Back to Journals » Psychology Research and Behavior Management » Volume 18
Influence of Inter-Parental Conflict on New-Onset Major Depressive Disorder in Chinese College Students
Authors Gao Y, Fang Q, Zhou Y, Si J, Liu M, Liu Y, Liu C, Li N, Zhai J, Yu H, Yang J
Received 18 September 2025
Accepted for publication 18 December 2025
Published 28 December 2025 Volume 2025:18 Pages 2451—2468
DOI https://doi.org/10.2147/PRBM.S559685
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Yan Gao,1,2,* Qing Fang,1,* Yanan Zhou,3 Jijian Si,1 Min Liu,4 Yan Liu,5 Chuanxin Liu,2 Na Li,2 Jinguo Zhai,2 Hao Yu,2 Jianli Yang1
1Department of Clinical Psychology,Tianjin Medical University General Hospital, Tianjin, 300052,People’s Republic of China; 2School of Mental Health, Jining Medical University, Jining, 272067, People’s Republic of China; 3Psychiatry department, Shandong Daizhuang Hospital, Jining, 272051, People’s Republic of China; 4School of Public Health, Peking University, Beijing, 100871, People’s Republic of China; 5School of Public Health, Jining Medical University, Jining, 272067, People’s Republic of China
*These authors contributed equally
Correspondence: Jianli Yang, Department of Clinical Psychology, Tianjin Medical University General Hospital, Tianjin, 300052, People’s Republic of China, Email [email protected]
Objective: Major depressive disorder (MDD) significantly impairs college students’ functioning. Inter-parental conflict (IPC) is a recognized risk factor for mental health issues, yet gender-specific mechanisms linking IPC to MDD in college students remain unclear. This study aimed to examine the association between IPC and new-onset MDD among Chinese university students, and to test whether this association differs by gender.
Methods: A retrospective controlled study was conducted between April 2018 and October 2019 among 8079 first-year students from two medical universities in Shandong Province, China, using cluster sampling.The Adolescent Self-rating Life Events Check List (ASLEC) assessed stressful life events, the lifetime severe traumatic events questionnaire evaluated traumatic experiences, the Egna Minnen Beträffande Uppfostran (EMBU) measured parenting styles, and the Composite International Diagnostic Interview (CIDI-3.0) diagnosed MDD based on DSM-IV criteria. With descriptive statistics computed by gender and logistic regression models employed to assess IPC’s impact on MDD risk.
Results: The overall incidence of new-onset MDD was 2.4% (2.1% in males, 2.6% in females). Multivariate analysis revealed that occasional physical violence (OR=2.114, 95% CI:1.059– 4.222) and chronic emotional neglect (OR=2.252, 95% CI:1.074– 4.724) during IPC significantly increased MDD risk in male students. Among female students, seeking help from relatives during parental conflicts was independently associated with increased MDD risk (OR=2.14, 95% CI:1.09– 4.20).
Conclusion: IPC is significantly associated with new-onset MDD among Chinese college students, and this relationship is moderated by gender. While male students show vulnerability to physical conflict and emotional neglect, female students face increased risk when involving relatives in conflict resolution. The findings support the development of gender-specific intervention strategies to mitigate familial risk and promote student mental health.
Keywords: major depressive disorder, family dynamics, risk factors, gender stratification
Introduction
Major depressive disorder (MDD), characterized by persistent low mood and anhedonia, constitutes a severe global public health challenge.1 It is estimated to affect approximately 280 million individuals worldwide and remains a leading cause of disability, imposing a substantial burden on healthcare and society through impaired functioning and reduced productivity.2 This burden is particularly acute among college students, a population in the critical developmental stage of emerging adulthood. Notably, a recent study found that up to two-thirds of college students with MDD experience suicidal ideation, severely threatening their psychosocial development and academic trajectory.3
The etiology of MDD is recognized as multi-factorial, involving genetic vulnerabilities, environmental stressors such as childhood trauma and acute stressful life events,4,5 and potent family-level influences. Among family factors, parenting styles have been consistently implicated. Notably, a recent large longitudinal study on Chinese freshmen confirmed that perceived maternal over-protection and parental disharmony are significant risk factors for the new-onset of MDD,6 highlighting the enduring impact of family dynamics on depression risk in this specific population.
Gender is a well-established moderator in depression epidemiology, with females consistently demonstrating a higher prevalence of MDD than males,7,8 and his disparity extends to the population of college students.9 Furthermore, gender disparities in depression may be mediated or compounded by several interlinked factors.These include a higher prevalence of adverse childhood experiences (ACEs) as well as anxiety and depressive disorders during developmental periods among females, gendered sociocultural roles that shape the exposure and response to stressors, and psychological traits related to differential vulnerability and coping efficacy.10 Importantly, gender differences extend beyond prevalence to the phenotypic expression of MDD, encompassing variations in the typical age of onset and the prominence of specific symptom clusters.11 This study employs a gender-stratified analytical approach to specifically investigate potential differences in how inter-parental conflict (IPC) influences the risk of new-onset MDD among Chinese college students.
Inter-parental conflict (IPC) refers to arguments or disputes between parents that may arise due to disagreements on some daily issues, emotional conflicts, or issues related to child rearing,12,13 represents a chronic and potent family stressor. A comprehensive meta-analysis has conclusively established IPC as a robust risk factor for a range of child and adolescent maladjustments, including both externalizing behaviors and internalizing problems like depression and anxiety.14 Importantly, these detrimental effects can extend into early adulthood, impacting the mental health of college students.15–17 Beyond the mere occurrence of conflict, the methods by which families resolve conflicts also have some impact on children’s mental health. Studies have found that offspring who experience negative family conflict resolution styles are 1.8 times more likely to have depressive symptoms than those who experience positive family conflict resolution styles,18 indicating a need to examine both IPC manifestations and resolution methods.
Numerous studies focus on parenting styles’ impact on depression, research specifically examining IPC and its gender-specific effects on MDD among college students remains limited, particularly in the Chinese cultural context.Few have concurrently examined the distinct roles of IPC manifestations and resolution strategies. And crucially, whether the association between IPC and MDD differs by gender,which is an independent risk factor for MDD,19 has not been sufficiently tested using a stratified analytical approach.
This study employed a retrospective controlled design to examine the association between IPC and new-onset MDD among Chinese college students, with a specific focus on gender differences. We hypothesized that: (1) Exposure to IPC (including its specific manifestations and resolution methods) is positively associated with the incidence of new-onset MDD. (2) The magnitude and/or patterns of this association differ significantly between male and female students.
The elucidation of gender-specific risk pathways is expected to provide a refined theoretical basis for the etiology of MDD in young adults and offer critical, actionable insights for developing targeted prevention and intervention programs in both clinical and campus-based settings.
Methods
Research Design and Participants
This study utilized data from a large-scale, longitudinal mental health cohort of Chinese college freshmen. The design, sampling methods, and primary data collection procedures for this cohort have been described in detail previously.20,21 Briefly, the present analysis focused on a subset of participants from two medical universities in Shandong Province, China: Weifang Medical University (Weifang campus) and Jining Medical University (main campus in Jining and a satellite campus in Rizhao). The baseline survey was administered from April to October 2018, with a follow-up conducted among the same participants from April to October 2019. Inclusion criteria were: (1) first-year students; (2) informed consent was obtained and participation was voluntary; (3) under the age of eighteen, additional parental or guardian consent was acquired. Exclusion criteria included: (1) diagnosis of MDD at baseline; (2) history of MDD, mania or hypomania, schizophrenia, and severe physical diseases; (3) incomplete or invalid questionnaires.
