Back to Journals » Journal of Inflammation Research » Volume 18
Inflammation Promotes Insulin Resistance: Analysis Based on Inflammation Indices Obtained from the Complete Blood Count
Authors Zhang X, Wei Y, Wang Y, Wang G ![]() , Liu J
, Liu J ![]()
Received 18 June 2025
Accepted for publication 7 November 2025
Published 18 November 2025 Volume 2025:18 Pages 16065—16077
DOI https://doi.org/10.2147/JIR.S547916
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Quan Zhang
Xinzhong Zhang,1,* Ying Wei,1,* Ying Wang,2 Guang Wang,1 Jia Liu1
1Department of Endocrinology, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China; 2Health Management Center, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guang Wang, Department of Endocrinology, Beijing Chao-yang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China, Email [email protected] Jia Liu, Department of Endocrinology, Beijing Chao-yang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China, Email [email protected]
Purpose: Systemic inflammation indices, including the aggregate index of systemic inflammation (AISI), monocyte-to-lymphocyte ratio (MLR), neutrophil-to-lymphocyte ratio (NLR), neutrophil-to-platelet ratio (NPR), systemic immune-inflammation index (SII) and systemic inflammation response index (SIRI) may contribute to the development of metabolic disorders. This study aimed to examine their associations with adipose tissue insulin resistance (Adipo-IR) and the homeostasis model assessment of insulin resistance (HOMA-IR).
Patients and Methods: This cross-sectional study included 11416 participants recruited at Beijing Chaoyang Hospital. Multiple linear and logistic regression models were used to assess associations between six inflammatory indices and both Adipo-IR and HOMA-IR. Subgroup analyses were performed based on age, sex and BMI to evaluate potential effect modification.
Results: All six inflammation indices were significantly associated with Adipo-IR, with higher levels conferring increased risk of high Adipo-IR after adjustment for confounding factors. Similar trends were observed for the association of AISI, NLR, NPR, SII, SIRI and HOMA-IR, whereas MLR showed no significant association. Subgroup analyses indicated that NLR and SII were more strongly associated with high Adipo-IR in women, and that SII was more strongly associated with both high Adipo-IR and HOMA-IR in participants aged 18– 44 years.
Conclusion: Elevated systemic inflammation indices were positively associated with both Adipo-IR and HOMA-IR. These findings suggest that routine blood count-derived indices may serve as cost-effective indicators of early metabolic dysfunction.
Keywords: adipose tissue, inflammatory, insulin resistance, CBC inflammatory marker
Introduction
Insulin resistance (IR) is a central pathological mechanism of type 2 diabetes mellitus (T2DM). Adipose tissue insulin resistance (Adipo-IR), defined as impaired insulin sensitivity within adipose tissue, is considered an early driver of systemic IR.1 Chronic inflammation in adipocytes triggers excessive release of free fatty acids (FFAs) into the circulation through activation of lipolysis and impairment of lipid storage, thereby inducing lipotoxicity, ectopic fat deposition and disruption of insulin signaling pathways.2 This mechanism establishes a critical link between adipose tissue dysfunction and systemic metabolic disturbances.
Adipo-IR has been implicated in the development of non-alcoholic fatty liver disease (NAFLD), dyslipidemia and glucose intolerance.3–5 In addition, our previous studies identified significant associations between Adipo-IR and hyperuricemia, glycemic abnormalities and thyroid hormone sensitivity, highlighting its pivotal role in metabolic dysfunction.6–8
Inflammation is increasingly recognized as a critical mediator of metabolic disease.9 In obesity, adipocyte hypertrophy promotes chemokine release and macrophage recruitment.10 Under chronic metabolic stress, macrophages shift toward the pro-inflammatory M1 phenotype, which secretes cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin-1β (IL-1β). These cytokines impair insulin signaling, aggravate Adipo-IR and contribute to systemic IR.11
In recent years, systemic inflammatory indices derived from complete blood count (CBC) have attracted increasing attention, such as the aggregate index of systemic inflammation (AISI), monocyte-to-lymphocyte ratio (MLR), neutrophil-to-lymphocyte ratio (NLR), neutrophil-to-platelet ratio (NPR), systemic immune-inflammation index (SII) and systemic inflammation response index (SIRI). Previous studies have reported positive associations of these indices with diabetes, cardiovascular diseases, cancers and autoimmune disorders.12–16 However, although inflammation is known to play a critical role in metabolic disease, the relationships between these indices and Adipo-IR remain unclear.
Therefore, this study aimed to evaluate whether CBC-derived inflammatory indices are independently associated with insulin resistance, including Adipo-IR and the homeostasis model assessment of insulin resistance (HOMA-IR).
Materials and Methods
Study Population
Participants were selected according to predefined inclusion and exclusion criteria. The inclusion criteria were: (1) participants who underwent physical examinations at Beijing Chaoyang Hospital between April 2017 and April 2023, and (2) age ≥ 18 years. The exclusion criteria were: (1) missing data on complete blood count (n = 8); (2) missing data on fasting blood insulin, FFA or plasma glucose (FPG) (n = 3); (3) history of diabetes (n = 1165); (4) severe renal dysfunction, defined as an estimated glomerular filtration rate (eGFR) < 60 mL/min/1.73m2 (n = 207); (5) severe liver dysfunction, defined as alanine transaminase (ALT) or aspartate transaminase (AST) levels exceeding three times the upper limit of normal (n = 45); and (6) presence of infection (n = 1144). Finally, a total of 11416 participants were included in the analysis. Based on prior research of 779 participants that examined the association between inflammation indices and IR, the sample size of 11416 in this study was considered sufficient to provide adequate statistical power.17 This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Beijing Chaoyang Hospital. All participants provided written informed consent.
