")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Influence Of Uncertainty, Depression, And Social Support On Self-Care Compliance In Hemodialysis Patients
Received 21 June 2019
Accepted for publication 6 October 2019
Published 22 October 2019 Volume 2019:15 Pages 1243—1251
DOI https://doi.org/10.2147/TCRM.S218934
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Bomi Kim,1 Jihyun Kim2
1Eumseong Support Center for Foreign Workers, Eumseong-Gun, Chungcheongbuk-Do 27703, Republic of Korea; 2Department of Nursing, Daejeon University, Dong-Gu, Daejeon 300-716, Republic of Korea
Correspondence: Jihyun Kim
Department of Nursing, Daejeon University, 62 Daehak-ro, Dong-gu, Daejeon 300-716, Republic of Korea
Tel +82-42-280-4651
Fax +82-42-280-2785
Email [email protected]
Purpose: This study was conducted to examine the associations among uncertainty, depression, social support, and self-care compliance in patients undergoing hemodialysis, and to identify the factors influencing self-care compliance.
Methods: A convenience sample of 152 patients receiving hemodialysis was selected. Data were analyzed using descriptive statistics, independent t-test, ANOVA, Pearson correlations, and hierarchical regression analysis with the SPSS 23.0 program.
Results: Participants performed a moderate level of self-care consisting of factors such as knowledge of hemodialysis, dietary knowledge of hemodialysis, dietary compliance with hemodialysis, and compliance with hemodialysis order. The self-care compliance of participants undergoing hemodialysis showed a significant relationship with depression, uncertainty, and social support. The factors significantly influencing self-care compliance were social support and occupation. These variables explained 24.9% of the variance in self-care compliance.
Conclusion: Findings from this study confirmed that uncertainty, depression, and social support are major factors affecting self-care compliance, and that the higher the patients’ uncertainty, the lower their self-care compliance. Thus, interventions should be performed to reduce uncertainty and to improve self-care through accurate information and education on disease progression and self-care.
Keywords: self care, social support, uncertainty, renal dialysis
Introduction
End-stage renal disease (ESRD), the final stage of chronic kidney disease that exists in 8–16% of the population worldwide,1 is characterized as irreversible impairments in kidney function, and its prevalence is increasing annually.2,3 Hemodialysis is an important and commonly used renal replacement therapy (RRT) for ESRD patients.4 According to the International Society of Nephrology, 2.62 million people received RRT to treat ESRD worldwide, of which most were treated with hemodialysis.
Although hemodialysis may help patients with chronic kidney disease to maintain their physical function and prevent complications, it is difficult to cure chronic kidney failure with hemodialysis alone, and the disease requires continued treatment and care.5 Self-care for hemodialysis patients may require significant restrictions in lifestyle habits and behaviors,6 yet only about 50.0% of patients adhere to recommended self-care strategies.7,8
Factors that may influence hemodialysis patients’ self-care compliance include the burden of a changed life, depression, social support, family support, hope, and knowledge, as well as complexity of their treatment.9,10 Among these influencing factors, anxiety and depression are the major emotional reactions that prevent hemodialysis patients from effectively coping with disease and treatment,5 and 40.2% of hemodialysis patients have been found to experience depression.11,12 Severe depression is also associated with a lower level of compliance with treatment,13 higher suicide risk,12 and lower quality of life.6 Nonetheless, social support reduces complications and mortality by facilitating health promoting behaviors, reducing stress, and helping individuals to adapt psychologically.9 Social support also contributes to lowering hemodialysis patients’ depression and suicidal ideation11 as well as reducing uncertainty.12 Kammerer et al14 reported that support from health professionals is a major factor that contributes to self-care compliance.
Uncertainty, a concept originating from Mishel’s uncertainty theory,15 is recognized when a patient cannot accurately understand the implications of disease-related events or predict the outcomes of the disease.15 For many hemodialysis patients, the inability to identify or predict treatment prognosis and disease progression may lead to a high level of uncertainty.16 Uncertainty acts as a major source of stress for hemodialysis patients:17 not only does uncertainty exacerbate psychological problems, such as depression, anxiety, and fear, experienced by patients during disease progression, but it also causes negative coping strategies and reduces self-care compliance.16–18 In this regard, a nursing intervention that can identify and control hemodialysis patients’ level of uncertainty could be applied to improve the patients’ coping and self-care compliance.
Hemodialysis patients’ self-care compliance is directly related to their health status and quality of life;6 thus, it is necessary to develop an intervention program that increases the patients’ self-care compliance. Although chronic disease patients’ sociopsychological problems, such as depression, anxiety, social support,11,13 and uncertainty,12 have been reported as factors that influence self-care compliance, few studies have examined the relationship between hemodialysis patients’ uncertainty and self-care compliance. Because uncertainty could act as a factor that causes negative emotions and ineffective coping behaviors during the disease process,12 it is important to examine the effect of hemodialysis patients’ uncertainty, along with social support and depression, on their self-care compliance.
Therefore, the major variables in this study stem from the general characteristics that were found to affect self-care practice in prior studies (sex, age, marital status, educational level, religion, employment status, income, regular exercise, hemodialysis period, weekly hemodialysis frequency, history of kidney transplantation, type of vascular access),19–21 uncertainty,16–18 depression,9,10,13 and social support,14,22 and we will assess how these variables affect self-care compliance among hemodialysis patients.