The study specifically targeted first-year undergraduate students enrolled in diverse majors, including basic medical sciences, clinical medicine, public health and pharmacy. Approximately 60% of the student population at the two universities originated from Shandong Province, with the remainder representing more than 25 other provinces and regions across China. Participants’ family residences varied widely, encompassing rural counties, towns, and medium-to-large urban areas.The study protocol was approved by the Medical Ethics Committee of Jining Medical University.
Data Collection
Data collection for both baseline and follow-up surveys took place in campus libraries at all three sites using a cluster sampling approach. A total of 8,079 participants completed the baseline survey.A follow-up survey was conducted from April to October 2019, in which 7,550 university students who participated in the baseline survey agreed to participate in the follow-up, excluding invalid and missing data and samples with MDD at baseline. Finally, a total of 6136 valid questionnaires were collected.
Data were gathered via a computer-based self-administered system equipped with logical checks and skip patterns, installed on 365 computers across the campuses.Four trained staff members were assigned to answer various questions that the participants might mention.Upon completion, data were immediately uploaded to a central server at Jining Medical University. No financial compensation was provided to participants.
Measurements
Major Depressive Disorder (MDD)
The Comprehensive International Diagnostic Interview (CIDI-3.0) is one of the unique tools for the epidemiological investigation of mental disorders.22 Huang et al (2010) reported that the Chinese version of the CIDI-3.0 demonstrates good criterion validity and satisfactory test–retest reliability which aligns with Chinese cultural background and language habits. Specifically, for the diagnosis of major depressive disorder, this instrument showed a sensitivity of 71.1%, a specificity of 89.0%, and a test–retest reliability of 0.74.23 It can be used not only as a tool for epidemiological studies of mental disorders, can also be an auxiliary diagnostic tool in psychiatric outpatient clinics. Therefore, this study used CIDI-3.0, evaluated based on DSM-IV criteria, to diagnose newly diagnosed MDD in college students at baseline and follow-up surveys. Subjects diagnosed with MDD at baseline were excluded because this study aimed to explore factors affecting the incidence of MDD in college students over one year. A history of mania or hypomania was also excluded.
Adolescent Self Rating Life Events Check List (ASLEC)
Adolescent Self rating Life Events Check List (ASLEC) is a self-rating questionnaire compiled by Liu XC et al to evaluate the social pressure of adolescents based on reference to relevant domestic and foreign literature.24 It has 27 items, such as “ In the past year, have you been discriminated against”, “ In the past year, have you failed or were not ideal”, and “In the past year, have you had disputes with classmates or friends”, “ In the past year, have your living habits (eating, rest, etc.) changed significantly”, “In the past year, have you ever disliked to go to school”, etc. Each item is a life event, and the research subjects choose according to whether life events occur: (0) “No”, (1) “Yes”, if the event occurs, continue to select the degree of impact: (0) “No impact”, (1) “Mild impact”, (2) “Moderate impact”, (3) “Severe impact”, (4) “Extreme impact.” Each question was answered by participants, with higher scores indicating more significant stress in the subject’s life. The Cronbach’s α for the scale in this study was 0.888.
Lifetime Severe Traumatic Events
This study was measured using a self-developed lifetime severe traumatic events questionnaire, which included 23 items such as “In your life, have the following events occurred: The death of a grandparent”, “In your life, have the following events occurred: Death of father or mother”, “In your life, have the following events occurred: Death of sibling”, “In your life, have the following events occurred: Have had a serious illness”, “In your life, have the following events occurred: Natural disasters such as fires, floods, and earthquakes”, “etc. The subjects were selected according to whether life events occurred: (0) “no”, (1) “yes”, and the number of major traumatic events experienced was counted. The Cronbach’s α for the scale in this study was 0.680.
Egna Minnen Beträffande Uppfostran (EMBU)
Egna Minnen Betraffande Uppfostran (EMBU) is a questionnaire developed in 1980 by Perris et al to assess parents’ parenting style.25 It was revised by Yue Dongmei et al in 1993 and has been widely used in China.26 EMBU consists of two sub-scales, the paternal and maternal parenting style scales. The Parenting Style subscale includes 58 items in six dimensions. For example, “I think my father interferes in everything I do”, “I can feel my father likes me very much through his words and expressions”, “My father loves me more than my brothers and sisters”, “I can feel my father’s love for me”, etc. The maternal parenting style subscale includes 57 items in five dimensions. For example: “I think my mother interferes in everything I do”, “I can feel my mother likes me very much through her words and expressions”, “My mother loves me more than my brothers and sisters”, “I can feel my mother’s love for me”, etc. Each item was rated on a four-point scale: (1) “Never”, (2) “Occasionally”, (3) “Frequently”, and (4) “Always”, and each question required a response from the participant. The higher a parent’s overall score, the more they tended to favor this dimension of parenting style. The Cronbach’s α for the scale in this study was 0.941.
Family Factor Scale
The Family Factor Scale used in this study was a self-developed instrument designed to collect demographic and family-related information. It included items assessing parental age, occupation, manifestations of inter-parental conflict, and conflict-resolution methods, such as: “father’s age”, “mother’s age”, “How do your parents usually resolve their conflicts?” and “What do you usually do when your parents have conflicts?”This scale aimed to systematically capture objective family characteristics and behavioral patterns rather than measuring psychological constructs.
Statistical Methods
All statistical analyses were performed using SPSS 26.0. Due to the large sample size (baseline N=8,079), the assumptions of normality for parametric tests were considered met per the Central Limit Theorem, and formal normality tests were not conducted.27 Descriptive statistics were computed overall and by gender. Group differences were assessed using independent-sample t-tests and Chi-square test(χ2), with P<0.05 considered statistically significant. Binary logistic regression was employed to evaluate the impact of IPC manifestations and resolution methods on new-onset MDD risk, with results expressed as odds ratios (ORs) and 95% confidence intervals (CIs).
Results
Characteristics of Participants
A total of 6,136 valid cases were included in the final analysis, consisting of 2,394 (39.6%) males and 3,742 (60.4%) females. The overall incidence of new-onset MDD was 2.4% (148 cases), with gender-specific rates of 2.1% (51 cases) among males and 2.6% (97 cases) among females.
Demographic characteristics of the total sample and by gender are presented in Table 1. Among male participants, 1,553 (64.9%) were from Jining and 841 (35.1%) from Weifang; 999 (41.7%) reported urban residence and 1,395 (58.3%) rural residence. Within the female group, 2,261 (60.4%) originated from Jining and 1,481 (39.6%) from Weifang; 1,279 (34.2%) lived in urban and 2,463 (65.8%) in rural areas. Further details regarding participant characteristics, mental health indicators, interparental conflict forms, conflict resolution styles, and parenting dimensions are summarized in Table 1.