Measurements of Clinical Parameters
Basic demographic and clinical data were collected for all participants and systematically recorded by qualified physicians, including sex, age, height, weight, systolic blood pressure, and diastolic blood pressure. All participants fasted for at least 8 hours before blood collection, which was conducted in the clinical laboratory at Beijing Chaoyang Hospital following standard procedures. Serum creatinine, total cholesterol (TC), triglyceride (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), ALT, AST, serum uric acid, FPG, glycated hemoglobin (HbA1c), fasting insulin and FFA levels were measured using an automatic analyzer (Advia 2400, Siemens Healthcare Diagnostics Inc., Tarrytown, New York, USA).
Variables and Definitions
Body mass index (BMI) was calculated as weight (kg) divided by the square of height (m2). Hypertension was diagnosed as systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg on two separate measurements, or current use of antihypertensive medication. Dyslipidemia was defined as TC ≥5.2 mmol/L, or TG ≥1.7 mmol/L, or LDL-C ≥3.4 mmol/L, or HDL-C <1.0 mmol/L, or non-high-density lipoprotein cholesterol (non-HDL-C) ≥4.1 mmol/L.18 Diabetes was diagnosed as FPG ≥7.0 mmol/L, or HbA1c ≥6.5%, or random blood glucose ≥11.1 mmol/L with typical hyperglycemic symptoms, or use of antidiabetic medications according to the American Diabetes Association (ADA) guidelines.19 The estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.20 The Adipo-IR index was calculated as fasting insulin (mIU/L) × FFA (mmol/L). The HOMA-IR was calculated as FPG (mmol/L) × fasting insulin (mIU/L) / 22.5. IR was defined as HOMA-IR >2.6 (mmol/L × mIU/L).21 AISI was calculated as (neutrophil count (NC, × 109/L) × platelet count (PC, × 109/L) × monocyte count (MC, × 109/L)) / lymphocyte count (LC, × 109/L). MLR was calculated as MC / LC. NLR was calculated as NC / LC. NPR was calculated as NC / PC. SII was calculated as (PC × NC) / LC. SIRI was calculated as (MC × NC) / LC.
Statistical Analysis
In this study, normally distributed variables were presented as mean ± standard deviation (SD), while non-normally distributed variables were presented as median (quartiles). Categorical variables were described as frequencies (percentages).
Inflammatory indices were categorized into quartiles, with the lowest quartile (Q1) as the reference group (Supplementary Table 1). In the crude analysis, Kruskal–Wallis test was used to compare the distributions of Adipo-IR and HOMA-IR across quartiles of inflammation indices. Linear regression models were used to evaluate associations between the inflammatory indices and continuous outcomes. Participants were further classified into IR (HOMA-IR > 2.6) and non-IR (HOMA-IR ≤ 2.6) groups,21 as well as high Adipo-IR (> 4.023) and low Adipo-IR (≤ 4.023) groups based on the median value, and logistic regression models were used to assess associations with binary outcomes. Three models were constructed, with Model 1 being unadjusted, Model 2 adjusted for age and sex, and Model 3 further adjusted for BMI, hypertension, hyperlipidemia, serum uric acid and eGFR. The variance inflation factor (VIF) was used to test multicollinearity and all covariates had VIF values <3. Non-normally distributed continuous variables (AISI, MLR, NLR, NPR, SII, SIRI, Adipo-IR and HOMA-IR) were log-transformed when they were put in regression models and when they were considered continuous for analysis. Subgroup analyses were performed stratified by age, sex and BMI. Interaction terms between the inflammation index and these modifiers were included in the regression models to test for an interaction effect. All analyses were two-tailed, with a P-value of < 0.05 considered statistically significant. Data analyses were performed using R software (version 4.4.2) and GraphPad Prism software (version 10.4.0).
Results
Baseline Information
A total of 11416 participants were included, comprising 5770 women (50.5%) and 5646 men (49.5%). The median age was 41 years, and the median BMI was 23.73 kg/m2. Compared with women, men had higher prevalences of hypertension (18.3% vs 10.5%) and hyperlipidemia (65.78% vs 46.15%), as well as higher levels of BMI, uric acid, FPG, fasting insulin and HOMA-IR. Adipo-IR levels were similar between men and women. For inflammatory indices, men had higher levels of AISI, MLR, NPR and SIRI, and lower levels of SII and NLR than women. The baseline information was shown in Table 1.
