Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Influences of Resistance versus Aerobic Exercise on Physiological and Physical Fitness Changes in Previously Inactive Men with Obesity: A Prospective, Single-Blinded Randomized Controlled Trial
Received 21 September 2019
Accepted for publication 16 January 2020
Published 4 February 2020 Volume 2020:13 Pages 267—276
DOI https://doi.org/10.2147/DMSO.S231981
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Bokun Kim,1 Seungyeol Kim2
1Faculty of Sports Health Care, Inje University, Gimhae, Gyeongsangnamdo, Republic of Korea; 2College of Arts and Sports, Dong-A University, Busan, Republic of Korea
Correspondence: Seungyeol Kim
College of Arts and Sports, Dong-A University, 37 Nakdong-Daero 550beon-gil Saha-Gu, Busan 604-714, Republic of Korea
Tel +82 10 8890 0643
Email [email protected]
Purpose: The purpose of this study was to comparatively investigate changes in physiological and physical fitness in previously inactive men with obesity in response to aerobic exercise (AE) or resistance exercise (RE).
Methods: A total of 27 inactive men with obesity, aged 34– 60 years, attended a 90-min AE or RE program 3 days/week for 12 weeks. The subjects underwent assessments of energy intake (by a 3-day weighted dietary record), body weight (by a digital scale), body composition (by whole-body dual-energy X-ray absorptiometry), VO2max (by a cycling ergometer), muscle strength (by a Biodex System 3 dynamometer) and blood analysis.
Results: There were no significant interactions (P = 0.100∼ 0.730) among energy intake variables. RE led to decreased fat mass (− 4.39%, P < 0.05) and improved cardiorespiratory capacity (+11.66%, P < 0.05), as well as increases in lean mass (+2.12%, P < 0.01) and muscle strength variables (+8.41∼+11.00%, P < 0.01 for all), without significant weight change. Although AE induced decreases in fat mass (− 5.91%, P < 0.05) and weight (− 2.28%, P < 0.05) and improved cardiorespiratory capacity (+19.07%, P < 0.01), lean mass and muscle strength variables remained unchanged. RE showed a stronger positive influence than AE on lean mass (P = 0.003) and muscle strength variables (P = 0.001∼ 0.015), and RE and AE had similar influences on weight, fat mass, cardiorespiratory capacity and blood markers.
Conclusion: It may be an efficient exercise regimen to perform RE first and then utilize AE to maintain the changes that occur in response to RE.
Keywords: aerobic exercise, body composition, blood marker, cardiorespiratory capacity, obesity, muscle strength, resistance exercise, weight
Introduction
As dietary habits and lifestyle in Japan are now similar to those in Western countries, the prevalence of obesity among the adult population is approximately 30% and has increased nearly 1.5-fold over the last 30 years among men.1 Excessive fat accumulation induced by body weight gain is associated with a broad range of internal diseases, including cardiovascular disease, diabetes and nonalcoholic fatty liver disease.2,3 Muscle mass and strength decline caused by physical inactivity can also lead to musculoskeletal disorders, such as pain, and osteoarthritis, and physical performance decline.4–6 Accordingly, it is widely accepted that a countermeasure for these conditions is necessary.
The benefits of exercise for obesity are well documented. Exercise guidelines for weight reduction and health promotion include aerobic exercise (AE) and resistance exercise (RE) as a part of the exercise prescription. RE has been recommended to ameliorate glucose tolerance and glycosylated hemoglobin, as well as muscle mass and strength.7 AE can improve several metabolic markers and cardiorespiratory capacity and decrease weight and fat mass.8 However, recent studies have reported that RE may also be beneficial in reducing fat mass and improving cardiorespiratory capacity and that AE has a positive effect on the maintenance of muscle mass and strength during weight reduction.9–11 The discrepancy between existing reports is likely to lead to misunderstandings regarding the influences of AE and RE.
Based on this consideration, we comparatively investigated the influences of AE and RE on weight, body composition, blood markers and physical fitness in previously inactive men with obesity. In other words, we wished to explore whether RE or AE is more beneficial for the management of obesity-related conditions. For this question, we evaluated differences between the AE and RE groups in terms of changes in outcomes after a 12-week prospective, single-blinded randomized controlled trial (RCT).
Method
Experimental Design and Participants
Study participants were recruited from April 1–16, 2014, from the community via advertisements in newspapers and distributed study flyers. The study participants satisfied the following criteria: (1) aged between 30 and 64 years, (2) body mass index (BMI) greater than 25 kg/m2, (3) not restricted from exercising by a doctor and (4) not engaged in frequent exercise (≤1 session per week and ≤30 min per session). Of the applicants, 47 individuals were enrolled according to the study criteria. After the pre-intervention assessment, which was held on the 3rd, 4th, 10th and 11th of May, 2014, 11 participants were excluded for the following reasons: 1 of them was younger than 30 years, 4 of them had inadequate BMIs, 3 of them did not participate in the assessment, 1 of them had surgery and 2 of them dropped out. We performed a prospective, single-blinded RCT for the present study. The 38 eligible participants were assigned to one of the two intervention groups at a 1:1 ratio by a computerized method (EXCEL 2010; Microsoft Corp, Redmond, USA) using block randomization with stratification for age and VO2max. A research assistant who had no interaction with the participants generated the random allocation sequence and enrolled the participants. During the 12-week intervention, which was conducted from the 27th of May to the 15th of August, 2014, and the post-intervention assessment, which was held on the 16th, 17th, 23rd, 24th of August, 2014, 6 participants from the AE group and 5 participants from the RE group were excluded for failure to participate in the assessment, dropping out, having missing data, etc. (Figure 1). Consequently, a total of 27 participants who remained in the present study after the post-intervention assessment (n = 14 in the RE group and n = 13 in the AE group) were included in the final analysis. The study purpose and design were adequately explained to every participant before they gave written informed consent. This study was approved by the Institutional Review Board of the University of Tsukuba Hospital (ID: H25–156) and conducted in accordance with the guidelines proposed in the Declaration of Helsinki. The authors established the study design, conducted the statistical analysis and wrote the manuscript. However, to exclude any influence on the study, the authors did not engage in the intervention and assessments. Experienced trainers supervised the intervention, and well-trained staff carried out the assessments.
