Back to Journals » International Journal of Nanomedicine » Volume 18
Innovative Therapeutic Approaches Based on Nanotechnology for the Treatment and Management of Tuberculosis
Authors Kia P ![]() , Ruman U
, Ruman U ![]() , Pratiwi AR, Hussein MZ
, Pratiwi AR, Hussein MZ ![]()
Received 24 June 2022
Accepted for publication 6 February 2023
Published 8 March 2023 Volume 2023:18 Pages 1159—1191
DOI https://doi.org/10.2147/IJN.S364634
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Lijie Grace Zhang
Pooneh Kia,1 Umme Ruman,2 Ariyati Retno Pratiwi,3 Mohd Zobir Hussein2
1Institute of Bioscience, Universiti Putra Malaysia, Serdang, Selangor, Malaysia; 2Nanomaterials Synthesis and Characterization Laboratory (NSCL), Institute of Nanoscience and Nanotechnology (ION2), Universiti Putra Malaysia, UPM Serdang, Selangor, Malaysia; 3Department of Oral Biology, Faculty of Dentistry, Universitas Brawijaya, Malang, Indonesia
Correspondence: Mohd Zobir Hussein, Email [email protected]
Abstract: Tuberculosis (TB), derived from bacterium named Mycobacterium tuberculosis, has become one of the worst infectious and contagious illnesses in the world after HIV/AIDS. Long-term therapy, a high pill burden, lack of compliance, and strict management regimens are disadvantages which resulted in the extensively drug-resistant (XDR) along with multidrug-resistant (MDR) in the treatment of TB. One of the main thrust areas for the current scenario is the development of innovative intervention tools for early diagnosis and therapeutics towards Mycobacterium tuberculosis (MTB). This review discusses various nanotherapeutic agents that have been developed for MTB diagnostics, anti-TB drugs and vaccine. Undoubtedly, the concept of employing nanoparticles (NPs) has strong potential in this therapy and offers impressive outcomes to conquer the disease. Nanocarriers with different types were designed for drug delivery applications via various administration methods. Controlling and maintaining the drug release might be an example of the benefits of utilizing a drug-loaded NP in TB therapy over conventional drug therapy. Furthermore, the drug-encapsulated NP is able to lessen dosage regimen and can resolve the problems of insufficient compliance. Over the past decade, NPs were developed in both diagnostic and therapeutic methods, while on the other hand, the therapeutic system has increased. These “theranostic” NPs were designed for nuclear imaging, optical imaging, ultrasound, imaging with magnetic resonance and the computed tomography, which includes both single-photon computed tomography and positron emission tomography. More specifically, the current manuscript focuses on the status of therapeutic and diagnostic approaches in the treatment of TB.
Keywords: tuberculosis, nanomedicine, theranostic, diagnostic, therapeutic
Introduction
Tuberculosis (TB) is possibly a contagious fatal illness that has a destructive effect on the human lungs. Mycobacterium tuberculosis, the TB-causing bacteria, can be spread through airborne droplets from one person to another by sneezes or coughs. In 1882, Robert Koch was awarded the Nobel Prize for this significant discovery. Mycobacterium tuberculosis (MTB) known as an intracellular pathogen and an acid-fast bacillus that has evolved a variety of survival mechanisms to resist of being destroyed by macrophages.1 MTB is one of the most effective pathogens, able to living for decades in the host without creating any signs or symptoms of TB.2 According to the latest evaluation, MTB has infected around 25% of the world’s population. The World Health Organization (WHO) estimated the TB global outbreak peaked between 2003 and 2019, and to be declining slowly and that 1.6 million people being killed of tuberculosis in 2019,3,4 whilst TB was labelled a worldwide health emergency by the World Health Organization in 1993. M. leprae, M. avium and M. kansasii are among species of the pathogenic Mycobacterium. M. kansasii and M. avium do not result in tuberculosis or leprosy but do cause pulmonary infection and are hence known as non-TB mycobacterium.
TB can persist as a latent or active infection, whilst the former is symptomless and does not cause for disease transmission and the latter one is severe and contagious. Some studies have shown that persons with latent tuberculosis have a 10% probability of developing active tuberculosis if they have a weak immune system. Hence, it is also necessary for diagnosing latent tuberculosis and preventing it from becoming active.5 Primarily Mycobacterium mostly affects the respiratory system; however, it has the ability to attack any part of the body, such as bones, bloodstream (miliary tuberculosis), lymphatic system, kidney, joints, genitourinary system and central nervous system (meningitis).6 Success or failure rate in the treatment of TB depends on various factors such as (a) smoking, (b) malnutrition, (c) patient adherence to treatment, (d) insufficient monitoring by clinical staff, and (e) and coexisting diseases like HIV.
The main issue with the current TB chemotherapy is the longer period for the medication to be administered orally or given intravenously, the systemic blood circulation distributes it throughout the body, and most of the molecules fail to reach to the target destinations; therefore most of it remains in the body, creating toxicities and destructive impacts. Drugs have low plasma life with a high clearance rate, which can limit their efficacy.7 To overcome the problems of the anti-tuberculosis medications and reestablish a better efficacy of TB therapy, a new generation of TB treatments must be developed, especially to overcome the tuberculosis clinical management.8
Some major challenges to the current TB therapies include (a) extended treatment duration and (b) continual and common varied drug doses, which often leads to patients’ poor or noncompliance with existing therapy. The patient’s poor complying is the predominant related cause in the re-emergence of the illness, as well as the multidrug resistance (MDR) TB and further serious condition known as extensively drug-resistant (XDR) TB.9 Furthermore, MDR-TB and XDR-TB are on the rise in emergent nations, placing medical researchers to the challenge as well as becoming a serious threat globally.
AIDS, which provides a favorable ground for MTB development in an immunocompromised host, is another key factor in the rising prevalence of tuberculosis.10 Spreading strains of MDR and XDR, as well as a lack of effective treatment strategies, emphasize the need for novel and efficacious anti-TB drugs to conquer issues of shorter treatment durations, drug resistance, and greater compliance.11 Nanotechnology-based treatment, or nanomedicine, has been studied in recent decades as a means of substituting the conventional practice of delivery of antibiotics or other pharmaceuticals using drug-encapsulated nanoparticles (NPs). Drug delivery via nanomedicine technology provides the advantages of a controlled-, slow-, and sustained-release from biodegradable nanoparticles.12 Nanoparticles with sizes defined as nanometers (<100 nm) are commonly employed as nanocarriers in drug delivery techniques. Drugs can be embedded onto the nanoparticles or loaded in a matrix of the nanocarriers for therapeutic reasons.12 Nanocarriers can be any biocompatible and biodegradable nanomaterials like polymers, which can be either solid, lipids, natural, or synthetic, etc.13 They penetrate cells more efficiently and successfully than the larger-sized molecules, making them a potential route for the target delivery system. The nanocarriers are engineered to allow for persistent, controlled- and slow-release of drugs from the matrix. In addition, nanomedicine has advantages over conventional tuberculosis therapy approaches owing to the targeted treatment of anti-tubercular drug-loaded nanocarriers, particularly into the lungs, where primary TB is grown. This innovation could well circumvent anti-TB drug metabolism by escaping the first-pass metabolism system, with fast permeation and therapeutic results owing to the alveolar large surface area, avoid non-targeted distribution by using theranostic and diagnostic capabilities, reducing cytotoxic activity (liver and renal toxicity), and promoting patients’ compliance towards the therapy.14 Despite the high deposition efficiency and consistency of drug delivery to targeted tissues, this delivery system may penetrate straight into the deep tissues of the lungs and alveolar macrophages and provide its therapeutic impact.15 Despite the targeted delivery, controlled and site-specific aerosolized target delivery in nanomedicine, which exhibits greater absorption into the alveoli as well as better macrophage uptake, the absence of medication persistence inside the lung’s alveoli inhibits clinical translation of this therapeutic alternative. As a result, delivery of intracellular nanomedicine that particularly targets medication release or distribution in infected cells can conquer all the therapeutic hurdles linked to conventional TB therapy.
Nanomedicine has received a lot of attention in the past few years as a viable replacement for conventional therapeutic applications for tuberculosis treatment due to its greater efficacy, the capability to deliver multiple therapeutic payloads at the same time, improve selectivity, the strategies to endure multiple drug resistance and thus increased drug strength. Nanomedicine eliminates side effects and toxicity of the drugs by delivering the medication to the target tissue in a particular way that avoids off-target release, whereas its nano-sized diameters increase the permeability and solubility of the drug loaded in the nanocarrier. Furthermore, this enhances the stability of drug by isolating it from other external factors, and it enhances the drug residence by preventing the drug from passing away, which results in greater therapeutic effects.16
This review will discuss different types of Mycobacterium tuberculosis infections, conventional diagnostics and treatments. In addition, research, development and innovation using nanotechnology approaches for the treatment of TB will also be discussed.
Genus of Mycobacterium
The famous scientist Robert Koch, a Nobel Laureate in Medicine in 1905 discovered and in 1882 isolated this microbe. Discovery and diagnosis of the cause factor of (MTB), on March 24, 1882, paved the way both for a preventive plan based on laboratory germ attenuation and an effective searching for something like a pharmaceutical therapy.17 Mycobacterium is the main genus in the Mycobacteriaceae family and belongs to the Actinomycetales order, which now contains about 100 identified genus or proposed species, as well as variety of saprophytic microorganisms and pathogenic of the warm-blooded animals. The presence of mycolic acids and acid-fastness are defining features of this genus. Mycobacteria are aerobic, slow-growing, rod-shaped, slender and free-living in soil and water and non-spore-forming microorganisms. The generation time of these bacteria is about 20 h, but identification and isolation may take up to 6 weeks. Moreover, they are acid-alcohol-fast microorganisms that resist decolorization when stained with strong mineral acids and acidified alcohol. This acid-fastness feature, caused by waxy cell walls, is critical for detecting mycobacteria.18 Since the rest of bacteria with Gram-positive features (such as Rhodococcus, Corynebacterium, or Nocardia) are frequently acid-fast; therefore, the staining process must be done carefully.
The MTB complex includes Mycobacterium tuberculosis, Mycobacterium bovis BCG, Mycobacterium pinnipedii, Mycobacterium africanum, Mycobacterium bovis, Mycobacterium caprae and Mycobacterium microti. These bacteria cause tuberculosis, which is defined by tubercles development as well as the caseous necrosis in tissues. The tubercle bacilli are derived from tuberculous individuals. M. tuberculosis is perpetuated by humans, while M. bovis is perpetuated by cattle, bison, and deer; and M. avium is perpetuated by chickens. M. tuberculosis, M. bovis, and M. avium can infect and transmit to wild mammals and birds, and these animals can be potential infection sources for the domestic animals.19
The MTB cell wall’s structural details and its interactions with anti-TB drugs are shown in Figure 1. Rifampin (RIF) and isoniazid (INH) are the two major anti-TB drugs with recognized mechanisms of resistance. Rifampin is used as the first-line drug in the treatment regimens. Rifampin functions by limiting synthesis of the RNA, commonly known as transcription, and eventually induce cell death. Since Rifampin resistance is usually coupled with Isoniazid resistance, resistance to this antibiotic is used to predict and estimate the multidrug-resistance TB.20
 |
Figure 1 Cell wall structure of MTB and its interaction with the anti-TB drugs. Notes: Adapted from Tuberculosis drugs and mechanisms of action. National Institute of Allergy and Infectious Diseases. https://www.niaid.nih.gov/diseases-conditions/tbdrugs. Accessed March 1, 2023.21 |
Mycobacteria are gram-positive bacteria that are immobile, slow-growing, and have a high genomic G+C content (61–71%). Mycobacteria is called acid-fast because of their staining properties under a microscope, that are mediated with mycolic acid inside the cell wall, and this is one of the reasons for mycobacteria’s hardiness.
There are three types of Mycobacteria complex,19 and this will be discussed below.
Nontuberculous Mycobacteria (NTM)
Biochemical differentiation of mycobacteria from the rest of similar genera was carried out by analysis of the mycolic acids or fatty acids. Mycobacteria have mycolic acid with chemo-type IV within their wall.22 Nelson staining is one of the most prevalent approaches and at the same time the easiest technique for the primary detection of mycobacteria. Runyon in the 1950s divided mycobacteria into four categories based on pigment production and growth rate. To some extent, the Runyon classification of nontuberculous mycobacteria is based on the rate of growth: photo-chromogen, non-chromogen, scoto-chromogen and fast-growing. Fast-growing mycobacteria formed in solid media grow in less than 7 days, while most non-tuberculosis (NTM) generations belong in this category. Other generations in the Runyon category were considered slow-growing kinds. It takes more than 7 days for these species to grow in solid media, and the bacilli of Mycobacterium tuberculosis complex and several non-tuberculosis species are classified in this group. It is reported that many slow-growing species were closely associated with disease in humans and animals. Unlike slow-growing species, most fast-growing species were less pathogenic to humans and were considered opportunistic pathogens.23
Mycobacterium tuberculosis
These nine species are the main group of the Mycobacterium which causes tuberculosis: Tuberculosis sensu stricto, M. africanum, M. canetti, M. bovis, M. caprae, M. microti, M. pinnipedii, M. mungi and M. orygis. Slow-growing Mycobacterium tuberculosis should be incubated in culture media for almost 3 to 8 weeks. It takes about 10 to 20 days for the Bacillus colonies to appear in a small, dry, scaly solid medium. Mycobacteria generation time is 14 to 15 hours and in some sources up to 18 hours. Owing to the existence of wax and fat in the bacterial wall, the transfer of nutrients into the cell is slow; therefore, the growth of this bacterium is slow.24
Mycobacterium leprae
Mycobacterium leprae is the pathogen that causes leprosy, an infectious disease which affects skin and nerves. Despite effective therapies in previous decades, the spread of the disease continues unabated, and the transmission channels are still unknown. Despite the widespread opinion which incurable M. leprae-infected individuals are the primary transmission source, little evidence suggests that environmental sources might serve as a reservoir. It was also looked at if M. leprae DNA may be found in soil in leprosy-endemic areas or places with potential animal reservoirs like armadillos and red squirrels.25
Pathogenesis of Tuberculosis
Tuberculosis is disseminated by MTB complex-containing droplet nuclei in the air and is 1–5 μm in diameter. Once people cough, sneeze, talk or sing while suffering from pulmonary or laryngeal TB, these droplet nuclei develop. Aerosol therapies, bronchoscopy aerosolization and lesions or tissue manipulation and sputum induction, or secretion processing in the hospital or laboratory might all result in them.26 Droplet nuclei contain two to three MTB organisms and are so tiny that they may be kept airborne for a long time by air currents found in any indoor area.27 They are tiny enough to go into the lungs’ alveoli, where the germs replicate.28 Although TB patients create bigger particles holding more bacilli, these particles are not recognized to be efficient transmitters for contagious infection since they are unable to remain in airborne and cannot penetrate the alveoli if inhaled. Organisms deposited on healthy mucosa or skin do not affect tissue. Once particles of a larger size are inhaled, these collide with the airway or upper respiratory tract wall, are caught in the mucous blanket and transported into the oropharynx, where they are digested or expectorated.29 The chance of MTB transmission is determined by the four parameters listed below.
- The quantity of organisms released into the air.
- Organism concentration in the air, which is defined by the space’s volume and ventilation.
- Time the exposed person is exposed to contaminated air.
- Immunological condition of the person who was exposed.
The droplet nucleus is transferred via the bronchial tubes and implanted in a bronchiole or respiratory alveolus immediately after inhalation. There is no question that an inhaled tubercle bacillus causes an infection in the lungs; nevertheless, the virulence of the bacterium as well as the ability of the microbicides alveolar macrophage that ingests it plays a significant role. The bacillus has a chance to multiply inside the alveolar macrophage if it survives the initial barrier. The tubercle bacillus replicates gradually in the macrophage, dividing every 25 to 32 hours. There are no known endotoxins or exotoxins in Mycobacterium TB; hence, there is no immediate host response to infection. The microorganisms develop for 2 to 12 weeks till they exceed a population of 103 to 104, that triggers a cellular immune response,30 It can be recognized by a TB skin test response.31 Before developing the cellular immunity, tubercle bacilli transmit from the lymphatics to the hilar lymph nodes and subsequently via the circulation to more distant regions.
