Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Injections Site Reactions and Biologics for Psoriasis: A Questionnaire Based Real Life Study
Authors Megna M ![]() , Battista T, Noto M, Picone V, Fabbrocini G, Ruggiero A
, Battista T, Noto M, Picone V, Fabbrocini G, Ruggiero A ![]() , Genco L
, Genco L
Received 8 December 2022
Accepted for publication 22 February 2023
Published 2 March 2023 Volume 2023:16 Pages 553—564
DOI https://doi.org/10.2147/CCID.S400679
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Matteo Megna, Teresa Battista,* Matteo Noto,* Vincenzo Picone, Gabriella Fabbrocini, Angelo Ruggiero,* Lucia Genco*
Department of Clinical Medicine and Surgery - Section of Dermatology, University of Naples Federico II, Naples, Italy
*These authors contributed equally to this work
Correspondence: Angelo Ruggiero, Section of Dermatology - Department of Clinical Medicine and Surgery, University of Naples Federico II, Via Pansini 5, Napoli, 80131, Italy, Tel +39 - 081 – 7462457, Fax +39 - 081 – 7462442, Email [email protected]
Background: Biologic selection for psoriasis treatment should take into account numerous factors including injection site reactions (ISRs) such as swelling at the injection site, pain, burning, erythema, all possibly reducing patient adherence.
Methods: A 6-months observational real life study was performed involving psoriasis patients. Inclusion criteria were age ≥ 18 years, moderate-to-severe psoriasis diagnosis since at least 1 year, patients being on biologic treatment for psoriasis ≥ 6 months. A 14-item questionnaire was administered to all patients enrolled to assess whether the patient ever experienced ISRs after the injection of the biologic drug.
Results: 234 patients were included: 32.5% received an anti-TNF-alpha drug, 9.4% received anti-IL12/23, 32.5% received an anti-IL17, 25.6% received an anti-IL23. 51.2% of study population reported at least one symptom related to ISR. 35.9% of patients experienced pain, 31.6% swelling, 28.2% burning sensation and 17.9% erythema. 3.4% of the surveyed population experienced anxiety or fear of the biologic injection due to ISRs symptoms. The greater incidence of pain was registered in anti-TNF-alpha and anti-IL17 groups (47.4% and 42.1%, p< 0.01). Ixekizumab proved to be the drug with the highest rate of patients experiencing pain (72.2%), burning (77.7%) and swelling (83.3%). No patients reported biologics discontinuation or delay for ISRs symptoms.
Conclusion: Our study highlighted that each different class of biologics for psoriasis was linked to ISRs. These events are more frequently reported with anti-TNF-alpha and anti-IL17.
Keywords: psoriasis, injection site reactions, biologic therapy
Introduction
Psoriasis is a chronic inflammatory skin disease that deeply impacts on patients’ life with a relapsing course.1–3 It globally has a prevalence of 3% in the general population, possibly differing among diverse countries.4,5 Psoriasis treatment includes topical treatments such as corticosteroid, vitamin D3 analogues and salicylic acid, conventional systemic therapies such as cyclosporine, methotrexate, fumarates and acitretin as well as new target therapies.6–9 Increased understanding of the pathogenetic mechanisms underlying psoriasis and involved pro-inflammatory cytokines (tumor necrosis factor (TNF)-α, interleukin (IL)-12, IL-17, IL-22, and IL-23) has deeply changed the treatment of psoriasis, providing more effective and targeted therapy for this disease.10–12 Several new systemic drugs are available such as biologics (anti-TNF-α, anti-IL-12–23, anti-IL-17, and anti-IL 23) as well as small molecules (apremilast), positively revolutionizing psoriasis treatment.10 Most of these drugs are administered subcutaneously (SC). There are significant advantages of SC injections over the other injection types, since skilled personnel are not required, in contrast to intravenous and intramuscular (IM) administrations, the risk of infection is lower and SC injections offer a wider range of alternative sites than IM injections for those who require multiple doses.13 Moreover, the SC administration route is widely used to administer different types of drugs given its high bioavailability and rapid onset of action. However, the sensation of pain at the injection site, for example, might reduce patient adherence.13,14 In this context, it has been shown that biologic selection for psoriasis treatment should take into account numerous factors ranging from disease severity, lesions’ location, comorbidities, as well as patients’ preferences which rely not only on the frequency of drug administration but also on injection site reactions (ISRs) such as swelling at the injection site, pain, burning, erythema, all possibly reducing patient adherence.15 ISRs are one of the most common side effects of biologics with an incidence rate of 0.5–40%.15 ISRs are generally mild and self-limited but can be unpleasant for some patients.13 This is the case also for pain or burning sensation during biologics injections, which also may reduce patient adherence, or conducing to treatment delay, all negatively impacting on best treatment outcomes. Hence, we performed an observational real-life study to compare all biologic therapies administered SC and approved for psoriasis treatment (anti-TNF-α such as etanercept, adalimumab, certolizumab pegol, ustekinumab (anti-IL-12/23), anti-IL-17 such as secukinumab, ixekizumab and brodalumab and anti-IL-23 like guselkumab, risankizumab and tildrakizumab)16,17 as regards ISRs, particularly frequency, duration and intensity of symptoms related to biologic SC injection. Indeed, the aim of our study was to analyze and highlight eventual differences among biologics regarding these symptoms which have been too often underestimated even if potentially impacting on quality of life and therapeutic adherence especially in long-term therapies such as those for psoriasis.
