Back to Journals » Clinical and Experimental Gastroenterology » Volume 11
Inflammatory bowel disease epidemiology in São Paulo State, Brazil
Authors Gasparini RG ![]() , Sassaki LY
, Sassaki LY ![]() , Saad-Hossne R
, Saad-Hossne R ![]()
Received 8 June 2018
Accepted for publication 31 August 2018
Published 30 October 2018 Volume 2018:11 Pages 423—429
DOI https://doi.org/10.2147/CEG.S176583
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Hoda Malaty
Rodrigo Galhardi Gasparini, 1 Ligia Yukie Sassaki, 2 Rogerio Saad-Hossne 3
1Department of Digestive Surgery and Gastroenterology, Sete Specialized Medical Center, Marília, Brazil; 2Department of Internal Medicine, Botucatu Medical School at Sao Paulo State University (UNESP), Botucatu, Brazil; 3Department of Surgery, Botucatu Medical School at Sao Paulo State University (UNESP), Botucatu, Brazil
Purpose: This study aimed to estimate the incidence and prevalence of inflammatory bowel disease (IBD) in São Paulo, Brazil, for 2012– 2015.
Patients and methods: This observational, descriptive, and cross-sectional study included 22,638 IBD patients out of 43,046,555 inhabitants, who had initiated their treatment through the Governmental Program of the Brazilian Unified National Health System between the years of 2012 and 2015. The onset of the disease (used to determine incidence) was established as the date of the patient’s initial registration in the Governmental Program with a diagnosis for Crohn’s disease (CD) or ulcerative colitis (UC). Every patient registered in the system as of December 2015 was included in determining the prevalence. The demographic and clinical data, such as age and sex, were collected for each patient. Statistical analysis included mean and SD, absolute and percentage frequencies, and Pearson’s chi-squared test (X²). The incidence and prevalence rates were calculated based on the estimated annual population of the State of São Paulo.
Results: The study population consisted of 10,451 (46.16%) CD patients and 12,187 (53.84%) UC patients. The mean age was 42.66 (SD± 16.2) years for the CD group and 47.87 (SD± 16.6) years for the UC group. There was a predominance of females corresponding to 59.70% of the study population (female:male =1.48:1.00; P< 0.0001). The incidence of IBD was 13.30 new cases/100,000 inhabitants per year, while the overall prevalence was 52.6 cases/100,000 inhabitants.
Conclusion: This population-based study demonstrated a stability in IBD incidence rates and an increase in IBD prevalence rates in São Paulo state between 2012 and 2015. The IBD incidence and prevalence rates were comparable to European countries, with a higher occurrence in the female participants.
Keywords: inflammatory bowel disease, Crohn’s disease, ulcerative colitis, epidemiology, incidence, prevalence
Corrigendum for this paper has been published
Introduction
Inflammatory bowel disease (IBD) is characterized by an inflammatory process that compromises the digestive tract, partially or totally. Ulcerative colitis (UC) and Crohn’s disease (CD) are its main representatives, with distinct and individual pathophysiological, clinical, and pathological characteristics.1–3 Although considered uncommon, IBD presents characteristics of chronicity, severity, evolution, and morbidity that significantly affect the quality of life of patients.1–3
Changes in the typical geographic distribution of IBD have been observed over the last years, with increasing rates of incidence and prevalence in regions with low incidence traditionally, such as Asia, South America, and Southern and Eastern Europe; as such, there has been an increase in the consideration of IBD as an emerging global disease.4–6 Brazil has been considered as a country with low incidence and prevalence of IBD, although an evident increase in the number of appointments and hospitalizations of patients for IBD has occurred.7–9
There are few Brazilian epidemiological studies, possibly because there is no integrated diagnostic notification system, for IBD. Thus, the aim of this study was to estimate the incidence and prevalence rates of IBD in the State of São Paulo, the most populous in Brazil, between the years of 2012 and 2015, and analyze the patients’ demographic characteristics.
Patients and methods
Study design and population
This observational, descriptive, and cross-sectional study included data from 22,638 patients who had initiated their treatment for IBD through the Governmental Program for free supply of high-cost medicines of the Brazilian Unified National Health System (SUS). All the patients registered in the program received salicylates and/or immunosuppressive and/or immunobiological drugs. No patient was excluded from the study.
The Governmental Program for free supply of high-cost medicines of the SUS is responsible for the coverage of ~70% of the population. Data from private health insurance were not included in this study.
The moment of interest of the study was established as the date of initial registration in the Governmental Program of the patient with a diagnosis of CD or UC, with that date being defined as the date of disease onset. The clinical and demographic data, such as age and sex, were collected at that moment. For determining the prevalence, every patient registered in the system was included, regardless of their registration date. For determining the incidence, only patients whose initial registration occurred between January 2012 and December 2015 were included. All information presented herein was extracted from the computerized system of SUS for the State of São Paulo. The International Classification of Diseases codes K50 and K51 were used to identify CD and UC patients, respectively.10
All the data accessed from the SUS is de-identified in order to preserve the privacy and the identity of the studied population.