Many tissues and organs are resistant to the bacilli’s subsequent multiplication. Mycobacteria are frequently found in the bone marrow, liver, and spleen, however uncontrolled growth of the bacteria in these places seems to be an exception. Sediment of organisms inside the upper lungs, brain, bones, and kidneys could find a suitable environment to grow, and numerous bacterial divisions may arise before particular cellular immunity develops and limits duplication. In individuals with flawless cell-mediated immunity, accumulations of activated T-cells and macrophages from granulomas restrict the multiplication and spread of the organism. Antibodies towards M. tuberculosis are shaped; however, they do not appear protective.32 The organisms are often concentrated in the centre of the granuloma, which commonly turns necrotic.33 Duplication of M. tuberculosis is stopped in most people with normal immune systems as soon as cell-mediated immunity forms, however, if a few numbers of live bacilli remain in the granuloma. Although a main complex could often be seen on a chest radiograph, the majority of pulmonary TB infections are clinically and radiographically undetectable.34 The most frequent sign that an infection with M. tuberculosis has occurred is indeed a positive tuberculin skin test result.
People who have latent TB infection but not the active ones, are not contagious, making it impossible to spread the organism. According to the studies, approximately 10% of those with TB infections who do not receive preventative treatment can spread active tuberculosis and the risk of infection is still significantly high during 2 years of infection, this is the time that half of cases will occur.35 Additionally, diseases like silicosis, diabetes mellitus, and illnesses related to immunosuppression, such HIV infection, along with corticosteroids and other immunosuppressive drugs, are likely to reduce the host’s capabilities to respond to the organism. In these conditions, the risk for developing and spreading TB is risen, particularly during the first 2 years of life.36 Figure 2 indicates the stages of bacteria that enter the lung tissue, which are generally digested by alveolar macrophages; however, several bacteria grow inside macrophages and once the macrophages die, they are eventually released. Living macrophages (carrying M. tuberculosis) can transfer the bacteria into tissues and organs via the lymphatic system or even the blood, resulting in extra pulmonary TB. Extra pulmonary TB infects the lymph nodes, meninges, kidneys, spine, and bones about 15–20%. Extra-pulmonary TB has an atypical clinical appearance, which is frequently stimulated by inflammation or neoplasia.37
 |
Figure 2 Pathogenesis of tuberculosis. |
Types of TB Infections
Tuberculosis infections and tuberculosis illness are two different things. Whenever a person is exposed to someone who has tuberculosis and breathes in the TB germs, this person is recognized as having TB infection. The majority of people with strong immune systems are able to stop the infection at that time and avoid developing TB. Some people with tuberculosis infection (positive TB skin test but normal chest X-ray) are not ill and is not infectious to others.
Medication therapy Tuberculosis can effectively destroy bacteria and stop future TB infections. Nevertheless, if a person with tuberculosis does not take preventative medication, the bacteria can develop and cause active tuberculosis. A persistent cough that lasts 2 or more weeks, pain in the chest, fatigue, and lack of appetite are all symptoms of tuberculosis.38 When a person has active TB disease, the individual may be contagious and cause infection in other people, specifically those with whom they spent the most contact. Anyone with active tuberculosis will need to take various TB drugs for several months to recover and not infect others. Although, after a few weeks of medication, they may no longer be contagious and will be allowed to return to work and normal activities while finishing their TB treatment. People can have active tuberculosis in any organ of the body, but this is only infectious to others when it is in the lungs or larynx.39
Table 1 shows some of the most common signs of active tuberculosis in the lungs: cough with sputum and blood at times, chest pains, weakness, weight loss, fever and night sweats.40 Latent TB occurs when a person is infected with tuberculosis but does not develop an overt disease. They have no symptoms, and their chest X-ray may even be clear. A reaction to a tuberculin skin test (TST) or an interferon-gamma release assay (IGRA) may be the only symptom of this interaction. Yet, there is a continuing possibility that the latent TB infection could escalate to the active TB. Other diseases, such as HIV, or medications that weaken the immune system, enhance the risk of infection as well. Furthermore, miliary tuberculosis is a rare type of active tuberculosis that arises when TB bacteria enter the bloodstream. In this condition, the bacteria rapidly spread throughout the body in tiny nodules and affect numerous organs at the same time. This kind of tuberculosis can be rapidly fatal.41
 |
Table 1 Symptoms Difference Between Latent and Active TB |
Classification of Mycobacterium
While TB affects the respiratory system, it may also infect other cells and tissues, for instance the spine, brain, and kidney. TB can be fatal if adequate medical treatment is not taken. The medical community classifies TB into two categories, pulmonary and extrapulmonary, which result in 11 different forms of tuberculosis (Table 2). Four of these are caused by pulmonary TB, whereas the remaining seven are caused by extrapulmonary tuberculosis. Extrapulmonary TB is the most common in those with a weakened immune system.
 |
Table 2 Classification of TB and Their Main Symptoms |
The Factor That Influences TB
There are two stages in the possibility of developing active TB after exposure to tuberculosis bacilli, and each stage is impacted by both internal and external risk factors. Furthermore, exogenous factors including bacillary concentration in sputum and contact with an active TB case play an essential role in speeding the development from exposure to infection. The progression of infection to active TB illness is also influenced by endogenous factors. Comorbidities like diabetes, indoor air pollution, alcohol, immunosuppressive medication use, and cigarette smoke, illicit drug use, in addition to well-established risk factors (such as HIV, malnutrition, and young age) have a massive effect on both populations and individuals.61 Socioeconomic status and behavioral aspects have also been shown to enhance infection susceptibility. Certain groups, including health care professionals and indigenous peoples, are also at a greater risk of catching TB. Figure 3 highlights the major risk variables that affect an individual’s risk of getting TB infection. It illustrates the primary features that influence an individual’s risk of contracting infection and disease.62
 |
Figure 3 TB infection risk factors. |
Tuberculosis Current Situation and Challenges
Tuberculosis (TB) is among the most deadly and oldest infectious diseases that harmed human skeletons for thousands of years.63 Until 1882, the major cause of TB was unclear. Dr Robert Koch reported the discovery of bacillus Mycobacterium tuberculosis as the major cause of the disease, during the second final decade of the nineteenth century. Every year since then, the 24th of March has been observed as “World Tuberculosis Day”.64 TB is a contagious illness that spreads readily from person to person. The main cause of tuberculosis is coughing, which occurs when a person afflicted with tuberculosis, expel the bacteria into the air. Data from the National vital registration systems indicate that in the late eighteenth century, tuberculosis was known as the leading cause of mortality in various European countries, North America, and other parts of the world. However, throughout the twentieth century, with rapid improvements in nutrition, income, and housing, the rate of TB cases began to decline, and the majority of TB casualties also started to drop, albeit slowly (1–2% each year).65 Since the early 1940s, the number of tuberculosis cases has been declining at a pace of 10% each year. Similarly, the rate of TB mortality has been dropping. One of the primary reasons for the decrease in the cash rate and the fatality rate was the innovation, progress, and administration of effective drug treatments. In several countries, tuberculosis is known as a disease of the past, owing to the low disease prevalence. These countries have less than one mortality per 100,000 people and fewer than 10 fatalities per year. Even though the prevalence of tuberculosis is declining, in some parts of the globe, tuberculosis remains a persistent and never-ending public health problem. With prompt diagnosis and appropriate medication therapy, tuberculosis (TB) can be cured.
In 1993, many international health agencies, including the World Health Organization (WHO) announced a worldwide health emergency. TB fatalities also increased in 2021, rising to 1.7 million from 1.6 million in 2020 (Including 187,000 people with HIV). TB is the second most common infectious cause of death, after COVID-19 (over HIV/AIDS), and the 13th largest cause of death overall. The COVID-19 pandemic had a negative impact on the fight against tuberculosis, undoing years of work in providing critical TB care and reducing disease burden. A (4.5%) rise in 2021 from 2020 is due to the wide range of misdiagnosed and untreated cases that contributed to the first spike in TB mortality in more than a decade.66,67 In addition, 450,000 instances of multidrug- or rifampicin-resistant (MDR/RR)-TB were recorded in 2021, representing a 3% rise in the incidence of drug-resistant tuberculosis from 2020. The excessive number of infections and death are related to a decline in crucial TB care since the pandemic starts in 2020.68
MDR-TB or multidrug-resistant tuberculosis is still a common health concern and a health security risk. The number of people with multidrug- or rifampicin-resistant tuberculosis (MDR/RR-TB) who were discovered and notified in 2019 was 206,030, which was an increase of 10% from 186,883 in 2018. Globally, from 2015 to 2019, the incidence of the TB disease fell by roughly 2% every year, the cumulative reduction was 9%. This was less than halfway to the End TB Strategy milestone of a 20% reduction between 2015 and 2020. TB diagnosis and treatment saved up approximately 60 million lives between 2000 and 2019. Ending the tuberculosis pandemic by 2030 is one of the United Nations Sustainable Development Goals’ health goals (SDGs).69–71
This disease is more frequent in males than in women, and in adults rather than in youngsters. According to some researchers, tuberculosis is one of the top 10 deadliest diseases on the planet. In terms of mortality, this disease ranks higher than HIV/AIDS. In 2014–2015, all UN and WHO members agreed to put an end to this pandemic disease. In May 2014, at the World Health Assembly, these states overwhelmingly approved and adopted the UN Sustainable Development Goals (SDGs) and WHO’s End Tuberculosis Strategy. The End TB Strategy’s and tuberculosis-related fatalities chief goal is to eradicate TB endemic by 2030–2035.72
The primary purpose for combining anti-tuberculosis drugs (ATDs) with diverse mechanisms of action is to prevent the growth of drug-resistant strains. However, inconsistencies in medication production, noncompliance with therapy, unsuitable regimens, and poor management all led to the formation of resistant strains. Multidrug-resistant (MDR) Mtb strains are those that are resistant to the essential antibiotics INH and RIF, whilst extensively drug-resistant (XDR) Mtb strains are those that are also resistant to a second-line injectable antibiotic (amikacin (AMK), capreomycin, or kanamycin) and fluoroquinolone (such levofloxacin or moxifloxacin (MXF)).73 Furthermore, multiple examples of strains resistant to all first- and second-line TB treatments have been documented in recent years. MDR-TB and XDR-TB treatments duration are almost between 18 and 20 months and need to be taken with second-line drugs, that costs more with higher toxicity effects than in compared to the first line. Injectable drugs additionally make it increasingly challenging to follow treatment plans. Furthermore, TB therapy in HIV patients is worsened by considerable drug–drug interactions between ATDs and antiretroviral treatments.74 The only three ATDs include pretomanid (2019), bedaquiline (BDQ, 2012) and delamanid (2014) authorized towards MDR-/XDR-TB treatment in the past four decades. Different therapies for MDR-/XDR-TB are being tested in clinical trials, such as the NiX-TB experiment. This 6-month all-oral regimen, which the Food and Drug Administration (FDA) lately authorised, combines linezolid, BDQ and pretomanid for the treatment of XDR-TB and other MDR-TB cases.66 It had a successful outcome; however, side effects were recorded. The majority of RR-/MDR-TB cases may be cured with completely oral regimens, according to the most recent WHO recommendations for the treatment of drug-resistant TB, with injectable drugs (particularly AMK) only being used in cases when other treatments are not possible. These reflect a significant requirement for shorter treatment times and more potent medicines with less toxicity side effects. To overcome the limits of existing TB treatment, nanotechnology provides various advantages.75–77
Current Conventional Methodology for the Diagnosis of Tuberculosis
To identify Mycobacteria, methods ranging from the most basic laboratory tests to the most complicated molecular and non-molecular approaches have been developed. Sputum smear and culture techniques are the most conventional techniques for identifying MTB. These methods are time-consuming, requiring experienced employees to conduct the test and requiring several days or weeks to obtain a result. Most conventional methods are so insensitive that they can only identify 50% of the active MTB. This was found that sensitivity is much lower in HIV co-infected patients or youngsters with a small active colony-forming unit. Diagnosing TB and its drug resistance in the early stages of the infection increases the chances of surviving, and by diagnosing contagious patients at an early stage, we can manage and treat them and try to decrease the number of fatalities.78 Table 3 provides a detailed overview of the many conventional methods utilized in tuberculosis diagnosis.
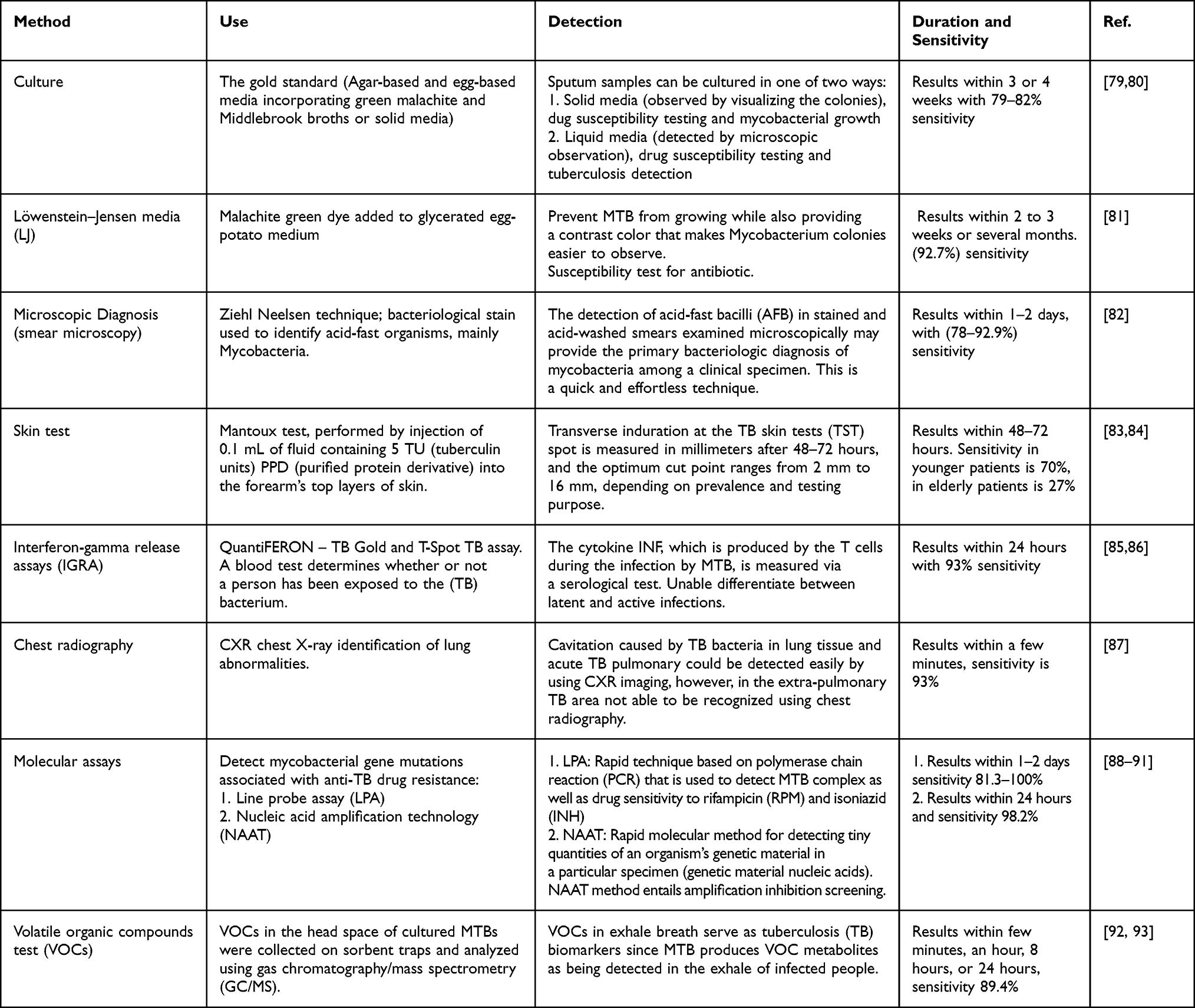 |
Table 3 Comprehensive Overview of the Various Conventional Technologies Used in Tuberculosis Diagnosis |
Current Tuberculosis Drugs
WHO, in 2021, updated the most recent guidance for treating patients with drug-susceptible TB. Based on this guidance, a 6-month treatment plan consisting of four first-line TB medicines, namely isoniazid, rifampicin, ethambutol, and pyrazinamide, is suggested. All four medications are used during the first 2 months of therapy, and two medications are utilized throughout the remaining 4 months of treatment until the treatment is finished. This is a strong recommendation based on data with intermediate certainty.94 This treatment regimen has been extensively accepted across the world, and about 85% who use this procedure will have a satisfactory treatment outcome. The present four-drug treatment program has been in effect over almost three decade and is based on foundational TB therapy research done in the 1980s according to the British Medical Research Council.