Materials and Methods
An observational real-life study was performed involving psoriasis patients attending the Dermatology Unit of the University of Naples Federico II from January 2022 to June 2022. Inclusion criteria were age ≥ 18 years, moderate-to-severe psoriasis diagnosis since at least 1 year, patients being on biologic treatment [anti-TNF-α such as etanercept, adalimumab, certolizumab pegol, ustekinumab (anti-IL-12/23), anti-IL-17 such as secukinumab, ixekizumab and brodalumab and anti-IL-23 like guselkumab, risankizumab and tildrakizumab] for psoriasis ≥ 6 months and maximum 3 years. A 14-item questionnaire was administered to all patients enrolled (Figure 1). The first part of the questionnaire (7 items) examined sociodemographic data and patients’ medical history. In particular age, sex, psoriasis data (duration, previous and current biologic treatment), presence of psoriatic arthritis (PsA) and comorbidities were collected for each patient. Questionnaire part II assessed ISR (7 items); particularly whether the patient ever experienced swelling, pain, burning, or developed erythema after the injection of the biologic drug currently employed. Numerical Rating Scale (NRS) (range 0–10) evaluated the amount of pain experienced. In addition, the duration of swelling, pain and erythema at the injection sites was evaluated. Finally, it was asked whether these ISRs symptoms ever caused delays or interruptions of biologic treatment and whether patients ever experienced fear or anxiety before drug administration. Patients completed their questionnaire anonymously after the medical examination such that their answers could not be influenced by the physicians in any way. This study has been approved by the local Ethical Committee (University of Naples Federico II).
 |
Figure 1 Injections site reactions questionnaire (ISRs). |
Statistical Analysis
Quantitative variables were expressed as the mean and standard deviation (SD). Qualitative variables were expressed as frequencies and percentages. Graph Pad Pro software (v 8.0; Graph Pad software Inc. La Jolla, CA, USA) was used for all statistical analyses. The Mann–Whitney test and Fisher test were used as appropriate to calculate statistical differences; a value of p ≤0.05 was considered significant. Pearson’s correlation coefficient was used to evaluate the statistical relationship, or association, between two continuous variables.
Results
We enrolled a total of 234 patients practising self-injections of the drug: 76 (32.5%) received an anti-TNF-alpha drug (32 Adalimumab; 20 Etanercept; 4 Golimumab; 20 Certolizumab), 22 (9.4%) received Ustekinumab (anti-IL12/23), 76 (32.5%) received an anti-IL17 (20 Secukinumab; 36 Ixekizumab; 20 Brodalumab), 60 (25.6%) received an anti-IL23 (20 Guselkumab; 20 Tildrakizumab; 20 Risankizumab) (Table 1). Study cohort comprised 114 males (48.7%) and 120 females (51.3%) with a mean age of 51.2 years ±15.6.
