Back to Journals » Clinical Interventions in Aging » Volume 18
Influence of Prosthodontic Rehabilitation Using Zygomatic Implants in Covid 19 Related Mucormycosis (Rhino–Orbital–Cerebral) Maxillectomy Patients Upon Post-Operative Stress, Anxiety and Functional Impairment: A Prospective Cohort Study
Authors Kumar L, Verma A, Pal US, Mattoo K ![]() , Algarni YA, Bin Hassan SA
, Algarni YA, Bin Hassan SA ![]() , Baba SM, Jeri SY, Khateeb SU
, Baba SM, Jeri SY, Khateeb SU
Received 16 March 2023
Accepted for publication 20 July 2023
Published 1 August 2023 Volume 2023:18 Pages 1201—1219
DOI https://doi.org/10.2147/CIA.S412625
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Video abstract of "Covid 19 related Mucormycosis maxillectomy rehabilitation with ZI" [ID 412625].
Views: 340
Lakshya Kumar,1 Aditi Verma,1 Uma Shanker Pal,2 Khurshid Mattoo,3 Youssef Abdullah Algarni,4 Saeed Awod Bin Hassan,4 Suheel Manzoor Baba,4 Sumaya Yousuf Jeri,5 Shafait Ullah Khateeb4
1Department of Prosthodontics, King George`s Medical University, Lucknow, Uttar Pradesh, 226003, India; 2Department of Oral and Maxillofacial Surgery, King George`s Medical University, Lucknow, Uttar Pradesh, 226003, India; 3Department of Prosthetic Dental Sciences, College of Dentistry, Jazan University, Jazan, 45142, Kingdom of Saudi Arabia; 4Department of Restorative Dental Sciences, College of Dentistry, King Khalid University, Abha, 61421, Kingdom of Saudi Arabia; 5Department of Orthodontics and Dentofacial Orthopedics, I.T.S Centre for Dental Studies and Research, Chaudhary Charan Singh University, Ghaziabad, Uttar Pradesh, 201206, India
Correspondence: Lakshya Kumar, Department of Prosthodontics, King George`s Medical University, Lucknow, Uttar Pradesh, 226003, India, Tel +91‐9412119778, Fax +91 522 2257539, Email [email protected]
Purpose: To determine the influence of prosthodontic rehabilitation using zygomatic implants in partial maxillectomy upon post-operative stress, anxiety and functional impairment, due to covid 19 associated rhino–orbital–cerebral mucormycosis (ROCM).
Patients and Methods: Twenty maxillectomy patients fulfilling study criterion, received zygomatic implants (ZI) (quad zygoma) (ZDI Simpladent, Switzerland) retained/supported complete maxillary denture. Assessment of stress, anxiety, masticatory performance and speech were determined using diurnal salivary cortisol level, Appearance Anxiety Inventory, multiple sieve technique and auditory perception analysis, respectively. Data were recorded at 6 different stages of rehabilitation (after maxillectomy, implant placement, and after prosthesis delivery (1 week, 1 month, 6 months and 1 year)). Demographic data were expressed as frequency distribution, while mean values were used to find differences between various rehabilitation stages using Friedman and chi-square test with statistical significance value at p < 0.05.
Results: Average daily salivary cortisol levels declined from post maxillectomy (22.80 ± 0.902) to 1 year after prosthesis wearing (8.65 ± 0.985), indicating stress reduction after ZI rehabilitation. Mean scores for appearance anxiety reduced from pre-prosthetic rehabilitation (27.350 ± 3.030) to 1 year (8.950 ± 0.887) following prosthesis wearing. Functional parameters for mastication and speech also improved significantly during the course of rehabilitation. All differences between pre-prosthetic to 1-year stage after prosthesis wearing were found to be statistically significant at p < 0.05.
Conclusion: Post ROCM maxillectomy cases after prosthetic rehabilitation using zygomatic implants showed significant improvement in the psychological (stress and anxiety) as well as function (mastication and speech) characteristics. Rehabilitation post ROCM maxillectomy with the present approach of fixed prosthesis using zygomatic implants mitigates deficient mastication and speech. It also impacts positively on patient psychology by decreasing stress and anxiety.
Keywords: mucormycosis, dental implant, maxillofacial prosthesis implantations, Covid-19
Introduction
A time period of 99 days between March 13, 2021 to June 19, 2021, saw an exponential increase in the number of coronavirus (COVID-19) cases (2.4 times) and related deaths (2.7 times) in India.1 The complacency of being vaccinated, lockdown relaxations saw super spreader gatherings (religious/ political/ marital) culminated into the second pernicious wave of coronavirus pandemic. Amidst the panic, a rare, serious, life threatening and/or disfiguring angioinvasive fungal infection surfaced in the Indian population. The term was popularized by both media and the general public as “black fungus”. The scientific term is Mucormycosis (MM), caused by fungi (Order – Mucorales) described first in 1876.2 The fungi dwell in soil, junk leaves, animal dung and air. The causative agent for MM though varies according to geographic distribution. The path of infection can be inhalation of spores which if unchecked can spread to lungs, sinuses, and also penetrate the blood brain barrier to extend into the brain and eyes.3 Persons infected with MM can present a varied clinical presentation that is reliant on the area involved. Its classification is based on involved organ/organs and is termed accordingly as rhino-orbital cerebral mucormycosis (RCOM), gastrointestinal MM, pulmonary MM, cutaneous MM.4 It may also present as disseminated form or uncommon and rare forms like endocarditis, peritonitis or osteomyelitis.5 Compared to the global prevalence (0.005 per 1.7 million), its prevalence in Indian population (140 per 1 million) is eighty times higher than developed nations.4 Both immunocompromised and immunocompetent patients can be affected, in latter case the effect can result due to traumatic inoculation of the fungus or through burns. Globally, MM has been seen to affect more in type II diabetic patients,4,6 which conforms to its predilection in countries like India, Iran and Mexico,7 while European nations reported hematological malignancy (acute myeloid leukemia, acute lymphoblastic leukemia, non-Hodgkin’s lymphoma, myelodysplastic syndrome) as common underlying diseases.4,6,8 Drug related MM like chronic corticosteroid use and nosocomial MM have also been reported.9,10 Association of MM in covid 19 patients was reported to be due to the use of systemic corticosteroids [n=2371 patients, 87% who used corticosteroids and 13% who did not].11 Macrophage migration, phagolysosome fusion and ingestion are compromised with corticosteroid use, besides chronic use leading to the development of drug induced diabetes.12 MM infection symbolizes in tissue necrosis due to invasion of blood vessels (angioinvasion) further leading to thrombosis, which describes it clinically aggressive, life threatening nature and overall high case fatality rates (50%).6 In cases affecting maxilla, invasion of a sinus through inhalation leads to necrosis of the nasal mucosa, turbinates, and palate. The disease has the ability to spread locally through the whole face, resulting in facial bone necrosis and penetration of orbits and cranium causing mortality. Such condition is called as rhino orbital cerebral mucormycosis and henceforth will be referred in this article as RCOM. Osteomyelitis presentation of RCOM in the maxilla is rare due to thin cortical plates and excellent blood supply, however angioinvasion affects endothelial lining of blood vessels, causing vascular insufficiency and bone necrosis resulting in mucormycosis osteomyelitis.13 Treatment of RCOM is based on controlling infection, improving systemic response and use of antifungal (intravenous) with planned surgical excision of the lesion. Local and systemic treatment is governed by various guidelines [European Conference on Infections in Leukemia (ECIL), European Confederation of Medical Mycology (ECMM)].14,15 The prognosis for RCOM infection largely depends upon early detection followed by medical treatment and surgical resection of the involved part, as the rate of spread of this infection is rapid. Patient-related factors like infection site, underlying condition (controlled/uncontrolled) and immunosuppression extent are key to recovery.16 Despite the fact that medical treatment resolves the infection, it is the surgical excision of the tissue from the body that leaves a permanent mark on the patient both physically and psychologically.
Maxilla is a paired jawbone, fused in the center (intermaxillary suture), the complexity of which lies in the fact that each bone articulates with 9 different bones of the skull (facial −7; cranial −2). It forms the main bulk of the middle third of the face and differentiates three separate facial cavities (oral, nasal and orbital). Maxillectomy is a surgical term/procedure that is used to describe the complete or partial removal of the maxilla, and defects left by maxillectomy pose total closure challenges that are correlated to restoring proper function.17 In covid related RCOM, maxillectomy has been reported to include orbital extensions,18 which further complicates the rehabilitation process. The elimination of the maxilla can have a substantial impact on an entity’s life, unsettling functions such as mastication, speech, swallowing and causing oro-nasal or oral-antral communication. The resulting facial deformity is often stigmatized in society, affecting the patient’s psychology negatively. To complicate things further, a complete resection of maxilla does not preclude an individual that RCOM will not recur. Maxillectomy associated with Covid 19 RCOM has also been the outcome of delayed presentation of symptoms which are often confused with dental pain. Rehabilitation of such cases is multifaceted as major parts of the maxilla is resected which renders prosthodontic treatments puzzling. In cases which are detected early, the resection is limited to maxilla with the zygomatic process remaining intact. In such cases, removable prosthodontic rehabilitation is not possible due to the defect. The concept of “remote bone anchoring” using zygomatic implants, were developed in 1998 and are specifically indicated in severe maxillary atrophy, or congenital/acquired maxillary defects like resection defects.19 Their survival rates have been reported to be high (77 to 100%) after the follow up of 10 years.20 Their survival has also been reported to be independent of primary or secondary placement, with survival as high as 100% been reported during primary ablative surgery placement.21 Conventional endosseous implant placement in maxillectomy patients for maxillary reconstruction requires bone graft augmentation for implant placement. Complications in the form of donor site morbidity, variable uncontrolled graft resorption, non-economical and need for additional surgery have paved way for more conservative implant placements (quad zygoma concept).22,23 Precision of implant placement within available zygomatic bone has improved with the advent of diagnostic aids like CBCT (cone beam computed tomography-CBCT), intra oral scanners, CADCAM (computer assisted design/computer-assisted manufacturing) and DMLS (direct metal laser sintering). Zygomatic implant placement therefore is one of the most conservative and viable rehabilitation options in these cases. By utilizing the trajectory forces of occlusion, the forces can be distributed more widely.24 While oral rehabilitation may bring some psychological and functional improvement in their quality of life, impaired functioning of dental prosthesis after such extensive surgical procedures can be detrimental. Pandemic associated stress followed by development of RCOM that resulted in loss of maxilla and finally a prosthesis that does not function properly can enhance stress/anxiety and lead to the development of depression or other mental health conditions. Therefore, improvement in quality of life that is completely an outcome of prosthetic rehabilitation and independent to loss of maxilla becomes an essential differentiation feature in such studies. This study therefore intended to rehabilitate post-Covid RCOM cases of partial maxillectomy by utilizing zygomatic implants. The aim and objective of the study being to assess the functional and psychological improvement after rehabilitation by evaluation of parameters like speech, masticatory performance and levels of stress and anxiety related to prosthesis functioning. We hypothesized that dental prosthesis supported by zygoma implants will improve mastication and speech and indirectly reduce stress and anxiety levels related to the patient’s inability to perform oral functions. Alternately, the null hypothesis states that no changes in these parameters will be observed at any point of time.
