")
Back to Journals » Patient Preference and Adherence » Volume 17
Inhalation Devices in 7- to 15-Year-Old Children with Asthma - A Patient Preference Study
Authors Tietz F, Adams I, Lücke E, Schreiber J
Received 20 July 2022
Accepted for publication 11 January 2023
Published 4 April 2023 Volume 2023:17 Pages 951—959
DOI https://doi.org/10.2147/PPA.S381486
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Qizhi (Cathy) Yao
Franziska Tietz,1 Ines Adams,2 Eva Lücke,1,* Jens Schreiber1,*
1Department of Pneumonology, University Medicine, Magdeburg, Germany; 2Department of Pediatrics, University Medicine, Magdeburg, Germany
*These authors contributed equally to this work
Correspondence: Jens Schreiber, Department of Pneumology, University Medicine Magdeburg, Leipziger Straße 44, Magdeburg, 39120, Germany, Tel +49 391 67 15421, Fax +49 391 67 13356, Email [email protected]
Background: Inhalation therapy is the cornerstone of treatment of bronchial asthma. A patient-specific selection of inhalation devices is necessary, as preference for a device plays an important role in terms of error rates in handling and adherence to therapy. However, there is no industry-independent study providing information on children’s preferences for common inhaler types. The aim of the present study was to investigate the preference of asthmatic children for inhaler types commonly used in Germany. The effects of age, gender and the type of school visited on device preferences as well as the frequency of patient education and the role of health care providers in the choice for an inhaler were investigated.
Methods: Eighty children were included in this prospective cross-sectional study (age: 10.87 ± 2.62 years). The analysis was based on a questionnaire and validated checklists. All participants tested the use of nine placebo inhalers (Breezhaler, Diskus, Respimat, Spiromax, Turbohaler, Autohaler, metered-dose inhaler, Easyhaler and Novolizer) in a randomized order. For each device, patients were asked to assess handling, rate different device characteristics and name the device they would prefer most or least.
Results: The most favored device was the Novolizer. Moreover, the Spiromax scored highest in numerous categories such as suitability in emergencies and “easiest” device to use. Patient preferences with respect to the addressed inhaler features were not significantly related to age, gender or school type.
Conclusion: The Novolizer and the Spiromax showed higher preference in pediatric patients as compared to other tested devices. Overall, there were significant differences in terms of preference when comparing the tested inhalers in different aspects.
Keywords: childhood asthma, inhaler devices, patient preferences, inhaler technique
Introduction
Asthma affects more than 339 million people worldwide and is the most common chronic disease in childhood.1 Drug therapy is mainly carried out using inhalers.2 Here, especially with respect to children, a disadvantage is that correct inhaler use requires intense training and that the different types of devices available significantly differ in their handling. An additional complication is that many of the inhalers were developed for adults and are difficult to handle for children in terms of their physical and cognitive abilities.3 Therefore, not every inhaler system is suitable for every child and the devices should be selected on a patient-individual basis.
These factors are frequently inadequately considered, certainly contributing to high error rates in the correct inhaler use in childhood. Error rates range from 45% to over 90%, and up to 55% of pediatric asthma patients therefore suffer from uncontrolled asthma.4–7 Poor inhaler technique not only leads to inadequate drug efficacy and side effects, but also has a significant impact on treatment adherence.8,9
Although these complications have existed for years, no significant improvement has been achieved over the past four decades.10 Among other factors, patient-specific inhaler selection and improved training are likely to support solving this issue.5,11 Current studies focus on patient preferences, as satisfaction with an inhaler has been shown to positively impact treatment adherence and asthma control.12–15
However, to our knowledge no industry-independent study on inhaler preferences in asthmatic children has been performed. The aim of the present study was to investigate different inhaler characteristics with respect to their importance in defining the preferred device in children 7 to 15 years of age. We further investigated the effects of age, gender and the type of school attended on the inhaler preference itself and on the importance of different device features for inhaler preference.
Patients and Methods
The main objective of the present study was to determine the preference for different types of widely used inhalers in children suffering from asthma. Furthermore, inhaler characteristics were evaluated according to their importance from the children’s point of view.
Study Design and Study Patients
We performed a prospective cross-sectional study on 80 asthmatic children in the the asthma outpatient department of the University Children’s Hospital Magdeburg between April 2017 and December 2018 during routine visits. A small number of participants (n = 5, 6.25%) were inpatients of this hospital. Inclusion criteria were an established diagnosis of asthma, age 7–15 years and informed consent of the patients and their parents. Exclusion criteria were a lack of a definite diagnosis of asthma, additional bronchopulmonary disorders and lack of written informed consent.