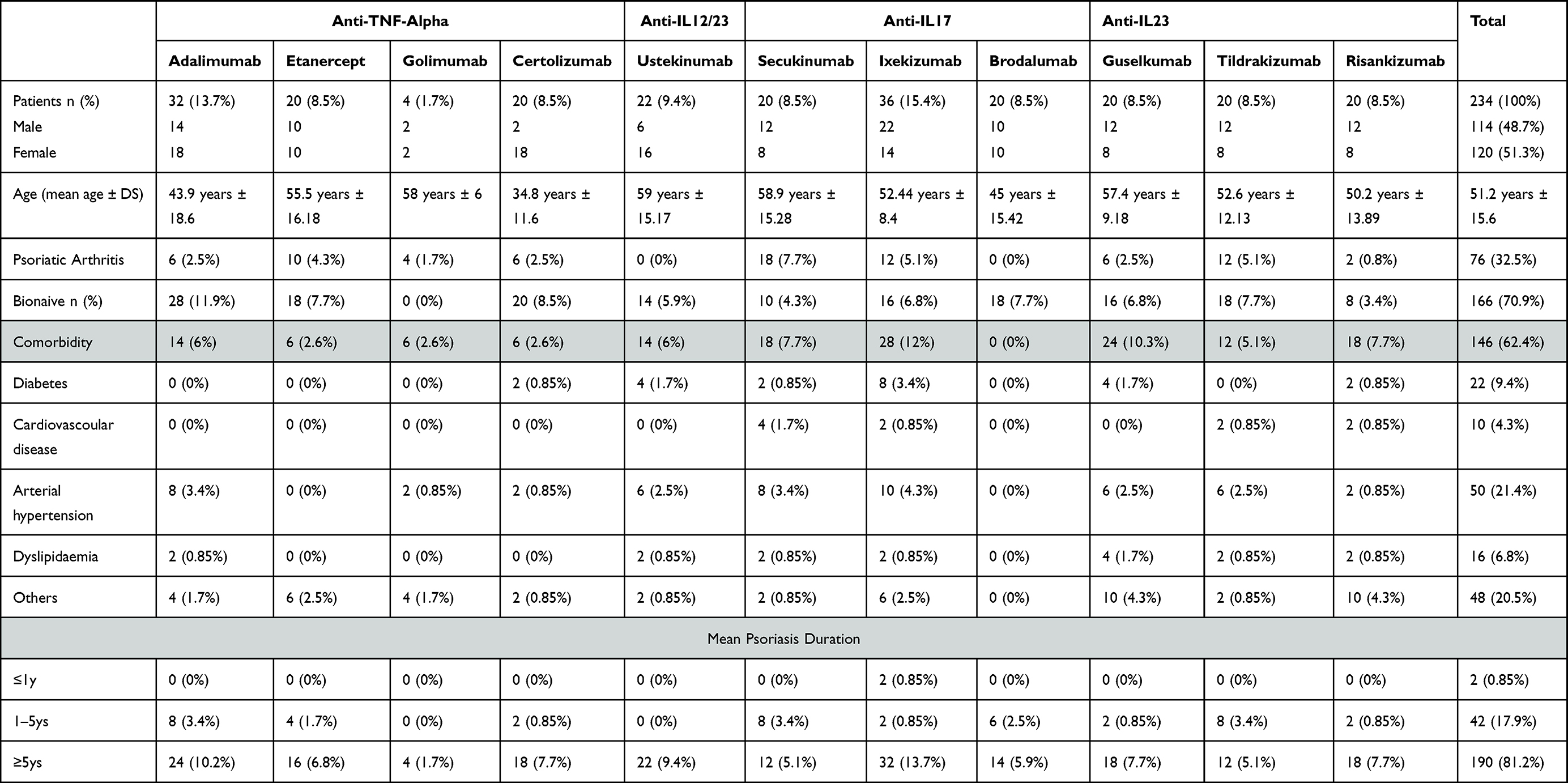 |
Table 1 Clinical and Demographics Characteristics of Our Population |
The majority of the patients (166, 70.9%) were bio-naïve: 28.20% vs 5.9% vs 18.8% vs 17.9% in anti-TNF-alpha vs anti-IL12/23 vs anti-IL17 vs anti-IL23 group, respectively. A significant higher percentage of bio-naïve subjects were hence observed for anti-TNF-alpha treated subjects (p<0.05) (Table 1).
Globally, study population showed a considerable psoriasis history. Indeed, psoriasis duration was ≥5 years in 190 patients (81.2%), between 1–5 years in 42 (17.9%) and ≤1 years in only 2 patients (0.9%) (Table 1).
PsA prevalence was 32.5%, particularly 11.1%, 0%, 12.8%, and 8.5%, in anti-TNF-alpha, anti-IL12/23, anti-IL17, and anti-IL23 groups, respectively (Table 1).
Among other comorbidities arterial hypertension was the most common one followed by diabetes and dyslipidaemia, almost equally also between different treatment groups of patients (see Table 1 for details). ISRs were evaluated in all study population, focusing on percent of patients experiencing pain, burning, erythema and swelling during drug injection through the above reported questionnaire. We also evaluated the duration of all the above reported symptoms and pain intensity through Visual Analogue Scale (VAS) score.
Reports of ISRs collected for each indicated biologics are given in Table 1. Globally, 51.2% of study population reported at least one symptom related to ISR. Overall, 35.9% of patients experienced pain, 31.6% swelling, 28.2% burning sensation and 17.9% erythema (Table 2). Therefore, pain and swelling represented the most frequent ISRs symptoms, followed by burning sensation and then erythema which was identified as the less common event (p<0.01). No difference was recorded between symptoms reported in bio-naive and bio-experienced patients.
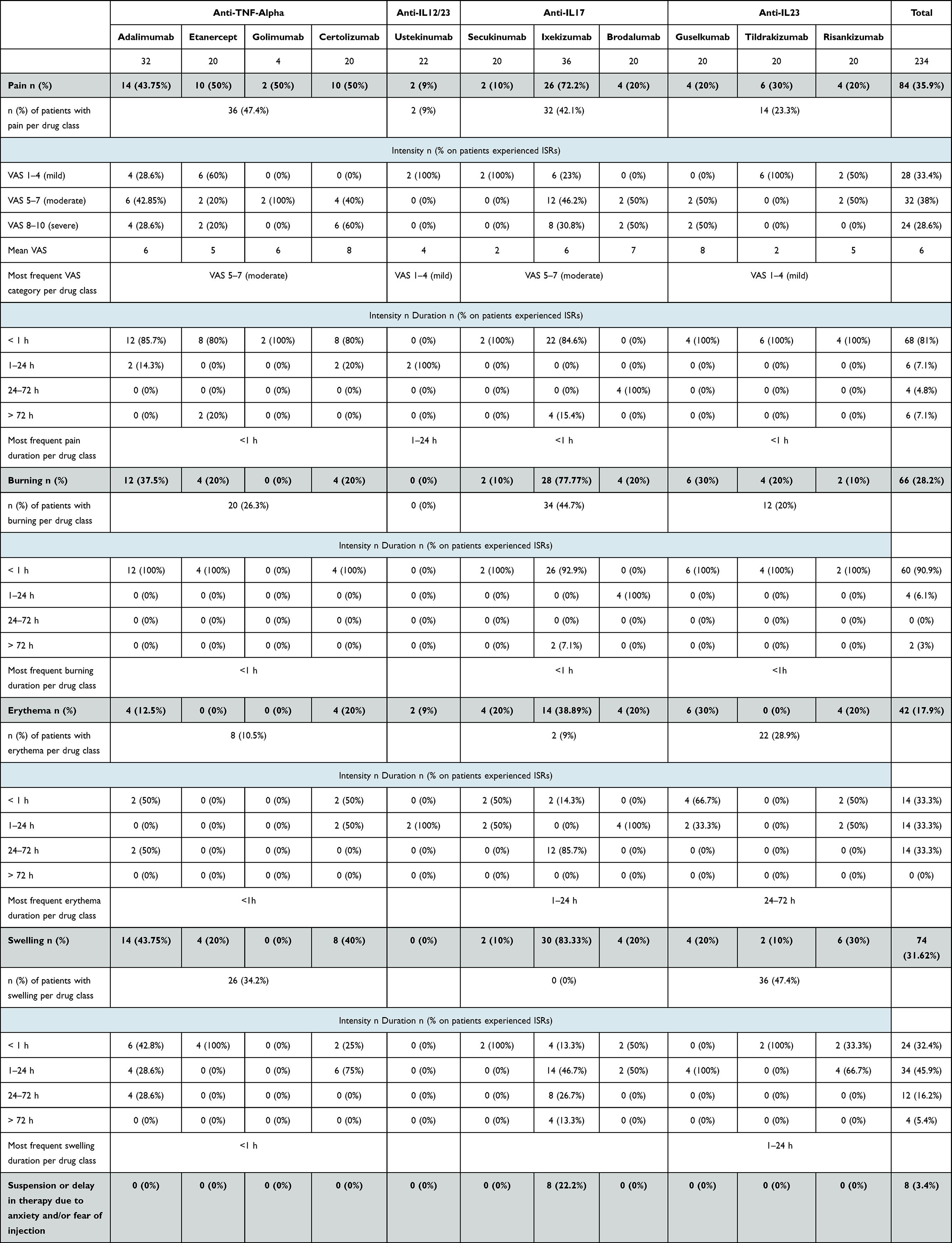 |
Table 2 Analysis of Injection Site Reactions (ISRs) and Suspensions or Delays of Administration Due to Anxiety or Fear of Injections, by Drug Class and Individual Drug |
Focusing on the different drug classes, the greater incidence of pain was registered in anti-TNF-alpha and anti-IL17 groups (47.4% and 42.1%) vs 9% and 23.3% in anti-IL12/23 and anti-IL23 (p<0.01). In addition, anti-TNF- alpha and anti-IL17 treated subjects also registered the highest pain intensity (mean VAS 6, moderate) despite of anti-IL12/23 and anti-IL23 groups which showed the lowest intensity (mean VAS 4, mild). However, interestingly, despite this great impact in terms of pain score, pain symptom duration was shorter (<1h) for anti-TNF-alpha and anti-IL17 compared to anti-IL12/23 group (1–24h) (Table 2).
