Back to Journals » Patient Preference and Adherence » Volume 17
Informing Patient-Provider Engagement for Shared Decision Making Through Mobile Health Applications
Authors Shih HJ ![]() , Xue H, Min H, Wojtusiak J, Chang J
, Xue H, Min H, Wojtusiak J, Chang J
Received 28 September 2023
Accepted for publication 18 December 2023
Published 21 December 2023 Volume 2023:17 Pages 3489—3501
DOI https://doi.org/10.2147/PPA.S438710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Huan-Ju Shih,1 Hong Xue,1 Hua Min,1 Janusz Wojtusiak,1 Jongwha Chang2
1Department of Health and Human Services, George Mason University, Fairfax City, VA, USA; 2Department of Pharmaceutical Sciences, Irma Lerma Rangel School of Pharmacy, Texas A&M University, College Station, TX, USA
Correspondence: Jongwha Chang, Department of Pharmaceutical Sciences, Irma Lerma Rangel School of Pharmacy, Texas A&M University, College Station, TX, 77843, USA, Tel +1-979-436-0664, Email [email protected]
Objective: The study utilized a cross-sectional dataset to identify demographic and health factors associated with patient utilization of mHealth applications for engaging with healthcare providers. The focus was on adults with chronic health conditions as the primary app user group. The goal was to reveal specific barriers and facilitators to app adoption among smartphone users, with the aim of highlighting opportunities for upgrades that promote patient empowerment as a prerequisite for shared decision-making (SDM).
Methods: Data from the Health Information National Trends Survey (HINTS 5, Cycle 4, 2020) with 3865 respondents (≥ 18 years old) stratified analyses and weighted logistic regression were used.
Results: The study found that individuals having a wellness app on a smartphone increased the likelihood (OR 2.68, CI: 2.02– 3.56, p-value < 0.0001) of discussing health conditions with providers. Furthermore, individuals with multiple chronic health conditions were more likely (OR 1.93, CI 1.26– 2.95, p-value < 0.01) to use apps to use mobile health applications to engage with healthcare providers. Other significant variables affecting app usage such as race, marital status, and educational level.
Conclusion: Due to difficulties obtaining in-person healthcare, the COVID-19 epidemic forced a swift deployment of mHealth technologies. Even in the absence of a crisis, mobile health applications continue to be crucial for improving patient-provider engagement and developing novel approaches to healthcare delivery. During the pandemic, people with numerous chronic diseases used apps to stay in touch with doctors and maintain their reliance on these platforms. Nonetheless, different smartphone users continue to use mHealth application in different ways. The findings revealing barriers in mHealth app adoption among certain patient subgroups suggest opportunities for developers, in collaboration with users and providers, to enhance inclusion and acceptability when upgrading mHealth application platforms.
Keywords: mobile health, digital equity, post-SARS Cov2 care management, healthcare policy, chronic care
Introduction
Mobile health applications (mHealth apps) have drawn much interest as promising tools for enhancing patient-provider communication and healthcare delivery, particularly during and after the SARS Cov2 pandemic.1,2 The health aim of health apps can be summarized as maintaining improving, or managing the user’s health.3 The use of mobile devices has increased over the years, and many new apps provide individuals with convenient access to health information and resources and the ability to discuss with their healthcare providers.3,4 However, not everyone who possesses a smartphone also uses mHealth apps.5,6 From the researcher’s and medical professional perspective, understanding the factors associated with smartphone users using the mHealth apps is essential as researchers can further investigate its impact on discussions with healthcare providers, which is crucial for optimizing healthcare delivery and promoting patient engagement. This information can also urge other stakeholders to seek ways to enhance patients’ use of mHealth apps to discuss with their healthcare professionals and improve patients’ health outcomes over time.7
The Shared Decision-Making (SDM) Model, first proposed by Elwyn et al, involves three key steps - introducing choice, describing options using patient decision aids, and supporting patients in exploring preferences and deciding on care plans.8 This collaborative approach aligns with leveraging mHealth apps by: a) increasing patient awareness of health choices enabled by mobile platforms, b) integrating these technologies to explain condition and treatment options, and c) allowing patients to access personalized information to clarify priorities while conveying their needs to providers.9 Ultimately SDM emphasizes that the expertise and values patients contribute should balance clinical knowledge in making healthcare decisions together.9 This egalitarian concept of group decisions considering patient preferences and circumstances is consistent with mHealth apps’ capacity to empower individuals via self-monitoring while enabling provider discussions. The theory indicated that patient knowledge of their health/experiences and values is just as valuable as medical knowledge. This is consistent with the potential of mHealth apps to empower patients by offering tracking some of their health information, medication reminders, and addressing communication barriers.10 By enabling people to access personalized information, monitor their progress, and actively participate in their care, mHealth apps can assist patients to have knowledge of their health and keep track of self-management.11–15
From the patient’s perspective, patients who are knowledgeable about their condition may have better control over their situation and are better equipped to deal with treatment and outcome uncertainties.16–18 Additionally, knowing how chronic health issues and patient characteristics affect the use of mHealth apps might help develop targeted interventions to reduce inequalities and enhance healthcare outcomes.