Each child was presented the following nine placebo inhalers before these were tested and evaluated in random order. All selected devices were approved products with a high market share in Germany.
- Dry powder inhalers (DPIs): Breezhaler, Diskus, Novolizer, Easyhaler, Spiromax, Turbohaler
- Pressurized metered dose inhaler (pMDI): Flutiform
- Breath-triggered inhaler: Autohaler
- Soft mist inhaler (SMI): Respimat
The study was approved by the ethics committee of the Otto-von-Guericke-University, Magdeburg, Germany (file reference 75/17) and was carried out in accordance with the Helsinki Declaration.
Data Collection and Evaluation of the Inhalers
The placebo inhalers were studied using two questionnaires, which were developed for the study based on the Patient Satisfaction and Preference Questionnaire (PASAPQ) and the Feeling of Satisfaction with Inhaler Questionnaire (FSI-10). The parents’ questionnaire collected sociodemographic data, information about disease duration, current and previous inhaler use, the use of a spacer and previous inhaler trainings as well as reasons for inhaler changes. The questionnaire for the children was completed in an oral interview situation, which was performed in a separate room while parents filled the parents’ questionnaire. The average examination time per patient was 20–30 minutes. In the first part of the interview, the importance of general inhaler characteristics was assessed: simple steps in the application procedure, existence of a counter, attractive design, color, unobtrusive design, inhalation resistance and of the time necessary for a single use. Each device feature could be rated as important, unimportant or not specified. Then the nine placebo inhalers were demonstrated by the investigator and afterwards tested by the children. A total of eight categories were evaluated: preparation, use, hand position, mouthpiece, error free use, emergency suitability, design and overall satisfaction. For example, children were asked “Do you evaluate the Spiromax inhaler easy to use?” and could answer “true”, “not true”, “partially true” or “no specification”. The results of this part of the study showed the children’s preference for one of the nine inhalers. In addition, the children demonstrated to the investigator the use of their current inhaler. Correct performance checklists were used to document whether inhalation was performed correctly.
For some parameters the sample size was inconstant, since some children did not answer single questions due to a lack of cooperation (eg, due to boredom, defiance). We decided not to completely exclude these patients from the study, as no relevant effects on the results of the other questions/parameters were expected and this would have led to an unnecessary loss of information.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics for Windows, Version 26.0 (Armonk, NY) IBM SPSS Statistics for Windows (Version 26.0. Armonk, NY). The associations between categorical variables were examined using chi-square tests. Cramer’s V was calculated as a measure of effect size in these tests. Individual columns were examined for equality using z-tests under Bonferroni correction. In evaluating associations with the metric variable age, the nonparametric procedures of the Kruskal–Wallis test for independent samples and the Mann–Whitney U-test for independent samples were applied to differences in mean tendency. To test for significance of differences in ratings of the importance of various inhaler properties, the nonparametric Cochran Q test was used with linked samples. Friedman’s two-factorial analysis of variance for connected samples was used to evaluate the ratings of the nine placebo inhalers. The distribution of positive and negative preferences was tested for deviations from uniform distribution using the chi-square test, because a significant preference exists only if the distribution of ratings is overrandom. The significance level was set at α = 0.05.
Results
Patient Characteristics
The mean age of the participating children was 10.87 ± 2.62 years. There were 43 boys (53.75%) and 37 girls (46.25%). The majority were elementary school students (German Grundschule from grades 1 to 4; n = 36, 45.0%), followed by high school students (German Gymnasium, highest level of school education and university entrance qualification; n = 25, 31.25%). The smaller proportion of children were attending secondary school (German Realschule, medium level of school education; n = 10, 12.5%), primary school (German Hauptschule, lowest level of school education; n = 1; 1.25%) or another form of school (n = 8, 10%).
Current Situation of Asthma Inhaler Treatment
Most children used a metered dose inhaler (n = 35, 41.67%) as their current inhaler at the time of the interview. The Diskus (n = 19, 22.62%) and the Easyhaler (n = 17, 20.24%) were also frequently used. Figure 1 shows the inhalers used by the children at the time of the study.
