Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Innovative Applications and Challenges of Artificial Intelligence in the Whole-Course Management of Chronic Obstructive Pulmonary Disease
Authors Chen S ![]() , Xing S, Zhang G, Qiu F
, Xing S, Zhang G, Qiu F
Received 19 September 2025
Accepted for publication 18 December 2025
Published 7 January 2026 Volume 2026:21 568919
DOI https://doi.org/10.2147/COPD.S568919
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Shanji Chen,1– 3,* Shisi Xing,1,3,* Guanghui Zhang,1,4 Fei Qiu1,3
1Department of Engineering Research Center, The First Affiliated Hospital of Hunan University of Medicine, Huaihua, Hunan, People’s Republic of China; 2Faculty of Public Health, Mahasarakham University, Kham Riang, Mahasarakham, Thailand; 3Department of Medical Technology, Hunan Primary Digital Engineering Technology Research Center for Medical Prevention and Treatment, Huaihua, Hunan, People’s Republic of China; 4The First Affiliated Hospital, Hunan University of Medicine, Huaihua, Hunan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shanji Chen, Department of Engineering Research Center, The First Affiliated Hospital of Hunan University of Medicine, Huaihua, Hunan, 418000, People’s Republic of China, Tel +86 15274921139, Email [email protected] Fei Qiu, Department of Engineering Research Center, The First Affiliated Hospital of Hunan University of Medicine, Huaihua, Hunan, 418000, People’s Republic of China, Tel +86 13607411442, Email [email protected]
Objective: To systematically map how artificial intelligence (AI) can transform whole-course chronic obstructive pulmonary disease (COPD) management across prevention, diagnosis, treatment and rehabilitation within a 4P (Predictive, Preventive, Personalized, Participatory) medicine framework, and to identify actionable strategies for overcoming current barriers.
Methods: A systematic search of PubMed, Web of Science and Embase was performed for articles published between January 2021 and June 2025. This review was conducted following the PRISMA guidelines. Forty empirical studies and reviews that applied AI/ML to COPD prevention, early detection, personalised therapy, exacerbation prediction or pulmonary rehabilitation were critically appraised. Data were extracted on technical foundations, data modalities, algorithms, validation metrics and implementation outcomes.
Results: AI models integrating multimodal data (imaging, wearables, environmental exposures, genomics) achieved AUC ≥ 0.80 for predicting acute exacerbations up to seven days in advance, were associated with a reduction in emergency visits of up to 98% and a lowering of readmission rates by 25– 48%. Screening tools using chest X-ray, CT or smartphone sensors attained ≥ 90% accuracy for early COPD detection in primary-care settings. Personalised treatment optimisation was linked to a 53% lowering of exacerbation risk in best-responding subgroups. Home-based AI rehabilitation platforms increased adherence by > 30% without additional equipment. Key implementation challenges include data heterogeneity, limited explainability, digital divide among older adults and unclear regulatory frameworks.
Conclusion: AI is poised to operationalise 4P COPD care, delivering substantial clinical and economic benefits. Future success depends on cross-centre data standards, explainable-AI toolchains, federated learning and inclusive reimbursement policies.
Keywords: chronic obstructive pulmonary disease, artificial intelligence, machine learning, exacerbation prediction, precision medicine, pulmonary rehabilitation
Introduction
Disease Burden and Management Challenges of COPD
Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disorder characterized by persistent airflow limitation. Its high global prevalence, disability, and mortality render COPD a major public health challenge.1 It currently ranks as the fourth leading cause of death worldwide, surpassed only by ischaemic heart disease, stroke, and cancer. The most recent Global Burden of Disease Study 2021 estimates that COPD caused 3.72 million deaths and 798 million disability-adjusted life-years (DALYs) in a single year, while global incident cases reached 16.9 million.2,3 These figures underscore an ongoing upward trajectory that is projected to continue beyond 2030.4 The disease predominantly affects middle-aged and older adults and is strongly associated with long-term tobacco smoking, ambient and household air pollution, and occupational exposures. Patients typically present with chronic cough, sputum production, and progressive dyspnoea, symptoms that markedly impair quality of life and predispose to acute exacerbations, cor pulmonale, and respiratory failure.5
Despite continual refinements in COPD management strategies, several persistent challenges hinder optimal clinical care. First, early diagnosis remains elusive, largely because of the limited availability and underutilisation of spirometry.6 Second, acute exacerbations are difficult to predict accurately, precipitating recurrent hospitalisations, heightened mortality risk, and escalating healthcare costs.7 Third, therapeutic regimens are insufficiently individualised, resulting in marked inter-patient variability in treatment response and suboptimal outcomes for many. Fourth, long-term adherence to pharmacological and non-pharmacological therapies is poor, undermined by adverse effects, financial constraints, and limited patient knowledge.8 Finally, pulmonary rehabilitation resources are unevenly distributed, many regions lack specialised facilities and trained personnel, restricting patients’ access to effective rehabilitative interventions.9 Collectively, these barriers—delayed diagnosis, imprecise exacerbation prediction, absence of precision medicine approaches, poor adherence, and inequitable access to rehabilitation—underscore the urgent need for more efficient, accurate, accessible, and patient-centred management tools to improve both prognosis and quality of life for individuals living with COPD.
Opportunities in the Intelligent Era: Convergence of Artificial Intelligence and Digital Health
The rapid advancement of technology has ushered in an “intelligent era” characterized by the integration of the Internet of Things (IoT), wearable devices, cloud computing, and big data,10 bringing profound transformations to the healthcare sector. In the management of chronic obstructive pulmonary disease (COPD), digital health technologies (DHTs) demonstrate significant potential:11 remote monitoring systems enable real-time collection of physiological data to facilitate early intervention; mobile applications provide personalized education to enhance self-management skills and treatment adherence; and the aggregation of multi-source data lays the foundation for precision medicine.12 However, these technologies also introduce challenges such as massive data volume and high heterogeneity,13 which are difficult to handle effectively using conventional methods. Artificial intelligence (AI), particularly machine learning (ML) and deep learning (DL), has emerged as a key solution,14 capable of integrating multimodal data, uncovering latent patterns, quantifying disease risks, and supporting clinical decision-making—for instance, predicting COPD exacerbations and generating personalized management recommendations.15
The impact of AI in COPD care extends beyond data processing and risk prediction. As shown in Figure 1, it is catalyzing a paradigm shift toward the 4P medicine framework—predictive, preventive, personalized, and participatory Predictively, AI synthesizes multidimensional patient profiles to anticipate disease progression and imminent exacerbations,16 Preventively, AI-driven analytics generate individualized risk-mitigation strategies. Personalization is achieved through AI-guided tailoring of therapeutic regimens to each patient’s unique phenotypic and genotypic signature. Finally, participatory engagement is facilitated by mobile platforms that empower patients to co-manage their disease, thereby improving adherence and quality of life.17 In sum, the synergy between AI and DHTs redefines COPD management across the entire care continuum, offering a viable path to operationalize 4P medicine and ultimately improving both prognosis and patient-centered outcomes.
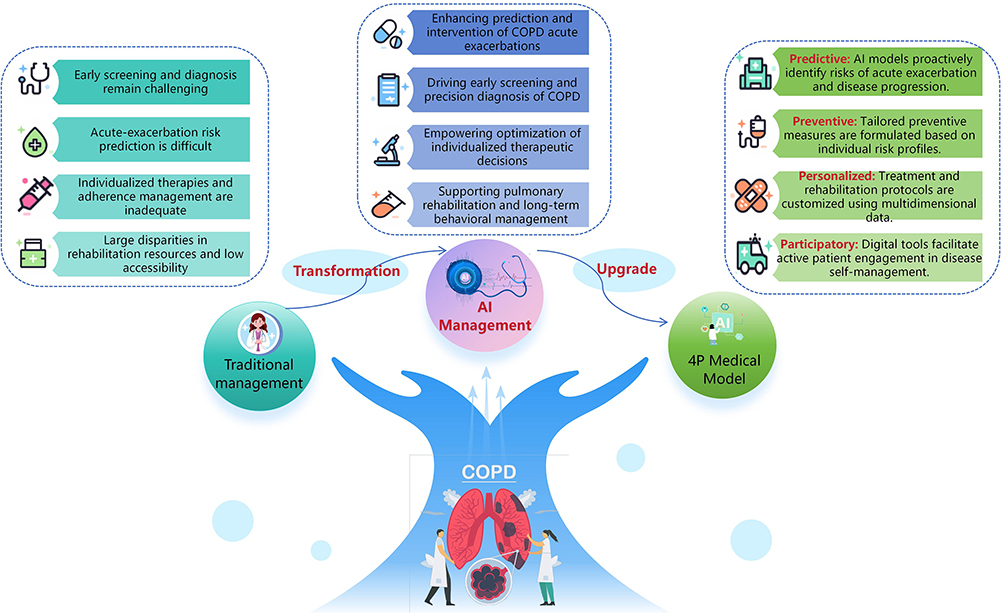 |
Figure 1 AI-Driven 4P Framework for Transforming COPD Management from Traditional Care to Precision Medicine. This figure illustrates the paradigm shift from reactive care to a proactive, AI-powered model. It maps specific AI solutions to key challenges in chronic obstructive pulmonary disease (COPD) management, operationalizing the 4P (Predictive, Preventive, Personalized, Participatory) medicine framework. |
Research Gaps and Objectives of This Review
Despite growing research on AI in COPD management, existing reviews remain fragmented, often focusing on narrow applications—such as imaging or exacerbation prediction—without providing a holistic view of whole-course care or adequately examining the technical foundations, data workflows, and real-world implementation barriers. This fragmentation limits their practical value for clinicians, researchers, and policymakers seeking to implement AI solutions. Furthermore, critical dimensions such as algorithmic fairness, data sovereignty, and the evolving regulatory landscape for AI in healthcare are often overlooked, yet are pivotal for building trust and ensuring equitable implementation.
