")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Influencing Factors of Treatment Outcomes Among Patients with Pulmonary Tuberculosis: A Structural Equation Model Approach
Authors Liu K , Zhang M, Luo D, Zheng Y, Shen Z, Chen B , Jiang J
Received 4 May 2023
Accepted for publication 9 July 2023
Published 4 August 2023 Volume 2023:16 Pages 2989—2999
DOI https://doi.org/10.2147/PRBM.S419906
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Kui Liu,1,* Mengdie Zhang,2,* Dan Luo,3 Yan Zheng,4 Zhenye Shen,4 Bin Chen,1 Jianmin Jiang1,5
1Department of Tuberculosis Control and Prevention, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang Province, People’s Republic of China; 2Department of Social Medicine of School of Public Health, Zhejiang University School of Medicine, Hangzhou, Zhejiang Province, People’s Republic of China; 3Department of Public Health, Hangzhou Medical College, Hangzhou, Zhejiang Province, People’s Republic of China; 4Department of Tuberculosis Control and Prevention, Fenghua Center for Disease Control and Prevention, Ningbo, Zhejiang Province, People’s Republic of China; 5Key Laboratory of Vaccine, Prevention and Control of Infectious Disease of Zhejiang Province, Zhejiang Provincial Center for Disease Control and Prevention, Hangzhou, Zhejiang Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Chen; Jianmin Jiang, Email [email protected]; [email protected]
Background: Pulmonary tuberculosis (PTB) is a serious infectious disease, and the factors and pathways that influence final treatment outcomes are unclear. Here, we aimed to assess the factors that influence treatment outcomes in patients with PTB using a structural equation model.
Methods: Participants completed a questionnaire covering demographics, understanding of PTB, psychological status, and history of medical treatment. Exploratory factor analysis and reliability testing were performed, and a structural equation model was constructed using the SPSS and Amos software.
Results: A total of 251 participants were enrolled. Symptoms of depression were observed in 94.4% of participants, whereas 6% showed mild or greater anxiety. Through factor rotation, four common factors were extracted with a total variation of 66.15%. The structural equation model indicated that regular tuberculosis-related follow-up behaviour had a direct and positive effect on the final treatment outcome, with a path coefficient value of 0.20; the level of PTB understanding had a direct positive effect on the testing behaviour for PTB, with a path coefficient of 0.26; patients’ psychological characteristics had a direct negative impact on regular testing behaviour, with a path coefficient of − 0.13. The psychological characteristics and level of disease understanding of patients exerted indirect effects on the treatment outcome by affecting the way patients approached tuberculosis detection behaviour.
Conclusion: Interventions aimed at improving the treatment outcomes of patients with PTB should mainly focus on financial support and improvements in psychological status in addition to a greater understanding and knowledge of PTB. Furthermore, patients should be encouraged to undergo regular PTB testing during the follow up period, as this mediates the effect of other factors on treatment outcomes and also helps in achieving favourable treatment outcomes.
Keywords: pulmonary tuberculosis, structural equation model, treatment outcome, depression
Introduction
Pulmonary tuberculosis (PTB) remains one of the leading causes of deaths globally.1 Based on the Global Tuberculosis Report released in 2022, the estimated number of newly diagnosed tuberculosis (TB) cases and multidrug resistant TB (MDR-TB)/rifampicin resistant TB (RR-TB) in China was 780,000 and 33,000 in 2021, with an estimated total TB incidence of 55/100,000 and an estimated MDR/RR-TB incidence of 2.3/100,000, respectively. China is still listed as one of 30 high TB-burden countries, ranking third after Indonesia and India.2 With the development of standardised treatment regimens recommended by the World Health Organization, the majority of people with PTB can achieve favourable treatment outcomes.3 However, several factors, such as financial situation and depression status, can cause poor individual compliance, ultimately contributing to poor treatment outcomes.4,5 Following the outbreak of the COVID-19 pandemic in 2019, containment and control measures further amplified the contribution of these influencing variables to PTB.6 In order to inform effective and efficient interventions, it is vital to understand what factors influence the treatment outcomes of PTB patients.
Common statistical methods, such as logistic regression and Cox proportional hazards regression analysis, have been widely used to explore the factors related to TB treatment outcomes.6–8 Although these methods can be used to determine the direct effects of potential factors, interactions and indirect relationships can be missed. A structural equation model (SEM) provides a robust alternative approach that not only allows for the exploration of potential mechanisms comprising direct and indirect effects from different variables but also explains the complex pathways related to the development of unfavourable treatment outcomes.9
In this study, we constructed a SEM to assess the factors influencing treatment outcomes, including demographic characteristics, psychological status, knowledge of PTB, and detection behaviour relating to PTB. Given the influence of the COVID-19 pandemic, the exploration of significant pathways and mediators associated with patient treatment outcomes will help to inform effective interventions.
Methods
Overview of the Study Area
The site of our study was the Fenghua county of Zhejiang Province. Fenghua county is located in the eastern area of Zhejiang Province, belonging to the Ningbo Municipality (Figure 1). It consists of 11 districts and 26 communities, with a cover area of 1253 km2. Fenghua county has one designated PTB hospital for case identification and 26 community health service centres implementing the directly observed treatment of short course strategy (DOTs) intervention.