Methods
Design
This was a quantitative cross-sectional study performed in a renal replacement therapy unit in Korea.
Participants
Data collection took place from December 15, 2018 to March 31, 2019. Investigators visited 5 hospitals (2 general hospitals and 3 hemodialysis centers) to explain the purpose and methods of the study. Data collection was conducted by a principal investigator and a sub-investigator who received training on data collection procedures. No pilot study was conducted prior to the present study.
The sample size was calculated using the G*Power software program. With 0.80 set for statistical power (1-β), 0.05 for p-value (α), and a moderate level of 0.15 for effect size in regression analysis, the sample size required for 15 independent variables was calculated as 143 patients. Considering the dropout rate of 20%, we administered questionnaire to 171 patients. The inclusion criteria were as follows: age >19 years, able to communicate, and presence of cognitive ability to respond to the instrument. The following exclusion criteria were adopted: presence of comprehension deficit for filling the instrument, having started hemodialysis within the past 3 months, and having clinical hemodynamically unstable condition. We excluded 19 participants whose responses were missing for 4 or more items.
Tools
Uncertainty
We used a tool adapted by Jung19 from Mishel’s Uncertainty in Illness Scale (MUIS)15 to examine uncertainty. The MUIS had a total of 33 items, which consisted of 4 sub-items of uncertainty (ambiguity, complexity, inconsistency, unpredictability) and other items. The MUIS used a 5-point Likert scale, in which a higher score represented a higher level of uncertainty. Cronbach’s α was 0.91 at the time when the tool was developed,15 0.08 in a study by Jang et al23 that assessed uncertainty in hemodialysis patients, and 0.79 in the present study. At the time of development, construct validity was determined by differentiation of medical, surgical, and diagnostic patients; individuals with unconfirmed diagnoses had higher uncertainty scores.24,25
Depression
Depression was assessed using the Patient Health Questionnaire-9 (PHQ-9) originally developed by Spitzer et al26 and adapted later by Shin et al27 The tool had 9 items in total and used a 4-point Likert scale, in which a higher score represented a higher level of depression. Cronbach’s α was 0.88 at the time when the tool was developed,26 0.92 in a study by Linda et al28 that measured depression in hemodialysis patients, and 0.81 in the present study. At the time of development, the concurrent validity was verified using SF-20,29 and it was verified as general health perceptions (r=0.55, p<0.001), social functioning (r=0.52, p<0.001), role functioning (r=0.43, p<0.001), physical functioning (r=0.37, p<0.001), and bodily pain (r=0.33, p<0.001).
Social Support
Social support was assessed in the present study using the Multidimensional Scale of Perceived Social Support (MSPSS) developed originally by Zimet et al30 and adapted later by Shin and Lee.31 The MSPSS had a total of 12 items, which consisted of support from family, significant others, and friends. The tool used a 5-point Likert scale, in which a higher score represented a higher level of social support. Cronbach’s α was 0.85 at the time the tool was developed,30 0.92 in a study by Lee et al32 that measured social support for hemodialysis patients, and 0.84 in the present study. At the time of development, the concurrent validity (r=−0.35, p<0.002) was verified using the Beck depression inventory.33
Self-Care Compliance
For the assessment of self-care compliance, the present study used a tool developed and validated by Lee and Lim34 for hemodialysis patients. The tool had 30 items and used a 4-point Likert scale, in which a higher score represented a higher level of self-care compliance. Cronbach’s α was 0.90 at the time the tool was developed34 and 0.87 in the present study. At the time of development, validity was verified with a significant positive correlation (r=0.66, p<0.001) through concurrent validity assessed using the self-care questionnaire on hemodialysis patients.
Ethical Considerations
Before collecting data, the present study obtained approval from the institutional review board (IRB) of the Daejeon university (1040647-201810-HR009-03) and written informed consent was obtained from all individual participants included. All investigations were conducted in accordance with the Declaration of Helsinki.
Statistical Analyses
Collected data were analyzed using the SPSS 23.0 statistics program. The differences in variables according to each participant’s characteristics were evaluated using independent sample t-test and ANOVA. A Shapiro–Wilk test was conducted to check for normal distribution. The correlation was analyzed using Pearson’s correlation coefficients. The factors that were hypothesized to influence self-care compliance were analyzed using hierarchical multiple regression analysis.
Results
Differences In Self-Care Compliance According To Participants’ Demographics And Disease Characteristics
The average age of the participants was 53.28 (±11.17) years, and 97 were men (63.8%) and 55 were women (36.2%). Ninety-eight (64.5%) of the participants were married. In total, 97 (63.8%) of the participants were unemployed. The hemodialysis period ranged from 3 months to 322 months, the average being 81.26 months (±70.01). There were significant differences in self-care compliance based on educational attainment, religion, occupation, and family monthly income. In particular, the participants whose educational level was elementary school or less showed the lowest level of self-care compliance (F=3.08, p=0.029) (Table 1).