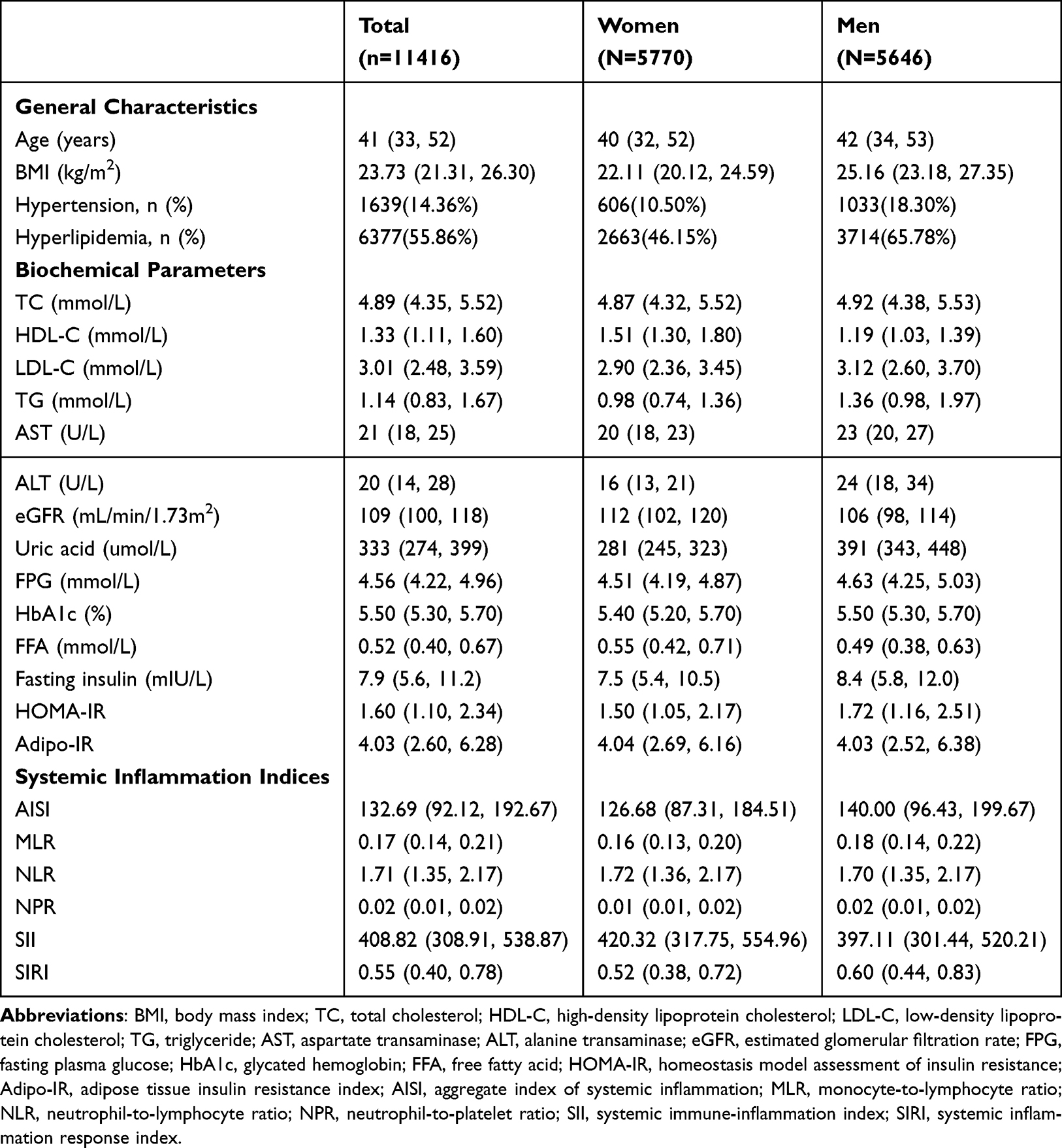 |
Table 1 Baseline Information of the Total Subjects |
Association Between Six Inflammation Indices and Insulin Resistance by Linear Regression
As shown in Figures 1 and 2, Adipo-IR and HOMA-IR increased progressively across quartiles of all six inflammation indices, except for MLR, which showed no significant association with HOMA-IR (P = 0.144). In linear regression analyses, after adjusting for age, sex, BMI, hypertension, hyperlipidemia, eGFR and uric acid, all six inflammatory indices were significantly associated with Adipo-IR (Table 2). Specifically, each unit increase in log AISI, log MLR, log NLR, log NPR, log SII and log SIRI was associated with 1.135 (e0.127 = 1.135), 1.052 (e0.051 = 1.052), 1.151 (e0.141 = 1.151), 1.242 (e0.217 = 1.242), 1.154 (e0.143 = 1.154) and 1.141 (e0.132 = 1.141) units increased in Adipo-IR after full adjustment, respectively. Consistently, quartile analyses revealed a graded positive association. Participants in the highest quartile of AISI, MLR, NLR, NPR, SII and SIRI had 1.206 (e0.187 = 1.206), 1.041 (e0.04 = 1.041), 1.128 (e0.12 = 1.128), 1.195 (e0.178 = 1.195), 1.172 (e0.159 = 1.172) and 1.188 (e0.172 = 1.188) higher levels of Adipo-IR, respectively, compared with those in the lowest quartile.