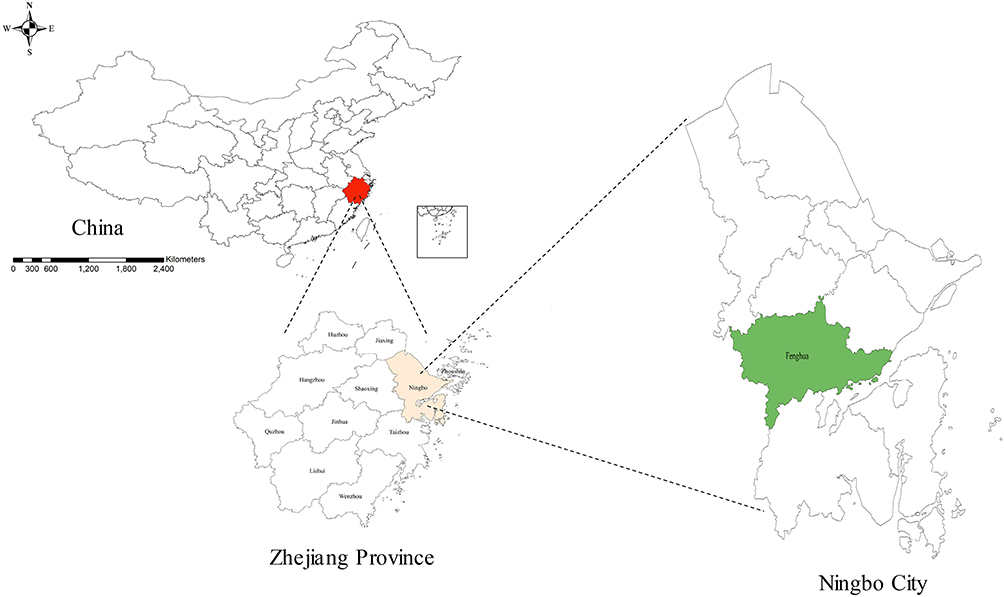 |
Figure 1 Location of the Fenghua county in Ningbo Municipality. |
Study Design, Procedures, and Participants
All locally diagnosed PTB cases during 2019–2020 in Fenghua county were selected. A total of 502 newly diagnosed PTB cases were notified in the Tuberculosis Information Management System (TBIMS) during the study period. We retrospectively traced the patients with PTB in 2022, and 301 of these participants provided informed consent and answered the questionnaires. The questionnaires were completed in face-to-face or through telephone interviews by trained investigators in the local Center for Disease Control and Prevention (CDC) and community doctors. The contents of the questionnaires included 1) gender, age, income, education, and other general demographic characteristics; 2) understanding of PTB, including the symptoms, prevention, curability, and its possible transmission; 3) psychological characteristics, assessed through the Center for Epidemiologic Studies Depression Scale (CES-D)10 and Self-rating Anxiety Scale (SAS);11 and 4) tuberculosis detection behaviour, characterised by whether the patient adhered to a recommended sputum and chest X-ray examination regimen during the follow-up period, as determined from the TBIMS or Hospital Information System (HIS) in the local designated hospital. The questionnaire was designed and performed by our research group with the language of Chinese. The Chinese translations of the CES-D and SAS (in Chinese) are widely used in China and have a high internal consistency.12 Ultimately, a total of 251 participants satisfactorily completed the questionnaires without logical errors and were included in the analysis.
Definition
All individuals with suspected PTB were diagnosed in accordance with the latest version of diagnostic criteria in China, using pathological examination, chest imaging, and other related auxiliary examinations. In this study, the cases comprised bacteriologically confirmed and clinically diagnosed patients, and cases were excluded if the further results from phenotypic or genotypic methods implied a possibility of drug resistance (Figure 2). Treatment outcomes were classified as completion of the treatment course, cure, and others (failure or adverse reaction). All definitions conform to the National Diagnostic Criteria for Pulmonary Tuberculosis (WS288-2017) and Classification of Tuberculosis (WS196-2017).13,14 With respect to the assessment of psychological characteristics, a CES-D score ≤15 indicated no symptoms of depression, 16–19 indicated probable symptoms of depression, and ≥20 indicated definite symptoms of depression. A SAS score <50 was considered to indicate no anxiety, 50–59 mild anxiety, 60–69 moderate anxiety, and ≥70 severe anxiety.
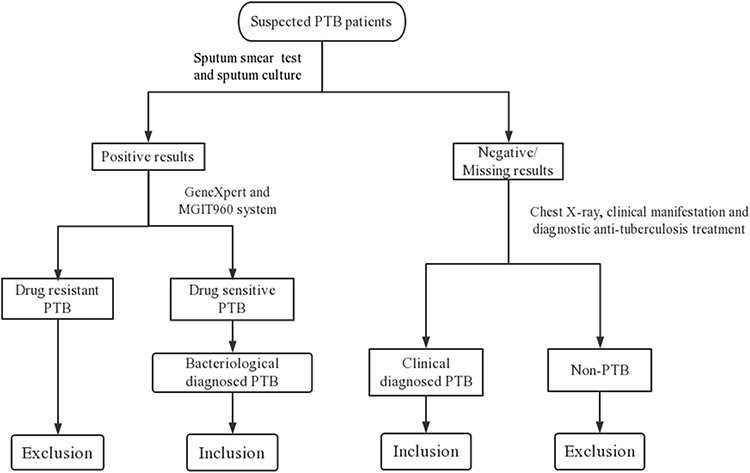 |
Figure 2 Flow chart of the included PTB patients in the study. |
Ethical Approval
This study was approved by the Ethics Committee of Zhejiang Provincial Center for Disease Control and Prevention; informed consent was obtained from all participants (2022–032-01). All data utilised in this study followed the Law of the Prevention and Treatment of Infectious Diseases in the People’s Republic of China and complied with the Declaration of Helsinki.