Quality of the present study was assessed with the Cochrane Collaboration-endorsed Newcastle-Ottawa Quality Assessment Scale (NOS), which was modified to assess aspects of quality relevant to population-based study of incidence.11
Data analyses
The data collected were initially imported into the DBase III database for processing and tabulation, after which they were exported to spreadsheets in the Microsoft Excel program. Statistical analysis was conducted with analysis of mean and SD, for quantitative analysis, and absolute and percentage frequencies for qualitative variables. The Pearson’s chi-squared test (χ2) of independence and adherence was used to analyze the qualitative variables and assess if the diseases followed a uniform distribution; mean estimate with a 99% confidence interval (CI 99%). Significance was defined as P<0.01 for all tests.
The incidence and prevalence rates were calculated based on the estimated annual population of the State of São Paulo as follows: 41,939,997 inhabitants in 2012 (20,409,123 males and 21,530,874 females); 42,304,694 inhabitants in 2013 (20,586,963 males and 21,717,731 females); 42,673,386 inhabitants in 2014 (20,766,532 males and 21,906,854 females); and 43,046,555 inhabitants in 2015 (20,948,275 males and 22,098,280 females).
The annual correction of population growth estimated was 0.87%.12,13
Ethical approval
This study was approved by the Research Ethics Committee of the Universidade Estadual Paulista “Júlio de Mesquita Filho” (Protocol Number: 33401214.5.0000.5411).
Results
The study involved epidemiological data of 22,638 individuals out of a total of 43,046,555 patients. CD patients comprised 10,451 (46.16%) and UC patients comprised 12,187 (53.84%) of the selected patients.
Age
The mean age of the overall study population was 45.5 (SD ±16.7) years, being 42.66 (SD ±16.2) years for the CD patients and 47.87 (SD ±16.6) years for the UC patients. The distribution of patients according to age is shown in Figure 1.