To address these gaps, this review systematically analyzes AI applications across all stages of COPD whole-course care—prevention, diagnosis, treatment, and rehabilitation—by examining technical foundations, data processes, and practical implementation. Specifically, our objectives are to: (1) map the current landscape of AI technologies and multimodal data sources used throughout the COPD care continuum; (2) synthesize empirical evidence on the efficacy and performance of these AI applications; (3) critically examine the technical, ethical, and societal challenges impeding real-world deployment; and (4) propose a structured framework and actionable future directions for developing and implementing trustworthy AI systems in COPD management. Through this integrated approach, the study seeks to establish a structured framework for AI-enabled COPD management and offer evidence-based guidance for both research and practice. (The key findings of this review are shown in Figure 2).
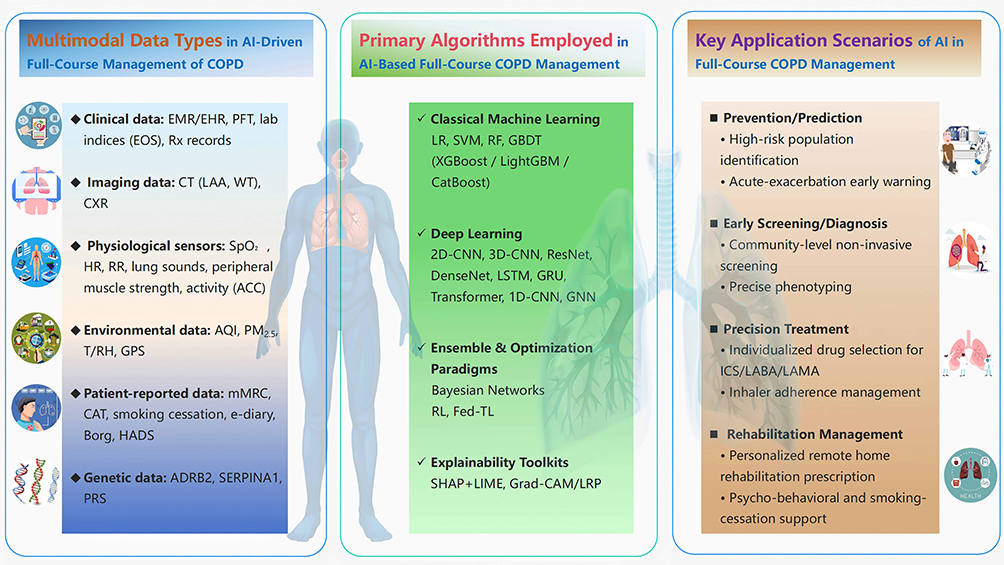 |
Figure 2 Key Findings of this Review: AI-Enabled End-to-End Chronic Obstructive Pulmonary Disease Management. This figure outlines the core ecosystem for AI in COPD care, integrating multimodal data (eg, EHR, PFT, CT, CXR, SpO2), a hierarchy of AI algorithms (from LR/SVM/RF to CNN/LSTM/Transformer and XAI tools like SHAP/LIME), and their translation into clinical applications across prevention, diagnosis, treatment, and rehabilitation. |
This review distinguishes itself by integrating the evidence into a cohesive 4P medicine framework and providing a critical analysis of implementation pathways, thereby offering a novel and structured roadmap that is not available in the existing, more narrowly focused literature.
Overview of the Article Structure
This review is structured as follows: Chapter 2 describes the research methodology, including literature search strategy, inclusion and exclusion criteria, data extraction, and quality assessment. Chapter 3 comprehensively examines AI applications across the core stages of COPD management—prevention, diagnosis, treatment, and rehabilitation—and delves into the supporting technical principles and data-flow mechanisms through multidimensional analysis. Chapter 4 systematically addresses challenges in AI implementation, including technical, social, and ethical issues, and proposes corresponding mitigation strategies. Chapter 5 provides a comprehensive discussion of AI applications in COPD care, summarizing advantages, limitations, and offering policy and practice recommendations. Finally, Chapter 6 concludes by summarizing key findings and suggesting directions for future research and implementation.
Methods
Literature Search Strategy
A systematic search was conducted across three electronic databases—PubMed, Web of Science Core Collection, and Embase—to identify relevant articles published between January 2021 and June 2025. The search strategy was designed around core concepts: “chronic obstructive pulmonary disease” (COPD), “artificial intelligence” (AI)/ “machine learning” (ML), and key management areas (eg, prevention, diagnosis, treatment, rehabilitation). A Boolean approach combining controlled vocabulary (eg, MeSH, Emtree) and free-text keywords was employed. Manual screening of reference lists supplemented the electronic search to ensure comprehensive and current coverage. This timeframe was selected to include the most recent advances in AI applications for whole-course COPD management.
Study Selection and Eligibility Criteria
All identified records were imported into EndNote for duplicate removal, and the subsequent study selection followed the PRISMA 2020 guidelines, as detailed in the flow diagram (Figure 3).
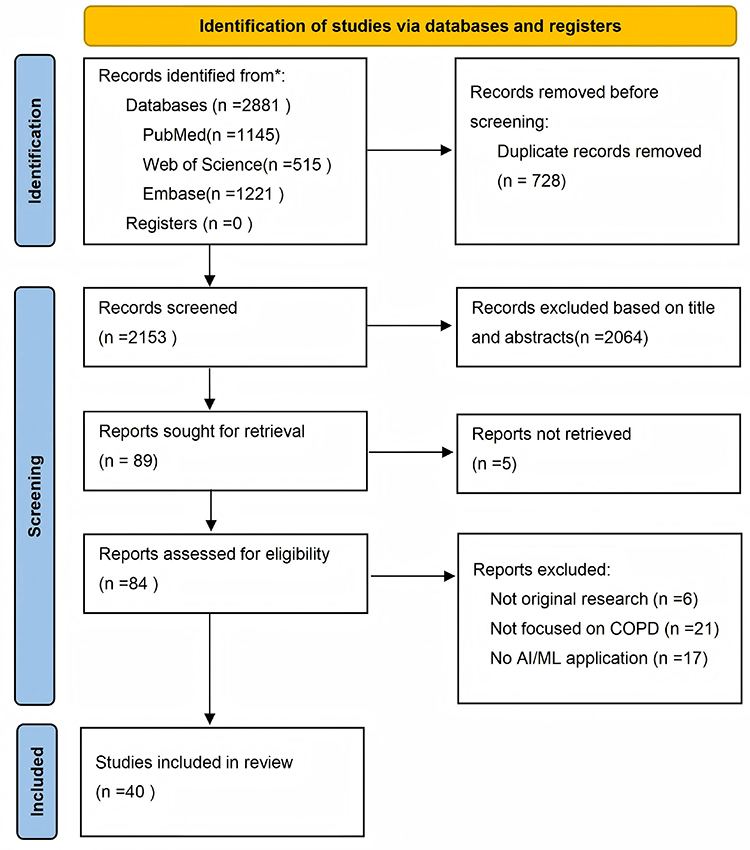 |
Figure 3 PRISMA Flowchart of Studies Through the Selection Process. |
Studies were included if they: (1) applied AI/ML methodologies to any stage of COPD management; (2) were original research or substantive reviews; and (3) were published in English within the specified timeframe. Studies were excluded if they were: (1) conference abstracts, editorials, or letters without detailed methods; (2) not focused on COPD; (3) lacking a core AI/ML component; or (4) unavailable in full text.
Data Extraction and Quality Assessment
Key data from included studies were extracted, including study design, data sources, AI algorithms, key outcomes, and performance metrics.
A formal quality and risk of bias appraisal was performed to assess the robustness of the evidence. Studies were evaluated across domains such as study design, sample size, data quality, and validation methods. Each study was assigned an overall quality rating (High, Moderate, or Low), which is summarized in the “Risk of Bias / Study Quality” column of Tables 1–4.