Materials and Methods
Ethics
This study was primarily conducted in the fixed division of the department of Prosthodontics at one of the recognized post-graduate institutes in northern India, where research studies on humans and animals are conducted strictly adhering to the declaration of Helsinki. This clinical study was duly approved by the college and university (King George Medical University, India) ethics committees (No 744/Ethics/21 – Ref code – 99 ECM IIB/P 53). The patients who participated in this study have given a written informed consent after they were briefed about the purpose and benefits of this study and commitment of maintaining their confidentiality in reporting the outcome of the study. All patients provided a written informed consent for publishing the results of the study with/without the use of images. The patient shown an exemplary case in the research article has provided a written informed consent for the images to be published.
Study Design
This study is a single-center, double-blind prospective cohort study that was conducted between the second quarter of year 2021 to the third quarter of year 2022. The study was conducted in three different stages: sampling, intervention and follow-up. Data collection for the study required a sample (purposive sampling) of patients from a general population (cross sectional) who are physically and mentally willing to place zygomatic implants (intervention) and respond during the follow-up period. The study implemented using both qualitative/quantitative measures for data collection and analysis.
Sample Selection, Preparation and Grouping
Dental patients visiting to the outpatient department (directly/referral) for prosthetic rehabilitation after having undergone maxillectomy as a consequence of RCOM associated lesion were considered eligible for the study. Selection of cases for this study was based on strict adherence to the criteria that were characterized as baseline and related to maxillectomy. The baseline criterion included age (18–50), gender (any), systemically uncompromised (except controlled type 2 diabetes), willing to place implants (specific – zygomatic) and participation in the study and positive mental attitude (philosophical or exacting). Maxillectomy associated to RCOM inclusion criteria were post-Covid-19 mucormycosis patients after 6 months of partial maxillary resection, partial maxillectomy with intact zygomatic process and zygomatic bone, vertical (class 1 and class 2) and horizontal component (a and b) for modified maxillectomy defect according to Brown’s classification,25 with or without local soft tissue flap closure, no sign of recurrence (histopathology/radiographic) and adequate amount of zygomatic bone assessed from preoperative CBCT. Any patient presenting with a sign or symptom of RCOM recurrence, chronic sinusitis, less than 6 months of maxillectomy, uncontrolled systemic diseases, drug/smoking/alcohol/tobacco users and medically not suitable for surgical intervention was excluded from the study. From a total of 26 patients screened for CBCT, twenty patients fulfilled the comprehensive criteria and were incorporated in the study.
Clinical Intervention Procedures
A detailed case history was recorded for all patients, which revealed a wide range of post-surgical complications common to all included mastication (difficult eating), phonetics (pronunciation, vowel speaking, consonants, unintelligible speech sounds), regurgitation (nasal to oral and vice versa) and overall poor quality of life. For data comparison at different time intervals, the stress assessment (diurnal salivary cortisol level), appearance anxiety inventory, masticatory performance (sieve method) and auditory perception analysis were all performed and recorded before surgical intervention. Preoperative photographs (frontal and lateral) (Figure 1A and B), orthopantomograph (Gendex GXDP-700 Series OPG System, KaVo, Germany) and a CBCT (CS9300 Carestream, Atlanta, GA) assessment were carried to outline the bone availability/quantity/quality around the remaining zygomatic complex (Figure 1C and D) and were taken/analyzed for all patients in the group (An exemplary case presented). With the help of DICOM (Digital Imaging and Communications in Medicine) file of CBCT, 3D printed acrylic models were obtained for all patients and an extra oral mock implant placement was done with these models for evaluation of implant angulation and anteroposterior spread for better prosthetic outcome (Figure 2A-D). A virtual surgical plan for each patient using a software (Die EXOCAD, Dental CAD, Darmstadt, Germany) planned both surgical and prosthetic mechanical aspects in a three-dimensional format for each zygomatic implant for maximum efficiency in terms of function and durability (Figure 3A-E). The basic surgical and prosthetic technical design for all patients included a three-piece prosthetic design, wide implant framework base covering zygoma, lateral orbit wall extension (bicortical screws), long bars with short connector design (prevent tissue impingement, encroach less restorative space, ensure soft tissue closure between bars), predetermined bar angulation (wider distribution of occlusal forces), cylinder threads attach equator bridge, abutment placement (natural canine and molar areas), bar supported cement retained prosthesis and self-cleansing design.
 |
Figure 1 An exemplary case presentation. (A) Extra oral frontal view of an exemplary patient maxillectomy related midfacial deformity. (B) Lateral view. (C) and (D) CBCT scan for locating zygomatic bone qualitatively and quantitatively. |
 |
Figure 2 3D printed acrylic models seen from (A) back and (B) front. (C) Mock implant placement on left. (D) Mock implant placement on the right. |
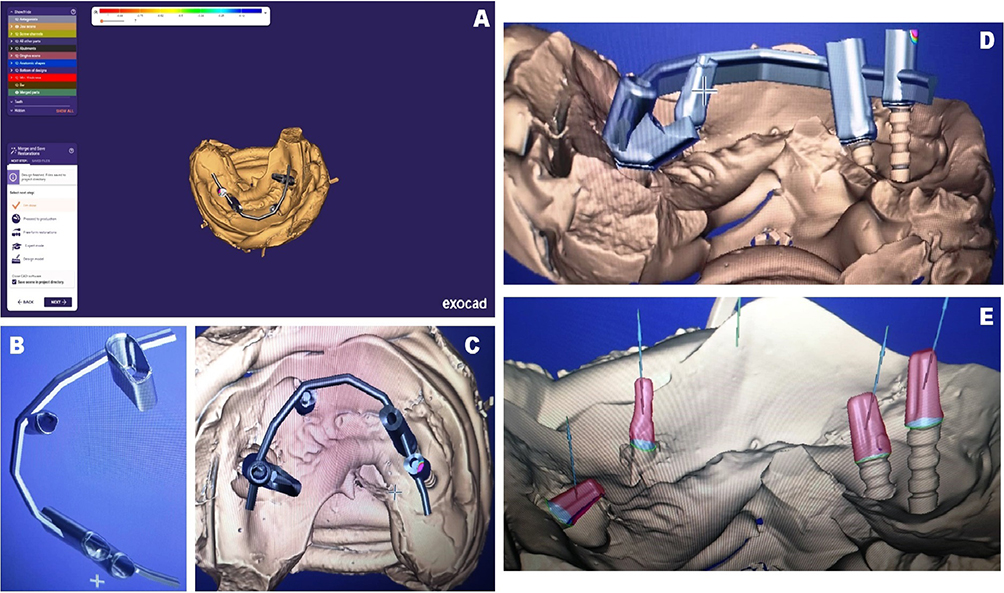 |
Figure 3 (A) Virtual surgical and prosthetic planning using exocad. (B) Isolated planned fixture. (C) Planned fixture superimposed on underlying tissue. (D) Horizontal view of planned fixture. (E) Abutments. |
Surgical Procedure
The surgical intervention was performed under long duration local anesthesia by a multidisciplinary team, following a strict protocol for infection control,26 and pandemic related current patient safety guidelines.27 A flap (full thickness) was raised bilaterally over the body of zygoma using a 15 c Surgical blade (Hu-Friday, Rockwell, St. Chicago). Fibrosed tissue, parotid duct and retracted mucosa were identified as significant surgical landmarks. The zygomatic arch root and frontozygomatic suture were accessed by sub-periosteal undermining over the body of zygoma (Figure 4A). Implant site osteotomy was performed with zygomatic implant drills using the conventional osteotomy preparation protocol. Four smooth surfaced zygomatic implants 4.6/37mm (ZDI Simpladent, Switzerland) (two on each side) were placed in the zygomatic process of maxilla with high primary stability [ISQ (implant stability quotient) > 70 Ncm]. Smooth surfaces on implants are self-cleansing and do not require maintenance. Implants were splinted to distribute the occlusal load to apical threads. Post-operative analgesics and antibiotics were prescribed to all participants. No post-surgical complication was noted and all implants obtained the primary stability.
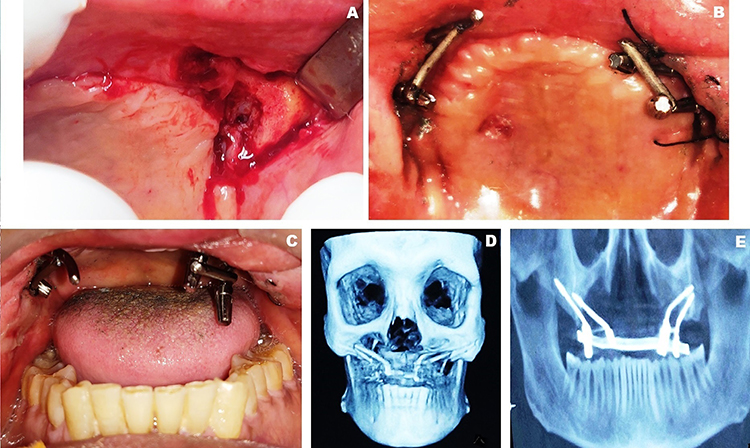 |
Figure 4 (A) Surgical exposure of zygomatic bone. (B) Implants welded using short solid bars. (C) Impression caps in place. (D) Prosthesis design as seen on CBCT. (E) Orthopantomograph with the framework (closed mouth). |
Prosthodontic Procedures
The prosthodontic planning included delivering the prosthesis within a week after surgery. The protruding implants were stabilized using cylindrical titanium bars by an intra-oral welding (International Implant Company, Verona, Italy) procedure/protocol described in the literature (Figure 4B). 28 Impressions with addition silicone elastomeric impression material were then made after placing the impression caps (Figure 4C). Superstructure in the form of bar was fabricated over the implants using metal laser sintering, which was first verified through radiographs (Figure 4D and E) and then cemented in place with resin modified GIC (GC Fuji plus) over the implants. Acrylic prosthesis was designed and fabricated on the bar following routine clinical and laboratory procedures for making single implant supported fixed/removable complete denture prosthesis opposing natural/artificial dentition. Silicon based soft liner (permanent) (Molloplast B, Detax GmbH & Co, KG Ettlingen, Germany) was used for the retention of acrylic prosthesis over the bar. Any part of the implant/implant attachment that would fit improperly was corrected using the chairside clinical technique described in the literature.29 Centric contacts were maintained on the prosthesis using a clinical remount procedure (Figure 5A and B). The patients were given post-insertion instructions regarding use and maintenance of the implant supported prosthesis. Since the list of instructions was for different categories (implant maintenance, prosthesis maintenance, practice for mastication and speech, etc.), the instructions were delivered verbally, written and in the form of an audio. Audio mediated patient health education has been reported to improve patient compliance especially during the course of the pandemic.30 The facial frontal profile observed more improvements (Figure 5C) than the lateral profile (Figure 5D).