From the physician’s perspective, chronic health conditions often involve multiple healthcare providers, specialists, and care settings. The mHealth apps facilitate seamless communication and information sharing between providers involved in an individual’s care.18 This promotes continuity of care, reduces the likelihood of fragmented information, and enhances collaboration among healthcare professionals, leading to a more comprehensive and coordinated approach to managing chronic conditions.12,13 The convenience, flexibility, and personalized nature of mHealth apps make them valuable tools for promoting collaborative and patient-centered care in managing chronic health conditions.14 Furthermore, mHealth apps provide a convenient platform for individuals to communicate with their providers, share health information, ask questions, and receive guidance.19,20 This can lead to more frequent and efficient communication, facilitating timely interventions and improved disease management.14,21,22
However, not every individual with chronic health conditions has access to healthcare services due to mobility issues, distance, or limited availability of specialists.23 The mHealth apps can bridge this gap by enabling remote consultations and telemedicine visits.24,25 This allows individuals to discuss their health concerns, receive virtual care, and access expert advice without the need for in-person visits, reducing barriers to healthcare access.24 Individuals with chronic health conditions can use these apps to monitor their health parameters and share the data with their healthcare providers. This real-time information helps providers make informed decisions, adjust treatment plans, and detect potential issues early.24,26
In this paper, we will be using the Health Information National Trends Survey (HINTS) which is a national survey that has been conducted periodically by the National Cancer Institute since 2003 to assess the American public’s access to and use of health information.25 This study utilizes data collected from February through June 2020 were the survey questions relevant to use of mobile health (mHealth) applications, facilitating analysis of factors associated with patient-provider engagement via these technologies. In addition, the data collection occurred during an unprecedented historical context, the emergence of the COVID-19 pandemic. During this crisis, constraints on in-person healthcare coupled with pressures on health systems dramatically accelerated adoption of digital health technologies out of sheer necessity.24 This study intended to assess the correlations between chronic conditions, demographics, and patient use of mHealth apps for provider discussions. The findings may reflect this unique crisis situation. In the methods section below, we will further detail the selection of relevant HINTS survey questions analyzed to address this study specific research aims related to mHealth apps use and patient-provider engagement.
Materials and Methods
Sample and Data Collection
The Health Information National Trends Survey (HINTS) is a biennial, cross-sectional survey of a nationally-representative sample of American adults used to assess the impact of the health information environment. Specifically, HINTS measures how people access and use health information, how people use information technology to manage health and health information, and the degree to which people are engaged in healthy behaviours. Finally, several items in HINTS specifically focus on cancer prevention and control. Among all the questionnaires, twenty-three were used for our analyses, and the responses were collected from 3865 respondents. This study was approved for waiver from the National Institute of Health (NIH) Office of IRB Operation (IRBO) (45 DFR 46.102).
The Outcome Measure of Health App Use
Respondents in the sample were asked a binary question, a) Has your tablet or smartphone helped you in discussions with your healthcare provider?
Independent Variables
We included demographic parameters, overall health and insurance status, and behavioral aspects, which were part of the HINT questionnaire. Demographic covariates included the following measures: age category (18–34 years, 35–49 years, 50–64 years, 65–84 years, 85–104 years); sex (male, female); race/ethnicity (white Non-Hispanic, black Non-Hispanic, Hispanic, Non-Hispanic Asian); educational attainment (less than high school degree, completed high school, attended some college/obtained associate degree, graduated from college, and post-degree); annual household income (less than $20,000, $20,000 to < $35,000, $35,000 to <$50,000, $50,000 to < $ 75,000 and $75,000 or more); marital status (married, divorced/widowed/separated, single, never been married); rural status (urban, rural); census region (Northeast, Midwest, South, and West), and employment status (employed, others). Health-related measures included BMI category (underweight, normal, overweight, obese), and health insurance types (uninsured, current or former employer or union, purchased directly from an insurance company). Behavioral factors included smoking status (current, former, never). We also considered chronic health conditions, such as ever being diagnosed with cancer (yes/no), depression or anxiety (yes/no), diabetes/ high blood sugar (yes/no), high blood pressure/hypertension (yes/no), heart problem (yes/no), and lung/asthma/emphysema, or bronchitis (yes/no). We also created two separate variables for analysis. The first variable, called chronic health, combined all the chronic health diseases into a frequency variable with three categories: none, one, and more than one. The second variable, insurance, combined all types of insurance into a binary variable.
Statistical Analysis
The unit of analysis is the individual who responds to the survey. To analyze the data, we utilized STATA SE 16 statistical software (StataCorp.2019. Stata Statistical Software: Version 16. College Station, TX: StataCorp LLC.). Basic statistical analysis, stratified analyses, and weighted logistic regression were used to calculate the percentage and standard error for each combination of variables with the outcome. Additionally, we conducted the Wald test to examine the hypothesis of equal proportions. Observations with incomplete information were not included in the final analytic sample. Two weighted binary logistic regression tests were conducted to evaluate the associations between (a) the use of a smartphone and communication with healthcare providers and (b) among those who have a smartphone and mHealth apps in communication with healthcare providers. Two additional stratified analyses were conducted to understand better the impact of chronic health conditions and gender on patients’ likelihood of discussing their health conditions with their providers. The significance threshold for the analyses was set at a P-value of 0.05.
