiple logistic regression models were fitted to identify factors associated with insecticide-treated nets utilization. Adjusted odds ratios along 95% CI were estimated to measure the strength of the association and declared statistical significance at a p-value < 0.05.
Results: Of a total respondents, 39.9% (95% CI: 34.9– 44.2%) utilize insecticide-treated nets. Pregnant women from rural (AOR = 2.05, 95% CI: 1.14, 3.38), employed women (AOR = 1.80, 95% CI: 1.13, 2.86), monthly income > 1050 Ethiopian total birr (AOR = 2.02, 95% CI: 1.06, 3.84), third trimester pregnancy (AOR = 2.19, 95% CI: 1.09, 4.40), and having antenatal care for current pregnancy (AOR = 3.86, 95% CI: 1.63, 9.10) were factors significantly associated with insecticide-treated nets.
Conclusion: The utilization of insecticide-treated nets is relatively low. Residence, occupational status, monthly income, stage of pregnancy, and antenatal care status were factors significantly associated with insecticide-treated net utilization among pregnant women.
Keywords: insecticide-treated nets, malaria, pregnant women, Miesso woreda, Ethiopia
Introduction
Malaria remains a significant world challenge an estimated 214 million new cases of malaria and 438,000 deaths occurred in 2015 despite the progress achieved towards malaria burden reduction and achieving elimination in developed countries.1 It is causing an unacceptable toll on the health and economic welfare, particularly in sub-Saharan African countries. Most malaria cases (88%) and deaths (90%) occurred in the World health organization (WHO) African Region in 2015.2
Malaria in pregnancy has serious health consequences for the mother, fetus, and newborn which can be preventable with inexpensive and cost-effective interventions that are available for over a decade.2,3 Malaria is associated with poor outcomes; maternal anemia, intrauterine growth restriction, low birth weight, and premature delivery.4 Worldwide an estimate of 200,000 infant deaths and 100,000 neonatal deaths occur annually, and 18% of global neonatal mortality are attributable to malaria.5
To avert all these poor outcomes, WHO recommends implementation of intermittent preventive treatment of malaria in pregnancy using sulfadoxine (1500mg)-pyrimethamine (75mg) (IPTp-SP) together with the distribution of insecticide-treated nets (ITNs) for all pregnant women attending antenatal care (ANC) services; receive IPTp-SP at each ANC visit until delivery, starting in the second-trimester of pregnancy, with subsequent doses provided at least one month apart.2,6
Even though most sub-Saharan Africa adopted WHO guidelines for malaria prevention, coverage of ITNs in pregnant women is still low where 28 million of pregnant women do not receive ITNs services. Likewise in Ethiopia only 13–51.4% pregnant women utilize ITNs,7–13 and factors associated with ITNs utilization varies from study to study.7,14–16 Moreover, in Ethiopia transmission of malaria is mostly seasonal and unstable in characteristics, it is predisposing majority of the pregnant women to frequent and often large scale epidemics. Even though, malaria is endemic in Miesso woreda there is no information about the level of ITNs utilization among pregnant women. Therefore, this study aimed to assess utilization of ITNs and its associated factors among pregnant women in Miessio woreda, Eastern Ethiopia.
Methods and Materials
Study Setting, Design and Period
A community-based quantitative cross-sectional study was conducted in Miesso woreda found in west Hararghe zone, Eastern Ethiopia from April 01–30, 2017. The woreda is located 301 km away from Addis Ababa and 25 km from Chiro the capital city of the west Hararghe zone. According to the 2007 statistical report of the population and housing census of Ethiopia, the woreda has a total population of 125,644 of whom 64,079 were male and 61,565 female.17 The woreda has 32,040 urban and 93, 604 rural populations. Also, the woreda has 2 urban kebeles and 30 rural kebeles. There are 3 health centers and 32 health posts in the woreda. The woreda was found at a longitude of 9°14ʹN 40° 45ʹE/9.233° N 40.750°E and altitude of 1394–1505 meters above sea level. Geographically, the woreda is located in the low land where most of its population is at risk of malaria. The woreda has a temperature between 29–37 °C and the majority of the populations in the woreda are pastoralists and small scale living with agriculture.
Sample Size Determination
The sample size was determined using a single population proportion formula with assumptions; prevalence of bed nets utilization among pregnant women to be 15.8% according to the study conducted in Southern Ethiopia,10 level of confidence 95%=1.96, margin of error 5% (d = 0.05), and design effect-2. Therefore for this study, a sample size of 444 was used with design effects of two and 10% non-respondent rate.
Sampling Technique, Study Population and Eligibility Criteria
A multi-stage cluster sampling technique was used to select the study participants. A list of all kebeles in the woreda was used as a sampling frame. All kebeles identified by the district health extension workers were selected and taken as the primary sampling unit. Fifty percent of urban kebeles and 33% of rural kebeles were selected by the Lottery method using the list of each cluster as a sampling frame. Hence, one urban kebeles and ten rural kebeles were selected. In the second stage, households in each randomly selected kebeles were used as secondary sampling units. The number of households to be selected from each identified kebele was determined by the households (population) proportion of respective kebeles. Pregnant women who were residents of Miesso woreda for greater than or equal to six months were included. Pregnant women who were mentally and critically ill and not able to speak at the time of data collection were excluded.