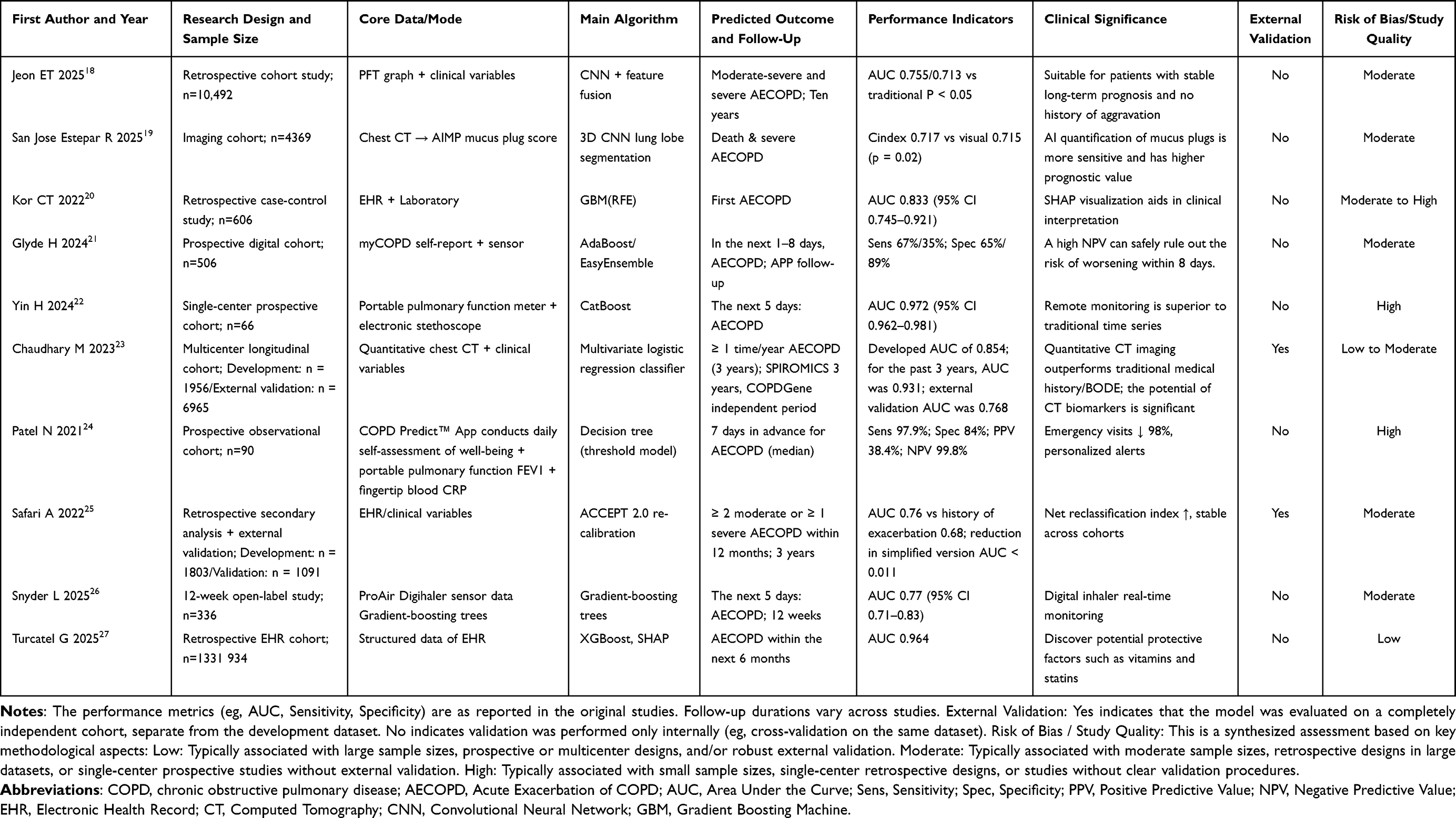 |
Table 1 Snapshot of Key Empirical Studies on Clinical Applications of AI-Driven Prediction and Intervention for COPD Exacerbations |
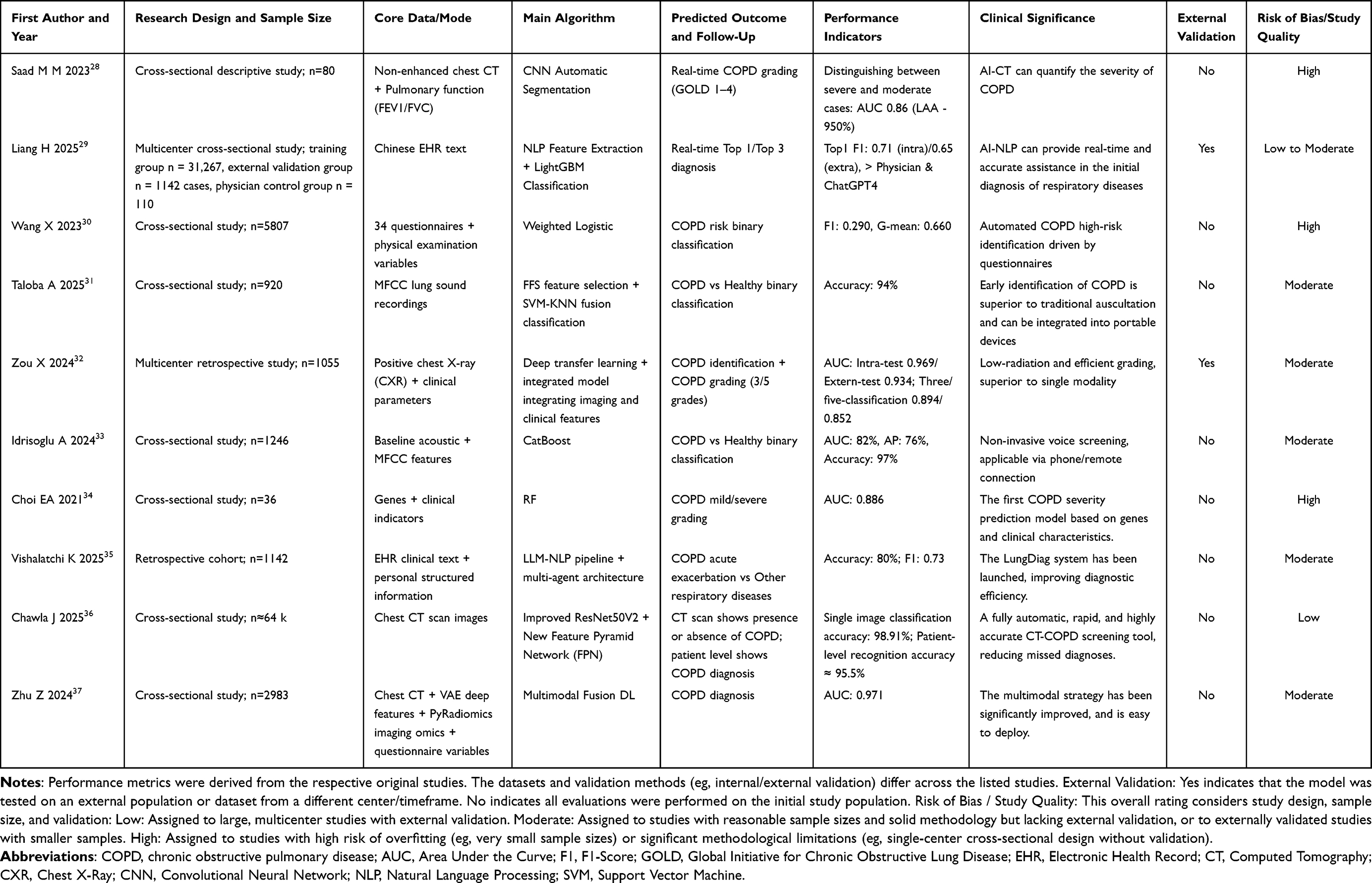 |
Table 2 Snapshot of Clinical Empirical Evidence on AI-Driven Early Screening and Precision Diagnosis of COPD |
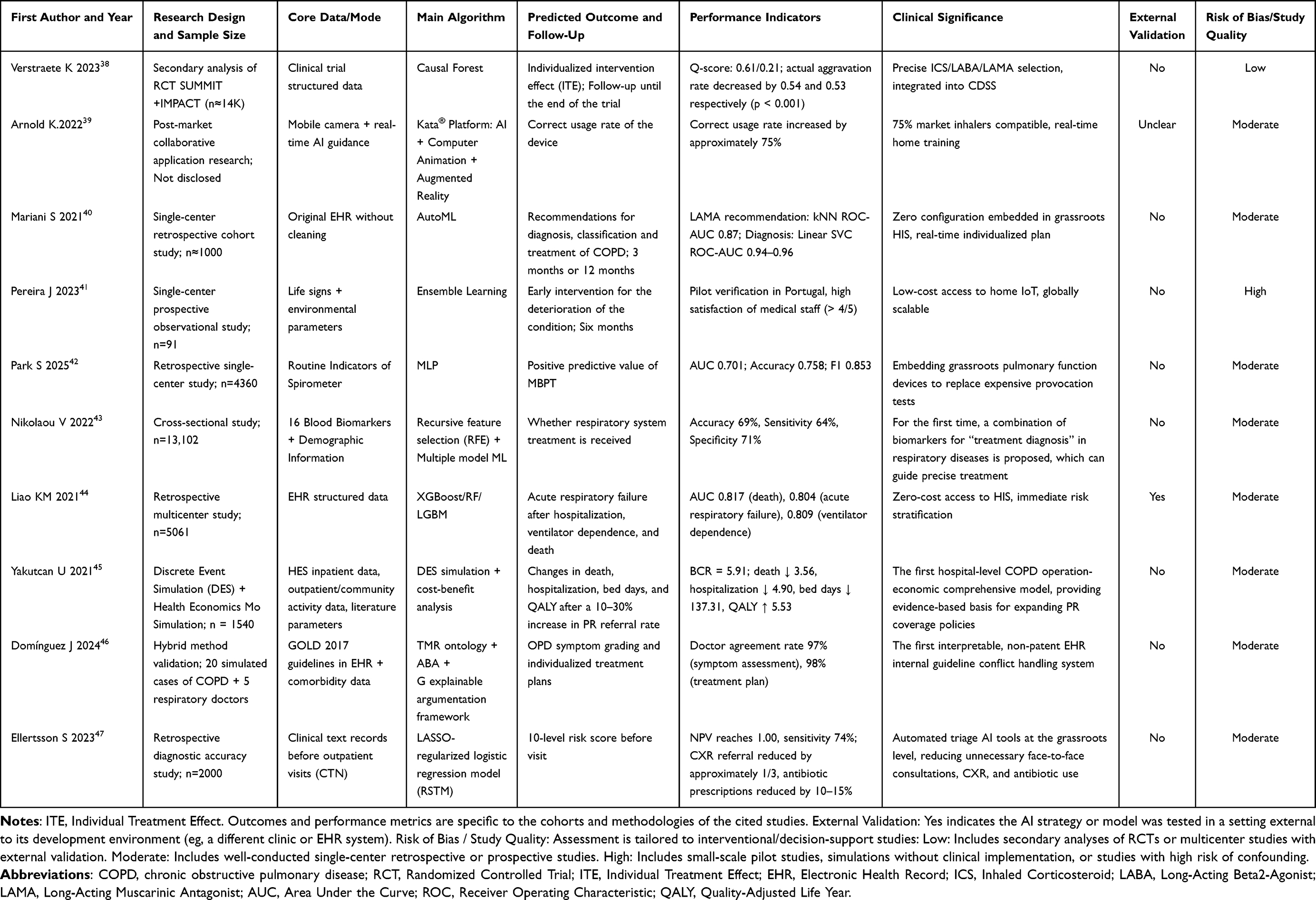 |
Table 3 Snapshot of Key Empirical Studies on AI-Empowered Optimization of Personalized Treatment Decisions in COPD |
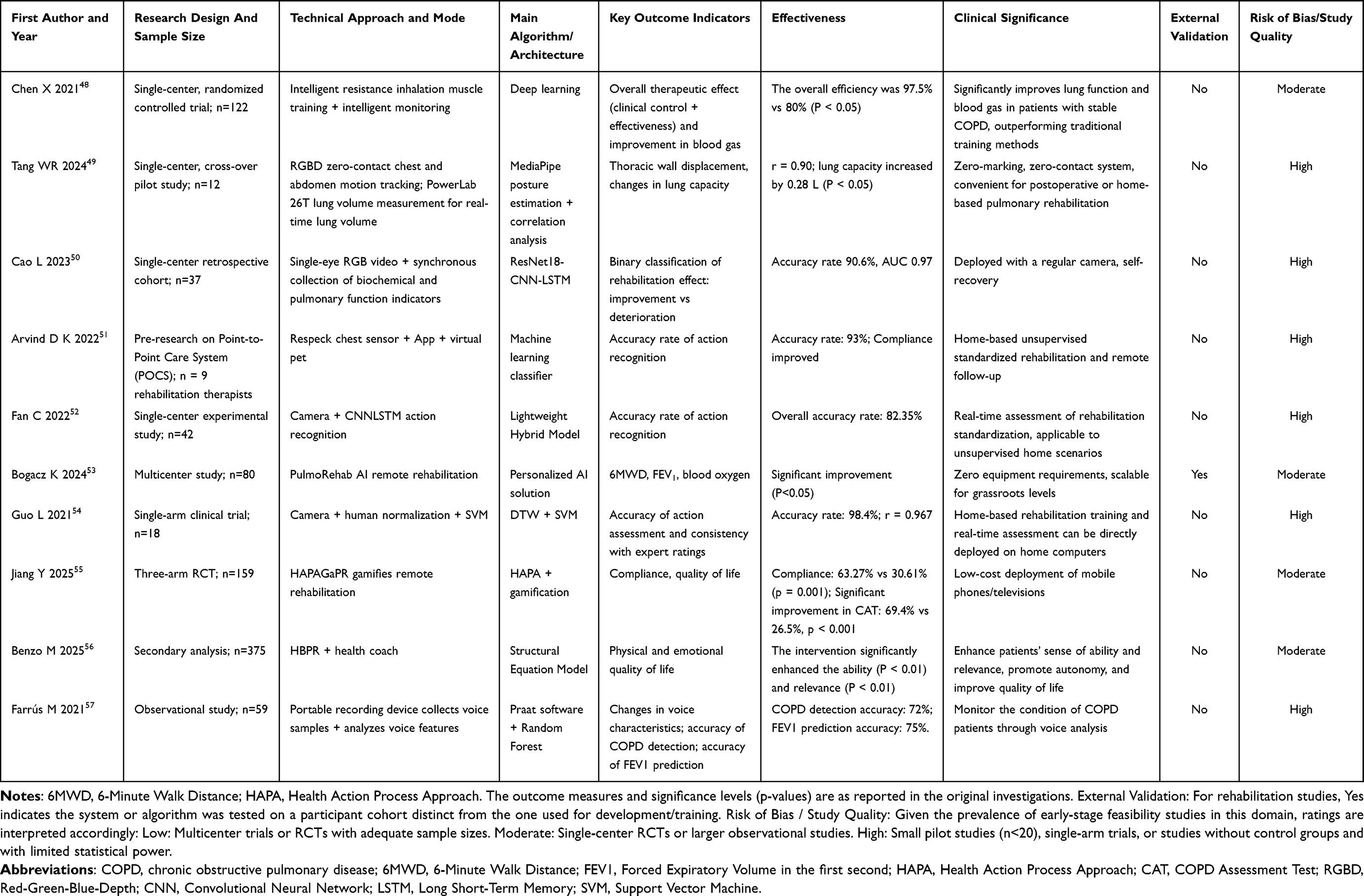 |
Table 4 Snapshot of Key Empirical Studies on AI-Supported Pulmonary Rehabilitation and Long-Term Behavioural Management in COPD |
Data Synthesis
Given the heterogeneity in AI applications and outcomes, a narrative synthesis was conducted. Findings were structured thematically according to the COPD care continuum to provide an integrated overview of AI technologies, their clinical applications, and implementation challenges.
AI in Whole-Course COPD Management: Technical Foundations, Data-Flow Governance, and Current Applications
AI Prediction and Intervention for Acute Exacerbation of COPD
Technical Foundations and Data Flows
Acute exacerbations of COPD accelerate lung function decline and increase mortality, making early prediction and intervention essential.58 AI models integrate multimodal dynamic data to enable risk stratification, early warning, and personalized decision support. Core data sources include: (i) mobile app-recorded symptom diaries; (ii) wearable-monitored physiological parameters (eg, SpO2, heart rate, respiratory rate);59 (iii) accelerometer-based activity data;60 (iv) environmental exposure metrics (eg, air quality via API); and (v) historical clinical records from EHRs (eg, prior exacerbations, medication history).61
Advancements in Clinical Evidence
A growing body of evidence supports the effectiveness of artificial intelligence in predicting and preemptively managing acute exacerbations of COPD. By leveraging diverse data sources—including imaging, wearable sensors, and electronic health records—coupled with machine and deep learning approaches, AI enables high predictive accuracy and meaningful clinical integration, significantly reducing hospitalizations through early intervention. Key studies demonstrate robust outcomes: Jeon et al18 developed the AIPFTClin model, combining pulmonary function images and clinical variables to achieve AUCs of 0.755 and 0.713 for moderate-to-severe and severe exacerbations, sustaining performance over 10 years. Patel et al24 implemented a decision-tree algorithm in the COPDPredict™ app, enabling 7-day advance predictions with 97.9% sensitivity and 84.0% specificity, and reducing ED visits by 98%. Chaudhary et al23 used CT biomarkers to develop a model with an AUC of 0.854, outperforming both exacerbation history and the BODE index.