The highest incidence of burning sensation was reported by patients in the anti-IL17 group (44.7%) with a statistically significant difference compared to anti-TNF class (26.3%, p<0.05) and anti-IL23 (20%, p<0.01), while no patients in the anti-IL12/23 class reported this symptom. For no drug class does the duration of the burning sensation exceed one hour (Table 2).
Regarding erythema, it was the least frequently reported ISRs symptoms among patients undergoing biological therapy (17.9%). It occurred more frequently among the anti-IL17 (28.9%) followed by anti-IL23 group (16.7%), anti-TNF-alpha group (10.5%) and anti-IL12/23 group (9%) even if with no statistically significant difference, except for TNF-alpha group (p<0.01).
It should also be noted that erythema is not only more frequently reported in anti-IL17 class; indeed, in these patients it is also longer-lasting in comparison to the other three classes of biologics (24–72h) (Table 2).
Finally, swelling was significantly more reported in the anti-IL17 population (47.4%) and anti-TNF population (34.2%) compared to the anti-IL23 group (20%, p<0.01) and ustekinumab group where no patients reported swelling (p<0.001) (Table 2).
Regarding the duration of this symptom, there is a tendency in the anti-IL17 and anti-IL23 class to last longer than in the anti-TNF-alpha class (1–24h vs <1h, respectively) (Table 2).
Finally, another finding examined was the discontinuation or delay in the administration of therapy due to anticipatory anxiety and/or fear of injection caused by ISRs.
Our study showed that even if ISRs symptoms were quite common (51.2% of the population reported at least one ISR among pain, burning, erythema and swelling), only 3.4% of the surveyed population experienced anxiety or fear of the biologic injection due to ISRs symptoms. All these patients were under ixekizumab treatment (n=8). This finding is compatible with the greatest impact in terms of pain, burning, erythema and swelling reported in this group (Table 2). Indeed, among all biologics, ixekizumab proved to be the drug with the highest rate of patients experiencing pain (26/36, 72.2%) with a mean VAS 6. It also proved to be the drug with the highest percentage of patients experiencing burning (28/36, 77.7%) and the highest incidence (30/36, 83.3%) and duration (1–24h) of swelling. Moreover, ixekizumab stands out in terms of sample size with erythema (14/36, 38.9%) and its duration (24–72h) (Table 2). Despite all these results reported above, no patient under ixekizumab delayed or discontinued treatment, highlighting that ISRs symptoms tend to be generally mild and easy to manage. Generally, this is the case of all biologics and not only ixekizumab. Indeed, in our study population no patients reported biologics discontinuation or delay for ISRs symptoms and/or anxiety or fear experienced for biologic injection.