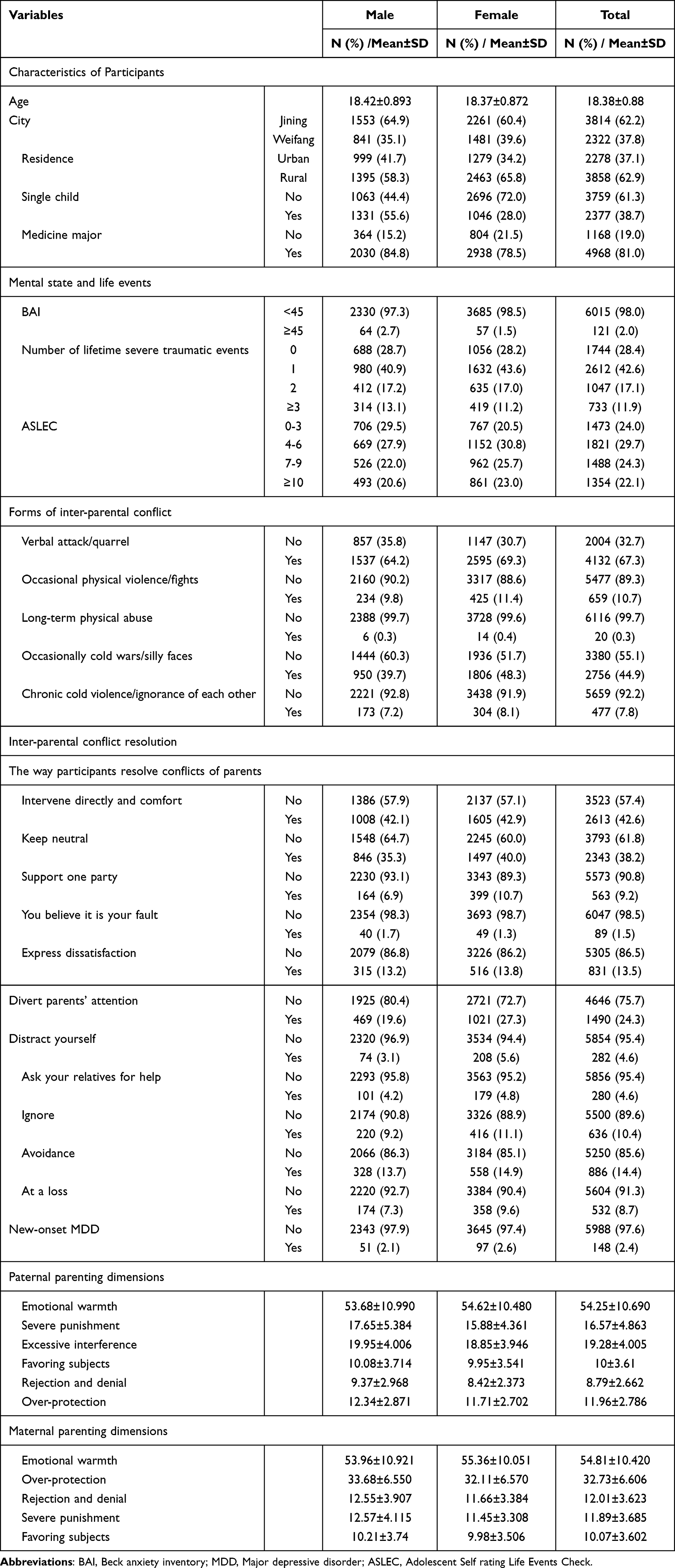 |
Table 1 Descriptive Statistics of Variables |
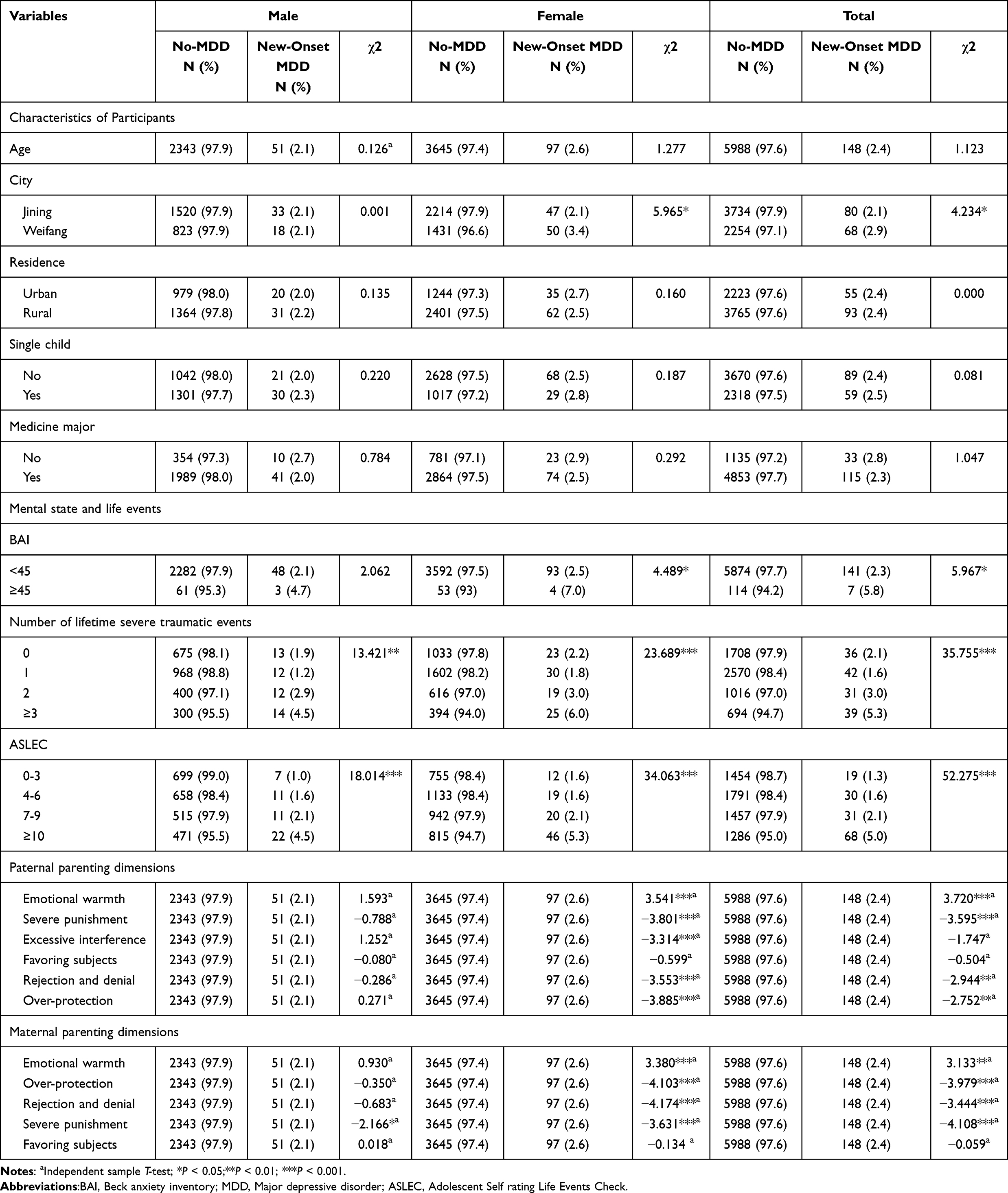 |
Table 2 Difference Analysis Between New-Onset MDD and Non-MDD |
Difference Analysis
To test for differences in control variables between the new-onset MDD and non-MDD populations, the Chi-square test and independent-sample t-test were used to analyze the differences (Table 2).
In the overall population, significant differences were observed in city of origin (χ2= 4.234, P<0.05), Beck Anxiety Inventory (BAI) scores (χ2=5.967, P<0.05), lifetime severe traumatic events (χ2=35.755, P<0.001), recent stressful life events (χ2=52.275, P<0.001), and multiple parenting dimensions,containing paternal emotional warmth (χ2=3.720; P < 0.05), paternal severe punishment (χ2=−3.595; P < 0.05), paternal rejection and denial (χ2=−2.944; P<0.05), paternal over-protection (χ2=−2.752; P<0.05), maternal emotional warmth (χ2=3.133; P<0.05), maternal over-protection (χ2=−3.979; P<0.05), maternal rejection and denial (χ2=−3.444; P < 0.05) and maternal severe punishment (χ2=−4.108; P<0.05) were statistical significance in the difference analysis between new-onset MDD and non-MDD.
