Back to Journals » Patient Preference and Adherence » Volume 19
Influence of Potential Pharmacodynamic Drug Interactions in Pharmacotherapy of Coronary Heart Disease with Comorbid Conditions on Treatment Adherence: A Cross-Sectional Study of a Ukrainian Patient Cohort
Authors Dolzhenko M ![]() , Bilousova NA
, Bilousova NA ![]() , Sirenko YM
, Sirenko YM ![]() , Lobach L, Kozhuharyova NA
, Lobach L, Kozhuharyova NA ![]()
Received 24 July 2025
Accepted for publication 30 October 2025
Published 15 November 2025 Volume 2025:19 Pages 3615—3632
DOI https://doi.org/10.2147/PPA.S552550
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Maryna Dolzhenko, Natalia Anatoliyivna Bilousova, Yuriy M Sirenko, Lidia Lobach, Nataliia Anatoliivna Kozhuharyova
Cardiology Department, Shupyk National Healthcare University of Ukraine, Kyiv, Ukraine
Correspondence: Natalia Anatoliyivna Bilousova, Cardiology Department, Shupyk National Healthcare University of Ukraine, Kyiv, Ukraine, Email [email protected]
Purpose: Coronary heart disease (CHD) is accompanied by a high level of comorbidity, which necessitates the use of complex treatment regimens in pharmacotherapy. In such cases, multicomponent pharmacotherapy significantly increases the risk of pharmacological interactions, which can result in either enhanced therapeutic effects (synergism) or adverse outcomes (antagonism, toxic effects). These drug interactions may influence the level of adherence to treatment in patients with CHD with comorbid conditions.
Purpose of the Study: To assess the systemic impact of potential drug-drug interactions (pDDI), classified by type of pharmacodynamic response (synergism, antagonism, toxicity), on adherence to pharmacotherapy in patients with CHD with comorbid conditions, with subsequent prediction of risks associated with reduced adherence to treatment.
Materials and Methods: The study examined medical data of patients with CHD with comorbid conditions (n = 145) based on the analysis of prescriptions from hospital medical records for pDDI using standardized databases Medscape and Drugs.com. This study is cross-sectional, as it involved a single analysis of complex treatment regimens for drug compatibility and patient surveys conducted within the defined time frame (from October 2024 to June 2025). A survey of patients was conducted to determine adherence to pharmacotherapy of CHD with comorbid conditions using the standardized Medication Adherence Report Scale (MARS-5) scale. Nonparametric statistical methods were used, Spearman correlation analysis, ordinal logistic regression, and prediction to establish associations and determine the impact between pDDIs present in pharmacotherapy of CHD with comorbid conditions in prescriptions for pharmacological synergism, antagonism, and toxic effects due to pDDIs on adherence to treatment. Retrospective, clinical-epidemiological, frequency, content analyses, comparisons, and generalizations were used.
Results: Unacceptable polypharmacy was identified in 95.86% of cases within the studied cohort. A strong positive correlation was noted between the number of pDDIs and pharmacodynamic synergism (rs = 0.738), antagonism (rs = 0.659), and toxic effects (rs = 0.554). The number of concurrently administered medications was associated with a proportional increase in pDDIs, reflecting fundamental principles of clinical pharmacology. Results from the Kruskal–Wallis test revealed statistically significant differences in the number of pDDIs among patient groups with varying levels of adherence to pharmacotherapy (Kruskal–Wallis H = 7.31, p = 0.0258). Notably, each unit increase (one drug prescription) in pharmacodynamic antagonism was associated with a 1.74-fold higher likelihood of non-adherence to treatment, holding other variables constant in the adherence model. Furthermore, higher levels of pharmacodynamic antagonism and toxic effects resulting from pDDIs were correlated with greater likelihood of refusal to continue pharmacotherapy. Specifically, each unit increase in drug-induced toxic effects due to pDDI was linked to a 1.36-fold increase in the probability of low treatment adherence, assuming the fixed effect of other model variables. Pharmacodynamic antagonism and toxic effects attributable to pDDIs are key determinants of reduced adherence to pharmacotherapy in patients with CHD with comorbidities. The increased probability of antagonistic or toxic interactions due to pDDIs indirectly diminishes patients’ willingness to comply with medication and treatment regimens.
Conclusion: Pharmacological pDDIs due to pharmacodynamic antagonism (OR ~ 1.74) and toxic effects resulting from pDDIs (OR ~ 1.36) significantly increase the risk of low adherence to treatment. The identified risks can be minimized by implementing a multidisciplinary approach to providing medical care and involving clinical pharmacists in the quality control of complex prescription regimens and in optimizing pharmacotherapy of CHD with comorbid conditions.
Keywords: polypharmacy, drug interactions, treatment adherence, pharmaceutical care, patient safety, Coronary Heart Disease
Introduction
CHD remains the leading cause of mortality in the world and in Ukraine.1 In modern clinical practice, the treatment of coronary heart disease increasingly involves complex drug regimens with the framework of multicomponent pharmacotherapy,2 especially among patients of elderly and senile age with comorbid conditions. Analysis of selected pharmaceutical components in drug prescriptions, based on current clinical recommendations and the European Society of Cardiology (ESC) guidelines on the management of CHD,3 with concomitant arterial hypertension (AH),4 dyslipidemia,5 chronic heart failure (CHF),6 type 2 diabetes mellitus (T2DM),6,7 and chronic kidney disease (CKD),8 showed the simultaneous use of more than 4–5 drugs in such patients and the prevalence of polypharmacy in 74% of prescriptions in Ukraine,9 which is also supported by data from international studies.2,10,11 Additionally, the ESC and AHA recommendations advocate for the use of different pharmacological classes of drugs but do not adequately address their compatibility when combining agents from distinct groups within complex treatment regimens for coronary heart disease, often accompanied by multiple comorbidities. This limitation hampers the safe administration of medications in such regimens, potentially resulting in adverse consequences due to drug incompatibility, decreased treatment effectiveness, and an increased risk of undesirable adverse drug reactions (ADRs).
It should be noted that there is no clear definition of the term “polypharmacy”. However, as noted in the Clinical Consensus Statement of the Heart Failure Association of the ESC, polypharmacy is defined as the daily intake of ≥ 5 drugs. At the same time, hyperpolypharmacy refers to the daily intake of ≥ 10 drugs.12
It is clear that, polypharmacy can be classified as acceptable (rational pharmacotherapy based on evidence-based medicine) and unacceptable (associated with an increased risk of drug interactions). In turn, drug-drug interactions (DDIs) may manifest as pharmacodynamic synergism, antagonism or increased toxic effects of drugs due to their interaction. Additionally, pharmacokinetic interactions must be considered, as they can lead to an enhancement or reduction of therapeutic effects due to alterations in absorption, distribution, and metabolism, taking into account the role of CYP450 isoenzymes such as 3A4, 2C9, 2C19, 2D6, etc.13
In the process of identifying factors influencing low adherence to treatment among patients with CHD with comorbid conditions in Ukraine (13.9% [95% CI: 13.9 ± 0.002; p < 0.0001]), we previously conducted a series of studies. According to their results, Ukrainian patients demonstrate a preference for original (brand-name) medicines (42.8%) and tend to choose effective pharmacotherapy (χ2 = 3,350.232; p = 0.067).14 Notably, only 7.8% of CHD patients with comorbidities reported using medications included in the national reimbursement program (“Affordable Medicines”) [95% CI: 7.8 ± 0.05; p < 0.0001].14 Our findings suggest that one of the primary barriers to adherence to this program is the absence of high-cost but essential drugs from the reimbursed list – such as direct oral anticoagulants, Sodium-Glucose Cotransporter 2 (SGLT2) inhibitors, and triple fixed-dose combinations.14 Furthermore, our research revealed that treatment adherence improved 22-fold (OR = 22.67) when patients received joint consultations from both physicians and pharmacists, compared to physician-only consultations. The most frequently cited reason for discontinuation of pharmacotherapy among Ukrainian CHD patients with comorbidities was “gastrointestinal complications” (49.4%).14
These findings led us to further investigate the potential causes of these gastrointestinal complaints.14 We hypothesized that the reported adverse effects could be attributed to DDIs. Therefore, we undertook an analysis of prescriptions to assess dose accuracy and drug compatibility, focusing on pharmacological interaction types. The goal was to determine whether inappropriate drug combinations might represent a novel factor contributing to treatment discontinuation due to gastrointestinal complications in this patient population.
Furthermore, our search for scientific data on the selected research topic revealed notable gaps in current knowledge, which heightened scientific interest and underscored the relevance of this problem. The results obtained will further enable the identification of specific areas where pharmacists can influence treatment adherence in patients with CHD with comorbid conditions, thereby supporting the development of targeted interventions to improve adherence, tailored to national characteristics of patients.
