Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Inhaler Adherence in COPD and Its Clinical and Contextual Associations: A Single-Center Cross-Sectional Study
Authors Bektaş Aksoy H ![]() , Günaydın S
, Günaydın S ![]() , Şimşek ŞM
, Şimşek ŞM ![]() , Takır S
, Takır S ![]()
Received 11 November 2025
Accepted for publication 21 February 2026
Published 3 March 2026 Volume 2026:21 580657
DOI https://doi.org/10.2147/COPD.S580657
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jill Ohar
Hayriye Bektaş Aksoy,1 Selda Günaydın,1 Şaban Melih Şimşek,1 Selçuk Takır2
1Giresun University Faculty of Medicine, Department of Chest Diseases, Giresun, Türkiye; 2Giresun University Faculty of Medicine, Department of Pharmacology, Giresun, Türkiye
Correspondence: Hayriye Bektaş Aksoy, Giresun University Faculty of Medicine, Department of Chest Diseases, Giresun, Türkiye, Email [email protected]
Purpose: Effective management of chronic obstructive pulmonary disease (COPD) depends on sustained adherence to inhaled therapies, yet real-world factors associated with inhaler adherence and disease awareness are not fully characterized. This study aimed to evaluate inhaler medication adherence among patients with COPD and to explore its associations with sociodemographic, clinical, and contextual factors, including self-reported disease awareness.
Patients and Methods: This single-center, cross-sectional descriptive study was conducted between July and October 2025 in the Chest Diseases Outpatient Clinic of a tertiary hospital. Patients aged ≥ 18 years with a confirmed diagnosis of COPD based on GOLD 2025 criteria were included. Sociodemographic and clinical data were collected using structured, interviewer-administered questionnaires. Inhaler adherence was assessed using a structured questionnaire adapted from the Test of Adherence to Inhalers (TAI). Symptom burden and dyspnea were evaluated using the COPD Assessment Test (CAT) and the modified Medical Research Council (mMRC) dyspnea scale, respectively. Statistical analyses were performed using IBM SPSS Statistics version 23.0, with a two-sided p value < 0.05 considered statistically significant.
Results: A total of 170 patients were included in the analysis (GOLD group A: 31.2%, group B: 44.1%, and group E: 24.7%). Marital status (p = 0.003), family history of COPD (p< 0.001), and home use of nebulizers or oxygen concentrators (p< 0.001) were significantly associated with higher inhaler adherence, whereas age, educational level, income status, and smoking status were not. TAI adherence scores did not differ significantly across GOLD groups (p> 0.05), whereas exacerbation frequency and hospitalization rates increased significantly with disease severity (p< 0.001).
Conclusion: In this single-center cross-sectional study, inhaler adherence in patients with COPD was found to be associated with contextual and social factors, such as marital status, family history of COPD, and home use of respiratory support devices, rather than with demographic characteristics or disease severity. These findings highlight the importance of routinely assessing inhaler use and adherence in clinical practice and suggest that contextual factors may play a role in adherence behaviors, in line with current GOLD recommendations.
Keywords: chronic obstructive pulmonary disease, disease awareness, inhaler adherence, TAI
Introduction
Chronic obstructive pulmonary disease (COPD) is a preventable and treatable condition characterized by persistent respiratory symptoms and airflow limitation resulting from airway and/or alveolar abnormalities, typically caused by prolonged exposure to harmful particles or gases.1 According to the World Health Organization, COPD remains one of the leading causes of morbidity and mortality worldwide, accounting for more than three million deaths annually. Despite advances in diagnostic methods and pharmacotherapy, insufficient patient awareness and poor adherence to prescribed inhaler regimens continue to significantly compromise disease control, resulting in more frequent exacerbations and hospital admissions.2
Pharmacologic therapy with inhaled bronchodilators and corticosteroids remains the cornerstone of COPD management, and its effectiveness depends largely on correct inhaler use and long-term adherence.3,4 Recent evidence suggests that poor adherence is strongly associated with greater disease severity, more frequent exacerbations, and higher healthcare utilization.5 Consequently, ensuring proper inhaler technique and regular adherence monitoring has become an essential part of comprehensive COPD management.
Behavioral and psychosocial determinants (including disease perception, health literacy, and patient–provider communication) play a crucial role in maintaining treatment continuity.6 Patients’ perceptions of COPD as a chronic condition may influence how they engage with long-term inhaler therapy; however, in observational studies, such perceptions are typically assessed indirectly and should be interpreted with caution. Furthermore, the type and number of inhalers affect adherence; simplified single-inhaler triple therapy regimens have been associated with improved adherence and persistence compared with multiple-inhaler combinations.3,4
The 2025 Global Initiative for Chronic Obstructive Lung Disease (GOLD) report underscores the importance of routinely assessing inhaler technique and providing patient education at every follow-up visit. It also recommends verifying both adherence and technique before intensifying pharmacologic therapy, emphasizing that treatment failure often stems from behavioral rather than pharmacologic causes.1
Most available studies have focused on hospital-based cohorts or clinical trial settings, which may not accurately reflect the challenges encountered in everyday clinical practice, particularly within single-center outpatient settings. Furthermore, differences in socioeconomic status, family support, and cultural attitudes toward chronic illness may influence treatment behaviors in diverse ways across regions.5,7
In this context, the present study aims to evaluate inhaler medication adherence among patients with COPD in a tertiary care outpatient setting. It also explores the associations between inhaler adherence and selected sociodemographic, clinical, and contextual factors, including patients’ self-reported understanding of their disease, as well as disease severity, exacerbation history, and inhaler type. By integrating patient-reported outcomes with clinical data, this study seeks to strengthen the evidence supporting continuous patient education, individualized inhaler selection, and simplified treatment strategies to optimize long-term COPD management.