In the male subgroup, only lifetime severe traumatic events (χ2=13.421, P<0.01), recent stressful life events (χ2=18.014,P<0.001), and maternal severe punishment (t= −2.166, P<0.05) were significantly associated with new-onset MDD.Compared with the whole group, there was no statistical significance in Paternal parenting dimensions and Maternal parenting dimensions (P>0.05).
In the female subgroup, significant differences were found in city (χ2=5.965, P <0.05), BAI scores (χ2=4.489,P<0.05), lifetime severe traumatic events (χ2= 23.689, P <0.001), recent stressful life events (χ2=34.063, P<0.001), and paternal and maternal parenting dimensions including paternal emotional warmth (χ2=3.541;P <0.05), paternal severe punishment (χ2=−3.801; P<0.05), paternal excessive interference (χ2=−3.314; P < 0.05), paternal rejection and denial (χ2=−3.553; P < 0.05), paternal over-protection (χ2=−3.885; P < 0.05), maternal emotional warmth (χ2=3.380; P<0.05), maternal over-protection (χ2=−4.103; P<0.05), maternal rejection and denial (χ2=−4.174; P<0.05) and maternal severe punishment (χ2=−3.631; P<0.05).There was statistical significance in the difference analysis between new MDD and non-MDD. Compared to the general population, the differences in the analysis of paternal over-interference in women were statistically significant.
Univariate Logistic Regression of Predictive Factors of New-Onset MDD
To further explore the specific associations between IPC manifestations, resolution methods, and new-onset MDD, univariate logistic regression analyses were conducted separately for male, female, and overall samples (Table 3).
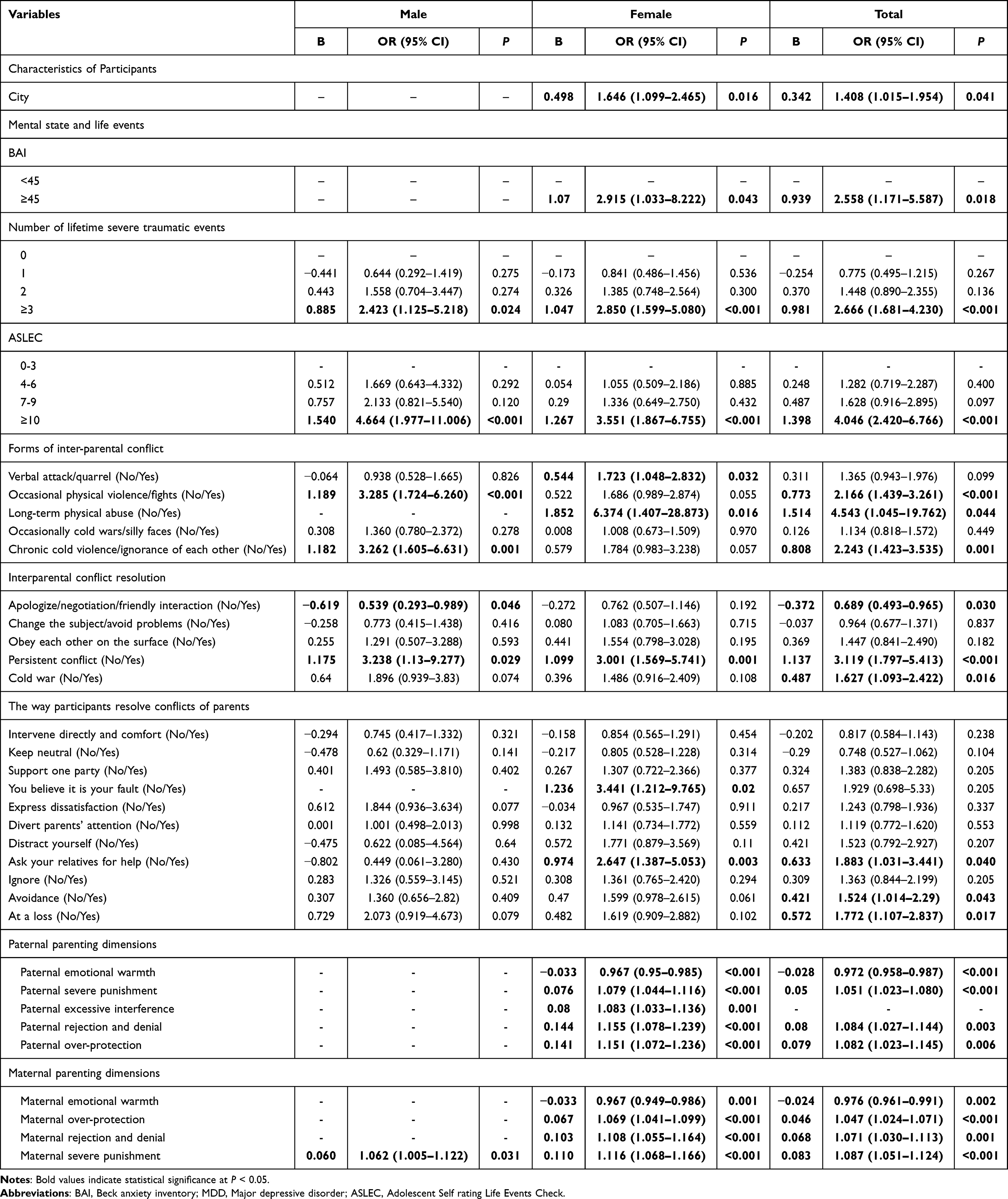 |
Table 3 Univariate Logistic Regression of Predictive Factors of New-Onset MDD |
In the overall sample, several IPC-related factors were significantly associated with new-onset MDD, including:occasional physical violence/fights (OR=2.166,95% CI: 1.439–3.261) and long-term physical abuse (OR=4.543,95% CI: 1.405–19.762) in IPC, persistent conflict (OR=3.119,95% CI: 1.797–5.413) and cold war (OR=1.627,95% CI: 1.093–2.422) in parental conflict resolution, asking your relatives for help (OR=1.883,95% CI: 1.031–3.441), avoidance (OR=1.524,95% CI: 1.014–2.290) and at a loss (OR=1.772, 95% CI: 1.107–2.837) in children’s resolution of parental conflict. Besides, paternal severe punishment (OR=1.051,95% CI: 1.023–1.080), paternal rejection and denial (OR=1.084,95% CI: 1.027–1.143), paternal over-protection (OR=1.082,95% CI: 1.023–1.145), maternal over-protection (OR=1.047,95% CI: 1.024–1.071), maternal rejection and denial (OR=1.071,95% CI: 1.030–1.113), and maternal severe punishment (OR=1.087,95% CI:1.051–1.124) were positively correlated with new-onset MDD among college students. Conversely, apologize/negotiation/friendly interaction (OR=0.689,95% CI: 0.493–0.965), paternal emotional warmth (OR=0.972,95% CI: 0.958–0.987), and maternal emotional warmth (OR= 0.976,95% CI: 0.961–0.991) were negatively correlated with new-onset MDD among college students.
Gender-stratified analyses revealed distinct patterns. Males in this study, occasional physical violence/fights (OR=3.285, 95% CI: 1.724–6.260), chronic cold violence/ignorance of each other (OR=3.262, 95% CI: 1.605–6.631), and persistent conflict (OR=3.238, 95% CI: 1.130–9.277) and maternal severe punishment in parenting style (OR=1.062, 95% CI: 1.005–1.122) were positively correlated with new-onset MDD among college students, while the parental conflict resolution style was apologized/negotiation/friendly interaction (OR=0.539, 95% CI: 0.293–0.989) was negatively correlated with new-onset MDD among college students.
