Back to Journals » Risk Management and Healthcare Policy » Volume 10
Injured workers’ perception of loss and gain in the return to work process
Authors Lai HS, Szeto GPY, Chan CCH
Received 10 August 2016
Accepted for publication 17 November 2016
Published 7 February 2017 Volume 2017:10 Pages 7—16
DOI https://doi.org/10.2147/RMHP.S119479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Frank Papatheofanis
Hon Sun Lai,1,2 Grace PY Szeto,1 Chetwyn CH Chan3
1Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, 2Total Rehabilitation Management (Hong Kong) Limited, 3Applied Cognitive Neuroscience Laboratory, Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, Hong Kong
Abstract: When a worker is injured at work, he has to face a tough decision-making process about when and how to return to work (RTW). This study tests how the prospect theory can be applied to influence the injured workers’ perceptions about this important choice. One hundred forty-one injured workers were presented with wage- and pain-related information in four different message framing (negatively or positively) and precision (smaller or larger number) conditions. After exposure to the specific combination of this wage and pain information, the participants were asked to express intentions to RTW in terms of perceived chance, confidence, and anticipated sick leave duration. When asked to predict their RTW outcome, 101 participants (72.3%) responded favorably, whereas only 40 (27.7%) indicated an expectation for staying on sick leave. The present results did not show significant differences in the participants’ responses to the positively and negatively framed information about wage and pain. However, it was noted that the control group that was presented with positive framing for both “wage” and “pain” information showed higher scores in expectation and confidence for RTW, whereas the Ambivalent Group that had both negative messages showed lower scores. Seventy-nine participants who had ≥60% perceived improvement in condition were selected for further analysis, and those who were presented with “wage loss” information rated significantly higher perceived chance of RTW than those in the “pain gain” group. More in-depth investigation is warranted on this topic, with a larger sample of injured workers to investigate the effects of message framing on the decision-making process about RTW.
Keywords: wages, injury, compensation, rehabilitation
Introduction
Decision making in return to work
In many countries, a delay in return to work (RTW) after a work injury has become a social problem that affects the injured workers, their family members, employers, and insurance companies.1,2 Traditionally, the management of and the research on RTW are based on a biomedical model that focuses on the recovery of impaired functions and the training of work capability. Recent research on occupational rehabilitation has shifted to an integrated, multidisciplinary, and biopsychosocial model that focuses on encompassing the individual personal factors of the worker and the workplace, as well as medical, economical, and social considerations.1–3
RTW involves a complex and dynamic process. Injured workers not only have to deal with physical disabilities but also have to overcome many psychological hurdles about their work abilities, chance of re-injury, and peer reactions.4 They also face issues in communicating with different stakeholders and service providers.1,5 As a result, injured workers are exposed to various sources of information about rehabilitation and work compensation. Eventually, injured workers must make decisions about RTW in order to re-integrate into the workforce.
RTW after injury can be regarded as an outcome that relates to the motivation and self-efficacy of workers.6 A worker’s motivation to RTW can be expressed as a function of expectations of recovery and the value placed on the work or employment, balanced by personal costs, such as pain.6–8 The potential gains and losses associated with RTW are important issues for consideration by the injured worker.9–11 It has been proposed that decisions about RTW involve personal considerations of motivation, expectation, confidence, and readiness for returning to work. Dersh et al12 conceptualized workers’ motivation about returning to work (or remaining off work) as a rivalry between secondary losses and gains following injuries. The losses would largely relate to the reduction of potential benefits, such as decreases in the sum of total compensation for early RTW. The gains are those concerning increases in potential benefits such as earning a full salary, maintaining job seniority after early RTW, or receiving disability benefits without having to work. From a different perspective, the losses could be lowering of comfort level or aggravation of symptoms, such as pain.