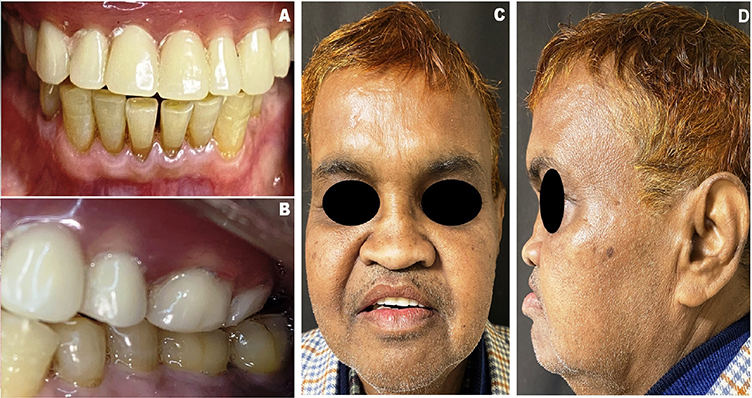 |
Figure 5 (A) Intra oral view showing zygomatic implant retained upper prosthesis against natural dentition. (B) Centric occlusion. (C) Frontal view after prosthesis in place. (D) Lateral view after prosthesis in place. |
Measures, Data Evaluation, Collection and Analysis
Stress Assessment
Measurement of stress was accomplished by a diurnal cortisol slope method.31 The method determines the changes in levels of stress – sensitive hormone (cortisol) from morning to evening, which respond to social and psychological stress by secretion (blood, saliva and urine). Salivary estimation is convenient to patients as it can be done by the patient in his own home setting. The assessment was performed at 6 different time intervals of treatment viz. after maxillectomy, immediately after implant placement, and four time intervals after prosthesis delivery (1 week, 1 month, 6 months and 1 year). At each interval, three recordings of salivary cortisol on the same day were made (at waking time – basal, 30 min after waking, at evening for 10 min – reactive). The tool for measuring cortisol levels in the laboratory was unstimulated mixed saliva (passive drool method). During saliva sample collection, all patients were instructed to be in a relaxed sitting position with the trunk slightly inclined towards the knees, so that the saliva can flow freely into the collection container. Patient advisory for the saliva sample collection included not to eat, drink or smoke (30 minutes least), not to perform any heavy or light exercise and not to swallow the saliva once the collection period starts. All samples were stored in an ice container till they were centrifuged. Centrifugation was done for 15 minutes at 3000 RPM using Eppendorf Centrifuge 5702, separated into Eppendorf tubes, and frozen at −80 °C until laboratory evaluation. Concentration of selected marker for cortisol in saliva was determined to use the appropriate diagnostic kits (Salivary Cortisol—DRG).32
Anxiety Assessment {Appearance Anxiety Inventory (AAI)}
This anxiety measuring tool includes questions (self-report 10 question scale) that are related to the appearance of an individual and how their appearance or change in appearance are affecting their personal and social life. This tool measures general body image anxiety and the cognitive and behavioral changes associated with such body dysmorphic changes.33 The questionnaire was first pilot tested, then retested for its internal consistency, reliability and validity (content, face and construct). It uses the person’s own cognitive ability to assess his distorted image and measures various constructs associated with the patient’s distorted image. The individual has to respond to each question from a score of 0 (not at all) to 4 (all the time). The total score is then summed up, which may range from 0 to 40. Two clinical psychological conditions, body dysmorphic disorder (BDD) and body image anxiety (BIA), can be diagnosed using the AAI. An individual suffering from these two conditions continuously thinks about his defect (in this case could be either perceived) or imperfections in his appearance (maxillectomy) and thus avoid social contact. The 10-item questionnaire assesses two constructs or subscales, avoidance (items 1, 3, 4, 7, 9, 10) and threat monitoring (items 2, 4, 6,8). Anxiety scores are totaled and then compared with the cutpoints for diagnosing BDD and BIA [score 0 to 19 – normal, 19 to 27 – high risk of clinical BDD, 27 and above – clinical diagnosis of BDD].34 If an individual scores 19 or above, then Caseness (clinical case of depression and anxiety related to BDD) is recognized. The assessment was performed at 5 different time intervals viz. after maxillectomy, immediately after implant placement, and three time intervals after prosthesis delivery (1 month, 6 months and 1 year).
Masticatory Performance
One of the measure for functional assessment was testing for masticatory efficiency before and after prosthesis placement using the simplified sieve method as described by Ohara et al.35 Masticatory tasks were performed by chewing the test material (reversible hydrocolloid) (first 10 then 20 strokes) by the participants. After finishing the masticatory process, the expectorate was gargled out over a filter holding glass beaker using plain drinking water. Storage of masticated particles followed in oven (80 degree Celsius for twenty minutes). The bits were then laid on a stack of different sieves (aperture size range 0.50 mm to 4.5 mm) in the machine (Bertel Industria Metalurgica, Brazil). Particles smaller than the sieve mesh were washed away in running tap water, and the remaining particles in the sieve were counted. The counting was performed by the two assessors (blinded) at alternate appointment to follow up following the standard protocol. The retained test particles were then weighed in an analytical balance (0.001 grams) (Mark 2060; Bel Engineering, Lombardy, Italy).36 Masticatory cycle performance was also calculated by the formula [Masticatory performance = [B − A] /10], where value A = number of particles collected in 10 strokes and value B = number of particles collected in 20 strokes. In order to examine the intra-test reproducibility, the procedure was carried out three times, ie, Morning, noon and evening of the same day. This procedure was repetitively done according to the follow-up protocol to examine the inter-test reproducibility. Masticatory performance was assessed at 5 different time intervals before rehabilitation, after rehabilitation with maxillary prosthesis, and three time intervals after prosthesis delivery (1 month, 6 months and 1 year).
Speech Analysis
Speech analysis was assessed through auditory perception analysis (APA).37 The patients were requested to count from 1 to 20 in one analysis and a sample of spontaneous speech for 30 seconds in another analysis, once before and after wearing the prosthesis. Similar standard protocol was followed at each follow-up appointment. The resonance and speech intelligibility were judged by an experienced listener who was a qualified speech therapist and was not aware (blinded) about the patient’s other parameter scores. The assessment is based on a score that is given for various parameters viz. audible nasal air escape, degree of consonant imprecision, open nasality and overall speech intelligibility. Four items are graded to 5-point scale (0 normal to 4 severe).38,39 Lower scores indicate less errors in parameters, while higher scores indicate the opposite.
Statistical Analysis
Data related to demographic characteristics of the patients in the cohort were expressed in frequency distributions for different parameters. Mean and standard deviations were quantified for salivary cortisol levels and masticatory performances, whereas the mean score with standard deviations was calculated in terms of scores for appearance anxiety inventory and speech analysis. Data distribution for normality was performed using the Kolmogorov–Smirnov test. The bounds (upper and lower) in the dataset were expressed at 25th and 75th percentile. Evaluation and comparison of data were done with standard tests such as Friedman test and Chi-square test using the statistical software SPSS 10.0 for Windows by blinded statistician. A probability (P) value less than 0.05 was considered statistically significant. Comparative differences in means for all parameters at various time intervals and various stages of prosthetic rehabilitation were determined using a non-parametric test in which the level of the degree of significance was determined on the value of p < 0.05. A chi square value was derived to indicate how far the mean ranks lie apart in the data obtained.
Results
The data obtained for the study was tabulated as per predefined protocol, and then assessment was performed. Out of all 26 assessed patients, 20 patients fulfilling the study criteria were included. There were no dropouts from sample preparation at each course of the study for the entire period of 12 months.
Demographic Variables
The individuals in the cohort involved a purposive sample of 20 patients (16 males, 4 females). The median age of total group was 58 ± 10.48 years [males (57.5 ± 11.02), females (60 ± 9.01)] (Table 1). Fifty-five percent of the patients belonged to the age group of above 60 years and were living in urban areas. Patients in the cohort completed their respective total treatment without anyone reporting any adverse effect during/after treatment. Other demographic variables like education, occupation, and economic rank were evenly distributed in the parameters (Table 1). Seventy percent of the patients were diabetic uncontrolled at the time of diagnosis of MM, and 40% were diagnosed to be caused by Apophysomyces variabilis while remaining by Apophysomyces elegans and Saksenaea vasiformis. Forty percent of the patients had natural teeth with either a Kennedy class 1 or class 2 partially edentulous arch opposing the resected maxilla.