Data Collection Tools, Procedures, and Measurement
A structured questionnaire and observational checklists were adapted from different published literatures10,18–20 and was designed to obtain participant information on socio-demographic characteristics, obstetrics factors, knowledge and utilization of ITNs.
The questionnaire initially was prepared in English and then translated to local language Afan Oromo then back to English version to ensure consistency. Data were collected by interviewer-administered questionnaires supported with direct observation for ITN utilization by eleven trained clinical nurses as data collector and two health officers as supervisor.
Utilization of ITNs was measured by pregnant women report of utilizing ITNs supplemented by observation of the households of pregnant women as they hanged (mounted) ITNs over their bed or sleeping area. Pregnant women sleeping under the ITNs during the early morning of observation day were categorized as they were utilized ITNs and vice versa.18,20,21
Data Quality Control
To ensure data quality, an appropriate data collection instrument was adapted. A pretest was conducted on 5% of the sample size in nearby kebeles which was not one of the recruitment sites for the main study, following which the questionnaire was revised, edited and any questions found to be unclear or ambiguous were removed or corrected accordingly. Trained data collectors were regularly supervised for proper data collection; all the questionnaires were checked for completeness and consistency on a daily basis by supervisors and principal investigator.
Data Processing and Analysis
The collected data were entered to Epi data version 3.1, cleaned, and transported to SPSS version 23.0 for data analysis. Descriptive statistics: frequencies and percentages were used to summarize the data. Continuous data distribution was checked using histogram and probability plot. Bivariate analysis was employed to identify factors associated with insecticide-treated nets. Variables that showed an association in the bivariate analysis with p < 0.25 were entered into a multivariate logistic regression model. Finally, the multivariate logistic regression model