Statistical Analysis
The general epidemiological characteristics of the participants, tests of the reliability, and validity of questionnaire data were performed using SPSS 24.0 (IBM Corp., Armonk, NY, USA). Exploratory factor analysis was firstly used to identify the observed variables corresponding to each latent variable that likely affected the treatment outcomes of patients with PTB. Then, each dimensionality was evaluated for its reliability. Finally, the structural relationships among variables associated with treatment outcomes in patients were analysed using the Amos 24.0 software. The following fit indices were used to evaluate the overall model: root mean square error of approximation (RMSEA), standardised root mean squared residual (SRMR), comparative fit index (CFI), incremental fit index (IFI), Tucker-Lewis index (TLI), the goodness-of-fit index (GFI), and the adjusted GFI (AGFI), in which the CFI, GFI, AGFI, IFI, and TLI values greater than 0.90, and RMSEA and SRMR values less than 0.08 indicate an acceptable fit.15,16
Results
General Characteristics of the Participants
The characteristics of the study participants are summarised in Table 1. The study included 251 participants; of these, 69.7% were male and 67.7% were aged > 35 years old. Most of the participants were employed as manual labourers, and almost 75% had not completed senior high school. The annual family income for 83.3% of the participants was <RMB 120,000. Most study participants (95.2%) had lived locally for more than six months. Definite symptoms of depression were exhibited by 94.4% of study participants, whereas 6.0% exhibiting mild or moderate symptoms of anxiety. The majority of participants (95.6%) were classified as having completed the treatment course or as cured.
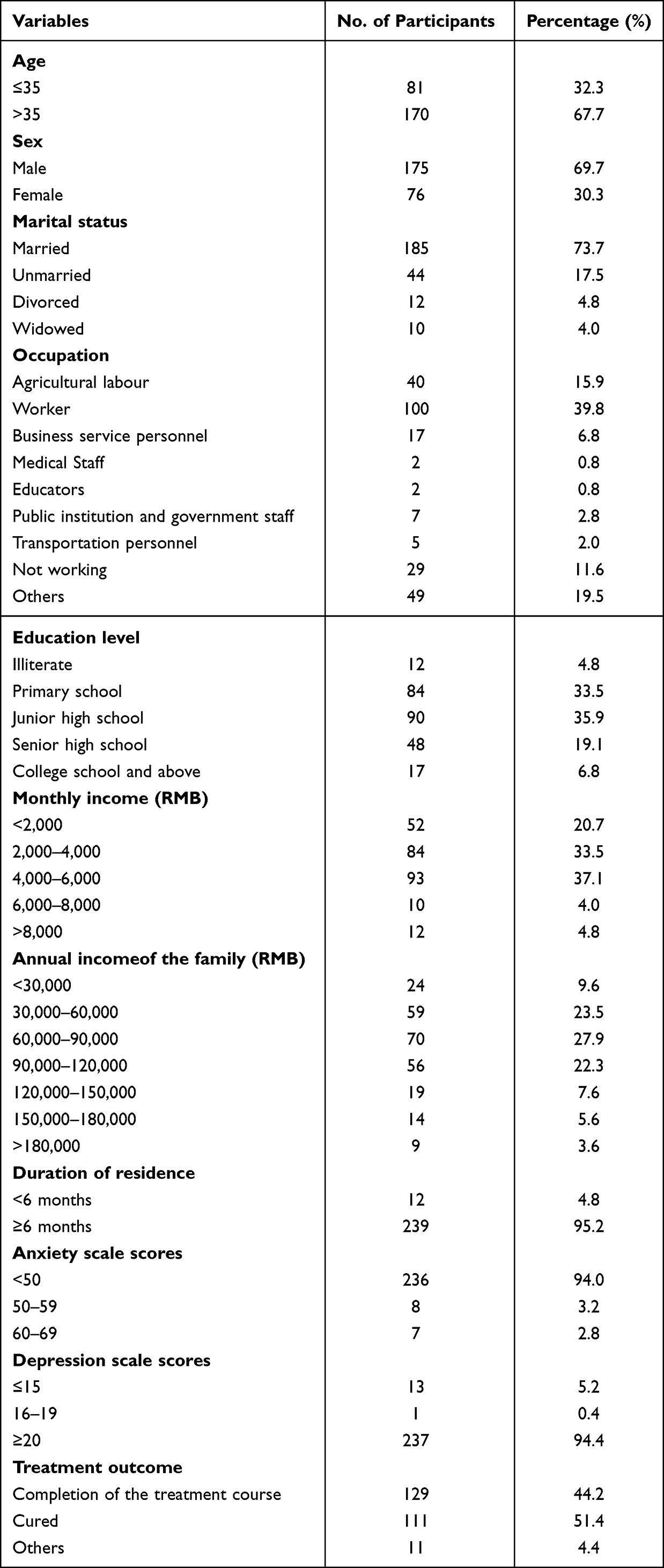 |
Table 1 General Characteristics of the Study Participants (N = 251) |
Exploratory Factor Analysis
In this study, participant demographic variables, anxiety scale score, depression scale score, understanding of PTB, and participation in regular sputum and chest X-ray examinations were included in the exploratory factor analysis. The Kaiser–Meyer–Olkin test value (0.628) and the approximate χ2 of Bartlett’s test of sphericity (728.782; degrees of freedom = 55, P < 0.001), indicated possible correlations among the included variables and that further factor analysis needed to be carried out. The principal component analysis method was used to extract factors. The factor was rotated using the Kaiser normalisation maximum variance method, which converged after six iterations, with the eigenvalues more than 1. Combined with the scree plot, four common factors were extracted, with a total variation of 66.15%. According to the variant content of the common factors, common factor 1 was defined as population characteristics, common factor 2 as PTB detection behaviour, common factor 3 as psychological characteristics, and common factor 4 as PTB understanding level (Table 2).