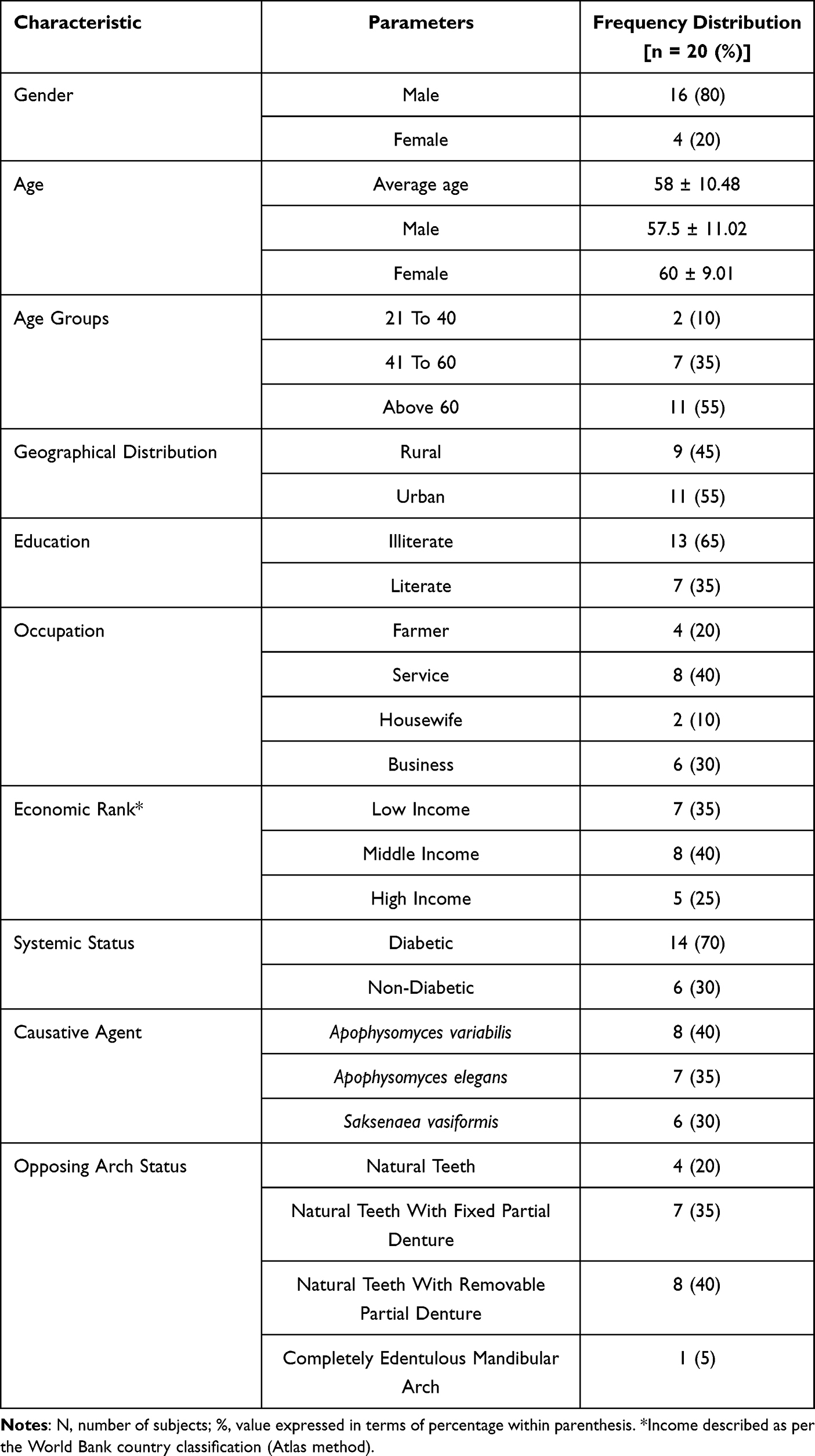 |
Table 1 Demographic Characteristics of the Mucormycosis Associated Partial Maxillectomy Treated with Zygomatic Implant Supported Prosthesis |
Stress Assessment
Stress assessment was performed in all the included participants by measuring diurnal salivary cortisol slope at three specific times of a day (Waking up, 30 min after waking and at evening between 6 and 9 pm). The first recording that was taken after maxillectomy (minimum 6 months according to criteria) showed the maximum value for all daily time intervals and was taken as a baseline for comparison (Table 2). Stress-related cortisol values were almost same till implant placement and showed a reduction in all time daily time intervals after prosthesis delivery. The level of waking up reduced from 22.750 ± 0.966 to 16.445 ± 0.604 in the first month after prosthesis placement which further reduced to 8.500 ± 1.277. Similar decline occurred in other time intervals that were 30 minutes after waking (24.500 ± 1.147 at maxillectomy to 10.600 ± 0.867 at 1 year) and in the evening (21.150 ± 0.745 at maxillectomy to 6.850 ± 0.812) (Table 2) (Figure 6). Graphic representation shows a decline in cortisol level from maxillectomy stage to 1 year follow-up. The differences in the means for all daily time intervals of cortisol levels and at various stages of prosthesis rehabilitation were found to be significant (p < 0.05), suggesting that the stress level was reduced after prosthetic rehabilitation with zygomatic implants.
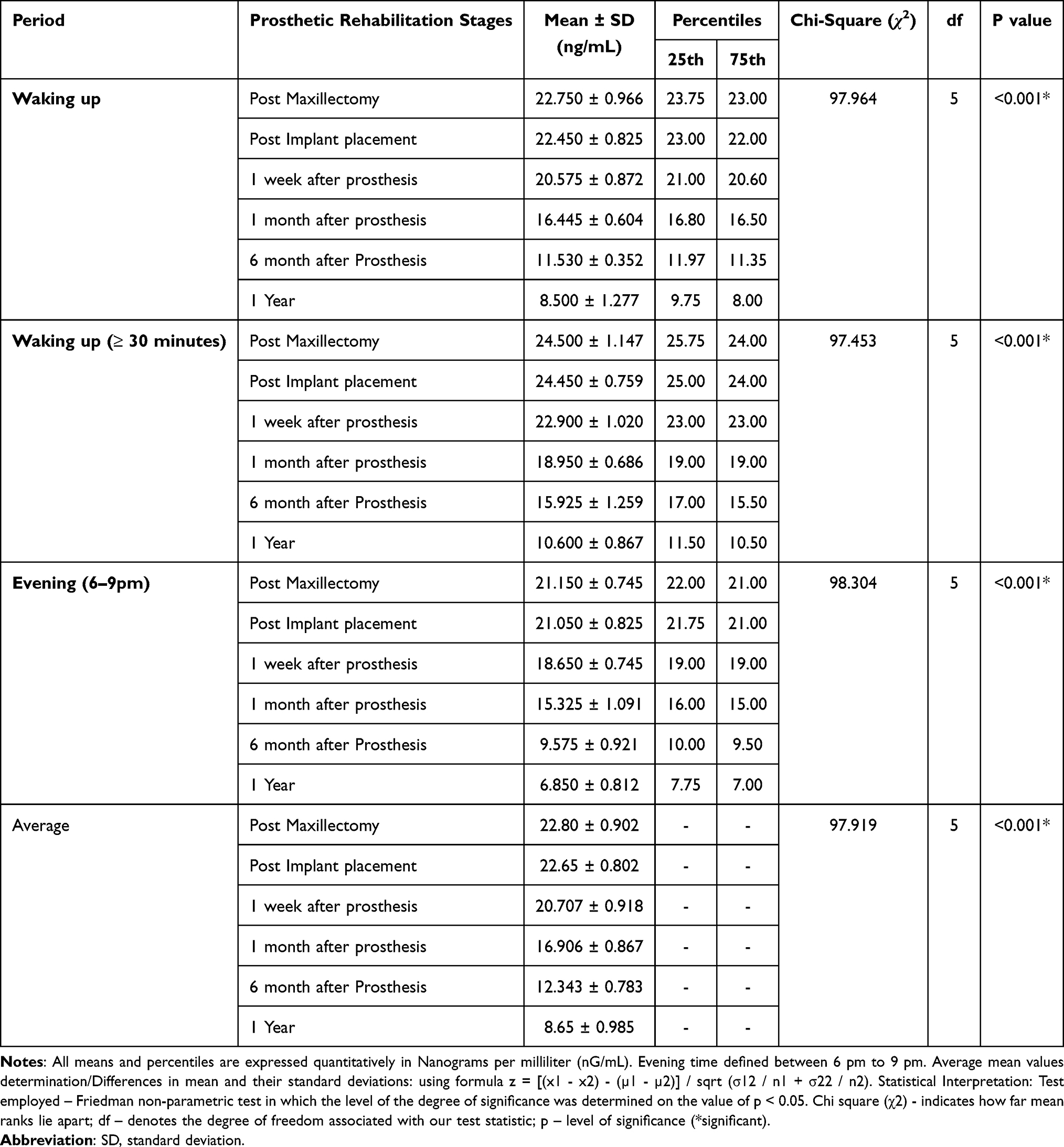 |
Table 2 Comparative Differences in Daily Salivary Cortisol Mean Levels Between Participants Over Three Different Periods of the Day at Different Stages of Prosthetic Rehabilitation |
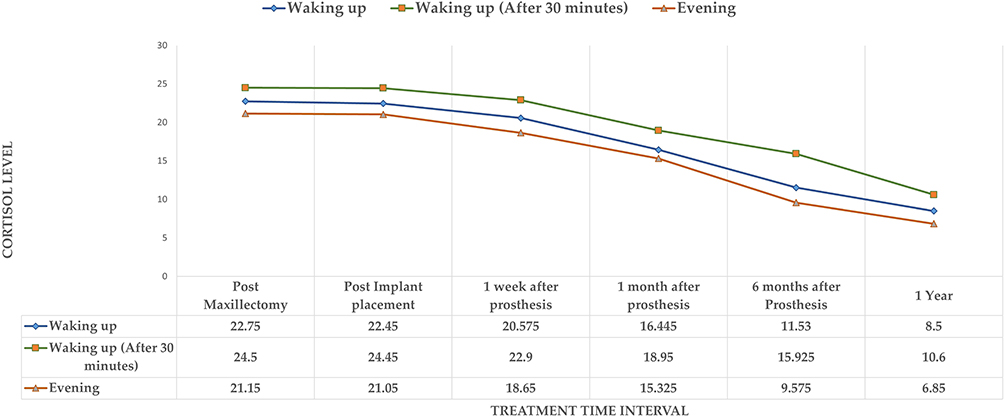 |
Figure 6 Comparative changes in daily salivary cortisol mean levels (ng/ml) during different periods of the day at various stages of prosthetic rehabilitation. |
Anxiety Assessment
A total score of 19 (range 0 to 40) is considered high which qualifies an individual to be diagnostically declared as a case of depression and anxiety (Caseness). Before prosthetic rehabilitation, the mean score in the cohort was 27.350 ± 3.030 which reduced to 16.700 ± 1.174 at immediate prosthetic rehabilitation and further reduced to 13.000 ± 1.486 at 1 month after prosthesis rehabilitation (Table 3). The least score was observed at 1 year (8.950 ± 0.887) which suggests that prosthetic rehabilitation was associated with a decline in anxiety. The differences in means between the rehabilitation stages were all found to be significant at the predetermined level of significance for p value (<0.05).