Prospect theory
Prospect theory was originally developed by two psychologists, Kahneman and Tversky13, as a behavioral economic theory. Over the past 30+ years, this theory has been widely applied to study how people evaluate risk in the field of finance and insurance.13–15 This theory stipulates that individuals will be more inclined to be “risk seeking” when they are confronted with information about potential losses but inclined to be “risk averse” when they are confronted with information about potential gains.14,15 The theory further suggests that preference for risk seeking or risk avoidance largely depends on how information is framed. The premise of framing is that whether information is presented in the form of a gain or of a loss can potentially influence an individual’s decision.16
A potential application of the prospect theory in work rehabilitation research is that injured workers may respond in a predictable manner in reaction to the anticipated gains and losses involved in RTW. Under Hong Kong’s Employers’ Compensation Ordinance, injured workers are paid four fifths of their wage during sick leave.17 This arrangement can be regarded as a gain or a loss depending on the perspective and framing of the message. The message can be framed negatively, which emphasizes “a loss of the full wage” during sick leave, or framed positively, which emphasizes “a gain of the full wage” if returning to work. Individuals were found to be more sensitive to differences presented in smaller numbers than larger numbers: 3% versus 7% absence rates and 97% versus 93% presence rates.16
Past research seldom examined the effect of message framing about pain or wage outcomes on injured workers’ decision-making processes in regards to RTW. Prospect theory hypothesizes that an individual’s decision is contingent on the perceived risks of potential gains or losses brought about by a decision, rather than the actual intensity or impact of its outcome.12,15,16 In the field of health psychology, gain and loss message framing is also a strategy to influence people in their health behaviors.18 In this study, we attempted to manipulate the way in which information was presented to the participants. We anticipated that information on wages, which is a facilitating factor, and pain, which is a de-facilitating factor, would influence a participant’s decision on RTW. In addition, the same kind of information presented in two opposite framings, positive (large numbers, 80%–100%) versus negative (small numbers, 0%–20%), would affect their decision making. We expected that the participants’ responses would be more significantly influenced by attributes presented in negative frames than in positive frames. Another variable manipulated in this experiment was the content of the information related to a worker’s RTW. We hypothesized that participants who were exposed to information on wage in the form of negative frames would be more inclined to make decisions on early RTW than those in other conditions such as positive frames and/or information on pain. A cohort of injured workers were invited to participate in this study, and we aimed to examine their responses in terms of confidence and expectation to RTW, immediately after being exposed to the message framing conditions, as well as re-visit the responses 6 months later.
Method
Research design
This study adopted a four-group repeated measures experimental design. The two main variables, information content and method of presentation, were combined to form four experimental conditions. The information content was wages and pain, whereas methods of presentation were positive and negative framing, resulting in a total of four information–presentation pairs. In each group, the participants were presented with stimuli composed of two information–presentation pairs (Figure 1). The pain gain (PG) group had information on gain in pain presented in a negative frame (small percentage values) and information on loss of wage presented in a positive frame (large percentage values). The control (CT) group had the wage and pain information presented in a positive frame. The ambivalence (AB) group had the wage and pain information presented in a negative frame. The wage loss (WL) group had the wage information presented in a negative frame and pain information presented in a positive frame. After presenting the two pairs of information, each participant was asked to make a rating of three RTW outcomes. These outcomes were 1) perceived chance of successful RTW, 2) confidence of successful RTW, and 3) anticipated sick leave to be taken before RTW. They were also required to respond to: 1) whether they would agree to RTW or stay on sick leave if they were instructed to RTW on the next day and 2) the mode of duty if choosing to RTW.
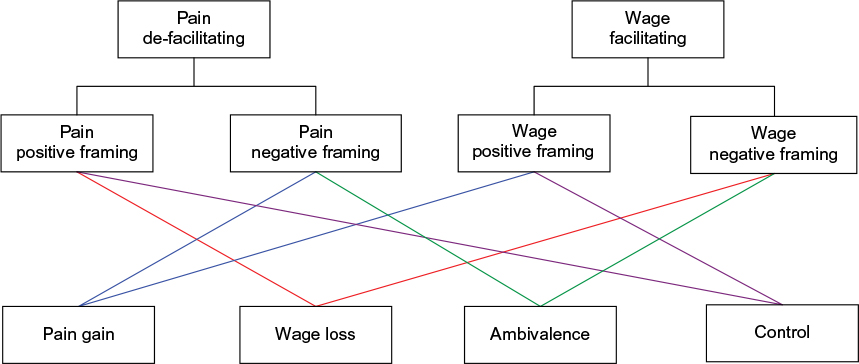 | Figure 1 Study design showing the combination of positive and negative framing arrangements in the 4 experimental groups: 1. pain gain group, 2. wage loss group, 3. ambivalent group, and 4. control group. |
The same participants were contacted again twice, at 2 and 6 months post injury, for a follow-up assessment on their RTW status and total sick leave taken. Those who had been on sick leave were presented with the same framing conditions as at the initial assessment and asked to complete the outcome measure on RTW a second time.
Participants
The participants were referred by insurance companies to receive case management, and they had different types of injuries (n=141). The inclusion criteria were 1) between 20 and 60 years old; 2) sustained musculoskeletal injuries; and 3) had taken <100 sick leave days. The exclusion criteria were 1) recent history of head injury, concussion, or memory loss; 2) known history of psychiatric illness, malignancy, cerebral vascular accident, heart problems, infection, or systemic inflammation; 3) a workplace injury claim that had not been settled prior to the present work-related injury; and 4) unclear liability for the workplace injury claim.
Informed consent was obtained from all the participants, and ethics approval was obtained from the Ethics Committee of the Department of Rehabilitation Sciences at The Hong Kong Polytechnic University. The participants, invited by the case manager to attend the initial assessment, were randomly assigned to one of the four experimental groups using the Latin Square Design (Figure 1). The participants were randomly divided into the four groups, by drawing a paper (numbered 1–4) out of a bag.