 |
Table 2 Multiple Linear Regression Between Six Inflammation Indices and Adipo-IR |
 |
Figure 1 Adipo-IR levels across quartiles of six inflammation indices (A) AISI, (B) MLR, (C) NLR, (D) NPR, (E) SII, (F) SIRI. Abbreviations: AISI, aggregate index of systemic inflammation; MLR, monocyte-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio; NPR, neutrophil-to-platelet ratio; SII, systemic immune-inflammation index; SIRI, systemic inflammation response index; Adipo-IR, adipose tissue insulin resistance index; Q1, the first quartile, Q2, the second quartile, Q3, the third quartile, Q4, the fourth quartile. Notes: Adipo-IR were presented as median with 95% confidence intervals and compared across quartiles using the Kruskal–Wallis test. |
 |
Figure 2 HOMA-IR levels across quartiles of six inflammation indices (A) AISI, (B) MLR, (C) NLR, (D) NPR, (E) SII, (F) SIRI. Abbreviations: AISI, aggregate index of systemic inflammation; MLR, monocyte-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio; NPR, neutrophil-to-platelet ratio; SII, systemic immune-inflammation index; SIRI, systemic inflammation response index; Q1, the first quartile, Q2, the second quartile, Q3, the third quartile, Q4, the fourth quartile. Notes: HOMA-IR were presented as median with 95% confidence intervals and compared across quartiles using the Kruskal–Wallis test. |
For HOMA-IR, similar associations were observed (Supplementary Table 2). Each unit increase in log AISI, log NLR, log NPR, log SII and log SIRI was associated with 1.066 (e0.064 = 1.066), 1.059 (e0.057 = 1.059), 1.137 (e0.128 = 1.137), 1.065 (e0.063 = 1.065) and 1.068 (e0.066 = 1.068) units increased in HOMA-IR after full adjustment, respectively. In the quartile analysis, participants in the highest quartile of AISI, NLR, NPR, SII and SIRI had 1.101 (e0.096 = 1.101), 1.048 (e0.047 = 1.048), 1.113 (e0.107 = 1.113), 1.069 (e0.067 = 1.069) and 1.099 (e0.094 = 1.099) higher levels of HOMA-IR, respectively, compared with those in the lowest quartile. In contrast, MLR showed no significant association with HOMA-IR.
Association Between Six Inflammation Indices and Insulin Resistance by Logistic Regression
Participants were divided into IR (HOMA-IR > 2.6) and non-IR (HOMA-IR ≤ 2.6) groups, and into low (≤ 4.023) and high (> 4.023) Adipo-IR groups.
As shown in Table 3, after full adjustment, each unit increase in log AISI, log MLR, log NLR, log NPR, log SII and log SIRI was associated with 50.1% (OR = 1.501, 95% CI: 1.394–1.616), 23.9% (OR = 1.239, 95% CI: 1.096–1.401), 54.3% (OR = 1.543, 95% CI: 1.380–1.724), 89.6% (OR = 1.896, 95% CI: 1.665–2.160), 55.7% (OR = 1.557, 95% CI: 1.412–1.718) and 52.7% (OR = 1.527, 95% CI: 1.407–1.658) higher risk of high Adipo-IR, respectively. A similar pattern was observed in the quartile analyses. Compared with participants in the lowest quartile, those in the highest quartile of AISI, MLR, NLR, NPR, SII and SIRI had 77% (OR = 1.77, 95% CI: 1.578–1.985), 16.1% (OR = 1.161, 95% CI: 1.035–1.302), 44.4% (OR = 1.444, 95% CI: 1.289–1.618), 70.9% (OR = 1.709, 95% CI: 1.520–1.921), 64.3% (OR = 1.643, 95% CI: 1.466–1.842) and 72.4% (OR = 1.724, 95% CI: 1.536–1.934) higher risk, respectively.