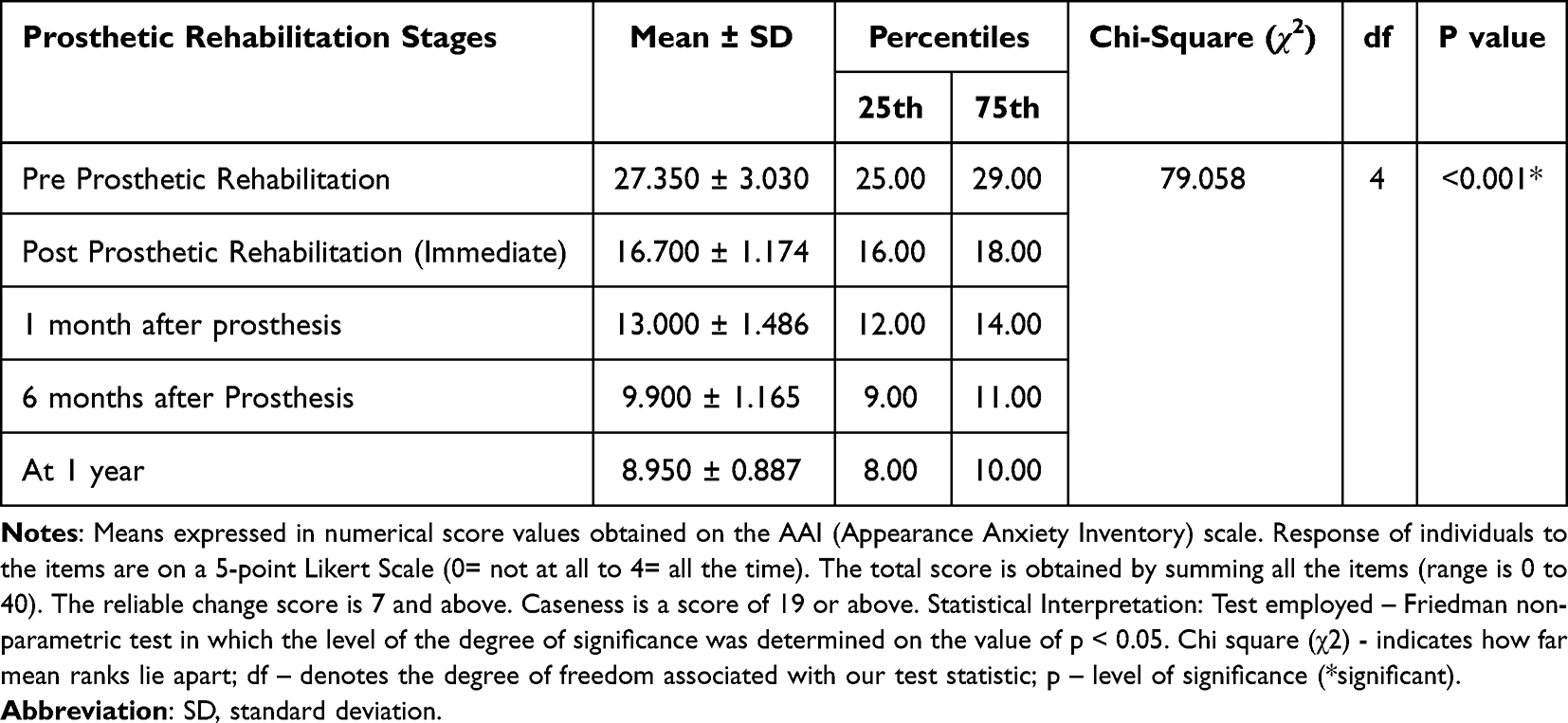 |
Table 3 Comparative Differences in Mean Total Scores of the Cohort on the Appearance Anxiety Inventory Scale at Various Stages of Prosthetic Rehabilitation |
Functional Assessment
Functional efficiency of the prosthesis was assessed for mastication and speech. The results of the study show that the mean weight of the retained particles on the sieve increased from pre-prosthetic rehabilitation (0.149 ± 0.198) to (0.951 ± 0.060) immediately after prosthesis was placed which at the end of 1 year increased further (1.184 ± 0.018) (Table 4). This signified improved mastication of the test food with differences between the baseline values and at the end of 1 year being significant at the p value of ≤0.05. For the function of speech, the results show higher scores of auditory perception analysis before prosthetic rehabilitation (11.100 ± 0.640) which are the sum of four different parameters for speech function. The score got lower with insertion of prosthesis (7.200 ± 1.151) which lowered to (4.250 ± 0.444) at 1 year (Table 5). This suggests that as the prosthesis was worn by the patients there was improvement in speech for parameters assessed (audible nasal air escape, degree of consonant imprecision, open nasality and overall speech intelligibility). The differences as estimated were found to be statistically significant at the p value of ≤0.05.
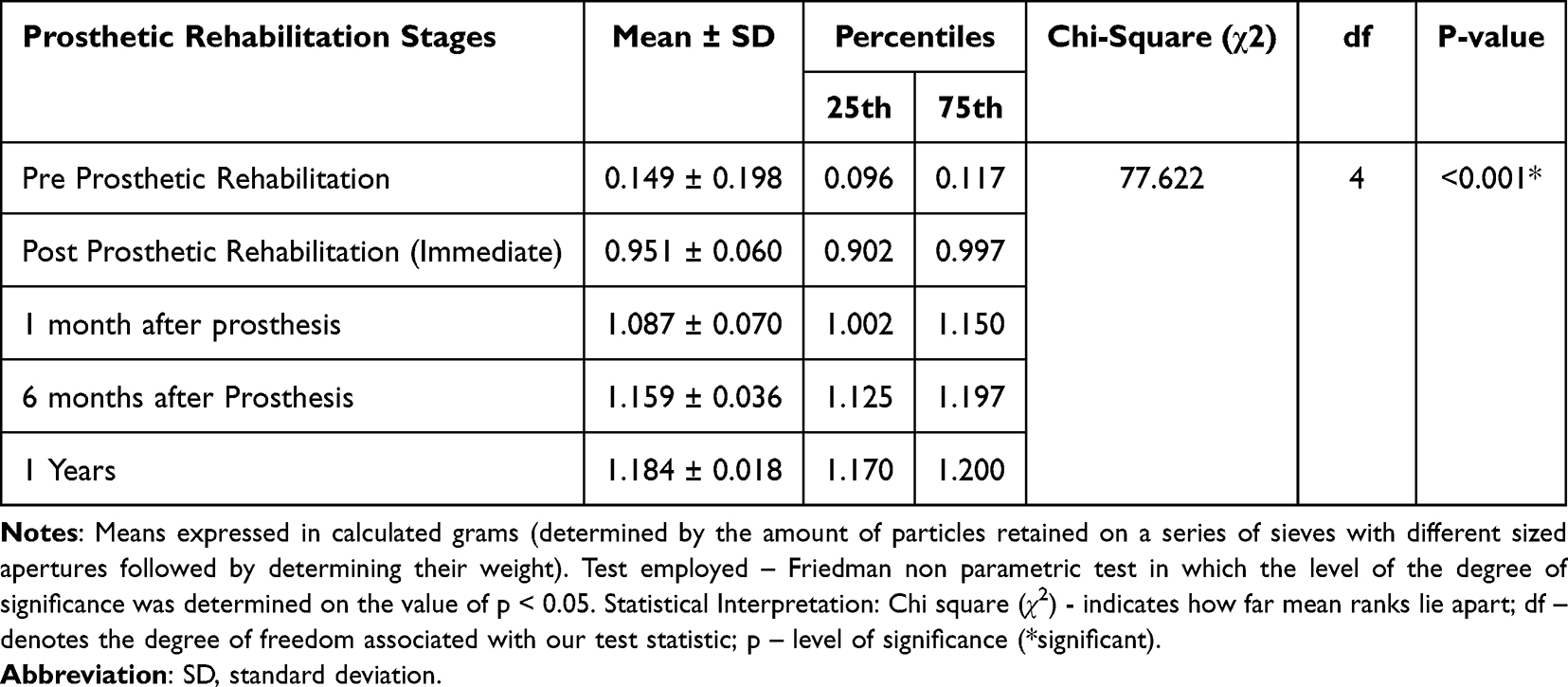 |
Table 4 Comparative Differences of the Mean Particle Size Distribution of the Cohort for Masticatory Performance at Various Stages of Prosthetic Rehabilitation |
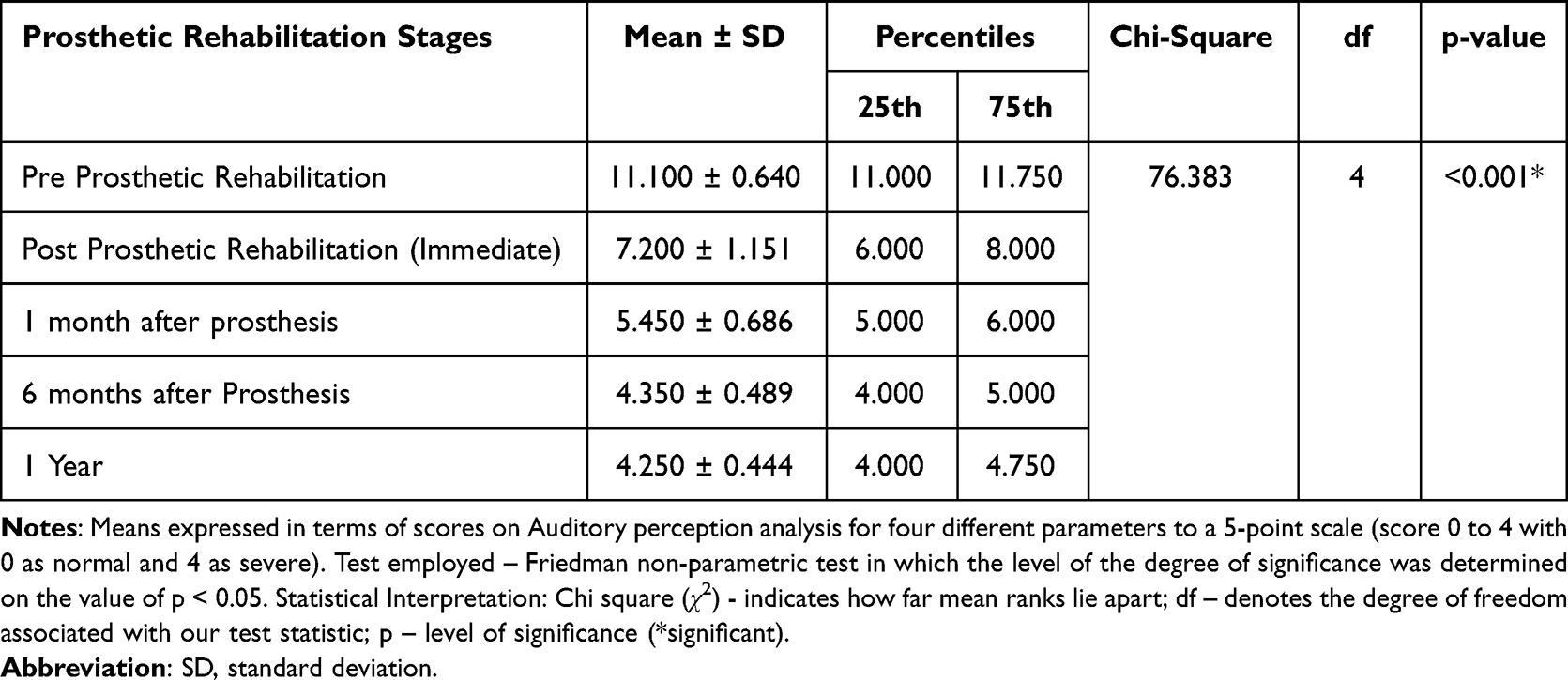 |
Table 5 Comparative Differences in the Total Mean Scores of the Cohort for Speech Assessment at Various Stages of Prosthetic Rehabilitation |
Discussion
This prospective cohort study was undertaken to evaluate the influence of prosthetic rehabilitation using zygomatic implants upon maxillectomy-related stress, anxiety and functional impairment that is commonly observed subsequent to such surgical procedures. The four clinical variables investigated covered two psychological and two functional variables. The main findings of the study demonstrate that after prosthetic rehabilitation there was a sequential reduction in stress as evidenced by gradual reduction of daily salivary cortisol levels (taken at waking up, 30 min after waking up and evening) as the stages of prosthetic rehabilitation were completed [average daily cortisol level of 22.8 ± 1.114 before prosthetic rehabilitation to 16.90 ± 1.054 at 1 month after prosthesis and 8.65 ± 0.907 at 1 year]. These results can also be looked upon as short-term (1 month) and long-term effects (1 year). For anxiety that was related to the appearance (in this case deformity/disfigurement), the average mean of 27.350 ± 3.030 before prosthetic rehabilitation was reduced to 13.000 ± 1.486 at the 1-month interval and to 8.950 ± 0.887 at the 1-year interval. A clinical diagnosis of a person suffering from depression and anxiety is declared when the score is 19 (Caseness); therefore, it can be interpreted that depression and anxiety that developed to deformity after maxillectomy were no longer present at 1-month and 1-year intervals. However, the differences in scores between 1 month and 1 year may not be clinically relevant or significant. For two parameters of functional assessment, there were improvements in both functions of mastication and speech. Mastication improved from 0.149 ± 0.198 before prosthesis to 1.087 ± 0.070 at 1 month and to 1.184 ± 0.018 at 1 year, which shows that maximum changes in masticatory function are observed immediately after prosthesis insertion. Improvement in speech was also observed with maximum being from pre-prosthetic (11.100 ± 0.640) to immediately after prosthesis (7.200 ± 1.151) which later improved gradually till 1 month (5.450 ± 0.686) after which there were not many changes (4.350 ± 0.489 at 6 months and 4.250 ± 0.444 at 1 year). This also suggests that the maximal changes in impaired phonetics are achieved within 1 month after prosthetic rehabilitation. For all the parameters investigated the differences at various time intervals and at various stages of prosthetic rehabilitation were found to be statistically significant, thus accepting the hypothesis that prosthetic rehabilitation brought improvement in all parameters at different time intervals.
Risk Factors for Covid Related ROCM
The patients in the cohort were obtained through purposive sampling which was based on exclusion and inclusion criteria. Eighty percent of the patients found were males, and the average age of both participants was 58 ± 10.48. These characteristics match closely with the reports on covid 12 associated ROCM that have been published independently11 and by the Indian government.40 During the pandemic, the average age of covid 19 patients (hospital admissions) was 45 to 50.7 years with 56 to 93% of them being male.41 Thirty percent of the patients in the group were immunocompetent and had no underlying systemic diseases, while the remaining 70% were diabetic (criteria for inclusion were only diabetic as systemic compromise). From patient’s previous medical records, all immunocompetent patients (n = 6) were diagnosed with causative agent being Apophysomyces elegans, which is in agreement with studies that are not related to covid 19 associated ROCM.42 Use of systemic corticosteroids and underlying untreated diabetes mellitus have been reported to be the strongest risk factors for patient with covid 19 developing ROCM.11,41,42 A diabetic patient receiving systemic corticosteroids has been reported to have very high risk for developing ROCM.11 The presence of diabetes irrespective of being controlled does not preclude an individual any security of not developing ROCM.
A wide-spread number of mucormycosis cases were seen during the COVID-19 recovery period in Indian population, suggesting that multiple factors facilitate fungal colonization. One of the major causes of getting delayed treatment was that patients might have overlooked the symptoms of Mucormycosis (especially pain) confusing it with the residual COVID-19 symptoms and therefore presented later to the hospital. In cases of ROCM, the warning signs include palsy (cranial nerve), double vision (diplopia), sinusitis, swelling (periorbital), ulcer (Palatine), proptosis and/or a syndrome (orbital apex syndrome). To limit the spread of necrosis, it is important to evaluate the maxillary bone involvement through CT (computed tomography) at an early stage.14,43 As soon as it was detected, resection was planned in respective cases depending upon the extent of spread.
Maxillectomy as Surgical Intervention and Role of Zygomatic Implants