These studies, along with other significant contributions—including advances in mucus-plug detection,19 interpretable machine learning,20 mobile health integration,21 and multimodal data fusion22,25–27—are comprehensively summarized in Table 1.
AI-Driven Early Screening and Precision Diagnosis of COPD
Technical Foundations and Data Flows
Artificial intelligence is transforming early screening and diagnostic pathways for COPD by enhancing detection rates in community settings, improving diagnostic accuracy, and enabling precise phenotyping—key enablers of personalized therapy.62 While traditional screening reliant on pulmonary-function tests (PFTs) faces challenges in primary care, AI-powered tools such as portable devices and mobile applications facilitate an integrated “screening–differentiation–phenotyping” workflow, significantly boosting clinical efficiency.
Multimodal data fusion underpins these advances, incorporating: time-series FEV1/FVC curves from portable spirometers; quantitative emphysema indices and airway-wall thickness from low-dose CT; cough-sound features captured via smartphones;63 electronic patient-reported outcomes (eg, mMRC/CAT);64 and physiological trends (eg, SpO2, heart rate) from wearables.65 Integration of these heterogeneous data streams allows AI models to effectively discriminate COPD from asthma, heart failure, and other diseases with symptomatic overlap.
Advancements in Clinical Evidence
The integration of artificial intelligence into COPD screening and diagnosis is advancing through diversified technical approaches and strengthened real-world clinical validation. Innovations leveraging imaging, acoustics, and electronic health records facilitate earlier detection and improved disease stratification beyond conventional pulmonary function tests. Notably, Liang et al29 developed the LungDiag system using multi-center EHRs, elevating the top-1 diagnostic F1-score from 0.44 by human experts to 0.651 in 1142 real-world cases. Zhu et al37 proposed a multimodal model combining CT-based deep learning, radiomics, and questionnaires, achieving an AUC of 0.971 in 2983 scans and outperforming single-modality methods. Additionally, Chawla et al36 introduced an enhanced ResNet50V2-based system trained on ~64,000 CT scans, which attained 98.91% accuracy and correctly identified 234 out of 245 cases, demonstrating high sensitivity even for small lesions.
Additional influential studies—including those utilizing voice biomarkers,33 chest X-ray imaging,32 lung sound analysis,31 and EHR-based natural language processing35—are comprehensively summarized in Table 2. Together, these works provide a broad overview of innovative algorithmic strategies, validation outcomes, and clinical relevance, reflecting the diverse and rapidly evolving landscape of AI applications in COPD diagnosis.