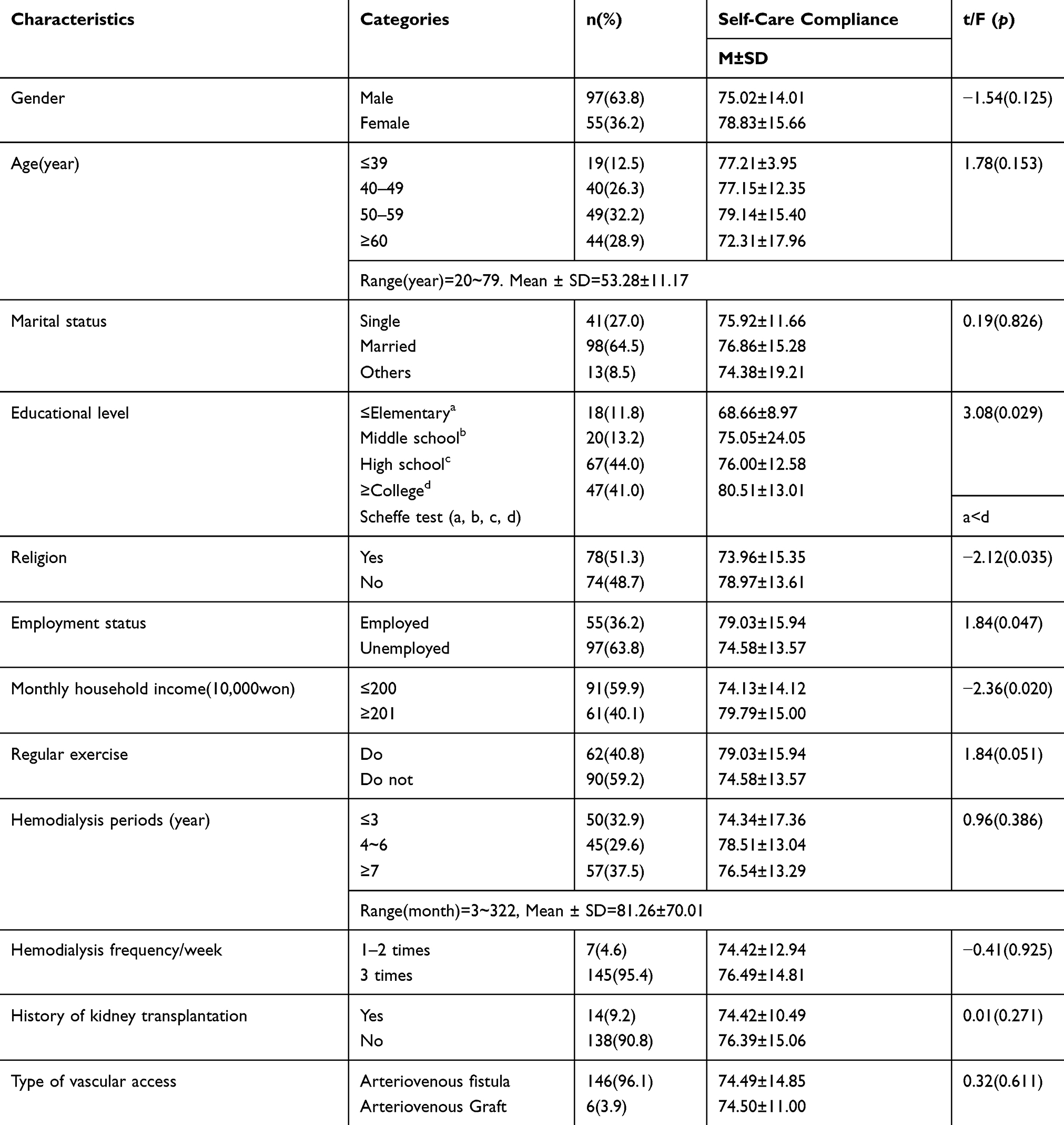 |
Table 1 Differences Of Self-Care Compliance According To Socioeconomic And Disease-Related Characteristics |
The weekly hemodialysis frequency was 3 in 145 (95.4%) participants and 1–2 in 7 (4.6%) participants. There was no significant difference in self-care compliance based on the HD frequency. There were 14 (9.2%) participants with a history of kidney transplantation, and 146 (96.1%) participants had hemodialysis through an arteriovenous fistula as the type of vascular access. There were no differences in self-care compliance based on the characteristics of hemodialysis (Table 1).
Levels Of Uncertainty, Depression, Social Support, And Self-Care Compliance In The Participants
The average self-care compliance score was 76.40 ± 14.70 (maximum: 120), and uncertainty score ranged from 33 to 165, with a mean value of 90.00 ± 11.63. The average depression score was 13.05 ± 4.85 (range: 0–27), and the average social support score was 44.19 ± 9.08 (range: 12–60). Among the sub-items of self-care compliance, the average score for dietary knowledge of hemodialysis and knowledge of hemodialysis were 20.86 ± 5.07 and 19.19 ± 4.97 (range: 4–28), respectively. The average compliance with hemodialysis and dietary compliance with hemodialysis scores were 17.28 ± 3.44 (range: 4–28) and 14.73 ± 4.11 (range: 4–24), respectively. The average compliance with hemodialysis score was 9.61 ± 2.70 (range: 4–12) (Table 2).