Materials and Methods
Study Design and Setting
This cross-sectional, descriptive study was conducted in the Chest Diseases Outpatient Clinic of a tertiary care hospital between July 1 and October 31, 2025. Patients were classified according to GOLD A, B, and E groups. Patient classification was performed according to the GOLD 2025 framework, which was the guideline in effect at the time of study design and data collection. The primary objective was to assess inhaler medication adherence and disease awareness among patients diagnosed with COPD. Secondary outcomes included symptom burden assessed by the COPD Assessment Test (CAT), dyspnea severity evaluated using the modified Medical Research Council (mMRC) scale, and the frequency of exacerbations and hospitalizations. Inhaler adherence was considered the primary outcome of the study, whereas variables related to patients’ knowledge and awareness of COPD were explored descriptively as contextual factors rather than as independent outcomes.
The study protocol was reviewed and approved by the Institutional Ethics Committee (Approval No: BAEK-337; Decision Date: May 28, 2025; Protocol No: 2025/07). All participants were provided with detailed information regarding the study procedures and objectives, and written informed consent was obtained prior to enrollment, in accordance with the ethical principles of the Declaration of Helsinki.
Study Population
The study population included adult patients (≥18 years) who had been diagnosed with COPD by a specialist physician according to the GOLD 2025 criteria and who attended the Chest Diseases Outpatient Clinic during the study period. Inclusion criteria were as follows: age 18 years or older, a confirmed diagnosis of COPD by a specialist, adequate motor function in at least one upper extremity sufficient for inhaler use, voluntary participation with written informed consent, and cognitive ability to understand and appropriately respond to the questionnaire. Exclusion criteria were pregnancy, absence or uncertainty of COPD diagnosis, incorrect or invalid COPD diagnosis, upper extremity paralysis preventing inhaler use, presence of an acute infectious pathology (except mild upper or lower respiratory tract infections), and cognitive or psychiatric impairment that interfered with comprehension of the questionnaire.
Grouping According to GOLD 2025
Patients were classified into three groups based on the GOLD 2025 criteria, which integrate symptom severity and exacerbation risk:
Accordingly, patients were analyzed in three groups.
Data Collection
Sociodemographic data (including age, sex, marital status, education level, income, smoking history, heating method, biomass exposure, and comorbidities) were collected using a structured questionnaire. Clinical information included COPD duration, GOLD stage, number and timing of exacerbations, and the use of home oxygen concentrators or nebulized medications.
Inhaler adherence was evaluated using a structured questionnaire adapted from the Test of Adherence to Inhalers (TAI). The questionnaire consisted of 12 items assessing regular use of inhaler medication, correct dosing, knowledge of inhaler technique, forgetfulness, difficulties during use or transport, motivation, side effects, prior training on inhaler use, and adherence to physician recommendations. Each item was scored as 1 point for “yes (always/regularly)”, 0.5 points for “sometimes”, and 0 points for “no (never)”. The total adherence score ranged from 0 to 12, with higher scores indicating better inhaler adherence. Based on the total score, patients were categorized as having high adherence (10–12 points), moderate adherence (7–9 points), or low adherence (0–6 points). All questionnaires and clinical scales were administered through face-to-face interviews conducted by trained healthcare personnel under the supervision of a pulmonologist.
The COPD Assessment Test (CAT) and the Modified Medical Research Council (mMRC) scale were also employed to assess symptom burden and dyspnea severity, respectively. Disease awareness was not assessed as a primary or validated outcome. Instead, patients’ self-reported understanding of their diagnosis and treatment was descriptively recorded during routine outpatient interviews, without the use of a standardized or validated disease-awareness scale. Although the original TAI is a validated instrument, the adapted scoring approach used in this study has not been formally validated and was therefore applied for exploratory and descriptive purposes.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics version 23.0 (IBM Corp., Armonk, NY, USA). The normality of quantitative variables was assessed using the Kolmogorov–Smirnov test. The Mann–Whitney U and Kruskal–Wallis tests were applied for comparisons of non-normally distributed variables, whereas the Independent Samples t-test and one-way ANOVA were used for normally distributed variables. The Chi-square test was used to analyze categorical data. Descriptive data were expressed as numbers and percentages n (%), mean ± standard deviation, or median (minimum–maximum), as appropriate. Logistic regression analyses were performed to identify factors associated with moderate-to-high inhaler adherence. Adherence was dichotomized based on the total adherence score, with scores ≥7 indicating moderate-to-high adherence and scores ≤6 indicating low adherence. Results were reported as odds ratios (ORs) with 95% confidence intervals. A p-value of <0.05 was considered statistically significant.
Results
A total of 170 patients were enrolled, including 53 (31.2%) in GOLD Stage A, 75 (44.1%) in Stage B, and 42 (24.7%) in Stage E. Although age distribution did not differ significantly (p=0.481), the proportion of patients aged ≥ 80 years was higher in Stage E. Male predominance was evident in all groups (p=0.417). Educational attainment and income level were similar (p>0.05). Marital status differed significantly (p=0.003); while most patients in Stages A and B were married (84.9% and 89.3%), this rate declined to 64.3% in Stage E. Biomass exposure was more frequent in Stages B and E, though not statistically significant (p=0.226). Smoking prevalence and duration were comparable across stages (p=0.252 and 0.570). Comorbidities were common in all groups (p=0.873) (Table 1).