 |
Figure 1 Flow chart of the study subjects. |
Exercise Protocol
Both the AE and RE plans were designed to gradually increase the amount and intensity of exercise, and they were executed under the supervision of several experienced physical trainers at the University of Tsukuba. The RE program was performed for 3 days/week for 12 weeks. A one repetition maximum (1-RM) strength assessment was executed to adjust the load in resistance training machines, and approximately 50% of the 1-RM strength was adopted for the load. The exercise began with 20–30 min of warm-up and cool-down and was conducted on 6 RE machines (Techno Gym) for 60 min. The resistance program consisted of three sets of the following seven exercises: crunch, high lat pull down, seated row, chest press, leg press, leg extension and leg curl. Participants conducted 10–12 repetitions to failure for each set except crunch. Crunch was performed for approximately 15 repetitions with the participant’s body weight. Participants were allowed 1–2 min of rest between each set. When the participants could easily perform the recommended repetitions, the load was increased. The amount of load lifted was adjusted according to the results of the monthly direct 1-RM strength test. Our trainers provided verbal encouragement to ensure that the participants performed to volitional fatigue. This RE protocol was designed on the basis of the ACSM 2009 position paper on progression models in resistance training for healthy adults.12 A 90-min AE program was held 3 days/week for 12 weeks. Each session began with 10–15 min of warm-up activities, such as stretching. This warm-up was followed by the main exercise, consisting of 60 min of jogging and running outdoors. On rainy days, indoor exercise using stationary cycling constituted the main exercise. Each session concluded with 10–15 min of cool-down exercises. The duration of AE increased gradually from 30 to 40 min per session for the first 4 weeks to 60 min per session at 5 weeks, which was then sustained for the rest of the period. Participants were encouraged to exercise at or near 65% to 85% of their maximum heart rate level. This AE protocol was used in the Tanaka laboratory for years, and the safety and validity were fully verified by several studies.13–17 Heart rates were monitored by short-range telemetry (Polar RS400, Kempele, Finland). During the study period, every participant was asked not to conduct the trial-specific exercise activities outside of the exercise intervention. We also asked participants to not change anything regarding their lifestyle and diet for 12 weeks.
Daily Energy Intake
Total energy intake (Kcal/d) and the intake amounts (g/d) of each nutrient (carbohydrate, protein and fat) were assessed before and after the 12-week intervention using a 3-day weighed dietary record method performed by a skilled dietitian.
Anthropometric Parameters and Body Composition
Height was assessed to the nearest 0.1 cm using a wall-mounted stadiometer (YG-200; Yagami, Nagoya, Japan), and body weight was assessed to the nearest 0.1 kg using a digital scale in light clothing and without shoes (TBF-551; Tanita, Tokyo, Japan). BMI was calculated as weight (kg) divided by height (m) squared. Body composition, including lean mass, fat mass and percentage of fat mass, was assessed using dual-energy X-ray absorptiometry (DEXA; QDR 4500, Hologic Inc., Bedford, MA). To evaluate muscle mass, lean mass was adopted in this study.
Knee Extensor Strength
Isokinetic knee extensor strength was assessed using a Biodex System 3 dynamometer (Biodex Medical Systems, Shirley, NY). We assessed isokinetic muscle strength at an angular velocity of 60°/s. For the isokinetic assessment of angular velocity at 60°/s, the participants executed 3 maximal extensions. The highest muscular force output at any moment during a repetition was defined as the peak torque, reported in absolute terms (N m). The amount of work accomplished for an entire set defined the total work and is reported as an absolute (W), while the average of total work divided by time defined the average power and is reported as an absolute (J). Every assessment was performed on each leg, and the average strength of both legs was calculated for lower-extremity muscle strength. This method has been previously described in detail.10,18,19
Cardiorespiratory Capacity Assessment
The participants conducted a maximal graded exercise test using a cycling ergometer (828E; Monark, Stockholm, Sweden) to assess maximal oxygen uptake (VO2max). We employed the criteria described by Tanaka et al to assess VO2max.20 After a 2-min warm-up at 15 W, the participants began the actual exercise protocol at the 30 W level. The workload was increased every 1 min by 15 W until volitional exhaustion. During the test, ventilation and expired gases were assessed using an open-circuit, computerized, indirect calorimeter (AE-310S, Minato Medical Science, Osaka, Japan), and heart rate was monitored using an electrocardiogram monitor (Dyna Scope, Fukuda Denshi, Tokyo, Japan).
1-RM Strength Assessment
Participants in the RE group were asked to execute a 1-RM strength test. Following a learning phase, the participants conducted a warm-up at a relatively light load. The warm-up was followed by a gradually increasing load until they achieved the 1-RM strength within 5 attempts, with 1–2 min of recovery between sets. We performed the tests taking into consideration assisting the recovery and reducing the influence of fatigue. The tests were alternated between the upper and lower extremities.