was used after controlling for confounding factors using regression. Hosmer-Lemeshow’s goodness of fit test was used to assess whether the necessary assumptions for the application of multivariate logistic regression had been fulfilled (0.86). Multi-co-linearity was assessed using standard error, and the variables were entered into the multivariate model without multi-co-linearity. Adjusted odds ratios (AOR) were calculated with 95% CIs, and statistical significance was declared at p≤ 0.05.
Ethical Considerations
Ethical approval was obtained from the Institutional Review Board of Haramaya University, College of Health and Medical Sciences (Ref.No. IHRERC/036/2017). More importantly, written informed consent was obtained from each randomly selected kebele leader, a study participant, and someone with parental/husband responsibility for participants aged less than 18 years. This study was conducted in accordance with the Declaration of Helsinki.
Results
Socio-Demographic Characteristics of Pregnant Women
In this study, a total of 424 pregnant women were interviewed out of 444, with a response rate of 95.5%. The mean age of respondents was 27.44 (± SD 5.27) years old. The majority (58.7%) of the women were in the 25–34 years age group, and almost all (96.7%) were married. Seven out of ten (69.6%) of the women were unemployed. Regarding the address of the pregnant women, three-fourths (75.2%) were rural residents. Similarly, three-fourths (74.1%) of the respondents had no formal education. The majority of the respondents were Oromo by ethnic (93.7% and Muslim followers (95.0%) (Table 1).
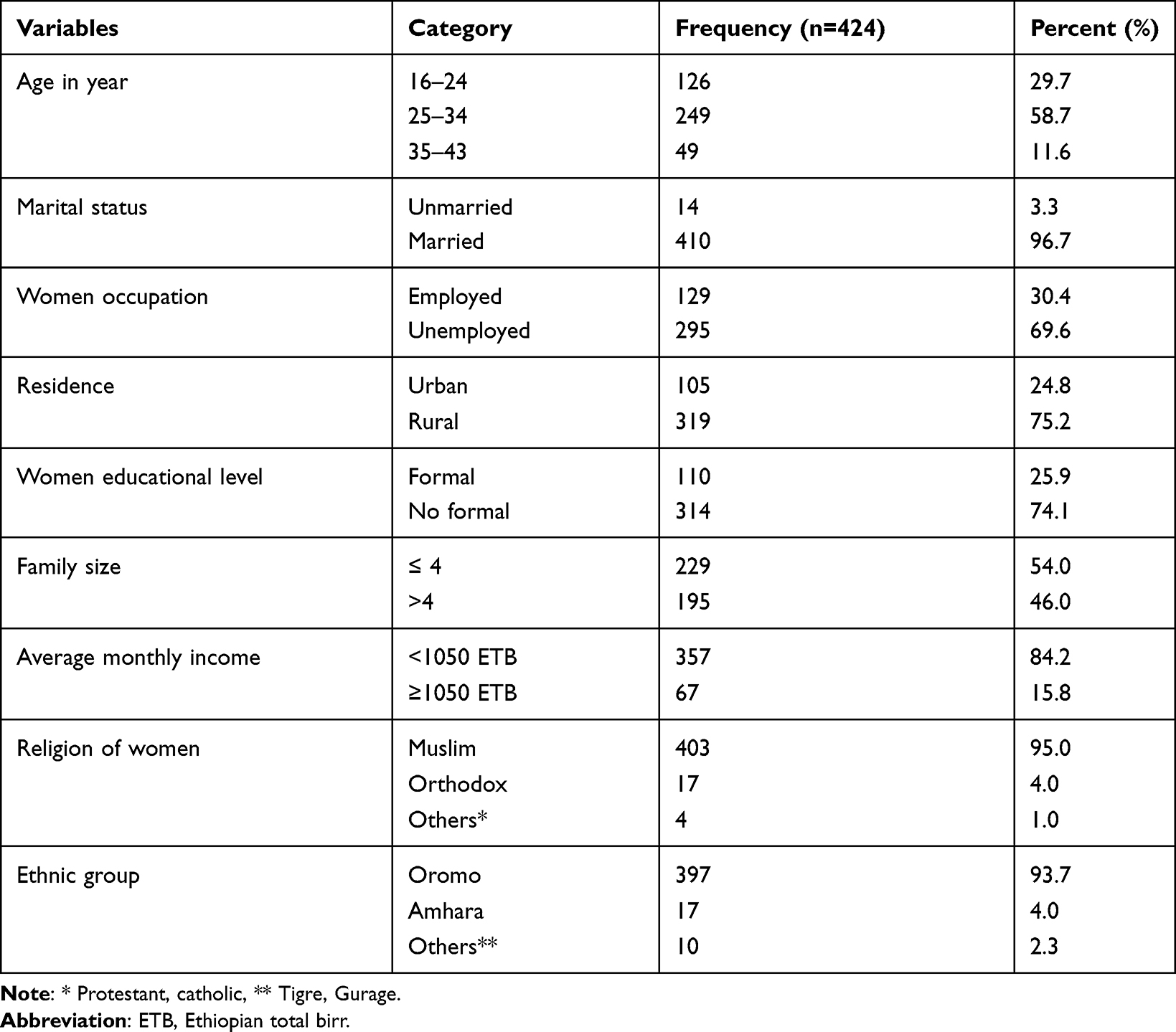 |
Table 1 Socio-Demographic Characteristics of Pregnant Women in Miesso Woreda, Eastern Ethiopia, 2017 |
Obstetrics Characteristics of Pregnant Women
Regarding the parity of the respondents, the majority (83.5%) were primipara. The third trimester is the most common stage of pregnancy of the respondents accounting for (46.5%) followed by the second trimester (42.2%). Nine out of ten (89.4%) pregnant women have antenatal care (ANC) for current pregnancy, and of majority (47.5%) have two visit (Table 2).
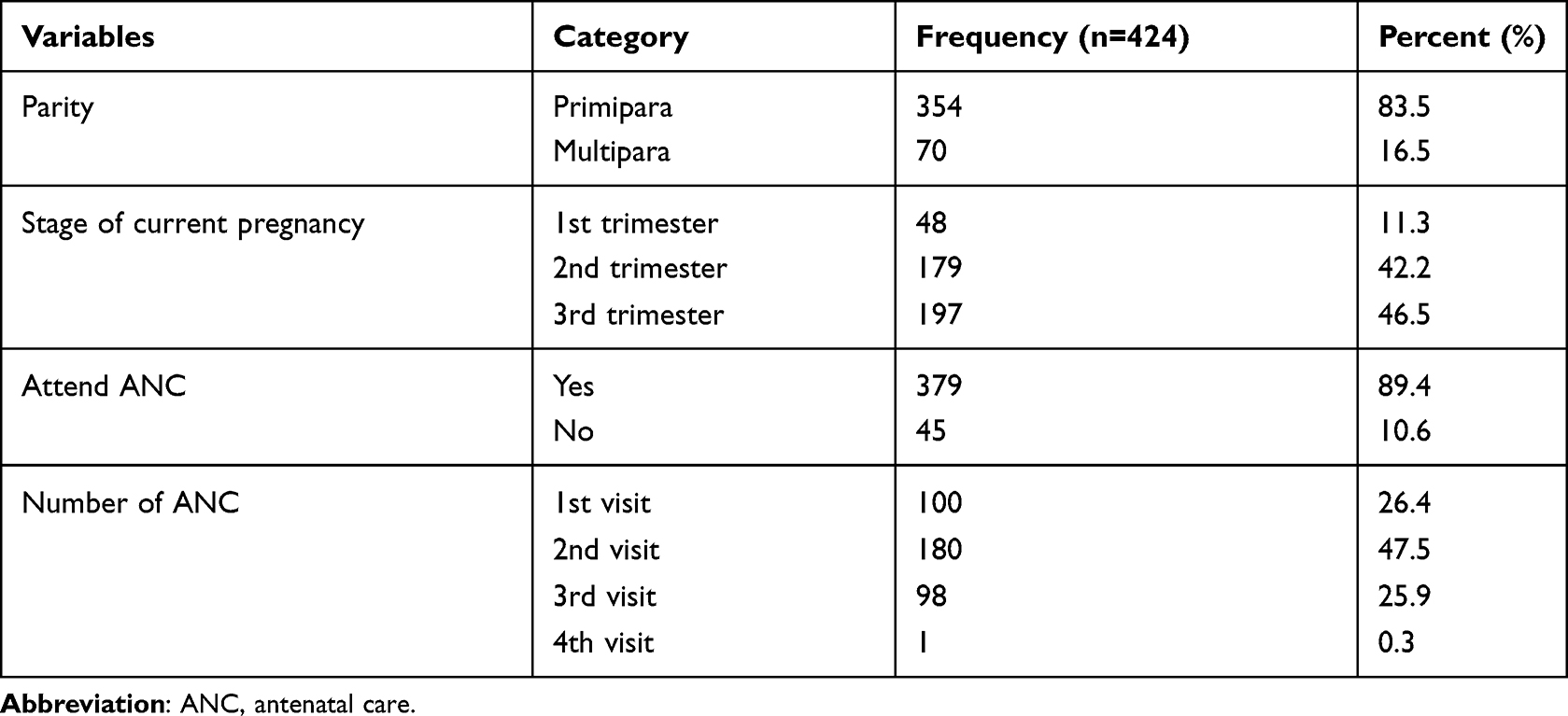 |