Results
Sample Characteristics
The descriptive analyses of our sample are provided in Table 1. Of the 3865 adults, 3239 (85.19%) reported having a smartphone and/or tablets and 1739 (54.84%) reported having a health app. The largest age group among the respondents was those aged 50 to 64 years old (27%). The majority of the respondents were female, 2052 (53%), Non-Hispanic White, 2133 (63%), and married 1978 (54%). In addition, 1663 (39%) of the respondents had some college degree, and 42% of the total population reported earning $75,000 or more a year. The majority of the respondents, 2280 (69%), were employed, 94% lived in an urban area, and 37% were from the country’s southern region. Almost half of our sample respondents (41%) reported having at least two or more chronic illnesses. Lastly, 1803 (50%) of the respondents indicated they have insurance through their current or former employer or union.
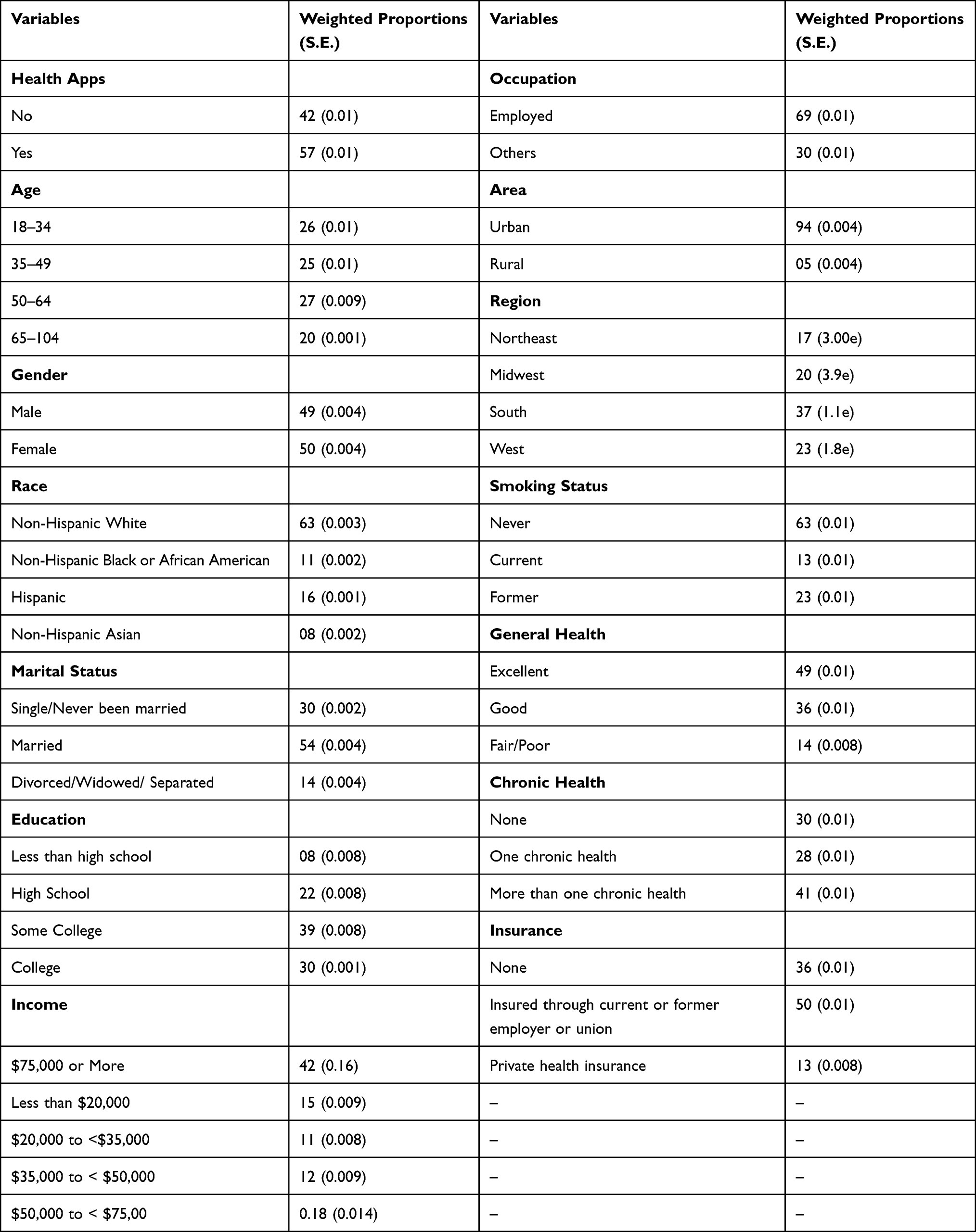 |
Table 1 Demographic Characteristics of Adults (N=3865) |
Prevalence of Using Smartphone/mHealth App Use and Associations with Discussing with the Providers
Table 2 presents the results of the logistic regression analysis conducted on the study population, showing the adjusted odds ratio (OR) for each independent variable in relation to using a tablet or smartphone with mHealth apps to facilitate discussions with healthcare providers. The findings indicated that people with several chronic health diseases were more likely to use the mHealth app to communicate about their health conditions compared to those without chronic health disorders. Furthermore, individuals who had wellness apps on their phones exhibited significantly higher odds (OR 2.68, CI: 2.02–3.56, p-value <0.0001) of communicating their health conditions with their healthcare providers. Specifically, females were 1.47 (1.08–1.99) times higher odds of discussing with their providers using health apps compared to males. Non-Hispanic Black or African American people were 2.41 (1.46–3.97) times were found to be more likely to engage with their healthcare providers through the use of a tablet or smartphone mHealth apps compared to Non-Hispanics White individuals. Married people had 1.54 (1.01–2.32) times higher odds of discussing their health with their providers. Similarly, people with at least a college degree had 2.50 (1.15–5.39) times higher odds of using a tablet or smartphone mHealth app than those without a high school degree. The odds ratios ranged from 1.35 (95% CI 0.99–1.84) for individuals with one chronic condition to 1.93 (95% CI 1.26–2.95) for those with multiple chronic diseases, compared to individuals without chronic diseases.