Blood Markers
Blood samples were collected in the morning after an overnight (≥8 h) fast. Serum total cholesterol and triglycerides were determined by the enzymatic method; serum high-density lipoprotein (HDL) cholesterol by the heparin-manganese precipitation method; serum low-density lipoprotein (LDL) cholesterol by the method of Friedewald et al; fasting plasma glucose (FPG) by a glucose oxidase method; and aspartate aminotransferase (AST), alanine aminotransferase (ALT), and gamma-glutamyl transferase (γ-GTP) by the transferable method of the Japan Society of Clinical Chemistry. We calculated surrogate markers for insulin resistance (HOMA-IR). Latex agglutination was employed to measure hemoglobin (Hb) A1C.
Statistical Analysis
Values are expressed as the means ± standard deviations or standard errors. To verify the normal distribution of the data, the Shapiro–Wilk test was performed. The unpaired t-test was employed to assess the statistical significance of between-group differences at baseline. The comparison of variables before and after the intervention program was conducted using the paired t-test. To compare the changes between groups, we applied a two-way, repeated-measures analysis of variance (ANOVA), adjusted for age. An analysis of covariance (ANCOVA) was also performed to investigate the between-group difference in changes of whole-body lean and fat mass and physical fitness, adjusted for age and body weight change. P < 0.05 was considered to indicate statistical significance. Every statistical analysis was performed with SPSS software, version 21.0 (IBM Inc., Armonk, NY, USA).
Results
Table 1 shows the baseline values and changes in energy intake for each group over the course of the exercise program. At baseline, no significant differences were found in the variables between the two groups. After the program, significant changes were not detected in any of the variables within each group. There were no significant interactions (P = 0.100–0.730) for any of the variables between the two groups.
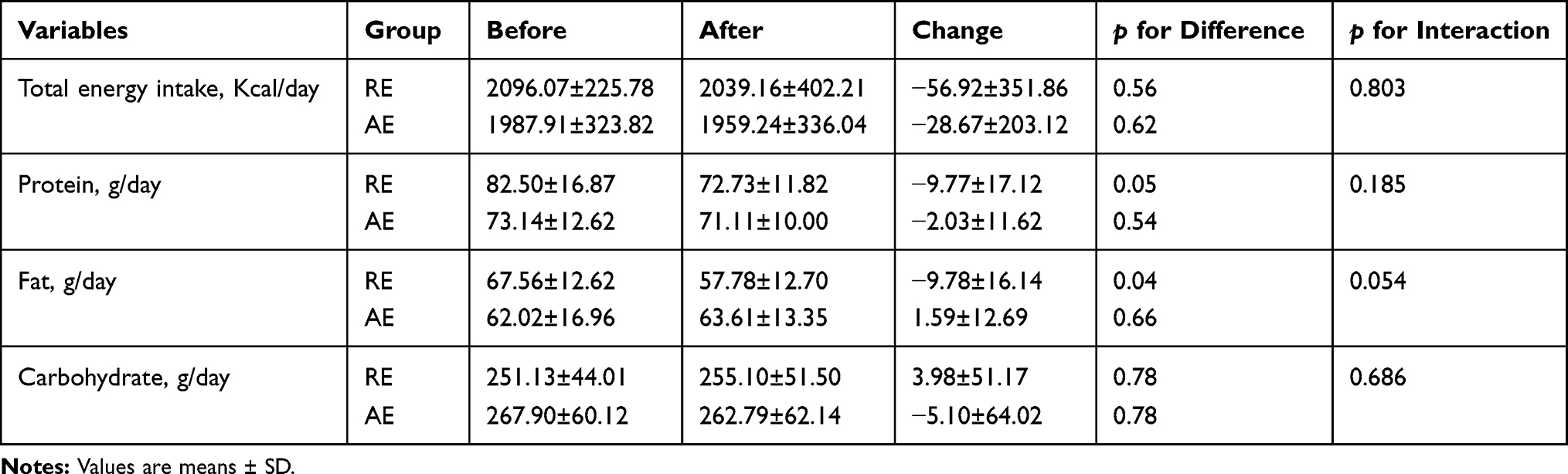 |
Table 1 Changes in Energy Intake Between the Resistance (n = 14) and Aerobic (n = 13) Groups |
The baseline values and changes in anthropometric parameters and body composition for each group (adjusted for age) are presented in Table 2. There were no significant differences between the two groups in any of the baseline measures. Significant changes were observed in body weight (−2.27%) and BMI (−2.33%) in the AE group, while RE did not induce significant changes in body weight (−0.16%) or BMI (−0.15%). Although body weight (−0.16%) was almost unchanged, lean mass (+2.06%) in the RE group was significantly increased. ANOVA revealed no significant interactions (P = 0.076–0.626) among any of the variables between the two groups except for lean mass (P = 0.003).