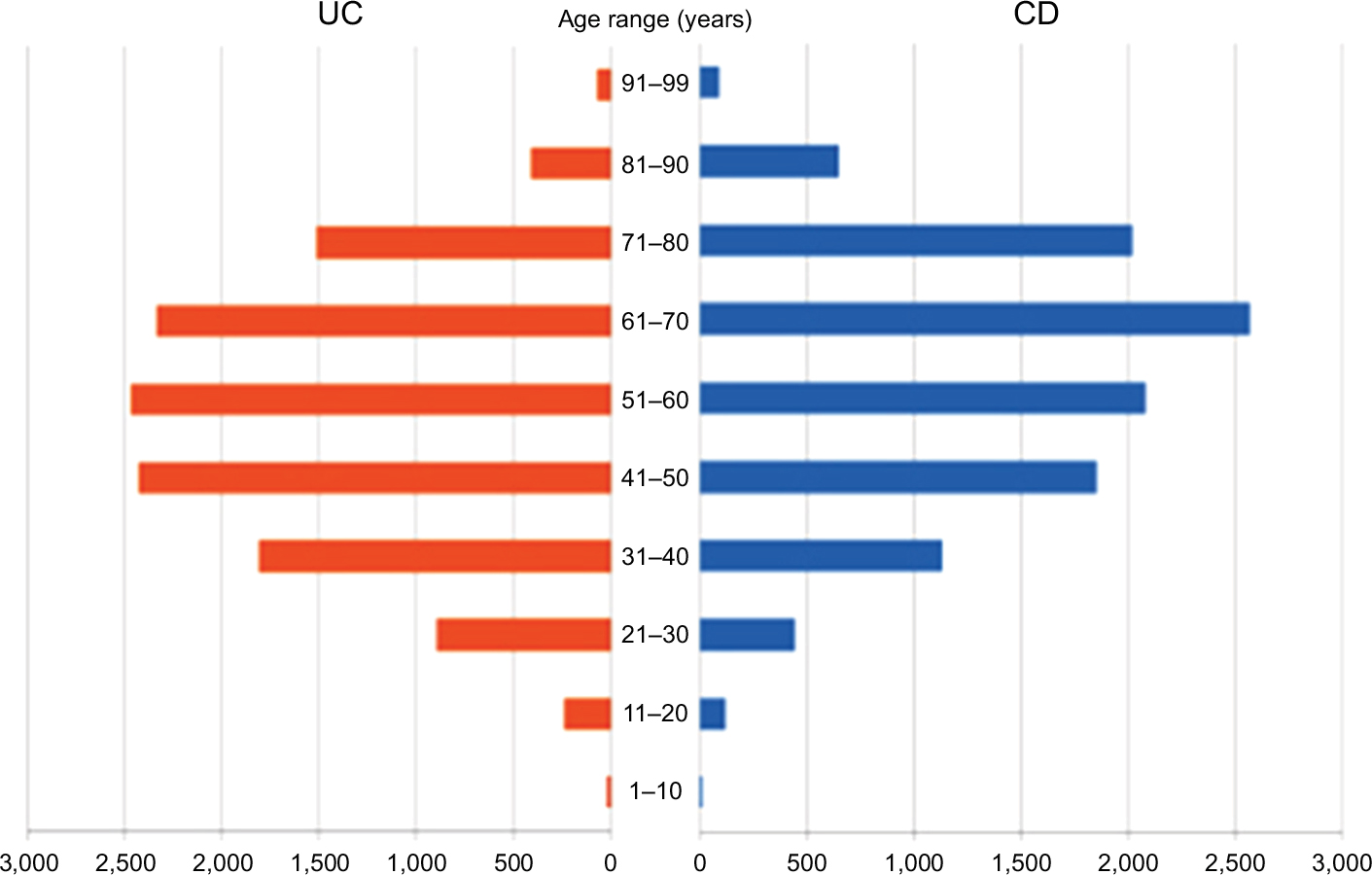 | Figure 1 Distribution of patients with CD (n=10.451) and UC (n=12.187) by age in the State of São Paulo (Brazil) for the period of 2012–2015. Abbreviations: CD, Crohn’s disease; UC, ulcerative colitis. |
Sex
There was a predominance of female sex, corresponding to 59.70% of the overall study population (female:male ratio =1.48:1.00; P<0.0001). The CD patients comprised 6,050 (57.9%) females and 4,401 (42.1%) males (female:male ratio =1.37:1.00; P<0.0001), while the UC patients comprised 7,464 (61.3%) females and 4,723 (38.7%) males (female:male ratio =1.58: 1.00; P<0.0001).
Incidence and prevalence
Incidence analyses of IBD cases, as well as CD and UC cases, between 2012 and 2015, are shown in Figures 2–4, respectively. The mean annual incidence of IBD was 13.30 new cases/100,000 inhabitants, considering incidence of CD as 6.14 new cases/100,000 inhabitants/year (mean) and incidence of UC as 7.16 new cases/100,000 inhabitants/year (mean).