It is known that pharmacodynamic antagonism may reduce the treatment efficacy by counteracting the action of another drug, while toxic effects due to interactions may increase the risk of ADR, thereby contributing to decreased adherence. At the same time, pharmacodynamic synergism may enhance therapeutic efficacy and improve clinical outcomes, but it may also complicate drug safety. Therefore, understanding these types of interactions has a significant impact on optimizing pharmacotherapy and ensuring the safe use of drugs, especially in cases of polypharmacy in patients with CHD with comorbid conditions, potentially improving outcomes and quality of life.
Thus, it is relevant to assess the systemic impact of pharmacodynamical pDDIs on adherence to treatment among patients with CHD with comorbid conditions. The use of evidence-based, individualized approaches in selecting rational pharmacotherapy and monitoring pDDIs may further improve treatment effectiveness and patient quality of life.
Materials and Methods of the Study
The study was conducted at the Department of Cardiology of the P.L. Shupyk National University of Health Care of Ukraine. In this study, a one-time survey on adherence to treatment CHD with concomitant comorbid conditions (complex treatment regimens) was conducted using paper questionnaires during the hospital inpatient stay. In addition, a one-time analysis of the medical histories of the patients was conducted during their stay in the hospital inpatient department using their medical records from October 2024 to June 2025. The collected data allowed us to establish the prevalence of polypharmacy in drug prescriptions in CHD with comorbid conditions and pDDIs. In addition, to identify associations between treatment adherence and pDDIs.
This study used a non-probability convenience sample, consisting of 145 patients who were consecutively recruited at a single healthcare facility during a defined data collection period. This design has both limitations and justifications.
The sample size (n=145) reflects the accessible population, rather than a pre-calculated minimum. Under the conditions of ongoing military conflict, it was not feasible to adhere to classical probability-based sampling or conduct randomized recruitment. The use of convenience sampling is ethically justified, as it enables rapid collection of critically important data for pilot and exploratory studies while minimizing operational and psychological burden on patients and healthcare staff.15 Although this approach limits the external generalizability of findings, it is acceptable in applied health research where the aim is to identify patterns and associations rather than to generate a fully representative population sample.16 Given the exploratory nature of the study and the non-normal distribution of adherence data, nonparametric statistical methods (Kruskal–Wallis test and median test) were applied. For the analysis, nonparametric criteria (Kruskal–Wallis and median test) were used, which are adequate under the condition of non-normal data distribution. The sample size (n=145), provided that in each compared subgroup n≥5, allows the application of χ2-approximation with a sufficient level of reliability. With n = 145 and subgroup sizes ≥ 5, the χ2-approximation for these tests remains statistically valid.17 This ensures adequate statistical power and high internal validity for detecting clinically relevant differences in adherence levels within the observed cohort. This approach provides high internal validity of the conclusions within a specific cohort group and confirms the statistical robustness of the chosen approach. The use of convenience sampling18 is a common practice in clinical and epidemiological studies assessing adherence to treatment and the factors that determine it (eg, studies of adherence to antihypertensive therapy in a tertiary care center),19 where the Cochrane method is used, because there are available statistical data on the prevalence of hypertension in patients.19 Although our study used a convenience sample, the achieved sample size (N = 145) is comparable to the sizes of similar adherence studies, in which minimum sample sizes were calculated using Cochran’s formula.19 This comparison provides an approximate benchmark, indicating that the chosen sample is sufficient to ensure robust statistical analysis, especially given the use of nonparametric methods and the observed subgroup sizes. For Ukraine, there are no such data for the given population. At the time of the military conflict in Ukraine, all statistical data is closed. The sample is representative of the accessible patient population rather than the entire national population, which limits external validity. However, internal validity is preserved due to the use of robust nonparametric methods and clearly defined inclusion criteria.
This approach represents a pragmatic compromise between scientific rigor, ethical considerations, and operational feasibility in an extreme research environment.
Inclusion criteria: patients with a diagnosis of CHD, who had a history of unstable angina, acute coronary syndrome (STEMI/NSTEMI), who had previously undergone percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) with and without an acute coronary event. With HF I–IV functional class according to NYHA. With/without T2DM, dyslipidemia, CKD. The study was conducted based on the analysis of medical documentation (extracts from the medical history of inpatients) and subsequent questionnaires of patients in the inpatient department. The duration of the cardiovascular event for each patient participating in the study was from six months to 2 years inclusive. The average age of the patients was 60.5 ± 5 years. A total of medical prescriptions in the medical histories of inpatients were analyzed and 145 patients were interviewed. Patients provided written informed consent for the use of medical data for scientific purposes.
Exclusion criteria included: malignant neoplasms, rheumatic diseases, myocardial infarction and stenting or coronary artery bypass grafting without an acute cardiovascular event for more than 2 years prior, acute cerebrovascular accidents (CVA), transient ischemic attacks (TIA), severe forms of CKD, decompensated diabetes, end-stage CHF and no patient required extracorporeal hemodialysis.
Analysis of clinical characteristics of patients between the categories of adherent and non-adherent to treatment was not performed due to the fact that this was not provided for by the design of our study.
We did not assess ADRs, because such observations did not occur and they were absent. In general, the studied patients were discharged from the hospital in satisfactory condition. Differentiation between the types and severity of ADRs did not occur, which is confirmed by the absence of completed adverse reaction cards of the Pharmacovigilance Center under the Ministry of Health of Ukraine.
Our study investigated the association between the number of concurrent pDDIs in the complex pharmacotherapy of CHD with comorbidities and the likelihood of pharmacodynamic synergism, antagonism, or toxic effects, as well as the subsequent impact on adherence to such pharmacotherapy.
The next step was to assess overall adherence to complex pharmacotherapy for CHD with comorbid conditions (hereinafter referred to as adherence to treatment) using the standardized MARS-5, which employs a five-point scale.20,21
We did not calculate a total MARS-5 score (ranging from 5 to 25). Instead, patients were classified into three groups based on their individual item response patterns to reflect clinically meaningful adherence levels.
The MARS-5 scale has demonstrated good internal consistency and construct validity across various patient populations (Cronbach’s α usually ranging from 0.68 to 0.89).20,22 Our study did not modify the instrument itself but rather applied a pragmatic categorization of the resulting scores to facilitate statistical comparison. This approach preserved the validated structure of MARS-5 while improving interpretability and addressing data sparsity issues.
The specified methodology assumed the frequency of taking or skipping medication: all the time (100% or 5 points); almost all the time (90% or 4 points); most of the time (75% or 3 points); about half the time (50% or 2 points); less than half the time (<50% or 1 point). In this study, we used a 5-point scale from 1 to 5, which further simplified the calculations for groups of adherent and non-adherent to treatment with natural numbers. In addition, the methodology we used to determine adherence to treatment was applied in the observational studies EUROASPIRE IV, V (Ukrainian patients participated)23 and INTERASPIRE,24 which followed a cohort of patients with clinical data similar to our patients. However, the name of the MARS-5 methodology is not mentioned in these studies. We then grouped the responses into three categories: category 1.0 included patients with the highest adherence to treatment (5 points); category 3.0 included patients (1 point) with the lowest adherence to treatment. All other patients (2–4 points) were assigned to category 2.0 with average adherence to treatment. This approach allowed us to conduct statistical analysis. Based on medical records and patient questionnaires, adherence to pharmacotherapy was categorized as follows:
1.0 – “high” (adherent to treatment) – “I take regularly” (5 points);
2.0 – “medium” (average adherence to treatment) – “sometimes missed medication – no more than once a week” (2–4 points);
3.0 – “low” (lack of adherence to treatment) – “I often miss medication – 2 or more times a week” (1 point).
Therefore, a score of 5 point on each MARS-5 item indicates maximum adherence (answering “never” to questions about skipping, changing doses, forgetfulness, etc).25 A point of 1 reflects minimal adherence to treatment (“very often” I skip). Points 2–4 correspond to intermediate behavior (partial or inconsistent adherence to treatment), which has common features: adherence is present, but it is insufficient. Thus, three logical levels are formed that have a clinical interpretation: minimal adherence to treatment (1 point); intermediate/partial adherence to treatment (2–4 point); maximal (5 point). In the literature, dichotomization is often performed according to the total MARS-5 score.26,27 Thus, MARS-5 categorization is a common practice. Our approach differs in that we create three categories instead of two to show gradations of adherence to treatment, which may have additional clinical value. In addition, the MARS-5 scale is prone to ceiling and floor effects (in cases where >15% choose the maximum/minimum point). This approach can lead to sparsity (small number of observations) in some intermediate categories (2, 3, 4) (if counted separately as separate subcategories of adherence to treatment), which avoids the use of sparse data.22 Thus, combining intermediate points (2–4) is a pragmatic solution for achieving stability, reliability of statistical results, in the case of an initial data distribution that is asymmetric and sparse.