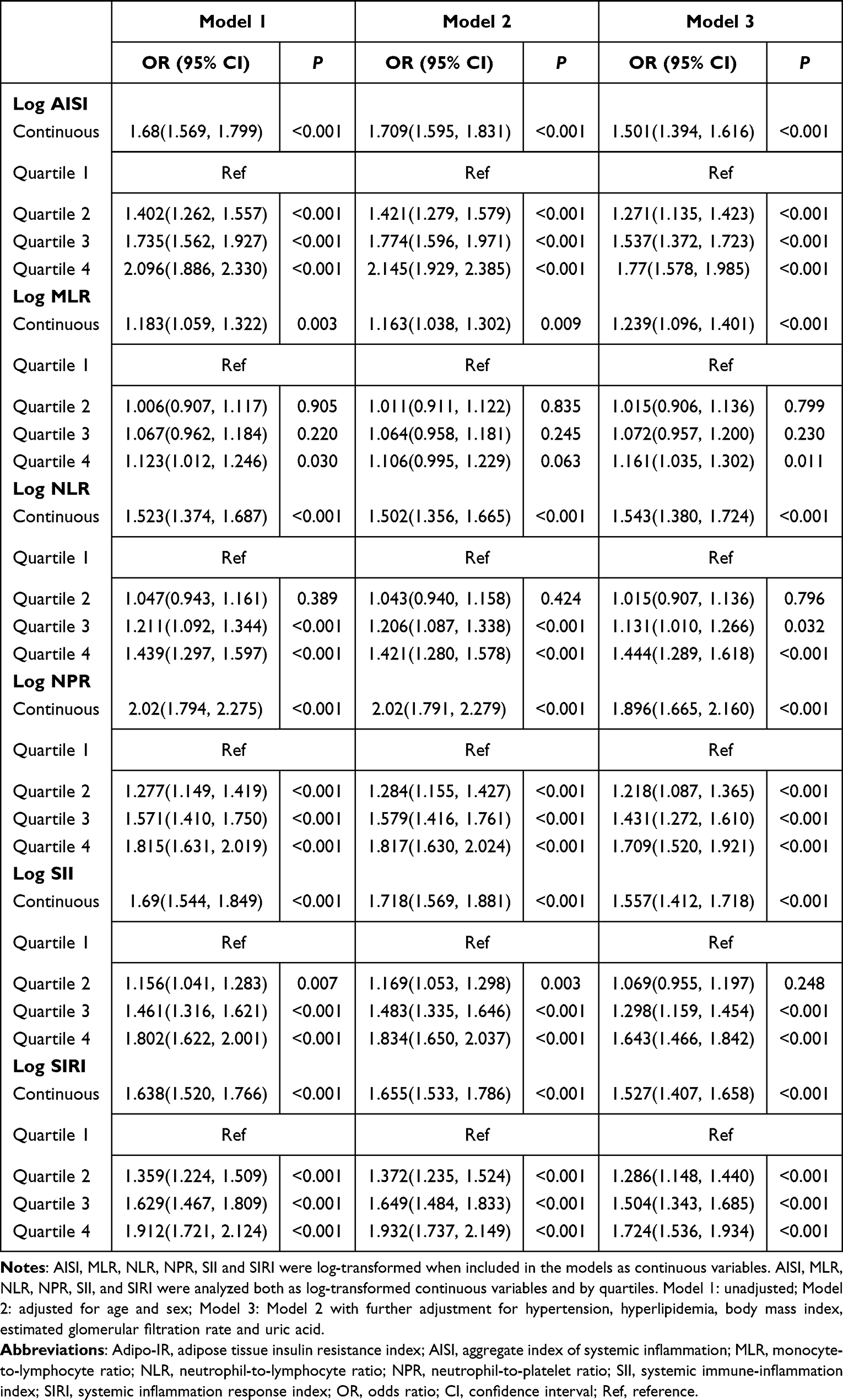 |
Table 3 Multiple Logistic Regression Between Six Inflammation Indices and Adipo-IR |
For HOMA-IR (Supplementary Table 3), after full adjustment, each unit increased in log AISI, log NLR, log NPR, log SII and log SIRI was associated with 30.6% (OR = 1.306, 95% CI: 1.186–1.438), 24.2% (OR = 1.242, 95% CI: 1.073–1.436), 70.2% (OR = 1.702, 95% CI: 1.435–2.018), 27.2% (OR = 1.272, 95% CI: 1.119–1.445) and 32% (OR = 1.320, 95% CI: 1.186–1.469) higher risk of IR, respectively. In the quartile analyses, participants in the highest quartile of AISI, NPR, SII and SIRI had 49.1% (OR = 1.491, 95% CI: 1.281–1.735), 52.9% (OR = 1.529, 95% CI: 1.308–1.788), 21.1% (OR = 1.211, 95% CI: 1.045–1.403) and 47.9% (OR = 1.479, 95% CI: 1.272–1.721) higher risk compared with those in the lowest quartile. MLR showed no significant association with IR in either continuous or quartile.
Subgroup Analysis
Subgroup analyses stratified by sex, age, and BMI were conducted to assess potential effect modification. As shown in Figure 3, age significantly modified the association between log SII and the risk of high Adipo-IR (P for interaction = 0.012). Specially, each unit increase in log SII was associated with a higher risk of high Adipo-IR in participants aged 18–44 years (OR = 1.705, 95% CI: 1.490–1.953) compared with those aged ≥45 years (OR = 1.401, 95% CI: 1.213–1.618). Sex significantly modified the associations of log NLR and log SII with high Adipo-IR (P for interaction = 0.027 and 0.01, respectively). In women, the ORs for each unit increase in log NLR and log SII were 1.733 (95% CI: 1.485–2.024) and 1.758 (95% CI: 1.534–2.015), compared with 1.325 (95% CI: 1.126–1.560) and 1.335 (95% CI: 1.175–1.563) in men.
 |
Figure 3 Subgroup analyses for the association between six inflammation indices and the risk of high Adipo-IR (A) Log AISI, (B) Log MLR, (C) Log NLR, (D) Log NPR, (E) Log SII, (F) Log SIRI. Abbreviations: Adipo-IR, adipose tissue insulin resistance index; AISI, aggregate index of systemic inflammation; MLR, monocyte-to-lymphocyte ratio; NLR, neutrophil-to-lymphocyte ratio; NPR, neutrophil-to-platelet ratio; SII, systemic immune-inflammation index; SIRI, systemic inflammation response index; OR, odds ratio; CI, confidence interval. Notes: AISI, MLR, NLR, NPR, SII and SIRI were log-transformed when included in the models as continuous variables. |
For IR as shown in Supplementary Figure 1, age also modified the association between log SII and the risk of IR (P for interaction = 0.018). The association was strongest in participants aged 18–44 years (OR = 1.417, 95% CI: 1.176–1.707), whereas no significant association was observed in those aged ≥45 years.