Discussion
The introduction of different classes of highly efficacious biologics for the treatment of moderate-to-severe psoriasis has made the algorithm of selecting the most suitable drug quite complex.18–20
Different conditions should be considered: the severity of the disease, lesions location, comorbidities, the presence of PsA, as well as patient’s work, habits, lifestyle and thus the timing of drug administration.19 However, signs and symptoms related to biologics injections (ISRs) are often underestimated but assumes relevance, especially in presence of numerous different therapeutic choices. Indeed, they may impact on adherence to therapy and thus on clinical outcome especially in subjects with belonephobia, or psychological comorbidities. Feldman et al demonstrated in both a German and a US population how the risk of SRI is as important as disease clearance for the patient in assessing treatment choice, if not even greater for those who have already experienced SRI.21 Hence, in order to highlight the patient’s point of view even before that of the clinician, we conducted the present observational questionnaire based real life study to examine the real impact of the ISRs on the psoriatic population afferent to our Center, focusing on the most common adverse events linked to biologics injections at the injection site: pain, burning sensation, erythema and swelling.22 We aimed to assess not only their occurrence but also their severity and duration, and their impact on patients willing to not continue biologic injection or to delay it.
Our analysis showed that all of the currently available biologic drugs for psoriasis (adalimumab, etanercept, certolizumab, ustekinumab, secukinumab, ixekizumab, brodalumab, guselkumab, tildrakizumab, risankizumab) reported at least one ISR, albeit with different incidence rates. In particular, ustekinumab was less likely to be involved in ISRs, which is in agreement with the results of the study by Grace et al.22 These authors conducted a post-marketing analysis of ISRs reports in the Federal Adverse Event Reporting System (FAERS), a US Food and Drug Administration (FDA) database of spontaneous reports of adverse events, medication errors and product quality. They found adverse events for each biologic considered (adalimumab, etanercept, ixekizumab, secukinumab and ustekinumab) and although there are ISRs recorded for each of them, conclusions about ustekinumab cannot be easily drawn given the small number of reports against it (8 ISRs against ustekinumab compared to 18,211 ISRs recorded among all the biologics under review).22 We analysed the ISRs data following both single biologic drug, but also collecting data regarding biologic drug class (anti-TNF, anti-IL12/23, anti-IL17 and anti-IL23) (Figure 2). Globally, 51.2% of our sample reported at least one symptom related to ISR. Of note, our results stem from the analysis of a homogeneous sample in terms of clinical and demographic characteristics, except for two considerations: 1) Mean age was comparable in all groups, except in the Certolizumab group that showed a mean age of 34.8 years±11.6, significantly lower than other groups (p<0.01), compatible with its ideal positioning in psoriasis of young women in childbearing age since it is the only biologics who does not cross human placenta23; 2) A significant higher percentage of bio-naïve subjects were observed for anti-TNF-alpha treated subjects (p<0.05). This data is compatible with the indication of anti-TNF-alpha biosimilars as the first line biological therapy in Italy due to biosimilars lower price compared to other biologics.24 In particular, in the adalimumab group there was the greatest number of bio-naïve (11.8%), although without a significant difference to the other members of the same class.