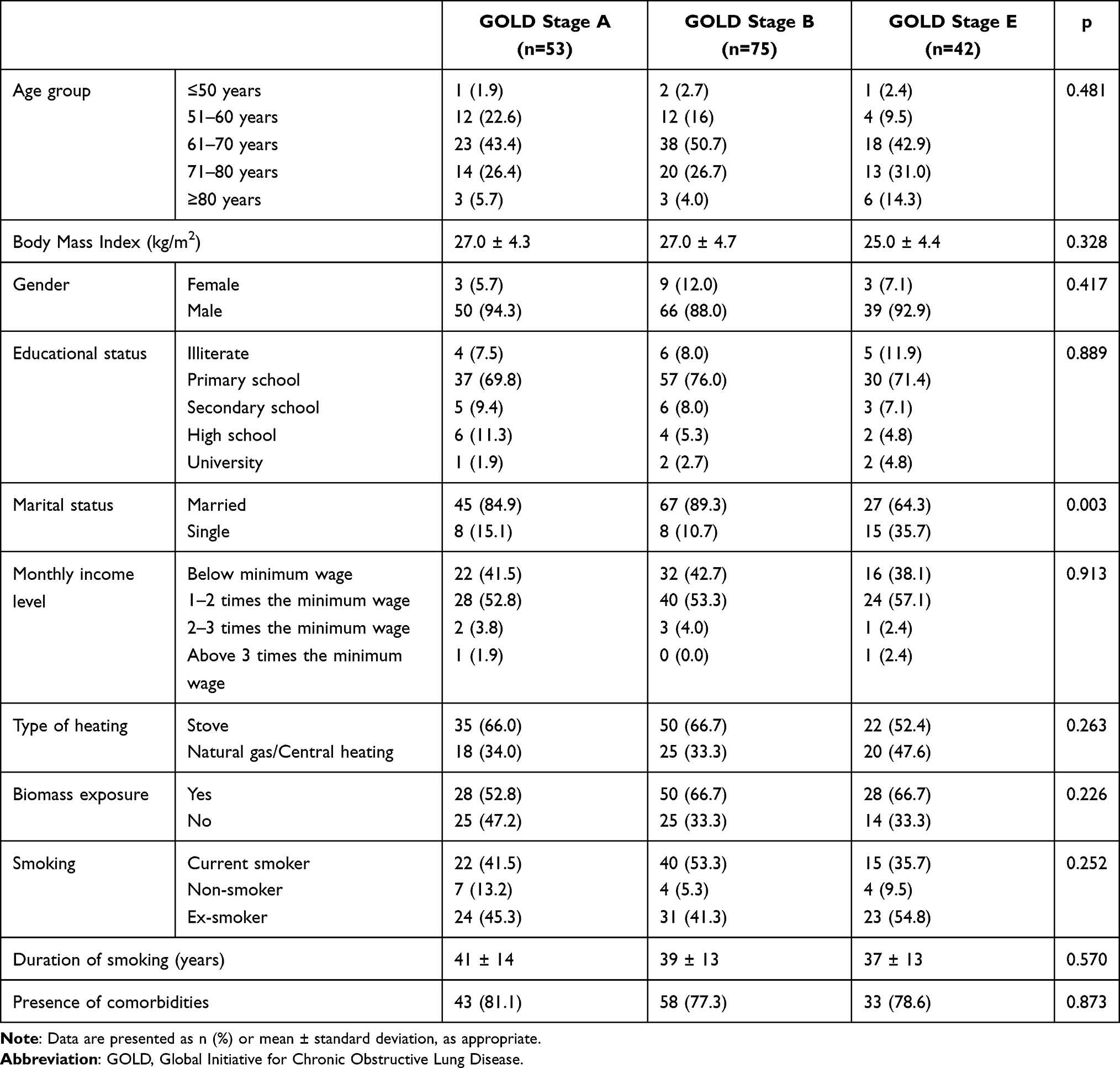 |
Table 1 Demographic and Sociodemographic Characteristics of the Study Population |
The duration of COPD diagnosis and inhaler use showed no difference among stages (p=0.188 and 0.479). Nearly all patients had received inhaler education (p=0.080). The use of SABA/SAMA combinations increased with disease severity (p=0.004), and triple therapy with ICS/LABA/LAMA was more frequent in Stage E (p=0.042). Nebulized medication (p<0.001) and oxygen device use (p=0.046) also rose markedly in advanced stages. A family history of COPD was significantly more common in Stage E (p<0.001). Symptom burden increased steadily; both mMRC and CAT scores were highest in Stage E (p<0.001). In contrast, medication adherence measured by TAI did not differ (p=0.155). When inhaler adherence was categorized into low, moderate, and high adherence groups, no significant differences were observed across GOLD stages (p = 0.316) (Table 2).
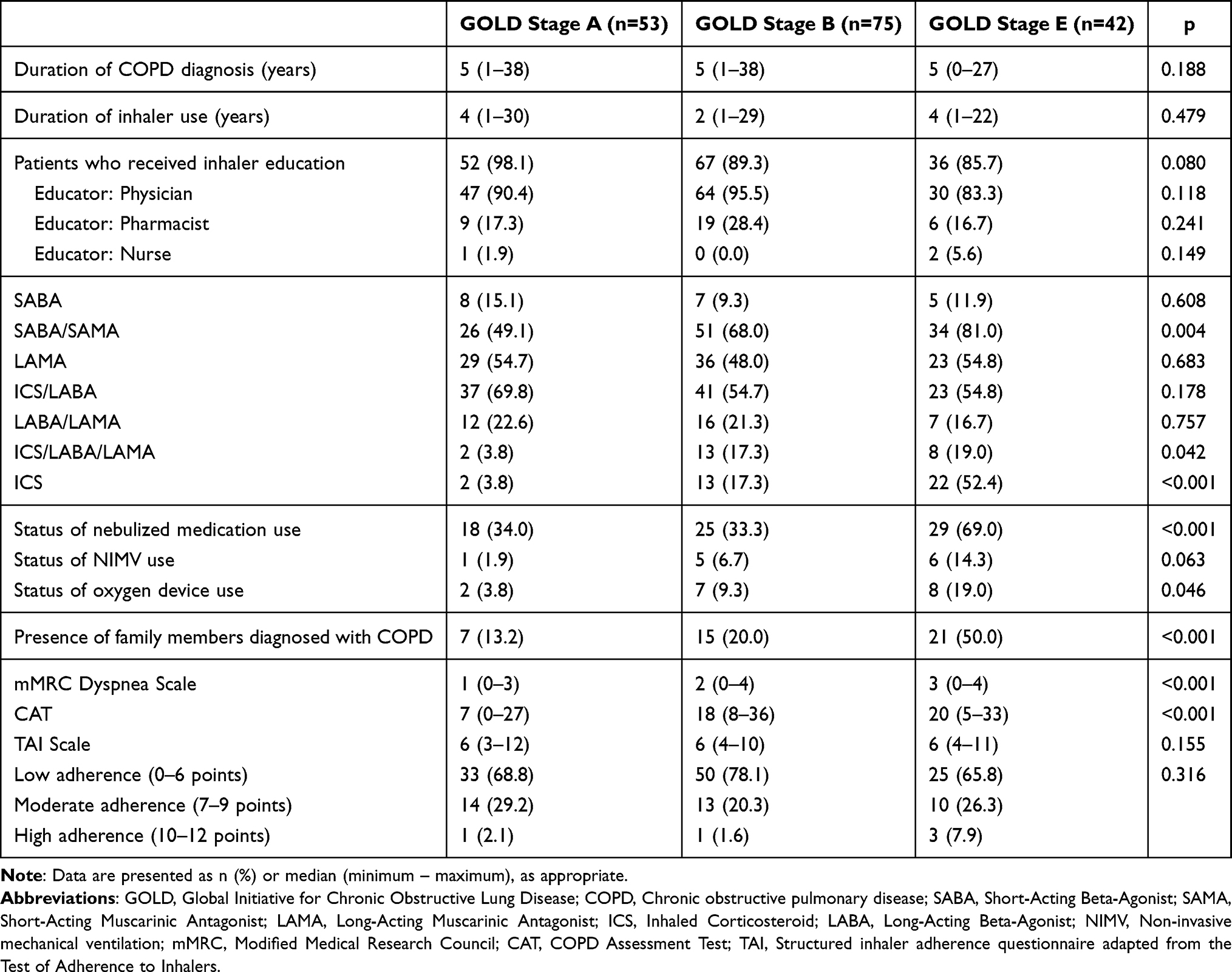 |
Table 2 Clinical Features, Treatment Regimens, Home Device Use and Comparison of mMRC/ CAT/TAI Scores Across GOLD Stages |
