Back to Journals » Clinical Ophthalmology » Volume 14
Initial Treatment Response in Ocular Myasthenia Gravis: A Comparison Between Low and Moderate Doses of Prednisolone
Authors Threetong T ![]() , Poonyathalang A
, Poonyathalang A ![]() , Preechawat P, Jindahra P, Padungkiatsagul T
, Preechawat P, Jindahra P, Padungkiatsagul T ![]() , Vanikieti K
, Vanikieti K
Received 7 May 2020
Accepted for publication 23 June 2020
Published 22 July 2020 Volume 2020:14 Pages 2051—2056
DOI https://doi.org/10.2147/OPTH.S261259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Thanatporn Threetong,1,2 Anuchit Poonyathalang,1 Pisit Preechawat,1 Panitha Jindahra,3 Tanyatuth Padungkiatsagul,1 Kavin Vanikieti1
1Department of Ophthalmology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Department of Ophthalmology, Faculty of Medicine, Burapha University, Chonburi, Thailand; 3Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Tanyatuth Padungkiatsagul
Department of Ophthalmology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Bangkok 10400, Thailand
Tel +662 201 1526
Fax +662 201 2729
Email [email protected]
Purpose: To evaluate the initial treatment response to low doses of prednisolone, compared with moderate doses, in ocular myasthenia gravis (OMG).
Patients and Methods: A retrospective chart review of patients with adult-onset (age ≥ 15 years old) OMG, who were treated with prednisolone, was conducted. Subjects were divided into two groups according to their prednisolone dosing regimen. The low-dose group was defined as those with an average 12-week cumulative dose of prednisolone < 0.435 mg/kg/day and the moderate-dose group averaged 0.435– 1.000 mg/kg/day. The primary outcome of interest was the comparison of clinical response to prednisolone at 12 weeks between the low-dose and moderate-dose groups. The secondary outcome was the difference in adverse events between treatment groups.
Results: Of 34 subjects, 16 subjects (47.1%) were male. The mean age at onset was 44.0± 18.1 years. The most common presenting ocular feature was ptosis with ophthalmoplegia (22 subjects, 64.7%), followed by isolated ptosis (nine subjects, 26.5%) and isolated ophthalmoplegia (three subjects, 8.8%). Half of the subjects were treated with low-dose prednisolone and the other half were treated with moderate-dose prednisolone. There were no substantial differences in baseline characteristics between treatment groups. After 12 weeks of treatment, nine of 17 subjects (52.9%) and 13 of 17 subjects (76.5%) in the low- and moderate-dose groups, respectively, were regarded as responsive to the prednisolone treatment (P=0.28). Adverse events were exclusively observed in the moderate-dose group.
Conclusion: Treatment of OMG with an average 12-week cumulative dose of prednisolone < 0.435 mg/kg/day (low dose) shows a comparable responsive outcome to 0.435– 1.000 mg/kg/day of prednisolone (moderate dose). Treating OMG with low-dose prednisolone can minimize prednisolone-related adverse events. However, a prospective randomized controlled trial with a larger study population is warranted in order to gain more insight into the proper dosage of prednisolone for OMG.
Keywords: ocular myasthenia gravis, low dose, moderate dose, prednisolone, treatment outcome
Introduction
Myasthenia gravis (MG) is an autoimmune disease with autoantibodies against the acetylcholine receptor, muscle-specific kinase (MUSK), lipoprotein-related protein 4 (LRP4) or agrin in the postsynaptic membrane of the neuromuscular junction.1 Clinical presentation depends on the muscles involved, but the hallmark of MG is fluctuation between normal function and muscle weakness, which worsens over the course of prolonged muscular activity. Ocular myasthenia gravis (OMG) is a subgroup of this disease, in which weakness is restricted to the ocular muscles (levator palpebrae superioris, orbicularis oculi and extraocular muscles), whereas in generalized myasthenia gravis (GMG), weakness manifests in muscles other than the ocular muscles. Overall, 60% of MG patients have some ocular muscle involvement at presentation and OMG accounts for 20% of all MG cases.2–5 Twenty percent of OMG patients convert to GMG and 70% of the conversions occur within 2 years after onset.6
Pyridostigmine—an acetylcholinesterase inhibitor—increases the acetylcholine level in neuromuscular junctions after stimulation, which results in a reduction in muscle weakness; it is the preferred symptomatic treatment.7 For patients who do not adequately respond to this symptomatic therapy, immunosuppressive drugs are the treatment modality of choice.