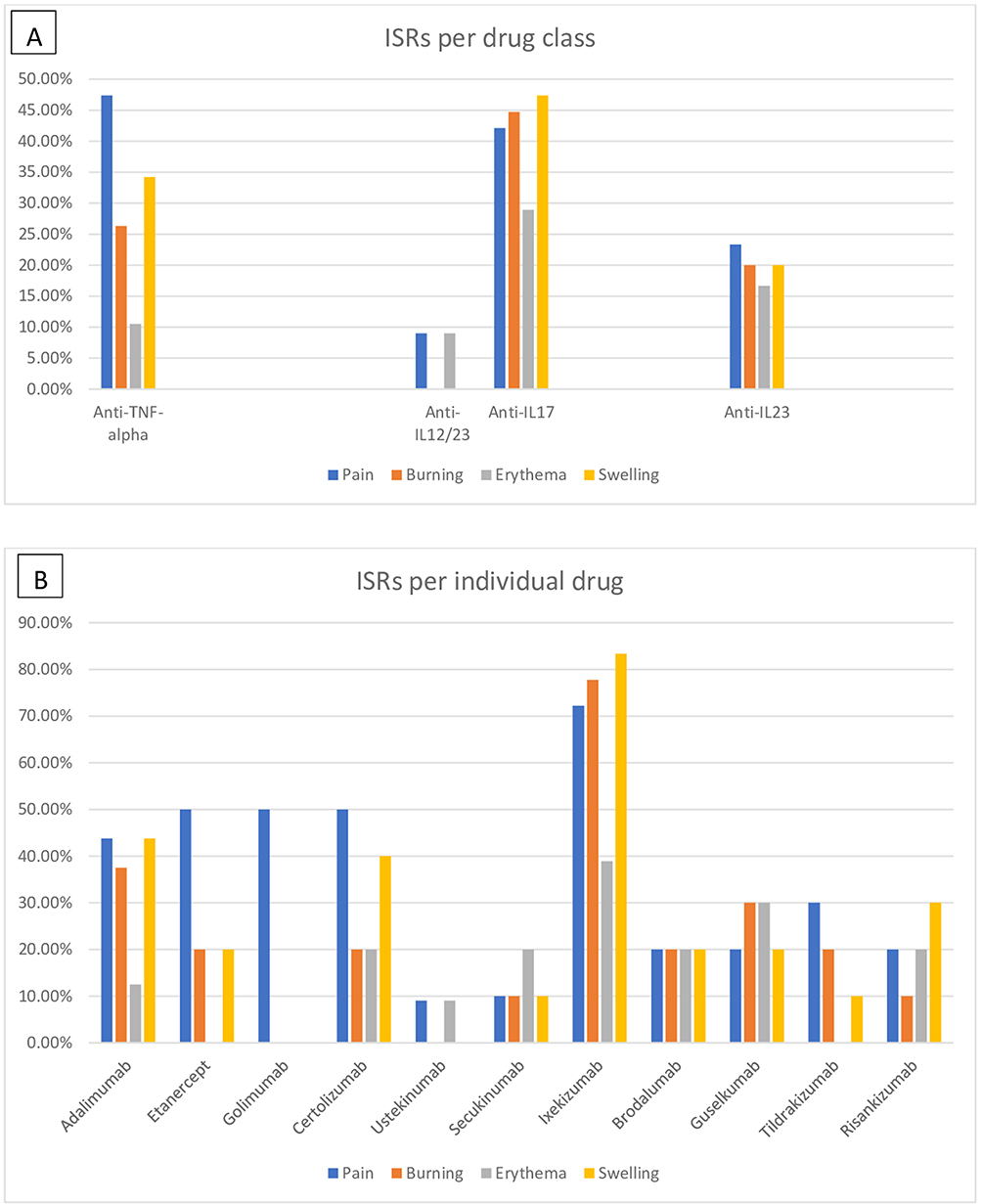 |
Figure 2 Percentages of injection site reactions (ISRs): (A) per drug class; (B) per individual drug. |
Focusing on the individual drug classes, we recorded the highest percentages of ISRs in anti-TNF [pain (47.4%) and swelling (34.2%)] and anti-IL17 groups [swelling (47.4%) and burning (44.7%), pain (42.1%)] (Figure 2).
Anti-TNFalpha and anti-IL17 proved to be the drugs with the highest incidence of pain (47.4% and 42.1%, respectively). No significant difference was observed as regards different anti-TNF drugs, whereas in anti-IL17 class, ixekizumab stands out with the highest percentage of patients experienced pain compared to brodalumab and secukinumab (72.2% vs 20% vs 10%, p<0.001).
Furthermore, the anti-IL17 class was the group with the highest incidence of burning compared to the other three drug classes. Again, ixekizumab, among anti-IL17 group, has the highest percentage of patients experienced such ISR compared to brodalumab and secukinumab (77.8% vs 10% vs 20%, respectively, p<0.01).
Anti-IL17 also presented as the group with the highest percentage of patients with erythema, although statistically significant exclusively compared to anti-TNF-alpha (28.9% vs 10.5% respectively, p<0.01). As regards swelling, again anti-IL17 and anti-TNF, were the drugs with the highest incidence of this symptom compared to anti-IL12/23 and anti-IL23 (p<0.001 and p<0.01, respectively).
Differently from pain and burning sensation, as regards erythema and swelling symptoms, no statistically significant differences between different anti-IL17 were registered.
In line with Grace et al results, we did not record a typical pattern of ISRs in the different classes of biologics.15 Evaluating each drug individually, ixekizumab presented the highest incidences of ISRs. There are numerous factors that may influence ISRs in the subcutaneous injection of ixekizumab, from pH (between 5.3–6.1) to excipients.25 In particular, very recently two new citrate-free formulations were studied that demonstrated a net decrease in negative experiences associated with ixekizumab injection.26 Chabra et al demonstrated, on a VAS scale (0–100 mm), a VAS at time of injection of 3.5 mm vs 25.2 mm for the citrate-free vs original commercial formulation respectively, with a statistically significant difference of 21.7 mm (p<0.0001), the difference decreasing to 4.5 (p<0.0001) at minute ten from injection.26 Chabra et al also demonstrating bioequivalence between the citrate-free and original commercial formulation.26
Citric acid has already been shown to be the major pain-inducing factor at the injection site in adalimumab formulations. Indeed, it was removed from the adalimumab formulation reducing ISRs.22 Thus, it is assumed that the introduction of this new formulation citrate-free will lower the ISRs rates for ixekizumab and thus also for the entire anti-IL17 class. This would be an important therapeutic breakthrough as although in a low percentage (3.4% of the entire population, n=8) patients may experience fear and anticipatory anxiety of the injection. Particularly, all these 8 patients reporting these symptoms were receiving ixekizumab (22.2% of subjects under ixekizumab). However, no cases of treatment discontinuation or delay were registered in our population.