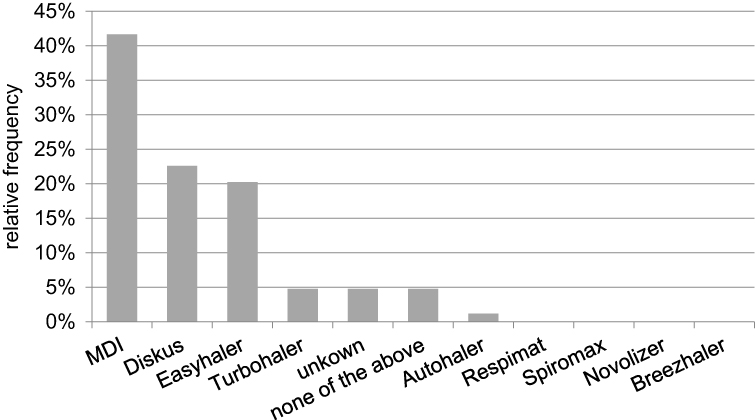 |
Figure 1 Current inhaler. Most common asthma inhaler types used at home, including multiple responses in the total sample (N = 78). Abbreviation: MDI, metered dose inhalers. |
Half of the children (n = 40, 50.0%) interviewed reported using or having used a spacer. The larger proportion of those children (n = 32, 80.0%,) reported that the spacer did not bother them or had not bothered them at the time of its use.
The children’s error rate in using their current inhaler was determined. Here, 76.25% (n=61) of the children demonstrated correct use of their current inhaler.
Most children (n=57, 71.25%) reported inhaling without the help of their parents. Furthermore, we investigated whether the children or their parents had received instructions for the correct use of the inhaler after prescription. A total of 93.7% (n=75) of the study participants received training for their current inhaler (S1). In most cases (n=60, 68.97%), training had been received from the physician. In 19.54% (n=17) of cases, training had been provided by a physician assistant and in 3.45% (n=3) by a pharmacist. Two patients (n=2.3%) had received training for the correct use of their inhaler during an inpatient rehabilitation stay (S2).
In 73% (n=59) of cases, correct use of the inhaler was demonstrated to parents and children together. In case of a past inhaler change, the study investigated which device had previously been used and the reason for the change. A total of n = 32 (40.0%) children had previously used another inhaler, most commonly the Diskus (n = 8, 28.57%). The second most common device switched away from was the Turbohaler (n = 3, 10.71%). In addition, n = 7 children (25%) reported previously having used an inhaler not listed in the questionnaire. In most cases, the use of an alternative device was at the request of the physician (n = 23, 76.67%). In n = 7 cases (23.33%) it was at the request of the patient and in no case of the pharmacy.
Importance of Different Inhaler Properties for Preference
In the first part of the interview, children were asked to rate general inhaler features with respect to their importance for preference (Figure 2). Each feature could be classified as important or unimportant (Figure 2). It was further possible to select “no preference”, as some children had no opinion in single case. A counter (81.3%), ease of use (66.3%) and the duration of inhalation (61.3%) were rated as important features. In contrast, the color (32.5%), attractive design (31.3%) and discrete handling design (33.8%) of the inhaler were predominantly rated as unimportant.
 |
Figure 2 Assessment of the importance of different inhaler features for inhaler preference in the total sample (N = 80). |
Inhaler Device Assessment
In the second part of the children’s interview, the nine placebo inhalers were demonstrated to the children by the investigator. The children were then asked to use and subsequently rate each of the placebo inhalers in different categories. With regard to preparation, the Spiromax achieved the highest score with 93.75% (n=75) agreement. The Breezhaler was least preferred in this category (n=23, 28.75%). With regard to use, the highest relative agreement value was for the Spiromax with 90% (n=27) and the lowest value (n=29; 36.25%) was obtained for the Respimat. With regard to hand position, the highest relative agreement value was indicated for the Spiromax with 83.75% (n=67) and the lowest for the Breezhaler with 55% (n=44). In the evaluation of the mouthpiece, the Novolizer emerged as the favorite inhaler with a relative agreement value of 81.25% (n=65). The Discus scored lowest in terms of the mouthpiece with a relative agreement value of 61.25% (n=49). With respect to correctness, the Novolizer was rated highest with a relative agreement of 85% (n=68). The Respimat was clearly rated lowest in this regard with only 21.25% (n=17) relative agreement. With respect to emergency use, the Spiromax was clearly favored with a relative agreement of 88.75% (n=71). The Breezhaler ranked lowest in this regard with an agreement of only 18.75% (n=15). With respect to design, the pressurized metered dose inhaler was favored with 70% agreement (n=56). The Respimat was rated lowest with 35% (n=28) agreement.