Maxillary partial or complete resection was performed in these cases, which although saved the patients’ lives, was associated with psychological and functional impediments. These include but are not limited to impaired mastication, swallowing difficulties (dysphagia), speech difficulties (Dysarthria) and a prodigious impact on the individual’s lifestyle and social interaction. Maxillary reconstruction after maxillectomy remains a great challenge for the reconstructive oral and maxillofacial surgeon and maxillofacial prosthodontist. The American Academy of Maxillofacial prosthetics have duly recognized and recommended obturator as immediate primary rehabilitation.44 The basis of such immediate primary rehabilitation lies in the fact that patients are more vulnerable to develop psychological, social, emotional distress during post-surgical healing.45 Zygomatic bone engagement is one of the most evidence-based techniques when restoring the resected or atrophic cases.46 Zygomatic single-piece implants distribute the occlusal stress through apically engaged threads, which are splinted, and their design is like the Toulouse leg screw with different core and thread diameters.47 Since they are of a single piece with a smooth surface, they have the most acceptable biological seal at the mucosal or skin level.48 Zygomatic implants provide an additional versatile prosthetic treatment option for clinicians in the prosthetic management of maxillary and mid-facial tumors, post-mucormycosis resection, traumatic resections, etc. Immediate or early restoration is allowed in zygomatic implant due to high primary stability within the predominantly compact zygomatic bones. It provides invaluable stability and anchorage for specialized obturator prostheses with much-improved function compared to standard tissue-borne prostheses. Most of the studies involving zygomatic implant associated rehabilitation have been small sampled; however, a larger study sample by Butterworth indicated an overall survival rate of 77 to 100% (131 implants) for a 10-year period, 94% – 1-year survival and 92% – 5-year survival.20 In studies that have reported a low survival rate (77%) for maxillary reconstruction (cases classified as extensive maxillectomy), the failures were attributed to having been done in oncology patients with all failures occurring prior to prosthetic rehabilitation. The complications associated with the surgical phase of zygomatic implants are failing to integrate (osseous), placement/positioning failures, development of oronasal communication, rhinorrhea and mucosal complication.24,42 Other less reported but nevertheless important complications reported are trismus, pain, paresthesia, and contracture. These drawbacks, however, have been overcome with the advent of CT (CBCT) scanning of available bone that determines the precise location where implant should be placed. The use of 3D acrylic models for mock implant placement has further enhanced clinician’s accuracy in implant positioning. The use of CBCT, DICOM, and virtual surgical planning software as done in this study are modern day answers to overcome difficulties in implant positioning at distant sites.
Stress, Anxiety and Functional Assessment
Widely known as the stress hormone, cortisol is released from the adrenal cortex in response to stress. Its release signifies the body to be in a state of high alert in response to a stimulus. Its release is accompanied by an increase in the heart and respiratory rates. This study used salivary cortisol as a biomarker to assess the stress. The schedule of collection of saliva was as per the recommended timings. The advantage of using saliva is that the cortisol levels in the collected saliva are not dependent on the salivary flow rates since they actually correlate with biologically active unbound plasma and serum fraction.31,49 An additional advantage is that cortisol is stable in saliva for up to three months at 5°C and at least one year at −20°C or −80°C.32 However, long-term storage of saliva samples at room temperature is not recommended because of decreased cortisol concentrations every month. The results from our study show that stress levels were decreased as prosthetic rehabilitation progressed. All cortisol levels taken at three different time intervals showed a corresponding decrease with greatest reduction seen in evening levels (Figure 6) [21.150 ± 0.745 post maxillectomy to 6.850 ± 0.812 at 1 year]. In patients with maxillectomy, however there are many variables that could contribute to stress which may confound the observations. Patients may have a continuous psychological stress that may be a result of the loss of an organ present on the face and the associated disfigurement. Such disfigurements have been known to create social detachment of individuals which has been found in it to be stressful.17,50 On the other hand, the stress could be also due to loss of function like mastication and speech. Changes in the stress pattern for three time intervals during various stages of prosthodontic rehabilitation indicate that the stress in these cases was more due to the loss of function and disfigurement associated with maxillectomy, rather than loss of maxilla in itself. However, future studies can be refined by first isolating the stress type and then measuring the two types separately. Higher anxiety levels in this study were observed before implant placement at all-time intervals. Since the idea of getting another surgery could increase the anxiety levels in the patients, the first reading of stress levels was recorded before developing the treatment plan and revealing the use of zygomatic implants as surgical intervention to the patients. The first recording was made subsequent to the first appointment of case history taking. Most of the studies undertaken in relation to maxillectomy associated psychological stress have been done through assessment of quality of life using questionnaire based measuring scales.51,52 Our results are in agreement with studies that have reported decrease in salivary cortisol levels after prosthesis wearing.53 In a study of hemimandibulectomy patients by Kosaka et al, the authors however, reported no significant decrease in salivary cortisol levels for short term prosthesis wear (subjects who had worn a prosthesis for less than 3 months). The differences can be explained on the type of prosthesis (removable versus fixed) and the differences of cases. A removable prosthesis needs more time to adapt and needs to be adjusted repeatedly in the follow up period. Salivary cortisol levels have also been reported to decrease significantly with adjustment of prosthesis.54 The changes have been reported to show a significant decrease after the third adjustment of the prosthesis. In our study, the maximal changes in salivary cortisol could be seen at 1 month after prosthesis. Since the prosthesis is fixed and required non-significant adjustments after wearing, it could be said that the differences between the studies are mainly due to the prosthesis designs (fixed prosthesis that requires minimal adjustments). All adjustments to the prosthesis were accomplished within first few days of follow-up for all patients in the present study.