Prednisolone is the first-line medication used for bridging therapy; that is, before other immunosuppressants (methotrexate, azathioprine and mycophenolate mofetil) reach levels sufficient for their therapeutic effects. Prior observational studies suggest that prednisolone treatment achieves clinical improvement and reduces the risk of developing GMG.8 The dosing regimens of oral prednisolone vary among studies; the standard dosing regimen of prednisolone has not been established because well-controlled studies are sparse. In one review, prednisolone was started at a relatively low dose of 20 mg/day, then increased by 5–10 mg/day every 3 days until symptoms resolved.2 Another study started prednisolone at 10 mg/day for 2 days, followed by 20 mg/day for 2 days, then the dose was increased to 50–60 mg/day for 1 week, and then gradually reduced by 10 mg/day each week until a level of 10 mg/day was reached, and then further reduced by 2.5 mg/day each week.9 One randomized controlled trial, the EPITOME (Efficacy of Prednisone for the Treatment of Ocular Myasthenia) study, demonstrated the safety and efficacy of low-dose prednisolone (starting dose of 10 mg every other day, adjusted to a maximum of 40 mg/day over 16 weeks).10
Our objective was to evaluate the initial treatment response to low doses of oral prednisolone, compared with moderate doses, in patients with OMG.
Materials and Methods
Study Design
A retrospective cohort study was performed at a single tertiary center, the Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand. Case inclusion criteria were: 1) adult subject (age ≥15 years old) with a diagnosis of OMG, and 2) received prednisolone (dosage did not exceed 1 mg/kg/day) as a treatment for OMG. The diagnosis of OMG was made according to one of the following methods.
- Improvement of ptosis and/or ophthalmoplegia after intravenous edrophonium hydrochloride injection (edrophonium test)
- Presence of serum acetylcholine receptor antibody (AChR Ab)
- Abnormal repetitive nerve stimulation (RNS) or single-fiber electromyography (SFEMG)
- Ptosis reversal with ice-pack test.
Individuals who had concomitant thyroid-associated ophthalmopathy, who were younger than 15 years old at onset, who were prescribed immunosuppressive drugs concomitantly and/or who converted to GMG during 12 weeks of treatment were excluded. Patients were included as subjects if the chart review satisfied the inclusion/exclusion criteria. All enrolled subjects were seen between January 2011 and December 2018. Approval for this study was obtained from the Institutional Review Board of the Faculty of Medicine Ramathibodi Hospital, Mahidol University. The study was conducted according to the tenets of the Declaration of Helsinki.
Demographic data, including age of onset and gender, presenting ocular features (ptosis and/or ophthalmoplegia), presence of AChR Ab, results of electromyography testing (RNS and SFEMG) and the edrophonium test, ice-pack test, thyroid function test, and the presence of thymoma/thymic hyperplasia were reviewed.
All subjects received pyridostigmine as an adjunct to oral prednisolone. However, pyridostigmine was not administered within 5 hours prior to the examination of subjects during follow-up. The prednisolone dosing regimen was adjusted, based on each individual’s response to oral prednisolone, by the treating physicians. The dose was not to exceed 1 mg/kg/day. The average 12-week cumulative dose of prednisolone was calculated as the total prednisolone (mg) received during 12 weeks, divided by the number of days taking prednisolone and then divided by body weight in kilograms. According to our knowledge, no standard cut-off level between low and moderate doses of prednisolone has been described in prior studies. Therefore, subjects were grouped according to average 12-week cumulative dosage (low-dose and moderate-dose groups) using the median of the average 12-week cumulative dose of prednisolone from all subjects, 0.435 mg/kg/day, as the cut-off, in order to allocate subjects to both treatment groups equally. This cut-off level was determined after the data collection process. The low-dose group consisted of patients who received an average 12-week cumulative dose of prednisolone of <0.435 mg/kg/day and those in the moderate-dose group received 0.435–1.000 mg/kg/day.