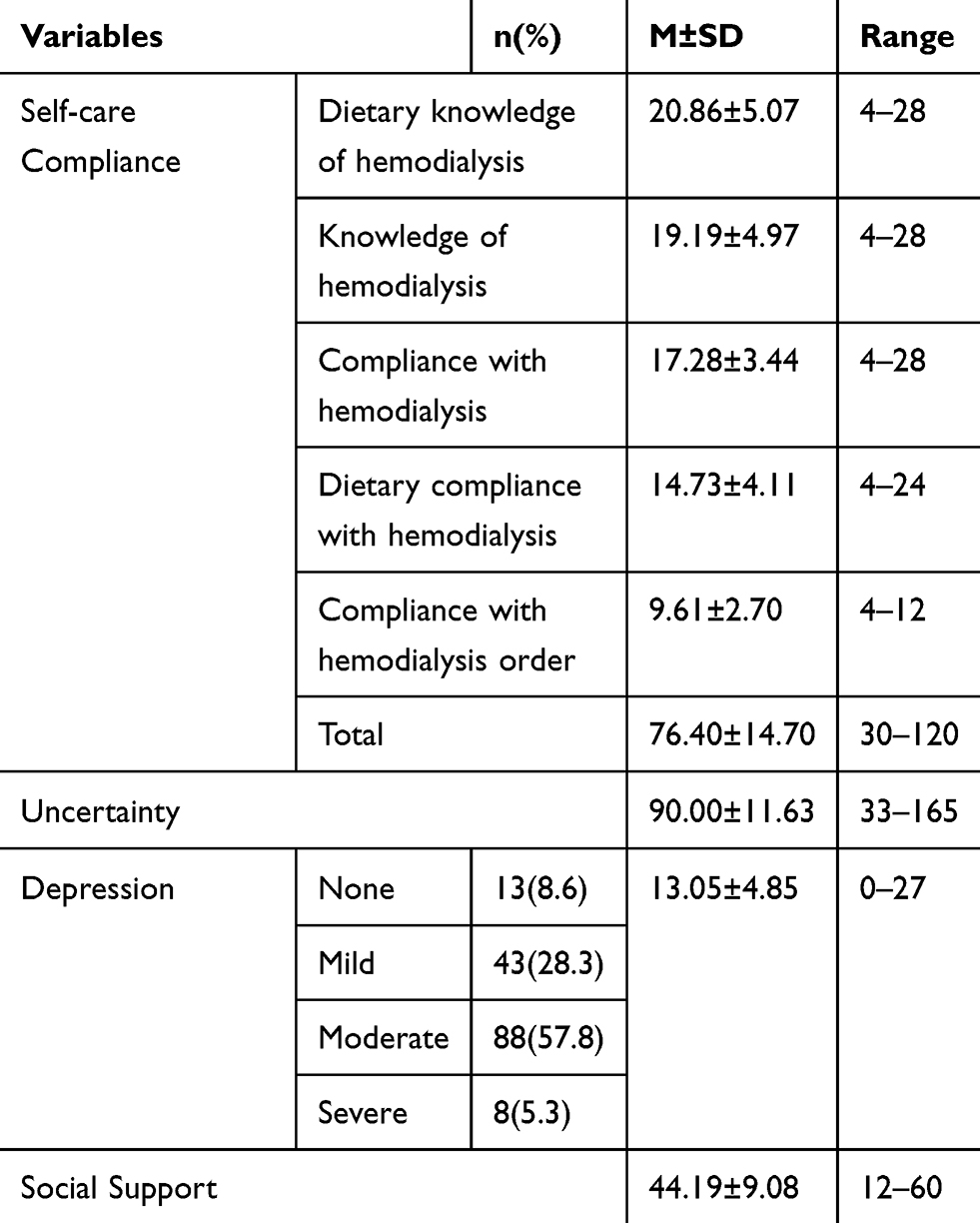 |
Table 2 Self-Care Compliance, Uncertainty, Depression And Social Support In Hemodialysis (N=152) |
Correlations Between The Participant Uncertainty, Depression, Social Support, And Self-Care Compliance
Self-care compliance showed significant negative correlations with uncertainty (r=−0.25, p=0.002) and depression (r=−0.30, p<0.001) and a positive correlation with social support (r=0.32, p<0.001). This finding suggested that a lower level of uncertainty and depression and a higher level of social support were associated with higher levels of self-care compliance in the HD patients (Table 3).
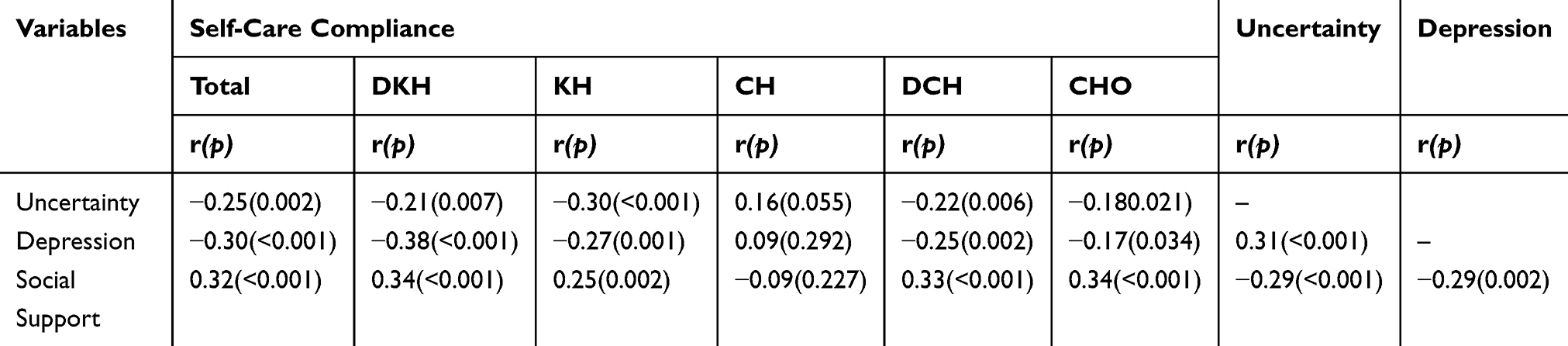 |
Table 3 Correlations Between Self-Care Compliance, Uncertainty, Depression And Social Support In Hemodialysis (N=152) |
Uncertainty had a significant positive correlation with depression (r=0.31, p<0.001) and a negative correlation with social support (r=−0.29, p<0.001). Depression and social support showed a significant negative correlation (r=−0.29, p=0.002) (Table 3).