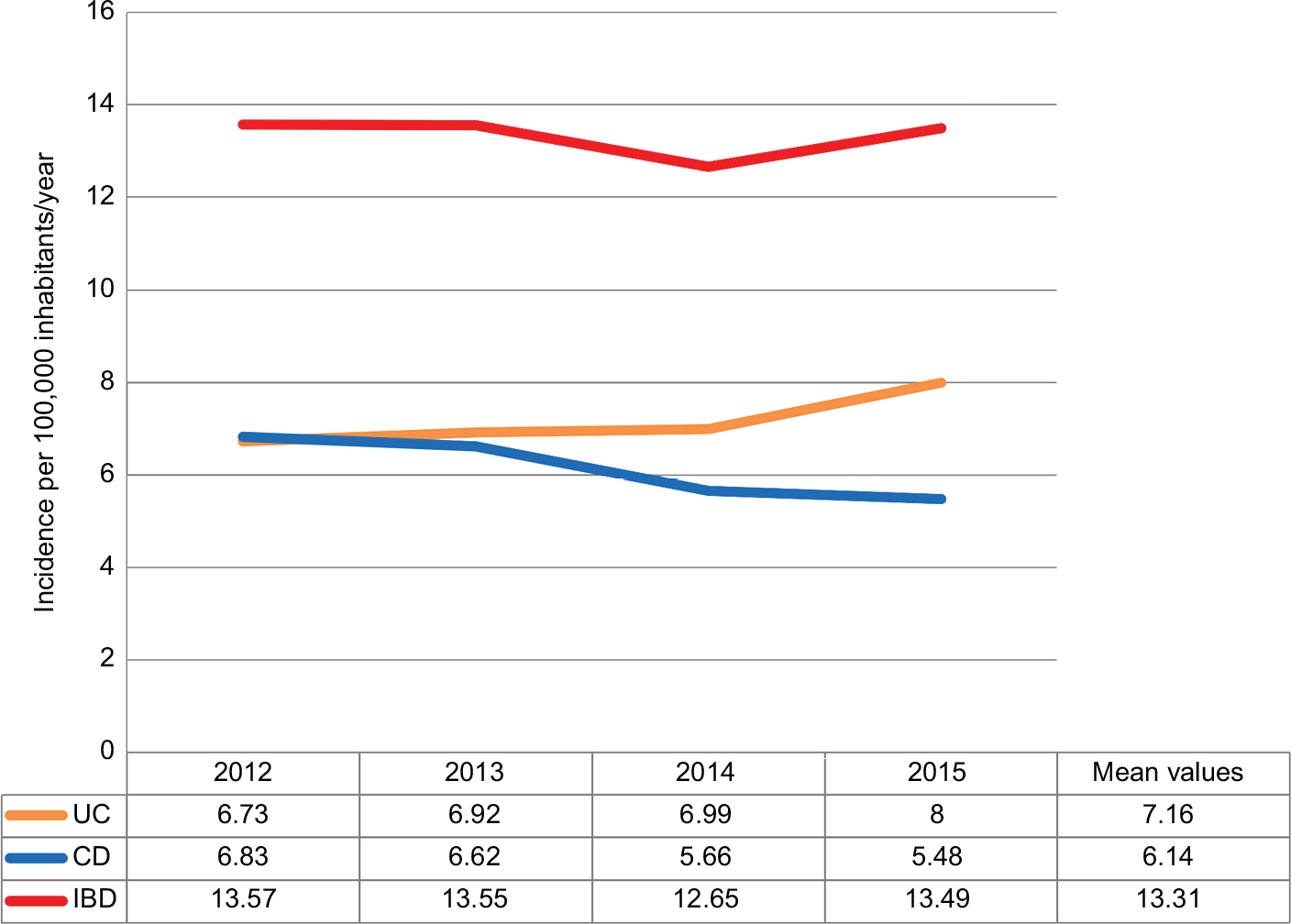 | Figure 2 Annual incidence rates for IBD, CD, and UC in the State of São Paulo. Note: Data are presented as new cases per 100,000 inhabitants/year. Abbreviations: CD, Crohn’s disease; IBD, inflammatory bowel disease; UC, ulcerative colitis. |
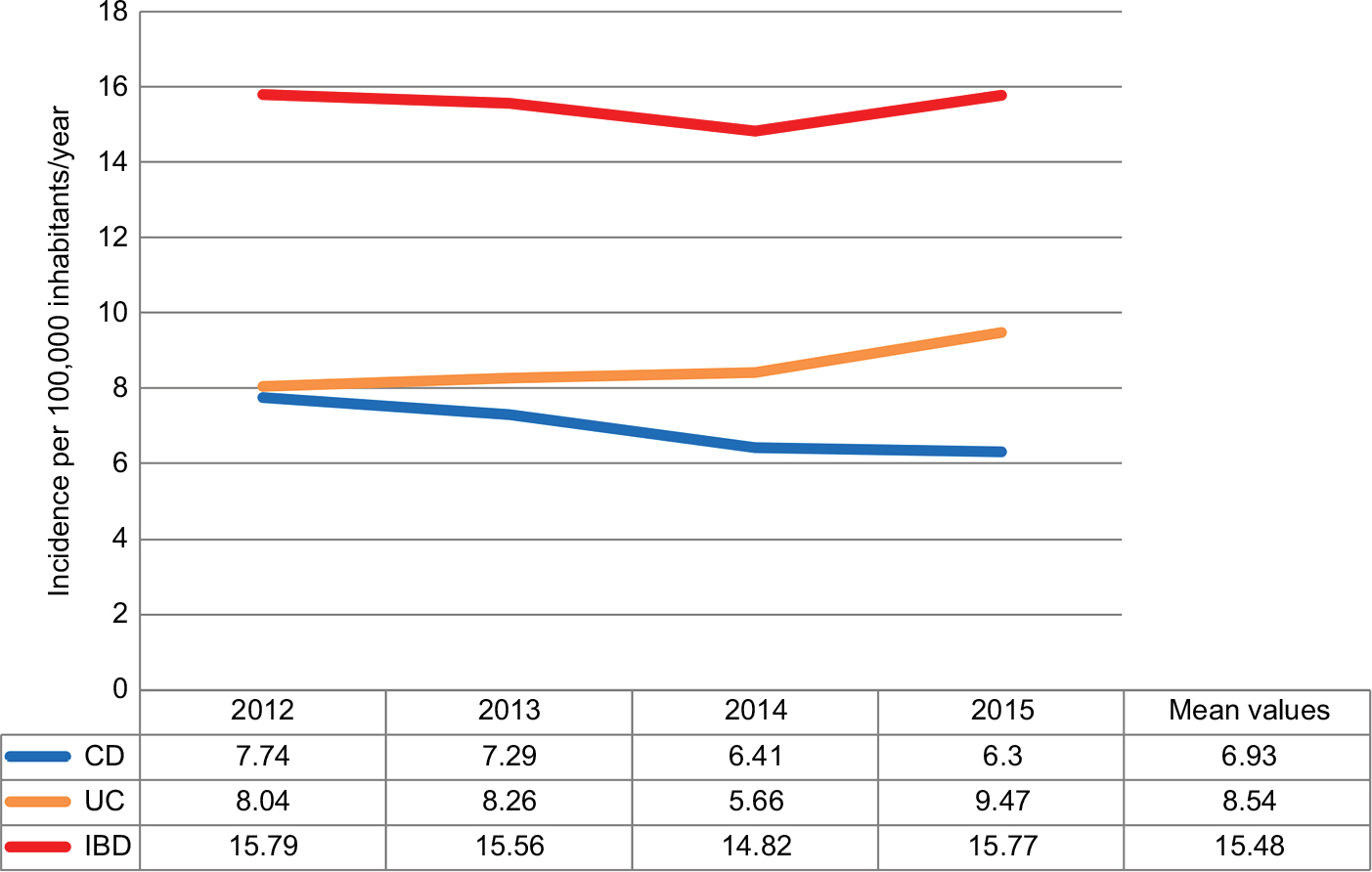 | Figure 3 Annual incidences of IBD, CD, and UC among the female participants in the State of São Paulo for the period of 2012–2015. Notes: Data are presented as new cases per 100,000 inhabitants/year. Abbreviations: CD, Crohn’s disease; IBD, inflammatory bowel disease; UC, ulcerative colitis. |
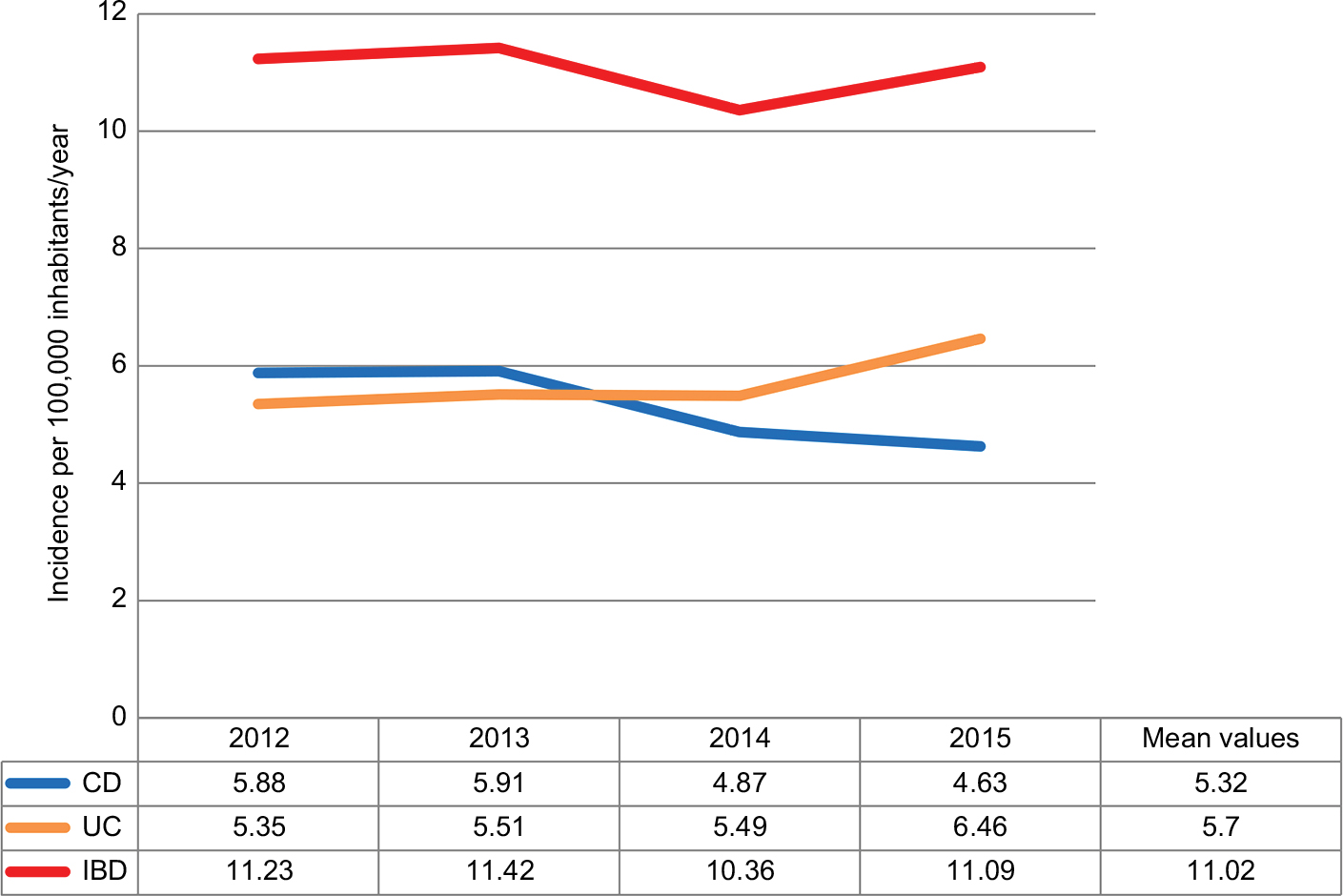 | Figure 4 Annual incidences of IBD, CD, and UC among the male participants in the State of São Paulo for the period of 2012–2015. Note: Data are presented as new cases per 100,000 inhabitants/year. Abbreviations: CD, Crohn’s disease; IBD, inflammatory bowel disease; UC, ulcerative colitis. |
The prevalence rates of IBD, both in general and by specific diseases (CD and UC), are shown in Table 1.