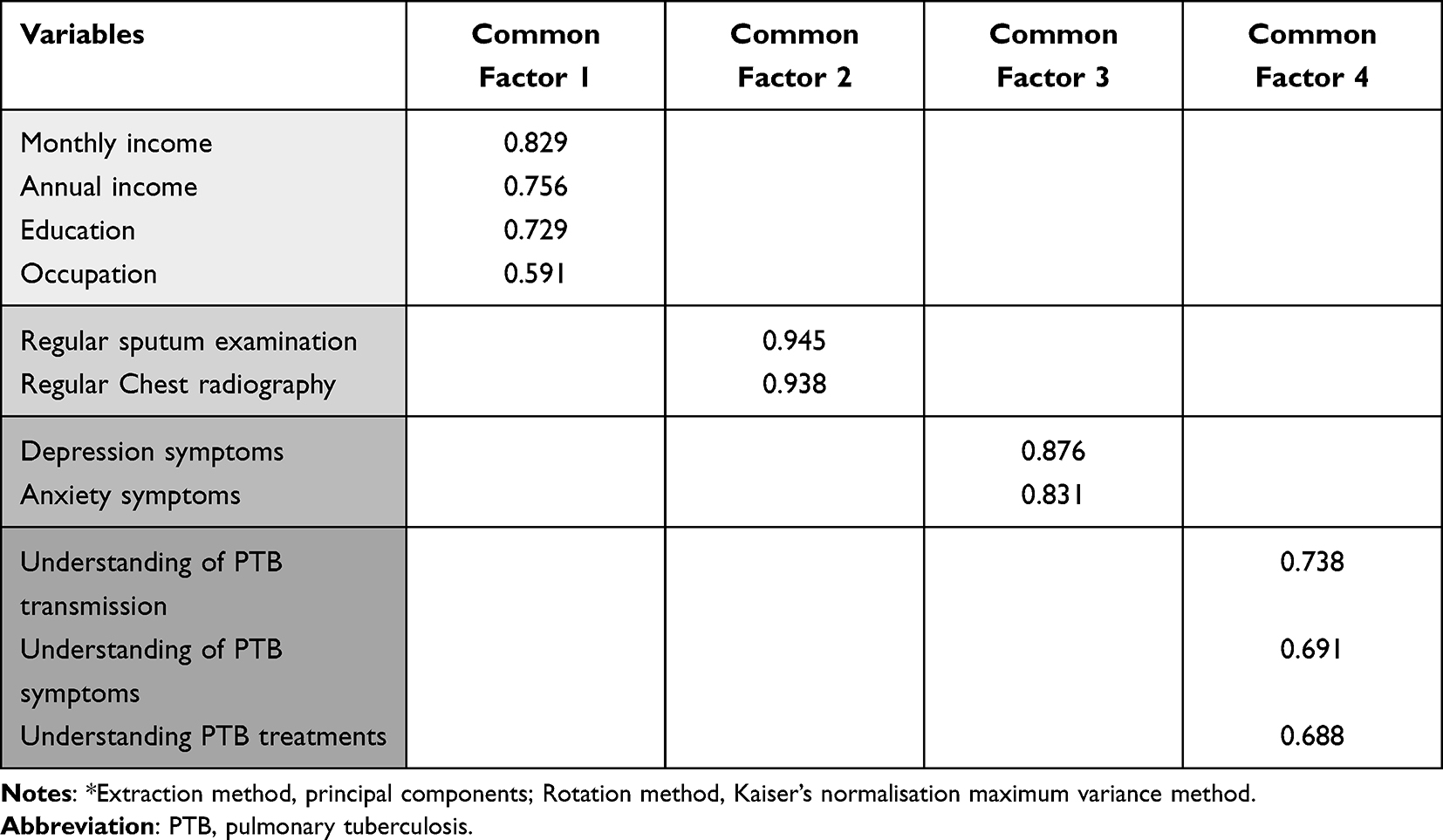 |
Table 2 The Component Matrix After Rotation* |
Questionnaire Reliability Test
Following exploratory factor analysis, four dimensions above were further analysed through reliability test. Reliability analysis showed that Cronbach’s α coefficients of all dimensions were greater than 0.7, and only one dimension was slightly less than 0.6 (Table 3).