During the preceding year, 28.3% of Stage A, 65.3% of Stage B, and 92.9% of Stage E patients reported at least one physician visit for an exacerbation (p<0.001). Multiple visits were significantly more frequent in advanced stages (p<0.001). Hospitalization rates increased sharply from 5.7% in Stage A and 2.7% in Stage B to 61.9% in Stage E (p<0.001). Recurrent admissions occurred exclusively in Stage E (26.2%; p<0.001). The intervals since the last exacerbation also differed (p<0.001): 15.1% of Stage A, 34.7% of Stage B, and 40.4% of Stage E patients experienced an episode within the past month, whereas 58.5% of Stage A but only 2.4% of Stage E patients had remained exacerbation-free for over a year (Table 3).
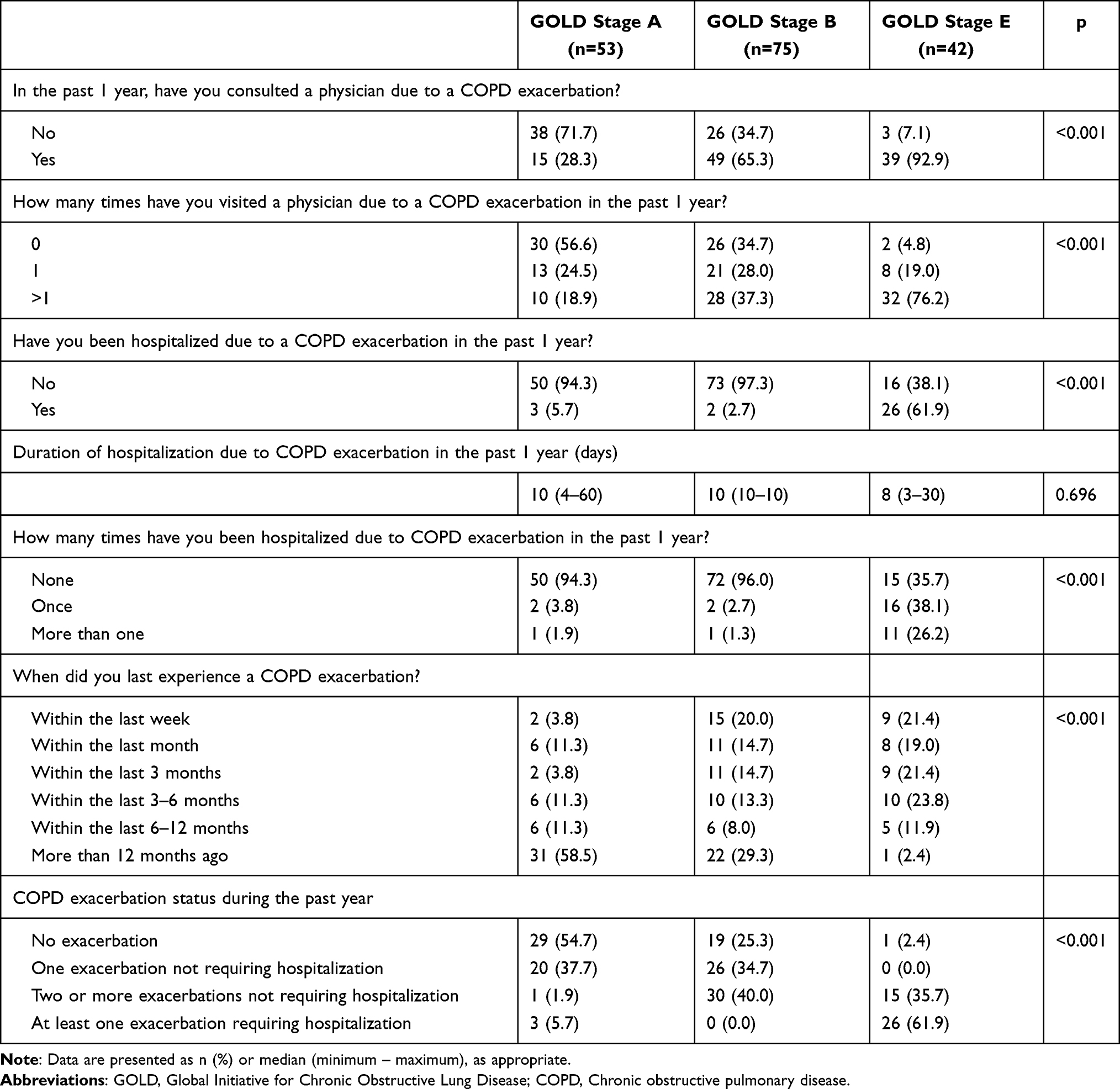 |
Table 3 Exacerbation Frequency, Hospitalizations, and Disease Severity by GOLD 2025 Classification |
Self-reported knowledge of COPD was similar across groups (p=0.531), with about 45% in each group describing their knowledge as moderate. Healthcare professionals were the main source of information in all stages (Table 4). Comparison of the COPD Knowledge Level questionnaire revealed no significant difference between groups (p>0.05) (Table 5).