Factors Influencing The Participants’ Self-Care Compliance
We found no autocorrelation as the Durbin-Watson statistic was 1.77, which was closer to the baseline of 2. Tolerance ranged from 0.73 to 0.87, which exceeded 0.1, and the variance inflation factor (VIF) ranged from 1.03 to 1.38, which indicated no evidence of multicollinearity. In addition, the significance probability in the Shapiro–Wilk test ranged from 0.07 to 0.91, which satisfied the assumption of normality of distribution and homoscedasticity of residuals and was therefore fit for a regression analysis model.
For the analysis of factors that influenced the participants’ self-care compliance, Model 1 used education level, religion, occupation, and household income, which showed significant correlations with self-care compliance as control variables. Model 1 revealed that the presence or absence of employment (β=0.38, p<0.001) had a significant effect, and its explanatory power was 18.1% (F=9.37, p<0.001). In Model 2, which included the independent variables, the explanatory power increased significantly to 24.9%, and when controlling for demographic characteristics, social support (β=0.20, p=0.013) was found to be the variable that influenced self-care compliance (F= 8.15, p<0.001) (Table 4).
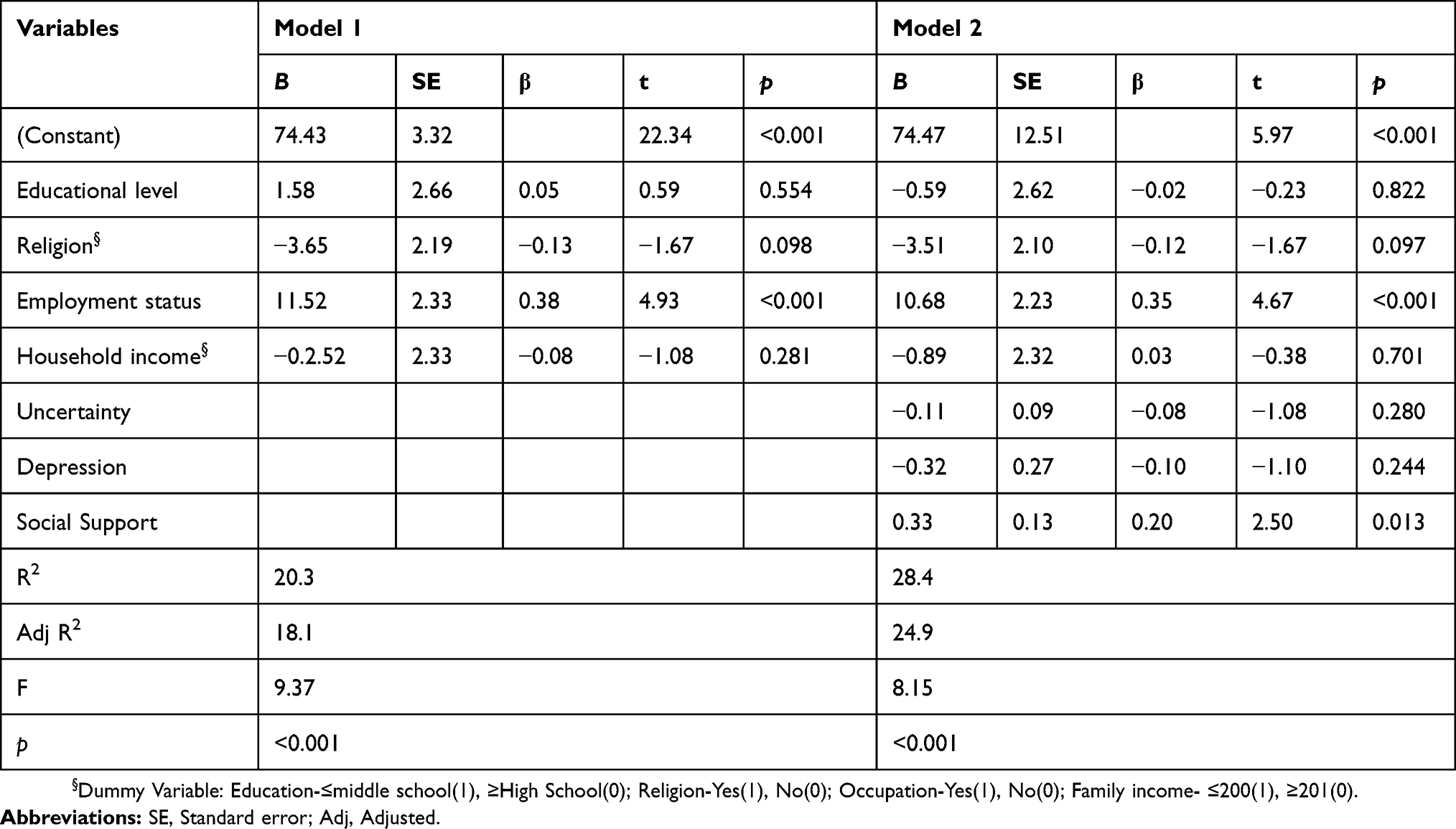 |
Table 4 The Influencing Factors On Self-Care Compliance (N=152) |
Discussion
The present study was conducted to identify the uncertainty, depression, social support, and self-care compliance levels of ESRD patients undergoing hemodialysis. We examined correlations between these variables, and the factors that influenced self-care compliance were examined.