Treatment response data were collected after 12 weeks of treatment, before other immunosuppressants (methotrexate, azathioprine or mycophenolate mofetil) achieved their therapeutic effects. The primary outcome measure was the treatment response. Treatment response was graded according to the categories of Kim et al: complete remission, major improvement, minor improvement, or no response or deterioration.11 The definitions of treatment response are summarized in Table 1. Complete remission, major improvement and minor improvement were classified as responsive, while no response and deterioration were classified as non-responsive. Subgroup analyses by age of onset, gender, presence of AChR Ab, presenting clinical features and thyroid function test were carried out. As a secondary outcome, we examined adverse events in both groups.
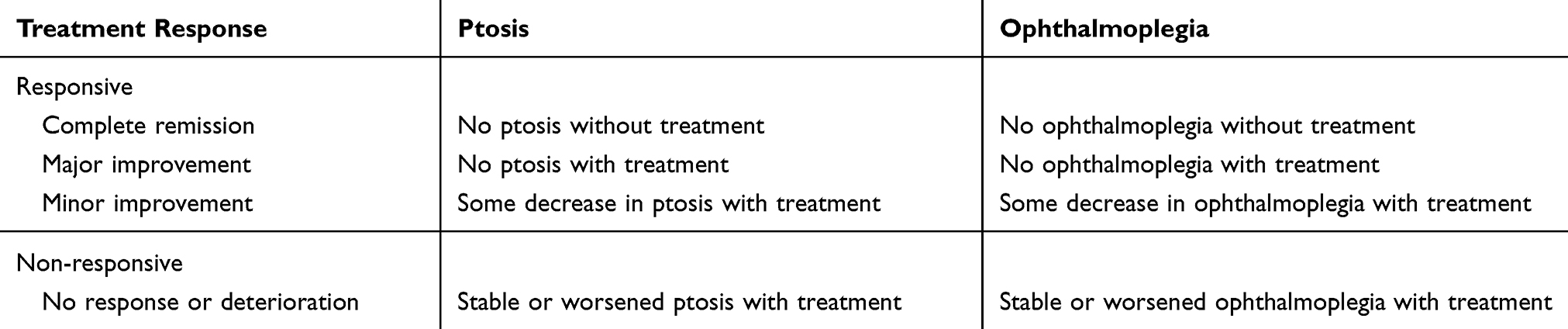 |
Table 1 Definitions of Treatment Responses |
Statistical Analysis
Fisher’s exact test was used to compare the incidence of treatment responses between the two treatment groups. A significance level of P<0.05 (two-tailed) was used for hypothesis testing.
Results
The medical records of 34 subjects were retrospectively reviewed. The age of onset was 44.0±18.1 years (mean±SD). The most common presenting ocular feature was ptosis with ophthalmoplegia (22 subjects, 64.7%), followed by isolated ptosis (nine subjects, 26.5%) and isolated ophthalmoplegia (three subjects, 8.8%). There were 17 subjects in each treatment group. In the low-dose group, the average 12-week cumulative dose was 0.23±0.11 mg/kg/day (mean±SD). In the moderate-dose group, the average 12-week cumulative dose was 0.65±0.15 mg/kg/day (mean±SD). There were no substantial differences between the treatment groups with respect to baseline characteristics (Table 2). The age of onset was 50.1±18.0 years (mean±SD) in the low-dose group and 37.9±16.1 years (mean±SD) in the moderate-dose group. There were 10 males (58.8%) in the low-dose group and six (35.3%) in the moderate-dose group. Three presenting clinical features were observed in both groups: isolated ptosis (six subjects [35.3%] in the low-dose group and three subjects [17.6%] in the moderate-dose group); isolated ophthalmoplegia (one subject [5.9%] in the low-dose group and two subjects [11.8%] in the moderate-dose group); and ptosis with ophthalmoplegia (10 subjects [58.8%] in the low-dose group and 12 subjects [70.6%] in the moderate-dose group).