Among females in this study, verbal attacks/quarrels (OR=1.723,95% CI: 1.048–2.832) and long-term physical abuse (OR=6.374,95% CI: 1.407–28.873) in IPC, persistent conflict (OR=3.001,95% CI: 1.569–5.741) in parental conflict resolution, believing it is your fault (OR=3.441,95% CI: 1.212–9.765) and asking your relatives for help (OR=2.647,95% CI: 1.387–5.053) in children’s resolution of parental conflict, and paternal severe punishment (OR=1.079,95% CI: 1.044–1.116), paternal excessive interference (OR=1.083,95% CI: 1.033–1.136),paternal rejection and denial (OR=1.155, 95% CI: 1.078–1.239), paternal over-protection (OR=1.151,95% CI: 1.072–1.236), maternal over-protection (OR=1.069, 95% CI: 1.041–1.099), maternal rejection and denial (OR=1.10,95% CI: 1.055–1.164), and maternal severe punishment (OR=1.116,95% CI: 1.068–1.166) were positively correlated with new on-set MDD among college students. Positive parenting dimensions,such as paternal warmth/understanding (OR=0.967,95% CI:0.950–0.985) and maternal warmth/understanding (OR=0.967, 95% CI: 0.949–0.986) were negatively correlated with new-onset MDD among college students.
At the same time, Table 3 also shows the relationship between life events and new-onset MDD in male, female, and general college students. Lifetime severe traumatic events≥3(OR=2.423, 95% CI: 1.125–5.218; OR=2.850, 95% CI: 1.599–5.080; OR=2.666, 95% CI: 1.681–4.230), adolescent stressful life events≥10 (OR=4.664, 95% CI: 1.977–11.006; OR=3.551,95% CI:1.867–6.755;OR=4.046, 95% CI:2.420–6.766) were positively correlated with new-onset MDD in male, female and general population.
Multivariate Logistic Regression of Predictive Factors of New-Onset MDD by Gender
To identify independent predictors of new-onset MDD and test the hypothesis that the association between IPC and MDD differs by gender, we performed multivariate logistic regression analyses controlling for age, lifetime traumatic events, recent stressful life events, and significant parenting dimensions (Table 4 for males, Table 5 for females).
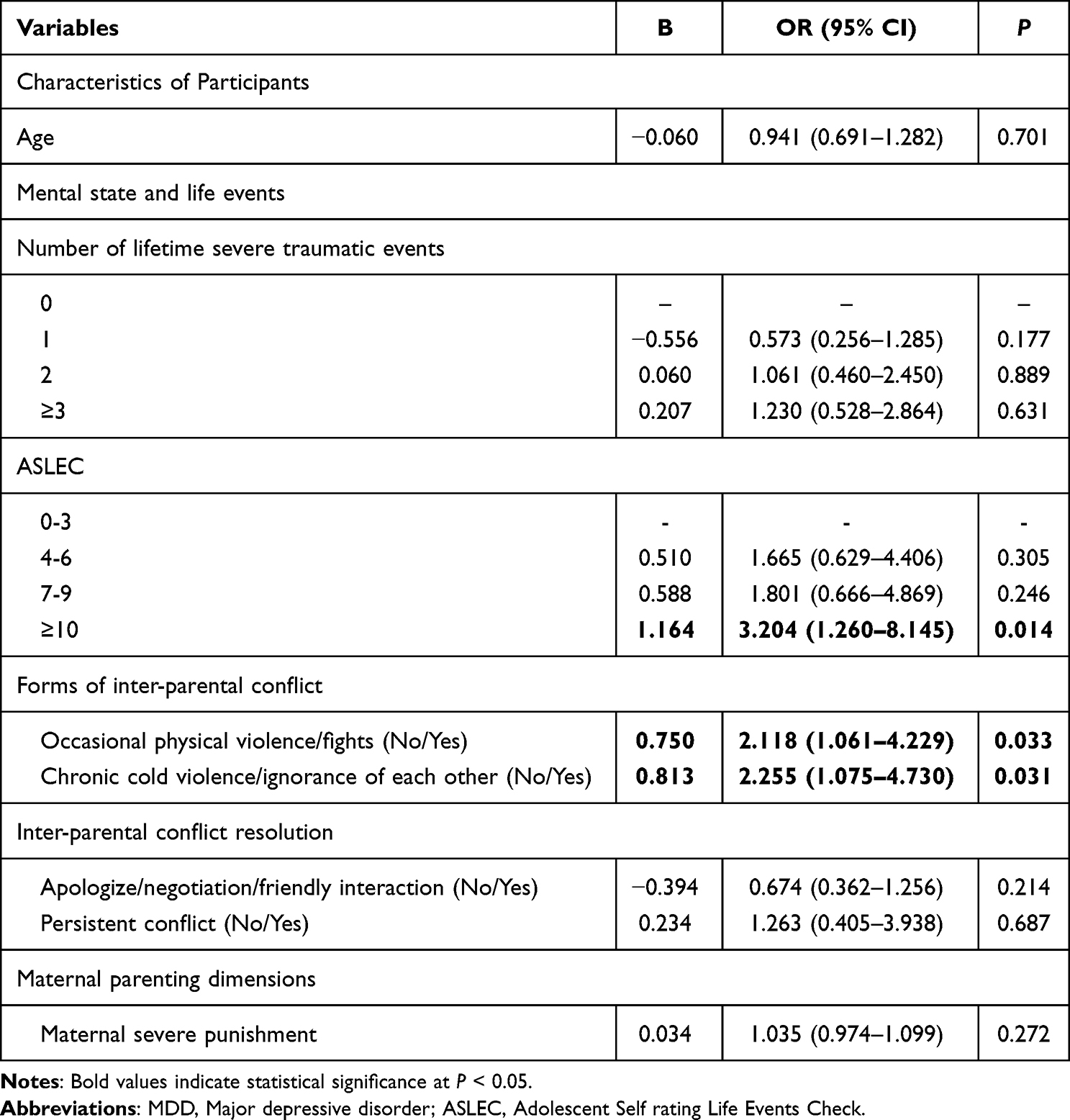 |
Table 4 Multivariate Logistic Regression of Predictive Factors of New-Onset MDD in Male College Students |
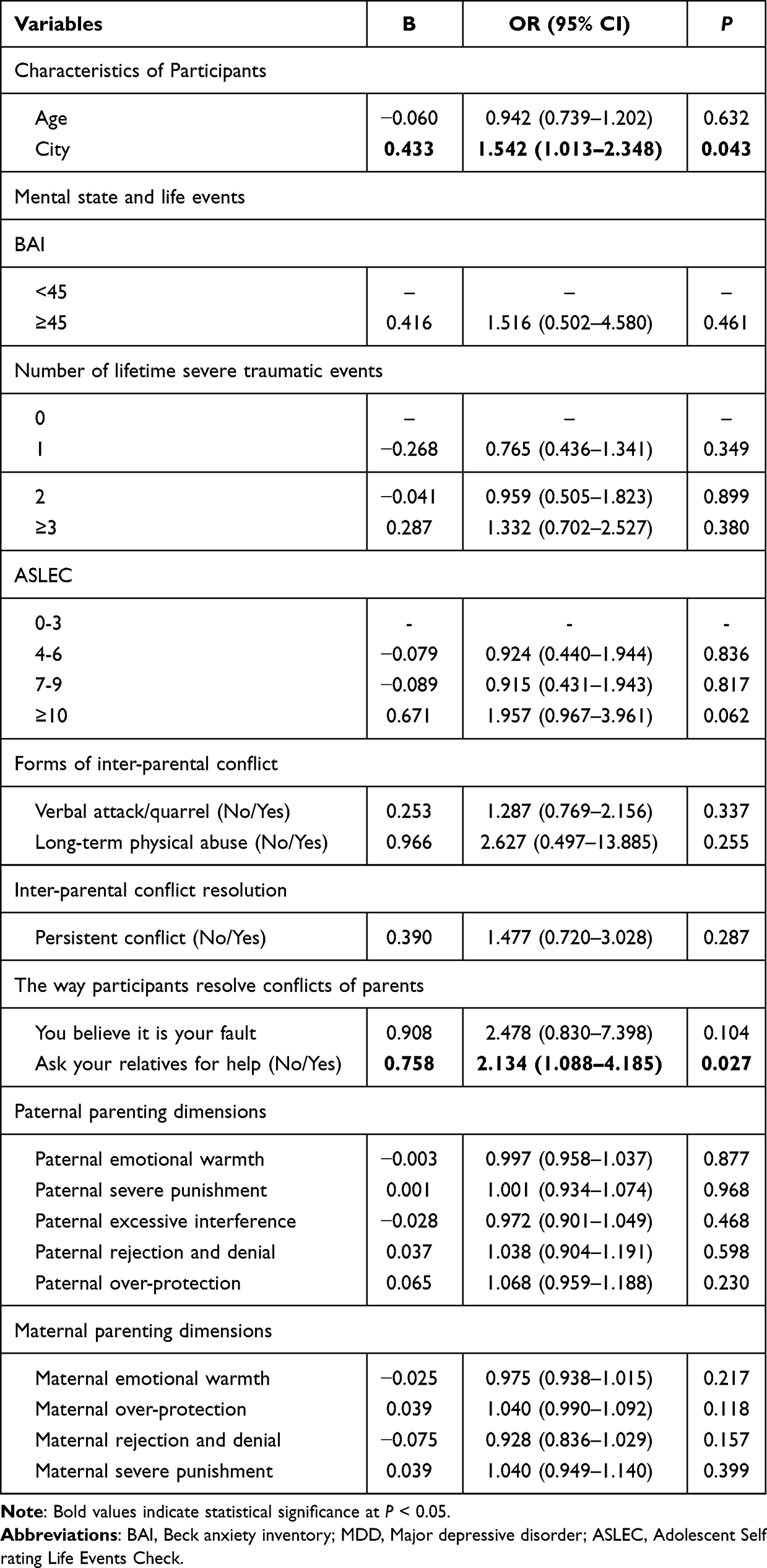 |
Table 5 Multivariate Logistic Regression of Predictive Factors of New-Onset MDD in Female College Students |
Among male students, after adjusting for covariates, two IPC-related factors remained significantly associated with new-onset MDD: occasional physical violence/fights (OR=2.118, 95% CI: 1.061–4.229) and chronic cold violence/ignorance of each other (OR=2.255, 95% CI: 1.075–4.730). At the same time, female college students had no statistical significance.
Among female college students, only one IPC-related factor was independently associated with new-onset MDD:Seeking help from relatives during parental conflict (OR= 2.134, 95% CI: 1.088–4.185),which is a risk factor, and it has no statistical significance in male college students. No other IPC manifestations or resolution methods remained significant in the final multivariate models for either gender.
Discussion
By analyzing relevant data from 6136 college students, this study shows that the overall incidence of MDD among college students is 2.3%, which is lower than the 6.9% incidence of MDD among college students in a previous foreign study.28 It is also lower than the 12-month prevalence estimates for MDD from recent global and national Chinese epidemiological surveys.29,30 The prevalence of MDD in men and women was 2.1% and 2.6%, respectively, lower than the prevalence of MDD in women (5.8%) and men (3.5%) at 12 months in a global study,31 which may be mainly due to population differences and regional differences. The results of this study show that the incidence of MDD in male college students is lower than that in female college students, which is consistent with the well-established epidemiological pattern of depression7,8 This difference has been attributed to a confluence of biological, psychological, and sociocultural factors, including interactions between sex hormones and stress-response systems,32 national economic level and gender equality rights differences,33 and differential exposure and reactivity to interpersonal stressors, and gender-role socialization.5,10
This study found that there were differences in the lifetime traumatic events of college students and the stressful life events of adolescents with new MDD, and lifetime severe traumatic events and recent stressful life events were significantly associated with new-onset MDD. Studies have showed that depression is a typical result of trauma exposure and mental health problems,such as insomnia and suicidal ideation in adolescents are associated with various types of traumatic events.3,34 Acute or ongoing stressful life events during adolescence—such as academic demands and interpersonal difficulties—represent significant environmental stressors that are positively associated with depressive symptoms in college populations.35,36 This study focused specifically on inter-parental conflict as a salient familial factor. Through gender-stratified analysis, we further demonstrated that specific manifestations of inter-parental conflict and distinct conflict resolution strategies were associated with the incidence of MDD, with significant gender differences observed.