In spite of proven efficacy and safety of ixekizumab in the treatment of moderate-to-severe psoriasis, the most frequently reported adverse event is ISRs (non-specific 9.5%, erythema 3.1% and pain 1.7%).23 As reported by Shear et al, typically ISRs are recorded in the first two weeks of treatment and rapidly the frequency of ISRs decreases over time, with mild-moderate reactions being easily manageable and/or self-limiting.27,28 Although our data compared to these authors show a higher percentage of patients with pain (72.2% vs 1.7%, respectively) and erythema (38.8% vs 3.1%, respectively), the intensity of ISRs are compatible and therefore do not lead to discontinuation or delay of therapy.29 As Shear et al also pointed out, the percentage difference in reported ISRs between clinical trials and real-life analyses may lie in the different injection conditions and techniques (pre-filled syringe vs auto-injector).14 Generally, our study showed that even if ISRs symptoms were quite common in real life (51.2% of population experienced at least one symptom related to ISR), involving all different class of biologics, only 3.4% of the surveyed population experienced anxiety or fear of the biologic injection due to ISRs symptoms and no cases of treatment discontinuation or delay was registered.
Conclusions
Despite ISRs, symptoms are frequently linked to biologics use in psoriasis they have been often underestimated even if possibly negatively impacting on quality of life and treatment adherence. Our real-life study highlighted that each different class of available biologics for psoriasis may be linked to ISRs. These events are more frequently reported with anti-TNF-alpha as well as an anti-IL17. No anti-TNF seems to stand out significantly, whereas ixekizumab seems to be the anti-IL17 with the highest incidence of ISRs. Conversely, ustekinumab seems to be the drug less frequently linked to such events. Generally, despite their frequency, injection related symptoms were easily overcome by patients, not linking to treatment interruption or delay, although they may lead to feelings of fear or anxiety in a very small and limited proportion of the population (3.4%). Our study has several limitations: it is a single-centre study, the symptomatology is reported by means of a questionnaire, so it is self-assessing, and the sample size is limited, especially for some specific biologicals.
Data Sharing Statement
Data sharing not applicable to this article as no datasets were generated or analysed during the current study.
Participant Consent and Ethical Approval
The Declaration of Helsinki’s guiding principles were followed in the conduct of this work. The present study was approved by the local ethic committee (University of Naples Federico II), and informed consent was taken from the participants.
Funding
There is no funding to report for this study.
Disclosure
Matteo Megna acted as a speaker or consultant for Abbvie, Novartis, Eli Lilly, Janssen, UCB, Amgen, Leo Pharma; Gabriella Fabbrocini acted as a speaker or consultant for Abbvie, Novartis, Eli Lilly, Janssen, UCB, Amgen, Leo Pharma, Almirall. The remaining authors report no conflicts of interest in this work.
References
1. Ruggiero A, Fabbrocini G, Cacciapuoti S, et al. Ocular manifestations in psoriasis screening (OcMaPS) questionnaire: a useful tool to reveal misdiagnosed ocular involvement in psoriasis. J Clin Med. 2021;10(5):1031. doi:10.3390/jcm10051031
2. Megna M, Cinelli E, Gallo L, et al. Risankizumab in real life: preliminary results of efficacy and safety in psoriasis during a 16-week period. Arch Dermatol Res. 2022;314(6):619–623. doi:10.1007/s00403-021-02200-7
3. Ruggiero A, Potestio L, Camela E, et al. Bimekizumab for the treatment of psoriasis: a review of the current knowledge. Psoriasis. 2022;8(12):127–137.
4. Parisi R, Iskandar IYK, Kontopantelis E, et al. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. BMJ. 2020;28;369:m1590. doi:10.1136/bmj.m1590
5. Ruggiero A, Fabbrocini G, Cinelli E, et al. Real world practice indirect comparison between guselkumab and risankizumab: results from an Italian retrospective study. Dermatol Ther. 2022;35(1):e15214. doi:10.1111/dth.15214
6. Megna M, Balato A, Napolitano M, et al. Psoriatic disease treatment nowadays: unmet needs among the “jungle of biologic drugs and small molecules”. Clin Rheumatol. 2018;37(7):1739–1741. doi:10.1007/s10067-018-4090-6
7. Megna M, Potestio L, Ruggiero A, et al. Risankizumab treatment in psoriasis patients who failed anti-IL17: a 52-week real-life study. Dermatol Ther. 2022;35(7):e15524. doi:10.1111/dth.15524
8. Megna M, Potestio L, Camela E, et al. Ixekizumab and brodalumab indirect comparison in the treatment of moderate to severe psoriasis: results from an Italian single-center retrospective study in a real-life setting. Dermatol Ther. 2022;35(9):e15667. doi:10.1111/dth.15667
9. Megna M, Tommasino N, Potestio L, et al. Real-world practice indirect comparison between guselkumab, risankizumab, and tildrakizumab: results from an Italian 28-week retrospective study. J Dermatolog Treat. 2022;33(6):2813–2820. doi:10.1080/09546634.2022.2081655
10. Henderson Berg MH, Carrasco D. Injection site reactions to biologic agents used in psoriasis and psoriatic arthritis. J Drugs Dermatol. 2017;16(7):695–698.