In addition, all patients’ prescriptions were analyzed the drug prescriptions from the medical history extracts for compatibility by a clinical pharmacist using a drug interaction calculator, based on standardized data from the “Drug Interaction Check” tools available on Drugs.com and Medscape.28,29 At the same time, the assessment of ADR in patients was not directly carried out, but only the theoretical probability of pDDIs was considered. The determination of the types and severity of ADR was not carried out, which was not foreseen by the design of this study. When analyzing the textual descriptions of pDDIs from the Drugs.com and Medscape databases in the “Drug Interaction Check” section,28,29 the content analysis method was applied.
The number of theoretical pDDIs was determined separately for each prescription and for all prescriptions collectively. The results of the analysis were grouped into the following categories: pharmacodynamic synergism, pharmacodynamic antagonism, and toxic effects resulting from drug interactions. All drug prescriptions were checked for compliance with clinical guidelines3 and for the rational use of prescribed dosages in accordance with the official drug instructions registered in Ukraine. This verification was performed using data from the State Register of Medicinal Products of Ukraine.30
To determine appropriate statistical methods for analyzing the variables “Number of Drugs per Prescription” and “Total pDDIs per Prescription”, a normality test of data distribution was conducted. Specifically, the Kolmogorov–Smirnov and Lilliefors tests were applied to assess the deviation of the empirical distribution from the theoretical normal distribution. The results obtained formed the basis for selecting subsequent statistical analysis methods, namely non-parametric approaches.
To compare three independent groups based on the level of adherence to treatment (“high”, “medium”, “low”) for a quantitative variable that did not meet the assumptions of parametric tests, the Kruskal–Wallis test and the Median test for independent samples were employed. The following hypotheses were formulated:
- Null hypothesis (H0): The distributions of the studied quantitative variable across the three adherence groups (“high”, “medium”, “low”) are the same; there are no statistically significant differences between the groups.
- Alternative hypothesis (H1): The distributions of the studied quantitative variable differ in at least one of the adherence groups; there is a statistically significant difference between at least two of the groups of adherence to treatment.
To assess the relationships between quantitative variables, Spearman’s rank correlation method was applied. This non-parametric approach is suitable for identifying monotonic associations without assuming normal distribution. In particular, the relationships between the variable “Total pDDIs per Appointment” and the pharmacodynamic effects of drugs – synergism, antagonism, and toxicity – were analyzed. Spearman correlation coefficients (rs) were calculated for each pair of variables, with statistical significance set at p < 0.05.
Furthermore, Ordinal Logistic Regression was used to predict the values of the dependent variable “Adherence to Treatment”, which is ordinal in nature with three ordered categories (“high”, “medium”, “low”). This method enables the modeling of the probability of an individual belonging to a specific or higher category of the dependent variable based on one or more independent variables. In this study, treatment adherence was predicted as a function of factors such as pharmacodynamic synergism, pharmacodynamic antagonism, and drug toxicity due to their interaction. For categorical independent variables, the results were interpreted by estimating the odds ratios of being in a higher adherence category.
Subsequently, the potential impact of pharmacodynamic synergism, antagonism, and toxic effects resulting from pDDIs on treatment adherence was evaluated. The results of an ordinal logistic regression model were also justified and employed to predict treatment adherence.
To predict treatment adherence in patients with high and very high cardiovascular risk, a set of associations between adherence and other clinical and pharmacological indicators was previously established for analysis:
- To confirm, using Spearman’s rank correlation, the reliability of associations between the “Total number of pDDIs” per appointment and parameters such as “Pharmacodynamic synergism”, “Pharmacodynamic antagonism”, and “Toxic drug effects” on the patient;
- To confirm, using the Kruskal–Wallis test, statistically significant differences in the distribution of the “Number of drugs” per appointment among different categories of “Adherence to treatment”.
However, while correlation analysis is valuable for identifying pairwise relationships between variables, it does not assess the combined impact of multiple predictors on a dependent variable, nor does it account for the effects of confounding variables. Additionally, it cannot model the likelihood of an observation belonging to a specific category of the dependent variable.
Given that the key dependent variable – “Adherence to treatment” – is ordinal in nature (ordered categories: high, medium, low), ordinal logistic regression was selected for predictive modeling.
The following predictors were included in the regression model:
- pharmacodynamic synergism;
- pharmacodynamic antagonism;
- toxic drug effects;
- total number of pDDIs per prescription.
The variable “Number of drugs” was also considered for inclusion, but its absence in the derived parameter tables required additional clarification.
A clinical-epidemiological method was used to analyze the prevalence of different types of pharmacodynamic interactions (synergism, antagonism, toxicity) in a cohort of patients with coronary heart disease and comorbid conditions. This enabled characterization of the epidemiological profile of the sample, including age, gender, comorbidities, disease duration, and prescription patterns.
A frequency analysis method was used to calculate the incidence of each type of pDDIs, allowing identification of the most common types of negative pharmacological interactions that impact treatment adherence.
The average number of drugs and the average age of patients, in the drug prescriptions were calculated using the following formula for mathematically determining the mean value of a data set:
 , where
, where  - number of medicines in one prescription/number of patients/, n - total number of prescriptions/total age of patients.31
- number of medicines in one prescription/number of patients/, n - total number of prescriptions/total age of patients.31
At the level of the CI 95%,  = 1,96; confidence interval (p<0.001), the difference in indicators was considered significant.
= 1,96; confidence interval (p<0.001), the difference in indicators was considered significant.
The accumulation, correction, systematization and visualization of the obtained results were performed using Microsoft Office Excel spreadsheets. Statistical processing was carried out using STATISTICA 13 and IBM SPSS Statistics.
The methods applied included: retrospective, statistical, clinical-epidemiological, frequency, content analysis, comparison, generalization, and prediction.
This study complies with the requirements of the Declaration of Helsinki of the World Health Organization “Ethical Principles for Medical Research Involving Human Subjects” (International Ethical Guidelines for Biomedical Research Involving Human Subjects, 2016). Protocol No. 9/5 dated October 24, 2024 of the Commission on Ethics and Academic Integrity of the Shupyk National University of Healthcare of Ukraine.
Results of the Study
The study included 145 patients with CHD with or without concomitant type T2DM (23.45% [95% CI: 23.45 ± 0.04; p < 0.001]), dyslipidemia (92.41% [95% CI: 92.41 ± 0.02; p < 0.001]), and CHF (45.52% [95% CI: 45.52 ± 0.04; p < 0.001]). The average age of the patients was 60.5 ± 5 years. In addition, the average number of drugs prescribed per single prescription was 6.27. A total of 64 drugs were used by international non-proprietary name, which are used for CHD with comorbid conditions, including antihypertensive, lipid-lowering, hypoglycemic, and antidepressant medicines. The distribution of the number of drugs per patient is presented in Figure 1.
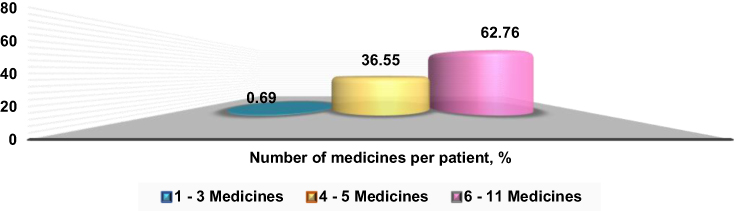 |
Figure 1 Distribution of the number of medicines per patient, in partial proportion. |
After checking the compatibility of the prescribed drugs, it was found that the median per drug prescription (treatment regimen) was 7 drug interactions, the upper-lower quartiles (25–75%) were 5 and 9 interactions, the minimum number was 0, the maximum number was 24 interactions. A total of 1119 pDDIs were identified. In 23 cases, the prescribed drug dosages did not comply with the official instructions for use (doses without indications for use; exceeding the maximum or minimum daily dose). It was established that accepted polypharmacy was observed in 4.14% of patients [95% CI: 4.14 ± 0.02; p < 0.001]. In the remaining 95.86% of prescriptions [95% CI: 95.86 ± 0.02; p < 0.001], unacceptable polypharmacy was identified, characterized by pDDIs not being accounted for, most commonly due to pharmacodynamic antagonism and toxic effects resulting from pDDIs (Figure 2).
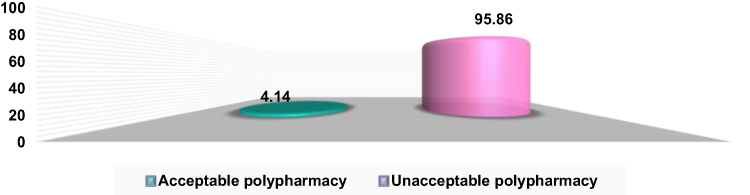 |
Figure 2 Distribution of drug prescriptions by rational use of drugs in prescribed pharmacotherapy (%). |
Further, pDDIs were classified into the following categories:
1.0 – Pharmacodynamic synergism;
2.0 – Pharmacodynamic antagonism;
3.0 – Toxic effect on the body as a result of pDDIs;
4.0 – an abnormal level of potassium in the blood (known as dyskalemia), which can be either too high (hyperkalemia) or too low (hypokalemia), further called dyskalemia.