Consistent with our first hypothesis, the results suggest that IPC has some degree of influence on the incidence of MDD among college students. Previous studies have shown that IPC has a particular impact on children’s behaviors, such as externalizing behaviors such as crime and cheating, and internalizing problems such as depression and anxiety.14,37 Other studies explored the relationship between adolescent academic participation and depressive symptoms and found that there was no direct relationship between co-parenting conflict and adolescent academic performance, but there was an indirect correlation between academic involvement and depressive symptoms and adolescent academic performance.16 Therefore, IPC impacts individual learning, mental health, and behavior. Our study extends this evidence to early adulthood, specifically among university students. Univariate analyses revealed that various dimensions of IPC—such as physical violence, emotional neglect, and destructive conflict resolution styles like persistent arguing or cold wars—were significantly associated with MDD risk in the overall sample. This aligns with the conceptual framework viewing chronic family discord as a potent stressor that can erode an individual’s sense of security and emotional well-being, potentially triggering or exacerbating depressive episodes.14 The findings reinforce the notion that the negative impact of family dynamics does not cease in childhood but can persist, influencing mental health during the critical transition to university life.15,16
Our analysis revealed that distinct forms of inter-parental conflict—such as physical violence and emotional neglect—as well as conflict resolution approaches, exerted differential influences on MDD risk in male and female students. In this study, occasional physical violence and prolonged cold violence in parental conflict may still hurt their mental health. Therefore, regardless of gender, the impact of parental conflict on mental health cannot be ignored, and early intervention and support are crucial to prevent depression.
The core contribution of this study lies in the evidence supporting our second hypothesis, revealing distinct gender-dependent mechanisms. After adjusting for key covariates including lifetime trauma and recent stressful life events—both confirmed as significant risk factors in our and others’ research4,34,36—multivariate models identified different IPC-related factors as independent predictors for males and females.
For male students, the experience of occasional physical violence/fights and chronic emotional neglect/cold violence between parents remained significant risk factors for new-onset MDD. This pattern may be interpreted through intersecting psychosocial and gendered lenses. Studies have found that after children experience psychological family violence, non-physical harm by mothers has a direct negative impact on children’s depression and anxiety.36 A study has shown that intimate partner violence (IPV) is often accompanied by child abuse and neglect, which hurts children’s physical and mental health.38 And a resent study suggested that lower levels of family functioning was associated with increased depression among adolescents.39 Therefore, IPC, whether physical or psychological domestic violence, can affect the development of a child’s mental health and may also hurt the mental health of male college students. In some cultures, men are given a more vital social role and are dominant in society.40 Compared with women, men are more likely to take action to maintain their gender status.41 However, in family relationships, their dominance may be highly diminished, which can lead to MDD in the face of parental physical violence. Studies have shown that men are more inclined to use avoidance to cope with some stressful events,40 so when affected by family physical violence, they may be more likely to internalize emotions, leading to the emergence of MDD. Other studies have found that numerous college boys believe that seeking psychological help is a shame, perhaps because male gender role socialization prohibits seeking help.42 As a result, when men face physical or cold violence from their parents, they do not have a strong desire to seek help from others, and their emotions are not alleviated, which may increase the risk of MDD. However, it should be noted that this does not mean that female university students are unaffected by parental conflict.