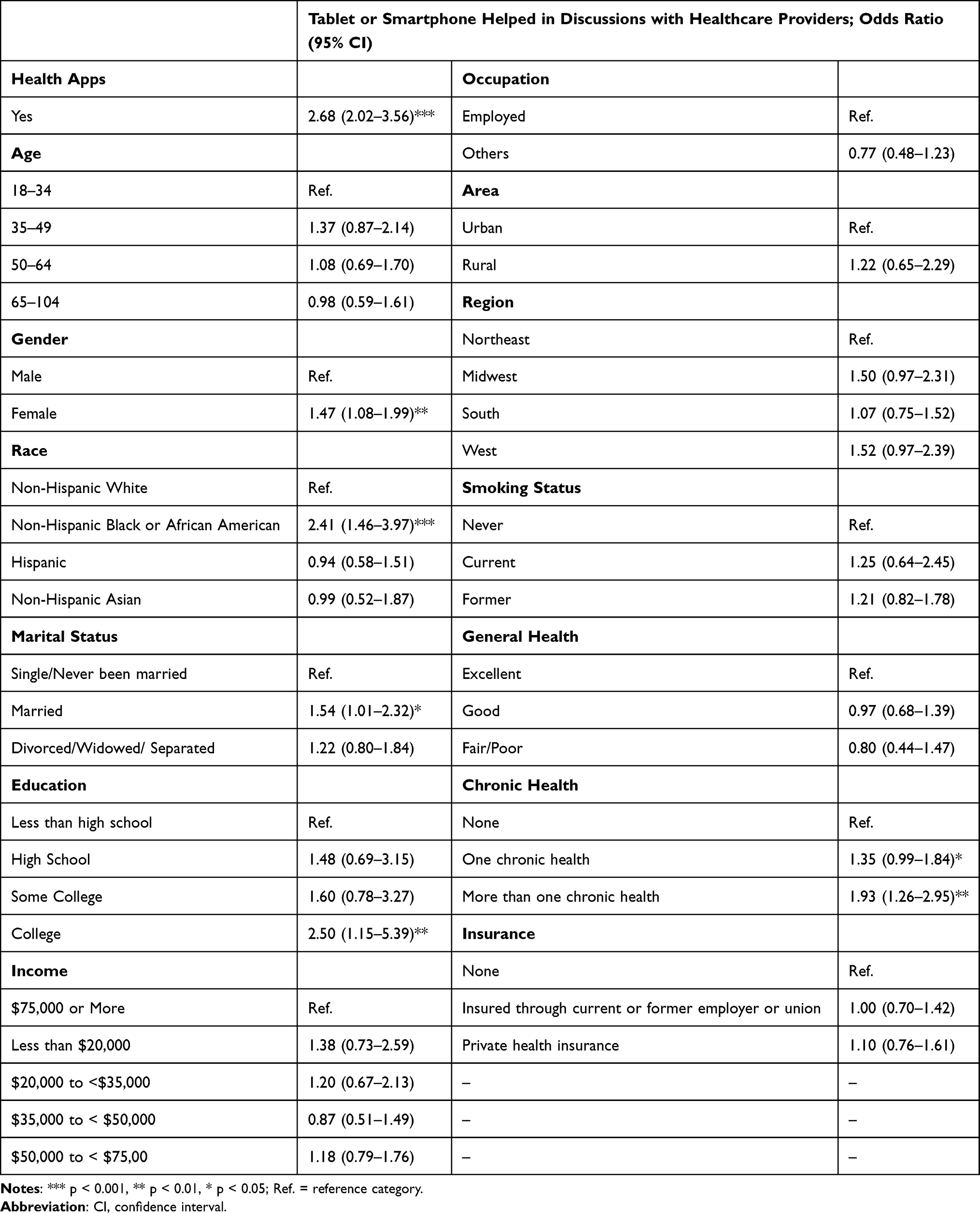 |
Table 2 Association of Smartphone mHealth App Users with Discussion with Healthcare Providers |
Stratified Analysis of mHealth App Usage on Discussing with the Providers
Table 3 and Table 4 present the results of two stratified analyses. Table 3 focuses on gender-related differences, while Table 4 examines adults with and without chronic health conditions. In Table 3, our findings suggest that males were more likely to use mHealth apps to communicate with their health providers than females. Males with one or more than one health condition had significantly higher odds (2.30, 95% CI: 1.05–5.05) and (3.35, 95% CI: 1.16–9.65), respectively, compared to those without any chronic health condition. On the other hand, there was no significant association between the use of mHealth apps and the number of chronic diseases for females. The odds were relatively smaller, with odds ratios of 1.15 (95% CI: 0.66–1.99) and 1.75 (95% CI: 0.91–3.39) for females with one chronic condition and more than one, respectively.