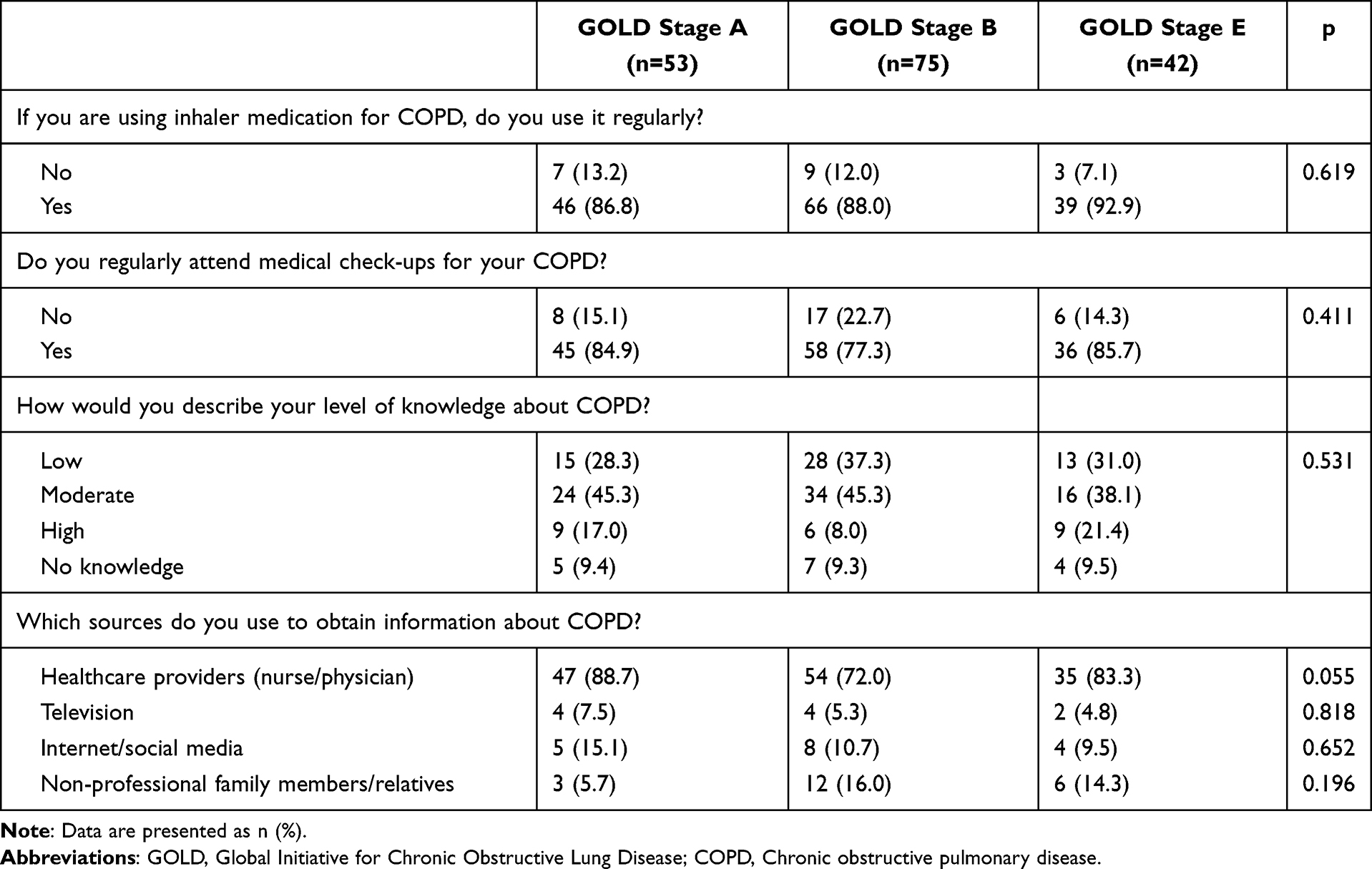 |
Table 4 Inhaler Use Patterns, Education on Device Technique, Level of Knowledge About COPD and Information Sources About COPD |
 |
Table 5 Patient Awareness and Knowledge About COPD and Treatment Across GOLD Stages |
In univariate logistic regression analysis, none of the evaluated sociodemographic, clinical, or treatment-related variables were significantly associated with moderate-to-high inhaler adherence (TAI ≥7). Age group, gender, marital status, educational status, smoking status, GOLD stage, use of nebulized medication, non-invasive mechanical ventilation or oxygen devices, family history of COPD, inhaler regimen (ICS/LABA/LAMA), CAT score, and mMRC dyspnea scale all showed no statistically significant associations with adherence (all p>0.05). Similarly, in multivariate logistic regression analysis, none of these variables remained independently associated with moderate-to-high inhaler adherence (Table 6). Notably, the absence of statistically significant independent predictors in both univariate and multivariate analyses indicates that inhaler adherence in this cohort could not be explained by any single sociodemographic, clinical, or treatment-related variable.