Table 2 Obstetrics Characteristics of Pregnant Women in Miesso Woreda, Eastern Ethiopia, 2017 |
Knowledge of ITNs
Among the respondents, the majority (97.9%) of the pregnant women have heard about ITNs, and a half (50.5%) of them heard from health providers. Regarding the source of ITNs, community volunteers account for more than half (50.7%). According to respondents’ responses, pregnant women were a higher risk group for malaria, and they have to take priority for ITNs (63.7% vs 82.5%). More than seven out of ten (70.8%) responded as ITNs kill mosquitoes (Table 3).
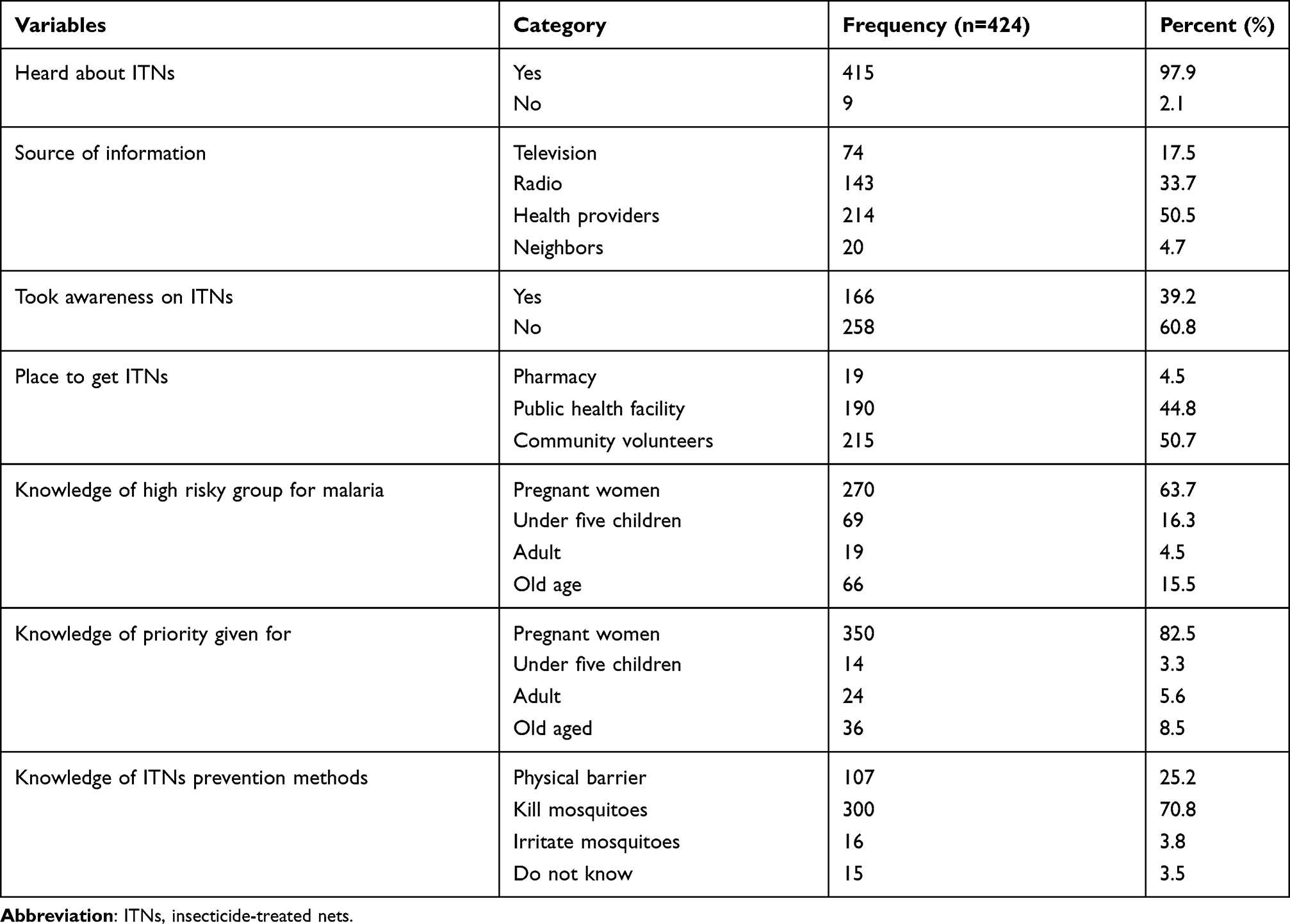 |
Table 3 Knowledge of ITNs Among Pregnant Women in Miesso Woreda, Eastern Ethiopia, 2017 |
Utilization of ITNs Among Pregnant Women
Of the total pregnant women who partook in the study, 39.9% (95% CI: 34.9, 44.2%) were utilized ITNs. More than eight out of ten (82.2%) pregnant women reported that they had slept under the ITNs last night. Regarding season for ITNs utilization, the majority (58%) utilized every season followed by the rainy season (32.5%). Of the total respondents, the majority (94.1%) pointed out they use ITNs for the prevention of Malaria (Table 4).
 |
Table 4 Utilization of ITNs Among Pregnant Women in Miesso Woreda, Eastern Ethiopia, 2017 |
Factors Associated with ITNs Utilization
In bivariate analysis, maternal age, maternal education, place of residence, marital status, occupational status, family size, antenatal care, monthly income, parity, stage of current pregnancy, and knowledge about ITNs were factors significantly associated with ITNs utilization at p-value ≤ 0.05.
In multivariate logistic regression analysis, the odds of ITNs utilization was almost two times higher among pregnant women who come from urban compared to those who come from rural (AOR=2.05, 95% CI: 1.14, 3.38). The odds of ITNs utilization was 1.80 times higher among employed compared to unemployed pregnant women (AOR=1.80, 95% CI: 1.13, 2.86). Similarly, pregnant women who have a monthly income of greater than 1050 birr were two times more likely to utilize ITNs than those who have ≤ 1050 birr (AOR=2.02, 95% CI: 1.06, 3.84). Third trimester pregnant women were 2.19 times more likely to utilize ITNs than first-trimester pregnant women (AOR=2.19, 95% CI: 1.09, 4.40). Also, pregnant women who have ANC for current pregnancy were 3.86 times more likely to utilize ITNs than their counterparts (AOR=3.86, 95% CI: 1.63, 9.10) (Table 5).