The results on anxiety levels in this study show that there was a radical reduction in anxiety scores between pre-prosthetic rehabilitation (27.350) and immediate prosthetic rehabilitation (16.7) which gradually reduced further to (8.95) at the end of 1 year. As mentioned previously in terms of anxiety assessment on this scale, a score of 19 is diagnostic of clinical depression. Sudden reduction in anxiety immediately after prosthodontic rehabilitation indicates that the origin of anxiety is more associated with the loss of functions that are inherent to maxillectomy. Another factor influencing anxiety levels could be because of the impact of facial deformity and impaired speech affects social life, which includes the ability to communicate properly with other people. The disfigurement caused by maxillectomy affects midfacial thirds of facial composition which was also enhanced by providing adequate labial and lip support through the prosthesis (exemplary case presentation Figures 1 and 5). Reconstruction of maxillectomy using bone grafts, free flap, obturators and zygoma implant borne prosthesis has been reported to increase patient’s activities and recreation.55 Comparatively, zygoma implant rehabilitation has been reported to be better than other surgical reconstructions (deep circumflex iliac artery flap (DCIA), fibula rehabilitation).56 For maxillectomy patients, the significant thing seems to be rehabilitated and return of loss of function. The type of rehabilitation may not matter in terms of reducing stress and anxiety.45 A study reported to have no difference in oral function between those rehabilitated with implant supported fixed prosthesis and implant supported obturators, but the same study concluded that those with obturators had poorer mental health as compared to fixed prosthesis.57
Functional analysis was done in the present study by assessment of masticatory performance using test material of equal dimension in all individuals before and after prosthesis. We found significant improvement in masticatory performance after zygomatic implant supported prosthesis and this improvement was increasing significantly on each follow-up. Masticatory performance has been reported to improve in multiple studies that include rehabilitation of maxillectomy defects with different prosthodontic treatment options and designs (conventional obturators, implant supported obturators, endosseous implants, zygomatic implants, etc.).35,36,58 Masticatory performance using implant supported obturators has been reported to have better efficiency than a conventional prosthesis.59 Hisashi et al used evaluation sheets for assessing masticatory performance in maxillectomy cases rehabilitated using zygomatic implants, and they found increased chewing scores after prosthodontic treatment with implants.60 Zygomatic implants have been reported to encourage hyperactivity of masticatory muscles in electromyography studies, in spite of absence of periodontal receptors.47,61 This is thought to be the result of fixed prosthesis anchored in the zygomatic bone providing a very stable occlusal table which is necessary in the well-balanced stomatognathic system. Another functional assessed in this study was patients’ improvement in speech using an indirect method that is based on identifying improvements in resonance and consonant expressions. Results show that there was a significant decrease in open nasality, decrease nasal air escape, decrease consonant imprecision and increase overall intelligibility after rehabilitating using zygomatic implants. In a study on conventional obturator, good speech intelligibility after obturator prosthesis has been reported.62 Numerous studies have reported that prosthesis definitely improves speech in patients having undergone surgical removal of oral tissues in cancer treatment.37,38,63 With zygomatic implants, difficulties in speech have been associated with those patients who were wearing a removable complete denture prosthesis before starting the treatment, which has been duly attributed to the problems in speech after zygomatic implant placement.64
Clinical Implications
Rehabilitation of maxillectomy cases post-mucormycosis resection with the present approach of fixed removable prosthesis using zygomatic implant has given satisfactory results in mastication and speech. It also had a positive impact on patient psychology by decreasing stress and anxiety.
Strength and Limitations of the Study
One of the limitations of this study is that the stress assessment that was done was not first established that whether it was due to the loss of an organ or due to loss of function. Since loss of an organ can influence the stress levels that may be also due to loss of function, it is imperative to first identify the nature of the stress first and accordingly assess the stress levels. The present study is also limited by less sample size and study done for 1 year. Future studies with increased number of participants and longer duration are advised.
Conclusion
This study concludes that patients with maxillectomy as a result of complication of covid 19-related RCOM can be successfully rehabilitated with zygomatic implants (four implants) in bringing improvement in stress and anxiety that are more related to loss of function (mastication and speech). This study, within its scope and limitations, also concludes that maxillectomy patients show less anxiety and stress after they are rehabilitated using zygomatic implant supported prosthesis. However, the results of this study pertain to the conditions and methods used in this study and interpretation of the results should be done accordingly.
Data Availability
Data collected during the study have been included in the manuscript. Raw data is in possession of the corresponding author (Lakshya Kumar) and can be provided upon formal request.
Acknowledgments
The authors would like to thank the staff of the surgical and medical department of the King George Medical College for providing the inputs and sharing patient information that was considered relevant to the study. The authors would also like to thank the support provided by the staff and computer specialists in the department of oral medicine and radiology for performing diagnostic tests like CBCT. We would also like to thank the dental technicians for laboratory work done during the course of rehabilitation of these patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Sumaya Yousuf Jeri reports recent affiliation with Basma Tadawi Dental Center, Mahalla, Abha, Kingdom of Saudi Arabia. The authors hereby declare that they had no conflict of interest while treating the patients or conducting this research or while reporting the results of this study.
References
1. Agarwala P, Bhargava A, Gahwai DK, Negi SS, Shukla P, Dayama S. Epidemiological characteristics of the COVID-19 Pandemic during the first and second waves in Chhattisgarh, Central India: a comparative analysis. Cureus. 2022;14(4):56.
2. Fürbringer P. Beobachtungen über Lungenmycose beim Menschen. Virchows Arch. 1876;66:330–365.
3. Sommer AP, Försterling HD, Naber KG, Pitchappan RM. Pulmonary and intranasal delivery of thymoquinone-loaded nanoparticles for Mucormycosis & Covid-19. Precision Nanomed. 2021;4(2):795–800.
4. Skiada A, Pavleas I, Drogari-Apiranthitou M. Epidemiology and diagnosis of mucormycosis: an update. J Fungi. 2020;6(4):265.
5. Revannavar SM, Supriya PS, Samaga L, Vineeth V. COVID-19 triggering mucormycosis in a susceptible patient: a new phenomenon in the developing world?. BMJ Case Reports CP. 2021;14(4):e241663.
6. Jeong W, Keighley C, Wolfe R, et al. The epidemiology and clinical manifestations of mucormycosis: a systematic review and meta-analysis of case reports. Clin Microbiol Infect. 2019;25(1):26–34.
7. Patel A, Kaur H, Xess I, et al. A multicenter observational study on the epidemiology, risk factors, management and outcomes of mucormycosis in India. Clin Microbiol Infect. 2020;26(7):944–e9.
8. Lanternier F, Dannaoui E, Morizot G, et al.; French Mycosis Study Group. A global analysis of mucormycosis in France: the RetroZygo Study (2005–2007). Clin Infect Dis. 2012;54(suppl_1):S35–43.
9. Kontoyiannis DP, Lewis RE. How I treat mucormycosis. Blood J Am Soc Hematol. 2011;118(5):1216–1224.
10. Rammaert B, Lanternier F, Zahar JR, et al. Healthcare-associated mucormycosis. Clin Infect Dis. 2012;54(suppl_1):S44–54.
11. Sen M, Honavar SG, Bansal R, et al. Epidemiology, clinical profile, management, and outcome of COVID-19-associated rhino-orbital-cerebral mucormycosis in 2826 patients in India–Collaborative OPAI-IJO Study on Mucormycosis in COVID-19 (COSMIC), Report 1. Indian J Ophthalmol. 2021;69(7):1670.
12. Jose A, Singh S, Roychoudhury A, Kholakiya Y, Arya S, Roychoudhury S. Current understanding in the pathophysiology of SARS-CoV-2-associated rhino-orbito-cerebral mucormycosis: a comprehensive review. J Maxillofac Oral Surg. 2021;20(3):373–380.
13. Jones AC, Bentsen TY, Freedman PD. Mucormycosis of the oral cavity. Oral Surg Oral Med Oral Pathol. 1993;75:455–460.
14. Cornely OA, Alastruey-Izquierdo A, Arenz D, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019;19(12):e405–21.
15. Groll AH, Pana D, Lanternier F, et al. 8th European Conference on Infections in Leukaemia: 2020 guidelines for the diagnosis, prevention, and treatment of invasive fungal diseases in paediatric patients with cancer or post-haematopoietic cell transplantation. Lancet Oncol. 2021;22(6):e254–69.
16. Said Ahmed WM, Elsherbini AM, Elsherbiny NM, El-Sherbiny M, Ramzy NI, Arafa AF. Maxillary mucormycosis osteomyelitis in post COVID-19 patients: a series of fourteen cases. Diagnostics. 2021;11(11):2050.
17. Mattoo K, Singh M, Rahman S. Rehabilitation of disfigurement associated with maxillectomy by a cheek plumper prosthesis. Am J Med Case Rep. 2014;2(10):200–203.
18. Kumari A, Rao NP, Patnaik U, et al. Management outcomes of mucormycosis in COVID-19 patients: a preliminary report from a tertiary care hospital. Med J Armed Forces India. 2021;77:S289–95.
19. Brånemark PI, Gröndahl K, Öhrnell LO, et al. Zygoma fixture in the management of advanced atrophy of the maxilla: technique and long‐term results. Scandinavian J Plastic Reconstructive Surg Hand Surgery. 2004;38(2):70–85.