The results showed that the average self-care compliance score in hemodialysis patients was 76.40 points when converted into a maximum of 120. This score is similar to that in a previous study that measured hemodialysis patients’ self-care.35 Among the sub-items, dietary knowledge of hemodialysis received the highest score, followed by knowledge of hemodialysis. Compliance with hemodialysis and dietary compliance with hemodialysis, which represents self-care compliance in practice, scored lower than the aforementioned knowledge sub-items. These results are consistent with those from Park et al.’s study20 on hemodialysis patients’ self-care. These findings suggest that hemodialysis patients experienced difficulty in practicing self-care, despite having knowledge about self-care. Compliance with hemodialysis and dietary compliance with hemodialysis are essential for hemodialysis patients to properly manage their disease. Recently, Riegel et al36 developed the middle-range theory of self-care of chronic illness and suggested that experience, skill, motivation, culture, confidence, habits, function, cognition, support from others, and access to care are the factors that have an effect on the self-care compliance of patients with chronic illness. The middle-range theory of Riegel et al36 may serve as a useful tool to develop a program that enhances the self-care of hemodialysis patients, and an education program for hemodialysis patients needs to be developed and applied on the basis of such evidence.
The degree of uncertainty in hemodialysis patients was above the moderate level, and it had a negative correlation with self-care practice as well as with self-care compliance. These results are consistent with those from a previous study35 that studied the relationship between hemodialysis patients’ self-care and uncertainty. They are also similar to the results of another study on the uncertainty of patients re-admitted after coronary interventions,37 which indicated that a higher level of uncertainty resulted in a lower level of patient compliance. hemodialysis patients experience a high level of uncertainty due to psychological problems, such as depression and anxiety, due to their condition and the treatment process because they cannot anticipate disease progression or the complications that may arise.12,16 hemodialysis patients’ uncertainty has a negative effect on self-care and health-promoting behaviors,18 which contributes to deterioration in health status and negatively affects the individual’s subjective perception of health.21 Stiegelis et al38 found that “ambiguity” was the most noticeable among other sub-items of uncertainty. Ambiguity intensifies when patients do not have enough information or knowledge about how to treat their disease, which can increase their uncertainty and cause negative treatment outcomes. Hence, to reduce hemodialysis patients’ uncertainty and ultimately increase their level of self-care, health professionals should provide detailed explanations to patients about their disease and treatment, and educate them from the beginning of treatment. This could decrease patients’ uncertainty and ultimately increase their level of self-care.
This study found that 63.1% of participants had a moderate or high level of depression. The prevalence of depression reported in our study is comparable to that documented in previous investigations in Jordan (51.5%)39 and China (45.9%).40 Furthermore, depression had a positive correlation with uncertainty and a negative correlation with self-care compliance. Keshin and Engin’s study41 on depression, suicidal ideation, and coping strategies among hemodialysis patients found that the higher the level of depression, the stronger the suicidal ideation and the lower the level of coping strategies. As such, high levels of depression increase a patient’s uncertainty and further hamper the compliance of self-care. Therefore, it would be important to develop and apply a psychological support program that can reduce hemodialysis patients’ depression. A study that analyzed the relationship between the levels of depression and physical activity in hemodialysis patients showed that an increase in physical activity reduces depression.
The present study’s regression analysis of the variables that influenced hemodialysis patients’ self-care compliance showed that social support and the presence or absence of employment had a significant effect. This finding indicates that a higher level of social support and being employed are more likely to increase self-care compliance. This finding that social support had a significant effect on hemodialysis patients’ self-care is similar to that of Cha’s study22 on the structural model of hemodialysis patients’ self-care, which showed that support from family, friends, fellow patients, as well as from health professionals had the biggest effect on self-care behaviors. In addition, Simmons42 found that a higher level of support from health professionals led to a higher level of self-care compliance. These results strongly suggest that various coping strategies, such as establishing a support system with family and health professionals beyond simply improving behaviors related to the disease are necessary to increase self-care compliance. Although these individuals represent a vulnerable group and need substantial social and institutional support to increase self-care compliance, this finding demonstrates a lack of connection between health services and local community support services.