Personalized Treatment Decision Optimization Enabled by AI
Technical Foundations and Data Flows
Artificial intelligence is advancing COPD treatment into a precision medicine framework, enabling individualized pharmacological selection, prediction of therapeutic response, improved inhaler adherence, and support for interventional therapies such as bronchoscopic lung volume reduction.66 By moving beyond traditional trial-and-error approaches, AI integrates multidimensional dynamic data to build evidence-based decision systems that are already demonstrating potential to redefine treatment pathways.
The underlying data architecture incorporates six key information types: clinical phenotypes and biomarkers (eg, blood eosinophil counts); genetic polymorphisms (eg, ADRB2 receptor genotypes);67 historical medication responses; home-monitored pulmonary function trends (eg, weekly FEV1 variability);68 CT-derived quantitative imaging features (airway-wall thickness, emphysema index); and patient-reported outcomes (PROs)69 Together, these elements form a comprehensive computational foundation for predicting treatment efficacy and guiding personalized care plans.
Advancements in Clinical Evidence
Recent real-world evidence confirms AI’s expanding role in guiding individualized COPD management. By integrating heterogeneous data streams with advanced algorithms, these systems now enable real-time therapeutic tailoring, improve medication adherence, and streamline clinical decision-making across diverse care settings. Verstraete et al38 trained a machine-learning model on SUMMIT and IMPACT data to forecast treatment response, isolating a subgroup whose exacerbation rates fell by >53% when guided by lung-function and eosinophil biomarkers. VisionHealth and Boehringer Ingelheim39 introduced the class IIaKata® app, whose AI-driven smartphone camera feedback corrects inhaler errors for ~75% of marketed devices, offering low-cost, home-based optimisation. Meanwhile, Mariani et al40 deployed an end-to-end AutoML pipeline on Dutch primary-care EHRs, simultaneously differentiating asthma from COPD, predicting key clinical indices, and recommending personalised interventions while integrating seamlessly into existing health-information systems.
Additional significant contributions—including remote intelligent decision-support systems,41 spirometry-based predictive models,42 biomarker discovery for treatment stratification,43 adverse-outcome prediction tools,44 cost-effectiveness simulation models,45 explainable clinical decision support systems,46 and AI-assisted triage platforms47—are comprehensively summarized in Table 3. These innovations collectively represent the expanding landscape of AI-driven solutions for personalized COPD management, offering improved treatment precision, enhanced resource utilization, and greater accessibility to specialized care. Through these advancements, AI is transforming COPD treatment from a traditional trial-and-error approach to a data-driven, personalized paradigm that optimizes therapeutic outcomes while maximizing healthcare efficiency. The integration of these technologies into clinical workflows promises to revolutionize patient care while addressing the growing challenges of chronic disease management in diverse healthcare settings.
AI-Powered Pulmonary Rehabilitation and Long-Term Behavioral Management
Technical Foundations and Data Flows
Artificial intelligence is transforming pulmonary rehabilitation and long-term behavioral management in COPD by overcoming the spatial and temporal limitations of traditional center-based programs. Through personalized rehabilitation planning, remote exercise supervision, and behavioral interventions, AI—supported by wearable devices and mobile health technologies—shifts care from episodic clinical interactions to continuous, home-based management, significantly enhancing patients’ quality of life and long-term outcomes.4,70
The foundation of AI-driven management lies in the integration of multisource dynamic data. Smartphones and wearable sensors continuously capture six key metrics: (1) activity capacity (eg, 6-minute walk distance via accelerometer/GPS);71 (2) exercise intensity (heart rate variability, energy expenditure); (3) muscle function (isokinetic strength from smart devices);72 (4) real-time symptom reporting (digital mMRC scores); (5) smoking cessation patterns (withdrawal symptoms and adherence); and (6) psychological state (digitized HADS scores).73 These continuous, objective data streams provide the empirical basis for precision interventions.
Advancements in Clinical Evidence
Artificial intelligence is rapidly transforming pulmonary rehabilitation and long-term behavioural management for COPD by enabling continuous, home-based care through remote sensors, computer vision, and mobile platforms. These systems overcome traditional barriers of access and adherence by delivering personalised feedback and digital therapeutics in real time. Chen et al48 deployed a deep-learning monitoring tool that achieved 97.5% accuracy in primary-care COPD management; combined with standardised therapy, it outperformed conventional care (80% accuracy) across lung function, blood gases, and symptom scores (p < 0.05). Jiang et al55 tested a 12-week gamified HAPA-based remote programme in 159 patients, surpassing both usual remote rehabilitation and HAPA-only controls in adherence, quality of life, and psychological outcomes, with benefits persisting to 24 weeks. Tang et al49 introduced a zero-contact RealSense/MediaPipe thoraco-abdominal tracker that strongly correlated chest-wall motion with spirometric volume (r = 0.90); real-time visual feedback increased chest excursion by 3 mm and lung volume by 0.28 L (p < 0.05), underscoring its suitability for unsupervised home rehabilitation.
Additional innovative approaches—including Respeck wearable sensors51 camera-based exercise recognition systems,52,54 multicentre tele-rehabilitation platforms,53 health coaching interventions,56 and speech biomarker analysis57—are comprehensively summarized in Table 4. These studies collectively illustrate the diverse and evolving landscape of AI-enabled pulmonary rehabilitation, highlighting trends toward non-contact monitoring, gamified engagement, and scalable home-based solutions.
Challenges and Countermeasures of AI in the Whole Process Management of COPD
Technical Challenges Faced
At present, the technical challenges confronting AI in whole-course COPD management mainly include: a) Data heterogeneity and lack of standardisation: physiological signals such as breath sounds, SpO2, and HRV lack unified standards in acquisition devices, sampling frequency, and ambient-noise control, leading to cross-centre model-transfer difficulties and a 5–15% AUC drop in new settings; CT images differ in slice thickness, reconstruction algorithms, and dose, causing radiomic-feature drift that necessitates recalibration.58 b) Small samples and data imbalance: acute exacerbations constitute only 5–10% of follow-up data, yielding models with high sensitivity but low specificity or requiring resampling that amplifies noise; low penetration of smart devices in older adults (23%) further shrinks training-set size.74 c) Insufficient algorithmic explainability: deep models cannot provide clinically intelligible decision rationales when predicting exacerbations, reducing physician acceptance d) Compute-power and deployment bottlenecks: resource disparities between hospital PACS and wearable terminals mean that even compressed models may introduce 300–500 ms latency, hampering real-time alerting.75
Ethical and Social Challenges Faced
Ethical and social challenges for AI in whole-course COPD management chiefly encompass: a) Informed consent and data sovereignty: continuous physiological monitoring generates massive personal data; patients lack clear understanding of secondary use and cross-border transfer, risking trust crises.76 b) Algorithmic bias and fairness: training sets predominantly comprise urban tertiary-hospital patients, under-representing rural and low-education groups, potentially skewing recommendations. c) Accountability: when AI alerts contradict clinicians’ judgement and lead to missed diagnoses, no unified legal framework assigns liability among algorithm developers, hospitals, or physicians.77 d) Technology access: poor digital perfusion in older adults impairs wearable SpO2 accuracy; 47% struggle to operate smart apps, widening the digital divide.74
Strategies for Overcoming Challenges
As shown in Figure 4, based on the research results, we have proposed a solution framework to address the obstacles and ethical challenges of trusted artificial intelligence technology in the management of chronic obstructive pulmonary disease.