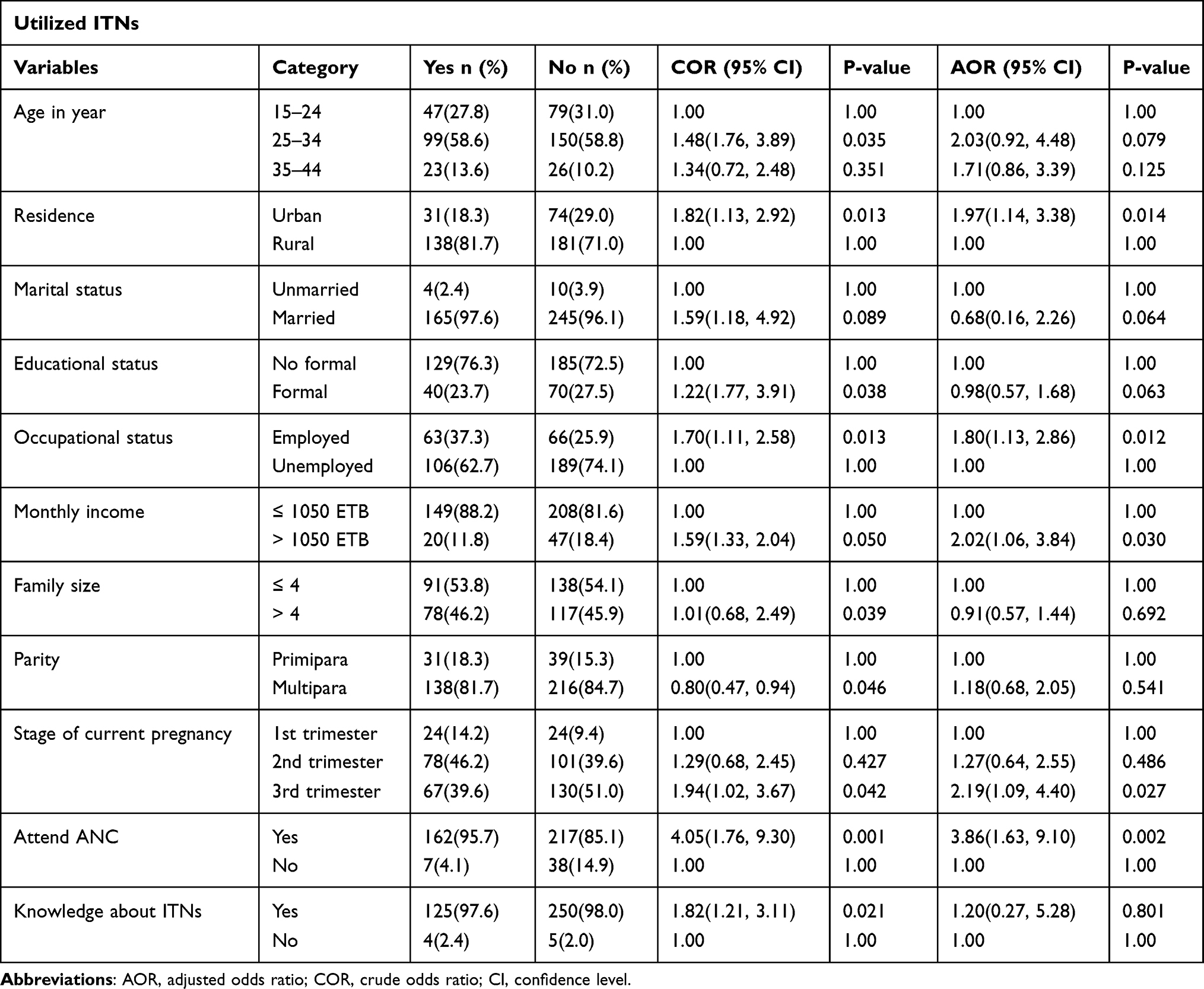 |
Table 5 Factors Associated with ITNs Utilization Among Pregnant Women in Miesso Woreda, Eastern Ethiopia, 2017 |
Discussion
There is few data regarding ITNs utilization among pregnant women in Ethiopia, and there is no study conducted in this study area. Therefore this study provides vital information regarding ITNs utilization among pregnant women as well as the associated factors.
Nearly four out of ten (39.9%) of the pregnant women were utilized ITNs. This finding is consonant with study findings in Adama (43.1%),12 Gida Ayana (37.1%),9 and Awabel district (33.6%).13 However, this finding is higher than the findings of the studies conducted in Shoshogo district (15.8%)10 and Benishangul (23.1%).11 This difference implies as time elapsed pregnant women became more familiar with malaria prevention methods such as ITNs utilization. Even though malaria is endemic in this study area, ITNs utilization by pregnant women was lower than the findings of the studies conducted in Kenya (70.5%),22 Gambella (51.4%),23 Northwest Ethiopia (56.5%),24 Damot district (63.1%),14 and Alamata district (69%).7 The reasons for the disparity could be most populations of Miessio woreda are pastoralists and live by livestock which makes it difficult for them to access ITNs and get information about malaria prevention methods. This difference implies as the governments, and different health sectors have to give more emphasis and invest in malaria prevention through ITNs provision for pregnant women and the community as a whole.
The odds of ITNs utilization was two times higher among urban resident pregnant women compared to the rural residents. This is consonant with the studies conducted in sub-Saharan Africa,25 Tigray,14 Northwest Ethiopia,24 and Adama.9 The reasons might be urban residents were near mass media, and health facilities/health professionals to get information and awareness regarding malaria prevention methods using ITNs, and they are near the market to buy ITNs.9,11,13,20,26,27