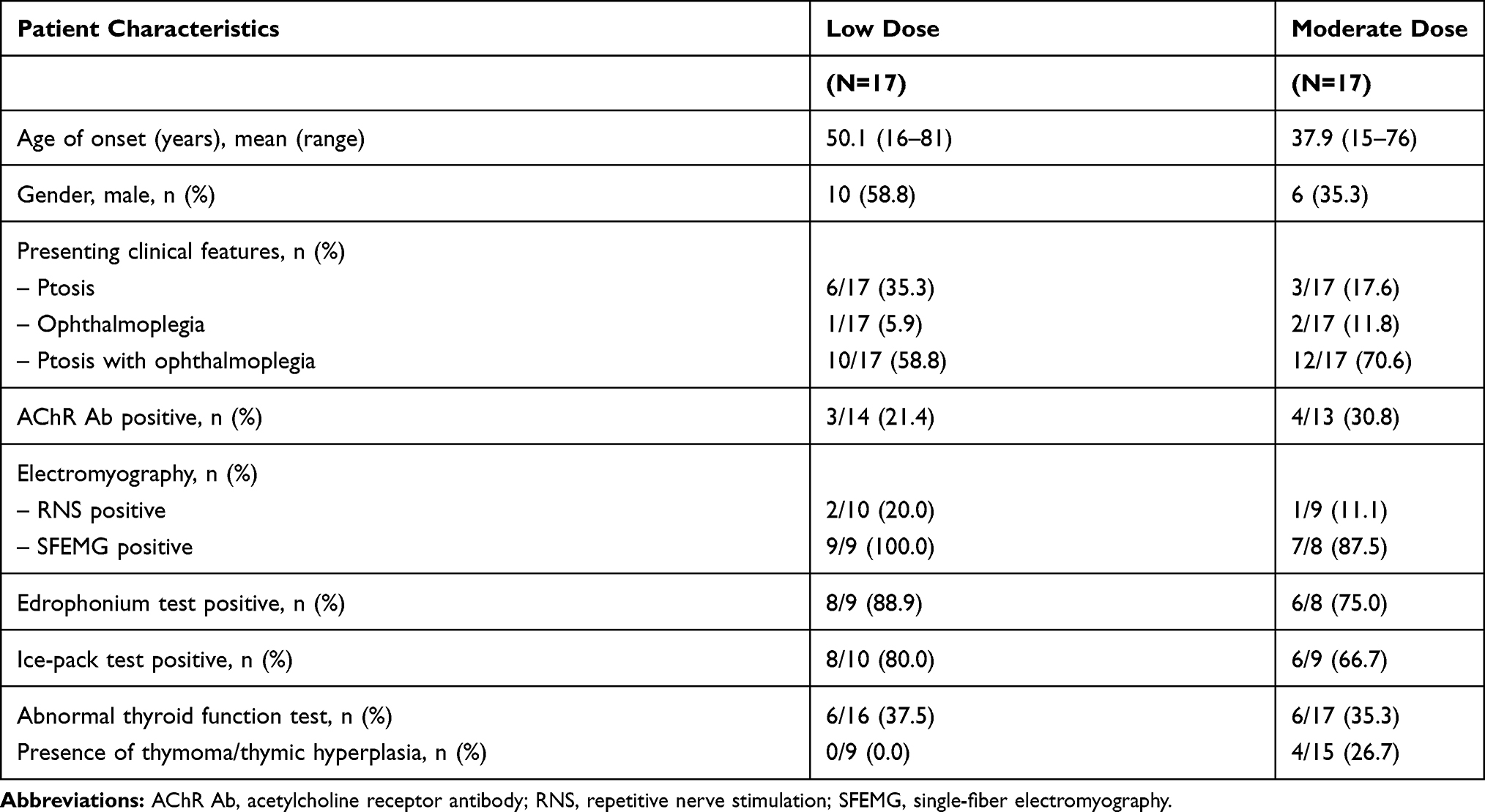 |
Table 2 Comparison of Patient Characteristics Between the Low-Dose and Moderate-Dose Groups |
Of those tested for AChR Ab, the result was positive in three of 14 subjects (21.4%) and four of 13 subjects (30.8%) in the low- and moderate-dose groups, respectively. In the electromyography study, SFEMG was positive more often than RNS in both groups (SFEMG: 100.0% and 87.5%; RNS: 20.0% and 11.1% in the low- and moderate-dose groups, respectively). The edrophonium test and ice-pack test were also performed in both treatment groups. The percentages of positive subjects were fairly similar in both treatment groups (Table 2). A thyroid function test was performed in 16 subjects in the low-dose group and all subjects in the moderate-dose group. Abnormal thyroid function results were found in six subjects in each treatment group (37.5% in the low-dose group and 35.3% in the moderate-dose group). Chest computed tomography (CT) screening for thymoma or thymic hyperplasia was conducted in nine and 15 subjects in the low- and moderate-dose groups, respectively. No thymoma or thymic hyperplasia was observed in the low-dose group, whereas four subjects in the moderate-dose group demonstrated thymoma or thymic hyperplasia (Table 2).