The results of the observation demonstrated the following quantitative distribution of drug interactions by specified category in natural indicators (Figure 3).
 |
Figure 3 Distribution of pDDIs by categories in natural indicators. |
The normality of the distribution of the variables “Number of Drugs per Prescription” and “Total pDDIs per Prescription” was assessed through both visual analysis and formal statistical tests. Visual inspection of histograms with superimposed normal distribution curves (in red color) indicated that the “Number of Drugs” variable exhibits asymmetry, characterized by a long right tail and a peak in the range of 4–5 drugs per prescription (Figure 4).
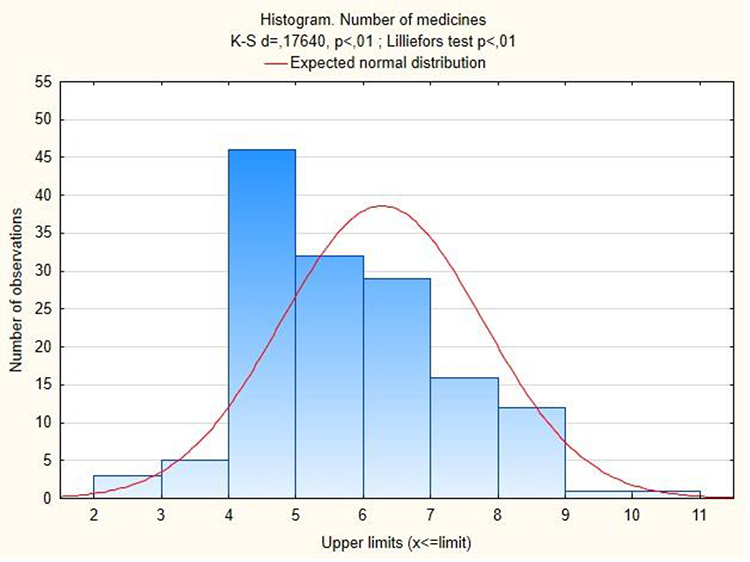 |
Figure 4 Histogram of the distribution of “Quantity of medicines” per single prescription with an overlaid normal distribution curve of the number of medicines per prescription. |
In contrast, the “Total pDDIs” variable appeared more symmetrical, with a peak around 5–10 pDDIs and tapered tails on both sides (Figure 5).
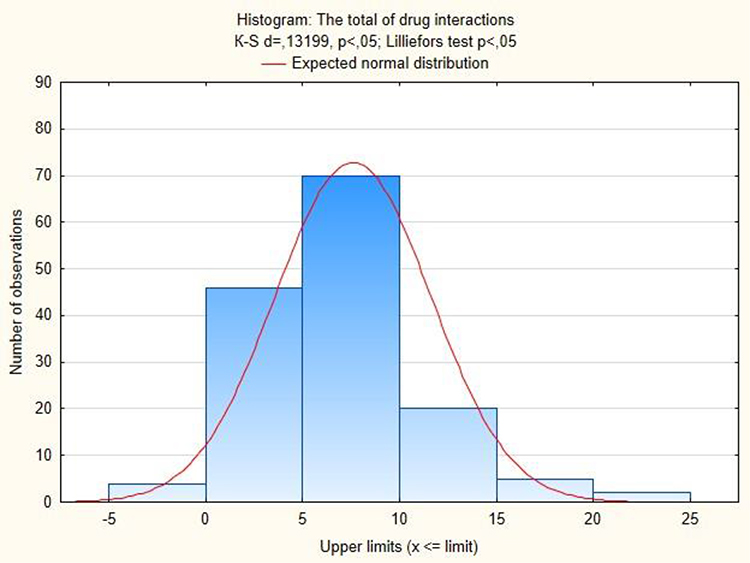 |
Figure 5 Histogram of the distribution of “Total pDDIs” with an overlaid normal distribution curve quantity of medicines. |
However, results from the formal Kolmogorov–Smirnov tests (d = 0.17640 and d = 0.13199, respectively; p < 0.01 and p < 0.05) confirmed that both variables significantly deviate from a normal distribution. Therefore, despite the partial visual resemblance of the “Total pDDIs” distribution to normality, statistical analysis must account for this deviation. As a result, non-parametric statistical methods that do not assume normality – such as the Kruskal–Wallis test – were selected for further analysis involving these variables and categorical group comparisons.
To compare the distribution of the variable “Number of Drugs per Prescription” among the three categories of “Adherence to Treatment”, non-parametric statistical tests were applied: the Kruskal–Wallis test and the Median test.
The results of the Kruskal–Wallis test revealed statistically significant differences in the number of prescribed drugs between groups of patients with varying levels of adherence to treatment (H = 19.18335, p = 0.0001). The obtained data confirm a significant difference between groups of patients with different levels of treatment adherence in the distribution of the number of medications prescribed per appointment. In addition, the median test further confirmed statistically significant differences in medians between groups (χ2 = 13.8293, df = 2, p = 0.0010).
The median value of the variable “Number of Drugs per Prescription” in the overall study sample was 6, reflecting the central tendency of the distribution (Figure 6).
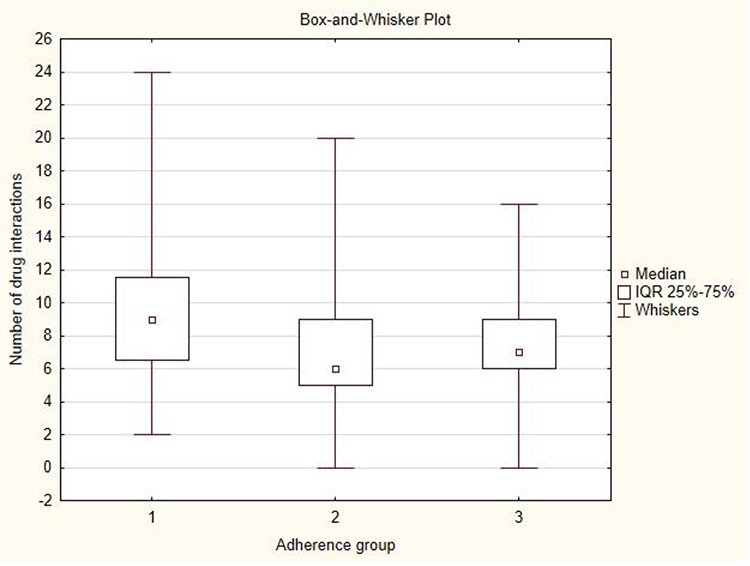 |
Figure 6 Distribution of “Number of medications taken” among different categories of “Adherence to treatment”. |
Based on the results of the analysis, non-parametric statistical tests were used to compare the distribution of the variable “Number of pDDIs per Prescription” across the three categories of “Adherence to Treatment”: the Kruskal–Wallis test and the Median test.
The results of the Kruskal–Wallis test revealed statistically significant differences in the number of pDDIs between groups of patients with different levels of adherence (H = 7.3146, p = 0.0258). The data obtained demonstrated a significant difference in the distribution of pDDIs among patient groups with different levels of treatment adherence.
According to the results of the median test (χ2 = 5.728496, df = 2, p = 0.0570), statistical significance was not confirmed (p > 0.05). The insufficient differences in medians did not reach the accepted level of significance, which may be attributed to high variability within groups or a limited sample size.
The median value for the variable “Number of pDDIs” per prescription in the overall study population was 7, indicating the central tendency of the distribution. Figure 7 presents a box and whisker plot illustrating the distribution of “Number of pDDIs” across the different adherence level groups.
 |
Figure 7 Normal value ± statistical error in groups “Number of pDDIs” per prescription with “Adherence to treatment”. |
The results of the Spearman correlation analysis for the variable “Number of pDDIs” per prescription in relation to pharmacodynamic synergism, antagonism, and toxic effects of drugs are presented in Table 1. The table shows Spearman correlation coefficients (rs). Statistically significant correlations at the p < 0.05 level are highlighted in bold.