Research into shortening the duration of TB treatment has increased during the past several years. As a result, several trials and other research have been conducted to determine whether therapy may be reduced while remaining highly effective. While this research has mostly concentrated on drug-resistant TB (owing to the fact that the typical duration of treatment was 18–24 months until recent years). A recent trial evaluated the effectiveness and safety of two 4-month regimens for the TB drug-susceptible treatment. One of these regimens, which included a fluoroquinolone and a high dosage of rifapentine, passed the non-inferiority test. This trial represents the recommended body of evidence for the forthcoming Guideline Development Group to evaluate (GDG).70 Table 4 illustrates the first and second-line TB drugs’ discovery year, primary features, and most often reported adverse effects.95 Table 4 includes the first- and second-line drugs for TB treatment.
 |
Table 4 The First- and Second-Line Drugs for TB Treatment |
Anti-TB therapy is typically used for a period of 6 months. For the first 2 months, only four drugs, namely pyrazinamide, isoniazid, rifampin, and in some cases, ethambutol are used. The use of rifampin and isoniazid is continued for the next 4 months (Table 4). Sometimes, the six-month regimen is termed as “short-course” anti-TB therapy. These drugs are administered daily. Now the questions remain that why does it take so long to TB disease in patients while the cultures of M. tuberculosis may be destroyed in a matter of mere hours to days? The existing model shows that numerous populations of bacilli must be dealt with in infected individuals: those that are growing rapidly, those growing slowly, and those that sporadically replicate. The cells of these separate populations are killed in two phases. At the first bactericidal phase, rapid multipliers are cleared. During the second sterilizing phase, the remaining multiplying organisms are being killed slowly and sporadically. Streptomycin and isoniazid are two types of drugs that had bactericidal activity when tested in animals. These drugs reduce the infection burden by a magnitude of four to five orders. However, these drugs failed to kill the infections. Thus, despite the fact that these drugs killed the inflections, the multiplying populations of M. tuberculosis remain persistent. These slowly and sporadically multiplying populations of M. tuberculosis can only be cleared with antibiotics possessing “sterilizing” activity. Sometimes, these persisted cells become more phenotypically resistant to anti-TB therapy and therefore can take longer to be cleared. Rifampin is sterilizing antibiotic that can decrease the bacillary counts to zero during the second stage of treatment in human beings. With the use of pyrazinamide during the first 2 months of therapy, the length of therapy is reduced. However, it shows minimal bacterial activity when used alone. Ethambutol is an effective drug for drug-susceptible M. tuberculosis and is normally included in the regimen when it is suspected that a certain population has drug-resistant TB.96
Sometimes treatment of TB diseases takes 6 to 9 months by taking several drugs. Only 10 drugs have been recommended by the United States Food and Drug Administration (FDA). Pyrazinamide (PZA), ethambutol (EMB), rifampin (RIF), and isoniazid (INH) are the first line of the approved drugs. These drugs form the core of treatment regimens.97 TB bacteria that is resistant to at least one of the first-line anti-TB drug, is a kind of TB drug-resistant. TB bacteria that are resistant to more than one anti-TB drug are called multidrug-resistant TB (MDR-TB). This bacteria is at least resistant to both rifampin (RIF) and isoniazid (INH). While another uncommon kind of MDR-TB is resistant to rifampin and isoniazid, fluoroquinolone is also one of at least three injectable intravenous second-line drugs – capreomycin, kanamycin, or amikacin – and is called extensively drug-resistant TB (XDR-TB). The treatment and cure of drug-resistant TB are very complicated. In order to treat this drug-resistant TB, a comprehensive consultation with a TB specialist is required.98
Clinically Approved ATD’s for Therapy and Diagnostic
To treat MTB, first-line drugs INH, PYR, EMB, and RIF have been given orally in combination in recent years. Second-line drugs are also combined with the first-line drugs in this treatment.
A combination of second-line drugs is also used to treat MDR-TB. Some of the medications on this list are polypeptides – enviomycin, viomycin and capreomycin; aminoglycosides – kanamycin and amikacin; thioamides – ethionamide, cycloserine and prothionamide viomycin; fluoroquinolones – moxifloxacin, levofloxacin and ciprofloxacin. Generally, first-line drugs are cheaper than second-line ones. Drugs that are now widely known as the third-line TB therapy are thioridazine, rifabutin, vitamin D, thioacetazone, macrolides, linezolid, arginine, and clarithromycin.99 Third-line drugs may not be as successful as first- and second-lines, though, as their effectiveness has not yet been shown and is still being researched.6
For the treatment of MDR, several medications have been proven in clinical research, while others still require further study. Bedaquiline, rifapentine, linezolid, and pretomanid are a few examples. A brand-new ATD called Bedaquiline (Phase 2 trial) has been approved for use in the management of drug-resistant TB. Due to its core heterocyclic quinolinic nucleus containing amine and alcohol side chains, bedaquiline (BDQ), a member of the diarylquinoline class of compounds, plays an important role in antituberculosis therapy. In addition to inhibiting synthesising mycobacterial ATP, it binds to and disrupts the interface of the a-c subunit, impairing the proton cycle and killing the Mycobacterium.100 A nitroimidazo-oxazine known as pretomanid has anti-replicating and anti-dormant mycobacterial activity by inhibiting the formation of mycolic acid and preventing the formation of cell walls. Furthermore, in anaerobic or hypoxic situation, pretomanid effects on non-replicating bacilli.101 Linezolid (LNZ), an oxazolidinone that has been modified and is currently in phase 2, prevents the production of proteins in mycobacteria. The creation of a 70S initiation complex is prevented by LNZ when it binds to the 50S ribosomal subunit’s 23S rRNA domain V.102 These medications’ efficacy is constrained by their fast release and shorter plasma half-life. Therefore, in order to increase the success rate of TB therapy, pharmacological treatments are required.102 Figure 4 includes the nanomedicines that are available on the global markets.
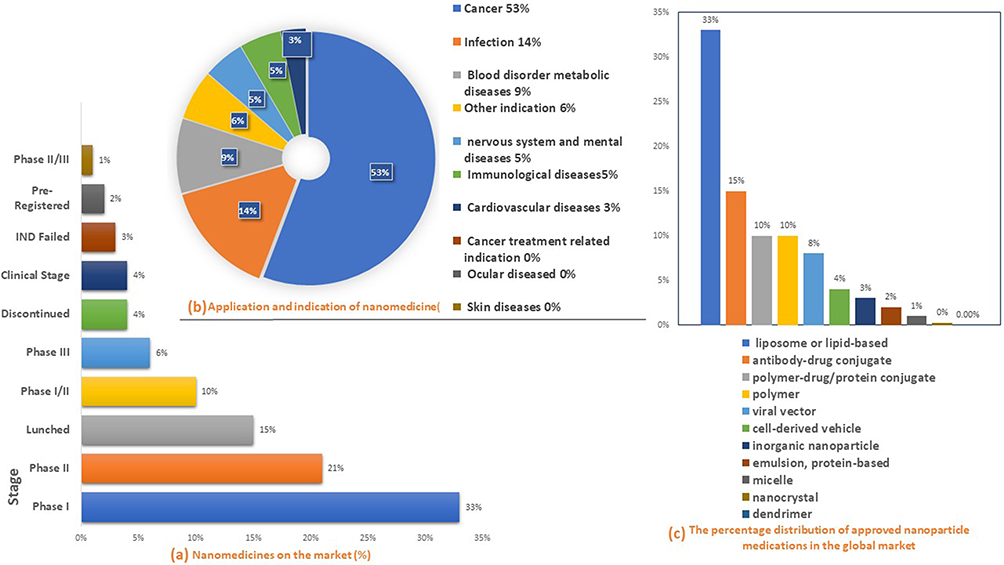 |
Figure 4 Authorized nanomedicines available on the global markets: (a) Current status of development, (b) indications, and (c) formulation. |
The Cortellis Drug Discovery Intelligence (CDDI) database was used to find nanomedicines that have been authorized for use on the market or in clinical studies. In June 2021 recent data was examined and evaluated, which indicated that there are now 563 nanomedicines in various phases of drug clinical trials and 100 nanomedicines on the market (663 totally). The majority of these are in clinical phases I and II in which (33%) for former and (21%) for later. They mostly target the treatment of cancer (53%) and infections (14%) respectively (Figure 4a). Recent advances in nanomedicine have enabled the treatment of more diseases affecting the nervous, immunological and metabolic systems, blood, brain, endocrine inflammatory, ophthalmic, cardiovascular and dermatitis problems among other diseases (Figure 4b). Additionally, they are used in the imaging diagnostics and vaccinations development. Liposomes, or lipid-based nanoparticles, account for the vast majority of nanomedicines on the market or in different phases of clinical development are (33%), next by antibody-drug conjugates (15%), polymer-drug/protein conjugates (10%), and polymers (10%). Viral vectors (8%), inorganic nanoparticles (3%), cell-derived vehicles (4%), emulsions, protein-based nanoparticles (3%), nanocrystals, micelles, and dendrimers are more forms of nanomedicines (Figure 4c).103,104
Current Tuberculosis Vaccine
The Bacillus Calmette–Guérin (BCG) vaccine was utilized to combat tuberculosis (TB) since 1921 and is regarded as the most extensively used vaccination in the world.105 However, it is recognized that the BCG protective effectiveness depends on the geographic region in which it is given.106
How BCG’S Response to Mycobacterium tuberculosis
BCG, a live-attenuated Mycobacterium-based immune complex vaccine, promotes immune activation and the local infection at the injection area, where existing dendritic cells (DCs), macrophages and monocytes react to the bacterium.107 BCG vaccine may survive inside dendritic cells for up to 2 weeks,108 producing the immune-polarizing cytokines, in the meantime causing the activation of costimulatory molecules, which are characterized by enhanced expression of the differentiation clusters including CD40, CD80, CD83, and CD86.109 BCG cell wall skeleton immunogenic parts, such as covalently linked mycolic acid, arabinogalactan, and peptidoglycan, are phagocytosed and destroyed by macrophages,107 which may also significantly stimulate an inflammatory response by activating several pattern recognition receptors (PRRs).110,111 While toll-like receptors constitute the first line of defense system against microbes (TLR) 2, signaling is activated by lipids and mycobacterial cell wall lipoglycans like lipomannan (LM). Other mycobacterial proteins, including as heat-shock proteins and glycoproteins, trigger by TLR4 signals.112,113 BCG CpG-DNA has been shown to induce TLR9 intracellular in macrophages and DCs, leading to activation of the cell and the generation of interleukin-12 (IL-12), tumor necrosis factor α (TNF-α), and monocyte chemoattractant protein-1 (MCP-1), a key mediator of the T helper type 1 (Th1) immunological responses.114,115 Similarly, the complement receptors CR3 and CR4, as well as nucleotide-binding oligomerization domain (NOD)-like receptors or even C-type lectins, have all been demonstrated to react with the cell wall components of bacteria and have a crucial role in BCG recognition and internalization.116 Similarly, research on BCG-immunized adults has shown that monocyte progenitors are reprogrammed with stronger PRR expression and enhanced responsiveness to stimuli like TLR agonists. Antigen-presenting cells, including DCs, macrophages, and B lymphocytes white blood cells (B cells), deliver BCG-derived antigen peptides to primary T-cells and major histocompatibility complex (MHC) molecules in the surrounding secondary spleen or lymphoid tissue in order to initiate an adaptive immune response (Figure 5).117,118
 |
Figure 5 BCG vaccination induces an immune response, with MTB-specific effects. (A) BCG is absorbed by DCs or macrophages and could activate the anti-TB immune response when their cell walls perform as PRRs and are connected to a co-stimulatory receptor-ligand. (B) The formation of plasma cells, memory cells, and antigens with particular antibodies is triggered by B cell activation.Memory T and B cells remain in lymph nodes after activation. |
After the BCG vaccine is given intravenously, macrophages, monocytes and dendritic cells (DCs) detect the BCG and create a powerful immunological response. DCs or macrophages detect and internalize BCG. BCG’s cell wall and other components operate as PRRs, binding to various ligands, upregulating costimulatory molecules in activated cells, and activating the anti-TB innate immunity. When B-activated DC cells move to lymph nodes, they trigger Th1-type, CD4+ and CD8+ T cells that are specific for mycobacteria and then secrete large quantities of cytokines like IFN-gamma and granzyme. Memory cells, plasma cells, and antigen-specific antibodies are produced all at once by B cells that react to BCG antigens.118
Activated DCs at the BCG vaccination spot move towards the draining lymph nodes, where they release tumor necrosis factor-alpha (TNF-α), Interleukin 6(IL-6), and Interleukin 12 (IL-12), which trigger both of the CD4+ and CD8+ T-cells.119,120 Activated CD4+ and CD8+ T cells produced IFN-γ, which boosts macrophage antimycobacterial activity.121 This demonstrates how people with IFN--γ mutations are more susceptible to TB.122 Neutrophils and activated DCs both works together to boost antigen-specific T-cell responses. According to some researchers, 10 weeks after BCG vaccination, newborns’ peripheral blood may contain a substantial amount of BCG-specific CD4+ and CD8+ T cells. Furthermore, the serum contains higher concentrations of IFN-γ, granzyme, TNF-α, and IL-2.123,124 Figure 6 indicates the BCG vaccination results in the formation of trained immunity.
 |
Figure 6 BCG vaccination results in the formation of trained immunity. |
BCG vaccination causes monocytes/macrophages to develop trained immunity, resulting in greater epigenetic reprogramming and host defensive abilities. When monocytes are exposed to non-specific infections (respiratory syncytial virus or yellow fever virus), chromatin rearrangement causes them to become “trained”, increasing the efficiency of their innate immune response and triggering the release of proinflammatory cytokines like IL-6, IL-1, and TNF-alpha (Figure 6). However, further research is needed to determine if this “training process” will try and stop SARS or other respiratory syndrome-like coronaviruses.