Discussion
This study was the first to comprehensively evaluate six CBC-derived inflammation indices (AISI, MLR, NLR, NPR, SII and SIRI) in relation to both HOMA-IR and Adipo-IR in a large Chinese adult population. All six indices were positively associated with Adipo-IR after full adjustment, and AISI, NPR, SII and SIRI were also significantly associated with HOMA-IR. Subgroup analyses revealed that the association of SII with high Adipo-IR and HOMA-IR was more pronounced among younger participants aged 18–44 years compared with older participants. Additionally, NLR and SII were more strongly associated with high Adipo-IR in women than in men. These findings indicated age-related and sex-related differences in the inflammatory regulation of insulin resistance.
The link between inflammation and insulin resistance has been extensively investigated. In adipose tissue, pro-inflammatory M1 macrophages secrete chemokines that recruit monocytes and lymphocytes, thereby amplifying local inflammation and worsening insulin resistance.11 Elevated platelet counts have also been implicated in promoting inflammatory responses and are associated with insulin resistance.22,23 Consistent with these mechanisms, we found that all six inflammatory indices from routine blood count were significantly associated with Adipo-IR. Our previous studies also identified similar associations between Adipo-IR and endocrine-related markers, such as thyroid hormone sensitivity indices and growth hormone, with effect sizes comparable to those of the inflammatory indices.7,24 Clinically, elevated Adipo-IR has been associated with various adverse metabolic outcomes. Prior studies have shown that individuals in the highest tertile of Adipo-IR had a 324% higher risk of diabetes in overweight or obese women and a 176% higher risk of metabolic syndrome, as well as an increased risk of hyperuricemia, by 253% in men and 102% in women, compared to those in the lowest tertile.1,25,26 In individuals with hyperlipidemia, each unit increase in log Adipo-IR was linked to a 385% greater risk of NAFLD in women and a 216% increase in men.6 Moreover, Adipo-IR demonstrated a stronger correlation with liver fibrosis than BMI or hepatic steatosis.4 These findings underscore the clinical utility of Adipo-IR as a sensitive marker for metabolic dysfunction.
HOMA-IR, a sensitive indicator of insulin resistance, was significantly associated with AISI, NPR, SII and SIRI, consistent with previous findings. A cross-sectional study in a Chinese population identified SII and SIRI as independent risk factors for insulin resistance.17 Similarly, analyses based on NHANES data reported that SII increased the risk of T2DM by approximately 4% and insulin resistance by about 5%, particularly in women and younger individuals,27 consistent with our subgroup analyses. Inflammatory indices have also been linked to diabetic complications. For example, NLR has been associated with proteinuria and eGFR decline in diabetic nephropathy,28 while SIRI has been strongly correlated with diabetic macular edema.29 Although MLR was not significantly associated with HOMA-IR in our study, previous reports suggest its involvement in complications such as diabetic nephropathy and retinopathy.30,31
It is important to note that insulin resistance can also promote inflammation. Insulin resistance can promote inflammatory pathways by impairing glucose uptake in immune cells, thereby shifting their metabolism toward fatty acid oxidation and fostering a pro-inflammatory state.32 Hyperinsulinemia may also dysregulate immune cell function, contributing to further metabolic and immune dysfunction.33 These reciprocal mechanisms highlight the complex interplay between metabolic and inflammatory processes. However, given our cross-sectional study design, causality cannot be established, and longitudinal or interventional studies are needed to further clarify these relationships.
Our study further found that the associations of log SII with high Adipo-IR and HOMA-IR were stronger in individuals aged 18–44 years, consistent with the findings of Guo et al and Zhao et al27,34 One possible explanation is that younger participants in our cohort had higher lymphocyte counts (1.98×109/L vs 1.87×109/L, P<0.001), which may reflect a more responsive immune system and greater capacity for inflammation resolution.27 In contrast, aging is associated with declines in immune function and structural changes in adipose tissue, potentially weakening the link between inflammation and insulin resistance.35 We also observed that the associations of log SII and log NLR with high Adipo-IR were stronger in women than in men. It may be related to sex-specific differences in fat distribution and hormonal regulation, rendering female adipose tissue more vulnerable to inflammatory stress.36–38 However, these remain hypotheses, and the underlying mechanisms for these differences require further investigation.
This study provides novel evidence identifying CBC-based indices as potential surrogate markers of Adipo-IR in a large general population. As these indices are derived from routine complete blood counts, they are inexpensive, widely available, and easily implementable in clinical and primary care settings, which may facilitate early detection of insulin resistance and support timely lifestyle or therapeutic interventions. Furthermore, they may serve as practical tools for longitudinal monitoring and follow-up. Further studies are warranted to assess their predictive performance, determine optimal cutoff values and explore their integration into clinical risk stratification models.
Several limitations should be noted. First, we lacked data on some potential confounders, including diet, physical activity and socioeconomic status. Second, our study population was recruited from a single center, which may limit the external validity and generalizability to other populations. Third, the cross-sectional study design limited the capacity to explore causal relationships. Fourth, we did not have data on circulating inflammatory cytokines, such as interleukin-6 and TNF-α, that could have helped us to better understand the role of systemic inflammation in insulin resistance. Fifth, we had no information on the use of medications, such as statins and NSAIDs, which may influence inflammation and insulin resistance. Future large-scale prospective studies are needed to confirm these findings.