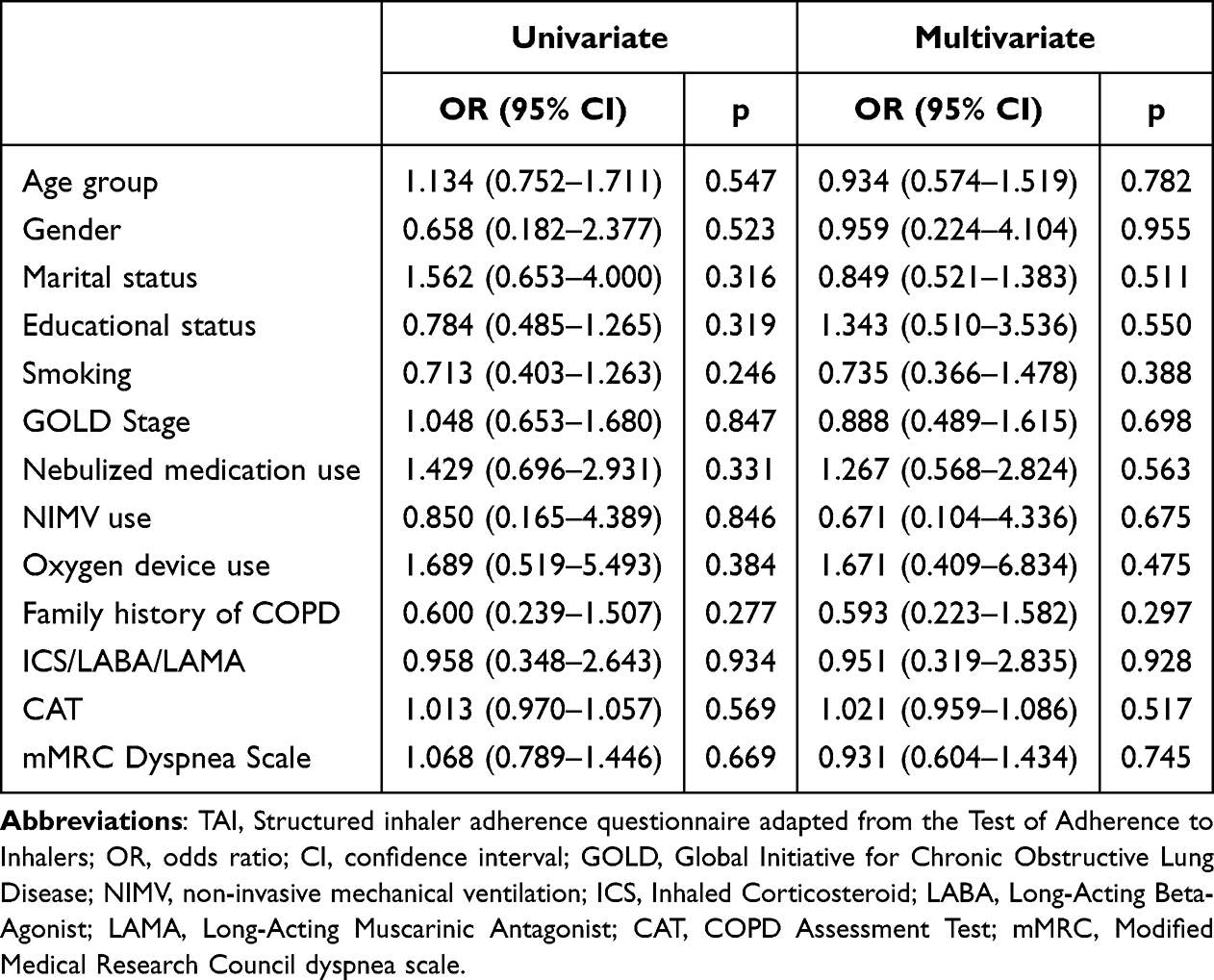 |
Table 6 Univariate and Multivariate Logistic Regression Analyses of Factors Associated with Moderate-to-High Inhaler Adherence (TAI ≥7) |
Discussion
Our findings showed that several commonly assumed predictors of inhaler adherence, including age, educational level, income status, smoking behavior, and environmental exposure, were not significantly associated with adherence in univariate analyses. Although certain contextual and social variables (such as marital status, having a family member with COPD, and home use of nebulizers or oxygen concentrators) showed associations with adherence at the descriptive or univariate level, none of these factors remained independently associated with adherence in multivariate analysis. This finding suggests that inhaler adherence in COPD is shaped by a multifactorial and largely behavior-driven structure, in which isolated sociodemographic or clinical variables have limited independent explanatory value. Rather than reflecting methodological inadequacy, the absence of independent predictors likely mirrors the complex interplay of patient behavior, treatment context, and healthcare engagement observed in real-world COPD populations.6,8
Similar findings have been reported in recent real-world COPD studies, where inhaler adherence was shown to reflect a complex interaction of behavioral, contextual, and healthcare-related factors rather than being driven by single clinical or sociodemographic variables.9 Similarly, a large cross-sectional study from northern China involving 977 COPD patients reported an adherence rate of approximately 40%, which was primarily associated with family support and regular follow-up rather than sociodemographic characteristics.8 Comparable results were reported in a Turkish study emphasizing the importance of device simplicity, repeated education, and healthcare professional support over income or educational status.7 These observations suggest that such variables may function as indirect markers or proxies of patients’ engagement with care and treatment routines, rather than as direct or independent determinants of inhaler adherence. This multifactorial structure of adherence has also been highlighted in recent modeling studies, which demonstrate that no single variable adequately explains adherence behavior in COPD populations.10 In line with this interpretation, previous studies have shown that patients’ understanding and perception of their disease are associated with better adherence, primarily through enhanced engagement with treatment rather than as independent determinants of behavior.11
In a 12-month real-world cohort of treatment-naïve COPD patients, those who accurately recognized the nature of the disease and understood its chronic, progressive course demonstrated significantly higher TAI scores and greater treatment persistence.6 In our cohort, the positive associations between having a family member with COPD and being married likely reflect the reinforcing role of familial observation and social interaction in enhancing disease awareness. Consistently, multivariate analysis did not identify any independent clinical or demographic predictors of inhaler adherence, underscoring the multifactorial and behavior-driven nature of adherence in COPD.