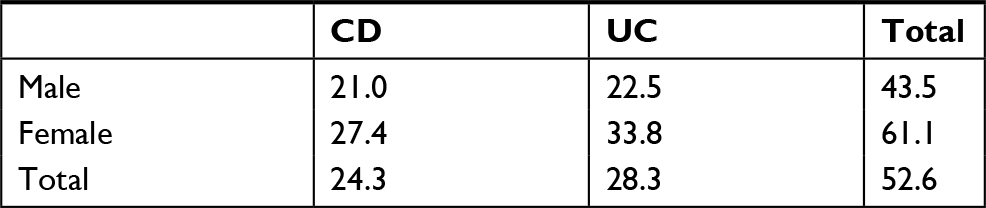 | Table 1 Prevalence of IBD in the State of São Paulo in December 2015 Note: Data are presented as new cases per 100,000 inhabitants. Abbreviations: CD, Crohn’s disease; IBD, inflammatory bowel disease; UC, ulcerative colitis. |
Discussion
Brazil is considered as a country with low incidence and prevalence of IBD.7,14 Although national databases on incidence and prevalence of these diseases are deficient, there are data that indicate an increasing trend in the occurrence of IBD, even in the absence of precise information on new cases.14
São Paulo State is the most developed state in South America; its near 43 million inhabitants represent 21% of the entire Brazilian population and account for 28.7% of the Brazilian gross national product. About three million immigrants live in the state, coming from more than 70 different nations, and this demographic profile is representative of the overall Brazilian population. In addition, the state utilizes a fully computerized system for its Governmental Program providing the free supply of high-cost medicines, which allows for a safe parameterization of the obtained data.13
The SUS is considered to be one of the largest health systems in the world and was established through the Brazilian Federal Constitution of 1988, since the legislation itself contemplates the right to health for all citizens. The free supply of medication is included in the assistance provided by the SUS.15 About 71.1% of the national population uses the system, with ~58% depending exclusively on it. The majority of IBD patients in Brazil obtain their drugs through the Governmental Program for providing the free supply of high-cost medicines, even with the increasing treatment of these patients in the private health system, which has been observed in recent years.15,16 Data from the private health insurance were not included in this study, which could either overestimate or underestimate the true incidence and prevalence rates. A study performed in Porto Rico showed the IBD prevalence was higher (61.75 cases) among commercial compared to government-sponsored managed health care insured individuals (14.36 cases).17
The slight drop in the incidence rates of CD observed in the study over the years can be explained by the drop in the number of patients enrolled in the Governmental Program in recent years. According to the present study, the incidence of CD was 6.14 new cases/100,000 inhabitants/year (mean) and the incidence of UC was 7.16 new cases/100,000 inhabitants/year (mean). The prevalence rate was 24.3 cases/100,000 inhabitants for CD and 28.3 cases/100,000 inhabitants for UC. The IBD epidemiologic study by Victoria et al published in 2009 and conducted in the Midwestern region of the State of São Paulo demonstrated increases in the incidence between 1986 and 2005 (from 1.0 to 8.0 cases per 100,000 inhabitants) and in the prevalence (from 1.2 to 20.5 cases per 100,000 inhabitants), accounting for 5.6 cases/100,000 inhabitants for CD and 14.8 cases/100,000 inhabitants for UC.7 Comparatively, we also observed a significant increase in the rates of incidence of CD and UC between 2012 and 2015. The rate of prevalence of IBD detected in this study, being 52.6 cases/100,000 inhabitants, suggests a growing trend for these diseases in the State of São Paulo.
The numbers determined in the present study are higher than those presented for Brazil in the systematic review by Ng et al, which demonstrated an incidence of CD from 0.81 to 1.94 new cases/100,000 inhabitants/year and an incidence of UC from 1.86 to 3.09 new cases/100,000 inhabitants/year. Concerning the prevalence, our data are also higher to those reported by Ng et al, which varied from 0.6 to 6.75 cases/100,000 inhabitants for CD and from 2.42 to 21 cases/100,000 inhabitants for UC.18
The incidence rate for CD in North America is over 6.38 new cases/100,000 inhabitants/year and for UC is over 7.71 new cases/100,000 inhabitants/year; these are similar to the rates for São Paulo determined in the present study. However, the North American prevalence rates greatly exceed the ones observed in our study, which show over 135.6 cases/100,000 inhabitants for CD and higher than the 198 cases/100,000 inhabitants for UC.18
The results of the present study show incidence rates of IBD in São Paulo comparable to European countries, such as Israel (13.2 new cases/100,000 inhabitants/year), Czech Republic (12.2 new cases/100,000 inhabitants/year), Portugal (11.1 new cases/100,000 inhabitants/year), and Ireland (13.2 new cases/100,000 inhabitants/year). The prevalence of CD was 1.5–213 cases per 100,000 inhabitants and that of UC was 2.4–294 cases per 100,000 inhabitants in these countries.19,20
There is little information on IBD epidemiology in Latin America, with data from countries such as Argentina, Uruguay, Puerto Rico, and Mexico referring to the beginning of the 21st century in particular. Those published rates are lower than those found in the present study, with incidence of UC between 2.2 and 4.3 new cases/100,000 inhabitants/year and of CD between 0.8 and 2.0 new cases/100,000 inhabitants/year.21,22 Despite the low prevalence of IBD in São Paulo, as compared to North America and Europe, the similarity of incidence rates allows us to infer that sometime in the future the prevalence data may equalize, considering the trend toward stabilization or even reduction of the incidence rates of IBD in developed countries that was demonstrated in the systematic review of Ng et al.18
The data of the present study and previous studies related to the epidemiology of IBD in Brazil are demonstrated in Table 2.