With regard to the treatment response definition (Table 1), a higher response rate was achieved in the moderate-dose group, compared with the low-dose group; 13 subjects (76.5%) and nine subjects (52.9%), respectively. However, this trend did not reach statistical significance (P=0.28). In subgroup analyses, there were no statistically significant differences in response rates between treatment groups based on the age of onset, gender, presenting clinical features, and presence of AChR Ab or thyroid function test (Table 3).
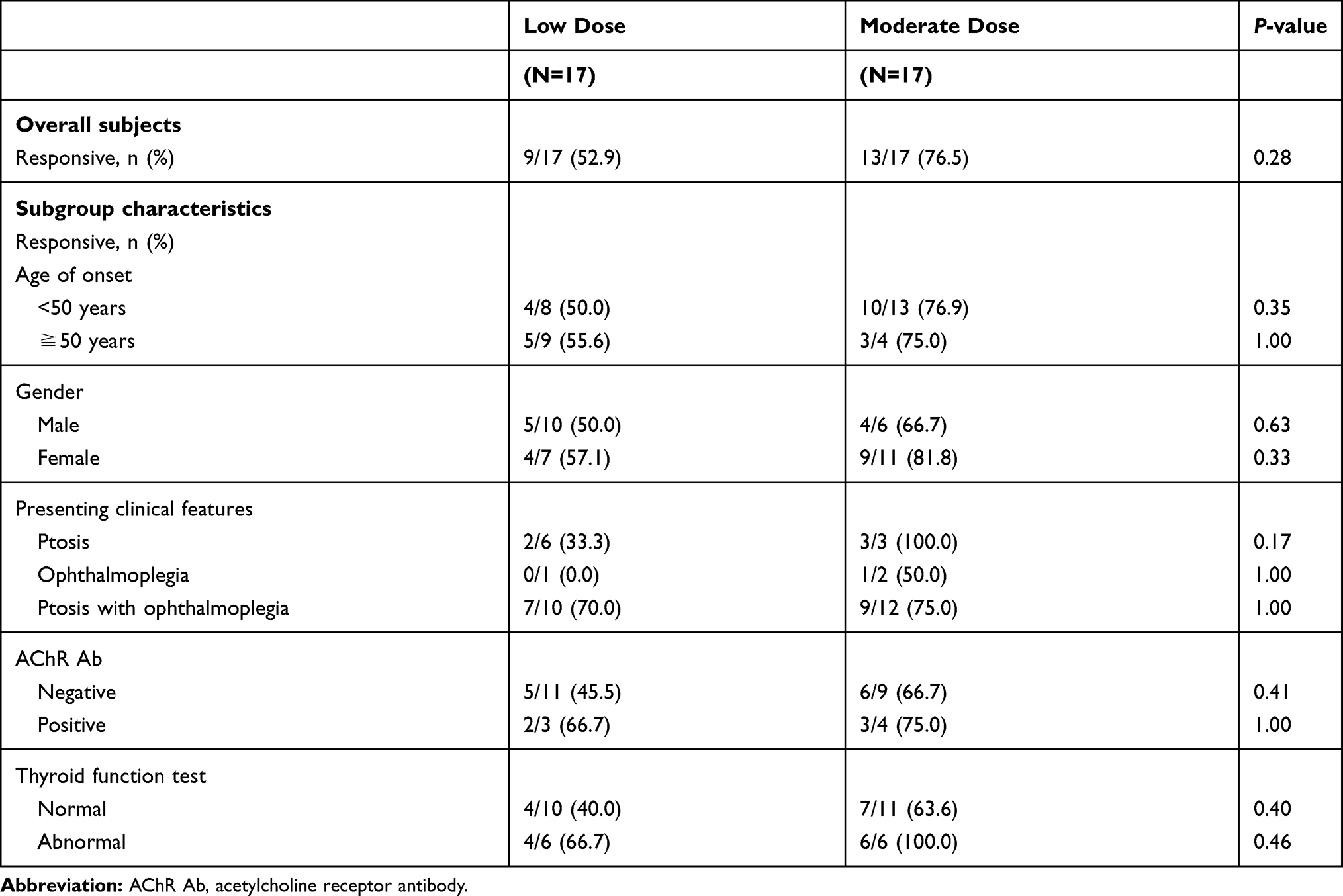 |
Table 3 Response Rates in Subjects Overall and Subgroup Characteristics Between Low-Dose and Moderate-Dose Groups |
Adverse events while on prednisolone therapy were documented in four subjects (23.5%) of the moderate-dose group, but none were reported in the low-dose group. The most common adverse event was insomnia (two subjects). The others were steroid-induced myopathy (one subject) and a skin abscess (one subject). No serious adverse events were observed in our study.
Discussion
This study was designed to shed light on the efficacy and safety of low-dose prednisolone for the treatment of patients with OMG who did not show adequate clinical improvement with symptomatic treatment (pyridostigmine). To our knowledge, this is the first study on OMG patients to perform a comparison between low-dose and moderate-dose prednisolone in terms of the initial treatment response at 12 weeks, before other immunosuppressants exert their therapeutic effects.
The primary outcome analysis showed that nine of 17 subjects (52.9%) and 13 of 17 subject (76.5%) achieved a responsive outcome in the low- and moderate-dose groups, respectively. Although the moderate-dose group showed a trend toward a higher responsive outcome, the difference did not reach the level of statistical significance (P=0.28). Subgroup analyses also lacked evidence to support a difference in responsive outcome between these two therapeutic groups among subgroups based on age of onset, gender, presenting clinical features, presence of AChR Ab and thyroid function test. These results suggest that low-dose prednisolone was comparable to the moderate dose, in terms of initial treatment response. Our study results demonstrated the efficacy of low-dose prednisolone in treating OMG, which is consistent with a prior study.10 The randomized controlled EPITOME trial, which compared low-dose prednisolone with placebo, also demonstrated the efficacy of low-dose prednisolone over 16 weeks (starting with a dose of 10 mg every other day, which increased to 10 mg/day, then 20 mg alternating with 10 mg, and finally the dose was adjusted to a maximum of 40 mg/day). Treatment failure was observed in only 17% of subjects in the low-dose group.10