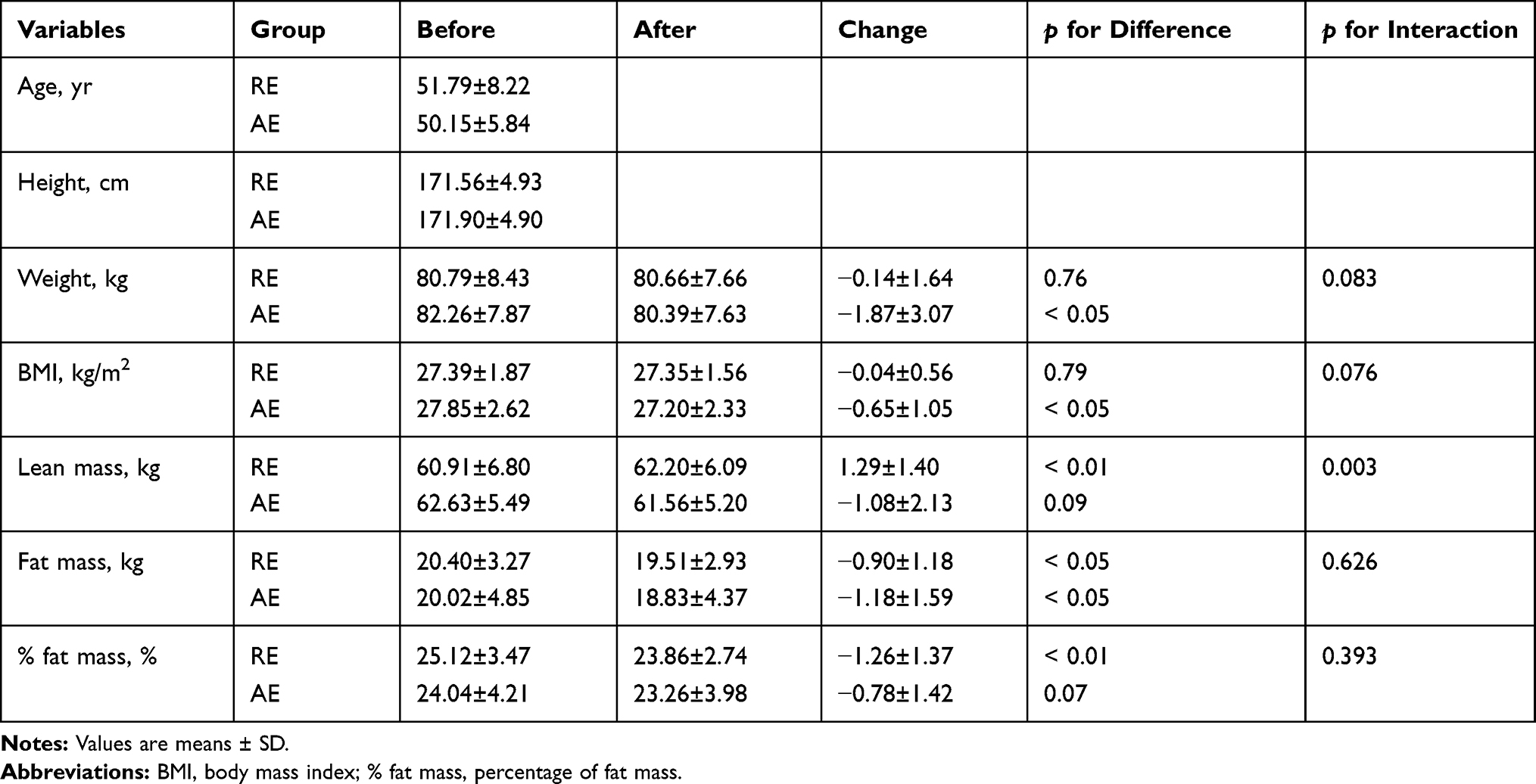 |
Table 2 Changes in Anthropometric Characteristics and Body Composition Between Resistance (n = 14) and Aerobic (n = 13) Group Adjusted for Age |
Table 3 contains the baseline values and changes in physical fitness for each group, adjusted for age. At baseline, no significant differences were found in any of the variables between the two groups. After completing each exercise program, a significant increase in VO2max was observed in both groups, but a significant interaction between the groups was not observed. For muscle strength variables, significant increases were detected in the RE group, while significant changes were not found in the AE group. There were significant interactions for all muscle strength variables between the two groups.
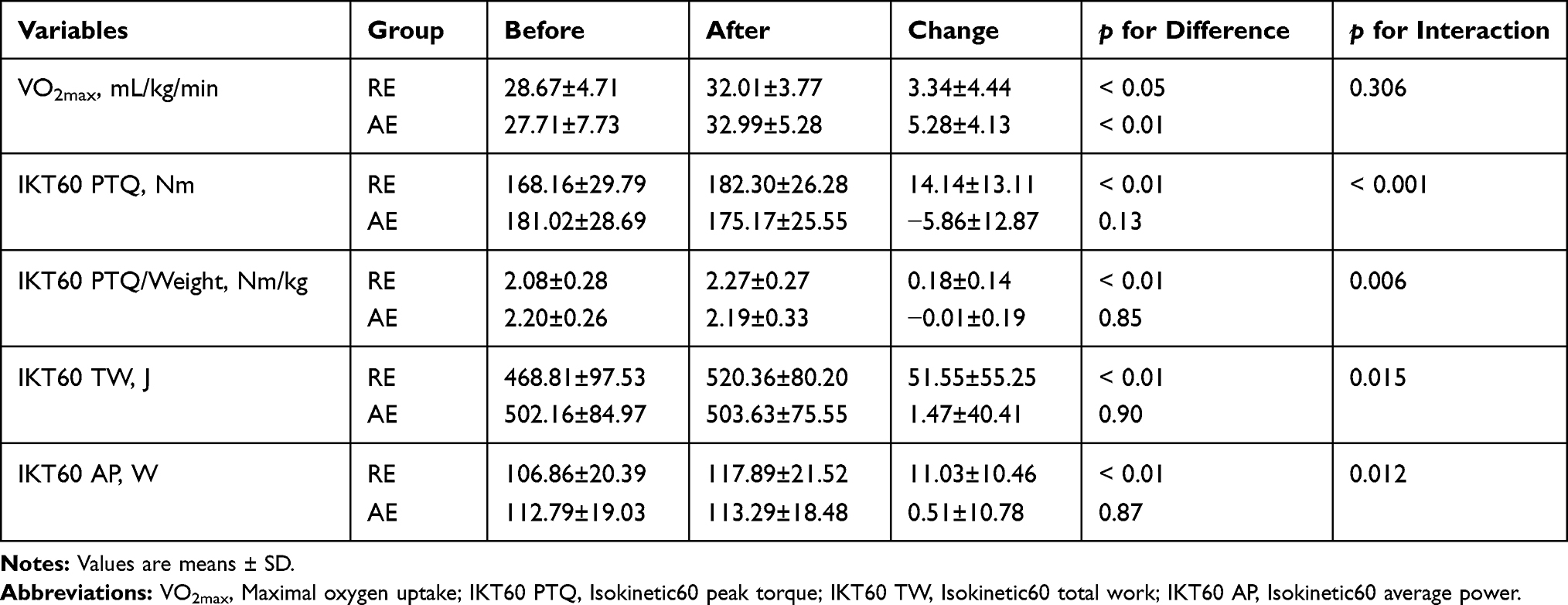 |
Table 3 Changes in Physical Fitness Between Resistance (n = 14) and Aerobic (n = 13) Group Adjusted for Age |
A comparison of the absolute value changes in body composition and physical fitness, adjusted for age and weight change is shown in Figure 2. A significant interaction between the groups was detected for lean mass and muscle strength-related variables (P = 0.002–0.018), while a significant interaction was not detected for fat mass (P = 0.613) or VO2max (P = 0.547) between the two groups.