20. Butterworth CJ. Primary vs. Secondary zygomatic implant placement in patients with head and neck cancer—A 10‐year prospective study. Head Neck. 2019;41(6):1687–1695.
21. Boyes-Varley JG, Howes DG, Davidge-Pitts KD, Brånemark PI, McAlpine JA. A protocol for maxillary reconstruction following oncology resection using zygomatic implants. Int J Prosthodontics. 2007;20(5):65.
22. Cerea M, Dolcini GA. (2018) Custom-made direct metal laser sintering titanium sub periosteal implants: a retrospective clinical study on 70 patients. Biomed Res Int. 2018;1–11.
23. Davó R, David L. Quad Zygoma Protocol. Atlas Oral Maxillofac Surg Clin North Am. 2021;29(2):243–251.
24. Schmidt BL, Pogrel MA, Young CW, Sharma A. Reconstruction of extensive maxillary defects using zygomaticus implants. J Oral Maxillofacial Surgery. 2004;62:82–89.
25. Brown JS, Rogers SN, McNally DN, Boyle M. A modified classification for the maxillectomy defect. Head Neck. 2000;22(1):17–26.
26. Al Makramani BMA, Al Sanabani F, Mattoo KA. Reviewing infection control in prosthodontic practice with a case of herpes simplex in the times of a coronavirus pandemic. Ann Romanian Soc Cell Biol. 2021;25(6):10898–10904.
27. Mattoo KA, Jain S. Managing prosthodontic (geriatric) patients during the SARS-CoV-2 pandemic. J Int Oral Health. 2020;12:S69–75.
28. Degidi M, Nardi D, Piattelli A. Immediate loading of the edentulous maxilla with a definitive restoration supported by an intraorally welded titanium bar and tilted implants. Int J Oral Maxillofac Implants. 2010;25:1175–1182.
29. Mattoo K, Singh SP, Brar A. A simple technique to align attachment components in implant supported mandibular overdenture. Int J Res Med Sci Technol. 2014;1(1):6–8.
30. Sindi AS, Mittal R, Mattoo K, et al. Impact of an Auditory Mediated Patient Health Education (PHE) Program on Treatment Compliance and Satisfaction Among Patients Seeking Prosthodontic Care During COVID Pandemic–A Prospective Interventional Study. Patient Prefer Adherence. 2022;16:1247–1255.
31. Adam EK, Quinn ME, Tavernier R, McQuillan MT, Dahlke KA, Gilbert KE. Diurnal cortisol slopes and mental and physical health outcomes: a systematic review and meta-analysis. Psychoneuroendocrinology. 2017;83:25–41.
32. Arafah BM, Nishiyama FJ, Tlaygeh H, Hejal R. Measurement of Salivary Cortisol Concentration in the Assessment of Adrenal Function in Critically Ill Subjects: a Surrogate Marker of the Circulating Free Cortisol. J Clin Endocrinol Metab. 2007;92:2965–2971.
33. Veale D, Eshkevari E, Kanakam N, Ellison N, Costa A, Werner T. The Appearance Anxiety Inventory: validation of a Process Measure in the Treatment of Body Dysmorphic Disorder. Behav Cogn Psychother. 2014;42:605–616.
34. Mastro S, Zimmer-Gembeck MJ, Webb HJ, Farrell L, Waters A. Young adolescents’ appearance anxiety and body dysmorphic symptoms: social problems, self-perceptions and comorbidities. J Obsessive Compuls Relat Disord. 2016;8:50–55.
35. Ohara A, Tsukiyama Y, Ozawa T, Koyano K. A simplified sieve method for determining masticatory performance using hydrocolloid material. J Oral Rehabil. 2003;30:927–935.
36. Gonçalves TM, Sanchez-Ayala A, Ambrosano GM, Garcia RC. Female hormonal fluctuation and masticatory function in patients with disc displacement-a case-control study. Int J Prosthodont. 2011;24(4):320–327.
37. Kent RD. Hearing and believing: some limits to the auditory-perceptual assessment of speech and voice disorders. Am J Speech Language Pathol. 1996;5(3):7–23.
38. Asal S, Hassan S. Speech Assessment in Patients Rehabilitated with Obturators Lined with New Permanent Soft Liner. Egypt Dent J. 2011;57(649):659.
39. Kotby MN, Haleem EK, Hegazy M, Safe I, Zaki M. Aspects of assessment and management of VP dysfunction in developing countries. Folia Phoniatrica and Logopedica. 1997;49:139–146.
40. Singh AK, Singh R, Joshi SR, Misra A. Mucormycosis in COVID‑19: a systematic review of cases reported worldwide and in India. Diabetes Metab Syndr. 2021.
41. Mohan A, Tiwari P, Bhatnagar S, et al. Clinico‑demographic profile and hospital outcomes of COVID‑19 patients admitted at a tertiary care centre in north India. Indian J Med Res. 2020;152:
42. Sridhara SR, Paragache G, Panda NK, Chakrabarti A. Mucormycosis in immunocompetent individuals: an increasing trend. J Otolaryngol. 2005;34:402–406.
43. Song G, Liang G, Liu W. Fungal co-infections associated with global COVID-19 pandemic: a clinical and diagnostic perspective from China. Mycopathologia. 2020;185(4):599–606.
44. Mattoo K, Jain K. Speech enhancing prosthesis for acquired cleft palate. J Med Sci Clin Res. 2015;3(2):4396–4399.
45. Kumar L, Rao J, Mattoo KA, Yadav A. Finger prosthesis with an alternative approach. J Coll Phys Surg Pak. 2012;22(01):58–60.
46. Chrcanovic BR, Albrektsson T, Wennerberg A. Survival and complications of zygomatic implants: an updated systematic review. J Oral Maxillofacial Surgery. 2016;74(10):1949–1964.
47. Lacroix T, Jaby P, Nokovitch L, Chaux-Bodard AG. Prosthetic rehabilitation with zygomatic implants after maxillectomy: a systematic review. J Dent Oral Disord. 2020;6:1132.
48. Migliorança RM, Irschlinger AL, Peñarrocha-Diago M, Fabris RR, Javier AV, Zotarelli Filho IJ. History of zygomatic implants: a systematic review and meta-analysis. Dent Oral Craniofac Res. 2019;5:1–9.
49. Fouladi DB, Nassiri P, Monazzam EM, Farahani S, Hassanzadeh G, Hoseini M. Industrial Noise Exposure and Salivary Cortisol in Blue Collar Industrial Workers. Noise Health. 2012;14:184–189.
50. Lebel S, Castonguay M, Mackness G, Irish J, Bezjak A, Devins GM. The psychosocial impact of stigma in people with head and neck or lung cancer. Psycho‐oncology. 2013;22(1):140–152.
51. Irish J, Sandhu N, Simpson C, et al. Quality of life in patients with maxillectomy prostheses. Head Neck. 2009;31(6):813–821.
52. Silveira AP, Gonçalves J, Sequeira T, et al. Patient reported outcomes in head and neck cancer: selecting instruments for quality of life integration in clinical protocols. Head Neck Oncol. 2010;2:32.
53. Kosaka M, Sumita YI, Otomaru T, Taniguchi H. Differences of salivary cortisol levels between long-term and short-term wearers of dento-maxillary prosthesis due to head and neck cancer resection. J Prosthodont Res. 2014;58(1):41–47.
54. Kosaka M, Sumita YI, Taniguchi H, Suzuki T, Sasaki K. Evaluation of salivary cortisol levels in relation to dento-maxillary prosthesis adjustment. J Prosthodont Res. 2019;63(1):73–77.
55. Rogers SN, Lakshmiah SR, Narayan B, et al. A comparison of the long-term morbidity following deep circumflex iliac and fibula free flaps for reconstruction following head and neck cancer. Plast Reconstr Surg. 2003;112(6):1517–1525.
56. Landes CA. Zygoma implant‐supported midfacial prosthetic rehabilitation: a 4‐year follow‐up study including assessment of quality of life. Clin Oral Implants Res. 2005;16(3):313–325.
57. Wang F, Huang W, Zhang C, Sun J, Qu X, Wu Y. Functional outcome and quality of life after a maxillectomy: a comparison between an implant supported obturator and implant supported fixed prostheses in a free vascularized flap. Clin Oral Implants Res. 2017;28(2):137–143.
58. Buurman DJ, Speksnijder CM, Engelen BH, Kessler P. Masticatory performance and oral health‐related quality of life in edentulous maxillectomy patients: a cross‐sectional study to compare implant‐supported obturators and conventional obturators. Clin Oral Implants Res. 2020;31(5):405–416.
59. Matsuyama M, Tsukiyama Y, Tomioka M, Koyano K. Subjective assessment of chewing function of obturator prosthesis wearers. Int J Prosthodontics. 2007;20(1):56.
60. Ozaki H, Sakurai H, Yoshida Y, Yamanouchi H, Iino M. Oral Rehabilitation of Oral Cancer Patients Using Zygomatic Implant-Supported Maxillary Prostheses with Magnetic Attachment: three Case Reports. Case Rep Dent. 2018;2018:1694063.
61. de Rossi M, Palinkas M, Lucas B, et al. Masticatory muscle activity evaluation by electromyography in subjects with zygomatic implants. Med Oral Patol Oral Cir Bucal. 2017;22(3):e392.
62. Rieger J, Wolfaardt J, Seikaly H, Jha N. Speech outcomes in patients rehabilitated with maxillary obturator prostheses after maxillectomy: a prospective study. Int J Prosthodontics. 2002;15(2):4565.
63. Bothur S, Garsten M. Initial speech problems in patients treated with multiple zygomatic implants. Int J Oral Maxillofacial Implants. 2010;25(2):89.
64. Gheorghiade M, Konstam MA, Burnett JC, et al. Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan (EVEREST) Investigators. Short term clinical effects of tolvaptan, an oral vasopressin antagonist, in patients hospitalized for heart failure: the EVEREST Clinical Status Trials. JAMA. 2007;297:1332–1343.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Rhino-Orbital-Cerebral Mucormycosis in a Young Diabetic Patient with COVID-19 in Ethiopia: A Case Report
Alemayehu FM, Abate HK, Soboka TA, Huluka DK, Worke AB, Abrie MT, Dibaba DK, Asnake YB
International Medical Case Reports Journal 2022, 15:251-257
Published Date: 19 May 2022