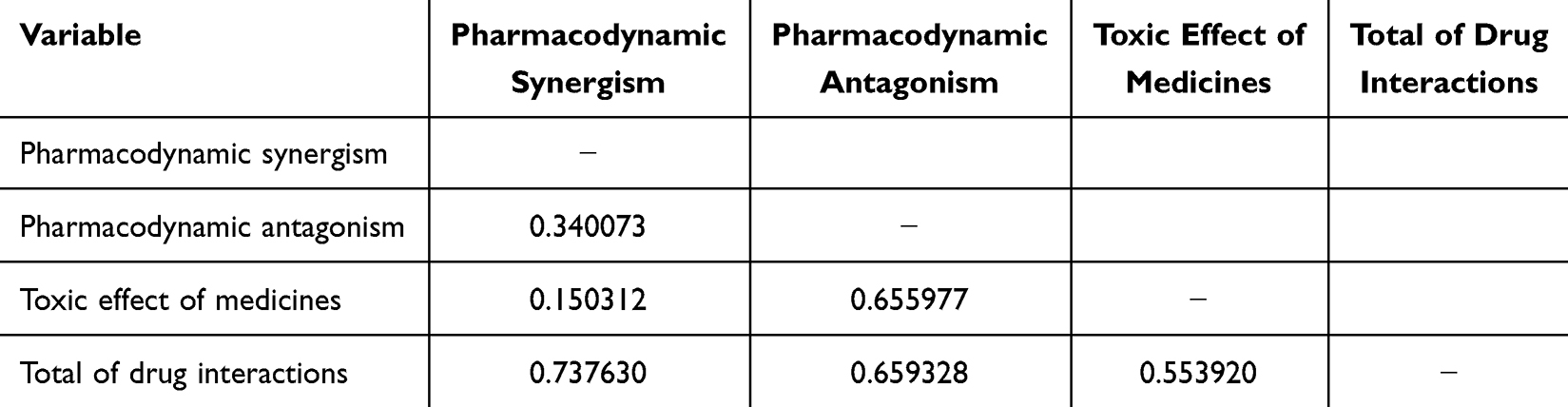 |
Table 1 Results of the Spearman Correlation Analysis: Associations Between Different Categories of pDDIs |
The results of the Spearman correlation analysis (Table 1) between the number of pDDIs per prescription and pharmacodynamic synergism yielded a Spearman correlation coefficient (rs) of 0.737630 at a significance level of p < 0.05.
This value (rs = 0.737630) indicates a strong positive monotonic relationship between the variables “Total of pDDIs” and “Pharmacodynamic synergism.” This implies that an increase in the total number of pDDIs is clearly associated with an increased likelihood of synergistic effects. The results suggest that as the number of drugs prescribed per patient increases, the incidence of pharmacodynamic synergism also rises. These synergistic interactions may have positive clinical outcomes, such as enhancing therapeutic efficacy, but they can also lead to adverse outcomes, depending on the nature of the interaction – for example, increasing the risk of bleeding or orthostatic hypotension due to cumulative drug effects.
The analysis of the Spearman correlation (Table 1) between “Total pDDIs” and “Pharmacodynamic antagonism” showed a correlation coefficient (rs) of 0.659328 at p < 0.05. This indicates a moderate to strong positive monotonic relationship, confirming that a higher number of pDDIs is associated with a greater likelihood of antagonistic pharmacodynamic effects. These results point to a direct relationship between multicomponent pharmacotherapy and the risk of pharmacodynamic antagonism, which may lead to a reduced therapeutic effect or the need to adjust drug dosages due to competing mechanisms of action.
In addition, the Spearman correlation coefficient between “Total pDDIs” and “Toxic effect on the body” was found to be rs = 0.553920 (p < 0.05), indicating a moderate positive monotonic relationship. This result suggests a clear trend: as the number of pDDIs increases, the risk of toxic effects on the body also rises. These toxic effects may result from increased metabolic burden on the liver or kidneys, altered plasma drug concentrations, or other pharmacokinetic and pharmacodynamic mechanisms.
The findings are critically important for ensuring drug safety in patients with CHD with comorbid conditions, as polypharmacy increases the risk of ADRs and complications related to drug accumulation, metabolic overload, and unfavorable interactions.
Particular attention was drawn to the indicators of “Toxic effects on the body” due to the use of certain drug combinations. In this study, the following combinations were observed in patients, along with their respective frequencies and confidence intervals:
- acetylsalicylic acid (ASC) with clopidogrel (34.48% [95% CI 34.48 ± 0.04; p<0.001]);
- ASC with ticagrelor (31.03% [95% CI 31.03 ± 0.04; p<0.001]);
- ASC with β-adrenergic blockers (74.48% [95% CI 74.48 ± 0.04; p<0.001]);
- ASC with angiotensin-converting enzyme inhibitors (ACEIs) (44.83% [95% CI 44.83 ± 0.04; p<0.001]);
- ASC with renin-angiotensin-2 blockers (ARBs) (18.62% [95% CI 18.62 ± 0.03; p<0.001]);
- ASC with β-adrenergic blockers and ACE inhibitors (42.07% [95% CI 42.07 ± 0.04; p<0.001]);
- ASC with β-adrenergic blockers and ARBs (15.17% [95% CI 15.17 ± 0.03; p<0.001]);
- ASC with β-adrenergic blockers and sacubiril/valsartan (2.76% [95% CI 2.76 ± 0.01; p<0.001]) (Figure 8).
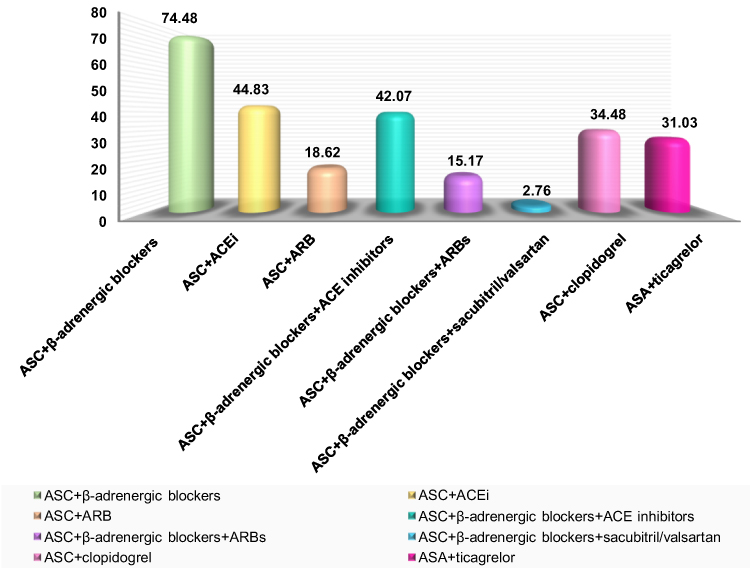 |
Figure 8 The frequency of use of common drug combinations within treatment regimens that exert toxic effects on the human body remains high, particularly among patients with CHD with comorbid conditions (%). Abbreviations: ASC, acetylsalicylic acid; ACE inhibitors, angiotensin-converting enzyme inhibitors; ARBs, renin-angiotensin-2 blockers. |
The observed association between the increasing number of concomitant medications and the increasing number of pDDIs is logically consistent with established principles of clinical pharmacology. The use of pharmacodynamic synergism in routine clinical practice potentially can enhance the therapeutic efficacy of treatment, particularly through the use of fixed-dose drug combinations provided the dose of the drug is correctly selected. However, this must be balanced against the increased risk of ADRs, such as bleeding, orthostatic hypotension, and electrolyte imbalances, which may arise from amplified pharmacodynamic effects. In contrast, pharmacodynamic antagonism, which weakens the overall therapeutic effect, may contribute to a loss of disease control and therapeutic failure, particularly in patients with CHD with chronic conditions. Among the most serious concerns is the toxic effect of drugs resulting from clinically significant interactions, especially under conditions of unacceptable polypharmacy. These effects may be particularly detrimental in patients with CHD with comorbidities, where the simultaneous use of multiple drugs is common. The findings of this study highlight the critical importance of conducting systematic drug monitoring and evaluating the pDDIs in clinical practice. This is essential for ensuring patient safety, optimizing therapeutic outcomes, and preventing ADR events associated with complex pharmacotherapy.
To obtain prediction results using ordinal logistic regression for the dependent variable “Adherence to treatment” (coded as: 1 – high adherence, 2 – partial adherence, 3 – low adherence), an analysis was performed using a model with an ordinal multinomial distribution and a logit link function. The parameter estimates derived from the constructed model are presented in Table 2.
 |
Table 2 Parameter Estimates From Ordinal Logistic Regression Using an Ordinal Multinomial Model: Analysis of the Relationship with Treatment Adherence |
Intercept 1 and Intercept 2 are threshold (cut-off) constants in the ordinal logistic regression model, representing the transition points between categories of adherence to treatment on the latent (underlying) scale when all independent variables are equal to zero. These parameters are technical components of the model and are not typically interpreted in terms of the influence of specific predictor variables.