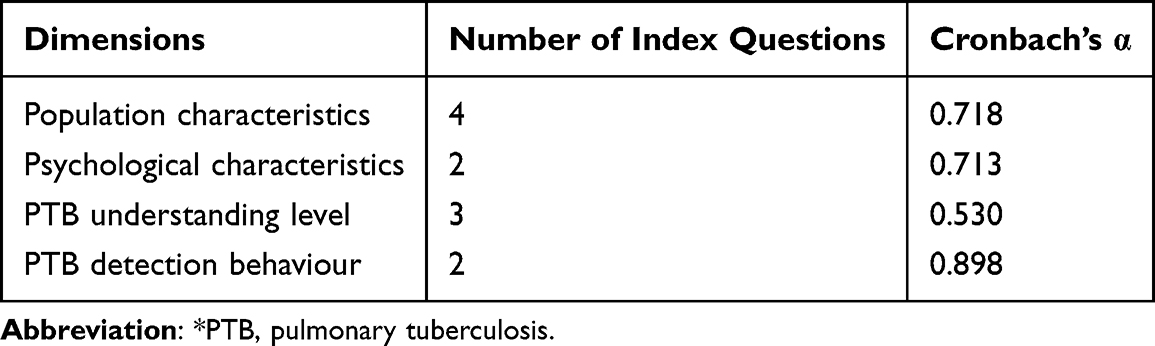 |
Table 3 Reliability Tests of four Dimensions* |
Construction and Modification of the Structural Equation Model
Our sample size of 251 meets the requirement for a sample size greater than 10 times the number of included variables. Based on exploratory factor analysis combined with available knowledge, four latent variables covering 12 observed variables were included in the SEM with a comparative well fitness. The final path diagram of the SEM and its fit indices with factor loading are shown in Figure 3 and Table 4, respectively. The fit indices for the SEM are presented in Table 5. The results demonstrated that the regular PTB-related detection behaviour had a direct and positive effect on the final treatment outcome, with a path coefficient value of 0.20. Additionally, the level of PTB understanding had a direct positive effect on the detection behaviour of PTB, with a path coefficient of 0.26, whereas the psychological characteristics (path coefficient −0.13) had a direct negative impact on PTB detection behaviour. Furthermore, the psychological characteristics and level of disease understanding exerted indirect effects on the treatment outcome by affecting detection behaviour during the follow-up period.
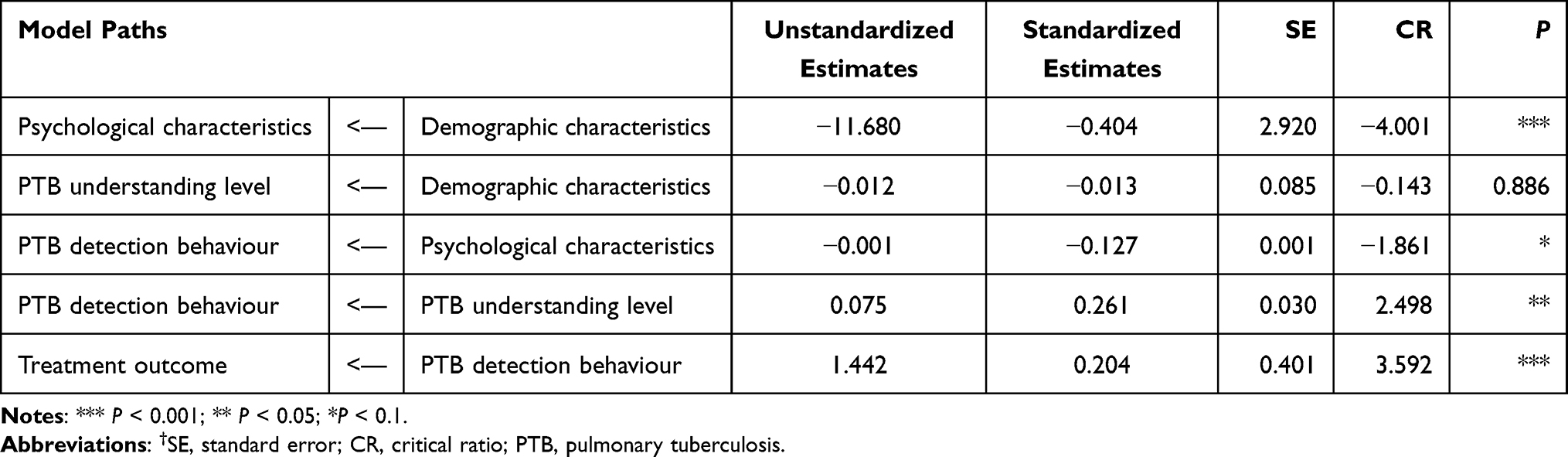 |
Table 4 Test Results of Path Relationship† |
 |
Table 5 Fit Indices of the Structural Equation Model* |
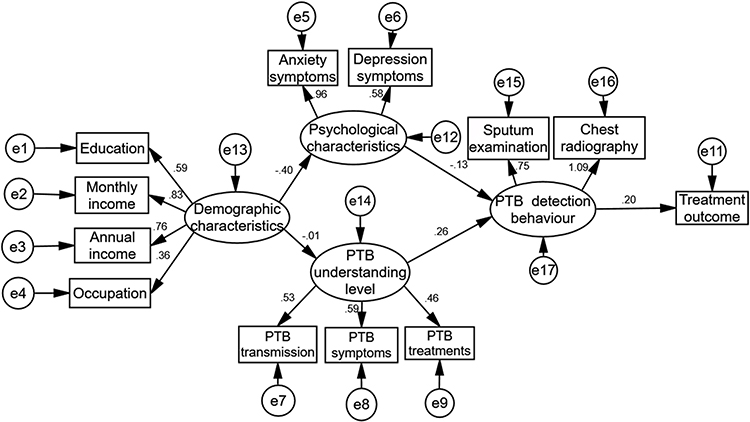 |
Figure 3 Structural equation model for treatment outcomes. |
Discussion
PTB is an infectious disease caused by Mycobacterium tuberculosis.17 Individuals experiencing this disease commonly require more than six months of treatment and are subject to discrimination and economic burden.18 Although enormous success has been achieved in the prevention and treatment of PTB recently, challenges such as the increase in drug-resistant PTB and the influence of the COVID-19 pandemic on individuals and health care systems can result in unsatisfactory treatment outcomes for patients with PTB.19 This study investigated the associations between treatment outcomes and variables such as regular detection behaviour, understanding of PTB, psychological characteristics, and population characteristics. To our knowledge, this is the first study to use a SEM to analyse the complex relationship between these factors, an approach that can provide a clearer understanding of the pathways mediating treatment outcomes and a new perspective for improving the treatment outcomes and management of patients with PTB.
In the present study, the fit indices of the SEM showed that standard PTB-related detection behaviour is the main factor that directly affects the treatment outcomes of patients with PTB. Methods of PTB detection mainly include regular sputum examination and chest X-ray examination, following the advice of the designated hospital’s doctor. During the treatment course, five sputum and two chest X-ray examinations in different months are required to understand dynamic changes in the illness status of patients with PTB. To some extent, regular detection behaviour also reflects which patients show comparatively good adherence to the treatment regimen, which is beneficial for achieving a favourable treatment outcome and reducing the occurrence of drug resistance.20,21