Our secondary outcome was the collection of adverse events, which were exclusively found in the moderate-dose group; the adverse events included insomnia, steroid-induced myopathy and skin abscess. Consistent with the prior study, our results support the safety of low-dose prednisolone for OMG.12 Only minor adverse events were documented in our study. However, in patients taking prednisolone, specific monitoring measures should be in place to reduce the risks of severe adverse events, including worsening blood glucose level, excess weight gain, worsening blood pressure, upper gastrointestinal bleeding, osteoporosis, avascular necrosis of the hip joint and infectious disease.
The strengths of our study are as follows: 1) it was the first study to compare low and moderate doses of prednisolone for OMG in terms of initial treatment response (12 weeks); and 2) the doses of prednisolone in our study were calculated per body weight (kg), which should help in generalization to different populations, regardless of body weight.
This study had some limitations. First, our study design was a retrospective analysis, with variable clinical evaluations and investigation patterns, which resulted in missing data. For example, the type and severity of ophthalmoplegia were lacking, and only half of the subjects had SFEMG results, which limits the analysis of certain features. Second, because of the small number of subjects, our study may not have been adequately powered to detect differences in treatment response between treatment groups. With a larger study population, differences may have reached statistical significance. Third, our study did not focus on the time to treatment response during the 12 weeks. Fourth, the dosage of prednisolone was not determined prior to the initiation of treatment. Subjects in the moderate-dose group may have had treatment failure from low-dose prednisolone, and then, in order to achieve a responsive result, the dose of prednisolone may have been increased until the average cumulative dose reached the moderate-dose group range. Therefore, the proportion of subjects in the low-dose group with a responsive outcome may be lower than reported. The final drawback of our study was the variability of dosing regimens prescribed among the treating physicians. We addressed this by using an average 12-week cumulative dose to represent the total dosing regimens, for data collection and analysis.