When assessing the influence coefficient of “pharmacodynamic antagonism” (Estimate = 0.55312; p < 0.000001), a positive coefficient value and high statistical significance are observed (Table 2). These results indicate that pharmacodynamic antagonism is a significant predictor in the model of treatment adherence. Specifically, an increase of one unit in pharmacodynamic antagonism is associated with an increase in the log-odds of transitioning to a higher category of the dependent variable, “Adherence to treatment”, which corresponds to lower adherence to pharmacotherapy. The odds ratio (OR), calculated as OR = exp (0.55312) ≈ 1.739, suggests that each unit increase in the level of pharmacodynamic antagonism increases the patient’s odds of non-adherence to treatment by approximately 1.74 times, assuming the effects of other variables in the model remain constant. Similarly, for the coefficient estimating the impact of the “Toxic effect of drugs” (Estimate = 0.31126; p = 0.000187), both the positive coefficient value (0.31126) and high statistical significance (p < 0.001) confirm that this factor is also reliably associated with lower adherence. An increase in the level of toxic effects by one unit results in a corresponding increase in the log-odds of transitioning to a higher category of the outcome variable, indicating reduced adherence to the pharmacotherapy of CHD with comorbid conditions.
The Odds Ratio (OR), calculated as OR = exp (0.31126) ≈ 1.365, indicates that a one-unit increase in the toxic effects resulting from pDDIs is associated with a 1.36-fold increase in the likelihood of low adherence to treatment, assuming all other variables in the model remain constant.
The coefficients for “pharmacodynamic antagonism” and “drug toxicity” in this study are statistically highly significant factors that negatively affect treatment adherence. In particular, increases in these indicators are associated with a greater likelihood of treatment discontinuation, which is clinically justified. In cases where a patient is aware of their high or very high cardiovascular risk and simultaneously experiences insufficient treatment efficacy (due to pharmacodynamic antagonism) or ADR (due to drug toxicity pDDIs), a natural and expected reaction is a decline in adherence to pharmacotherapy.
Thus, the results clearly demonstrate an interrelationship between pharmacological factors and adherence to treatment. Pharmacodynamic antagonism can reduce the clinical effectiveness of pharmacotherapy, while toxic pDDIs may contribute to delayed ADR. Both factors are key determinants of reduced adherence to treatment in patients with CHD with comorbid conditions. The increased likelihood of pharmacodynamic antagonism or toxic effects due to pDDI indirectly reduced patients’ willingness to adherence to medication and treatment regimens. These findings are both expected and clinically grounded.
Discussion
In our study, a significant difference in the distribution of “Number of medications taken” between different categories of “Adherence to treatment” was confirmed (p = 0.001). At the same time, the number of medications taken (or pDDIs) depended on patients’ adherence to treatment and differed in subgroups of patients by categories of adherence to treatment. These findings are supported by numerous clinical studies, which form the basis of clinical practice guidelines3–6, and which recommend the use of fixed-dose drug combinations to enhance adherence to the pharmacotherapy of CHD in patients with comorbid conditions. In addition, the use of polypills (fixed-dose combinations, FDCs) and their effect on improving treatment adherence – by a factor of 1.29 (1.29 [95% CI: 1.29 ± 0.06]; p < 0.00001) – is also of significant importance, as confirmed by data from a systematic review and meta-analysis.32 It is important to note that fixed-dose combinations are designed with consideration for the safe co-administration of multiple active agents whose combined action results in pharmacodynamic synergism.32 The results of our analysis, demonstrating a strong positive monotonic relationship between “Total pDDIs” and “Pharmacodynamic synergism” (Spearman’s coefficient rs = 0.737630), further support this approach33 This statistically significant association confirms a consistent trend: as the total number of drug interactions increases, so does the likelihood of pharmacodynamic synergism, which contributes to enhanced pharmacotherapeutic efficacy of the prescribed treatment regimens. However, while the use of fixed-dose combinations and polypills can improve treatment adherence, it may also limit the ability to implement individualized approaches to pharmacotherapy, particularly those based on optimized and personalized treatment selection. In addition, they can lead to phenomena such as orthostatic hypotension or bleeding.28,29
It is known that the combination of ACE inhibitors, ARBs, and β-adrenergic blockers, sacubitril/valsartan with ASC (a nonsteroidal anti-inflammatory drug, NSAID), even in low doses, may lead to toxic effects primarily due to reduced renal function and suppressed prostaglandin synthesis.28,29,34 Moreover, the concomitant use of these pharmacological groups can result in both pharmacodynamic synergism (eg, enhanced antihypertensive or cardioprotective effects) and pharmacodynamic antagonism (eg, reduced efficacy or increased risk of adverse effects). These drug combinations are commonly included in treatment regimens for patients with CHD with comorbid conditions, including CKD, hypertension, and T2DM. The frequency and potential risks associated with these combinations are illustrated in Figure 8. At the same time, the combination of clopidogrel with ACE inhibitors, ARBs, β-adrenergic blockers, and sacubitril/valsartan is safe to use.28,29
Of particular note is the use of dual antiplatelet therapy (DAPT) in our cohort, observed in 65.51% of patients (95% CI: 65.51 ± 0.04; p < 0.001). As highlighted in a systematic review of 58 clinical trials, patients with high and very high cardiovascular risk in outpatient settings commonly receive, in addition to DAPT, statin therapy of varying intensity, ACE inhibitors, ARBs, sacubitril/valsartan, and other pharmacological agents13 – a pattern that is consistent with findings from our study. According to the literature, the combination of these medications significantly increases the risk of ADRs, due to potential alterations in drug metabolism and reduced platelet inhibition efficacy, particularly, when antiplatelet agents are combined with calcium channel blockers (8.97% [95% CI: 8.97 ± 0.02; p < 0.001] in our cohort) or statins (59.31% [95% CI: 59.31 ± 0.04; p < 0.001]).13 These drug interactions necessitate regular monitoring of liver, kidneys function and clinical risks of bleeding to ensure a comprehensive evaluation of CHD with comorbid conditions.13 Furthermore, the widespread combination of ACE inhibitors, ARBs, or sacubitril/valsartan with acetylsalicylic acid, a mainstay in modern DAPT regimens following index cardiovascular events and second prevention, significantly increases the risk of toxic effects on renal function.28,29,34
It is important to emphasize that the combination of renin-angiotensin-aldosterone system (RAAS) blockers with other medications commonly used in the treatment of cardiovascular diseases may result in dyskalemia, or angioedema,35 primarily due to pharmacodynamic antagonism. In our study, 340 pDDIs were identified that potentially affected plasma potassium levels (both elevations and reductions), which could have contributed to a decrease in treatment adherence. However, we did not assess the clinical outcomes associated with these specific pDDIs, as electrolyte monitoring was not routinely performed in the patient cohort during the observation period.
In addition, we have observed dangerous combinations of amiodarone with clopidogrel, which can lead to the formation of the active metabolite of clopidogrel;36 with direct oral anticoagulants, which can increase the concentration of the latter and lead to bleeding, especially in the case of the use of dabigatran (12–60%) or edoxaban (40%);36 statins, which can lead to myopathies.36
Our findings regarding the negative impact of pharmacodynamic antagonism, which reduces the probability of treatment adherence by approximately 1.74 times in patients with CHD with comorbidities (OR = exp (0.55312) ≈ 1.739), underscore the critical importance of routine pharmacotherapy reviews to ensure the safe use of medications. These findings further support the integration of pharmacists and clinical pharmacists into multidisciplinary healthcare teams. Additionally, the observed negative toxic effect of drug interactions, which decreases treatment adherence by 1.36 times (OR = exp(0.31126) ≈ 1.365), highlights the need for proactive risk assessment of pDDIs based on the pharmacological profiles of prescribed medications. This is particularly relevant given the high prevalence of unacceptable polypharmacy (95.86% in our study), where pDDIs are not adequately considered. Our previous study37 demonstrated that the overall medication burden, measured by the number of pills taken, significantly affects treatment adherence (U = 4.895; Z-score = −2.793 (unadjusted), −2.844 (adjusted); p = 0.0052 and 0.0045, respectively). These findings advocate for the wider use of fixed-dose combinations and the incorporation of deprescription practices during clinical decision-making, facilitated through collaboration between physicians and pharmacists/clinical pharmacists. An illustrative example is the irrational use of hypoglycemic therapy observed in our cohort, where 2.76% of patients with CHD and T2DM received a simultaneous combination of biguanides, sulfonylureas, and SGLT2 inhibitors, contradicting the ESC clinical recommendations.6,7 Such cases further justify the need for systematic monitoring of pharmacotherapy for CHD with comorbid conditions to ensure appropriate prescribing practices and optimized therapeutic dosing. Furthermore, our results align with the recommendations of the ESC Heart Failure Association’s Clinical Consensus Statement,13 and are supported by clinical trials demonstrating the positive impact of pharmacist or clinical pharmacist interventions on adherence to treatment and the quality of life in patients with CHF.38
The results of ordinal logistic regression analysis revealed a significant association between pharmacodynamic antagonism (OR ≈ 1.74) and toxic effects resulting from drug interactions (OR ≈ 1.36) with an increased risk of low treatment adherence in patients with CHD with comorbid conditions. It is important to highlight that treatment adherence assessment was performed post hoc, ie, after completion of the prescribed pharmacotherapy. This methodological approach allows for more reliable assumptions regarding the directionality of influence. It should be emphasized that adherence to treatment was assessed after the prescription of pharmacotherapy for CHD with comorbid conditions. This approach allows us to infer the direction of influence and account for factors such as forgetfulness, patients’ educational level, and emotional state during their involvement in the treatment process, which were previously examined in our earlier research. Thus, the present findings are not only statistically robust but also theoretically substantiated, providing compelling evidence for the impact of pharmacological interactions on reducing adherence to pharmacotherapy in patients with CHD and comorbidities. These results underscore the critical importance of individualized pharmacotherapy planning and the integration of clinical pharmacists in managing complex treatment regimens to enhance therapeutic adherence and patient outcomes.