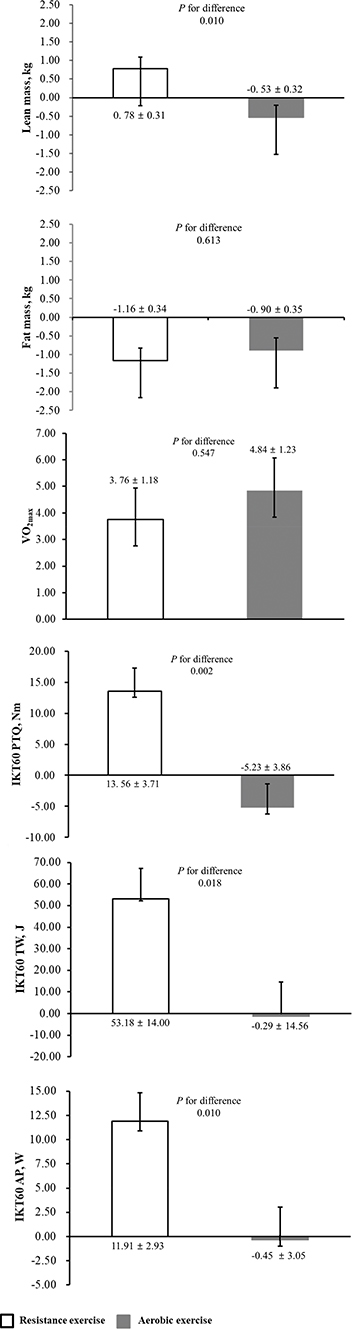 |
Figure 2 Comparison of changes in body composition and physical fitness adjusted for age and weight changes in response to resistance (n = 14) and aerobic (n = 13) exercise. |
Table 4 shows the baseline values and changes in blood markers for each group over the course of the exercise program, adjusted for age. No significant differences in any of the baseline measures were detected between the two groups. Among the nine metabolic and liver function markers, two liver function markers, ALT (−16.24%) and γ-GTP (−30.35%), in the RE group were significantly improved (P < 0.05 for both), while none of the markers in the AE group were significantly improved. A significant interaction between the two groups was not observed for any blood markers (P = 0.055–0.947).
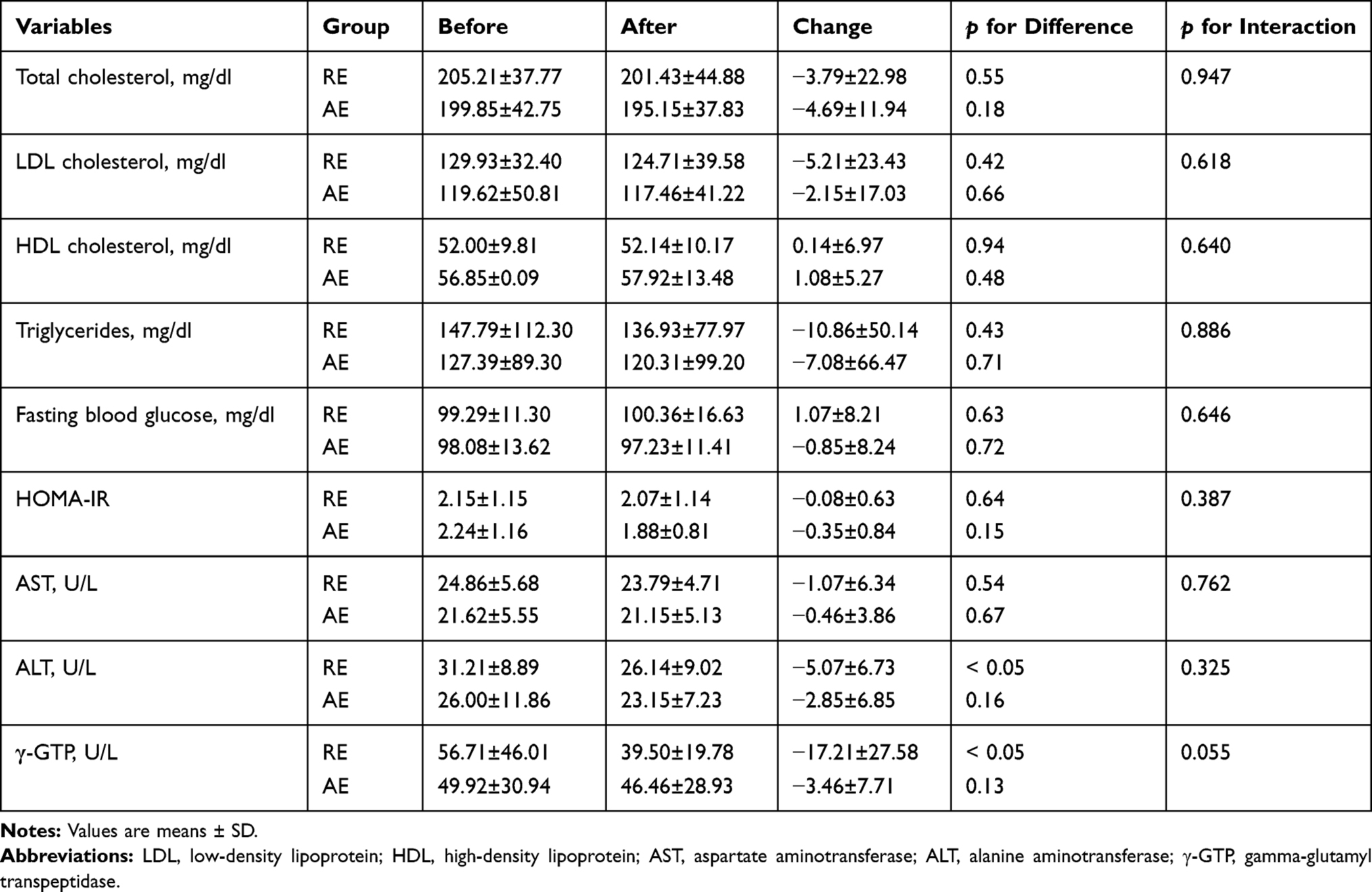 |
Table 4 Changes in Metabolic Markers and Liver Functions Between the Resistance (n = 14) and Aerobic (n = 13) Groups |
Discussion
We performed a prospective, single-blinded RCT to comparatively investigate changes in physiological and physical fitness in previously inactive men with obesity in response to AE or RE. The main findings in this study were as follows: 1) RE led to decreased fat mass and improved cardiorespiratory capacity, as well as increases in lean mass and strength, without significant weight change. 2) Although AE induced decreases in fat mass and weight and improved cardiorespiratory capacity, lean mass and muscle strength remained unchanged. 3) RE showed a stronger positive influence than AE on lean mass and muscle strength, and RE and AE had a similar influence on weight, fat mass, cardiorespiratory capacity and blood markers. Based on these findings, it may be an efficient exercise regimen to perform RE first and then utilize AE to maintain the changes that occur in response to RE for previously inactive men with obesity.
It has long been recognized that AE causes body weight reduction, which cannot be expected through RE. In this study, AE led to significant weight reduction, while RE did not cause significant weight reduction. Considering that when individuals are exposed to a similar period of AE or RE, AE leads to greater energy expenditure than RE, this may be considered a natural consequence. However, there was not a significant interaction between the two groups, and the mere comparison of weight, consisting of muscle and fat mass, was not sufficient. If the muscle mass increase exceeds the fat mass decrease in response to engaging in exercise, body weight can increase. Accordingly, we should pay greater attention to body composition than weight.