Current treatment recommendations in OMG are generally based on low-level evidence guidelines from clinical experiences, expert opinions and consensus reports. Further prospective and randomized controlled studies to compare the efficacy of low-dose and moderate-dose prednisolone are encouraged, to confirm our results. These could lead to a new standard treatment guideline being established to address this disease with optimism, maximize therapeutic responses and minimize adverse events.
Conclusions
Treatment of OMG with an average 12-week cumulative dose of prednisolone <0.435 mg/kg/day (low dose) shows a comparable responsive outcome to 0.435–1.000 mg/kg/day of prednisolone (moderate dose). Treating OMG with low-dose prednisolone can minimize prednisolone-related adverse events. However, a prospective randomized controlled trial with a larger study population is warranted in order to gain more insight into the proper dosage of prednisolone for OMG.
Acknowledgment
We thank Claire Barnes, from Edanz Group, for editing a draft of this manuscript.
Disclosure
The authors report no conflicts of interest in this work. This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
References
1. Gilhus NE, Verschuuren JJ. Myasthenia gravis: subgroup classification and therapeutic strategies. Lancet Neurol. 2015;14(10):1023–1036. doi:10.1016/S1474-4422(15)00145-3
2. Meriggioli MN, Sanders DB. Autoimmune myasthenia gravis: emerging clinical and biological heterogeneity. Lancet Neurol. 2009;8(5):475–490. doi:10.1016/S1474-4422(09)70063-8
3. Gilhus NE. Myasthenia and the neuromuscular junction. Curr Opin Neurol. 2012;25(5):523–529. doi:10.1097/WCO.0b013e3283572588
4. Querol L, Illa I. Myasthenia and the neuromuscular junction. Curr Opin Neurol. 2013;26(5):459–465. doi:10.1097/WCO.0b013e328364c079
5. Verschuuren JJ, Huijbers MG, Plomp JJ, et al. Pathophysiology of myasthenia gravis with antibodies to the acetylcholine receptor, muscle-specific kinase and low-density lipoprotein receptor-related protein 4. Autoimmun Rev. 2013;12(9):918–923. doi:10.1016/j.autrev.2013.03.001
6. Nagia L, Lemos J, Abusamra K, Cornblath WT, Eggenberger ER. Prognosis of ocular myasthenia gravis: retrospective multicenter analysis. Ophthalmology. 2015;122(7):1517–1521. doi:10.1016/j.ophtha.2015.03.010
7. Skeie GO, Apostolski S, Evoli A, et al. Guidelines for treatment of autoimmune neuromuscular transmission disorders. Eur J Neurol. 2010;17(7):893–902. doi:10.1111/j.1468-1331.2010.03019.x
8. Benatar M, Kaminski H. Medical and surgical treatment for ocular myasthenia. Cochrane Database Syst Rev. 2006;2.
9. Kupersmith MJ. Ocular myasthenia gravis: treatment successes and failures in patients with long-term follow-up. J Neurol. 2009;256(8):1314–1320. doi:10.1007/s00415-009-5120-8
10. Benator M, McDermott MP, Sanders DB, et al. Efficacy of prednisone for the treatment of ocular myasthenia (EPITOME): a randomized, controlled trial. Muscle Nerve. 2016;53(3):363–369. doi:10.1002/mus.24769
11. Kim JH, Hwang JM, Hwang YS, Kim KJ, Chae J. Childhood ocular myasthenia gravis. Ophthalmology. 2003;110(7):1458–1462. doi:10.1016/S0161-6420(03)00460-3
12. Bruce BB, Kupersmith MJ. Safety of prednisone for ocular myasthenia gravis. J Neuroophthamol. 2012;32(3):212. doi:10.1097/WNO.0b013e3182536558
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.