Presentation of the wage and pain factors
The wage loss factor
Information on wage was presented as the potential financial loss if the participant chose to stay off work. The percentage of wage loss made reference to the regulation set by the Workers’ Compensation Ordinance of Hong Kong.17 The negative frame was the worker will have no financial loss (0%) if choosing to RTW or a 20% loss if choosing not to RTW. The positive frame was that the worker will receive a 100% wage gain if they choose to RTW or an 80% gain if they choose not to RTW.
The pain gain factor
The information on pain was presented as the potential gain in pain if the participant chose to RTW. The negative frame was the worker will have a 13% chance of experiencing an increase in pain if choosing RTW or a 2% chance of experiencing an increase in pain if choosing not to RTW. The positive frame was that the worker will have an 87% chance of experiencing no increases in pain if choosing RTW or a 98% chance of experiencing no increases in pain if choosing not to RTW.
The task protocol
The participants were invited to attend the first assessment at the investigator’s office. A research assistant (RA) collected their personal information and presented them with the framing conditions. The RA presented all the instructions and stimuli in a standardized manner to the participant.
Baseline assessment
The participants were asked to complete an information sheet, which covered their personal particulars, social and work history, job characteristics, and nature of their injury. At the initial assessment, the participants were asked to report their self-perceived percentages of improvement on a visual analog scale with 0% indicating “no improvement” and 100% indicating “full recovery”. The participants’ “incurred” duration of sick leave was defined as the period between the date of the accident and the date of the initial assessment.
Presentation of experimental stimuli
The experimental stimuli were presented to each subject according to their assigned groups. The order of presentation of the wage and pain factors was standardized, with the wage factor (positive or negative frame) presented before the pain factor (positive or negative frame). The participant was given 1 to 2 minutes to respond to the stimuli and could ask questions if he or she did not understand the content of the stimuli.
After the stimuli were presented to the participants, the participants were required to respond to five items of the anticipated RTW outcomes. These items were modified from a number of studies that examined RTW outcomes.19,20 The five items of the anticipated RTW outcomes were as follow:
Perceived chance of successful RTW. The ratings were made on a 0 to 10-point scale with 0 indicating “no, never” and 10 indicating “yes, definitely”.
Perceived confidence of successful RTW. The ratings were made on a 0 to 10-point scale with 0 indicating “absolutely not” and 10 indicating “yes, definitely”.
Anticipated sick leave to be taken before returning to work. The response was given in terms of the number of months.
The preference for staying on sick leave or for returning to work. The responses were “staying on sick leave” or “RTW”.
Mode of duty arrangements if returning to work. The responses were “same employer, same time,” “same employer, less time,” “different employer, same time,” and “different employer, less time”.
Follow-up assessment
The participants were contacted by telephone around 2 months after the stimuli presentation and baseline assessment. They were asked about their RTW status and, if they had succeeded in returning to work prior to the call, about their total sick leave duration. The sick leave duration of participants was defined as the period between the date of the accident and the date of the initial assessment. Appointments were made for those who were still on sick leave and had not achieved a RTW status to attend an interview session conducted by the researcher. The experimental protocols of the first session were then repeated. The participants were presented with the same framing conditions of wages and pain. They were asked to complete the same five items on anticipated RTW outcomes. Those who had already returned to work were not required to complete the experimental protocol or the assessments.
Data analysis
The baseline characteristics of the participants in terms of demographics, job, and injury profile were compared among the four experimental groups using one-way analysis of variance (ANOVA) or chi-square test. One-way ANOVAs were conducted to compare differences among the four groups on each of the dependent variables. All significant variables were then entered as the predictors of the dummy variable regression analysis. This tested the extent to which these variables would interact with the framing effect that influences the decision making of the participants with regard to RTW outcomes, which is the perceived chance, perceived confidence, and anticipated sick leave duration. Possible significant factors could be the percentage of improvement and sick leave duration. To further refine the analysis, participants were selected according to the perceived percentage of improvement and the amount of sick leave at the time of the initial assessment. One-way ANOVA was rerun to test the framing effects influencing the perceived RTW outcomes of the participants. Similar strategies were used to analyze the participants’ results obtained at the 2-month follow-up assessment.
Results
There were 141 participants who completed the baseline assessment, experimental conditions, and the 2-month follow-up assessment. At the follow-up assessment, 94 participants (66.6%) managed to resume working and 47 participants (33.3%) had not managed to RTW.
There were significantly more male participants (n=91, 64.5%) than female (n=50, 35.5%; Table 1). The mean age of the participants was 40.6 years (SD=11.0), and no significant differences were found in the age of participants among the four experimental groups (F3,137=0.696, p=0.556; Table 1). A high proportion of the workers (n=93, 66%) were involved in manual labor, with a majority of them being either unskilled or semiskilled workers. Most of the participants earned a monthly salary <HK$15,000 (or ~US$1,920; n=122, 86.5%), which could be considered low- or middle-class income earners.