At the end of the evaluation of each category of inhalers, the children were asked whether they were “very satisfied”, “partly satisfied” or “not satisfied” with the tested inhaler. In a comparison of all inhalers, the Spiromax was most frequently rated with “very satisfied” with a relative agreement of 67.5% (n=54), while the Respimat was rated lowest with a very low agreement of 12.5% (n=10).
No significant difference was found between different age groups (7–9 years, 10–12 years, 13–15 years) with respect to the preference for a specific inhaler (p= 0.154), nor was there a significant difference in gender (X²(7, N = 78) 11.87, p = 0.105) or school type (X²(28, N = 78) 45.74, p = 0.19). The sample exhibits selection bias, as primary school students were not represented with one person participating in the study.
Positive or Negative Preferences
The final question asked after the inhalers had been tested, was which inhaler the children would most and least prefer for daily use. This evaluation showed that, in contrast to the previous evaluation in which the Spiromax scored best (see previous section), the Novolizer was most frequently named as the overall favored inhaler. Most positive ratings (Figure 3) were indicated for the Novolizer with 33.3% (n = 26), followed by the Spiromax with 20.5% (n = 16) and the Breezhaler with 15.4% (n = 12). This distribution of positive ratings was significantly different from the equal distribution with χ² (7, N = 78) 45.49, p < 0.001). Regarding statistical tests to control for preferences depending on experience with a particular inhaler, we would like to point out that our study did not address this question, which could have potentially biased the results. Regarding age, gender and school type, no significant differences were observed with respect to the overall positive inhaler preference.
 |
Figure 3 Distribution of positive and negative assessments of the different inhalation types in the total sample (N = 78). Preferred inhalers were colored in dark gray, and non-preferred inhalers were colored in light gray. Abbreviation: MDI, metered dose inhalers. |
Participants distributed the most negative ratings to the Respimat with 31.5% (n = 23), followed by the Breezhaler with 27.4% (n = 20) and the Diskus with 12.3% (n = 9) (Figure 3). The distribution of negative evaluations was significantly different from the uniform distribution (χ² (7, N = 79) 50.76, p < 0.001), which also indicated a significant negative evaluation of these three inhaler types. No negative evaluations were indicated for the Novolizer. In contrast, the Respimat obtained the most negative ratings and received no positive rating.
Discussion
Our industry-independent study provides important insights into children’s preferences with respect to commonly used inhalers available for the treatment of asthma on the German market.
In terms of inhaler characteristics important to children for defining their inhaler preference, a counter, ease of use and short duration of inhalation were most frequently considered as important features. No differences were found with respect to age, the school type visited by the participants or gender with respect to the preferences identified.
Our results show that there are large differences between different inhaler models, highlighting the importance of patient-specific preferences in inhaler choice. Indeed, also both the current National Health Care Guideline and GINA emphasize the role of patient-specific preferences.2,16 Therefore, it is necessary to provide evidence-based recommendations which inhalers are suited for children. While previous literature is largely focused on adults,17–19 a specific evaluation of the most appropriate inhalers is particularly important in children, as they physically and cognitively differ from adults.16,20,21 Simple application steps and no or few coordinating steps are preferred.20,21 We confirm that the ease of use correlates positively with children’s preferences, which has already been shown for adults.22,23
In our study, most children used a metered-dose inhaler as their current inhaler, followed by the Diskus and the Easyhaler. Aerosol characteristics are often an important consideration when choosing an inhaler and the selection of an inhaler is clearly determined by its approval for pediatric use. Metered dose inhalers cover a wide age range and are used by young children with a spacer as well as older children without coordination problems.24 In addition, many children have a metered dose inhaler for acute symptoms, because unlike powder inhalers, a low lung volume is enough for efficient use.25 In contrast, the frequent use of the Diskus and Easyhaler is more difficult to explain because, to our knowledge, there is no literature demonstrating that these inhalers are particularly suitable for children. Previous studies have found that the choice of inhaler is often determined by the healthcare professional.26,27 This observation is particularly evident in our study when comparing the three most commonly used inhalers to the inhalers favored by the participating children. The Novolizer, Spiromax and Breezhaler were named as the three most appropriate inhalers. In contrast to this preference, however, none of these inhalers was currently used by the children at home. The Novolizer is approved for use from the age of six years and would therefore also in principle be approved for use in the study group investigated. For the Spiromax and Breezhaler, on the other hand, it must be taken into account that these inhalers are not approved for use in children.28
Other studies report much higher error rates (ranging from 45% to over 90%5–7) than our study (correct demonstration of the use in 76.25%). These differences can possibly be explained by regular trainings in correct inhaler use as part of the regular asthma consultations in our study participants. For example, 94% of our participants reported having received training on their current inhaler, which appeared to have a positive effect on error-free inhaler use. Other studies confirmed that repeated instructions were associated with improved inhaler technique.5 However, the lack of such training is unfortunately widespread in clinical practice,29 despite the fact that its benefits are well established.