The utilization of ITNs was 1.8 times among government-employed pregnant women compared to their counterparts. Similarly, Yitayew et al, 201815 reported that government-employed pregnant women were more likely to utilize it. This might be because government-employed pregnant women have a good income to buy ITNs and access health facilities/health care providers to be informed about the advantage of ITNs utilization.
Similarly, the odds of ITNs utilization was two times higher among pregnant women with monthly income >1050 Ethiopian total birr compared to their counterparts. This is supported by the findings of the studies conducted from sub-Saharan Africa25 and North western Ethiopia28 where pregnant women with income ≥151 dollar were more likely to utilize ITNs. This might be due to pregnant women with high income being able to access health services and having the ability to buy ITNs.29 To increase its accessibility all volunteers, and governments give priority to ITNs distribution for the endemic area, pregnancy, and family with low income.30
A woman with third-trimester pregnancy was 2.19 times more likely to utilize ITNs compared to women with first-trimester pregnancy. Pregnant women with advanced stages of pregnancy are more likely to attend ANC and aware of malaria prevention methods from health providers.31,32
The odds of ITNs utilization was 4.89 times higher among pregnant women who attended ANC than their counterparts. Likewise Obol et al, 201331 pointed out that women who have ANC were more likely to utilize ITNs. Evidence suggested that providers’ counseling during ANC is very crucial to boost ITNs utilization.8,33
Strengths and Limitations
This study was supplemented with observation to assess ITNs utilization and associated factors among pregnant women who are at high risk for malaria. Nevertheless, this study only focuses on pregnant women without considering ITNs utilization at the household level. The other limitation is that the cross-sectional study design cannot establish a temporal relationship between the outcome and response variables.