Previous studies indicated that depression is a critical cause of poor treatment compliance and that it even causes unfavourable outcomes.22 Our results showed that psychological characteristics had a direct negative impact on PTB detection behaviour but did not affect the treatment outcome directly. It is suggested that patients with poor psychological status are more likely to have irregular PTB detection behaviour. A previous study demonstrated that patients with PTB having psychological problems commonly had less awareness of the importance of regular testing and treatment, and related treatment compliance is also likely to decline.23 Furthermore, it has been found that during the COVID-19 pandemic, some patients with PTB developed psychological problems, such as depression and anxiety, due to the contagiousness of the disease itself, complexity of the treatment process, and inevitable financial burden.24 It has been reported that compared to that in the general population, the prevalence of depression and anxiety is higher among patients with PTB.25,26 In our study, the depression score, as assessed by CES-D, among patients with PTB during the COVID-19 pandemic reached 27.71 ± 9.35 (mean ± standard deviation), which was higher than that reported in previous studies of the general population (13.24 ± 10.33) and patients with PTB (15.86 ± 8.26).12,27 Indeed, the sharp increase in depression score may be inseparable from the COVID-19 pandemic.28 Thus, comprehensive interventions for PTB cases should not only providing needful aid funds and drug for free but also the indispensable psychological care to improve treatment adherence. It is also suggested that the health detection package including psychological care should be considered in the routine examination of PTB cases.
Our findings suggest that the psychological status of patients is considerably affected by their socio-demographic characteristics, with individual monthly income and annual income of the whole family having the greatest effect. Patients with high incomes commonly had comparatively low levels of depression and anxiety; those with better economic circumstances may be able to handle the financial pressure more effectively, for example from work interruption, during the treatment process.29 Patients with PTB not only have to bear the medical expenses for disease diagnosis and treatment but also suffer from the impact of reduced productivity and income caused by health damage.30 Although the strategy of free diagnosis and treatment of tuberculosis has been implemented in China, patients still have to bear high costs; hence, it is necessary to consider providing more adequate financial support for patients with PTB.31
The level of understanding of PTB was another factor that had a direct positive effect on the detection behaviour of patients with PTB. The higher the level of understanding of the disease, the higher was the level of regular detection and compliance. On the other hand, the patients with PTB who lacked disease-related knowledge often lost confidence during the prolonged management phase, resulting in poor treatment compliance.27,32 Previous studies have shown that a lack of knowledge of PTB can lead to negative attitudes and behaviours in patients.33 Therefore, educating patients about PTB can improve their health-related behaviours during initial treatment and help them comply with standard PTB detection and treatment requirements, thereby leading to better treatment outcomes.