In our study, 40.0% of the children reported a past change in the inhaler used, mostly initiated by the physicians and only rarely at the request of the patient. However, when such a change occurs, it is important that the patient is involved in the process. Otherwise, especially in the absence of instructions, this may lead to lower efficacy and higher error rates with the new device.30
We identified several features of the inhaler devices that were especially important to children in the age from 7 to 15 years. foremost this was the presence of a dose counter, but also ease of use and short duration of inhalation. The counter was probably considered important because it provides a control function for patients and thus a sense of security regarding correct inhalation. Studies specifically addressing this issue have shown that a counter increases satisfaction and adherence by removing the fear of running out of medication or applying a subtherapeutic dose.31,32 However, the counter does not control the inhalation technique33 and incorrect inhalations are also counted. A color change or clicking sound, such as in the Novolizer or Autohaler, would be a more suitable control mechanism in this case. However, even these control functions do not cover all errors. A better solution to control correct inhalation could be the use of newer digital functions34 or sensors attached to the inhaler that measure inhalation technique and adherence.35,36
The features ease of use and short duration are important not only for children but also for adults, and they are associated with correct inhalation technique, good symptom control and good adherence.9,17,22,23 This is especially important in children, as inhalation in any case is challenging for coordination and cognition.16,20,21
Color, design and discreet design were found to be least relevant. With regard to design and color, despite its overall low importance in the cohort, it could be shown that these characteristics seem to be more relevant for younger children than for older children. With increasing age, consistent with previous studies,37 these characteristics were increasingly rated as unimportant (data not shown).
In terms of the control function for correct inhalation and the mouthpiece, the Novolizer performed best. In terms of design, the metered dose inhaler was cited as the favorite. The Spiromax performed best in terms of simple preparation steps, easy handling, hand-holding, suitability in an emergency and overall satisfaction. It was contradicting that the Spiromax performed best in most categories, yet was not named most frequently as the overall preferred device (“Which inhaler would you name as your favorite?”). Here, the Novolizer was indicated most frequently. A possible explanation is that the Novolizer was mainly convincing due to its control function that the other features appeared to be “less relevant”. This assumption can also be strengthened by the fact that the counter was rated as the most important feature and is often equated with “control function”.31,32 In contrast, the Breezhaler and Respimat were the least favored inhalers and in conclusion, our results show a clear difference between the individual inhalers.
In our opinion, all paediatric inhalers should be easy to use and have a counter. Our study should serve as an incentive for medical staff to ensure that these features are present when prescribing inhalers for children and thus improve patient compliance in the long term.
Conclusion
Our study compared nine inhalers commonly used in Germany. Novolizer and Spiromax were rated highest by the children. In terms of individual inhaler characteristics, the presence of a counter, ease of use and short duration of inhalation were rated the most important. Neither age, gender, nor the type of school attended significantly influenced the preferences identified.
Data Sharing Statement
The datasets used and/or analysed during the study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Written informed consent was obtained from each participant and their parents, as all patients were under 18 years of age. The study complies with the Declaration of Helsinki and the study protocol was approved by the local ethics committee of Otto von Guericke University Magdeburg, Germany. Reference number: 75/17.
Aknowledgment
We thank all the children and parents who made a great contribution and made the work so special. Furthermore, we would like to thank all staff members of the asthma outpatient clinic of the Department of Pediatrics and the Department of Pneumology of the University Medicine Magdeburg. In particular, we thank Dr. rer. nat. Sabine Stegemann-Koniszewski and Dr. med. Annett Lambrecht as well as Dipl.-Phys., M.Sc. Dirk Schomburg from the Institute of Biometry and Medical Informatics (IBMI).