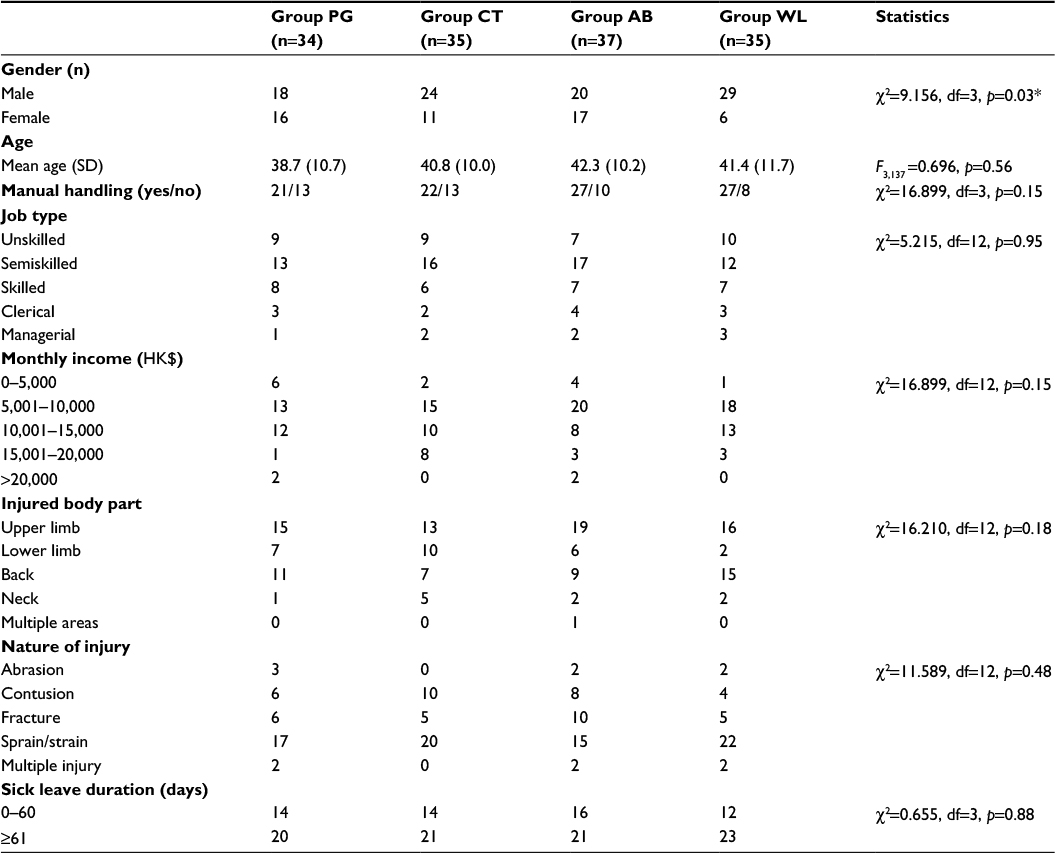 | Table 1 Baseline demographic and injury characteristics of the participants in four experimental groups Notes: All data are presented as frequency counts, except age (mean+SD). *p<0.05. Abbreviations: AB, ambivalent; CT, control; PG, pain gain; SD, standard deviation; WL, wage loss. |
The injury characteristics showed that most of the workers had sustained either an upper limb injury (44.7%) or a back injury (29.8%), and no significant difference was found among the four experimental groups (χ2=16.210, df=12, p=0.18).
Effects of pain and wages on RTW decision making
When the participants were asked to indicate their predicted choice of RTW, 101 (72.3%) selected the RTW option, while only 40 (27.7%) indicated an expectation for staying on sick leave (Table 2). Comparing the mean values in terms of the three variables of perceived chance of RTW, perceived confidence and anticipated sick leave, the AB group seemed to show a trend of unfavorable scores compared to the other three groups. However, no significant differences in the proportions of participants choosing to RTW was found among the four groups (χ2=2.261, df=3, p=0.52). When the participants were asked their preferred mode of RTW if they had to RTW the next day, 109 responded that they preferred to return to the same employer and 22 preferred the same employer but with modified duties and same work hours (Table 2). However, 32 participants responded that they wanted to change employers. The distribution of the preferred mode of RTW was statistically not significant (χ2=8.579, p=0.48).