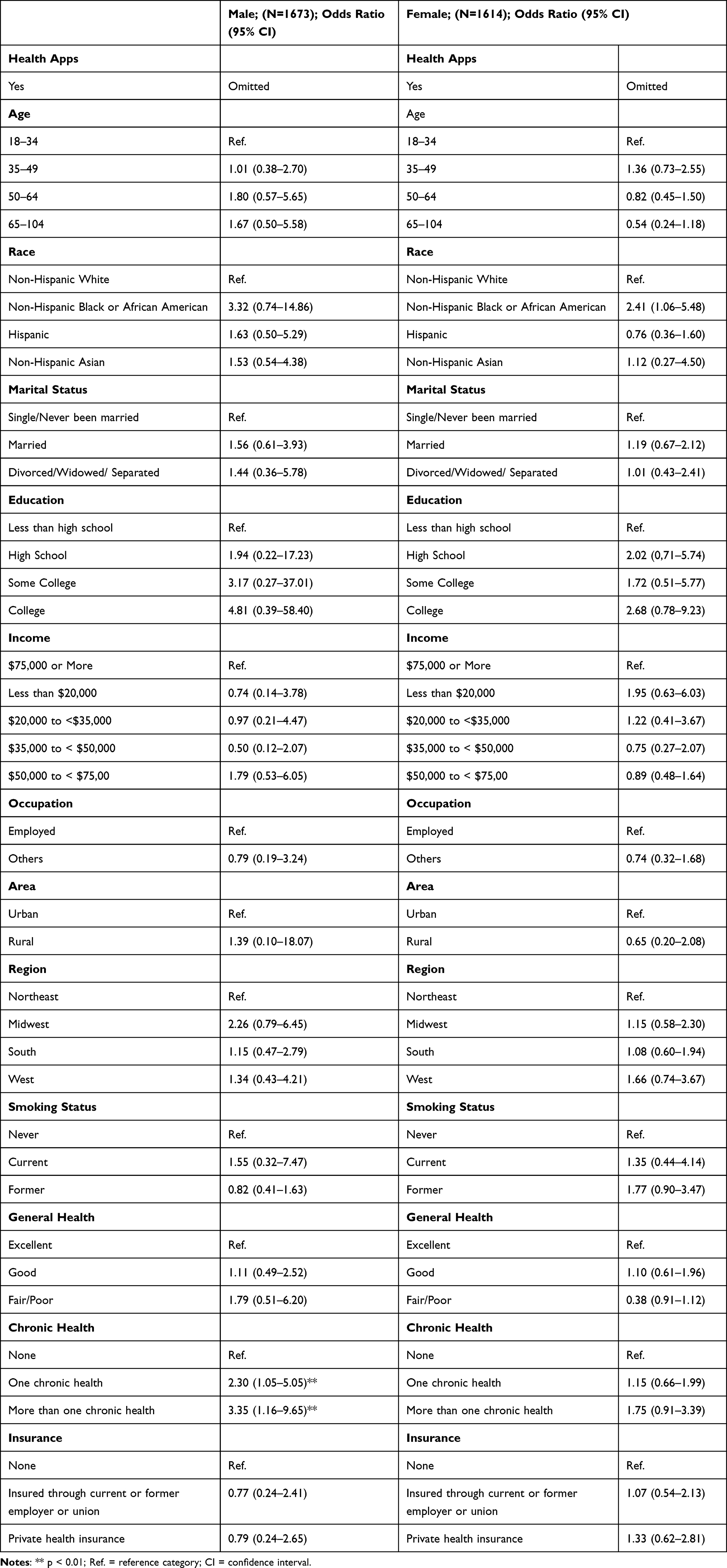 |
Table 3 Stratified Analysis Among Adults Based on Gender Differences (Male Vs Female) |
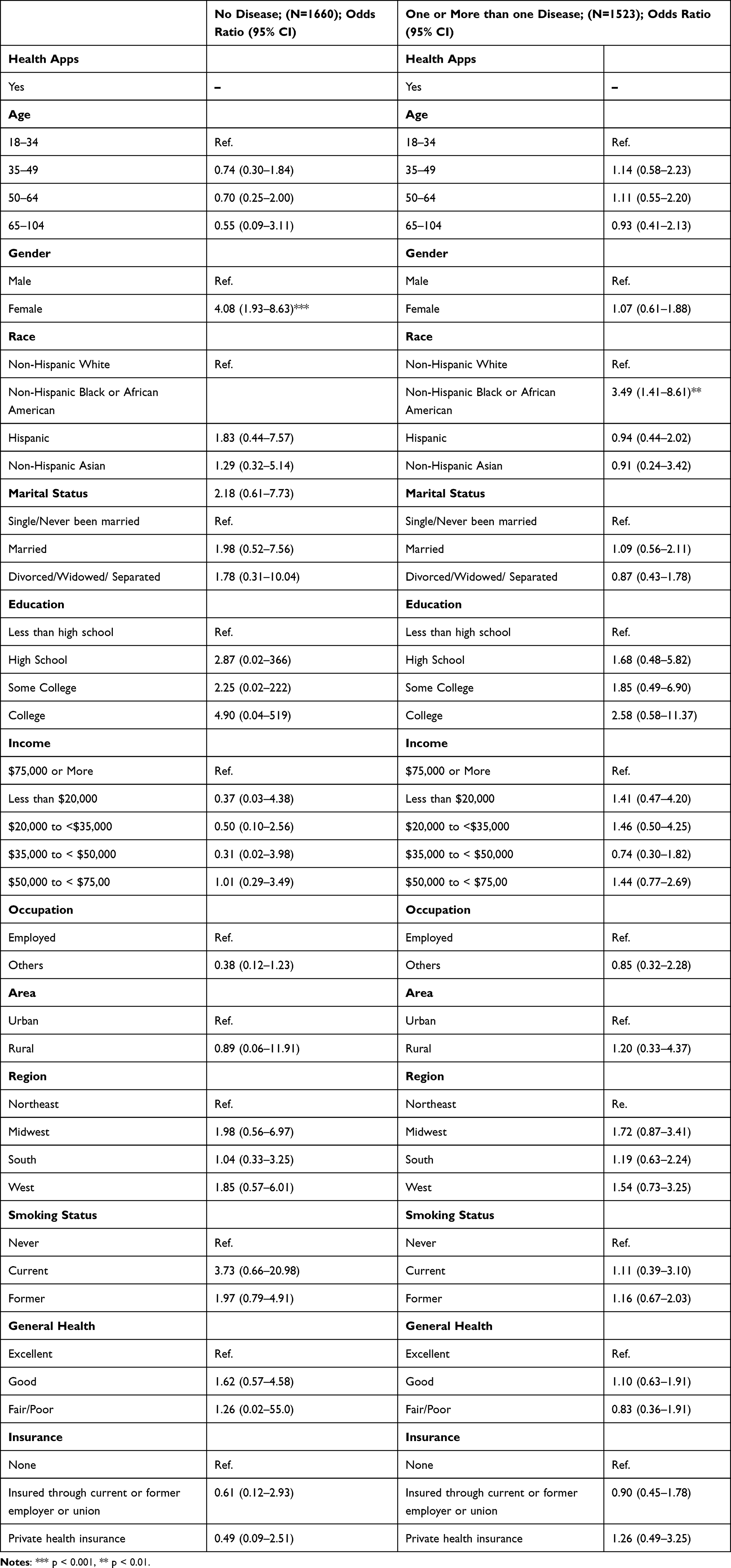 |
Table 4 Stratified Analysis Among Adults with Chronic Health (None Vs One or More Than One Disease) |
Table 4 shows that females had higher odds among individuals without any chronic health disease (OR 4.08, 95% CI: 1.93–8.63) compared to males in terms of discussing their health conditions with healthcare providers. Among those with one more chronic disease, non-Hispanic Black or African American people were significantly more likely than non-Hispanic White people to talk to healthcare professionals about their health concerns. However, there is no difference in the likelihood of discussing health conditions with healthcare professionals among Hispanic or non-Hispanic Asian individuals compared to non-Hispanic White individuals.
Discussion
This study focused on examining analyzed the relationship between owning mHealth apps and using smart devices for health discussions with healthcare providers among non-institutionalized individuals in the US The study utilized data from HINT 5, Cycle 4, a publicly available resource.27 This dataset provided valuable insights into the prevalence and characteristics of adults using smartphones, tablets, and health apps. This study aimed to explore the usage patterns and trends related to mHealth apps and their impact on patient-provider communication.
The findings revealing differences in mHealth apps use across demographic and health factors have important implications for advancing shared decision-making (SDM) through these technologies. As discussed previously, SDM emphasizes collaborative choices incorporating patient priorities and values on par with clinical expertise. However, this study demonstrated that the use of apps for patient-provider discussions remains uneven across groups, suggesting exiting platforms insufficiently empower diverse individuals. Patients managing multiple chronic conditions showed higher odds of leveraging apps to engage providers. Subgroups like racial minorities, unmarried adults, and those with lower education saw less benefit, likely reflecting app design and implementation shortcomings.28