Conclusion
In summary, this large cross-sectional study demonstrates a positive association between several systemic inflammation indices and markers of insulin resistance, including Adipo-IR and HOMA-IR. These findings suggest that routine blood count-derived indices may hold potential as cost-effective indicators of early metabolic dysfunction. However, due to the study’s observational nature, further prospective and interventional studies are needed to confirm causality and to evaluate their clinical utility in screening or risk stratification.
Data Sharing Statement
Some or all datasets generated during and/or analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request (Guang Wang: [email protected]).
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of Beijing Chaoyang Hospital. All participants provided written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Key R&D Program of China (2022YFA0806400), the National Natural Science Foundation of China (82470889) and the Beijing Hospitals Authority’s Ascent Plan (DFL20220302).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang K, Pan H, Wang L, Yang H, Zhu H, Gong F. Adipose tissue insulin resistance is closely associated with metabolic syndrome in Northern Chinese Populations. Diabetes Metab Syndr Obes. 2021;14:1117–1128. doi:10.2147/dmso.S291350
2. Sancar G, Birkenfeld AL. The role of adipose tissue dysfunction in hepatic insulin resistance and T2D. J Endocrinol. 2024;262(3). doi:10.1530/joe-24-0115
3. Rosso C, Kazankov K, Younes R, et al. Crosstalk between adipose tissue insulin resistance and liver macrophages in non-alcoholic fatty liver disease. J Hepatol. 2019;71(5):1012–1021. doi:10.1016/j.jhep.2019.06.031
4. Kalavalapalli S, Leiva EG, Lomonaco R, et al. Adipose tissue insulin resistance predicts the severity of liver fibrosis in patients with type 2 diabetes and NAFLD. J Clin Endocrinol Metab. 2023;108(5):1192–1201. doi:10.1210/clinem/dgac660
5. Kerr AG, Andersson DP, Dahlman I, Rydén M, Arner P. Adipose insulin resistance associates with dyslipidemia independent of liver resistance and involves early hormone signaling. Arterioscler Thromb Vasc Biol. 2023;43(6):1054–1065. doi:10.1161/atvbaha.123.319227
6. Wei Y, Liu J, Wang G, Wang Y. Sex differences in the association between adipose insulin resistance and non-alcoholic fatty liver disease in Chinese adults. Biol Sex Differ. 2023;14(1):69. doi:10.1186/s13293-023-00549-0
7. Wei Y, Li X, Cui R, Liu J, Wang G. Associations between sensitivity to thyroid hormones and insulin resistance in euthyroid adults with obesity. Front Endocrinol. 2024;15:1366830. doi:10.3389/fendo.2024.1366830
8. Lu Y, Wang J, An Y, et al. Impaired sensitivity to thyroid hormones is associated with hyperuricemia in a Chinese euthyroid population. Front Endocrinol. 2023;14:1132543. doi:10.3389/fendo.2023.1132543
9. Hotamisligil GS. Inflammation and metabolic disorders. Nature. 2006;444(7121):860–867. doi:10.1038/nature05485
10. van Baak MA, Mariman ECM. Obesity-induced and weight-loss-induced physiological factors affecting weight regain. Nat Rev Endocrinol. 2023;19(11):655–670. doi:10.1038/s41574-023-00887-4
11. Xu H, Barnes GT, Yang Q, et al. Chronic inflammation in fat plays a crucial role in the development of obesity-related insulin resistance. J Clin Invest. 2003;112(12):1821–1830. doi:10.1172/jci19451
12. Nie Y, Zhou H, Wang J, Kan H. Association between systemic immune-inflammation index and diabetes: a population-based study from the NHANES. Front Endocrinol. 2023;14:1245199. doi:10.3389/fendo.2023.1245199
13. Liao M, Liu L, Bai L, et al. Correlation between novel inflammatory markers and carotid atherosclerosis: a retrospective case-control study. PLoS One. 2024;19(5):e0303869. doi:10.1371/journal.pone.0303869
14. Gong P, Liu Y, Gong Y, et al. The association of neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and lymphocyte to monocyte ratio with post-thrombolysis early neurological outcomes in patients with acute ischemic stroke. J Neuroinflammation. 2021;18(1):51. doi:10.1186/s12974-021-02090-6
15. Shen X, Xiang M, Tang J, et al. Evaluation of peripheral blood inflammation indexes as prognostic markers for colorectal cancer metastasis. Sci Rep. 2024;14(1):20489. doi:10.1038/s41598-024-68150-y
16. Yin X, Zou J, Yang J. The association between the aggregate index of systemic inflammation and risk of rheumatoid arthritis: retrospective analysis of NHANES 1999–2018. Front Med Lausanne. 2024;11:1446160. doi:10.3389/fmed.2024.1446160
17. He R, Sun H, Liu H, Li J. The relationship between novel inflammatory markers SII, SIRI, MHR, UHR and insulin resistance in patients with type 2 diabetes: based on a retrospective analysis. Front Endocrinol. 2025;16:1648823. doi:10.3389/fendo.2025.1648823