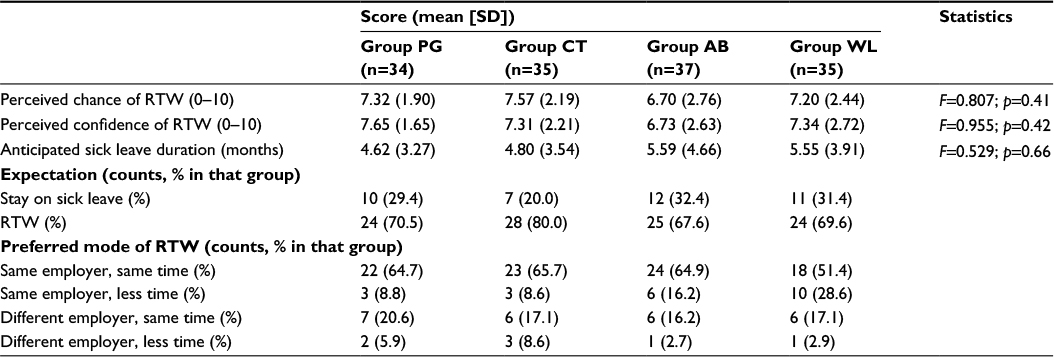 | Table 2 Comparison of participants’ scores on anticipated RTW outcomes across four experimental groups at baseline Abbreviations: AB, ambivalent; CT, control; PG, pain gain; RTW, return to work; WL, wage loss. |
The framing effect
Variables found to exert significant effects on the participants’ ratings of RTW outcomes were percentage of improvement and sick leave duration. Results of the linear regression showed that both sick leave duration and perceived percentage of improvement can significantly predict perceived chance of RTW, perceived confidence of RTW, and anticipated sick leave duration (Table 3). As the medians of the percentage of improvement and sick leave duration were 60% and 60 days, these figures were used for the next stage of statistical analysis.
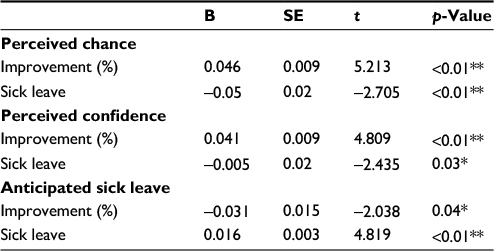 | Table 3 Result of linear regression on the percentage of improvement and sick leave duration Notes: *p<0.05, **p<0.01. |
Participants with ≥60% perceived improvement
Seventy-nine participants who had ≥60% perceived improvement in condition were selected for further analysis (Table 4). The results indicated a significant group effect on the participants’ ratings of perceived chance of RTW (p=0.03) but not on the confidence of RTW (p=0.23) or the anticipated sick leave duration (p=0.92). The CT and WL groups (mean=8.70 and 8.67, respectively) showed the highest mean rating on the perceived chance followed by the PG group (mean=7.43) and then the AB group (mean=7.29). Post hoc comparisons further suggested that participants in the WL and CT groups rated perceived chance of RTW significantly higher than those in the PG group. In contrast, participants in the AB group scored significantly lower than those in the CT group.
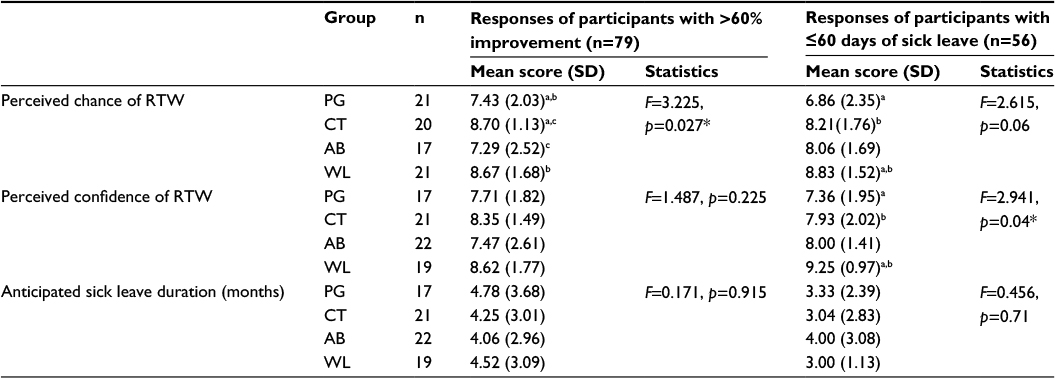 | Table 4 Analysis for perceived chance of RTW, perceived confidence of RTW, and anticipated sick leave duration for the participants with 60% improvement and those with <60 days of sick leave Notes: *p<0.05. a,b,cGroups with significant post hoc pairwise differences at p<0.05; aPG vs CT, bPG vs WL and cCT vs AB. Abbreviations: AB, ambivalent; CT, control; PG, pain gain; RTW, return to work; SD, standard deviation; WL, wage loss. |
Participants with ≤60 days sick leave duration
Fifty-six participants (39.7%) who took ≤60 days of sick leave were selected for further analysis (Table 4). The group effect was found to be not significant on the participants’ ratings of perceived chance of RTW (p=0.06) and anticipated sick leave duration (p=0.71). However, the group effect was significant on the confidence of RTW (p=0.04). The WL group showed the highest rating on the confidence (mean=9.25) which was followed by the AB and CT groups (mean=8.00 and 7.93, respectively). The PG group had the lowest rating on the confidence (mean=7.36). Post hoc comparisons suggested that participants in the WL group rated significantly higher on the confidence of RTW than the PG and CT groups. No significant differences were found between the other groups.