Limitation
This study has some notable limitations. First, since this was a cross-sectional study that enrolled a relatively small number of adult patients with ESRD treated by hemodialysis, the probability of identifying additional risk factors was low. Future research should analyze data from a larger sample of participants and study self-care compliance at various levels in order to assess the influence of various hemodialysis-related characteristics on self-care compliance. Second, previous studies18,43 report that uncertainty evaluation had a significant correlation with the participants’ coping strategies. Hence, a follow-up study should more closely examine hemodialysis patients’ level of uncertainty, uncertainty evaluation, and coping strategies.
Conclusion
The findings from this study are significant as they highlight the relationship between hemodialysis patients’ self-care compliance, uncertainty, depression, and social support. hemodialysis patients were found to experience moderate levels of uncertainty, which had a positive correlation with depression and was a factor that impeded compliance with self-care. These results suggest that thorough discussion, education, and information about the treatment process and decision-making during the early stage of hemodialysis, as well as support from close relationships, could reduce participants’ uncertainty and ultimately contribute to increasing their self-care compliance and health status.
Funding
This paper was supported by Daejeon University Research Grant of 2018.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
References
1. Yang B, Xu J, Xue Q, et al. Non-pharmacological interventions for improving sleep quality in patients on dialysis: systematic review and meta-analysis. Sleep Med Rev. 2015;23:68–82. doi:10.1016/j.smrv.2014.11.005
2. Brown PDS, Rowed K, Shearer J, MacRae JM, Parker K. Impact of intradialytic exercise intensity on urea clearance in hemodialysis patients. Appl Physiol Nutr Metab. 2018;43(1):101–104. doi:10.1139/apnm-2017-0460
3. Carletti CO, Rosa CS, Souza GD, Ramirez AP, Daibem CG, Monteiro HL. Intradialytic exercise and postural control in patients with chronic kidney disease undergoing hemodialysis. Fisioter Mov. 2017;30(2):247–254. doi:10.1590/1980-5918.030.002.ao05
4. Bhave N, Agodoa LY, Bragg-Gresham J. US renal data system 2017 annual data report: epidemiology of kidney disease in the United States. Am J Kidney Dis. 2018;71(4):501.
5. Chiou CP, Chung YC. Effectiveness of multimedia interactive patient education on knowledge, uncertainty and decision-making in patients with end-stage renal disease. J Clin Nurs. 2012;21(9–10):1223–1231. doi:10.1111/j.1365-2702.2011.03793.x
6. Suh SR, Cho IH. Influence of hemodialysis patient’s stress and acceptance on their psychosocial adaptation and quality of life. J Korea Contents Assoc. 2014;14(11):829–837. doi:10.5392/JKCA.2014.14.11.829
7. Kutner NG, Zhang R, McClellan WM, Cole SA. Psychosocial predictors of non‐compliance in hemodialysis and peritoneal dialysis patients. Nephrol Dialysis Transplant. 2002;17(1):93–99. doi:10.1093/ndt/17.1.93
8. DiMatteo MR. Variations in patients’ adherence to medical recommendations: a quantitative review of 50years of research. Med Care. 2004;42(3):200–209. doi:10.1097/01.mlr.0000114908.90348.f9
9. Kara B, Caglar K, Kilic S. Nonadherence with diet and fluid restrictions and perceived social support in patients receiving hemodialysis. J Nurs Scholarship. 2007;39(3):243–248. doi:10.1111/j.1547-5069.2007.00175
10. Yeun YR. Systematic review of research on adherence among hemodialysis patients in korea. J Korea Academia Ind Cooperation Soc. 2012;13(12):5993–6000. doi:10.5762/KAIS.2012.13.12.5993
11. Yoon SH, Kim SS. Influence of depression, hope, and social support on suicidal ideation in renal dialysis patients. J Korean Acad Soc Adult Nurs. 2012;24(3):209–218. doi:10.7475/kjan.2012.24.3.209
12. Kim YJ, Choi HJ. The influence of uncertainty and social support on general well-being among hemodialysis patients. Korean J Rehabil Nurs. 2012;15(1):20–29. doi:10.7587/kjrehn.2012.20
13. Kim SS, Ryu EJ. Control effect of illness perception on depression and quality of life in patients with hemodialysis: using structural equation modeling. J Korean Biol Nurs Sci. 2018;20(4):221–227. doi:10.7586/jkbns.2018.20.4.221
14. Kammerer J, Garry G, Hartigan M, Carter B, Erlich L. Adherence in patients on dialysis: strategies for success. Nephrol Nurs J. 2007;34(5):479–486.
15. Mishel MH. The measurement of uncertainty in illness. Nurs Res. 1981;30(5):258–263.
16. Tong A, Sainsbury P, Chadban S, et al. Patients’ experiences and perspectives of living with CKD. Am J Kidney Dis. 2009;53:689–700. doi:10.1053/j.ajkd.2008.10.050
17. Yun SJ, Lee YH. Factors influencing uncertainty in dialysis patient by duration of dialysis. Korean J Adult Nurs. 2012;24(6):597–606. doi:10.7475/kjan.2012.24.6.0597
18. Jang HS, Lee CS, Yang YH. Influence of uncertainty and uncertainty appraisal on self-management in hemodialysis patients. J Korean Acad Nurs. 2015;45(2):271–279. doi:10.4040/jkan.2015.45.2.271
19. Jung CW, Kim MJ, Rhee MH, Do HG. Functional status and psychosocial adjustment in gynecologic cancer patients receiving chemotherapy. Korean J Women Health Nurs. 2005;11(1):58–66. doi:10.4069/kjwhn.2005.11.1.58
20. Park JS, Lee HS, Lee SY, Im HB, Oh HS. Relationship between knowledge and adherence to self management guidelines, and influencing factors of adherence for hemodialysis patients. Korean J Rehabil Nurs. 2011;14(1):9–46.