Conventional TB Drug Therapy Disadvantages
Clinical management in TB therapy is presently seen as one of the most difficult challenges. Drugs are transported all over the body by systemic blood circulation after being taken orally or intravenously, and many molecules aggregate in other parts of the body rather than targeting the right site, triggering disadvantages including nephrotoxicity, hepatotoxicity, ocular toxicity, and ototoxicity. Most TB drugs are administered orally, which leads to pharmacokinetic issues like limited bioavailability and a low therapeutic index. Drug therapy in a conventional route necessitates a lengthy therapy regimen that includes frequent and continuous administration of multiple drugs, leading to lower patient adherence to existing treatments. This is a critical indicator sign of infection recurrence, as well as formation of multidrug-resistant MDR-TB and the more severe extensively drug-resistant XDR-TB.9
In undeveloped countries, the outbreak of MDR-TB is steadily growing. This is a source of a big problem and concern for the health care services.125 Although present anti-TB medications are successful, there seems to be a critical need to find effective and sustainable solutions with producing new short-term regimens that combine novel drugs to tackle the challenges of treatment length, drug resistance and adhere to the treatment.11 As a result, a method will be developed to overcome the therapeutic limitations associated with conventional treatment. Higher bioavailability, effective drug loading, longer retention time, and improved drug encapsulation capacity in body cells, and gradual and consistent drug release might lead to reduced frequency and multiple-drug dosage. Moreover, it was mentioned that when a drug is delivered to the targeted tissue, localised drug exposure is preferable over systemic exposure in order to reduce or indeed prevent systemic side effects. Hence, targeted drug therapies have gained a lot of attention as a way to reduce such systemic adverse effects.126
Advantages and Disadvantages of Nano Drug Delivery System
To overcome the challenges and the side effect of conventional treatment, researchers have brought new novel formulation of nanomedicine which can provide effective therapeutics index. Inhalable nanoparticles are biodegradable and biocompatible, which contain high drug loading capacity this made them to enhanced mucosal cell adhesion, and improved drug delivery to the respiratory system for the treatment of (TB).127 Although nanocarriers based drug delivery agents are achieved high drug loading, high stability, effective drug tolerability, reduce multidrug and extra drug resistance, controlled release, and site-specific delivery, the clinical phases are slow for the benefit of human. Physical and biological factors like pH, protein, phagocytic sequestration, enzyme, shear forces, renal clearance, and aggregation create hostile environments for nanocarriers. The nanocarrier-based medicines have marketed in the pharmaceutical industry at a slow phase.128
For TB drug delivery, the nanocarriers cannot often reach to the deep lung since majority of the drug doses are exhaled. The nanocarriers administer in different routes in TB treatment such oral, topical, intravenous, and pulmonary delivery. These routes have different various limitations, barriers of biological environment, interaction of biological components such as protein corona, loose of nanocarriers before reaching the disease sites, clearance by phagocyte system and so on. The nanocarriers with low water solubility, low bioavailability and low biodistribution exhibit biological and anatomical barriers in the respiratory tract as well as gastrointestinal tract and liver. Beside these barriers, the inhaled therapeutics agents in lung airways exhibit some obstacles in reaching the target TB cells. As a result, the deposition of nanocarriers’ physicochemical properties, particle size, size distribution, density, shape, and electrostatic charge play an important role to reach in deep lung deposition. The composition of the nanocarriers’ inhaled particles should be very small enough to reach the lung TB cells and avoid the deposition in the airways by sedimentation or loss by exhalation. The size and composition become challenging nowadays for the researchers to deliver nanocarriers. To overcome these limitations and achieve the highest efficiency, the nanocarrier characteristics could be tailor-made to target and function effectively for the desired delivery routes.129,130 Nanocarrier based delivery has shown potentially remarkable feature such as biodegradable particle, slow, sustained, controlled release. Although different animal models have been studied to develop the anti-TB therapy based on nanotechnology against M. tuberculosis , unfortunately the clinical management of tuberculosis remains a difficult task and many models do not stand up to the expectations of human TB treatment. Several studies have been conducted by researcher for nanocarrier-based TB therapy. Bhardwaj et al used spray-dried lipid–polymer hybrid nanoparticles for the delivery of isoniazid to TB cells. The formulation was found to be proven to have more uptake by TB cells.131 Recently, Ahmed et al has developed dendrimer-based nanocarrier system to load rifampicin and delivered to TB cells and has found that the drug carrier has high drug loading, negligible toxicity, and extended-release pattern for rifampicin. Although nanocarrier-based systems are more effective than conventional treatments, many studies need to be conducted due to the high necessity of TB effective treatment as well as reduction of the limitations of nanocarrier-based treatment.132
Barriers to Nanoparticle Drug Delivery to the Lung Anatomy
The airway defense system, tight epithelial cell layer, as well as the mucus hypersecretion are the key barriers to NP delivery for chronic lung diseases. However, this will vary depending upon the type of delivery system, respiratory system disease area and the development of the disease. Intranasal, inhaled, or intravenous delivery all were employed to treat pulmonary (TB), even though each brings its own set of challenges. The appropriate route will be determined by the kind of NP, the required bioavailability, as well as the airway target tissue. Targeted nanoparticles towards the lungs must contend with not just the particular structure of the lung but also intravascular, specialized pulmonary, and intracellular barriers.133 In terms of drug delivery, the respiratory tract in lung anatomy is divided into two sections: the top, which includes the nasal cavity, pharynx, whilst the bottom includes the larynx, trachea, bronchi, and alveolar. There are two principal bronchi in this trachea, which branch into the tinier bronchioles inside the lungs, creating air pathways toward the alveoli terminal. The tubes become smaller and split into even more tubes as they pass down from the trachea to the respiratory tract.
There were also reported to be 20 to 23 divisions, all of which led to the alveolus. Although each bronchus or bronchiole has a lower cross-sectional size, the total surface area is bigger due to the huge number of them. As a result, resistance in the terminal bronchioles was reduced. Because of the turbulence, the majority of the resistance is positioned three to four divisions from the trachea. Despite their small size, alveoli contain a significant overall surface area that allows for effective and sufficient gas exchange. Moreover, alveoli contain a single epithelial (400 nm) cell layer that separates the air from the capillaries.134 Rather than being a barrier, this wide surface area offers a great capacity for drug absorption, and thus escape the first-pass metabolism helps to make the pulmonary route desirable for theranostic NP drug delivery.135
Pulmonary Barriers
Many barriers related to pulmonary are formed in healthy lungs, and many more are formed in diseased lungs for exogenous nanoparticles, the airway’s mucociliary system is the primary defensive mechanism for removing dust and eliminating microorganisms. The first barrier goes to submucosal glands, and goblet cells create mucous that coats the whole respiratory system and increases the mucus thickness of the airways in disease from 2–30 to >260 m. Mucous is pushed forward as the periciliary liquid layer beneath helps the cilia’s consonant rhythmic beating repetitively into the proximal airways, where it is either ingested or expelled.
The second barrier is, pulmonary surfactants lower the surface tension and prevent collapse at the alveolar air-liquid interface; however, surfactant proteins SP-A and SP-D also play a significant role in pulmonary immune defense.134 Surfactant proteins SP-A and SP-D are key components in pulmonary immunology because by opsonizing and binding the invading microbes from the lung allowing them to be cleared by alveolar macrophages (AM).136 Alveolar macrophages are prominent in inhaled particles or fiber removal from the lung. AM size variations across species may alter the amount and size range of particles/fibers which can then be phagocytized and removed by AM.137 Because both SP-A and SP-D may attach to NPs and induce clearance from the lungs, this characteristic of these molecules offers the most serious challenge for NP administration. Both molecules were found to increase the AM uptake of NPs in recent research; however, the effect was maximum with SP-D for hydrophilic NPs and most pronounced with SP-A for hydrophobic NPs. However, despite the different NP surfaces, both different kinds of NPs interact with AM to a roughly equal extent in the existence of native surfactants in this research, implying that SP-A and SP-D activities with NPs need to be studied further to completely comprehend this complex of the lung clearance process.138
The third barrier is, respiratory illnesses including cystic fibrosis, COPD, and asthma alter lung bifurcation angles, causing turbulent flow and obstructing airways. This decreases particle deposition to around 2% in the most obstructed parts, which are in most need of treatment. Applying NPs to solve these issues will provide significant benefits when using the pulmonary route. Nanoparticles can easily enter the systemic circulation due to the great level of vascularization, the enormous surface area of the respiratory tract, as well as the super-thin barrier in between the pulmonary lumen and the capillaries.135
Intravascular Barriers
The high ionic strength of the blood may result in particle agglomeration and sequestration after intravenous injection of NPs loaded with drug given via systemic circulation.96 Extracellular proteins or opsonins as part of plasma proteins may also adsorb with NPs, causing phagocytic identification and removal of the NPs from the circulation shortly after delivery. Since NPs need to extravasate through the blood circulation and lymphatic vessels to reach target area, size restrictions imposed by various endothelium layers all across the body may have still another obstacle.139 These intravascular barriers can sometimes help with targeted delivery, and even in the situation of “leaky” tumor vasculature, which allows NPs to extravasate more easily in tumor tissues than in healthy parts. Due to inadequate lymphatic drainage and defective vasculature, NPs can easily accumulate in the tumor interstitium, causing increased penetration and persistence.140
Intracellular Barriers
To have a therapeutic effect, it is necessary that NPs can pass through cell membranes and penetrate the cytoplasm, nucleus as well as other organelles of the target cells after reaching the diseased tissue. As lipophilic cell membrane would be the first barrier that intracellularly targeted NPs encounter, larger charged molecules like DNA, drugs, and proteins cannot enter cells through the lipophilic cell membrane; however, endocytosis is expected.141 A useful technique for receptor-targeted NP absorption is clathrin-mediated endocytosis; however, NPs that enter the cell by this mechanism may get trapped by late endosomes, where they combine with lysosomes.142
The Application of Nanotechnology to Overcome Delivery Barriers in the Respiratory System
The design and fabrication of materials at the atomic and molecular nanoscales is known as nanotechnology. The term “nanomedicine” refers to the use of nanotechnology in medicine. Nanomedicine is capable to overcome several limitations in diagnosis, treatment, and bring a drastic change in healthcare, and human illness management. For the last many decades, a lot of efforts have been made to introduce nanotechnology-based platforms in order to enhance the treatment and diagnosis of different kinds of diseases including disease-related to lungs. However, there are certain barriers that limit the application of nanotechnology against acute and chronic respiratory diseases. Nanotechnology’s utilization in medical applications is quickly expanding, and it has tremendous potential in a wide range of applied scientific domains.143
To address the barriers posed by lung biology and anatomy, NPs with particular alteration in their shape, hydrodynamic dimension, and surface charge/hydrophobicity have been emerged. In order to evade the mucus barrier, the electrostatic, hydrophobic and steric characteristics of NPs should be adjusted. To improve NP’s stability, it is preferable to coat the NP’s surface by surfactants, proteins, lipids, dendrimers, polymers, copolymers, and inorganic molecules. Dextran or polyethylene glycol polymer coatings provide biocompatibility onto NPs and provide significantly longer blood circulation durations. NP surfaces’ most prevalent functional groups are amines and carboxyls, which allow antibodies, fluorescent dyes, peptides, radionuclides, therapeutic agents aptamers, quantum dots and other small molecules to bind. The NPs may be directed to a certain location or kind of cell using antibodies and peptides, and they can be imaged using quantum dots and fluorescent dyes.144
Nanotechnology is rapidly being used in medical application for therapeutic and diagnostic purposes, and it has great promise in various applications. Nanoparticles have been used as drug delivery systems and diagnostic imaging agents, paving the way for tissue target delivery that can significantly enhance therapeutic efficiency while reducing drug side effects.145 By designing and preparing dual-purpose nanomaterials that can serve as both diagnostic medical devices and drug delivery systems, it is also conceivable to integrate these two functionalities in one particle.
Theranostic is a term that was used to describe the idea of combining diagnostics and therapy.146 Researchers define a theranostic agent as a system that simultaneously allows and monitors drug delivery and outcomes, consequently allowing a proper therapy–patient match.147 Figure 7 illustrates the theranostic NPs and their uses.
 |
Figure 7 Theranostic NPs and their functions. |
Nanotheranostic Agents for the Treatment of TB Synthesized Using the Host–Guest Supramolecular Chemistry
Host–guest supramolecular chemistry is the chemistry of non-covalent intermolecular molecular assemblies of the host and the guest species. For the synthesis of TB nano-theranostics, usually, the hosts are selected from nanomaterials with a high specific surface area so that they can host one or more active agents to simultaneously serve as the TB diagnostic and therapeutic purposes. Otherwise, diagnostic and therapeutic active agents can be loaded separately onto the host, resulting in the nano delivery system for diagnostic and therapeutic, respectively. Nanomaterials such as layered hydroxides,148–150 carbon nanomaterials such as CNTs, graphene and their derivatives,151–153 chitosan154 polymeric155 and inorganic156 nanoparticles are subjected to intense research for these purposes.
Generally, any nanomaterials – 0-, 1-, 2- or 3-dimensional – can be used to host the guests; any active agents for anti-TB drugs such that the final product of the host–guest complex can be formed through various non-covalent bonding between them. Under a suitable microenvironment, due to the presence of external forces such as the higher affinity of the incoming ions or the disintegration of the host, the breaking of the bonds between the host and the guest will be taken place, resulting in the guest will be released gradually (due to the reversible, non-covalent bond between the host and the guest) and therefore resulting in the slow or controlled release of the drug, which later taken by the adsorbed on the target cell. This will reduce the over-dosage and under-dosage drug concentration, and maintain the drug concentration in the therapeutic window, therefore enhancing the drug availability, improving efficacy and therefore better compliancy of the patients.
Theranostics successfully combines therapy and diagnostics to create more specific and individualized treatment methods for various pathologies, as well as to combine diagnostic and therapeutic agents together in a one agent, resulting in an effective therapeutic approach that includes diagnosis and drug target delivery, and finally monitoring the treatment responses. Theranostics is indeed a revolution from examination and development of drugs to prediction, prevention, and drug customization that leads to enhanced the quality of the treatment.157 Theranostic agents are classified as integrated nontherapeutic systems that able to diagnose, provide targeted therapy along with monitor the treatment response. This integrated strategy provides several prospects for the advancement of customized medicines. It provides the monitoring of the release of drugs, biodistribution and accumulation at the targeted area, dosage modification to individual patients, and consequently, tracking of disease progression.158 Recent therapies for the treatment and diagnosis of TB mostly relied on complicated and lengthy multidrug treatments. Although these therapies are effective in the early stage of infection, they lose effectiveness on latent infection and in the later stage of the treatment. Besides this, the development of drug resistance has negatively affected the effectiveness of the current treatments of TB. The same situation exists in antibiotic drug market.
However, recently, the TB infection awareness and understanding have inspired researchers to develop host-directed approaches and inhaled TB therapies.159 Lung anatomy and biology have posed several obstacles, while multifunctional NPs with specific modifications in size, surface charge and structure have been produced and these properties should be adjusted in order to pass these NPs into the mucus barrier and reach the target site. Furthermore, covering the NP with copolymers, dendrimers, polymers, inorganic compounds, proteins, surfactants, and lipids can increase its surface stability. To some extent, polymer coatings based on polyethylene glycol or dextran maintain NPs biocompatible and allow for longer blood circulation durations.
Multi-functional NPs can play multiple purposes simultaneously, for example, treatment and imaging of the target disease with theranostic NPs. Therapists can diagnose diseases at earlier phases, monitor treatment noninvasively, facilitate site-specific drug delivery to reduce side effects, and enhance preoperative staging only with the help of therapeutic molecule combination with effective and safe contrast agents. Table 5 lists the various forms of NP contrast agents as well as certain theranostic NPs that incorporate with them.
 |
Table 5 The Benefits and Drawbacks of Various Contrast Agents for Nanotheranostic Applications |
Medical imaging is used to diagnose and monitor many diseases by using techniques like positron emission tomography (PET), X-ray computed tomography (CT) and magnetic resonance imaging (MRI). They are simple to use, have a low level of invasiveness, and may provide clear images with details. PET scans are frequently combined with MRI or CT images for therapy since the combination provides metabolic and anatomic details related to a tumor. In addition, in vivo imaging from metabolic, physiological, and molecular activity may be accomplished via near-infrared fluorescence optical imaging. A wide range of organic dyes such as radioisotopes as well as chelated metal ions conjugated to targeting ligands was designed to provide contrast and improve the effectiveness of medical imaging, and though due to their advantages, plenty of innovative NPs including fullerenes, carbon nanotubes, transition metal oxides, semiconductor quantum dots, and noble metals have obtained considerable interest to be used as contrast agents. Organic materials including liposomes, micelles, and polymers are employed to create NPs which also are encapsulated and delivered the new contrast agents. Theranostic NPs, with their imaging and therapeutic capabilities, have the opportunity to prognosis, diagnosis and treat the diseases. For the treatment of any kind of disease, swift treatment, early and accurate detection are the most vital steps.