Follow-up assessment
A total of 47 participants were reported as not having RTW and were involved in the follow-up reassessment. Significant differences existed between the baseline assessment and the 2-month follow-up assessment in the percentage improvement (p=0.01). Participants scored significantly lower at the follow-up than at the initial assessment on perceived chance of RTW (p=0.03) and perceived confidence of RTW (p=0.03). In addition, they anticipated a significantly longer sick leave duration at the 2-month follow-up assessment than at initial assessment (p<0.01). There was no interaction among perceived chance of RTW, perceived confidence of RTW, anticipated sick leave duration, and the pain and wage factors.
We followed up with all the participants again at 6 months post-injury in order to determine the relationship between the baseline prediction of RTW status and the actual RTW status after 6 months. A logarithmic regression showed that the predicted choice of RTW could predict the actual RTW outcome at 6 months (OR=9.86; p<0.01; 95% CI: 4.16–23.37) but not at the 2-month follow-up assessment (OR=1.40; p=0.45; 95% CI: 0.59–3.33).
Discussion
There has been very little research conducted that explores the extent to which the effect of message framing can influence the decision-making process in the minds of injured workers when facing an RTW scenario. Injured workers need to make decisions on their RTW continuously throughout the rehabilitation process. Such a decision is involved when they progress through different stages of change, such as from contemplation to preparation and action stage with regard to RTW.19–21 To the injured worker, RTW can be regarded as taking a risk because it is uncertain whether he or she will be capable of resuming pre-injury duties.
This study explored how pain- and wage-related information influences RTW decision making of injured workers. We hypothesized that the decision making of workers could be influenced by the way in which the pain- and wage-related information was framed or presented to the worker. While the results did not reveal significant between-group differences in the perceived confidence and anticipation for RTW outcomes, some interesting findings were noted. Of the four experimental conditions, the CT group involved presenting the wage and pain information in a “positive” frame, whereas the AB had both wage and pain information presented in a negative frame. It is logical that the CT group showed higher scores in perceived chance and confidence of RTW and lower scores in anticipated sick leave, as both messages were presented in a positive frame. However, this difference was not statistically significant which may be due to the small sample size. Both PG and WL groups were presented with one kind of positively framed information and one negatively framed information. The differences in their scores were not so obvious. One explanation of this result may be related to the small sample size in each group. It is also possible that there may be a “trade-off” when one message is framed in a positive way while the second one is in negative frame.
There are many different factors that will influence a worker’s decision about RTW. According to the “Readiness for Return-to-Work” model,19,20 the behavioral changes that individuals undergo are likely to involve a sequential progression from pre-contemplation, contemplation, preparation, action, and maintenance of the desirable behaviors. He et al22 reported that among the various physical, psychosocial, and stage-of-change parameters, the reduction of pre-contemplation and an increase in actions taken on rehabilitation and job-related activities were the most significant predictors of successful RTW. In the current study, the sample of injured workers had a mean sick leave days of ~107 days, which suggest that they were already into the sub-acute or chronic stage of disability. They may be in different stages of readiness to RTW. This may also affect their response to the wage and pain conditions posed to them.
Framing effects of loss of wage versus gain in pain
It has been proposed that wages were a significant facilitating factor considered by injured workers when they contemplated the RTW decision.12 It would be common sense that earning a full wage upon returning to work is a facilitating factor that can motivate any worker. However, if the message is framed in a negative way, that is, they would lose 20% of their wages when they are on sick leave, this message may have a different influence on the worker.
In the present study the wage and pain information was only given once, and there was no other intervention involved. According to the prospect theory, decisions that involve risks, such as discontinuing sick leave by returning to work, can be presented as potential gains or losses. The results suggest that individuals would be more inclined to take risks when confronted with potential losses and are risk averse when confronted with potential gains.13,14 It is plausible that the loss of 20% wage is viewed as an important loss when the participants choose to continue to have sick leave and not return to the workplace. Previous research by Gross and Battie11 also reported that those with more negative “expectations for recovery” were associated with slower claim closure and more unfavorable RTW outcomes.