Although mMRC dyspnea and CAT scores increased with advancing disease severity, adherence measures assessed by TAI did not show significant stage-dependent variation in our cohort. Previous real-world studies have reported that treatment simplification, particularly through single-inhaler triple therapy, has been associated with improved adherence and persistence compared with multiple-inhaler regimens.3,4,12–14 These findings suggest that treatment-related factors, such as regimen simplicity and inhaler usability, may influence adherence behaviors independently of clinical severity. However, as the present study did not evaluate treatment modifications or longitudinal outcomes, these observations should be interpreted in the context of existing literature rather than as causal evidence. Accordingly, contemporary adherence frameworks emphasize that meaningful and sustained improvements are most often achieved through multicomponent approaches addressing treatment complexity, patient behavior, and healthcare delivery simultaneously.15 While treatment simplification strategies, such as single-inhaler regimens, have been associated with improved adherence in prior studies, the present analysis did not specifically evaluate treatment modifications and therefore focuses on broader, non–treatment-specific determinants of adherence.
In a Korean study, misuse of soft-mist inhalers was reported in more than 58% of patients and was significantly linked to older age, lower education, and reduced handgrip strength.16 Kocks et al found that critical inhaler errors were associated with poorer health status and increased exacerbation rates rather than sociodemographic characteristics, while Ng et al reported that over 80% of patients made at least one inhaler error, which was mitigated through nurse-led interventions.17,18 In parallel, Calle Rubio et al showed that, in routine clinical practice, a high prevalence of inhaler misuse before hospital admission was strongly correlated with poor adherence and disease control.19 Together, these results underscore that inhaler misuse and technique errors are widespread and emphasize the need for continuous patient education and regular assessment of inhaler technique. Recent evidence further indicates that even when self-reported adherence appears acceptable, deterioration of inhaler technique over time may substantially limit clinical benefit, highlighting the importance of repeated technique assessment beyond adherence measures alone.20
In our cohort, the number and timing of COPD exacerbations differed significantly across GOLD stages, consistent with previous evidence reporting an association between poor adherence and higher exacerbation frequency. A recent systematic review and meta-analysis reported that poor inhaler adherence increases exacerbation risk by nearly 40%.2 Similarly, Ballal et al found that poor adherence was significantly associated with more frequent hospital visits and exacerbations.5
The GOLD 2025 report emphasizes that in patients with COPD who show a suboptimal response to treatment, inhaler technique, adherence, and comorbidity burden should be reassessed before pharmacologic escalation.1 In this context, the present findings are consistent with current GOLD recommendations, highlighting the importance of routine adherence assessment and patient-centered follow-up in clinical practice. However, given the cross-sectional design of the study, these observations should be interpreted as supportive rather than confirmatory. Consistent with this perspective, prior studies have shown that the impact of educational interventions on inhaler adherence is heterogeneous and influenced by patient characteristics and healthcare context rather than uniformly effective across all COPD populations.21
Limitations
This study has several limitations that should be acknowledged. First, it was conducted in a single tertiary care center, which may limit the generalizability of the findings to broader COPD populations or primary care settings. Second, inhaler adherence was assessed using a questionnaire adapted from the TAI framework with a simplified scoring system, which has not been formally validated; therefore, the findings related to adherence should be interpreted with caution. Third, although multivariable analyses were performed, no independent predictors of moderate-to-high inhaler adherence were identified, which may reflect the multifactorial and behavior-driven nature of adherence in real-world COPD populations. Fourth, the cross-sectional design precludes causal inference; thus, associations between adherence and clinical outcomes (such as exacerbation frequency) should be interpreted cautiously. Fifth, disease awareness was assessed based on patients’ self-reported understanding without the use of a standardized or validated awareness scale, which may have limited the precision of this construct. Finally, the study did not systematically assess the quality or frequency of prior inhaler education, nor did it include data on cognitive function or psychological status, all of which may influence adherence behaviors. Despite these limitations, the study provides real-world insights into the contextual and behavioral factors associated with inhaler adherence in patients with COPD and highlights the importance of routine adherence assessment in clinical practice.
Conclusion
In this single-center cross-sectional study, inhaler adherence among patients with COPD appeared to be more closely related to contextual and social factors (such as marital status, family history of COPD, and home use of respiratory support devices) than to traditional sociodemographic or disease severity indicators. While age, education, income level, and smoking status were not significantly associated with adherence, the observed patterns suggest that patients’ engagement with treatment and care routines may be influenced by broader contextual factors rather than by clinical severity alone. Although inhaler adherence did not differ significantly across disease stages, exacerbation frequency increased with advancing severity, underscoring the importance of regular adherence assessment in clinical practice. In line with current GOLD recommendations, routine evaluation of inhaler technique, individualized patient education, and consideration of simplified treatment regimens should be integrated into COPD management, while acknowledging that causal inferences cannot be drawn from the present study.
Ethics Approval
The application numbered BAEK-337 for the study titled “Inhaler Medication Adherence and Disease Awareness in COPD Patients: A Single-Center Study” was evaluated by Giresun Training and Research Hospital Scientific Research Ethics Committee in terms of compliance with ethical principles and rules at the meeting dated 28.05.2025; it was deemed appropriate by the unanimous vote of the members attending the meeting and approved with the decision number 28.05.2025/07. All participants provided written informed consent before enrollment in the study.
Acknowledgment
The authors would like to thank all the patients who participated in this study and the clinical staff of the Department of Chest Diseases for their valuable assistance and cooperation throughout the data collection process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no conflicts of interest related to this study.
References
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease; 2015.