This study has some limitations. Firstly, the samples were collected from one county, and information collection was carried out using a retrospective questionnaire; therefore, it may be affected by recall bias. Secondly, due to the limited designs, some relationships between population characteristics and PTB detection behaviour may have remained undetected. Finally, due to the limited sample size, the further research stratified by age was not performed, which may result in some bias. Nevertheless, our study provides useful insights into the factors associated with successful PTB treatment outcomes, which should be beneficial for the further advancement of clinical diagnosis and treatment. Besides, larger retrospective or prospective analyses are still needed to confirm our findings.
Conclusion
Interventions aimed at improving the treatment outcomes of patients with PTB should mainly focus on providing financial support, regular PTB knowledge education, and psychological counselling to patients during the treatment period. More importantly, monitoring of regular PTB detection behaviour should be strengthened, which mediates the effect of other factors on treatment outcomes and also are essential to favourable treatment outcomes.
Abbreviations
TB, Tuberculosis; PTB, Pulmonary tuberculosis; SEM, Structural equation model; DOTs, Directly observed treatment of short course strategy; TBIMS, Tuberculosis Information Management System; CDC, Center for Disease Control and Prevention; CES-D, Center for Epidemiologic Studies Depression Scale; SAS, Self-rating Anxiety Scale; HIS, Hospital Information System; RMSEA, Root mean square error of approximation; SRMR, Standardised root mean squared residual; CFI, Comparative fit index; IFI, Incremental fit index; TLI, Tucker-Lewis index; GFI, Goodness-of-fit index; AGFI, Adjusted goodness-of-fit index; SE, Standard error; CR, Critical Ratio; Df, Degrees of freedom.
Data Sharing Statement
All data and materials were included in this paper. The corresponding author could provide all data upon reasonable request.
Ethics Declaration
Our study was approved by the Ethics Committee of the Zhejiang Provincial Center for Disease Control and Prevention (ZJCDC). Besides, all data used in this study followed the Law of the Prevention and Treatment of Infectious Diseases in the People’s Republic of China.
Acknowledgments
We appreciated the local center for disease control and prevention (CDCs), community healthcare centers, and TB designated hospitals to implement our study. We also thanked the assistance from Leonardo Martinez in Boston University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Zhejiang Provincial Medical and Health Project (Grant Nos. 2021KY618 and 2019RC135). Bin Chen is the recipient of the foundations and was responsible for the manuscript in our study.
Disclosure
The authors declare no conflict of interest.
References
1. Zhan Y, Wang Y, Zhang W, Ying B, Wang CJJo CM. Diagnostic accuracy of the artificial intelligence methods in medical imaging for pulmonary tuberculosis: a systematic review and meta-analysis. J Clin Med. 2022;12(1):303. doi:10.3390/jcm12010303
2. Organization GWH. Global Tuberculosis Report 2022. Organization GWH; 2022.
3. Bloom BR, Atun R, Cohen T, et al. Tuberculosis. In: Holmes KK, Bertozzi S, Bloom BR, Jha P, editors. Major Infectious Diseases. Washington (DC): The International Bank for Reconstruction and Development / The World Bank © 2017 International Bank for Reconstruction and Development / The World Bank; 2017.
4. Rouf A, Masoodi MA, Dar MM, Khan SMS, Bilquise R. Depression among Tuberculosis patients and its association with treatment outcomes in district Srinagar. J Clin Tuberc Other Mycobact Dis. 2021;25:100281. PMID: 34888421; PMCID: PMCPMC8637130. doi:10.1016/j.jctube.2021.100281
5. Koo HK, Min J, Kim HW, et al. Prediction of treatment failure and compliance in patients with tuberculosis. BMC Infect Dis. 2020;20(1):622. PMID: 32831044; PMCID: PMCPMC7446045. doi:10.1186/s12879-020-05350-7
6. Daly M, Robinson E. Depression and anxiety during COVID-19. Lancet. 2022;399(10324):518. PMID: 35123689; PMCID: PMCPMC8813060. doi:10.1016/s0140-6736(22)00187-8
7. Méchaï F, Bachelet D, Han L, et al. Tuberculosis treatment outcomes among precarious patients in France. Infect Dis. 2022;52(7):389–395. PMID: 36064101. doi:10.1016/j.idnow.2022.08.004
8. Liu K, Ai L, Pan J, et al. Survival analysis and associated factors for pulmonary tuberculosis death: evidence from the information system of tuberculosis disease and mortality surveillance in China. Risk Manag Healthc Policy. 2022;15:1167–1178. PMID: 35669895; PMCID: PMCPMC9166951. doi:10.2147/rmhp.S368593
9. Brunner J, Austin PC. Inflation of Type I error rate in multiple regression when independent variables are measured with error. Can J Stat. 2009;37(1):33–46. doi:10.1002/cjs.10004
10. Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. doi:10.1177/014662167700100306
11. Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
12. Jie Zhang ZW, Ge F, Juan L, Han B, Chen Z. Development of the Chinese age norms of CES-D in urban area. Chin Ment Health J. 2010;24(2):139–143.