For the last few decades, several nanotechnology-based platforms have been created and employed to enhance the diagnosis and treatment of diseases.96 Contrast agents imaging has been created to enhance the quality and quantity of the information collected through MRI procedures. Metals are used in most of these agents to produce contrast; however, those including gadolinium, may be quite toxic. The weak or poor signal intensity of MRI imaging of the lungs is a key obstacle to diagnosing lung diseases; however, emerging nanotechnology is overcoming this constraint. Nanoparticles loaded with metals with shorter relaxation time and entrapment of potentially toxic metal ions offer opportunities as effective and safe MRI contrast agents in biomedicine. Recently, Branca et al employed superparamagnetic iron oxide NPs (SPIONs) worked with luteinizing hormone-releasing hormone to use high-resolution hyperpolarized 3He MRI to specifically target and observe pulmonary micrometastases.160 From another aspect, barium and iodinated substances used as clinical X-ray CT contrast agents have large densities that seem to cause them to appear radiopaque through the CT scan.
Even though there are not any NPs contrast agents that have been approved by the medical community for scanning, initial CT surveys have been conducted to look into utilizing the gold having high atomic numbers and densities, which gives a significant improvement in contrast compared to conventional iodine contrast agents. Recently, a study was published by Wang et al on the use of embedded gold NPs in modified dendrimers with folic acid for the targeted CT scanning of a patient with lung cancer.161 Most NP contrast agents are currently in the early phase of research or preclinical testing, despite their helpful features and prospective applications. Although the importance of inflammatory signaling and oxidative stress in chronic obstructive pulmonary disease COPD and cystic fibrosis CF has been proven, the absence of real-time diagnosis of inflammatory/oxidative states may also lead to incorrect therapy, which can result in chronic and deadly pulmonary pathophysiology. Cho et al synthesized chemiluminescent micelles capable of peroxalate interactions in order to detect hydrogen peroxide (H2O2) concentrations as low as 100 nm and imaging of H2O2 delivered in mice in a recent work.162
Mycobacterium DNA detection for clinical samples via NPs has now been discovered, and it has a bright future ahead. A practical and inexpensive biosensor technology for detecting mycobacteria from the Mycobacterium TB complex was recently presented, consisting of a photodetector nanocrystalline silicon with appropriate application to reduce human errors and failures. To identify gold NPs in clinical sputum samples, ultrasensitive approaches based on scan-based, fluorometric, colorimetric, surface-enhanced Raman scattering, and electrochemical procedures have been developed. The detection of gold NPs generated by thiol-modified oligonucleotides has been established to be accurate, simple, and inexpensive. With the use of these NPs, Mycobacterium TB may be identified from other Mycobacterium species. In addition, quantum dots, fluorescent semiconductor and magnetic beads have been employed to identify Mycobacterium species DNA, without the PCR requirement. A probe consisting of superparamagnetic iron oxide NPs was developed for detecting extrapulmonary TB.163
Table 5 indicates the benefits and drawbacks of various contrast agents for nanotheranostic applications.
Nanocarrier-Based Therapeutic Agents for the Treatment of Tuberculosis
Nanoparticles are particle structures with a diameter of fewer than 100 nanometers. The bioactive is trapped in the polymatrix structures as solid solutions or entangled particulates, and it could be physically or chemically bonded to the particle surface. There are approximately 2300 kilometers of airways and 300 million alveoli in the human lungs for gas exchange. In adults, lungs’ surface area ranges from 75 to 140 m2. In comparison to the airways, the alveoli have an extremely large surface size and intimate air-blood contact, making them less well-defended towards inhaled NPs.41 The nanocarrier system of antibiotics was created with the goal of eliminating the issue of drug resistance, shortening treatment duration, and reducing drug side effects with antiretroviral treatment. However, the first generations of ATDs still are effective. The main goals of pharmaceutical technology are to eliminate the therapeutic agents’ major technological disadvantages, for example, reduced aqueous solubility and stability, and bioavailability, in order to improve adherence and compliance, and to achieve better drug’s effectiveness by concentrating on infection reservoirs (for example, alveolar macrophages). Hence, nanocarriers appear to be one of the most promising technologies in this context.
Nanocarrier technologies have rekindled interest in targeted drug delivery in pulmonary tuberculosis. Lungs are a desirable target for drug delivery because of their noninvasive structure, which allows them to possibly have high systemic bioavailability, avoid initial metabolism, have faster therapeutic activity, and also have a large specific surface area. There are several advantages of using nanocarrier drug delivery in pulmonary; to obtain relatively uniform drug dose distribution amongst alveoli, enhanced drug solubility beyond its own aqueous solubility, sustained drug release, that lessen dosing frequency, suitability for macromolecule delivery, lower chance of side effects, better patient adherence and its possibility for drug internalization by cells.173,174 Carriers enable us to construct multiple delivery agents but also give flexibility for designing the delivery route. Consequently, according to the formulations, ATDs may be delivered via implants/injections, or by respiratory or oral.175,176
Carriers can be broadly classified into natural or synthetic. Poly(
Polymeric Nanoparticles
Natural biodegradable polymers indeed are prominent application for managing the drug release. Langer and Folkman generated the drug-delivery method with polymer-based for macromolecule delivery in 1976. The first polymeric NPs had limited therapeutic effects due to their fast release through the reticuloendothelial system (RES) following intravenous injection. This issue was resolved in 1994 with the development of long-circulating stealth polymeric NPs.176,177 Polymeric NPs have various significant properties that make them ideal to deliver the antimicrobial drugs. To some extent, polymeric NPs are sustainable, and may be produced with a narrower size dispersion. Additionally, nanoparticle parameters such as size, zeta potential, and drug-release pattern may be precisely regulated during synthesis using different polymer lengths, surfactants, and organic solvents. Furthermore, the functional groups on the surfaces of polymeric NPs can be changed chemically with targeting ligands and drug moieties. For antimicrobial drug delivery, polymeric NPs now come in two varieties. First is created by the spontaneous self-assembly of diblock copolymers with hydrophilic and hydrophobic regions. This hydrophobic part creates a polymer core that holds the drugs, whilst the hydrophilic part protects the core against opsonization and destruction. The hydrophobic chain length can be modified to control the rate of drug release. A number of biopolymers, including polycaprolactone (PCL) and poly(cyanoacrylate) (PCA), have been employed to produce the hydrophobic polymeric core, while polyethylene glycol (PEG) was utilized as a hydrophilic part. Hence, due to the general hydrophobic properties of the NP core, polymeric NPs are frequently employed to deliver drugs that are less water-soluble.46
Solid Lipid Nanoparticles
Since 1990, solid lipid nanoparticles (SLNs) are subjected to intense interest as an antibacterial drug delivery system. For several drug-delivery purposes, SLNs are generally particulate systems with average sizes ranging from 50 to 1000 nm. Solid-phase lipids make up the vast majority of SLNs, which could prepare at room temperature and surfactants for emulsifying agents.178 Stearic acid, cetyl palmitate, etc, are solid lipids used in the formulation of SLN. Surfactants including phosphatidylcholine, soybean lecithin, sodium cholate, poloxamer 188, and sodium glycocholate are often employed as emulsifying agents to sustain lipid dispersion. Ultrasonication, high-shear mixing, spray drying and high-pressure homogenization (HPH) are standard techniques for producing SLNs.179 TB infection can move from the lungs to the lymphatic system in certain severe forms. ATDs like INH, RIF and PZA can be delivered to the lymphatic systems as well as the lungs via SLNs. These SLNs after phagocytosed by AMs, delivered to lymphoid organs after they reach the lungs. Radio-labeled aerosolized SLNs were used to evaluate the SLN delivery process and biodistribution via pulmonary delivery in mice. Effective uptake of radio-labeled SLNs by the lungs was observed and indicated a sustained release of the antibiotic payloads carried by the SLNs, that can efficiently clear the viruses and bacteria hosted at these lymphatic zones.41
Liposomes
Liposomes are defined as multilayer carriers with a membranous lipid bilayer enclosing an aqueous volume. They are the most extensively researched approaches for controlled drug delivery to the lungs as they are capable to entrap both hydrophobic and hydrophilic drugs since they may be created by phospholipids endogenous to the lungs as surfactants.180 Drugs encapsulated in liposomes have higher bactericidal efficacy than free drugs, notably in the monocytes and macrophages treatment.41 The release of the drug from the liposome may help the drug to maintain its position inside the lungs while inhibiting its release to other tissues. Liposomes-based drug delivery is superior; low toxicity, a wide range of sizes (20 nm–1 mm), ability to solubilize drugs with poor water-solubility, facilitating their nebulization, represent as a biobased pulmonary reservoir with prolonged residence period, minimize mucociliary clearance of drugs owing to their surface viscosity, used as a targeting agent within the lung, particularly to infected or impaired AMs and the lung epithelial tissue. This unique delivery method along with the presence of the nanocarriers can be delivered to the lungs in a variety of methods: insufflations, nebulization, instillation, etc.181
Microspheres
Microspheres are tiny spheres with sizes in micrometers sizes, usually 1 to 1000 μm. This drug carrier can be made in a variety of particle sizes, which is important for nanocarrier’s in vivo deposition. Also, drugs may be readily integrated with great loading and efficiency, and variable drug-release ratios may be obtained by manipulating the synthetic synthesis technique. In vitro and in vivo, microspheres have greater chemical and physical stability. Entrapped drugs represent longer duration of action with a slower rate of release. The increased stability facilitates the formulation.41
Chitosan Nanoparticles
The applications of natural polymers for anti-tubercular drug delivery for therapeutic or theranostic purposes are enormously grown in past decades. Chitosan (CS) is among the drug delivery methods that play a vital application in anti-TB drug delivery field. It is a cationic polysaccharide with unique properties that makes CS a potential delivery vehicle.182 CS has been utilized as a matrix or coating material to protect drugs from chemical or enzymatic degradation. As a result, CS-based nanocarrier systems have been significantly used for targeted drug administration for TB treatment.16
Gold Nanoparticles
Gold NPs have recently received substantial attention for drug delivery purposes. Gold NPs (AuNPs) recently are utilized for the drug delivery system for TB therapy and successfully and significantly suppress the TB cell growth.183
Silica Nanoparticles
Silica NPs exhibited various unique advantages such as biocompatibility, biodegradability, hydrophobicity, stability, resistance to pH difference, and capability to incorporate with a therapeutic agent.
Graphene and Graphene Oxide
Graphene and graphene oxide are becoming popular nanocarrier systems for TB drug delivery. Its high specific surface area enables them to host single or multiple active agents to be transported to the target location.184
Carbon Nanotubes
Carbon nanotubes (CNTs) recently are developed as nanocarriers to explore their potential function as nanocarriers. Owing to chemical and physical unique features, CNTs have also been utilised as a nano-drug delivery structure for anti-TB drugs.184
Niosomes
The self-assembly of non-ionic amphiphiles inside an aqueous phase generates non-ionic surfactant-based vesicles (niosomes), which are closed bilayer nanostructures. The assembly is seldom spontaneous, and it often needs some form of energy input, like mechanical agitation or temperature. Thus, the hydrophobic sections of the compound are protected from the aqueous solvent, while the hydrophilic head sections have the most interaction with it. These structures, which are similar to liposomes, can encapsulate aqueous solutes and perform as drug delivery nanocarriers. Non-ionic surfactants have been used as a substitute for phospholipids due to their low cost and higher stability.185
Dendrimer
A dendrimer is a new form of polymer material. They are receiving increasing attention due to their distinct structure, the maximum level of control over molecular weight, and morphology, that is resulted in the production of unimolecular micelles. Poly(propylene imine) (PPI) dendrimers are among the many potential dendrimers that have just recently been formed on a large scale and analyzed either experimentally or by molecular modeling. The PPI dendrimers’ potential applications are based on their following characteristics; standard morphology and sizes, the greater amount of freely available end groups, nitrile or amino groups, the capability of end group adjustment to control solubility properties, stability, toxicity, reactivity, polyelectrolyte property, glass transition temperature, and the capability to encapsulate guest molecules are all important factors to consider. Dendrimers must be non-toxic and biocompatible if they are to be used as drug carriers.41,186
Dry Powder
Pulmonary drug delivery with the method of dry powder inhalers (DPIs) has accelerated progress in recent decades to realize the full potential for lung disease therapy, both local and systemic, due to its propellant-free nature, great patient adherence, higher drug dosage loading and drug stability. However, DPIs’ effectiveness is dependent on several factors, including the inhaler’s design, the powder formula, and the patient’s airflow. DPI performance has increased dramatically over the last decade due to the use of engineered nanoparticles and improved dosage formulations.187
Cyclodextrins
Cyclodextrins contain oligo-saccharides made up of six to eight glucose molecules connected by β-1,4-glucosidic linkages. These cyclical compounds have an inner hydrophobic cavity as well as a hydrophilic external surface, making them susceptible to forming complexes with other hydrophobic compounds. They have been utilized in order to deliver a large amount of drugs and maintain their stability and solubility.188
Nanoemulsions
Nanoemulsions are oil-in-water (o/w) colloidal carriers and the particle sizes ranging from 10 to 100 nm that are thermodynamically stable. The fundamental benefit of these methods is that they are self-generated and can be mass-produced without requiring high energy for homogenization. Filtration can also be used to sterilize them. The increased absorption of nanoemulsions by phagocytic cells explained the nanocarrier’s passive targeting features. After oral administration, these are also absorbed by lipoprotein receptors, which are mostly found in the liver.189
Nanosuspensions
Nanosuspensions are defined as colloidal dispersions from the pure drugs that are sustained by surfactants and exist in sub-micron sizes. The reduction of particles to nanoscale which is called “nanonization” is a beneficial platform helping to enhance and boost the drug solubility with a high melting point and great solute–solute interactions, along with low lipid and water solubility. The pure drug particles’ solid and dense states offer a maximum mass per volume ratio, which is extremely important in methods that need heavy loadings of the drug. Considering its potential features, several researches aimed at improving TB medication have been published.189
The aforementioned nanocarriers are examples of carriers that can overcome drug resistance and facilitate ATD delivery to MTB infection. As a consequence, medicines that are well known for their beneficial effects can be safely used for effective TB treatment in the form of nanocarriers. The novel negative effects caused by the usage of these carriers, on the other hand, must be investigated. Tables 6 indicates the list of nanocarriers used for the treatment of TB.
 |
Table 6 Nanocarriers That Have Been Used for the Treatment of TB |
Ligand Anchored Nanocarrier Systems for Pulmonary Tuberculosis
To improve the targetability, the nanocarriers are conjugated with ligand, which targets the receptors present on the desire sites or the macrophage surface as the nanocarriers are excreted from the body by the process of opsonization and phagocytosis. Various ligands have been used as a ligand to target the TB sites such as mannose, mycolic acid, ;ectin, pH-sensitive liposomes, aptamers, etc, are being used for targeting antitubercular drugs.