It has been broadly accepted that RE has positive influences on muscle mass and strength, whereas AE does not;21 however, in recent years, reports in which AE has led to positive effects on the maintenance of muscle mass during intentional weight reduction have increased.9 Carolina et al22 reported that both AE and RE induced an increase in motor unit conduction velocity, showing electrophysiological adaption of the muscle fiber membrane properties in a similar direction. Given these reports, it appears that AE also positively influences muscle mass and strength; in this study, however, there were significant interactions between the groups with respect to lean mass for muscle mass and all of the muscle strength-related variables. In addition, after adjusting for age and weight change, changes in the absolute values caused by AE were significantly smaller than those derived from RE. These findings indicate that it is difficult to obtain similar increases in muscle mass and strength from AE and RE.
Studies on RE-related fat mass reduction have been inconsistent. Davidson et al23 and Olson et al24 detected no change in fat mass, whereas Williams et al25 and Donnelly et al26 reported that RE caused the fat mass reduction. The findings in this study were consistent with the latter reports. Fat mass was significantly decreased in both groups, and there was no significant interaction for fat mass between the groups after adjusting for age. The same result was detected between the groups after adjusting for age and weight change. After completing the RE program, fat mass was decreased without any change in body weight, and maintained weight was caused by increased lean mass. Recommendations from the American College of Sports Medicine26 suggest the following potential mechanism through which RE may cause fat mass loss: “though the energy expenditure related to RE is not great, RE induces an increase in muscle mass, and then increased muscle mass causes resting energy expenditure to increase.” Based on this mechanism, it can be expected that executing RE for a long period leads to fat mass loss, as well as muscle mass and strength increases.