Author Contributions
All authors have made significant contributions to the report, whether in its conception, design, execution, analysis, interpretation, or all of the above; have participated in the drafting, revision, or critical review of the article; have given final approval for the version to be published; have agreed on the journal to which the article was submitted; and agree to be responsible for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. World Health Organisation (WHO). Asthma: key facts; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/asthma.
2. Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention; 2021. Available from: https://ginasthma.org/.
3. Takahashi S, Iwasaki K, Shirato H, Ho M, Umezu M. Comparison of supportive regulatory measures for pediatric medical device development in Japan and the United States. J Artif Organs. 2020;24(1):90–101. doi:10.1007/s10047-020-01216-6
4. Samady W, Rodriguez VA, Gupta R, Palac H, Karamanis M, Press VG. Critical errors in inhaler technique among children hospitalized with asthma. J Hosp Med. 2019;14(6):361–365. doi:10.12788/jhm.3195
5. Gillette C, Rockich-Winston N, Kuhn JBA, Flesher S, Shepherd M. Inhaler technique in children with asthma: a systematic review. Acad Pediatr. 2016;16(7):605–615. doi:10.1016/j.acap.2016.04.006
6. Pappalardo AA, Karavolos K, Martin MA. What really happens in the home: the medication environment of urban, minority youth. J Allergy Clin Immunol Pract. 2017;5(3):764–770. doi:10.1016/j.jaip.2016.09.046
7. Pedersen S, Dubus JC, Crompton G. The ADMIT series — issues in inhalation therapy. Inhaler selection in children with asthma. Prim Care Respir J. 2010;19(3):209–216. doi:10.4104/pcrj.2010.00043
8. Plaza V, Giner J, Calle M, et al. Impact of patient satisfaction with his or her inhaler on adherence and asthma control. Allergy Asthma Proc. 2018;39(6):437–444. doi:10.2500/aap.2018.39.4183
9. Takemura M, Kobayashi M, Kimura K, et al. Repeated instruction on inhalation technique improves adherence to the therapeutic regimen in asthma. J Asthma. 2010;47(2):202–208. doi:10.3109/02770900903581692
10. Sanchis J, Gich I, Pedersen S. Systematic review of errors in inhaler use: has patient technique improved over time? Chest. 2016;150(2):394–406. doi:10.1016/j.chest.2016.03.041
11. Gibson PG, Powell H, Coughlan J, et al. Self-management education and regular practitioner review for adults with asthma. Cochrane Database Syst Rev. 2003;1. doi:10.1002/14651858.CD001117
12. Ding B, Small M, Scheffel G, Holmgren U. Maintenance inhaler preference, attribute importance, and satisfaction in prescribing physicians and patients with asthma, COPD, or asthma–COPD overlap syndrome consulting for routine care. Int J Chron Obstruct Pulmon Dis. 2018;13:927–936. doi:10.2147/COPD.S154525
13. Hauser K, Koerfer A, Kuhr K, Albus C, Herzig S, Matthes J. Outcome-relevant effects of shared decision making. Dtsch Arztebl Int. 2015;112(40):665–671. doi:10.3238/arztebl.2015.0665
14. Usmani OS, Lavorini F, Marshall J, et al. Critical inhaler errors in asthma and COPD: a systematic review of impact on health outcomes. Respir Res. 2018;19(1):10. doi:10.1186/s12931-017-0710-y
15. Baggott C, Chan A, Hurford S, et al. Patient preferences for asthma management: a qualitative study. BMJ Open. 2020;10(8):e037491. doi:10.1136/bmjopen-2020-037491
16. Bundesärztekammer (BÄK), Kassenärztliche Bundesvereinigung (KBV), Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen, Fachgesellschaften (AWMF). Nationale Versorgungsleitlinie Asthma – langfassung, 4. Auflage; 2021. Available from: https://www.leitlinien.de/themen/asthma.