The study also found that more than half of the respondents reported having a health app, indicating significant opportunities to encourage patients to use the mHealth app for discussions with their healthcare providers. Overall, the results from the binary logistic regressions supported the previous literature review findings, showing that Non-Hispanic Black or African American individuals who reported using mHealth apps had higher odds of discussing their health with providers than Non-Hispanic White individuals.28 Similarly, individuals with at least a college degree had higher odds of discussions with healthcare providers using mHealth apps.29 Additionally, individuals with multiple chronic diseases had higher odds of informing their providers of their health status using mHealth apps. Gender and marital status were also found to influence the likelihood of utilizing mHealth apps for communication with providers. The stratified analyses provided further insights into gender differences and the impact of chronic health conditions on mHealth app usage for discussions with healthcare providers. Some results are consistent with another study, indicating that users of mHealth apps for communicating with healthcare professionals are more likely to have chronic health conditions and to have wellness apps on their phones.29
Additionally, it has been discovered that using health apps for consulting with doctors about medical concerns is related to demographic factors like gender, race/ethnicity, marital status, and educational level. These results align with one of the studies indicating that shared decision-making is essential, but there are some barriers to implementing entirely due to various reasons, such as literacy barriers, different styles of communication, and or low socioeconomic status.8,30–32 However, variables such as occupational were inconsistent.33 In this study, employment status does not predict using the device to discuss with healthcare professionals.