2. Vauterin D, Van Vaerenbergh F, Grymonprez M, Vanoverschelde A, Lahousse L. Medication adherence to inhalation therapy and the risk of COPD exacerbations: a systematic review with meta-analysis. BMJ Open Respir Res. 2024;11(1):e001964. doi:10.1136/bmjresp-2023-001964
3. Cuperus LJA, van der Palen J, Aldenkamp A, et al. Adherence to single inhaler triple therapy and digital inhalers in Chronic Obstructive Pulmonary Disease: a literature review and protocol for a randomized controlled trial (TRICOLON study). BMC Pulm Med. 2024;24(1):317. doi:10.1186/s12890-024-03044-3
4. Jokšaitė S, Wood R, Ismaila A, et al. Comparative adherence and persistence of single-inhaler and multiple-inhaler triple therapies among patients with chronic obstructive pulmonary disease in Japan: a retrospective cohort study. BMJ Open. 2024;14(12):e080864. doi:10.1136/bmjopen-2023-080864
5. Ballal P, Katipalla A, Srinivas S, Dhanusha S, Pujar P, Sudeesh S. Impact of patient compliance with inhaler therapy on chronic obstructive pulmonary disease severity: a rural tertiary care perspective. Egypt J Intern Med. 2025;37(1):1–11.
6. Garcia-Pachon E, Grau-Delgado J, Baeza-Martínez C, Zamora-Molina L, Galán-Negrillo M, Beléndez-Vázquez M. Patients’ beliefs about medicines and adherence to inhalers. Open Respir Archiv. 2024;6(2):100322. doi:10.1016/j.opresp.2024.100322
7. Özdemir ST, Yeşilbalkan ÖU, Akyol A. Adherence to inhaler therapy in patients with chronic obstructive pulmonary disease and contributing factors. Profess Stud. 2024;28(2):21–28.
8. Liu L, Xiao J, Yu S. A survey and analysis of inhalation medication adherence among 977 COPD patients in a region of northern China. Eur J Med Res. 2025;30(1):258. doi:10.1186/s40001-025-02535-1
9. Turegano-Yedro M, Trillo-Calvo E, Navarro IRF, et al. Inhaler adherence in COPD: a crucial step towards the correct treatment. Int J Chron Obstruct Pulmon Dis. 2023;18:2887–2893. doi:10.2147/COPD.S431829
10. Liu Y-R, Wang Y, Chen J, et al. Developing and validating a nomogram for non-adherence to inhaler therapy among elderly chronic obstructive pulmonary disease patients based on the social ecological model. Patient Prefer Adherence. 2024;18:1741–1753. doi:10.2147/PPA.S472625
11. Lopez-Pintor E, Grau J, Lumbreras B. Patient’s awareness on COPD is the strongest predictor of persistence and adherence in treatment-naïve patients in real life: a prospective cohort study. BMC Pulm Med. 2021;21(1):388. doi:10.1186/s12890-021-01754-6
12. Mannino D, Bogart M, Wu B, et al. Adherence and persistence to once-daily single-inhaler versus multiple-inhaler triple therapy among patients with chronic obstructive pulmonary disease in the USA: a real-world study. Respir Med. 2022;197:106807. doi:10.1016/j.rmed.2022.106807
13. Lin L, Liu C, Cheng W, et al. Comparison of treatment persistence, adherence, and risk of exacerbation in patients with COPD treated with single-inhaler versus multiple-inhaler triple therapy: a prospective observational study in China. Front Pharmacol. 2023;14:1147985. doi:10.3389/fphar.2023.1147985
14. Requena G, Camidge LJ, Ford A, et al. Effectiveness of switching from multiple-inhaler to once-daily single-inhaler triple therapy in patients with COPD in a real-world setting in Japan. Int J Chron Obstruct Pulmon Dis. 2025;20:565–580. doi:10.2147/COPD.S478455
15. van de Hei SJ, Dierick BJH, Aarts JEP, Kocks JWH, van Boven JFM. Personalized medication adherence management in asthma and chronic obstructive pulmonary disease: a review of effective interventions and development of a practical adherence toolkit. J Allergy Clin Immunol Pract. 2021;9(11):3979–3994. doi:10.1016/j.jaip.2021.05.025
16. Jang JG, Lee YS, Hong KS, Ahn JH. Risk factors associated with misuse of soft mist inhaler in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2024;19:1225–1232. doi:10.2147/COPD.S458200
17. Kocks J, Bosnic-Anticevich S, van Cooten J, et al. Identifying critical inhalation technique errors in Dry Powder Inhaler use in patients with COPD based on the association with health status and exacerbations: findings from the multi-country cross-sectional observational PIFotal study. BMC Pulm Med. 2023;23(1):302. doi:10.1186/s12890-023-02566-6
18. Ng S-W, Lit MP, Lai AY. Nurses’ reports of inhaler use errors in patients with chronic obstructive pulmonary disease in Hong Kong. Int J Chron Obstruct Pulmon Dis. 2024;Volume 19:2775–2785. doi:10.2147/COPD.S482243
19. Calle Rubio M, Adami Teppa PJ, Rodríguez Hermosa JL, et al. Insights from real-world evidence on the use of inhalers in clinical practice. J Clin Med. 2025;14(4):1217. doi:10.3390/jcm14041217
20. Bosnic-Anticevich S, Bender BG, Shuler MT, Hess M, Kocks JWH. Recognizing and tackling inhaler technique decay in asthma and Chronic Obstructive Pulmonary Disesase (COPD) clinical practice. J Allergy Clin Immunol Pract. 2023;11(8):2355–2364e5. doi:10.1016/j.jaip.2023.04.031
21. Sanchez-Nieto JM, Bernabeu-Mora R, Fernandez-Munoz I, et al. Effectiveness of individualized inhaler technique training on low adherence (LowAd) in ambulatory patients with COPD and asthma. NPJ Prim Care Respir Med. 2022;32(1):1. doi:10.1038/s41533-021-00262-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.