Given the growing body of scientific evidence demonstrating the impact of pharmacodynamic antagonism,37,39,40 synergism,35 and toxicity due to pDDIs40,41 on final clinical outcomes in patients with CHD with comorbid conditions, we believe that further investigation of these ADR is warranted as they represent important determinants of treatment adherence. The results of our study highlight the necessity of systematically addressing issues related to unacceptable polypharmacy, the medication burden measured by the number of prescribed tablets, and the development of evidence-based strategies and models to improve treatment adherence.
In this study, we did not observe the effect of pDDI on the deterioration of the patients’ condition, as they were in the inpatient ward and did not have any complaints or clinical signs. However, the effect of pDDI may have a delayed effect, exacerbated by the complexity of treatment regimens and polypharmacy, taking into account the use of drugs at therapeutic doses that are safe to use. Scientific evidence emphasizes the need for continuous monitoring of such patients in the inpatient and outpatient settings.42 The likelihood of developing delayed DDI effects increases not only with complex pharmacotherapy regimens, but also in the presence of comorbidities and in old age. Clinically, such observations may manifest as a gradual decrease in the effectiveness of pharmacotherapy, the appearance of cardiac arrhythmias, and deterioration of renal or hepatic function.42,43
Important directions of our study include the use of real-world clinical data, the application of standardized and validated pDDI sources (Drugs.com, Medscape), and the deployment of ordinal logistic regression, which allowed for a comprehensive analysis of the combined impact of multiple pharmacological factors on treatment adherence. Additionally, the study was based on a representative patient sample with a typical comorbid profile, enhancing the external validity and generalizability of the findings. The insights obtained from this analysis have direct applicability in clinical practice, offering a foundation for the optimization of pharmacotherapy in CHD with comorbid conditions and for targeted interventions aimed at enhancing medication adherence. These results support a paradigm shift toward more personalized and pharmacologically sound therapeutic strategies, with active involvement of clinical pharmacists as part of multidisciplinary care teams.
This study has certain limitations that should be acknowledged. One notable limitation is the absence of laboratory assessment of electrolyte disturbances, particularly plasma potassium levels, which could have provided a more comprehensive understanding of the toxic effects of pharmacotherapy due to pDDIs. Additionally, we did not include an evaluation of psychosocial factors, such as educational attainment, psychological stress, anxiety, depression, patient-physician trust, and patients’ attitudes toward generic versus innovative medications. However, these psychosocial dimensions have been previously explored in our earlier research, as reflected in prior scientific publications, thereby partially mitigating this limitation in the present study. Another important consideration is the potential for reverse causality: patients with low adherence to treatment may have self-excluded from taking certain pharmacological classes (eg, DAPT, direct oral anticoagulants, glucagon-like peptide-1 receptor agonists). This non-adherence may have artificially lowered the total number of observed pDDIs, thus potentially underestimating the true scope of pharmacological risk in these individuals. Despite these limitations, the study provides a robust analysis of the influence of pharmacodynamic drug interactions on treatment adherence in patients with CHD with comorbid conditions, laying the groundwork for further investigations that integrate biochemical monitoring and psychosocial profiling. This study was conducted over a relatively short period in conditions of military conflict, which limits the ability to further assess changes in treatment adherence over time in relation to pharmacotherapy adjustments for CHD with comorbid conditions.
The findings emphasize the critical role of involving clinical pharmacists/pharmacists in multidisciplinary care teams to enhance treatment efficacy and reduce the incidence of pDDIs when prescribing therapy components in accordance with current clinical guidelines. In the absence of a clinical pharmacists/pharmacists, it is recommended that physicians utilize standardized resources – such as Drugs.com or Medscape – to assess the pharmacodynamic properties (synergism, antagonism, toxicity) of prescribed pharmacotherapy to ensure both its effectiveness and safety.
Conclusions
- An assessment of the impact of pharmacological interaction types revealed that, in the studied population of patients with CHD with comorbid conditions, unacceptable polypharmacy was present in 95.86% of prescriptions (95% CI: 95.86 ± 0.02; p < 0.001). This level of polypharmacy may be associated with clinically significant pDDIs.
- It was established that the total number of pDDIs per prescription is statistically significantly correlated with the types of pharmacodynamic synergism (rs = 0.737), antagonism (rs = 0.659), and toxic effects (rs = 0.554).
- A statistically significant association was identified between the presence of pharmacodynamic antagonism (OR ~ 1.74) and toxic effects due to drug interactions (OR ~ 1.36) and an increased likelihood of low treatment adherence. These findings highlight the clinical relevance of these factors in influencing treatment response in patients with CHD with comorbid conditions when guidelines pharmacotherapy is prescribed.
- The study found that an increase in the number of pDDIs is associated with changes in the pharmacodynamic profile of prescribed combinations of drugs from different pharmacological classes. These changes may potentially reduce the effectiveness or safety of treatment and, consequently, lead to lower patient adherence to pharmacotherapy in individuals with CHD with comorbid conditions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yurochko T, Skipalsky A, Kurylo I, Dumcheva A. Improving indicators of non-communicable diseases: barriers and opportunities of the healthcare system in Ukraine. Ukrainian-Swiss project “Act for Health”; January 2023. Reducing the prevalence of risk factors for non-communicable diseases in Ukraine. Available from: https://idss.org.ua/arhiv/Аналитичный%20звыт%20з%20НИЗ-web_Kurylo.pdf.
2. Corica B, Romiti GF, Boriani G, et al. Patterns of pharmacological treatment in patients with atrial fibrillation: an analysis from the prospective GLORIA-AF Registry Phase III. BMC Med. 2025;23(1). doi:10.1186/s12916-025-03858-w
3. Vrints C, Andreotti F, Koskinas KC, et al. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024;45:3415–3537. doi:10.1093/eurheartj/ehae177
4. McEvoy JW, McCarthy CP, Bruno RM, et al. 2024 ESC Guidelines for the management of elevated blood pressure and hypertension. Eur Heart J. 2024. doi:10.1093/eurheartj/ehae178
5. Mach F, Baigent C, Catapano AL, et al. 2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. 2019;41(1):111–188. doi:10.1093/eurheartj/ehz455
6. McDonagh TA, Metra M, Adamo M, et al. 2023 focused update of the 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2023;44:3627–3639. doi:10.1093/eurheartj/ehad195
7. American Diabetes Association Professional Practice Committee; 10. Cardiovascular disease and risk management: standards of medical care in diabetes—2022. Diabetes Care. 2021;45(Supplement_1):S144–S174. doi:10.2337/dc22-s010
8. Stevens PE, Ahmed SB, Carrero JJ, et al. KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int. 2024;105(4):S117–S314. doi:10.1016/j.kint.2023.10.018
9. Bilousova NA, Dolzhenko MM. An analysis of prescriptions for coronary heart disease with comorbid conditions in health care institutions of Ukraine. Curr Issues Pharm Med Sci Pract. 2025;18(1):45–56. doi:10.14739/2409-2932.2025.1.320493
10. Sheikh-Taha M, Asmar M. Polypharmacy and severe potential drug-drug interactions among older adults with cardiovascular disease in the United States. BMC Geriatr. 2021;21(1). doi:10.1186/s12877-021-02183-0
11. Osanlou R, Walker L, Hughes DA, Burnside G, Pirmohamed M. Adverse drug reactions, multimorbidity and polypharmacy: a prospective analysis of 1 month of medical admissions. BMJ Open. 2022;12(7):e055551. doi:10.1136/bmjopen-2021-055551
12. Stolfo D, Iacoviello M, Chioncel O, et al. How to handle polypharmacy in heart failure. A clinical consensus statement of the Heart Failure Association of the ESC. Eur J Heart Fail. 2025;27:747–759. doi:10.1002/ejhf.3642
13. Huang X, Song J, Zhang X, et al. Understanding drug interactions in antiplatelet therapy for atherosclerotic vascular disease: a systematic review. CNS Neurosci Amp Ther. 2025;31(2). doi:10.1111/cns.70258
14. Dolzhenko MM, Bilousova NA, Mykhalchuk VM, Tkachenko NO, Luchinskaya YO. Study of the influence of medication properties and lifestyle of patients with ischemic heart disease on adherence to treatment. Wiadomosci Lekarskie. 2025;860–875. doi:10.36740/WLek/203897
15. Ford N, Mills EJ, Zachariah R, Upshur R. Ethics of conducting research in conflict settings. Confl Health. 2009;3(1). doi:10.1186/1752-1505-3-7
16. Etikan I. Comparison of convenience sampling and purposive sampling. Am J Theor Appl Stat. 2016;5(1):1. doi:10.11648/j.ajtas.20160501.11
17. Conover WJ. Practical Nonparametric Statistics.
18. StatPlus help - compare multiple independent samples [Kruskal-Wallis, Median Test]. Analysis Made Easy | analystSoft | statPlus:Mac | statPlus | bioStat | statFi. Available from: https://www.analystsoft.com/en/products/statplus/content/help/analysis_nonparametric_statistics_comparing_multiple_independent_samples_kruskal-wallis_anova_median_test.html.