Conversely, for female students, the significant independent risk factor was seeking help from relatives during parental conflicts. In society, women are considered to be more emotionally sensitive and more likely to express inner pain.43 However, due to cultural differences, high adherence to familial norms means that individuals may not seek help, while participants with low adherence to familial norms are likely to seek help regardless of their respective families’ opposition.44 Rather than seeking professional help, adolescents, and male adolescents particularly, may attempt to resolve their difficulties alone.45 In such cases, seeking help from relatives may increase their exposure to negative emotions and stress at the family level, which may increase their risk of developing MDD. Studies have shown that the presence of relatives who have consulted mental health services may indicate a certain willingness to discuss mental health issues in the family system, which may contribute to children’s mental health.46 However, few people in China seek professional psychological help.45,47 As a result, when they seek help from relatives, they are likely to receive no practical support and understanding, which may further exacerbate negative thinking and negative emotions in more emotionally sensitive women, which may increase the risk of further MDD at a later stage.
There are some differences in how men and women understand and respond to IPC and how it contributes to the onset of MDD. Therefore, when dealing with family conflicts, we should take into account the characteristics and needs of members of different genders and provide them with appropriate support to help reduce their psychological burden and promote their normal development. This study found that IPC is a risk factor for new MDD in college students, so addressing IPC can reduce psychological stress and contribute to their normal emotional development and excellent psychological quality. A resent study show that improving parent-child relationships and enhancing youths’ perceptions of social safety may improve adolescent health.48 Effective communication, understanding, compromise, working together to resolve conflicts between parents, and creating a harmonious and pleasant family environment can also play a positive role in the healthy development of adolescents’ psychological levels.
Limitations
Although this is a large-sample longitudinal cohort study, it still has certain limitations. First, the samples were collected only from two medical universities in Shandong Province, China, which may limit the generalizability of the findings. In future work, we will expand the sample scope to a multicenter setting to enhance representativeness. Second, the data were collected through self-report questionnaires, instruments such as the EMBU, relyed on retrospective recall and were therefore susceptible to recall bias. In future studies, we will refine both the item content and the administration format of these scales to reduce confounding factors and enhance the scientific rigor. Finally, regarding the sample size, although this is a large-sample study, the subgroup analysis revealed a notably smaller number of New-onset MDD cases compared to No-MDD cases. While this aligns with the epidemiological characteristics of MDD, the results should still be interpreted with caution. Future studies should further expand the sample size to enhance statistical power.
Conclusion
This study investigated the association between IPC and the risk of new-onset MDD among Chinese college students, with a specific focus on gender differences. Exposure to specific manifestations and resolution methods of IPC was significantly associated with an increased incidence of new-onset MDD in the overall student population. For male students, experiences of occasional physical violence and chronic emotional neglect (characterized as cold violence or mutual ignorance) between parents emerged as independent risk factors for new-onset MDD. Conversely, for female students, the act of seeking help from relatives during parental conflicts was identified as a unique and significant risk factor.
These findings indicate that IPC influences MDD risk through gender-specific pathways, underscoring the need for gender-sensitive prevention strategies.Targeted interventions should address overt physical or chronic emotional conflict for male students, and the tendency to involve relatives in parental disputes for female students. Ultimately, improving family communication and providing gender-appropriate coping resources are essential to mitigate the long-term mental health impact of IPC and enhance resilience during university transition.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author Jianli Yang upon reasonable request.
Ethics Statement and Informed Consent
This study was approved by the Medical Research Ethics Committee in Jining Medical University, Jining, China, code: 2019-JS-004. This study complies with Declaration of Helsinki. All participants provided informed consent.
Acknowledgment
The authors would like to thank the participants for their involvement in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Taishan Scholars Program of Shandong Province (tsqn201909145), Youth Fund of National Natural Science Foundation of China (Grant number: 81901391),Ministry of Education Industry-University Cooperation Collaborative Education Program (No.240904727200051),The Ministry of Education’s Employment Education Project for Supply-Demand Matching (No.2024110630461, No.2025030329663). All funders had no role in the design and conduction of this study.
Disclosure
All authors declare that they have no conflicts of interest associated with this work.
References
1. Zhuo C, Li G, Lin X, et al. The rise and fall of MRI studies in major depressive disorder. Transl Psychiatry. 2019;9(1):335. doi:10.1038/s41398-019-0680-6
2. Collaborators GBDMD. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet Psychiatry. 2022;9:137–150.
3. Zhou SC, Luo D, Wang XQ, et al. Suicidal ideation in college students having major depressive disorder: role of childhood trauma, personality and dysfunctional attitudes. J Affect Disord. 2022;311:311–318. doi:10.1016/j.jad.2022.05.085
4. Sun T, Zhang L, Liu Y, et al. The relationship between childhood trauma and insomnia among college students with major depressive disorder: mediation by the role of negative life events and dysfunctional attitudes. Compr Psychiatry. 2023;122:152368. doi:10.1016/j.comppsych.2023.152368
5. Shi J, Han X, Liao Y, et al. Associations of stressful life events with subthreshold depressive symptoms and major depressive disorder: the moderating role of gender. J Affect Disord. 2023;325:588–595. doi:10.1016/j.jad.2023.01.050
6. Cheng J, Liu D, Zheng H, et al. Perceived parenting styles and incidence of major depressive disorder: results from a 6985 freshmen cohort study. BMC Psychiatry. 2023;23:230. doi:10.1186/s12888-023-04712-0
7. Eid RS, Gobinath AR, Galea LAM. Sex differences in depression: insights from clinical and preclinical studies. Prog Neurobiol. 2019;176:86–102. doi:10.1016/j.pneurobio.2019.01.006
8. Lu J, Xu X, Huang Y, et al. Prevalence of depressive disorders and treatment in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2021;8(11):981–990. doi:10.1016/S2215-0366(21)00251-0
9. Pedrelli P, Borsari B, Lipson SK, et al. gender differences in the relationships among major depressive disorder, heavy alcohol use, and mental health treatment engagement among college students. J Stud Alcohol Drugs. 2016;77(4):620–628. doi:10.15288/jsad.2016.77.620
10. Jin Y, Fan Y, He J, et al. Symptomatic associations and sexual differences in depression and communication. Npj Mental Health Research. 2024;3(1):59. doi:10.1038/s44184-024-00098-3
11. Schuch JJ, Roest AM, Nolen WA, et al. Gender differences in major depressive disorder: results from the Netherlands study of depression and anxiety. J Affect Disord. 2014;156:156–163. doi:10.1016/j.jad.2013.12.011
12. Pawlak JL, Klein HA. Parental conflict and self-esteem: the rest of the story. J Genetic Psychol. 1997;158(3):303–313. doi:10.1080/00221329709596670
13. Du Rocher Schudlich TD, Cummings EM. Parental dysphoria and children’s adjustment: marital conflict styles, children’s emotional security, and parenting as mediators of risk. J Abnorm Child Psychol. 2007;35:627–639. doi:10.1007/s10802-007-9118-3
14. van Eldik WM, de Haan AD, Parry LQ, et al. The interparental relationship: meta-analytic associations with children’s maladjustment and responses to interparental conflict. Psychol Bull. 2020;146:553–594. doi:10.1037/bul0000233
15. Zhen S, Liu J, Qiu B, et al. Interparental conflict and early adulthood depression: maternal care and psychological needs satisfaction as mediators. Int J Environ Res Public Health. 2022;19. doi:10.3390/ijerph19031402
16. Yang H, Wu C, Chen JK. Interparental and intergenerational co-parenting conflict and adolescent academic performance: the mediating roles of adolescent academic engagement and depression. Int J Environ Res Public Health. 2022;19(23):15952. doi:10.3390/ijerph192315952
17. Espinoza CN, Goering M, Mrug S. Inter-parental conflict and empathy in early adolescence as predictors of dating violence perpetration in adolescence and adulthood. J Res Adolesc. 2024;34(4):1287–1299. doi:10.1111/jora.12987
18. Choi DW, Han KT, Jeon J, et al. Association between family conflict resolution methods and depressive symptoms in South Korea: a longitudinal study. Arch Womens Ment Health. 2020;23:123–129. doi:10.1007/s00737-019-00957-5
19. García-Montero C, Ortega MA, Alvarez-Mon MA, et al. The problem of malnutrition associated with major depressive disorder from a sex-gender perspective. Nutrients. 2022;14(5):1107. doi:10.3390/nu14051107
20. Li N, Zhang X, Zheng Y, et al. The impact of perfectionism on the incidence of major depression in Chinese medical freshmen: from a 1-year longitudinal study. Psychol Res Behav Manag. 2024;17:4053–4062. doi:10.2147/PRBM.S479381
21. Wang J, Liu D, Li G, et al. The impact of self-efficacy on first onset and prognosis of major depressive disorder: findings from a longitudinal study in a sample of Chinese first-year university students. Psychol Med. 2022;52(1):178–183. doi:10.1017/S0033291721003238
22. Kessler RC, Ustün TB. The World Mental Health (WMH) survey initiative version of the World Health Organization (WHO) Composite International Diagnostic Interview (CIDI). Int J Methods Psychiatr Res. 2004;13:93–121. doi:10.1002/mpr.168
23. Huang YQ, Xie SF, Lu J, et al. Community-based evaluation of the reliability and validity of Chinese version of composite international diagnostic interview-3.0. Chin Mental Health J. 2010;24:21–24+28.