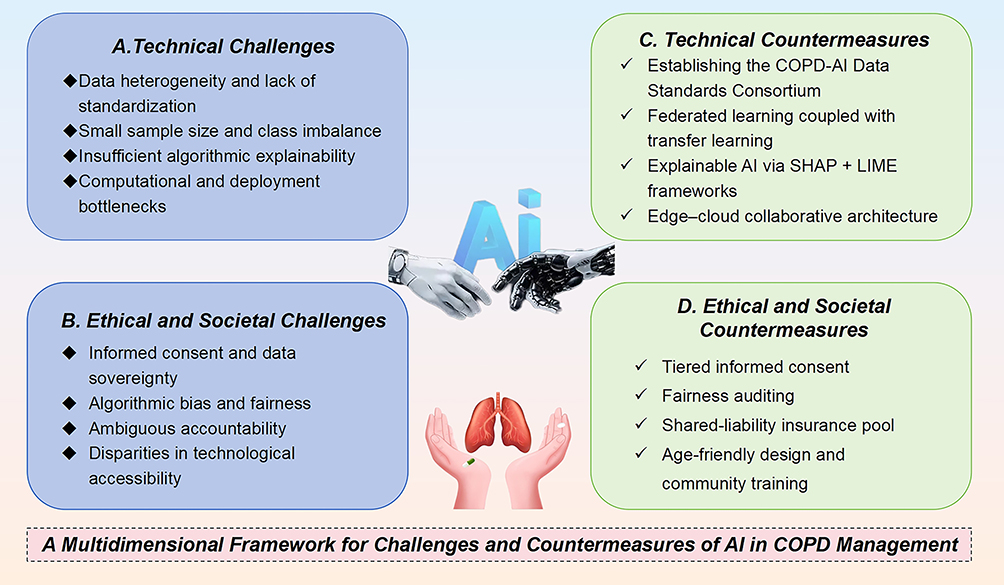 |
Figure 4 Toward Trustworthy AI in COPD Care: A Framework for Technical and Ethical Hurdles. This figure presents a multidimensional framework pairing major implementation barriers with targeted solutions. Technical challenges (eg, data heterogeneity) are addressed by countermeasures like federated learning (FL) and explainable AI (XAI). Ethical challenges (eg, algorithmic bias) are met with strategies such as fairness auditing and tiered consent, guiding the development of reliable and equitable AI systems. |
Technical Dimension
Technical mitigation strategies include: a) Establish the COPDAI Data Standards Consortium: formulate minimum information checklists (MIADECOPD) for breath sounds, CT, and questionnaires, releasing open format-conversion scripts b) Federated learning + transfer learning: jointly train on multi-centre heterogeneous data under privacy protection, then fine-tune with small local datasets to address small-sample and domain-shift issues.78 c) Explainable-AI toolchains: embed SHAP + LIME dual-interpretation frameworks in exacerbation-prediction models, outputting “key vital-sign contribution heat maps” for clinical verification. d) Edge–cloud co-architecture: lightweight CNNs extract features on wearables, deep analysis occurs in the cloud, balancing real-time performance and accuracy.79
Ethical and Social Dimension
Ethical and social mitigation strategies include: a) Tiered informed consent: three-layer consent forms for basic monitoring, secondary research use, and commercial purposes, all supporting withdrawal at any time. b) Fairness audits: every six months evaluate model sensitivity across age, sex, and education groups with an independent test set; retraining is triggered if disparity >10%.80 c) Shared-liability insurance: hospitals, technology firms, and reinsurers jointly fund an “AI medical-liability pool”, sharing compensation proportional to participation. d) Age-friendly design: voice interaction plus one-touch call functions reduce complexity; community AI-experience corners provide free training.74
Discussion
Advantages and Limitations of AI in COPD Management
Artificial intelligence demonstrates significant potential across the COPD care continuum, with core advantages in three areas: (1) Prediction and early intervention: AI models (eg, XGBoost, LSTM) leveraging multisource data—wearable sensors, environmental APIs, and EHRs—improve exacerbation prediction (AUC >0.8), enabling 5–7-day early warnings and reducing readmissions by 25–48%.18,24 Multi-omic models (eg, CatBoost) identify high-risk populations with 10-year prediction AUC of 0.81. (2) Diagnostic efficiency and personalization: AI-assisted tools (eg, CNN-based CT or spirometry analysis) achieve >90% accuracy, lowering misdiagnosis by 15–30%.28,32,37 Treatment optimization via reinforcement learning and GNNs tailors therapies and reduces exacerbation risk by 53%.38 (3) Resource optimization and access: AI-powered remote monitoring (eg, myCOPD) boosts rehabilitation adherence by >30% and cuts ED visits by 98%.21,39,49
Nevertheless, AI applications face notable limitations: (1) Limited generalizability: Model performance drops in cross-center validation (eg, radiomics AUC decrease of 0.08–0.12); data imbalance reduces specificity; 58,74,78 (2) Clinical integration challenges: Black-box decisions erode trust; heterogeneous data and hardware constraints hinder real-time use.75 (3) Socio-ethical issues: Digital literacy gaps (47% among elderly), algorithmic bias, and data sovereignty concerns may worsen disparities.74
While the reported performance of AI models is promising, it is crucial to contextualize these findings within the limitations of the underlying evidence. As summarized in Tables 1–4, the included studies varied considerably in design and quality. Many were retrospective in nature and conducted in single centers, and a significant proportion lacked external validation, which may inflate performance estimates and limit generalizability. Furthermore, the predominance of observational studies introduces potential for confounding bias.
Future Research Directions
To overcome current limitations, future research should focus on: (1) Multimodal fusion and dynamic modelling: integrate multi-temporal data (breath sounds, air-pollution exposure, medication logs) to build a “digital-twin patient” platform that simulates long-term effects of intervention strategies (eg, QALY gains and hospitalisation costs).44,45 (2) Explainable AI and causal reasoning: develop dual SHAP+LIME frameworks to enhance transparency (eg, “key-vital-sign heat maps” for exacerbation prediction) and combine reinforcement learning to generate auditable, individualised treatment pathways. (3) Cross-domain generalisation: advance federated learning for privacy-preserving multi-centre collaboration and apply transfer learning to address data-distribution shifts, improving model robustness in grassroots settings.78 (4) Health-economics validation: design multi-centre RCTs to quantify the cost-effectiveness of AI-enabled whole-course management (eg, QALYs, direct medical costs) to provide evidence for reimbursement policy.5,45
Policy and Practice Recommendations
Scaling AI adoption in COPD management requires multi-stakeholder synergy: (1) Regulatory innovation: develop “Key Review Points for COPD AI Software”, specifying data-quality controls (eg, MIADECOPD standards), external validation, and dynamic-update cycles. (2) Payment reform: include “AI-assisted whole-course COPD management” in DRG add-on payments, incentivising healthcare institutions with 300–500 RMB per patient per year.5,45 (3) Grassroots empowerment: establish “COPD AI Shared Hubs” within county medical communities to centrally procure compute and model services, lowering deployment costs;74 develop age-friendly interfaces (voice interaction + one-touch call) and community AI-training corners to improve digital literacy. (4) Ethical governance: conduct biannual algorithmic-fairness audits (sensitivity disparities <10%) and create a tripartite “hospital–enterprise–insurance” shared-liability mechanism.77,80
Artificial intelligence is moving COPD care from “experience” to “data”. Gains in prediction, efficiency, and personalisation are clear, yet generalisability, explainability, and equity still limit bedside use. Embedding multimodal fusion, explainable AI, and federated learning within adaptive regulation and payment models is required to build a “prediction–prevention–personalisation” ecosystem that delivers precise, affordable COPD management worldwide.
Conclusions
This review systematically evaluates the transformative role of artificial intelligence (AI) across the full spectrum of COPD management. By synthesizing evidence from 40 studies, we demonstrate that AI models leveraging multimodal data within advanced computational frameworks can achieve AUCs >0.8 for tasks such as exacerbation prediction and personalized therapy, correlating with substantial reductions in hospital readmissions (25–48%) and emergency visits (up to 98%). These advancements significantly advance the 4P (Predictive, Preventive, Personalized, Participatory) medicine paradigm for COPD.
However, the promising results reported herein must be interpreted with caution. The effect sizes are primarily derived from specific, often research-oriented settings, and their generalizability to broader, more diverse populations requires further validation. Moreover, the clinical adoption of these technologies faces significant headwinds, including data heterogeneity, limited model explainability, the digital divide among elderly patients, and unresolved ethical concerns regarding data sovereignty and algorithmic bias. This review itself is subject to limitations, such as the heterogeneity of the included studies and potential publication bias, which future work with prospective registration and formal meta-analysis could address.
Ultimately, the translation of AI from research to routine practice is not automatic. It is conditional upon a concerted, multi-stakeholder effort. Future work must prioritize the development of cross-institutional data alliances, explainable AI systems, and robust digital twin platforms. Concurrently, policy support is indispensable, encompassing reimbursement reforms for AI-enabled care, the establishment of shared-computing infrastructures, and the promotion of age-friendly interfaces. Only by simultaneously addressing these technical, validation, and socio-ethical dimensions can we realize the full potential of AI to enable equitable and effective global access to precision COPD care.
Abbreviations
AI, Artificial Intelligence; AUC, Area Under the Receiver Operating Characteristic Curve; CNN, Convolutional Neural Network; DL, Deep Learning; EHR, Electronic Health Record; EMR, Electronic Medical Record; GBM, Gradient Boosting Machine; GNN, Graph Neural Network; LIME, Local Interpretable Model-agnostic Explanations; LSTM, Long Short-Term Memory; ML, Machine Learning; NLP, Natural Language Processing; RF, Random Forest; RL, Reinforcement Learning; SHAP, SHapley Additive exPlanations; SVM, Support Vector Machine; XAI, Explainable Artificial Intelligence; 6MWD, 6-Minute Walk Distance; ACC, Accelerometer; BMI, Body Mass Index; Borg, Borg Scale; CAT, COPD Assessment Test; EOS, Eosinophils; FEV1, Forced Expiratory Volume in the first second; FVC, Forced Vital Capacity; HR, Heart Rate; HADS, Hospital Anxiety and Depression Scale; mMRC, modified Medical Research Council Dyspnea Scale; PRO, Patient-Reported Outcome; RR, Respiratory Rate; SpO2, Peripheral Oxygen Saturation; AECOPD, Acute Exacerbation of Chronic Obstructive Pulmonary Disease; CDSS, Clinical Decision Support System; COPD, Chronic Obstructive Pulmonary Disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; PFT, Pulmonary Function Test; CT, Computed Tomography; CXR, Chest X-Ray; LAA, Low-Attenuation Area; WT, Wall Thickness; DRG, Diagnosis-Related Group; HAPA, Health Action Process Approach; HBPR, Home-Based Pulmonary Rehabilitation; ICS, Inhaled Corticosteroid; LABA, Long-Acting Beta2-Agonist; LAMA, Long-Acting Muscarinic Antagonist; PR, Pulmonary Rehabilitation; QALY, Quality-Adjusted Life Year; RPM, Remote Patient Monitoring; FL, Federated Learning; GPS, Global Positioning System; IoMT, Internet of Medical Things; PHR, Personal Health Record.
Data Sharing Statement
All data used in this review are available via the databases PubMed, Web of Science and Embase, subject to the requisite subscription or access permissions. No original datasets were generated or analysed in the course of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that financial support was received for the research and/or publication of this article. This work was supported by Hunan Primary Digital Engineering Technology Research Center for Medical Prevention and Treatment (no. 2023TP2170); Hunan Engineering Research Center of TCM Real-World Clinical Practice.