Research on fear avoidance behavior sheds light on the behavioral changes among participants in the PG group.23 According to the “fear-avoidance behavior” theory, the fear of aggravating pain could result in individuals avoiding movements of the injured limbs, causing them to not engage in activities. When applied to injured workers, the fear of increased pain may lead to avoidance behavior associated with RTW. Previous research indicated that aggravation of pain was one major concern that could have prevented injured workers from RTW.10,11 The contradicting information on gain in pain and loss of wage (both using smaller numbers) appears to further aggravate the negative attitudes among the participants. In a comprehensive review, Wasiak et al24 suggested that RTW outcomes can be examined in different personal dimensions including intentions, expectations, motivation, and satisfaction. A common approach in these studies is to use established questionnaire instruments with outcomes such as quality of life, health status, pain, and function. Questions about loss and gain in wage and pain are seldom posed to the injured workers. Another recent review by Ebrahim et al8 summarized the findings on patients’ expectations about recovery, and only a few studies examined the effects of expectation of pain and time on the discontinuation of compensation benefits. These studies have reported similar trends as our research.
We further demonstrated that the use of small numbers, rather than large, are effective to shape the content of the information as proposed by Wong and Kwong.16 It is plausible that smaller numbers can help improve the preciseness of information. When coupled with prospect theory, for example, a loss initiating risk taking behavior, the 20% loss of wage appears to elicit significant effects on initiating more positive attitudes among the participants toward RTW. However, it is important to note that this approach could also lead to undesirable outcomes because of the use of smaller numbers, such as 13% increase in pain. The negative work-related information could elicit significant negative effects on initiating more negative attitudes. These findings confirm the importance of how work-related information received by injured workers can influence their beliefs and behaviors.
Clinical implications
Practitioners in occupational rehabilitation may consider emphasizing the loss of wage when injured workers are deciding to RTW after completing a rehabilitation course. For instance, practitioners may consider to convey the message that “you would lose 20% of wages if not returning to work” to those workers who are contemplating between staying off work or returning to work. To facilitate a more successful RTW process, it is recommended that the “gain in pain” message is avoided or downplayed. Practitioners may consider using the “gain in comfort” level. Different from the loss of wage, the gain in comfort can be expressed using larger number. The combination of these messages can potentially result in less ambivalent and more positive outcomes of RTW. It is crucial that all parties involved in communicating with the injured workers have an appreciation of the importance of message framing, including human resource personnel, insurance agents, healthcare professionals, and supervisors.21,24
However, it should be noted that wage and pain are not the only concerns of injured workers. It has been proposed that the perception of “fairness” or “justice” in the employer’s approach to the injured worker can exert important influence on the worker’s subsequent attitudes and mental health.25
The present study was conducted with a limited sample of injured workers, and future studies should be larger in scale and involve a randomized controlled trial for testing the gain and loss effects on actual RTW outcomes. In the present study, each participant was only presented with one particular combination of wage and pain gain/loss information. Future research should explore how people will react if they are presented with different combinations of such information. In addition, a longer follow-up period on the injured workers after they RTW would be useful. By improving the understanding of the injured workers’ responses to such pain and wage-related information, it is possible to develop counseling interventions or communication guidelines for healthcare professionals in managing injured workers during the rehabilitation process.21,24 A recent publication has demonstrated favorable results supporting the implementation of a workplace-based intervention program that emphasizes worker–supervisor communication and problem-solving skills, with reduced sick leave and improved health outcomes.26–28 In Hong Kong, the emerging practice of engaging case managers to coordinate the rehabilitation process of injured workers will also benefit from developing appropriate communication strategies involving gains and losses in the RTW process.27,28
Conclusion
Return to work is a complicated process affected by many physical, psychosocial, social, legislative, and labor relations factors. The present study has demonstrated the potential importance of message framing about wage and pain information that can contribute to the cognitive appraisal by injured workers and affect different outcomes in return to work process. As key players in this process, healthcare professionals and other stakeholders, such as case managers, insurance agents, and employers, may find this information useful when communicating with injured workers who are going through the occupational rehabilitation processes.
Acknowledgments
The authors would like to acknowledge the valuable advice of Professor Ellick Wong of the Hong Kong University of Science and Technology on the study design and application of the prospect theory. They would also like to thank Dr. Raymond Chung for his advice on the statistical analysis and the staff at TRM (HK) Ltd for their assistance in contacting the participants in the study. This study was partially supported by an internal research fund awarded to Professor Chetwyn Chan from The Hong Kong Polytechnic University.
Disclosure
The authors report no conflicts of interest in this work.