18. Joint committee for guideline revision. 2016 Chinese guidelines for the management of dyslipidemia in adults. J Geriatr Cardiol. 2018;15(1):1–29. doi:10.11909/j.issn.1671-5411.2018.01.011
19. American Diabetes Association Professional Practice Committee. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S17–s38. doi:10.2337/dc22-S002
20. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
21. Ascaso JF, Pardo S, Real JT, Lorente RI, Priego A, Carmena R. Diagnosing insulin resistance by simple quantitative methods in subjects with normal glucose metabolism. Diabetes Care. 2003;26(12):3320–3325. doi:10.2337/diacare.26.12.3320
22. Park JM, Lee JW, Shim JY, Lee YJ. Relationship between platelet count and insulin resistance in Korean adolescents: a Nationwide Population-Based Study. Metab Syndr Relat Disord. 2018;16(9):470–476. doi:10.1089/met.2018.0016
23. Lim HJ, Seo MS, Shim JY, Kim KE, Shin YH, Lee YJ. The association between platelet count and metabolic syndrome in children and adolescents. Platelets. 2015;26(8):758–763. doi:10.3109/09537104.2014.995613
24. Li X, Zhou B, Yao Y, Wang G, Meng H. Reduced growth hormone predicts worsening adipose tissue insulin resistance in adults with obesity. Obes Facts. 2023;16(4):401–410. doi:10.1159/000530734
25. Akter T, Song Z, Takada M, et al. Association of adipose tissue insulin resistance with risk of diabetes incidents in middle-aged Japanese workers according to BMI states: 17 years of follow-up of Aichi Worker’s Cohort study. J Epidemiol. 2025. doi:10.2188/jea.JE20250025
26. Sun H, Chang X, Bian N, et al. Adipose tissue insulin resistance is positively associated with serum uric acid levels and hyperuricemia in Northern Chinese Adults. Front Endocrinol. 2022;13:835154. doi:10.3389/fendo.2022.835154
27. Zhao Q, Liu X, Xu J, Rao X, Liu M. Association of systemic immunity-inflammation index with type 2 diabetes and insulin resistance in NHANES 2005–2018. Sci Rep. 2024;14(1):30133. doi:10.1038/s41598-024-79763-8
28. Li X, Wang L, Liu M, Zhou H, Xu H. Association between neutrophil-to-lymphocyte ratio and diabetic kidney disease in type 2 diabetes mellitus patients: a cross-sectional study. Front Endocrinol. 2023;14:1285509. doi:10.3389/fendo.2023.1285509
29. Gong Y, Wang L, Li Q, et al. Evaluating neutrophil-lymphocyte ratio, systemic immune-inflammation index, and systemic inflammation response index for diagnosing and predicting progression in diabetic retinopathy: a cross-sectional and longitudinal study. BMC Ophthalmol. 2025;25(1):398. doi:10.1186/s12886-025-04222-5
30. Kocak MZ, Aktas G, Duman TT, et al. Monocyte lymphocyte ratio as a predictor of diabetic kidney injury in type 2 diabetes mellitus; The MADKID Study. J Diabetes Metab Disord. 2020;19(2):997–1002. doi:10.1007/s40200-020-00595-0
31. Yue S, Zhang J, Wu J, Teng W, Liu L, Chen L. Use of the monocyte-to-lymphocyte ratio to predict diabetic retinopathy. Int J Environ Res Public Health. 2015;12(8):10009–10019. doi:10.3390/ijerph120810009
32. Zhou J, Zhang X, Ji L, Jiang G. Identification of potential biomarkers of type 2 diabetes mellitus-related immune infiltration using weighted gene coexpression network analysis. Biomed Res Int. 2022;2022:9920744. doi:10.1155/2022/9920744
33. Berbudi A, Khairani S, Tjahjadi AI. Interplay between insulin resistance and immune dysregulation in type 2 diabetes mellitus: implications for therapeutic interventions. Immunotargets Ther. 2025;14:359–382. doi:10.2147/itt.S499605
34. Guo H, Wan C, Zhu J, Jiang X, Li S. Association of systemic immune-inflammation index with insulin resistance and prediabetes: a cross-sectional study. Front Endocrinol. 2024;15:1377792. doi:10.3389/fendo.2024.1377792
35. Borgoni S, Kudryashova KS, Burka K, de Magalhães JP. Targeting immune dysfunction in aging. Ageing Res Rev. 2021;70:101410. doi:10.1016/j.arr.2021.101410
36. Goossens GH, Jocken JWE, Blaak EE. Sexual dimorphism in cardiometabolic health: the role of adipose tissue, muscle and liver. Nat Rev Endocrinol. 2021;17(1):47–66. doi:10.1038/s41574-020-00431-8
37. Park YM, Pereira RI, Erickson CB, Swibas TA, Cox-York KA, Van Pelt RE. Estradiol-mediated improvements in adipose tissue insulin sensitivity are related to the balance of adipose tissue estrogen receptor α and β in postmenopausal women. PLoS One. 2017;12(5):e0176446. doi:10.1371/journal.pone.0176446
38. Li X, Liu J, Zhou B, et al. Sex differences in the effect of testosterone on adipose tissue insulin resistance from overweight to obese adults. J Clin Endocrinol Metab. 2021;106(8):2252–2263. doi:10.1210/clinem/dgab325
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.