13. Commission NHaFP. Classification of Tuberculosis. Beijing: National Health and Family Planning Commission; 2018.
14. China MoPHo. China: Diagnostic Criteria for Pulmonary Tuberculosis. Beijing: People’s Medical Publishing House; 2008.
15. Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Modeling. 1999;6(1):1–55. doi:10.1080/10705519909540118
16. Kenny DA, McCoach DB. Effect of the number of variables on measures of fit in structural equation modeling. Struct Equ Model. 2003;10:333–351. doi:10.1207/S15328007SEM1003_1
17. Yu Y, Wu B, Wu C, Wang Q, Hu D, Chen W. Spatial-temporal analysis of tuberculosis in Chongqing, China 2011–2018. BMC Infect Dis. 2020;20(1):531. doi:10.1186/s12879-020-05249-3
18. Lal AA, Rapose A, Rapose A. Latent tuberculosis infection: treatment initiation and completion rates in persons seeking immigration and health care workers. Am J Med. 2019;132(11):1353–1355. doi:10.1016/j.amjmed.2019.04.036
19. Zhi-ping Z, Xian-xiang LI, Yu-feng WEN, Chao J, Yu Z. Analysis of drug resistance characteristic of 342 sputum culture positive pulmonary tuberculosis. Prev Med. 2015;42(03):522–525.
20. Jaiswal A, Ogden JA, Porter JD, et al. Adherence to tuberculosis treatment: lessons from the urban setting of Delhi, India. Trop Med Int Health. 2003;8(7):625–633. doi:10.1046/j.1365-3156.2003.01061.x
21. Garner P, Munro S, Volmink J. Promoting adherence to tuberculosis treatment. Bull World Health Organ. 2007;85(5):404–406. PMCID: PMC PMC2636642. doi:10.2471/blt.06.035568
22. Ruiz P, Zamudio C, Canaza L, Otero L, Kruger H, Seas C. Association of major depressive episode with negative outcomes of tuberculosis treatment. PLoS One. 2013;8(7):e69514. PMCID: PMCPMC3726639. doi:10.1371/journal.pone.0069514
23. Naidoo P, Dick J, Cooper D. Exploring tuberculosis patients’ adherence to treatment regimens and prevention programs at a public health site. Qual Health Res. 2009;19(1):55–70. PMID: WOS:000261732300006. doi:10.1177/1049732308327893
24. Dos Santos AP, Lazzari TK, Silva DR. Health-related quality of life, depression and anxiety in hospitalized patients with tuberculosis. Tuberc Respir Dis. 2017;80(1):69–76. PMID: 28119749; PMCID: PMCPMC5256348. doi:10.4046/trd.2017.80.1.69
25. Aghanwa HS, Erhabor GE. Demographic/socioeconomic factors in mental disorders associated with tuberculosis in southwest Nigeria. J Psychosom Res. 1998;45(4):353–360. PMID: WOS:000075755100006. doi:10.1016/S0022-3999(98)00006-3
26. Westaway MS, Wolmarans L. Depression and self-esteem: rapid screening for depression in black, low literacy, hospitalized tuberculosis patients. Soc Sci Med. 1992;35(10):1311–1315. PMID: 1439914. doi:10.1016/0277-9536(92)90184-r
27. Qiu L, Yang Q, Tong Y, Lu Z, Gong Y, Yin X. The mediating effects of stigma on depressive symptoms in patients with tuberculosis: a structural equation modeling approach. Front Psychiatry. 2018;9:618. PMID: 30534088; PMCID: PMCPMC6275230. doi:10.3389/fpsyt.2018.00618
28. Santomauro DF, Herrera AMM, Shadid J, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398(10312):1700–1712. PMID: WOS:000715856000024. doi:10.1016/S0140-6736(21)02143-7
29. Tanimura T, Jaramillo E, Weil D, Raviglione M, Lonnroth K. Financial burden for tuberculosis patients in low- and middle-income countries: a systematic review. Eur Respir J. 2014;43(6):1763–1775. PMID: 24525439; PMCID: PMCPMC4040181. doi:10.1183/09031936.00193413
30. Liu Y, Xu CH, Wang XM, et al. Out-of-pocket payments and economic consequences from tuberculosis care in eastern China: income inequality. Infect Dis Poverty. 2020;9(1):14. PMID: 32019611; PMCID: PMCPMC7001258. doi:10.1186/s40249-020-0623-8
31. Sangsang Qiu HL, Zhang S, Jiang W, Huang L, Wang J. Comparative study on the economic burden of patients with tuberculosis. J Nanjing Med Univ. 2014;14(05):354–358.
32. Buregyeya E, Mitchell EM. Tuberculosis infection control knowledge and attitudes among health workers in Uganda: a cross-sectional study. BMC Infect Dis. 2016;16(1). PMCID: PMCPMC4986352. doi:10.1186/s12879-016-1740-7
33. Kigozi NG, Heunis JC, Engelbrecht MC, van Rensburg APJ, van Rensburg HC. Tuberculosis knowledge, attitudes and practices of patients at primary health care facilities in a South African metropolitan: research towards improved health education. BMC Public Health. 2017;17. PMID: WOS:000412684800006. doi:10.1186/s12889-017-4825-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.