Disclosure
Shanji Chen and Shisi Xing are co-first authors for this study. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Han H, Hao L. Revealing lncRNA biomarkers related to chronic obstructive pulmonary disease based on bioinformatics. Int J Chronic Obstr. 2022;Volume 17:2487–18. doi:10.2147/COPD.S354634
2. Hu S, Chen H, Wang J, et al. Global, regional, and national burden of COPD among women from 1990 to 2021 and projections to 2050: a systematic analysis for the global burden of disease study 2021. Ann Global Health. 2025;91(1):73. doi:10.5334/aogh.4883
3. Wu Z, Zhang X, Zhang P, et al. The burden and risk factors of chronic obstructive pulmonary disease (COPD) in Asia and its countries from 1990 to 2021: a systematic analysis based on the 2021 global burden of disease study. Front Med. 2025;12:1641719. doi:10.3389/fmed.2025.1641719
4. Chen Z, Hao J, Sun H, et al. Applications of digital health technologies and artificial intelligence algorithms in COPD: systematic review. BMC Med Inf Decis Making. 2025;25(1):77. doi:10.1186/s12911-025-02870-7
5. Welte T, Vogelmeier C, Papi A. COPD: early diagnosis and treatment to slow disease progression. Int J Clin Pract. 2015;69(3):336–349. doi:10.1111/ijcp.12522
6. Zhou J, Li X, Wang X, et al. Accuracy of portable spirometers in the diagnosis of chronic obstructive pulmonary disease A meta-analysis. Npj Prim Care Respiratory Med. 2022;32(1):15. doi:10.1038/s41533-022-00275-x
7. Yamada H, Matsumoto I, Makita N, et al. Effect of timing of bronchodilator therapy initiation on exacerbations in patients with chronic obstructive pulmonary disease: a retrospective cohort study. Respir Res. 2022;23(1):255. doi:10.1186/s12931-022-02184-6
8. Zeng Y, Cai S, Chen Y, et al. Current status of the treatment of COPD in China: a multicenter prospective observational study. Int J Chronic Obstr. 2020;Volume 15:3227–3237. doi:10.2147/COPD.S274024
9. Jiménez-Reguera BA, Maroto López E, Fitch S, et al. Development and preliminary evaluation of the effects of an mHealth web-based platform (HappyAir) on adherence to a maintenance program after pulmonary rehabilitation in patients with chronic obstructive pulmonary disease: randomized controlled trial. JMIR mHealth uHealth. 2020;8(7):e18465. doi:10.2196/18465
10. Yadav A, Gupta V, Sahu H, Shrimal S. Artificial intelligence-new era. Int J New Technol Res. 2017;3(3):263339.
11. Bosnic-Anticevich S, Bakerly ND, Chrystyn H, et al. Advancing digital solutions to overcome longstanding barriers in asthma and COPD management. Patient Preference Adherence. 2023;Volume 17:259–272. doi:10.2147/PPA.S385857
12. De Santis KK, Mergenthal L, Christianson L, et al. Digital technologies for health promotion and disease prevention in older people: scoping review. J Med Internet Res. 2023;25:e43542. doi:10.2196/43542
13. Adnan K, Akbar R, Khor SW, Ali AB. Role and challenges of unstructured big data in healthcare. In:
14. Ahmed Z, Mohamed K, Zeeshan S, et al. Artificial intelligence with multi-functional machine learning platform development for better healthcare and precision medicine. Database. 2020;2020:baaa010. doi:10.1093/database/baaa010
15. Kobrinskii B, Grigoriev OG, Molodchenkov AI, et al. Artificial intelligence technologies application for personal health management. IFAC-PapersOnLine. 2019;52(25):70–74. doi:10.1016/j.ifacol.2019.12.448
16. Fernandez-Granero MA, Sanchez-Morillo D, Leon-Jimenez A. An artificial intelligence approach to early predict symptom-based exacerbations of COPD. Biotechnol Biotechnol Equip. 2018;32(3):778–784. doi:10.1080/13102818.2018.1437568
17. Carlin C, Taylor A, van Loon I, et al. Role for artificial intelligence in respiratory diseases—Chronic obstructive pulmonary disease. J Hospital Manag Health Policy. 2021;5:27. doi:10.21037/jhmhp-20-119
18. Jeon E-T, Park H, Lee J-K, et al. Deep learning–based chronic obstructive pulmonary disease exacerbation prediction using flow-volume and volume-time curve imaging: retrospective cohort study. J Med Internet Res. 2025;27:e69785. doi:10.2196/69785
19. San Jose Estepar R, Nardelli P, San Jose Estepar R, et al. Comparing AI-detected versus visually detected airway mucus plugs in predicting mortality and exacerbations in COPD. Am J Respir Crit Care Med. 2025;211(Abstracts):A7380–A7380. doi:10.1164/ajrccm.2025.211.Abstracts.A7380
20. Kor C-T, Li Y-R, Lin P-R, et al. Explainable machine learning model for predicting first-time acute exacerbation in patients with chronic obstructive pulmonary disease. J Personalized Med. 2022;12(2):228. doi:10.3390/jpm12020228
21. Glyde HMM. Predictive modelling acute exacerbations of chronic obstructive pulmonary disease. University of Bristol; 2024.
22. Yin H, Wang K, Yang R, et al. A machine learning model for predicting acute exacerbation of in-home chronic obstructive pulmonary disease patients. Comput Methods Programs Biomed. 2024;246:108005. doi:10.1016/j.cmpb.2023.108005
23. Chaudhary MF, Hoffman EA, Guo J, et al. Predicting severe chronic obstructive pulmonary disease exacerbations using quantitative CT: a retrospective model development and external validation study. Lancet Digital Health. 2023;5(2):e83–e92. doi:10.1016/S2589-7500(22)00232-1
24. Patel N, Kinmond K, Jones P, et al. Validation of COPDPredictâ„¢: unique combination of remote monitoring and exacerbation prediction to support preventative management of COPD exacerbations. Int J Chronic Obstr. 2021;Volume 16:1887–1899. doi:10.2147/COPD.S309372
25. Safari A, Adibi A, Sin DD, et al. ACCEPT 2·0: recalibrating and externally validating the acute COPD exacerbation prediction tool (ACCEPT). EClinicalMedicine. 2022;51:101574. doi:10.1016/j.eclinm.2022.101574
26. Snyder LD, DePietro M, Reich M, et al. Predictive machine learning algorithm for COPD exacerbations using a digital inhaler with integrated sensors. BMJ Open Respiratory Res. 2025;12(1):e002577. doi:10.1136/bmjresp-2024-002577
27. Turcatel G, Xiao Y, Caveney S, et al. Predicting asthma exacerbations using machine learning models. Adv Ther. 2025;42(1):362–374. doi:10.1007/s12325-024-03053-y
28. Saad MM, Bayoumy AA, EL-Nisr MM, et al. Assessment of artificial intelligence-aided chest computed tomography in diagnosis of chronic obstructive airway disease: an observational study. Egypt J Radiol Nucl Med. 2023;54(1):97. doi:10.1186/s43055-023-01043-8
29. Liang H, Yang T, Liu Z, et al. LungDiag: empowering artificial intelligence for respiratory diseases diagnosis based on electronic health records, a multicenter study. MedComm. 2025;6(1):e70043. doi:10.1002/mco2.70043
30. Wang X, Ren H, Ren J, et al. Machine learning-enabled risk prediction of chronic obstructive pulmonary disease with unbalanced data. Comput Methods Programs Biomed. 2023;230:107340. doi:10.1016/j.cmpb.2023.107340
31. Taloba AI, Matoog R. Detecting respiratory diseases using machine learning-based pattern recognition on spirometry data. Alexandria Eng J. 2025;113:44–59. doi:10.1016/j.aej.2024.11.009
32. Zou X, Ren Y, Yang H, et al. Screening and staging of chronic obstructive pulmonary disease with deep learning based on chest X-ray images and clinical parameters. BMC Pulm Med. 2024;24(1):153. doi:10.1186/s12890-024-02945-7
33. Idrisoglu A, Dallora AL, Cheddad A, et al. COPDVD: automated classification of chronic obstructive pulmonary disease on a new collected and evaluated voice dataset. Artif Intell Med. 2024;156:102953. doi:10.1016/j.artmed.2024.102953
34. Choi E-A, Kim JW, Nah G, et al. Prediction of COPD severity based on clinical data using machine learning. In:
35. Vishalatchi K, Thenmoezhi N, Sivagurunathan PT, Udhayamoorthi M. AI-powered NLP systems for differential diagnosis: improving COPD exacerbation detection. In:
36. Chawla J, Walia N. Design of artificial intelligence based technique for classification chronic pulmonary disease from chest X-RAY. Multidisciplinary Sci J. 2025;7(1):2025021. doi:10.31893/multiscience.2025021
37. Zhu Z, Zhao S, Li J, et al. Development and application of a deep learning-based comprehensive early diagnostic model for chronic obstructive pulmonary disease. Respir Res. 2024;25(1):167. doi:10.1186/s12931-024-02793-3
38. Verstraete K, Gyselinck I, Huts H, et al. Estimating individual treatment effects on COPD exacerbations by causal machine learning on randomised controlled trials. thorax. 2023;78(10):983–989. doi:10.1136/thorax-2022-219382