There is predominantly a negative view regarding the change of VO2max in response to RE, as only a few existing studies have reported positive results. These studies showed that RE led to the improvement of VO2max in young subjects whose VO2max at baseline was lower than 40 mL/kg/min and old subjects whose VO2max at baseline was lower than 25 mL/kg/min.27–29 In this study, the initial VO2max of middle-aged subjects in the RE program was 28.67 mL/kg/min, which was close to the VO2max of old subjects in the previous study. Additionally, similar to the existing studies, subjects in this study showed significant VO2max improvement in response to RE. Based on these findings, the effectiveness of RE on VO2max is not deniable when subjects have a low VO2max; however, the exact mechanism for VO2max improvement caused by RE is unclear. One possible mechanism is through the amelioration of arterial venous oxygen differences derived from an increase in capillary density, myoglobin concentration, muscle mitochondria content and enzyme activity.30–32 In addition, it is also estimated that increases in muscle mass and blood flow to exercising muscles, which indicates amelioration in peripheral vascular resistance, also contributes to the improvement of VO2max.33,34
For years, it has been widely accepted that changes in blood markers that indicate metabolic and liver functions are largely affected by the degree of fat mass and weight change. Based on the perception that AE is better than RE for decreasing fat mass and weight, it has been recognized that AE should be chosen for improving metabolic and liver functions rather than RE. Recently, however, studies that report different results are increasing. Bacchi et al reported that similar to AE, RE improves metabolic features and insulin sensitivity, and that RE and AE are equally effective in improving liver condition.35,36 Hallsworth et al also reported that RE ameliorated lipid oxidation, glucose control and insulin resistance without weight reduction.37 In fact, in this study, RE induced significant improvements in liver function markers such as ALT and γ-GTP without significant weight reduction. Additionally, almost all of the metabolic markers showed positive change after RE, though the differences were not significant. Based on these results, RE is also effective for improving metabolic and liver function. Concerning the mechanism of RE-induced metabolic amelioration, Bacchi et al reported that changes in VO2max and trunk fat may be major determinants of exercise-induced metabolic improvement.36 With respect to liver function, Hallsworth et al reported that improved metabolic flexibility and insulin sensitivity are the cause of liver function amelioration, regardless of weight reduction.37
There are two limitations of this study. First, all of the subjects in this study were middle-aged Japanese men, and some factors, including age, sex and lifestyle, can influence changes in the studied variables in response to exercise. For this reason, a long-term prospective cohort study is required in the future. Second, we could not determine the exact mechanisms by which RE caused fat mass reduction, cardiorespiratory capacity improvement and blood marker amelioration. Thus, future avenues for research should include data on the mechanisms of these changes in response to RE.
In summary, RE led to decreased fat mass and improved cardiorespiratory capacity, as well as increases in lean mass and muscle strength, without significant weight change. Although AE induced decreases in fat mass and weight and improved cardiorespiratory capacity, lean mass and muscle strength remained unchanged. RE showed a stronger positive influence than AE on lean mass and muscle strength, and RE and AE had a similar influence on weight, fat mass, cardiorespiratory capacity and blood markers. Thus, these findings suggest that it may be an efficient exercise regimen to perform RE first and then utilize AE to maintain the changes that occur in response to RE for previously inactive men with obesity.
Funding
This work was supported in part by the National Research Foundation of Korea grant funded by the Ministry of Education (No. NRF-2017R1A6A3A01077087, NRF-2019S1A5B5A07107393 and NRF-2019S1A5B5A07106956).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Eguchi E, Tanabe N, Wada Y, et al. Healthy lifestyle behaviours and cardiovascular mortality among Japanese men and women: the Japan collaborative cohort study. Eur Heart J. 2012;33(4):467–477. doi:10.1093/eurheartj/ehr429
2. WHO. Regional Office for the Western Pacific. Obesity in the Pacific: Too Big to Ignore. Nouméa, New Caledonia: WHO; 2002.
3. Oh S, Han G, Kim B, et al. regular exercise as a secondary practical treatment for nonalcoholic fatty liver disease. Exerc Med. 2018;2(4):4. doi:10.26644/em.2018.004
4. Vincent HK, Lamb KM, Day TI, et al. Morbid obesity is associated with fear of movement and lower quality of life in patients with knee pain-related diagnoses. PM&R. 2010;2(8):713–722. doi:10.1016/j.pmrj.2010.04.027
5. Vincent HK, Heywood K, Connelly J, et al. Obesity and weight loss in the treatment and prevention of osteoarthritis. PM&R. 2012;4(5):S59–S67. doi:10.1016/j.pmrj.2012.01.005
6. WHO. The Burden of Musculoskeletal Disease at the Start of the New Millennium. Geneva, Switzerland: WHO; 2003.
7. McCarthy O, Moser O, Eckstein ML, et al. Resistance isn’t futile: the physiological basis of the health effects of resistance exercise in individuals with type 1 diabetes. Front Endocrinol (Lausanne). 2019;10:507. doi:10.3389/fendo.2019.00507
8. Oh S, So R, Shida T, et al. High-intensity aerobic exercise improves both hepatic fat content and stiffness in sedentary obese men with nonalcoholic fatty liver disease. Sci Rep. 2017;7:43029. doi:10.1038/srep43029
9. Yoshimura E, Kumahara H, Tobina T, et al. Aerobic exercise attenuates the loss of skeletal muscle during energy restriction in adults with visceral adiposity. Obes Facts. 2014;7(1):26–35. doi:10.1159/000358576
10. Kim B, Tsujimoto T, So R, et al. Changes in lower extremity muscle mass and muscle strength after weight loss in obese men: a prospective study. Obes Res Clin Pract. 2015;9(4):365–373. doi:10.1016/j.orcp.2014.12.002