21. Cha JE. Structural equation modeling of self-management in patients with hemodialysis. J Korean Acad Nurs. 2017;47(1):14–24. doi:10.4040/jkan.2017.47.1.14
22. Cha JE, Yi MS. A path analysis of social support in patients with hemodialysis: based on the self-regulation model. J Korean Clin Nurs Res. 2015;21(1):116–126.
23. Jang HS, Lee CS, Yang YH. Influence of uncertainty and uncertainty appraisal on self-management in hemodialysis patients. J Korean Acad Nurs. 2015;45(2):271–279. doi:10.4040/jkan.2015.45.2.271
24. Mishel MH. Parents’ perception of uncertainty concerning their hospitalized child. Nurs Res. 1983;32(6):324–330.
25. Mishel MH. Perceived uncertainty and stress in illness. Res Nurs Health. 1984;7:163–171.
26. Spitzer RL, Kroenke K, Wiliams JB. Patient health questionnaire primary care study group. valiation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary evaluation of mental disorders. Patient health questionnaire. JAMA. 1999;282(18):1737–1744. doi:10.1001/jama.282.18.1737
27. Shin JH, Kim HC, Jung CH, et al. The standardization of the Korean version of the patient health questionnaire-2. J Korean Neuropsychiatic Assoc. 2013;52(3):115–121. doi:10.4306/jknpa.2013.52.3.115
28. Linda YB, Maria KM, Mary AS, et al. Longitudinal associations of depressive symptoms and pain with quality of life in patients receiving chronic hemodialysis. Hemodialysis Int. 2015;19(2):216–224. doi:10.1111/hdi.12247
29. Cooke RG, Robb JC, Young LT, Joffe RT. Well-being and functioning in patients with bipolar disorder assessed using the MOS 20-ITEM short form (SF-20). J Affect Disord. 1996;39(2):93–97. doi:10.1016/0165-0327(96)00016-x
30. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
31. Shin JS, Lee YB. The Effects of social supports on psychosocial well-being of the unemployed. Korean J Social Welfare. 1999;37:241–269.
32. Lee KS, Kim HY, Lee MH. Factors influencing psychosocial adjustment in hemodialysis patients. Korean J Adult Nurs. 2019;31(1):38–49.
33. Beck AT, Steer RA, Garbin MG. Psychometric properties of the beck depression inventory: twenty-five years of evaluation. Clin Psychol Rev. 1988;8:77–100. doi:10.1016/0272-7358(88)90050-5
34. Lee KM, Lim SM, Kang YH. Psychometric evaluation of self-management scale for hemodialysis patients with arteriovenous fistula. Korean J Adult Nurs. 2017;29(6):637–646. doi:10.7475/kjan.2017.29.6.637
35. Cho YM, Seo YH, Park MJ. Relationship between uncertainty in illness, subjective health status, and compliance with sick role behavior according to levels of health literacy in hemodialysis patients. Korean J Adult Nurs. 2018;30(4):437–446. doi:10.7475/kjan.2018.30.4.437
36. Riegel B, Moser DK, Buck HG, et al. Self-care for the prevention and management of cardiovascular disease and stroke: a scientific statement for healthcare professionals from the American Heart Association. J Am Heart Assoc. 2017;6(9):e006997. doi:10.1161/JAHA.117.006997
37. Lee MJ. Uncertainty, appraisal of uncertainty and health-related quality of life in recovering clients discharged from hospital after CABG. Health Nurs. 2009;21(1):49–63.
38. Stiegelis HE, Hagedoorn M, Sanderman R, et al. The impact of an informational self-management intervention on the association between control and illness uncertainty before and psychological distress after radiotherapy. Psycho-Oncology. 2004;13(4):248–259. doi:10.1002/pon.738
39. Knuth B, Radtke V, Rocha P, et al. Prevalance of depression symptoms and serum levels of interleukin-6 in hemodialysis patients. Psychiatry Clinic Neurosci. 2014;68:275–282. doi:10.1111/pcn.12130
40. Hung KC, Wu CC, Chen HS, et al. Serum IL-6, albumin and co –morbidities are closely correlated with symptoms of depression in patients on maintenance hemodialysis. Nephrol Dialysis Transplant. 2011;26:658–664. doi:10.1093/ndt/gfq411
41. Keskin G, Engin E. The evaluation of depression, suicidal ideation and coping strategies in hemodialysis patients with renal failure. J Clin Nurs. 2011;20:2721–2732. doi:10.1111/j.1365-2702.2010.03669.x
42. Simmons L. Dorthea Orem’s self care theory as related to nursing practice in hemodialysis. Nephrol Nurs J. 2009;36(4):419–421.
43. Nam KH, Tae YS, Kim CS, Lee SM. Influence of uncertainty and uncertainty appraisal on quality of life in prostate cancer patients after prostatectomy. Asian Oncol Nurs. 2017;17(1):45–54. doi:10.5388/aon.2017.17.1.45
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.