Lectin
Mycobacterium tuberculosis (Mtb) is recognized by various pathogen recognition receptors (PRRs) which are expressed on the surface of innate and adaptive immune cells. The category of pathogen recognition receptors (PRRs), which include C-type lectin receptors, may identify a wide range of exogenous and endogenous ligands.211 C-type lectins have been identified as determinant players in the early recognition of invading pathogen.212 Lectin can be employed as a mucosal ligand to promote the absorption of TB drugs and enhance the target and binding of nanocarrier to the surface.213
Mycolic Acid
Numerous substances found in the mycobacterial cell wall can act as receptors for ligand targeting. Since mycolic acids (MA) are the predominant lipids in the outer cell wall of Mycobacterium species, they are among the potential ligands.214 Lemmer et al conducted a study on Mycolic acid as a ligand using PLGA nanoparticles (NPs) for targeting the TB cells. They found that MA can be a promising mycobacterial ligand of nano-encapsulated drugs carrier for targeting the tuberculosis mannose.196
Another ligand that can be used as to target the Mtb is mannose. In situ gel-based nanocarrier system with mannose-conjugated rifampicin-loaded chitosan nanocarrier has been developed by Prabhu et al. This approach ensures localization in the intra-articular cavity, prolonged release, and conjugation of nanocarrier with mannose as ligand to increase high uptake and deliver the rifampicin drug.215 In order to target and improve the therapeutic index of rifampicin, Vieira et al created solid lipid nanoparticles (SLNs) employing mannose as a lectin receptor ligand. The research indicate that the mannosylated models are an effective and safe approach to treating tuberculosis.216 Mannosylated chitosan nanoparticles conjugated hyaluronic acid (HA) that loaded with isoniazid were synthesized by Mukhtar et al in 2022 and successfully used as an inhalation powder for the treatment of TB.217
Ligand-Anchored pH-Sensitive Liposomes
Drug delivery for TB can be accomplished using ligand-anchored pH-sensitive liposomes. A dry powder inhaler with a ligand-anchored pH-sensitive liposome was designed and described by Bhardwaj et al for the specific delivery of TB drugs to the lungs. The sustained drug release and efficient in vitro cellular absorption were reported. They concluded that ligand-anchored pH-sensitive liposomes are one of the most successful delivery systems for targeted drug delivery in pulmonary TB.218 Bhardwaj et al 217 by using macrophage-specific ligands also created ligand-appended liposomes encapsulated with ATDs in the surface of liposome and delivered in the respiratory system to enhance the impact of chemotherapy over the pulmonary TB.219
Nanoembedded Microparticles
For the purpose of TB drug delivery, nanoembedded microparticles also were formulated. Goyal et al encapsulated RIF and INH into nanoembedded microparticles for pulmonary delivery and discovered that the drugs’ effectiveness was improved while systemic toxicity was significantly reduced. Thus, it may be a potential carrier for ATD’s delivery. In a mouse model of TB infection, Grenha et al synthesized nanoembedded microparticles that were loaded with isoniazid and rifabutin which was significantly successful.219
Future Research and Development
Nanotechnology’s application in medicine has already yielded several achievements and is on its way to becoming an important part of the medical sector. The ever-increasing number of research articles and patents awarded in the subject of nanocarrier systems for drug delivery attests to this reality. Multidrug resistance (MDTB) with toxic side effects that lead to diagnosis and treatment failure is still a major concern in the treatment of tuberculosis. The target for the future is to develop or manufacture efficient and effective nano theranostic treatments that reduce treatment time, eliminate drug toxicity, and also have better bioavailability, as well as to discover a method to eliminate the transmission of causative organisms, however this is challenging, multifaceted, and difficult cause of limitations in diagnosis, multidrug resistance, and poor patients’ adherence to therapy. A range of novel anti-TB potential nano-medications are in the pipeline; however, key concerns are included: lack of systematic research effort, massive costs, difficulties in targeting MDR and latent bacilli, along with toxicities of drugs. These are the motivations that drive the future research for novel and unique alternative nano-therapeutic drugs. It was discovered that nanoparticle-based therapies and nanotheranostic as a combination of diagnostic and therapeutic features through one platform might provide a possible benefit over conventional TB therapy, with the future goal of decreasing TB drug dosage and enhance patient compliance.
Conclusion
Tuberculosis is among the most serious health issues worldwide with an annual rise in the number of patients. Nowadays, the conventional anti-tubercular therapeutic method needs high dosages of numerous drugs over a longer duration. This tends to result in drug-related detrimental effects or the development of MDR. Furthermore, the drugs currently in use have practical limits of solubility, stability, and penetration. Also, it may lead to resistance over time, resulting in relapse, and extend to peripheral body parts, which caused secondary TB.
In this review, current developments in methodologies and concepts for pulmonary drug delivery systems have been briefly outlined. New drug delivery techniques based on nanocarriers and ligands were explored, and various nano delivery systems were summarized. The use of pulmonary nanodrug delivery systems as a therapeutic agent for the treatment of TB has become extremely useful. Targeted drug delivery, enhanced drug solubility, decreased toxicity, reduced side effects compared to conventional drug regimens that cause MDR and XDR, and synergistic therapeutic effects are among the benefits of using nanomaterials to deliver drugs for the treatment of infectious lung diseases. It might be challenging to determine if a certain drug delivery system feature is advantageous or disadvantageous since it depends on the treatment procedures and targets that have been defined. Although nanomedicines have great potential, they are currently in the middle of their development. Research is still being done on concerns including physicochemical analysis, pharmacological activity, and pharmacodynamic applications. It is anticipated that new drugs will be available as a nanomedicine therapy, particularly the respiratory system, during the next several years based on current trends in clinical trial stages. Consequently, the overall future for nanoparticle drug delivery systems is promising, since they are being developed not just for diagnosing and treating respiratory diseases but also for a wide range of other diseases.
Acknowledgments
This work was supported by Gran Putra Berimpak, Grant No. UPM/800-3/3/1/GPB/2019/9678800.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Cooper AM. Cell-mediated immune responses in tuberculosis. Annu Rev Immunol. 2009;27:393–422.
2. Stewart GR, Robertson BD, Young DB. Tuberculosis: a problem with persistence. Nat Rev Microbiol. 2003;1(2):97–105.
3. World Heath Organization. Rapid Communication: Key Changes to the Treatment of Drug-Resistant Tuberculosis. World Heath Organization; 2022.
4. WHO G. Global tuberculosis report 2020. Glob Tuberc Rep. 2020;2020:S7–S12.
5. World Heath Organization. WHO Declares Tuberculosis a Global Emergency. World Heath Organization; 1993:0303–8408.
6. Debjit B, Chandira R, Jayakar B, Kumar KS. Recent trends of drug used treatment of tuberculosis. J Chem Pharm Res. 2009;1(1):113–133.
7. Greenblatt DJ. Elimination half-life of drugs: value and limitations. Annu Rev Med. 1985;36(1):421–427.
8. Dye C, Watt CJ, Bleed DM, Hosseini SM, Raviglione MC. Evolution of tuberculosis control and prospects for reducing tuberculosis incidence, prevalence, and deaths globally. JAMA. 2005;293(22):2767–2775.
9. Chan ED, Iseman MD. Multidrug-resistant and extensively drug-resistant tuberculosis: a review. Curr Opin Infect Dis. 2008;21(6):587–595.
10. Gladwin MT, Plorde JJ, Martin TR. Clinical application of the Mycobacterium tuberculosis direct test: case report, literature review, and proposed clinical algorithm. Chest. 1998;114(1):317–323.
11. Griffiths G, Nyström B, Sable SB, Khuller GK. Nanobead-based interventions for the treatment and prevention of tuberculosis. Nat Rev Microbiol. 2010;8(11):827–834.
12. Nasiruddin M, Neyaz M, Das S. Nanotechnology-based approach in tuberculosis treatment. Tuberc Res Treat. 2017;2017. doi:10.1155/2017/4920209
13. Müller R, Mehnert W, Lucks J-S, Schwarz C, Zur Mühlen A. Solid lipid nanoparticles (SLN): an alternative colloidal carrier system for controlled drug delivery. Eur J Pharm Biopharm. 1995;41(1):62–69.
14. Sharma A K, Sharma R, Jhorar R, Kumar R. Nanomedicine in therapeutic intervention of tuberculosis meningitis. Curr Nanosci. 2015;11(1):15–22.
15. Kumar M, Jha A, Dr M, Mishra B. Targeted drug nanocrystals for pulmonary delivery: a potential strategy for lung cancer therapy. Expert Opin Drug Deliv. 2020;17(10):1459–1472.
16. Sarkar K, Kumar M, Jha A, Bharti K, Das M, Mishra B. Nanocarriers for tuberculosis therapy: design of safe and effective drug delivery strategies to overcome the therapeutic challenges. J Drug Deliv Sci Technol. 2021;67:102850.
17. Martini M, Besozzi G, Barberis I. The never-ending story of the fight against tuberculosis: from Koch’s bacillus to global control programs. J Prev Med Hyg. 2018;59(3):E241.
18. Hadi SA, Brenner EP, Mani R, Palmer MV, Thacker T, Sreevatsan S. Genome Sequences of Mycobacterium tuberculosis Biovar bovis Strains Ravenel and 10-7428. Microbiol Resour Announc. 2021;10(24):e00411–e00421.
19. Robinson RK. Encyclopedia of Food Microbiology. Academic press; 2014.
20. Moreno S. Tuberculosis multirresistente: epidemiología actual, esquemas terapéuticos, nuevos fármacos. Rev Esp Quimioter. 2016;29(1):35–38.
21. Tuberculosis drugs and mechanisms of action. National Institute of Allergy and Infectious Diseases. https://www.niaid.nih.gov/diseases-conditions/tbdrugs.
22. Ochi K. Phylogenetic analysis of mycolic acid-containing wall-chemotype IV actinomycetes and allied taxa by partial sequencing of ribosomal protein AT-L30. Int J Syst Evol Microbiol. 1995;45(4):653–660.
23. Tsukamura M. A review of the methods of identification and differentiation of mycobacteria. Rev Infect Dis. 1981;3(5):841–861.
24. Karami-Zarandi M, Bahador A, Gizaw Feysia S, et al. Identification of non-tuberculosis mycobacteria by line probe assay and determination of drug resistance patterns of isolates in Iranian patients. Arch Razi Inst. 2019;74(4):375–384.
25. Tió-Coma M, Wijnands T, Pierneef L, et al. Detection of Mycobacterium leprae DNA in soil: multiple needles in the haystack. Sci Rep. 2019;9(1):1–7.
26. Nardell EA. Transmission and institutional infection control of tuberculosis. Cold Spring Harb Perspect Med. 2016;6(2):a018192.
27. Chapter C. Transmission and Pathogenesis of Tuberculosis. US: Taylor and Francies; 2016.
28. Fennelly KP. Particle sizes of infectious aerosols: implications for infection control. Lancet Respir Med. 2020;8(9):914–924.
29. Murray JF. The Normal Lung: the Basis for Diagnosis and Treatment of Pulmonary Disease. WB Saunders Company; 1986.
30. Dannenberg A. Pathogenesis of Pulmonary Tuberculosis: Host-Parasite Interactions, Cellmediatedd Immunity, and Delayed-Type Hypersensitivity: Basic Principles. New York: Springer Verlag; 1994.
31. Smith DW, Wiegeshaus EH. What animal models can teach us about the pathogenesis of tuberculosis in humans. Rev Infect Dis. 1989;11(Supplement_2):S385–S393.
32. Reggiardo Z, Middlebrook G. Failure of passive serum transfer of immunity against aerogenic tuberculosis in rabbits. Proc Soc Exp Biol Med. 1974;145(1):173–175.
33. Canetti G. The Tubercle Bacillus in the Pulmonary Lesion of Man: Histobacteriology and its Bearing on the Therapy of Pulmonary Tuberculosis. Springer Publishing Company; 1955.
34. Dannenberg JAM. Immune mechanisms in the pathogenesis of pulmonary tuberculosis. Rev Infect Dis. 1989;11(Supplement_2):S369–S378.
35. Styblo K, Enarson DA. Epidemiology of Tuberculosis. Vol. 24. Royal Netherlands Tuberculosis Association The Hague; 1991.
36. Bass JB, Farer LS, Hopewell PC, Jacobs RF, Snider DE. Diagnostic standards and classification of tuberculosis. Am Rev Respir Dis. 1990;142(3):725–735.
37. Susilawati TN, Larasati R. A recent update of the diagnostic methods for tuberculosis and their applicability in Indonesia: a narrative review. Med J Indones. 2019;28(3):284–291.
38. Cobat A, Orlova M, Barrera L, Schurr E. Host genomics and control of tuberculosis infection. Public Health Genomics. 2013;16(1–2):44–49.
39. Rate C. Tuberculosis in Alameda County; 2015.
40. Yu WY, Wang YX, Mei JZ, Hu FX, Ji LC. Overview of Tuberculosis. In: Tuberculosis Control in Migrating Population. Springer; 2020:1–10.
41. Gupta S, Kumar P, Gupta MK, Vyas SP. Colloidal carriers: a rising tool for therapy of tuberculosis. Crit Rev Ther Drug Carr Sys. 2012;29(4):299–353.
42. Wen Z, Li T, Zhu W, Chen W, Zhang H, Wang W. Effect of different interventions for latent tuberculosis infections in China: a model-based study. BMC Infect Dis. 2021;22:488.
43. Lee SH. Tuberculosis infection and latent tuberculosis. Tuberc Respir Dis. 2016;79(4):201–206.
44. Esmail H, Barry III CE, Wilkinson RJ. Understanding latent tuberculosis: the key to improved diagnostic and novel treatment strategies. Drug Discov Today. 2012;17(9–10):514–521.
45. Vonasek B, Ness T, Takwoingi Y, et al. Screening tests for active pulmonary tuberculosis in children. Cochrane Database Syst Rev. 2020;7. doi:10.1002/14651858.CD013693.pub2
46. Kaur J, Gill G, Jeet K. Characterization and Biology of Nanomaterials for Drug Delivery. The Netherlands: Elsevier Amsterdam; 2019.
47. Lee SH. Diagnosis and treatment of latent tuberculosis infection. Tuberc Respir Dis. 2015;78(2):56–63.
48. Piccazzo R, Paparo F, Garlaschi G. Diagnostic accuracy of chest radiography for the diagnosis of tuberculosis (TB) and its role in the detection of latent TB infection: a systematic review. J Rheumatol Suppl. 2014;91:32–40.
49. Kiazyk S, Ball T. Tuberculosis (TB): latent tuberculosis infection: an overview. Can Commun Dis Rep. 2017;43(3–4):62.
50. Özüdogru E, Cakli H, Altuntas E, Gürbüz M. Effects of laryngeal tuberculosis on vocal fold functions: case report. Acta otorhinolaryngologica italica. 2005;25(6):374.
51. Lee KM, Choe KH, Kim SJ. Clinical investigation of cavitary tuberculosis and tuberculous pneumonia. Korean J Intern Med. 2006;21(4):230.
52. Ray S, Talukdar A, Kundu S, Khanra D, Sonthalia N. Diagnosis and management of miliary tuberculosis: current state and future perspectives. Ther Clin Risk Manag. 2013;9:9.
53. Jeon D. Tuberculous pleurisy: an update. Tuberc Respir Dis. 2014;76(4):153–159.
54. Kelestimur F. The endocrinology of adrenal tuberculosis: the effects of tuberculosis on the hypothalamo-pituitary-adrenal axis and adrenocortical function. J Endocrinol Invest. 2004;27(4):380–386.
55. Benjelloun A, Darouassi Y, Zakaria Y, Bouchentouf R, Errami N. Lymph nodes tuberculosis: a retrospective study on clinical and therapeutic features. Pan Afr Med J. 2015;20:65.
56. Johnson JL, Ellner JJ. Tuberculosis and atypical mycobacterial infections. In: Tropical Infectious Diseases. Elsevier Inc; 2006:394–427.
57. Srivastava U, Almusa O, Tung KW, Heller MT. Tuberculous peritonitis. Radiol Case Report. 2014;9(3):971.
58. Daher EDF, da Silva Junior GB, Barros EJG. Renal tuberculosis in the modern era. Am J Trop Med Hyg. 2013;88(1):54.
59. Chin JH. Tuberculous meningitis: diagnostic and therapeutic challenges. Neurol Clin Pract. 2014;4(3):199–205.
60. Mayosi BM, Burgess LJ, Doubell AF. Tuberculous pericarditis. Circulation. 2005;112(23):3608–3616.
61. Silva DR, Muñoz-Torrico M, Duarte R, et al. Risk factors for tuberculosis: diabetes, smoking, alcohol use, and the use of other drugs. Jornal Brasileiro de Pneumologia. 2018;44:145–152.
62. Narasimhan P, Wood J, MacIntyre CR, Mathai D. Risk factors for tuberculosis. Pulm Med. 2013;2013. doi:10.1155/2013/828939
63. Hershkovitz I, Donoghue HD, Minnikin DE, et al. Tuberculosis origin: the Neolithic scenario. Tuberculosis. 2015;95:S122–S126.
64. Sakula A. Robert Koch: centenary of the discovery of the tubercle bacillus, 1882. Thorax. 1982;37(4):246–251.
65. Glaziou P, Floyd K, Raviglione MC. Global epidemiology of tuberculosis. Thieme Med Publish. 2018;34:271–285.
66. Baranyai Z, Soria-Carrera H, Alleva M, et al. Nanotechnology-Based targeted drug delivery: an emerging tool to overcome tuberculosis. Adv Ther. 2021;4(1):2000113.