While promising for telehealth expansion, it is highly likely this uptick stems largely from pandemic-driven necessity rather than organic adoption. Constraints on in-person care coupled with stresses on health systems compelled many patients to employ mHealth tools out of urgency. These findings have important implications for apps developers, highlighting the need to target interventions and app upgrades based on specific population subgroups. Customization of mHealth apps to meet the needs and preferences of different user groups can enhance their effectiveness.34,35 Moreover, understanding the influence of chronic health conditions and patient characteristics on mHealth app usage can guide the development of tailored interventions to address disparities and improve healthcare outcomes.36,37 In addition, this paper urges the importance of holding various stakeholders accountable in promoting the use of mHealth apps for discussions with healthcare providers. Encouraging patients to use the mHealth apps can facilitate timely access to care and improve the overall patient-provider communication experience.38
Limitations
It is important to recognize the various limitations of this study. First off, using mHealth apps for patient-provider talks and establishing causal links between the variables investigated are made impossible by the cross-sectional design. Furthermore, depending solely on self-reported survey data has the potential for recall bias, response bias, or misreporting of medical issues. Also, it is crucial to understand that the COVID-19 pandemic emerged at the same time as this HINTS survey circle, which ran from February to June 2020. Adoption of mHealth technology during this period was probably forced by widespread social limitations more so than by reliance on applications in non-pandemic scenarios. Overall, while this study highlights important variables related to patients using mHealth apps to communicate with doctors during an unparalleled adoption cycle, further research conducted during the post-pandemic era will shed light on long-term effects on care delivery.
Conclusion
Important variables that highlights the potential factors influencing patients to utilize mHealth apps for discussions with healthcare providers from this research, as over half of the respondents reported owning a health app. The binary logistic regression results were consistent with existing literature, revealing that factors such as race, education level, and chronic health conditions played pivotal roles in predicting the likelihood of discussions with providers through mHealth apps. Stratified analyses provided deeper insights into gender disparities and the influence of chronic health conditions on mHealth app usage for communication with healthcare providers. This aligns with previous research, underscoring the significance of shared decision-making while acknowledging barriers such as varying communication styles and literacy levels. The results from this research emphasize the need for further research and explore effective interventions to promote mHealth app usage among diverse populations. In addition, long-term associations for those using mHealth apps to share health information and communicate through the mHealth app have helped their health outcomes over time.
Ethics Approval and Consent to Participate
We use secondary data, and all of the patient’s data is encrypted and unable to be identified. This study was approved for a waiver from the National Institute of Health (NIH) Office of IRB Operation (IRBO) (45 DFR 46.102).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
No financial or otherwise connections would cause a declaration of interest in this article.
References
1. Fagherazzi G, Goetzinger C, Rashid MA, et al. Digital health strategies to fight COVID-19 worldwide: challenges, recommendations, and a call for papers. J Med Internet Res. 2020;22:e19284. doi:10.2196/19284
2. John Leon Singh H, Couch D, Yap K. Mobile health apps that help with COVID-19 management: scoping review. JMIR Nurs. 2020;3:e20596. doi:10.2196/20596
3. Hamilton EC, Saiyed F, Miller CC, et al. The digital divide in adoption and use of mobile health technology among caregivers of pediatric surgery patients. J Pediatr Surg. 2018;53:1478–1493. doi:10.1016/j.jpedsurg.2017.08.023
4. Baniasadi T, Niakan Kalhori SR, Ayyoubzadeh SM, et al. Study of challenges to utilise mobile-based health care monitoring systems: a descriptive literature review. J Telemed Telecare. 2018;24:661–668. doi:10.1177/1357633X18804747
5. Insid. Intell. Most US consumers are mobile health app users. Available from: https://www.insiderintelligence.com/content/nearly-two-thirds-of-us-consumers-mobile-health-app-users.
6. Outsourcing. Most older adults don’t use health apps, according to poll med prod. Available from: https://www.mpo-mag.com/contents/view_breaking-news/2022-02-09/most-older-adults-dont-use-health-apps-according-to-poll/.
7. Llorens-Vernet P, Miró J. Standards for mobile health–related apps: systematic review and development of a guide. JMIR MHealth UHealth. 2020;8:e13057. doi:10.2196/13057
8. Resnicow K, Catley D, Goggin K, et al. Shared decision making in health care: theoretical perspectives for why it works and for whom. Med Decis Making. 2022;42:755–764. doi:10.1177/0272989X211058068
9. Davidson KW, Mangione CM, Barry MJ; US Preventive Services Task Force. Collaboration and shared decision-making between patients and clinicians in preventive health care decisions and us preventive services task force recommendations. JAMA. 2022;327:1171–1176. doi:10.1001/jama.2022.3267
10. Tsai -C-C, Liu C-F, Lin H-J, et al. Implementation of a patient-centered mobile shared decision making platform and healthcare workers’ evaluation: a case in a medical center. Inform Health Soc Care. 2023;48:68–79. doi:10.1080/17538157.2022.2054344
11. Emerson MR, Buckland S, Lawlor MA, et al. Addressing and evaluating health literacy in mHealth: a scoping review. mHealth. 2022;8:33. doi:10.21037/mhealth-22-11
12. Källander K, Tibenderana JK, Akpogheneta OJ, et al. Mobile Health (mHealth) Approaches and lessons for increased performance and retention of community health workers in low- and middle-income countries: a review. J Med Internet Res. 2013;15:e2130. doi:10.2196/jmir.2130
13. Nannini S, Penel N, Bompas E, et al. Shortening the time interval for the referral of patients with soft tissue sarcoma to expert centers using mobile health: retrospective study. JMIR MHealth UHealth. 2022;10:e40718. doi:10.2196/40718
14. Cozad MJ, Crum M, Tyson H, et al. Mobile health apps for patient-centered care: review of United States rheumatoid arthritis apps for engagement and activation. JMIR MHealth UHealth. 2022;10:e39881. doi:10.2196/39881
15. Bruce C, Harrison P, Giammattei C, et al. Evaluating patient-centered mobile health technologies: definitions, methodologies, and outcomes. JMIR MHealth UHealth. 2020;8:e17577. doi:10.2196/17577