References
Pransky G, Shaw WS, Franche R, Clarke A. Disability prevention and communication among workers, physicians, employers, and insurers-current models and opportunities for improvement. Disabil Rehabil. 2004;6(11):625–634. | ||
Schultz IZ, Stowell A, Feuerstein M, Gatchel RJ. Models of return to work for musculoskeletal disorders. J Occup Rehabil. 2007;17(2):327–352. | ||
Krause N, Frank JW, Sullivan TJ, Dasinger LK, Sinclaire SJ. Determinants of RTW and duration of disability after work related injury and illness: challenges for future research. Am J Indus Med. 2001;40(4):464–484. | ||
Linton SJ, Gross D, Schultz IZ, Main C, Cote P, Pransky G. Prognosis and identification of workers risking disability: research issues and direction for future research. J Occup Rehabil. 2005;15(4):459–474. | ||
Pransky G, Gatchel R, Linton SJ, Loisel P. Improving return to work research. J Occup Rehabil. 2005;15(4):453–457. | ||
Rossler RT. Motivational factors influencing return to work. J Appl Rehabil Counsel. 1989;20(2):14–17. | ||
Cole D, Mondloch M, Hogg-Johnson S. Listening to injured workers: how recovery expectations predict outcomes-a prospective study. Can Med Assoc J. 2002;166(6):749–754. | ||
Ebrahim S, Malachowski C, el Din MK, Mulla SM, Montoya L, Bance S, Busse JW. Measures of patients’ expectations about recovery: a systematic review. J Occup Rehabil. 2015;25(1):240–255. | ||
Fishbain DA, Rosomoff HL, Cutler RB. Secondary gain concept: a review of the scientific evidence. Clin J Pain. 1995;11(1):6–21. | ||
Gatchel RJ, Adams L, Polatin PB, Kishino ND. Secondary loss and pain-associated disability: theoretical overview and treatment implication. J Occup Rehabil. 2002;12(2):99–110. | ||
Gross DP, Battie MC. Work-related recovery expectations and the prognosis of chronic low back pain within a workers’ compensation setting. J Occup Environ Med. 2005;47:428–433. | ||
Dersh J, Polatin PB, Leeman G, Gatchel RJ. The management of secondary gain and loss in medicolegal settings: strengths and weakness. J Occup Rehabil. 2004;14(4):267–279. | ||
Kahneman D, Tversky A. Prospect theory: an analysis of decision under risk. Econometrica. 1979;47(2):263–291. | ||
Kahneman D, Tversky A. Choices, Value and Frames. Cambridge: Cambridge University Press; 2000. | ||
Barberis NC. Thirty years of prospect theory in economics: a review and assessment. J Econ Perspect. 2013;27(1):173–196. | ||
Wong KFE, Kwong JY. Comparing two tiny giants or two huge dwarfs? preference reversals owing to number size framing. Organ Behav Hum Decis Process. 2005;98(1):54–65. | ||
Hong Kong Labour Department. Annual report of the protection of wages on insolvency fund board. Hong Kong: Hong Kong Labour Department; 2002. Available from: http://www.labour.gov.hk/eng/public/wcp/AnnualReport02-03.pdf. Accessed December 1, 2016. | ||
Rothman AJ, Bartel RD, Wlaschin J, Salovey P. The strategic use of gain and loss framed message to promote healthy behaviour: how theory can inform practice. J Commun. 2006;56(Suppl 1):202–220. | ||
Prochaska JO, Diclemente CC. Stages of change in the modification of problem behaviors. Prog Behav Modif. 1992;28:183–218. | ||
Franche RL, Corbiere M, Lee H, Curtis Bresline F, Gail Hepburn C. The readiness for Return-to-Work (RRTW) scale: development and Validation of a Self-report Staging Scale in lost-time claimants with musculoskeletal disorders. J Occup Rehabil. 2007;17(3):450–472. | ||
Franche R, Baril R, Shaw WS, Nicholas M, Loisel P. Workplace-based return-to-work interventions: optimizing the role of stakeholders in implementation and research. J Occup Rehabil. 2005;15(4):525–542. | ||
He Y, Hu J, Yu ITS, Gu W, Liang Y. Determinants of return to work after occupational injury. J Occup Rehabil. 2010;20(3):378–386. | ||
Fritz JM, George SZ, Delitto A. The role of fear-avoidance beliefs in acute low back pain: relationship with current and future disability and work status. Pain. 2001;94(1):7–15. | ||
Wasiak R, Young AE, Rossler RT, McPherson KM, van Poppel MN, Anema JR. Measuring return to work. J Occup Rehabil. 2007;17(4):766–781. | ||
Hepburn CG, Kelloway EK, Franche RL. Early employer response to workplace injury: What injured workers perceive as fair and why these perceptions matter. J Occup Health Psychol. 2010;15(4):409–420. | ||
Linton SJ, Boersma K, Traczyk M, Shaw W, Nicholas M. Early workplace communication and problem solving to prevent back disability: results of a randomized controlled trial among high-risk workers and their supervisors. J Occup Rehabil. 2016;26(2):150–159. | ||
Lai HS, Chan CCH. Implementing a pilot work injury management program in Hong Kong. J Occup Rehabil. 2007;17(4):712–26. | ||
Kong WM, Tang D, Luo XY, Tak ISY, Liang YX, He YH. Prediction of return to work outcomes under an injured worker case management program. J Occup Rehabil. 2012;22(2):230–240. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.