 | Table 2 Data from the present study and from the previous studies related to the IBD epidemiology in Brazil Notes: Incidence is presented as new cases per 100,000 inhabitants/year. Prevalence is presented as new cases per 100,000 inhabitants. Abbreviations: CD, Crohn’s disease; UC, ulcerative colitis. |
Regarding age, the results of the present study show an evident prevalence of IBD in individuals between 20 and 50 years. In the group of patients with UC, there was a tendency toward an increase in incidence among patients over 60 years old. Such results are indistinct from the ones obtained in other Brazilian studies, such as those by Silva and Souza et al, and international studies, such as those by Burisch and Munkholm and Chouraki et al.8,14,19,23 We admit, however, that delay in the diagnosis of IBD can influence the outcome of the incidence distribution by age groups. In a recent study undertaken in the Northeast region of Brazil, a delay of up to 28.2 months was observed between the beginning of the clinical manifestations and the diagnostic confirmation of IBD.24
The results of the present study demonstrated a greater prevalence of IBD among female participants, both for CD and UC. Similar results were observed in studies of other regions of Brazil as well as in Chile, and in the systematic review by Hovde and Moum.1,7,14,25,26 A recent Brazilian study demonstrated that males seek less health services (63.9%) than females (78%), demonstrating that cultural factors may influence this result.27
The self-reported ethnic group was also evaluated in the study population, with results showing a predominance of the ethnic group self-declared Caucasian (19%), followed by the ethnic group self-declared mixed race (0.3%), African descent (0.1%), oriental descent (0.25%), and indigenous (0.17%), and there was no statistically significant difference between CD and UC patients. These results show ethnic data comparable to those obtained in 2007 from the city of São Paulo, in the POLI study, which demonstrates a predominance of the group self-declared Caucasian (68.9%), followed by the African descent group (7.8%), mixed race (1.5%), oriental descent (1.5%), and indigenous (0.5%).28
In this study, however, 77% of the patients did not declare their ethnic background, making the ethnicity data of the present study only illustrative. The present study is the first in Brazil regarding incidence and prevalence of IBD in a large sample and represents real-life data from a regional population. According to the Cochrane Collaboration-endorsed NOS, our study can be classified as representative of the target population.11 Limitations of this study were the non-inclusion of all patients with IBD in Brazil and the lack of other clinical data, such as medications in use, and other data concerning the disease, such as disease extension and presence of complications.
Conclusion
According to the study design and applied methodology, there was a stability in IBD incidence rates and an increase in the IBD prevalence rates in São Paulo state between 2012 and 2015, with a small decrease in CD rates and an increase in UC rates according to SUS data, but with a significant increase in these rates compared to previous studies. The age groups between 20 and 60 years had the highest rates of incidence and prevalence. A higher occurrence was observed in females for both CD and UC. This study also shows that there is much to be explored in relation to the epidemiology of IBD in Brazil, and it is essential for the development of broader surveys that better define the national rates of IBD incidence and prevalence.
Disclosure
The authors report no conflicts of interest in this work.