24. Liu XC, Liu LQ, Yang J, et al. Development and reliability and validity test of adolescent life events scale. Shandong J Psych. 1997;01:15–19.
25. Perris C, Jacobsson L, Lindström H, et al. Development of a new inventory assessing memories of parental rearing behaviour. Acta Psychiatr Scand. 1980;61(4):265–274. doi:10.1111/j.1600-0447.1980.tb00581.x
26. Yue DM, Li MG, Jin KH, et al. Premiliminary revision of EMBU and its application in neurotic patients. Chin Mental Health. 1993;7:97–101+143.
27. Gosselin RD. Testing for normality: a user’s (cautionary) guide. Lab Anim. 2024;58(5):433–437. doi:10.1177/00236772241276808
28. Ebert DD, Buntrock C, Mortier P, et al. Prediction of major depressive disorder onset in college students. Depress Anxiety. 2019;36:294–304. doi:10.1002/da.22867
29. GBD. Diseases and Injuries Collaborators. Global incidence, prevalence, years lived with disability (YLDs), disability-adjusted life-years (DALYs), and healthy life expectancy (HALE) for 371 diseases and injuries in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet.2024. 2021;403(10440):2133–2161. doi:10.1016/S0140-6736(24)00757-8
30. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
31. Ferrari AJ, Somerville AJ, Baxter AJ, et al. Global variation in the prevalence and incidence of major depressive disorder: a systematic review of the epidemiological literature. Psychol Med. 2013;43:471–481. doi:10.1017/S0033291712001511
32. Shansky RM. Estrogen, stress and the brain: progress toward unraveling gender discrepancies in major depressive disorder. Expert Rev Neurother. 2009;9:967–973. doi:10.1586/ern.09.46
33. Salk RH, Hyde JS, Abramson LY. Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol Bull. 2017;143:783–822. doi:10.1037/bul0000102
34. Liu H, Ye B, Hu Y. Stressful life events and depression during the recurrent outbreak of COVID-19 in China: the mediating role of grit and the moderating role of gratitude. Psychol Res Behav Manag. 2022;15:1359–1370. doi:10.2147/PRBM.S360455
35. Wang F, Rong L, Luo L, et al. Associations between psychological stress and the risk of first onset of major depression disorder: results from a longitudinal study in 6,985 Chinese first-year students. Psychol Res Behav Manag. 2024;17:3585–3593. doi:10.2147/PRBM.S482482
36. Chen WY, Lee Y. Mother’s exposure to domestic and community violence and its association with child’s behavioral outcomes. J Community Psychol. 2021;49:2623–2638. doi:10.1002/jcop.22508
37. Zhang Z, Wang Y, Zhao J. Longitudinal relationships between interparental conflict and adolescent depression: moderating effects of school connectedness. Child Psychiatry Hum Dev. 2023;54(5):1489–1498. doi:10.1007/s10578-022-01355-2
38. Pu DF, Rodriguez CM. Spillover and crossover effects: mothers’ and fathers’ intimate partner violence, parent-child aggression risk, and child behavior problems. Child Maltreat. 2021;26:420–430. doi:10.1177/1077559520985936
39. Luo R, Chen F, Ke L, et al. Interparental conflict and depressive symptoms among Chinese adolescents: a longitudinal moderated mediation model. Dev Psychopathol. 2023;35(2):972–981. doi:10.1017/S0954579422000190
40. Berke DS, Liautaud M, Tuten M. Men’s psychiatric distress in context: understanding the impact of masculine discrepancy stress, race, and barriers to help-seeking. J Health Psychol. 2022;27:946–960. doi:10.1177/1359105320977641
41. Stanaland A, Gaither S, Gassman-Pines A.When is masculinity “fragile”? An expectancy-discrepancy-threat model of masculine identity. Pers Soc Psychol Rev. 2023;27:359–377. doi:10.1177/10888683221141176
42. Booth NR, McDermott RC, Cheng HL, et al. Masculine gender role stress and self-stigma of seeking help: the moderating roles of self-compassion and self-coldness. J Couns Psychol. 2019;66:755–762. doi:10.1037/cou0000350
43. Thomas M, Gaudeau-Bosma C, Bouaziz N, et al. Gender-related brain activations during an emotional task: an fMRI study. Neuropsychobiology. 2019;78:128–135. doi:10.1159/000499977
44. Ishikawa RZ, Cardemil EV, Falmagne RJ. Help seeking and help receiving for emotional distress among Latino men and women. Qual Health Res. 2010;20:1558–1572. doi:10.1177/1049732310369140
45. Yong N, Luo J, Luo JM, et al. Non-suicidal self-injury and professional psychological help-seeking among Chinese left-behind children: prevalence and influencing factors. BMC Psychiatry. 2023;23(1):291. doi:10.1186/s12888-023-04801-0
46. Zwaanswijk M, van der Ende J, Verhaak PF, et al. Help-seeking for child psychopathology: pathways to informal and professional services in the Netherlands. J Am Acad Child Adolesc Psychiatry. 2005;44(12):1292–1300. doi:10.1097/01.chi.0000181038.98712.c6
47. Shi W, Shen Z, Wang S, et al. Barriers to professional mental health help-seeking among Chinese adults: a systematic review. Front Psychiatry. 2020;11:442. doi:10.3389/fpsyt.2020.00442
48. Alley J, Tsomokos DI, Mengelkoch S, Slavich GM. Childhood maternal warmth, social safety schemas, and adolescent mental and physical health. JAMA Psychiatry. 2025;82(7):709–717. doi:10.1001/jamapsychiatry.2025.0815
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.