Conclusion
The majority of the pregnant women in this study had not utilized ITNs. Only four out of ten (39.9%) pregnant women had utilized ITNs which is lower than the target set by the Ministry of Health by the year 2007 ITNs coverage among vulnerable people. Being urban residency, employed, high income, third-trimester pregnancy, and attending ANC were factors significantly associated with ITNs utilization. The government and health sectors should encourage pregnant women to engage themselves in ANC follow-up to have awareness on ITNs to increase its utilization.
Data Sharing Statement
The datasets used for analysis are available from the corresponding author on reasonable request.
Acknowledgment
We would like to thank our data collectors for their invaluable effort without them this study would not have come to be completed. Also, our deep gratitude go to our study subjects who were volunteered and took their time to give us all the relevant information for the study.
Author Contributions
The authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or Publication of this article.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. World Health Organization. World malaria report; 2015. Avaliable from: https://www.googleadservices.com/pagead/aclk?sa=L&ai=DChcSEwjq3ca0jan1AhWHtO0KHSUYAOYYABAAGgJkZwæ2&ohost=www.google.com&cid=CAASEuRofwtXTanMxZn8IwI3_qN1TQ&sig=AOD64_0jy35fGBidoAGEpf39f7PRJLPJ1Q&q&adurl&ved=2ahUKEwjKjr-0jan1AhU1Q0EAHRIoAL8Q0Qx6BAgEEAE.
2. World Health Organization. World malaria report; 2015. Avaliable from: https://reliefweb.int/report/world/world-malaria-report-2015#:~:text=Globally%2C%20about%203.2%20billion%20people,%25)%20and%20deaths%20(78%25).
3. Yartey J. Malaria in pregnancy: access to effective interventions in Africa. Int J Gynecol Obstet. 2006;94(3):364–373. doi:10.1016/j.ijgo.2006.04.026
4. Lufele E, Umbers A, Ordi J, et al. Risk factors and pregnancy outcomes associated with placental malaria in a prospective cohort of Papua New Guinean women. Malar J. 2017;16(1):1–10. doi:10.1186/s12936-017-2077-4
5. Millar K. The need for malaria integration in maternal and newborn health; 2014. Avaliable from: https://www.mhtf.org/2014/07/11/the-need-for-malaria-integration-in-maternal-and-newborn-health/.
6. World Health Organization. WHO policy brief for the implementation of intermittent preventive treatment of malaria in pregnancy using sulfadoxine-pyrimethamine (IPTp-SP); 2013. Avaliable from: https://www.who.int/malaria/publications/atoz/iptp-sp-updated-policy-brief-24jan2014.pdf?ua=1.
7. Araya GD, Reda HL, Tesema AG. Utilization of long lasting insecticidal nets among household in malarious areas of Raya Alamata District, Tigray, Ethiopia. Sci J Public Health. 2015;3(2):216–221. doi:10.11648/j.sjph.20150302.19
8. Elmosaad YM, Elhadi M, Khan A, Malik EM, Mahmud I. Communication for behavioural impact in enhancing utilization of insecticide-treated bed nets among mothers of under-five children in rural North Sudan: an experimental study. Malar J. 2016;15(1):1–11. doi:10.1186/s12936-016-1551-8
9. Felema B. Assessment of Insecticide Treated Nets (Itns) Utilization Among Children Under Five Years of Age and Pregnant Women of Adama Woreda, Oromia Regional State. Ethiopia: Addis Ababa University; 2007.
10. Fuge TG, Ayanto SY, Gurmamo FL. Assessment of knowledge, attitude and practice about malaria and ITNs utilization among pregnant women in Shashogo District, Southern Ethiopia. Malar J. 2015;14(1):1–9. doi:10.1186/s12936-015-0755-7
11. Legesse Y, Tegegn A, Belachew T, Tushune K. Ownership and use of treated bed nets in urban communities of Assosa Zone. Western Ethiopia. Ethiop J Health Sci. 2008;18(1):1–10.
12. Tadele G, Samuel A, Adeba E. Replacement of long lasting insecticide treated nets in malarious kebeles of Gida Ayana district, East Wollega zone, Ethiopia. Sci Technol Arts Res J. 2014;3(2):162–166. doi:10.4314/star.v3i2.21
13. Tariku MK, Dagnew Z, Misikir SW, Belete AH Utilization of long-lasting insecticide treated net and associated factors among pregnant women in Malarious Kebeles in Awabel District, North-West Ethiopia, 2017. 2020.