11. Megna M, Potestio L, Fabbrocini G, et al. Long-term efficacy and safety of guselkumab for moderate to severe psoriasis: a 3-year real-life retrospective study. Psoriasis. 2022;12:205–212. doi:10.2147/PTT.S372262
12. Ruggiero A, Martora F, Picone V, et al. The impact of COVID-19 infection on patients with psoriasis treated with biologics: an Italian experience. Clin Exp Dermatol. 2022;47(12):2280–2282. doi:10.1111/ced.15336
13. Usach I, Martinez R, Festini T, Peris JE. Subcutaneous injection of drugs: literature review of factors influencing pain sensation at the injection site. Adv Ther. 2019;36(11):2986–2996. doi:10.1007/s12325-019-01101-6
14. Megna M, Camela E, Battista T, et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part I: focus on pediatric patients. Expert Opin Drug Saf. 2023. doi:10.1080/14740338.2023.2173171
15. Thomaidou E, Ramot Y. Injection site reactions with the use of biological agents. Dermatol Ther. 2019;32(2):e12817. doi:10.1111/dth.12817
16. Megna M, Ocampo-Garza SS, Potestio L, et al. New-onset psoriatic arthritis under biologics in psoriasis patients: an increasing challenge? Biomedicines. 2021;9(10):1482. doi:10.3390/biomedicines9101482
17. Ruggiero A, Potestio L, Cacciapuoti S, et al. Tildrakizumab for the treatment of moderate to severe psoriasis: results from a single center preliminary real-life study. Dermatol Ther. 2022;35(12):e15941. doi:10.1111/dth.15941
18. Potestio L, Genco L, Villani A, et al. Reply to ‘Cutaneous adverse effects of the available COVID-19 vaccines in India: a questionnaire-based study’ by Bawane J et al. J Eur Acad Dermatol Venereol. 2022;36(11):e863–e864. doi:10.1111/jdv.18341
19. Ruggiero A, Camela E, Potestio L, et al. Drug safety evaluation of tildrakizumab for psoriasis: a review of the current knowledge. Expert Opin Drug Saf. 2022;21(12):1445–1451. doi:10.1080/14740338.2022.2160447
20. Megna M, Camela E, Battista T, et al. Efficacy and safety of biologics and small molecules for psoriasis in pediatric and geriatric populations. Part II: focus on elderly patients. Expert Opin Drug Saf. 2023. doi:10.1080/14740338.2023.2173171
21. Feldman SR, Poulos C, Gilloteau I, et al. Exploring determinants of psoriasis patients’ treatment choices: a discrete-choice experiment study in the United States and Germany. J Dermatolog Treat. 2022;33(3):1511–1520. doi:10.1080/09546634.2020.1839007
22. Grace E, Goldblum O, Renda L, et al. Injection site reactions in the federal adverse event reporting system (FAERS) post-marketing database vary among biologics approved to treat moderate-to-severe psoriasis. Dermatol Ther (Heidelb). 2020;10(1):99–106. doi:10.1007/s13555-019-00341-2
23. Mariette X, Förger F, Abraham B, et al. Lack of placental transfer of certolizumab pegol during pregnancy: results from CRIB, a prospective, postmarketing, pharmacokinetic study. Ann Rheum Dis. 2018;77(2):228–233. doi:10.1136/annrheumdis-2017-212196
24. Gisondi P, Fargnoli MC, Amerio P, et al. Italian adaptation of EuroGuiDerm guideline on the systemic treatment of chronic plaque psoriasis. Ital J Dermatol Venerol. 2022;157(1):1–78. doi:10.23736/S2784-8671.21.07132-2
25. Shear NH, Paul C, Blauvelt A, et al. Safety and Tolerability of Ixekizumab: integrated Analysis of Injection-Site Reactions from 11 Clinical Trials. J Drugs Dermatol. 2018;17(2):200–206.
26. Chabra S, Gill BJ, Gallo G, et al. Ixekizumab Citrate-Free Formulation: results from Two Clinical Trials. Adv Ther. 2022;39(6):2862–2872. doi:10.1007/s12325-022-02126-0
27. Annunziata MC, Patrì A, Ruggiero A, et al. Cutaneous involvement during COVID-19 pandemic: an emerging sign of infection. J Eur Acad Dermatol Venereol. 2020;34(11):e680–e682. doi:10.1111/jdv.16769
28. Zagaria O, Villani A, Ruggiero A, et al. New-onset lichen planus arising after COVID-19 vaccination. Dermatol Ther. 2022;35(5):e15374. doi:10.1111/dth.15374
29. Megna M, Potestio L, Ruggiero A, et al. Guselkumab is efficacious and safe in psoriasis patients who failed anti-IL17: a 52-week real-life study. J Dermatolog Treat. 2022;33(5):2560–2564. doi:10.1080/09546634.2022.2036674
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Tildrakizumab in a Patient with Chronic HBV Infection
Potestio L, Piscitelli I, Fabbrocini G, Martora F, Ruggiero A, Megna M
Clinical, Cosmetic and Investigational Dermatology 2023, 16:369-373
Published Date: 5 February 2023
Two Cases of Immune Drift Phenomena Caused by Biologic Agents for Treating Psoriasis and Atopic Dermatitis
Ma X, Li T, Han G
Clinical, Cosmetic and Investigational Dermatology 2023, 16:3521-3525
Published Date: 7 December 2023
Immunosenescence in Older Patients with Psoriasis: Mechanistic Insights and Opportunities for Biologic Therapy
Wang W, Zha S, Sun L, Zhou D
Psoriasis: Targets and Therapy 2026, 16:604199
Published Date: 27 May 2026