17. Rönmark P, Jagorstrand B, Safioti G, Menon S, Bjermer L. Comparison of correct technique and preference for Spiromax®, Easyhaler® and Turbuhaler®: a single-site, single-visit, crossover study in inhaler-naïve adult volunteers. Eur Clin Respir J. 2018;5(1):1529536. doi:10.1080/20018525.2018.1529536
18. O’Hagan P, Dederichs J, Viswanad B, Gasser M, Walda S. Patient preference for a maintenance inhaler in chronic obstructive pulmonary disease: a comparison of breezhaler and respimat. J Thorac Dis. 2018;10(10):5727–5735. doi:10.21037/jtd.2018.09.126
19. Hodder R, Reese P, Slaton T. Asthma patients prefer respimat soft mist inhaler to turbuhaler. Int J Chron Obstruct Pulmon Dis. 2009;4:225–232. doi:10.2147/COPD.S3452
20. Ciciliani AM, Langguth P, Wachtel H. Handling forces for the use of different inhaler devices. Int J Pharm. 2019;560:315–321. doi:10.1016/j.ijpharm.2019.01.053
21. Everard ML. Inhaler devices in infants and children: challenges and solutions. J Aerosol Sci. 2004;17(2):186–195. doi:10.1089/0894268041457129
22. Schreiber J. Sonnenburg, Luecke E: inhaler devices in asthma and COPD patients- a prospective cross-sectional study on inhaler preferences and error rates. BMC Pulm Med. 2020;20(1):222. doi:10.1186/s12890-020-01246-z
23. Ruessel K, Luecke E, Schreiber J. Inhaler devices in a geriatric patient population: a prospective cross-sectional study on patient preferences. Patient Prefer Adherence. 2020;14:1811–1822. doi:10.2147/PPA.S262057
24. Janssens HM, Tiddens HA. Aerosol therapy: the special needs of young children. Paediatr Respir Rev. 2006;7:S83–S85. doi:10.1016/j.prrv.2006.04.167
25. Amirav I. Metered-dose inhaler accessory devices in acute asthma. Arch Pediatr Adolesc Med. 1997;151(9):876. doi:10.1001/archpedi.1997.02170460014003
26. Upton J, Fletcher M, Madoc-Sutton H, Sheikh A, Caress AL, Walker S. Shared decision making or paternalism in nursing consultations? A qualitative study of primary care asthma nurses’ views on sharing decisions with patients regarding inhaler device selection. Health Expect. 2011;14(4):374–382. doi:10.1111/j.1369-7625.2010.00653.x
27. Gravel K, Légaré F, Graham ID. Barriers and facilitators to implementing shared decision-making in clinical practice: a systematic review of health professionals’ perceptions. Implement Sci. 2006;73(3):526–535.
28. Vogelberg C, Kremer HJ, Ellers-Lenz B, et al. Clinical evaluation of the peak inspiratory flow generated by asthmatic children through the novolizer. Respir Med. 2004;98(10):924–931. doi:10.1016/j.rmed.2004.03.024
29. Stelmach R, Robles-Ribeiro PG, Ribeiro M, Oliveira JC, Scalabrini A, Cukier A. Incorrect application technique of metered dose inhalers by internal medicine residents: impact of exposure to a practical situation. J Asthma. 2007;44(9):765–768. doi:10.1080/02770900701645694
30. Doyle S, Lloyd A, Williams A, et al. What happens to patients who have their asthma device switched without their consent? Prim Care Respir J. 2010;19(2):131–139. doi:10.4104/pcrj.2010.00009
31. Cotterell E, Gazarian M, Henry R, O’Meara M, Wales S. Child and parent satisfaction with the use of spacer devices in acute asthma. J Paediatr Child Health. 2002;38(6):604–607.
32. Nikander K, Nicholls C, Denyer J, Pritchard J. The evolution of spacers and valved holding chambers. J Aerosol Med Pulm Drug. 2014;27(S1):S–4.
33. Conner JB, Buck PO. Improving asthma management. The case for mandatory inclusion of dose counters on all rescue bronchodilators. J Asthma. 2013;50(6):658–663.
34. Virella Pérez YI, Medlow S, Ho J, Steinbeck K. Mobile and web-based apps that support self-management and transition in young people with chronic illness. Systematic review. J Med Internet Res. 2019;21(11):e13579.
35. Sidani S, Epstein DR, Fox M, Collins L. The contribution of participant, treatment, and outcome factors to treatment satisfaction. Res Nurs Health. 2018;41(6):572–582.
36. Mäkelä MJ, Backer V, Hedegaard M, Larsson K. Adherence to inhaled therapies, health outcomes and costs in patients with asthma and COPD. Respir Med. 2013;107(10):1481–1490.
37. Pradel FG, Hartzema AG, Bush PJ. Asthma self-management: the perspective of children. Patient Educ Couns. 2001;45(3):199–209.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.