39. Arnold K, Keller B. DGAP-news: visionHealth and boehringer ingelheim: digital therapy support for asthma and COPD.
40. Mariani S, Metting E, Lahr MMH, et al. Developing an ML pipeline for asthma and COPD: the case of a Dutch primary care service. Int J Intell Syst. 2021;36(11):6763–6790. doi:10.1002/int.22568
41. Pereira J, Antunes N, Rosa J, et al. Intelligent clinical decision support system for managing COPD patients. J Personalized Med. 2023;13(9):1359. doi:10.3390/jpm13091359
42. Park S, Yi Y, Han -S-S, et al. Development of an AI model for predicting methacholine bronchial provocation test results using spirometry. Diagnostics. 2025;15(4):449. doi:10.3390/diagnostics15040449
43. Nikolaou V, Massaro S, Fakhimi M, et al. Using machine learning to detect theranostic biomarkers predicting respiratory treatment response. Life. 2022;12(6):775. doi:10.3390/life12060775
44. Liao K-M, Liu C-F, Chen C-J, et al. Machine learning approaches for predicting acute respiratory failure, ventilator dependence, and mortality in chronic obstructive pulmonary disease. Diagnostics. 2021;11(12):2396. doi:10.3390/diagnostics11122396
45. Yakutcan U, Demir E, Hurst JR, et al. Operational modeling with health economics to support decision making for COPD patients. Health Services Res. 2021;56(6):1271–1280. doi:10.1111/1475-6773.13652
46. Domínguez JS, Prociuk D, Marović B, et al. ROAD2H: development and evaluation of an open†-source explainable artificial intelligence approach for managing co†-morbidity and clinical guidelines. Learn Health Syst. 2024;8(2):e10391. doi:10.1002/lrh2.10391
47. Ellertsson SR, Hlynsson HD, Loftsson H, et al. Triaging patients with artificial intelligence for respiratory symptoms in primary care to improve patient outcomes: a retrospective diagnostic accuracy study. Anna Family Med. 2023;21(3):240–248. doi:10.1370/afm.2970
48. Chen X, Yao Y, Teekaraman Y. Intelligent monitoring of care status for COPD patients based on deep learning. Contrast Media Mol Imag. 2021;2021(1):5690442. doi:10.1155/2021/5690442
49. Tang W-R, Su W, Lien JJ, Chang CC, Yen YT, Tseng YL. Development of a real-time RGB-D visual feedback-assisted pulmonary rehabilitation system. Heliyon. 2024;10(1).
50. Cao L, Xie Z, Liu T, et al. A deep learning framework-based exercise assessment for rehabilitation of chronic obstructive pulmonary disease. J Mech Med Biol. 2023;23(09):2340089. doi:10.1142/S0219519423400894
51. Arvind D, Georgescu T, Bao W, Bates CA. A virtual/digital pet point-of-care system for self-management of COPD patients. In:
52. Fan C, Lu B, Ren J, et al. An effective action recognition approach used in physical exercise for copd patients. J Mech Med Biol. 2022;22(09):2240051. doi:10.1142/S0219519422400516
53. Szczegielniak J. Assessment of rehabilitation effectiveness in patients with COPD as part of the project” PulmoRehab—Access to healthcare services through a personalized care system for patients with COPD, including remote monitoring and tele rehabilitation based on Artificial Intelligence methods.
54. Guo L, Zhang B, Yang Z, Wang X, Wang J. Motor function evaluation system based on machine vision for COPD patients. In:
55. Jiang Y, Sun M, Nuerdawulieti B, et al. Effectiveness of remote gamification pulmonary rehabilitation intervention based on the health action process approach theory in older adults with chronic obstructive pulmonary disease: a pilot randomized controlled trial. Front Med. 2025;12:1576256. doi:10.3389/fmed.2025.1576256
56. Benzo M, Lee M, Clark MM, et al. The basic science of behavior change in COPD: testing self-determination theory to support home-based rehabilitation with health coaching. J Cardiopulmonary Rehab Prevention. 2025;45(4):286–293. doi:10.1097/HCR.0000000000000957
57. Farrã°s M, Codina-Filbà J, Reixach E, et al. Speech-based support system to supervise chronic obstructive pulmonary disease patient status. Appl Sci. 2021;11(17):7999. doi:10.3390/app11177999
58. Wu Y, Xia S, Liang Z, et al. Artificial intelligence in COPD CT images: identification, staging, and quantitation. Respir Res. 2024;25(1):319. doi:10.1186/s12931-024-02913-z
59. Coutu F-A, Iorio OC, Ross BA. Remote patient monitoring strategies and wearable technology in chronic obstructive pulmonary disease. Front Med. 2023;10:1236598. doi:10.3389/fmed.2023.1236598
60. Yamane T, Yamasaki Y, Nakashima W, et al. Tri-axial accelerometer-based recognition of daily activities causing shortness of breath in COPD patients. Physical Activity Health. 2023;7(1):64–75. doi:10.5334/paah.224
61. Sivakumaran S, Alsallakh MA, Lyons RA, et al. Identifying COPD in routinely collected electronic health records: a systematic scoping review. ERJ Open Res. 2021;7(3):00167–2021. doi:10.1183/23120541.00167-2021
62. Yang X. Application and prospects of artificial intelligence technology in early screening of chronic obstructive pulmonary disease at primary healthcare institutions in China. Int J Chronic Obstr. 2024;Volume 19:1061–1067. doi:10.2147/COPD.S458935
63. Windmon A, Minakshi M, Chellappan S, Athilingam P, Johansson M, Jenkins BA. On detecting chronic obstructive pulmonary disease (COPD) cough using audio signals recorded from smart-phones. In:
64. Ekstrãm M, Lewthwaite H, Li PZ, et al. Identifying abnormal exertional breathlessness in COPD: comparing modified medical research council and COPD assessment test with cardiopulmonary exercise testing. Chest. 2025;167(3):697–711. doi:10.1016/j.chest.2024.10.027
65. Chan P, Ryan NP, Chen D, et al. Novel wearable and contactless heart rate, respiratory rate, and oxygen saturation monitoring devices: a systematic review and meta†analysis. Anaesthesia. 2022;77(11):1268–1280. doi:10.1111/anae.15834
66. Calzetta L, Pistocchini E, Chetta A, et al. Experimental drugs in clinical trials for COPD: artificial intelligence via machine learning approach to predict the successful advance from early-stage development to approval. Expert Opin Invest Drugs. 2023;32(6):525–536. doi:10.1080/13543784.2023.2230138
67. Hegab AE, Sakamoto T, Saitoh W, et al. Polymorphisms of IL4, IL13, and ADRB2 genes in COPD. Chest. 2004;126(6):1832–1839. doi:10.1378/chest.126.6.1832
68. Buyse GM, Rummey C, Meier T, et al. Home-based monitoring of pulmonary function in patients with duchenne muscular dystroph. J Neuromusc Dis. 2018;5(4):419–430. doi:10.3233/JND-180338
69. Jones P, Miravitlles M, van der Molen T, et al. Beyond FEV1 in COPD: a review of patient-reported outcomes and their measurement. Int J Chronic Obstr;2012:697–709. doi:10.2147/COPD.S32675
70. Davids J, Lidstrã¶mer N, Ashrafian H. Artificial intelligence for physiotherapy and rehabilitation. In: Artificial Intelligence in Medicine. Springer; 2022:1789–1807.
71. Ã Breasail MCL, Biswas B, Smith M, et al. Wearable GPS and accelerometer technologies for monitoring mobility and physical activity in neurodegenerative disorders: a systematic review. Sensors. 2021;21(24):8261. doi:10.3390/s21248261
72. De Fazio R, Mastronardi VM, De Vittorio M, et al. Wearable sensors and smart devices to monitor rehabilitation parameters and sports performance: an overview. Sensors. 2023;23(4):1856. doi:10.3390/s23041856
73. Hickey BA, Chalmers T, Newton P, et al. Smart devices and wearable technologies to detect and monitor mental health conditions and stress: a systematic review. Sensors. 2021;21(10):3461. doi:10.3390/s21103461
74. Pan Z, Li S, Chen Y. Research progress and prospects of internet of things technology in chronic obstructive pulmonary disease management. Chin General Pract. 2024;27(35):4446.
75. Shaw J, Rudzicz F, Jamieson T, et al. Artificial intelligence and the implementation challenge. J Med Internet Res. 2019;21(7):e13659. doi:10.2196/13659
76. Lee C, Britto S, Diwan K. Evaluating the impact of artificial intelligence (AI) on clinical documentation efficiency and accuracy across clinical settings: a scoping review. Cureus. 2024;16(11).
77. Bleher H, Braun M. Diffused responsibility: attributions of responsibility in the use of AI-driven clinical decision support systems. AI Ethics. 2022;2(4):747–761. doi:10.1007/s43681-022-00135-x
78. Chen X, Dong X, Chen Q, et al. Application of artificial intelligence in physiological measurement based screening and diagnosis of chronic obstructive pulmonary disease: a review. Expert Syst Appl. 2025;293:128694. doi:10.1016/j.eswa.2025.128694
79. Wang Y, Yang C, Lan S, et al. End-edge-cloud collaborative computing for deep learning: a comprehensive survey. IEEE Commun Surveys Tutorials. 2024;26(4):2647–2683. doi:10.1109/COMST.2024.3393230
80. Landers RN, Behrend TS. Auditing the AI auditors: a framework for evaluating fairness and bias in high stakes AI predictive models. Am Psychologist. 2023;78(1):36. doi:10.1037/amp0000972
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.