11. Willis LH, Slentz CA, Bateman LA, et al. Effects of aerobic and/or resistance training on body mass and fat mass in overweight or obese adults. J Appl Physiol. 2012;113(12):1831–1837. doi:10.1152/japplphysiol.01370.2011
12. American College of Sports Medicine. American college of sports medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports Exerc. 2009;41(3):687–708. doi:10.1249/MSS.0b013e3181915670
13. Sasai H, Katayama Y, Nakata Y, et al. The effects of vigorous physical activity on intra-abdominal fat levels: a preliminary study of middle-aged Japanese men. Diabetes Res Clin Pract. 2010;88(1):34–41. doi:10.1016/j.diabres.2009.12.018
14. Oh S, Shida T, Yamagishi K, et al. Moderate to vigorous physical activity volume is an important factor for managing nonalcoholic fatty liver disease: a retrospective study. Hepatology. 2015;61(4):1205–1215. doi:10.1002/hep.v61.4
15. So R, Sasai H, Matsuo T, et al. Multiple-slice magnetic resonance imaging can detect visceral adipose tissue reduction more accurately than single-slice imaging. Eur J Clin Nutr. 2012;66(12):1351–1355. doi:10.1038/ejcn.2012.147
16. Kumagai H, Zempo-Miyaki A, Yoshikawa T, et al. Increased physical activity has a greater effect than reduced energy intake on lifestyle modification-induced increases in testosterone. J Clin Biochem Nutr. 2016;58(1):84–89. doi:10.3164/jcbn.15-48
17. Kim M, Tomita T, Kim M, et al. Aerobic exercise training reduces epicardial fat in obese men. J Appl Physiol (1985). 2009;106(1):5–11. doi:10.1152/japplphysiol.90756.2008
18. Kim B, Tsujimoto T, So R, et al. Weight reduction does not induce an undesirable decrease in muscle mass, muscle strength, or physical performance in men with obesity: a pilot study. J Exerc Nutr Biochem. 2017;21(4):37–44. doi:10.20463/jenb.2017.0029
19. Kim B, Tsujimoto T, So R, et al. Changes in muscle strength after diet-induced weight reduction in adult men with obesity: a prospective study. Diabetes Metab Syndr Obes. 2017;10:187–194. doi:10.2147/DMSO
20. Tanaka K, Takeshima N, Kato T, et al. Critical determinants of endurance performance in middle-aged and elderly endurance runners with heterogeneous training habits. Eur J Appl Physiol Occup Physiol. 1990;59(6):443–449. doi:10.1007/BF02388626
21. Lee S, Bacha F, Hannon T, et al. Effects of aerobic versus resistance exercise without caloric restriction on abdominal fat, intrahepatic lipid, and insulin sensitivity in obese adolescent boys: a randomized, controlled trial. Diabetes. 2012;61(11):2787–2795. doi:10.2337/db12-0214
22. Carolina VC, Deborah F, Dario F. Motor unit behavior during submaximal contractions following six weeks of either endurance or strength training. J Appl Physiol. 2010;109:1455–1466. doi:10.1152/japplphysiol.01213.2009
23. Davidson LE, Hudson R, Kilpatrick K, et al. Effects of exercise modality on insulin resistance and functional limitation in older adults: a randomized controlled trial. Arch Intern Med. 2009;169(2):122–131. doi:10.1001/archinternmed.2008.558
24. Olson TP, Dengel DR, Leon AS. Changes in inflammatory biomarkers following one-year of moderate resistance training in over weight women. Int J Obes. 2007;31:996–1003. doi:10.1038/sj.ijo.0803534
25. Williams MA, Haskell WL, Ades PA, et al. Resistance exercise in individuals with and without cardiovascular disease: 2007 update: a scientific statement from the American Heart Association council on clinical cardiology and council on nutrition, physical activity, and metabolism. Circulation. 2007;116(5):572–584. doi:10.1161/CIRCULATIONAHA.107.185214
26. Donnelly JE, Blair SN, Jakicic JM, et al. American college of sports medicine position stand. Appropriate physical activity intervention strategies for weight loss and prevention of weight regain for adults. Med Sci Sports Exerc. 2009;41(2):459–471. doi:10.1249/MSS.0b013e3181949333
27. McCarthy JP, Agre JC, Graf BK, et al. Compatibility of adaptive responses with combining strength and endurance training. Med Sci Sports Exerc. 1995;27(3):429–436. doi:10.1249/00005768-199503000-00021
28. Vincent KR, Braith RW, Feldman RA, et al. Improved cardiorespiratory endurance following 6 months of resistance exercise in elderly men and women. Arch Intern Med. 2002;162(6):673–678. doi:10.1001/archinte.162.6.673
29. Wieser M, Haber P. The effects of systematic resistance training in the elderly. Int J Sports Med. 2007;28(1):59–65. doi:10.1055/s-2006-924057
30. Cesar Mde C, Borin JP, Gonelli PR, et al. The effect of local muscle endurance training on cardiorespiratory capacity in young women. J Strength Cond Res. 2009;23(6):1637–1643. doi:10.1519/JSC.0b013e3181b3dbaa
31. Coggan AR, Spina RJ, King DS, et al. Skeletal muscle adaptations to endurance training in 60- to 70-yr-old men and women. J Appl Physiol. 1992;72(5):1780–1786. doi:10.1152/jappl.1992.72.5.1780
32. Frontera WR, Meredith CN, O’Reilly KP, et al. Strength training and determinants of VO2max in older men. J Appl Physiol. 1990;68(1):329–333. doi:10.1152/jappl.1990.68.1.329
33. Phillips B, Williams J, Atherton P, et al. Resistance exercise training improves age-related declines in leg vascular conductance and rejuvenates acute leg blood flow responses to feeding and exercise. J Appl Physiol. 2012;112(3):347–353. doi:10.1152/japplphysiol.01031.2011
34. Abe T, Kearns CF, Fukunaga T. Sex differences in whole body skeletal muscle mass measured by magnetic resonance imaging and its distribution in young Japanese adults. Br J Sports Med. 2003;37(5):436–440. doi:10.1136/bjsm.37.5.436
35. Bacchi E, Negri C, Targher G, et al. Both resistance training and aerobic training reduce hepatic fat content in type 2 diabetic subjects with nonalcoholic fatty liver disease (the RAED2 randomized trial). Hepatology. 2013;58(4):1287–1295. doi:10.1002/hep.v58.4
36. Bacchi E, Negri C, Zanolin ME, et al. Metabolic effects of aerobic training and resistance training in type 2 diabetic subjects: a randomized controlled trial (the RAED2 study). Diabetes Care. 2012;35(4):676–682. doi:10.2337/dc11-1655
37. Hallsworth K, Fattakhova G, Hollingsworth KG, et al. Resistance exercise reduces liver fat and its mediators in non-alcoholic fatty liver disease independent of weight loss. Gut. 2011;60(9):1278–1283. doi:10.1136/gut.2011.242073
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.