67. Pardhi VP, Jain K. Impact of binary/ternary solid dispersion utilizing poloxamer 188 and TPGS to improve pharmaceutical attributes of bedaquiline fumarate. J Drug Deliv Sci Technol. 2021;62:102349.
68. Pai M, Kasaeva T, Swaminathan S. Covid-19’s devastating effect on tuberculosis care—a path to recovery. NEJM. 2022;386(16):1490–1493.
69. Chakaya J, Petersen E, Nantanda R, et al. The WHO global tuberculosis 2021 report–not so good news and turning the tide back to End TB. Int J Infect Dis. 2022;124:S26–S29.
70. World Health Organization. Global Tuberculosis Report 2020: Executive Summary. World Health Organization; 2020.
71. World Health Organization. Global Tuberculosis Report 2020. World Health Organization; 2021.
72. Singh R, Dwivedi SP, Gaharwar US, Meena R, Rajamani P, Prasad T. Recent updates on drug resistance in Mycobacterium tuberculosis. J Appl Microbiol. 2020;128(6):1547–1567.
73. MacNeil A, Glaziou P, Sismanidis C, Date A, Maloney S, Floyd K. Global epidemiology of tuberculosis and progress toward meeting global targets—worldwide, 2018. MMWR. 2020;69(11):281.
74. Regazzi M, Carvalho AC, Villani P, Matteelli A. Treatment optimization in patients co-infected with HIV and Mycobacterium tuberculosis infections: focus on drug–drug interactions with rifamycins. Clin Pharmacokinet. 2014;53(6):489–507.
75. World Health Organization. Global Tuberculosis Report 2013. World Health Organization; 2013.
76. Marais B, Zumla A. Advancing global tuberculosis control after the UNGA-HLM. Lancet. 2018;392(10153):1096–1097.
77. Glaziou P, Sismanidis C, Floyd K, Raviglione M. Global epidemiology of tuberculosis. Cold Spring Harb Perspect Med. 2015;5(2):a017798.
78. Sudha S. Tuberculosis diagnosis-an overview to the conventional diagnostic methodology and need for nanodiagnosis. Int J Med Eng Inform. 2016;8(1):27–40.
79. Drancourt M, Carrieri P, Gévaudan M-J, Raoult D. Blood agar and Mycobacterium tuberculosis: the end of a dogma. J Clin Microbiol. 2003;41(4):1710–1711.
80. Parker RA. Implications of tuberculosis sputum culture test sensitivity on accuracy of other diagnostic modalities. Am J Respir Crit Care Med. 2019;199(5):664–664.
81. Pestariati P, Rachmawati M. Solid Media (Lowenstein Jensen) and Liquid Media (Mycobacteria Growth Indicator Tube) Usage Against Mycobacterium tuberculosis Culture in Sputum Suspect Tuberculosis. Health Notions. 2021;5(6):220–224.
82. Abdelaziz MM, Bakr WM, Hussien SM, Amine AE. Diagnosis of pulmonary tuberculosis using Ziehl–Neelsen stain or cold staining techniques? J Egypt Public Health Assoc. 2016;91(1):39–43.
83. Lee JE, Kim H-J, Lee SW. The clinical utility of tuberculin skin test and interferon-γ release assay in the diagnosis of active tuberculosis among young adults: a prospective observational study. BMC Infect Dis. 2011;11(1):1–7.
84. Rose DN, Schechter CB, Adler JJ. Interpretation of the tuberculin skin test. J Gen Intern Med. 1995;10(11):635–642.
85. Trajman A, Steffen R, Menzies D. Interferon-gamma release assays versus tuberculin skin testing for the diagnosis of latent tuberculosis infection: an overview of the evidence. Pulm Med. 2013;2013. doi:10.1155/2013/601737
86. Walsh MC, Camerlin AJ, Miles R, et al. The sensitivity of interferon-gamma release assays is not compromised in tuberculosis patients with diabetes. Int J Tuberc Lung Dis. 2011;15(2):179–184.
87. Nalunjogi J, Mugabe F, Najjingo I, et al. Accuracy and incremental yield of the chest X-Ray in screening for tuberculosis in Uganda: a cross-sectional study. Tuberc Res Treat. 2021;2021. doi:10.1155/2021/6622809
88. Desikan P, Panwalkar N, Mirza SB, et al. Line probe assay for detection of Mycobacterium tuberculosis complex: an experience from Central India. Indian J Med Res. 2017;145(1):70.
89. Ninan MM, Gowri M, Christopher D, Rupali P, Michael JS. The diagnostic utility of line probe assays for multidrug-resistant tuberculosis. Pathog Glob Health. 2016;110(4–5):194–199.
90. Shaw JA, Irusen EM, Koegelenberg CF. Pleural effusion: tuberculous effusion; 2019.
91. Laraque F, Griggs A, Slopen M, Munsiff SS. Performance of nucleic acid amplification tests for diagnosis of tuberculosis in a large urban setting. Clin Infect Dis. 2009;49(1):46–54.
92. Phillips M, Cataneo RN, Condos R, et al. Volatile biomarkers of pulmonary tuberculosis in the breath. Tuberculosis. 2007;87(1):44–52.
93. Vishinkin R, Busool R, Mansour E, et al. Profiles of volatile biomarkers detect tuberculosis from skin. Adv Sci. 2021;8:2100235.
94. World Health Organization. Treatment of Drug-Susceptible Tuberculosis: Rapid Communication. World Health Organization; 2021.
95. Laurenzi M, Ginsberg A, Spigelman M. Challenges associated with current and future TB treatment. Infect Disord Drug Targets. 2007;7(2):105–119.
96. Howell M, Wang C, Mahmoud A, Hellermann G, Mohapatra S, Mohapatra S. Dual-function theranostic nanoparticles for drug delivery and medical imaging contrast: perspectives and challenges for use in lung diseases. Drug Deliv Transl Res. 2013;3(4):352–363.
97. Control CfD, Prevention. Treatment for TB disease. US department of Health and Human Services; 2016. Available from https://www.cdc.gov/tb/topic/treatment/tbdisease.htm.
98. Coelho MRT. Impact of mycobacterial recognition by toll like receptors in the regulation of IL-10 and T helper type of responses; 2012.
99. Grange JM, Zumla A. The global emergency of tuberculosis: what is the cause? J R Soc Promot Health. 2002;122(2):78–81.
100. Pym AS, Diacon AH, Tang S-J, et al. Bedaquiline in the treatment of multidrug-and extensively drug-resistant tuberculosis. Eur Respir J. 2016;47(2):564–574.
101. Gils T, Lynen L, de Jong BC, Van Deun A, Decroo T. Pretomanid for tuberculosis: a systematic review. Clin Microbiol Infect. 2021;28(1):31–42.
102. Olayanju O, Esmail A, Limberis J, Gina P, Dheda K. Linezolid interruption in patients with fluoroquinolone-resistant tuberculosis receiving a bedaquiline-based treatment regimen. Int J Infect Dis. 2019;85:74–79.
103. Shan X, Gong X, Li J, Wen J, Li Y, Zhang Z. Current approaches of nanomedicines in the market and various stage of clinical translation. Acta Pharmaceutica Sinica B. 2022;12:3028–3048.
104. Rodrigues AM, Gonçalves SS, de Carvalho JA, Borba-Santos LP, Rozental S, Camargo Z. Current progress on epidemiology, diagnosis, and treatment of sporotrichosis and their future trends. J Fungi. 2022;8(8):776.
105. Dye C. Making wider use of the world’s most widely used vaccine: Bacille Calmette–Guérin revaccination reconsidered. J R Soc Interface. 2013;10(87):20130365.
106. Matsuo K, Yasutomi Y. Mycobacterium bovis Bacille Calmette-Guerin as a vaccine vector for global infectious disease control. Tuberc Res Treat. 2011;2011. doi:10.1155/2011/574591
107. Dockrell HM, Smith SG. What have we learnt about BCG vaccination in the last 20 years? Front Immunol. 2017;8:1134.
108. Jiao X, Lo-Man R, Guermonprez P, et al. Dendritic cells are host cells for mycobacteria in vivo that trigger innate and acquired immunity. J Immunol. 2002;168(3):1294–1301.
109. Tsuji S, Matsumoto M, Takeuchi O, et al. Maturation of human dendritic cells by cell wall skeleton of Mycobacterium bovis bacillus Calmette-Guerin: involvement of toll-like receptors. Infect Immun. 2000;68(12):6883–6890.
110. Azuma I, Ribi EE, Meyer TJ, Zbar B. Biologically active components from mycobacterial cell walls. I. Isolation and composition of cell wall skeleton and component P3. J Natl Cancer Inst. 1974;52(1):95–101.
111. Kleinnijenhuis J, Oosting M, Joosten LA, Netea MG, Van Crevel R. Innate immune recognition of Mycobacterium tuberculosis. Clin Dev Immunol. 2011;2011. doi:10.1155/2011/405310
112. Jung S-B, Yang C-S, Lee J-S, et al. The mycobacterial 38-kilodalton glycolipoprotein antigen activates the mitogen-activated protein kinase pathway and release of proinflammatory cytokines through toll-like receptors 2 and 4 in human monocytes. Infect Immun. 2006;74(5):2686–2696.
113. Kim K, Sohn H, Kim JS, et al. Mycobacterium tuberculosis Rv0652 stimulates production of tumour necrosis factor and monocytes chemoattractant protein-1 in macrophages through the Toll-like receptor 4 pathway. Immunology. 2012;136(2):231–240.
114. Li J, Fu L, Wang G, Subbian S, Qin C, Zhao A. Unmethylated CpG motif-containing genomic DNA fragment of Bacillus Calmette-Guerin promotes macrophage functions through TLR9-mediated activation of NF-κ B and MAPKs signaling pathways. Innate Immun. 2020;26(3):183–203.
115. Tokunaga T, Yamamoto T, Yamamoto S. How BCG led to the discovery of immunostimulatory DNA. Jpn J Infect Dis. 1999;52(1):1–11.
116. Gagliardi MC, Teloni R, Giannoni F, et al. Mycobacterium bovis Bacillus Calmette-Guérin infects DC-SIGN–dendritic cell and causes the inhibition of IL-12 and the enhancement of IL-10 production. J Leukoc Biol. 2005;78(1):106–113.
117. Kaufmann SH. Tuberculosis Vaccines: Time to Think About the Next Generation. Elsevier; 2013:172–181.
118. Li J, Zhan L, Qin C. The double-sided effects of Mycobacterium Bovis bacillus Calmette–Guérin vaccine. NPJ Vaccines. 2021;6(1):1–11.
119. Bollampalli VP, Harumi Yamashiro L, Feng X, et al. BCG skin infection triggers IL-1R-MyD88-dependent migration of EpCAMlow CD11bhigh skin dendritic cells to draining lymph node during CD4+ T-cell priming. PLoS Pathog. 2015;11(10):e1005206.
120. Su H, Peng B, Zhang Z, Liu Z, Zhang Z. The Mycobacterium tuberculosis glycoprotein Rv1016c protein inhibits dendritic cell maturation, and impairs Th1/Th17 responses during mycobacteria infection. Mol Immunol. 2019;109:58–70.
121. Bertholet S, Ireton GC, Kahn M, et al. Identification of human T cell antigens for the development of vaccines against Mycobacterium tuberculosis. J Immunol. 2008;181(11):7948–7957.
122. Rossouw M, Nel HJ, Cooke GS, van Helden PD, Hoal EG. Association between tuberculosis and a polymorphic NFκB binding site in the interferon γ gene. Lancet. 2003;361(9372):1871–1872.
123. Hanekom WA. The immune response to BCG vaccination of newborns. Ann N Y Acad Sci. 2005;1062(1):69–78.
124. Soares AP, Kwong Chung CK, Choice T, et al. Longitudinal changes in CD4+ T-cell memory responses induced by BCG vaccination of newborns. J Infect Dis. 2013;207(7):1084–1094.
125. Dahanayake MH, Jayasundera AC. Nano-based drug delivery optimization for tuberculosis treatment: a review. J Microbiol Methods. 2021;181:106127.
126. Dahanayake MH, Jayasundera AC. Nano-based drug delivery optimization for tuberculosis treatment: a review. J Microbiol Methods. 2020;181:106127.
127. Pham -D-D, Fattal E, Tsapis N. Pulmonary drug delivery systems for tuberculosis treatment. Int J Pharm. 2015;478(2):517–529.
128. Ruman U, Fakurazi S, Masarudin MJ, Hussein MZ. Nanocarrier-based therapeutics and theranostics drug delivery systems for next generation of liver cancer nanodrug modalities. Int J Nanomedicine. 2020;15:1437.
129. Pulivendala G, Bale S, Godugu C. Inhalation of sustained release microparticles for the targeted treatment of respiratory diseases. Drug Deliv Transl Res. 2020;10(2):339–353.
130. Dhand C, Prabhakaran MP, Beuerman RW, Lakshminarayanan R, Dwivedi N, Ramakrishna S. Role of size of drug delivery carriers for pulmonary and intravenous administration with emphasis on cancer therapeutics and lung-targeted drug delivery. RSC Adv. 2014;4(62):32673–32689.
131. Bhardwaj A, Mehta S, Yadav S, et al. Pulmonary delivery of antitubercular drugs using spray-dried lipid–polymer hybrid nanoparticles. Artif Cells, Nanomed Biotechnol. 2016;44(6):1544–1555.
132. Ahmed R, Aucamp M, Ebrahim N, Samsodien H. Supramolecular assembly of rifampicin and PEGylated PAMAM dendrimer as a novel conjugate for tuberculosis. J Drug Deliv Sci Technol. 2021;66:102773.
133. Roy I, Vij N. Nanodelivery in airway diseases: challenges and therapeutic applications. Nanomedicine. 2010;6(2):237–244.
134. Marianecci C, Di Marzio L, Rinaldi F, Carafa M, Alhaique F. Pulmonary delivery: innovative approaches and perspectives. J Biomater Nanobiotechnol. 2011;2(05):567.
135. Zarogoulidis P, Chatzaki E, Porpodis K, et al. Inhaled chemotherapy in lung cancer: future concept of nanomedicine. Int J Nanomedicine. 2012;7:1551.
136. Sanders N, Rudolph C, Braeckmans K, De Smedt SC, Demeester J. Extracellular barriers in respiratory gene therapy. Adv Drug Deliv Rev. 2009;61(2):115–127.
137. Krombach F, Münzing S, Allmeling A-M, Gerlach JT, Behr J, Dörger M. Cell size of alveolar macrophages: an interspecies comparison. Environ Health Perspect. 1997;105(suppl 5):1261–1263.
138. Ruge CA, Schaefer UF, Herrmann J, et al. The interplay of lung surfactant proteins and lipids assimilates the macrophage clearance of nanoparticles. PLoS One. 2012;7(7):e40775.
139. Dobrovolskaia MA, Aggarwal P, Hall JB, McNeil SE. Preclinical studies to understand nanoparticle interaction with the immune system and its potential effects on nanoparticle biodistribution. Mol Pharm. 2008;5(4):487–495.
140. Maeda H. The enhanced permeability and retention (EPR) effect in tumor vasculature: the key role of tumor-selective macromolecular drug targeting. Adv Enzyme Regul. 2001;41:189–207.
141. Soldati T, Schliwa M. Powering membrane traffic in endocytosis and recycling. Nat Rev Mol Cell Biol. 2006;7(12):897–908.
142. Torchilin VP. Recent approaches to intracellular delivery of drugs and DNA and organelle targeting. Annu Rev Biomed Eng. 2006;8:343–375.
143. Formoso P, Muzzalupo R, Tavano L, De Filpo G, Pasquale Nicoletta F. Nanotechnology for the environment and medicine. Mini Rev Med Chem. 2016;16(8):668–675.