14. Angesom T, Gebreyesus H, Gebremariam B. Long-lasting insecticidal net utilization and associated factors among pregnant women in Asgede Tsimbla District, Northern Ethiopia, 2017. Environ Health Insights. 2020;14:1178630220919393. doi:10.1177/1178630220919393
15. Nesga D, Abate D, Birhanu G, Addissie A. Assessment of malaria vector control measures (ITNs & IRS) utilization and factors affecting it in Adama District, East Shoa Zone, Oromia Region Ethiopia, 2018. J Fam Med Health Care. 2020;6(2):46–51. doi:10.11648/j.jfmhc.20200602.13
16. Shonga AA, Boltena MT, Boltana TF. Insecticide-treated bed nets utilization among pregnant mothers and associated factors in Damot Pulasa District, Southern Ethiopia. J Health Med Nurs. 2018;46:224–230.
17. CSA. Statistical report of the population and housing census of West Wollega, Ethiopia; 2007. Avaliable from: https://wwwrevolvy.com/page/WestWelegaZone.
18. Belay M, Deressa W. Use of insecticide treated nets by pregnant women and associated factors in a pre‐dominantly rural population in northern Ethiopia. Trop Med Int Health. 2008;13(10):1303–1313. doi:10.1111/j.1365-3156.2008.02159.x
19. Singh M, Brown G, Rogerson SJ. Ownership and use of insecticide-treated nets during pregnancy in sub-Saharan Africa: a review. Malar J. 2013;12(1):1–10. doi:10.1186/1475-2875-12-268
20. Yeshaneh A, Adane D. Insecticide Treated Net (ITN) utilization and associated factors among pregnant women’s in Halaba Kulito Town, South Ethiopia, 2016: cross-Sectional Study. Methods. 2005;4.
21. Yassin I, Rosnah S, Osman M. Factors influencing the usage of insecticide treated mosquito nets among pregnant women. Int J Health Res. 2010;3(3):139–144.
22. Njoroge F, Kimani V, Ongore D, Akwale W. Use of insecticide treated bed nets among pregnant women in Kilifi District, Kenya. East Afr Med J. 2009;86(7). doi:10.4314/EAMJ.V86I7.54145
23. Watiro AH, Awoke W. Insecticide-treated net ownership and utilization and factors that influence their use in Itang, Gambella region, Ethiopia: cross-sectional study. Risk Manag Healthc Policy. 2016;9:101. doi:10.2147/RMHP.S104311
24. Yirsaw AN, Gebremariam RB, Getnet WA, Mihret MS. Insecticide-treated net utilization and associated factors among pregnant women and under-five children in East Belessa District, Northwest Ethiopia: using the Health Belief model. Malar J. 2021;20(1):1–12. doi:10.1186/s12936-021-03666-6
25. Ameyaw EK. Individual, community and societal correlates of insecticide treated net use among pregnant women in sub-Saharan Africa: a multi-level analysis. BMC Public Health. 2021;21(1):1–13. doi:10.1186/s12889-021-11635-6
26. Ankomah A, Adebayo S, Arogundade E, et al. The effect of mass media campaign on the use of insecticide-treated bed nets among pregnant women in Nigeria. Malar Res Treat. 2014;2014:1–7. doi:10.1155/2014/694863
27. Nwachukwu CA, Anorue LI. Exposure to mass media malaria messages and use of insecticide-treated nets and artemisinin combination therapy among Southeast Nigeria residents. Afr Pop Stud. 2019;33(1). doi:10.11564/33-1-1351
28. Yitayew AE, Enyew HD, Goshu YA. Utilization and associated factors of insecticide treated bed net among pregnant women attending antenatal clinic of Addis Zemen hospital, North-western Ethiopia: an institutional based study. Malar Res Treat. 2018;2018:1–9. doi:10.1155/2018/3647184
29. Tapera O. Determinants of long-lasting insecticidal net ownership and utilization in malaria transmission regions: evidence from Zimbabwe Demographic and Health Surveys. Malar J. 2019;18(1):1–7. doi:10.1186/s12936-019-2912-x
30. USAID. Increasing equity of Insecticide-Treated Net Ownership in Sub-Saharan Africa from 2003 to 2014; 2015. Avaliable from: https://dhsprogram.com/pubs/pdf/AS52/AS52.pdf.
31. Obol J, Ononge S, Orach C. Utilisation of insecticide treated nets among pregnant women in Gulu: a post conflict district in northern Uganda. Afr Health Sci. 2013;13(4):962–969. doi:10.4314/ahs.v13i4.15
32. CDC. Intermittent Preventive Treatment of Malaria for Pregnant Women (IPTp); 2018. Avaliable from: https://www.cdc.gov/malaria/malaria_worldwide/reduction/iptp.html.
33. Ezire O, Adebayo SB, Idogho O, Bamgboye EA, Nwokolo E. Determinants of use of insecticide-treated nets among pregnant women in Nigeria. Int J Womens Health. 2015;7:655. doi:10.2147/IJWH.S77807
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.