16. Improving health literacy. Available from: https://www.who.int/activities/improving-health-literacy.
17. Yadav AK, Budhathoki SS, Paudel M, et al. Patients understanding of their diagnosis and treatment plans during discharge in emergency ward in a tertiary care centre: a qualitative study. JNMA J Nepal Med Assoc. 2019;57:357–360. doi:10.31729/jnma.4639
18. Rowland SP, Fitzgerald JE, Holme T, et al. What is the clinical value of mHealth for patients? NPJ Digit Med. 2020;3:4. doi:10.1038/s41746-019-0206-x
19. Whitehead L, Seaton P. The effectiveness of self-management mobile phone and tablet apps in long-term condition management: a systematic review. J Med Internet Res. 2016;18:e97. doi:10.2196/jmir.4883
20. NEJM. The influence of finasteride on the development of prostate cancer. https://www.nejm.org/doi/full/10.1056/NEJMoa030660.
21. Alwashmi MF, Fitzpatrick B, Farrell J, et al. Perceptions of patients regarding mobile health interventions for the management of chronic obstructive pulmonary disease: mixed methods study. JMIR MHealth UHealth. 2020;8:e17409. doi:10.2196/17409
22. Mollard E, Michaud K. A mobile app with optical imaging for the self-management of hand rheumatoid arthritis: pilot study. JMIR MHealth UHealth. 2018;6:e12221. doi:10.2196/12221
23. Schwarz T, Schmidt AE, Bobek J, et al. Barriers to accessing health care for people with chronic conditions: a qualitative interview study. BMC Health Serv Res. 2022;22:1037. doi:10.1186/s12913-022-08426-z
24. Abbaspur-Behbahani S, Monaghesh E, Hajizadeh A, et al. Application of mobile health to support the elderly during the COVID-19 outbreak: a systematic review. Health Policy Technol. 2022;11:100595. doi:10.1016/j.hlpt.2022.100595
25. USC EMHA. How to improve access to health care: issues & solutions. USC EMHA online; 2022. Available from: https://healthadministrationdegree.usc.edu/blog/how-to-improve-access-to-health-care/.
26. Monaghesh E, Hajizadeh A. The role of telehealth during COVID-19 outbreak: a systematic review based on current evidence. BMC Public Health. 2020;20:1193. doi:10.1186/s12889-020-09301-4
27. HINTS. Survey Instruments. Available from: https://hints.cancer.gov/data/survey-instruments.aspx.
28. Voruganti T, Grunfeld E, Makuwaza T, et al. Web-based tools for text-based patient-provider communication in chronic conditions: scoping review. J Med Inter Res. 2017;19(10):3366. doi:10.2196/jmir.7987
29. Lee M, Kang D, Yoon J, et al. The difference in knowledge and attitudes of using mobile health applications between actual user and non-user among adults aged 50 and older. PLoS One. 2020;15:e0241350. doi:10.1371/journal.pone.0241350
30. Levinson W, Kao A, Kuby A, et al. Not all patients want to participate in decision making. A national study of public preferences. J Gen Intern Med. 2005;20:531–535. doi:10.1111/j.1525-1497.2005.04101.x
31. Ayanian JZ, Cleary PD, Weissman JS, et al. The effect of patients’ preferences on racial differences in access to renal transplantation. N Engl J Med. 1999;341:1661–1669. doi:10.1056/NEJM199911253412206
32. Cao L, Chongsuvivatwong V, McNeil EB. The sociodemographic digital divide in mobile health app use among clients at outpatient departments in inner mongolia, China: cross-sectional survey study. JMIR Hum Factors. 2022;9:e36962. doi:10.2196/36962
33. Jembai JVJ, Wong YLC, Bakhtiar NAMA, et al. Mobile health applications: awareness, attitudes, and practices among medical students in Malaysia. BMC Med Educ. 2022;22:544. doi:10.1186/s12909-022-03603-4
34. Kaptein M, Markopoulos P, de Ruyter B, et al. Personalizing persuasive technologies: explicit and implicit personalization using persuasion profiles. Int J Hum-Comput Stud. 2015;77:38–51. doi:10.1016/j.ijhcs.2015.01.004
35. Bol N, Høie NM, Nguyen MH, et al. Customization in mobile health apps: explaining effects on physical activity intentions by the need for autonomy. Digit Health. 2019;5(2055207619888074). doi:10.1177/2055207619888074
36. Kruse C, Betancourt J, Ortiz S, et al. Barriers to the use of mobile health in improving health outcomes in developing countries: systematic review. J Med Internet Res. 2019;21:e13263. doi:10.2196/13263
37. Sarkar U, Karter AJ, Liu JY, et al. Social disparities in internet patient portal use in diabetes: evidence that the digital divide extends beyond access. J Am Med Inform Assoc. 2011;18:318–321. doi:10.1136/jamia.2010.006015
38. Petersen C, Adams SA, DeMuro PR. mHealth: don’t forget all the stakeholders in the business case. Medicine. 2015;4:e4. doi:10.2196/med20.4349
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.