19. Bhusal L, Deep Pathak B, Dhakal B, et al. Determination of level of self‐reported adherence of antihypertensive drug(s) and its associated factors among patient with hypertension at a tertiary care center. J Clin Hypertens. 2022;24:1444–1450. doi:10.1111/jch.14592
20. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosomatic Res. 1999;47(6):555–567. doi:10.1016/s0022-3999(99)00057-4
21. Chan HY, Horne R, Hankins M, et al. The medication adherence report scale: a measurement tool for eliciting patients’ reports of nonadherence/A. Br J Clin Pharmacol. 2020;86(7):1281–1288. doi:10.1111/bcp.14193
22. Spetz K, Olbers T, Östbring M, Moon Z, Horne R, Andersson E. Using the 5-item Medication Adherence Report Scale (Mars-5) to screen for non-adherence to vitamin and mineral supplementation after bariatric surgery. Obes Surg. 2024;34:576–582. doi:10.1007/s11695-023-07027-x
23. Bacquer, Dirk Deet al.for the EUROASPIRE IV and V surveys of the European Observational Research Programme of the European Society of Cardiology OUP accepted manuscript. Eur J Prev Cardiol. 2021. doi:10.1093/eurjpc/zwab115
24. McEvoy JW, Jennings C, Kotseva K, et al. INTERASPIRE: an International Survey of Coronary Patients; Their cardiometabolic, renal and biomarker status; and the quality of preventive care delivered in all WHO Regions. Curr Cardiol Rep. 2021;23(10). doi:10.1007/s11886-021-01568-2
25. Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new Medication Adherence Rating Scale (Mars) for the psychoses. Schizophr Res. 2000;42(3):241–247. doi:10.1016/s0920-9964(99)00130-9
26. Syafhan NF, Donnelly R. Harper R та ін. Adherence to metformin in adults with type 2 diabetes: a combined method approach. J Pharm Pract. 2022;15(1). doi:10.1186/s40545-022-00457-5
27. Assiri G, Alabdulkarim D, Alanazi A, Altamimi S, Alanazi NL, Khawagi W. Description of patient characteristics and medication adherence among medication access mobile application users and nonusers: a single-center questionnaire-based cross-sectional study. BMC Digit Health. 2023;1(1). doi:10.1186/s44247-023-00039-8
28. Drug Interaction Checker - find unsafe combinations. Drugs.com [homepage on the Internet]. Available from: https://www.drugs.com.
29. Medscape Interaction Checker - find unsafe combinations. Medscape.com. [homepage on the Internet]. Available from: https://reference.medscape.com/drug-interactionchecker.
30. State Register of Medicinal Products of Ukraine. [homepage on the Internet]. Available from: http://www.drlz.com.ua/ibp/ddsite.nsf/all/shlist?opendocument.
31. Liu W, Bretz F, Cortina-Borja M. Reference range: which statistical intervals to use? Stat Methods Med Res. 2020;096228022096179. doi:10.1177/0962280220961793
32. Wei Q, Zhou J, Li H, et al. Medication adherence with fixed-dose versus free-equivalent combination therapies: systematic review and meta-analysis. Front Pharmacol. 2023:14. doi:10.3389/fphar.2023.1156081
33. Paczkowska-Walendowska M, Sip S, Staszewski R, Cielecka-Piontek J. Single-pill combination to improve hypertension treatment: pharmaceutical industry development. Int J Environ Res Health. 2022;19(7):4156. doi:10.3390/ijerph19074156
34. Caiati C, Arrigoni R, Stanca A, Lepera ME. Kidney toxicity of drugs for the heart: an updated perspective. Metabolites. 2025;15(3):191. doi:10.3390/metabo15030191
35. Mohamed Pakkir Maideen N, Balasubramanian R, Muthusamy S, Nallasamy V. An overview of clinically imperative and pharmacodynamically significant drug interactions of renin-angiotensin-aldosterone system (RAAS) blockers. Curr Cardiol Rev. 2022;18:18. doi:10.2174/1573403x18666220511152330
36. Merino JL, Tamargo J, Blomström-Lundqvist C, et al. Practical compendium of antiarrhythmic drugs: a clinical consensus statement of the European Heart Rhythm Association of the ESC. Europace. 2025. doi:10.1093/europace/euaf076
37. Dolzhenko MM, Bilousova NA, Yakovenko LI, Nesukai VA, Kozhuharyova NA. The impact of polypharmacy on adherence to pharmacotherapy for coronary heart disease with comorbid conditions: insights from the EUROASPIRE V observational study in Ukraine. Modern Med Technol. 2025;17(2):91–101. doi:10.14739/mmt.2025.2.322403
38. Schulz M, Griese‐Mammen N, Schumacher PM, et al. The impact of pharmacist/physician care on quality of life in elderly heart failure patients: results of the PHARM‐CHF randomized controlled trial. ESC Heart Fail. 2020;7(6):3310–3319. doi:10.1002/ehf2.12904
39. Lewis BS. Cardiovascular disease and cardiovascular pharmacotherapy: the challenges and the research continue. Eur J Cardiovasc Pharmacother. 2025;11:1–2. doi:10.1093/ehjcvp/pvae099
40. Su M, Qin XS, Li Y, et al. Association between medication adherence and cardiovascular outcomes in patients with both diabetes and hypertension in primary care settings in Canada: a retrospective cohort study. PLoS One. 2025;20(4):e0319991. doi:10.1371/journal.pone.0319991
41. Rodríguez-Bernal CL, Sánchez-Saez F, Bejarano-Quisoboni D, et al. Assessing concurrent adherence to combined essential medication and clinical outcomes in patients with acute coronary syndrome. a population-based, real-world study using group-based trajectory models. Front Cardiovasc Med. 2022:9. doi:10.3389/fcvm.2022.863876
42. Poulsen MH, Krogh ML. Major drug interactions. In: Andersen LV, Poulsen BK, editors. The ESC Handbook on Cardiovascular Pharmacotherapy. Oxford University Press; 2019:387–410. doi:10.1093/med/9780198759935.003.0023_update_001
43. Hughes JE, Moriarty F, Bennett KE, Cahir C. Drug‐drug interactions and the risk of adverse drug reaction‐related hospital admissions in the older population. Br J Clin Pharmacol. 2023;90:959–975. doi:10.1111/bcp.15970
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence of Multiple Chronic Conditions in Older Adults with Undiagnosed Mild Cognitive Impairment and Alzheimer’s Disease and Related Dementias in Primary Care
Summanwar D, Owora AH, Ben Miled Z, Dexter PR, Kulshreshtha A, Strunk S, Jiang B, Coppedge K, Disla S, Galvin JE, Boustani M, Fowler NR
Clinical Interventions in Aging 2025, 20:1799-1809
Published Date: 24 October 2025
Implementation and Evaluation of a Real-Time Prescription Alert System to Optimize Antiretroviral Therapy and Medication Adherence in People Living with HIV. SANPAT PROJECT
Morillo-Verdugo R, Solis-Martin C, Marquez-Saavedra E, Robustillo-Cortes MDLA, Romero Gil E, Contreras-Macias E
Patient Preference and Adherence 2025, 19:3493-3508
Published Date: 7 November 2025
Impact of a CMO-Based Pharmaceutical Care Model on 3-HIT Criteria in Older People Living with HIV: The DIS3HIT Project
Roldán Galnares M, Morillo-Verdugo R, Robustillo-Cortes MDLA, Vélez-Díaz-Pallarés M, Company Albir MJ, Proy Vega B, Losa López L, Marín Ventura L, Ferris Villanueva M, Mora Atorrasagasti O, Gutiérrez E
Patient Preference and Adherence 2026, 20:569460
Published Date: 30 January 2026