144. Cabral H, Nishiyama N, Kataoka K. Supramolecular nanodevices: from design validation to theranostic nanomedicine. Acc Chem Res. 2011;44(10):999–1008.
145. Ahmed N, Fessi H, Elaissari A. Theranostic applications of nanoparticles in cancer. Drug Discov Today. 2012;17(17–18):928–934.
146. Funkhouser J. Reinventing pharma: the theranostic revolution. Curr Drug Discov. 2002;2:17–19.
147. Wyszogrodzka-Gaweł G, Dorożyński P, Giovagnoli S, et al. An inhalable theranostic system for local tuberculosis treatment containing an isoniazid loaded metal organic framework Fe-MIL-101-NH2—From Raw MOF to drug delivery system. Pharmaceutics. 2019;11(12):687.
148. Zhao J, Wu H, Zhao J, et al. 2D LDH-MoS 2 clay nanosheets: synthesis, catalase-mimic capacity, and imaging-guided tumor photo-therapy. J Nanobiotechnology. 2021;19(1):1–16.
149. Sargazi S, Hajinezhad MR, Rahdar A, et al. CoNi alloy nanoparticles for cancer theranostics: synthesis, physical characterization, in vitro and in vivo studies. Appl Physics A. 2021;127(10):1–12.
150. Guo Z, Xie W, Lu J, et al. Ferrous ions doped layered double hydroxide: smart 2D nanotheranostic platform with imaging-guided synergistic chemo/photothermal therapy for breast cancer. Biomaterials Sci. 2021;9(17):5928–5938.
151. Wu J, Williams GR, Zhu Y, et al. Ultrathin chalcogenide nanosheets for photoacoustic imaging-guided synergistic photothermal/gas therapy. Biomaterials. 2021;273:120807.
152. Choi G, Choy JH. Recent progress in layered double hydroxides as a cancer theranostic nanoplatform. Wiley Interdiscip Rev. 2021;13(2):e1679.
153. Alagarsamy KN, Mathan S, Yan W, et al. Carbon nanomaterials for cardiovascular theranostics: promises and challenges. Bioactive Material. 2021;6(8):2261–2280.
154. Lee S, Kim SY. Gold Nanorod/reduced graphene oxide composite nanocarriers for near-infrared-induced cancer therapy and photoacoustic imaging. ACS Applied Nano Material. 2021;4(11):11849–11860.
155. Fahmi MZ, Sholihah NF, Wibrianto A, Sakti SC, Firdaus F, Chang JY. Simple and fast design of folic acid-based carbon dots as theranostic agent and its drug release aspect. Mater Chem Phys. 2021;267:124596.
156. Shi J, Zhang H, Wang L, et al. PEI-derivatized fullerene drug delivery using folate as a homing device targeting to tumor. Biomaterials. 2013;34(1):251–261.
157. Tang C, Li H, Hong J, Chai X. Application of nanoparticles in the early diagnosis and treatment of tumors: current status and progress. Tradit Med Res. 2020;5(1):34–43.
158. Sumer B, Gao J. Theranostic nanomedicine for cancer; 2008.
159. Pandey N, Menon JU, Takahashi M, et al. Thermo-responsive fluorescent nanoparticles for multimodal imaging and treatment of cancers. Nanotheranostics. 2020;4(1):1.
160. Branca RT, Cleveland ZI, Fubara B, et al. Molecular MRI for sensitive and specific detection of lung metastases. Proc Natl Acad Sci. 2010;107(8):3693–3697.
161. Wang H, Zheng L, Peng C, Shen M, Shi X, Zhang G. Folic acid-modified dendrimer-entrapped gold nanoparticles as nanoprobes for targeted CT imaging of human lung adencarcinoma. Biomaterials. 2013;34(2):470–480.
162. Cho S, Hwang O, Lee I, et al. Chemiluminescent and antioxidant micelles as theranostic agents for hydrogen peroxide associated-inflammatory diseases. Adv Funct Mater. 2012;22(19):4038–4043.
163. Banyal S, Malik P, Tuli HS, Mukherjee TK. Advances in nanotechnology for diagnosis and treatment of tuberculosis. Curr Opin Pulm Med. 2013;19(3):289–297.
164. Lee C-N, Wang Y-M, Lai W-F, et al. Super-paramagnetic iron oxide nanoparticles for use in extrapulmonary tuberculosis diagnosis. Clin Microbiol Infect. 2012;18(6):E149–E157.
165. Chen Y, Chen H, Zhang S, et al. Structure-property relationships in manganese oxide-mesoporous silica nanoparticles used for T1-weighted MRI and simultaneous anti-cancer drug delivery. Biomaterials. 2012;33(7):2388–2398.
166. Zhou Y, Kong Y, Kundu S, Cirillo JD, Liang H. Antibacterial activities of gold and silver nanoparticles against Escherichia coli and bacillus Calmette-Guérin. J Nanobiotechnology. 2012;10(1):1–9.
167. Sani A, Cao C, Cui D. Toxicity of gold nanoparticles (AuNPs): a review. Biochem Biophys Rep. 2021;26:100991.
168. Huang H, Li J, Shi S, et al. Detection of interferon-gamma for latent tuberculosis diagnosis using an immunosensor based on CdS quantum dots coupled to magnetic beads as labels. Int J Electrochem Sci. 2015;10:2580–2593.
169. Qi L, Gao X. Emerging application of quantum dots for drug delivery and therapy. Expert Opin Drug Deliv. 2008;5(3):263–267.
170. Wu T, Tang M. Toxicity of quantum dots on respiratory system. Inhal Toxicol. 2014;26(2):128–139.
171. Mohanta D, Patnaik S, Sood S, Das N. Carbon nanotubes: evaluation of toxicity at biointerfaces. J Pharm Anal. 2019;9(5):293–300.
172. Indoria S, Singh V, Hsieh M-F. Recent advances in theranostic polymeric nanoparticles for cancer treatment: a review. Int J Pharm. 2020;582:119314.
173. Mansour HM, Rhee Y-S WX. Nanomedicine in pulmonary delivery. Int J Nanomedicine. 2009;4:299.
174. Kammona O, Kiparissides C. Recent advances in nanocarrier-based mucosal delivery of biomolecules. J Control Release. 2012;161(3):781–794.
175. Pandey R, Khuller G. Nanotechnology based drug delivery system (s) for the management of tuberculosis; 2006.
176. Gref R, Minamitake Y, Peracchia MT, Trubetskoy V, Torchilin V, Langer R. Biodegradable long-circulating polymeric nanospheres. Science. 1994;263(5153):1600–1603.
177. Zhang L, Pornpattananangkul D, Hu C-M, Huang C-M. Development of nanoparticles for antimicrobial drug delivery. Curr Med Chem. 2010;17(6):585–594.
178. Pramanik S, Mohanto S, Manne R, et al. Nanoparticle-based drug delivery system: the magic bullet for the treatment of chronic pulmonary diseases. Mol Pharm. 2021;18(10):3671–3718.
179. Rai M, Dos Santos CA. Nanotechnology Applied to Pharmaceutical Technology. Springer; 2017.
180. Kobayashi S, Müllen K. Encyclopedia of Polymeric Nanomaterials. Springer Berlin Heidelberg; 2015.
181. Bekraki AI. Liposomes-and niosomes-based drug delivery systems for tuberculosis treatment. In: Nanotechnology Based Approaches for Tuberculosis Treatment. Elsevier; 2020:107–122.
182. Yusefi M, Chan H-Y, Teow S-Y, et al. 5-fluorouracil encapsulated chitosan-cellulose fiber bionanocomposites: synthesis, characterization and in vitro analysis towards colorectal cancer cells. Nanomaterials. 2021;11(7):1691.
183. Ahmad A, Ahmad I, Khan A, Abdullah M, Chee CY, Verpoort F. Introduction to nanomedicine an overview. Nanomed Manufactu Appli. 2021;1–20. doi:10.1016/B978-0-12-820773-4.00001-9
184. Debnath SK, Srivastava R. Drug delivery with carbon-based nanomaterials as versatile nanocarriers: progress and prospects. Front Nanotechnol. 2021;3:15.
185. Souto EB. Patenting Nanomedicines: Legal Aspects, Intellectual Property and Grant Opportunities. Springer Science & Business Media; 2012.
186. Vijayaraj Kumar P, Agashe H, Dutta T, Jain NK. PEGylated dendritic architecture for development of a prolonged drug delivery system for an antitubercular drug. Curr Drug Deliv. 2007;4(1):11–19.
187. Frijlink H, De Boer A. Dry powder inhalers for pulmonary drug delivery. Expert Opin Drug Deliv. 2004;1(1):67–86.
188. Machelart A, Salzano G, Li X, et al. Intrinsic antibacterial activity of nanoparticles made of β-cyclodextrins potentiates their effect as drug nanocarriers against tuberculosis. ACS Nano. 2019;13(4):3992–4007.
189. Rahimpour Y, Hamishehkar H, Nokhodchi A. Lipidic Micro-and Nano-Carriers for pulmonary drug delivery–a state-of-the-art review. Pulm Drug Deliv. 2015;123–142. doi:10.1002/9781118799536.ch6
190. Jafari A, Mosavari N, Movahedzadeh F, et al. Bactericidal impact of Ag, ZnO and mixed AgZnO colloidal nanoparticles on H37Rv Mycobacterium tuberculosis phagocytized by THP-1 cell lines. Microb Pathog. 2017;110:335–344.
191. Ivask A, ElBadawy A, Kaweeteerawat C, et al. Toxicity mechanisms in Escherichia coli vary for silver nanoparticles and differ from ionic silver. ACS Nano. 2014;8(1):374–386.
192. Jafari A, Kharazi S, Mosavari N, et al. Synthesis of mixed metal oxides nano-colloidal particles and investigation of the cytotoxicity effects on the human pulmonary cell lines: a prospective approach in anti-tuberculosis inhaled nanoparticles. Orient J Chem. 2017;33(3):1529.
193. Martínez-Carmona M, Gun’Ko Y, Vallet-Regí M. ZnO nanostructures for drug delivery and theranostic applications. Nanomaterials. 2018;8(4):268.
194. Saifullah B, Chrzastek A, Maitra A, et al. Novel anti-tuberculosis nanodelivery formulation of ethambutol with graphene oxide. Molecules. 2017;22(10):1560.
195. Rawal T, Patel S, Butani S. Chitosan nanoparticles as a promising approach for pulmonary delivery of bedaquiline. Eur J Pharm Sci. 2018;124:273–287.
196. Prabhu P, Fernandes T, Chaubey P, et al. Mannose-conjugated chitosan nanoparticles for delivery of rifampicin to osteoarticular tuberculosis. Drug Deliv Transl Res. 2021;11(4):1509–1519.
197. Öztürk AA, Yenilmez E, Özarda MG. Clarithromycin-loaded poly (lactic-co-glycolic acid)(PLGA) nanoparticles for oral administration: effect of polymer molecular weight and surface modification with chitosan on formulation, nanoparticle characterization and antibacterial effects. Polymers. 2019;11(10):1632.
198. Nemati E, Mokhtarzadeh A, Panahi-Azar V, et al. Ethambutol-loaded solid lipid nanoparticles as dry powder inhalable formulation for tuberculosis therapy. AAPS PharmSciTech. 2019;20(3):1–9.
199. Ali HR, Ali MR, Wu Y, et al. Gold nanorods as drug delivery vehicles for rifampicin greatly improve the efficacy of combating Mycobacterium tuberculosis with good biocompatibility with the host cells. Bioconjug Chem. 2016;27(10):2486–2492.
200. Varma JR, Kumar TS, Prasanthi B, Ratna JV. Formulation and characterization of pyrazinamide polymeric nanoparticles for pulmonary tuberculosis: efficiency for alveolar macrophage targeting. Indian J Pharm Sci. 2015;77(3):258.
201. Zaru M, Mourtas S, Klepetsanis P, Fadda AM, Antimisiaris SG. Liposomes for drug delivery to the lungs by nebulization. Eur J Pharm Biopharm. 2007;67(3):655–666.
202. Vishwa B, Moin A, Gowda D, et al. Pulmonary Targeting of inhalable moxifloxacin microspheres for effective management of tuberculosis. Pharmaceutics. 2021;13(1):79.
203. Xia X, Pethe K, Kim R, et al. Encapsulation of anti-tuberculosis drugs within mesoporous silica and intracellular antibacterial activities. Nanomaterials. 2014;4(3):813–826.
204. Zomorodbakhsh S, Abbasian Y, Naghinejad M, Sheikhpour M. The effects study of isoniazid conjugated multi-wall carbon nanotubes nanofluid on Mycobacterium tuberculosis. Int J Nanomedicine. 2020;15:5901.
205. El-Ridy MS, Yehia SA, Kassem MA, Mostafa DM, Nasr EA, Asfour MH. Niosomal encapsulation of ethambutol hydrochloride for increasing its efficacy and safety. Drug Deliv. 2015;22(1):21–36.
206. Ahmed RM. Development of Rifampicin Loaded in Surface-Modified 4.0 G PAMAM Dendrimer as a Novel Antituberculosis Pulmonary Drug Delivery System. Elsevier; 2020.
207. Garcia-Contreras L, Sung JC, Muttil P, et al. Dry powder PA-824 aerosols for treatment of tuberculosis in guinea pigs. Antimicrob Agents Chemother. 2010;54(4):1436–1442.
208. Basha RY, Doble M. Dual delivery of tuberculosis drugs via cyclodextrin conjugated curdlan nanoparticles to infected macrophages. Carbohydr Polym. 2019;218:53–62.
209. Henostroza MAB, Melo KJC, Yukuyama MN, Löbenberg R, Bou-Chacra NA. Cationic rifampicin nanoemulsion for the treatment of ocular tuberculosis. Colloids Surfaces A. 2020;597:124755.
210. Peters K, Leitzke S, Diederichs J, et al. Preparation of a clofazimine nanosuspension for intravenous use and evaluation of its therapeutic efficacy in murine Mycobacterium avium infection. J Antimicrob Chemother. 2000;45(1):77–83.
211. Goyal S, Klassert TE, Slevogt H. C-type lectin receptors in tuberculosis: what we know. Med Microbiol Immunol. 2016;205(6):513–535.
212. Ragas A, Roussel L, Puzo G, Riviere M. The Mycobacterium tuberculosis cell-surface glycoprotein apa as a potential adhesin to colonize target cells via the innate immune system pulmonary C-type lectin surfactant protein A. J Biol Chem. 2007;282(8):5133–5142.
213. Minnikin DE. Complex lipids, their chemistry biosynthesis and roles. Bio Mycobacteria. 1982;1:95–184.
214. Lemmer Y, Kalombo L, Pietersen R-D, et al. Mycolic acids, a promising mycobacterial ligand for targeting of nanoencapsulated drugs in tuberculosis. J Control Release. 2015;211:94–104.
215. Vieira AC, Chaves LL, Pinheiro M, et al. Mannosylated solid lipid nanoparticles for the selective delivery of rifampicin to macrophages. Artif Cells, Nanomed Biotechnol. 2018;46(sup1):653–663.
216. Mukhtar M, Csaba N, Robla S, et al. Dry powder comprised of isoniazid-loaded nanoparticles of hyaluronic acid in conjugation with mannose-anchored chitosan for macrophage-targeted pulmonary administration in tuberculosis. Pharmaceutics. 2022;14(8):1543.
217. Bhardwaj A, Kumar L, Narang R, Murthy R. Development and characterization of ligand-appended liposomes for multiple drug therapy for pulmonary tuberculosis. Artif Cells Nanomed Biotechnol. 2013;41(1):52–59.
218. Goyal AK, Garg T, Rath G, Gupta UD, Gupta P. Development and characterization of nanoembedded microparticles for pulmonary delivery of antitubercular drugs against experimental tuberculosis. Mol Pharm. 2015;12(11):3839–3850.
219. Grenha A, Alves AD, Guerreiro F, et al. Inhalable locust bean gum microparticles co-associating isoniazid and rifabutin: therapeutic assessment in a murine model of tuberculosis infection. Eur J Pharm Biopharm. 2020;147:38–44.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.