References
Figueroa CC, Quera PR, Valenzuela EJ, Jensen BC. [Diseases intestinal inflammations: Experience of two Chilean centers] Enfermedades inflamatorias intestinales: Experiencia de dos centros chilenos. Revista médica de Chile. 2005;133(11):1295–1304. Spanish. | ||
Cardozo WS, Sobrado CW. Doença Inflamatória Intestinal. 2 ed. Barueri-SP: Manole; 2015. | ||
Barbalho SM, Goulart RA, Gasparini RG. Associations between inflammatory bowel diseases and vitamin D. Crit Rev Food Sci Nutr. 2017;13:1–10. | ||
Bernstein CN, Shanahan F. Disorders of a modern lifestyle: reconciling the epidemiology of inflammatory bowel diseases. Gut. 2008;57(9):1185–1191. | ||
Goh K, Xiao SD. Inflammatory bowel disease: a survey of the epidemiology in Asia. J Dig Dis. 2009;10(1):1–6. | ||
Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142(1):46–54.e42; quiz e30. | ||
Victoria CR, Sassak LY, Nunes HR. Incidence and prevalence rates of inflammatory bowel diseases, in midwestern of São Paulo State, Brazil. Arq Gastroenterol. 2009;46(1):20–25. | ||
da Silva BC, Lyra AC, Mendes CM. The Demographic and Clinical Characteristics of Ulcerative Colitis in a Northeast Brazilian Population. Biomed Res Int. 2015;2015:359130. | ||
Kleinubing-Júnior H, Pinho Mdesl, Ferreira LC, Bachtold GA, Merki A. [Profile of outpatients with inflammatory bowel diseases] Perfil dos pacientes ambulatoriais com doenças inflamatórias intestinais. ABCD. Arquivos Brasileiros de Cirurgia Digestiva. 2011;24(3):200–203. Portugese. | ||
Saúde OMda. [ICD-10 International Statistical Classification of Diseases and Related Health Issues] CID-10 Classificação Estatística Internacional de Doenças e Problemas Relacionados Saúde. 10a rev. São Paulo: Universidade de São Paulo; 1997. Portugese. | ||
Wells GA, Shea B, O’Connell D. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses; 2014. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. August 02, 2018. | ||
Instituto Brasileiro de Geografia e Estatística (IBGE). Censo; 2010. Available from: http://censo2010.ibge.gov.br. November 25, 2017. | ||
Fundação Sistema Estadual de Análise de Dados (SEADE). Portal de Estatísticas do Estado de São Paulo. Available from: http://www. seade.gov.br. November 25, 2017. | ||
Souza MH, Troncon LE, Rodrigues CM, et al. [Evolution of the occurrence (1980-1999) of Crohn’s disease and rectocolitis idiopathic ulcer disease and analysis of its clinical features in a university hospital in southeastern Brazil] Evolução da ocorrência (1980-1999) da doença de Crohn e da retocolite ulcerativa idiopática e análise das suas características clínicas em um hospital universitário do sudeste do Brasil. Arq Gastroenterol. 2002;39(2):98–105. Portuguese. | ||
Instituto Brasileiro de Geografia e Estatística (IBGE). 2015. Available from: http://www.ibge.gov.br. December 06, 2018. | ||
Instituto de Pesquisa Econômica Aplicada (IPEA). Available from: http://www.ipea.gov.br. December 06, 2018. | ||
Vendrell R, Venegas HL, Pérez CM, Morell C, Roman RV, Torres EA. Differences in prevalence of inflammatory bowel disease in Puerto Rico between commercial and government-sponsored managed health care insured individuals. Bol Asoc Med P R. 2013;105(2):15–19. | ||
Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2018;390(10114):2769–2778. | ||
Burisch J, Munkholm P. Inflammatory bowel disease epidemiology. Curr Opin Gastroenterol. 2013;29(4):357–362. | ||
Burisch J, Pedersen N, Cˇukovic´-Cˇavka S, et al; EpiCom-group. East-West gradient in the incidence of inflammatory bowel disease in Europe: the ECCO-EpiCom inception cohort. Gut. 2014;63(4):588–597. | ||
Farrukh A, Mayberry JF. Inflammatory bowel disease in Hispanic communities: a concerted South American approach could identify the aetiology of Crohn’s disease and ulcerative colitis. Arq Gastroenterol. 2014;51(4):271–275. | ||
Kotze PG. Research in inflammatory bowel diseases in Latin America: a challenge ahead. Arq Gastroenterol. 2014;51(4):269–270. | ||
Chouraki V, Savoye G, Dauchet L, et al. The changing pattern of Crohn’s disease incidence in northern France: a continuing increase in the 10- to 19-year-old age bracket (1988-2007). Aliment Pharmacol Ther. 2011;33(10):1133–1142. | ||
Parente JM, Coy CS, Campelo V, et al. Inflammatory bowel disease in an underdeveloped region of Northeastern Brazil. World J Gastroenterol. 2015;21(4):1197–1206. | ||
Souza MM, Belasco AGS, Aguilar-Nascimento JE. [Epidemiological profile of patients with inflammatory bowel disease of the state of Mato Grosso] Perfil epidemiológico dos pacientes portadores de doença inflamatória intestinal do estado de Mato Grosso. Rev Bras. Colo-proctol. 2008;28(3):324–328. Portuguese. | ||
Hovde Ø, Moum BA. Epidemiology and clinical course of Crohn’s disease: results from observational studies. World J Gastroenterol. 2012;18(15):1723–1731. | ||
Gomes R, Nascimento EF, Araújo FC. [Why do men use health services less than women? Explanations by men with low versus higher education]. Por que os homens usam os serviços de saúde? menos que as mulheres? Explicações de homens com baixa versus alta escolaridade. Cad. Saúde Pública. 2007;23(3):565–574. Portuguese. | ||
Poli DD. Impacto da ancestralidade na apresentação e evolução da doença de Crohn no Brasil. São PauloUniversidade de São Paulo: Faculdade de medicina; 2007. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.