Back to Journals » Risk Management and Healthcare Policy » Volume 16
Infection Prevention and Control Practices and Associated Factors Among Healthcare Cleaners in Gondar City: An Analysis of a Cross-Sectional Survey in Ethiopia
Authors Tesfaye AH ![]() , Mekonnen TH
, Mekonnen TH ![]() , Desye B
, Desye B ![]() , Yenealem DG
, Yenealem DG ![]()
Received 27 April 2023
Accepted for publication 11 July 2023
Published 19 July 2023 Volume 2023:16 Pages 1317—1330
DOI https://doi.org/10.2147/RMHP.S419110
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Amensisa Hailu Tesfaye,1 Tesfaye Hambisa Mekonnen,1 Belay Desye,2 Dawit Getachew Yenealem1
1Department of Environmental and Occupational Health and Safety, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Environmental Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
Correspondence: Amensisa Hailu Tesfaye, Department of Environmental and Occupational Health and Safety, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, P.O. Box 196, Gondar, Ethiopia, Tel +251-934-803-290, Fax +251-58-114-1240, Email [email protected]
Background: Healthcare-associated infections are a global health problem and are more prevalent in developing countries such as Ethiopia, but there is a paucity of research on the infection prevention practices of cleaning staff. Therefore, this study aimed to assess infection prevention and control practices and associated factors among cleaners working in healthcare facilities in Gondar City, Ethiopia.
Methodology: A cross-sectional survey was conducted among healthcare cleaning staff from May to June 2022. A total of 428 cleaners took part in the survey. Data were collected using a semi-structured interviewer-administered questionnaire. The data were entered into EpiData version 4.6 and analyzed using Stata version 14 software. A multivariable binary logistic regression analysis was used to ascertain the significance of associations at < 0.05 p-value and the adjusted odds ratio (AOR) with a 95% confidence interval (CI).
Results: Among the 390 study participants included, 294 (75.1%) were female. Of the surveyed participants, 186 (47.7%) had good knowledge of infection prevention and control practices. This study revealed that out of the 390 healthcare cleaners, 204 (52.3%) had good infection prevention and control practices with 52.3% [95% CI (47.2, 56.4)]. Good knowledge of infection prevention and control [AOR: 1.56, 95% CI (1.03, 2.37)] and the availability of infection prevention and control guidelines in the workplace [AOR: 1.54, 95% CI (1.01, 2.33)] were significant factors associated with infection prevention and control practice.
Conclusion: The present study found that almost half of the healthcare cleaners had poor IPC practices. The finding underlines the importance of good IPC knowledge and the accessibility of IPC guidelines to improve IPC practices among healthcare cleaning staff. The findings of this study also highlight that behavioral change interventions and paying attention, particularly to nonclinical staff such as cleaners in health care settings, are critical to reducing infection in health care settings.
Keywords: healthcare-associated infection, infection prevention, healthcare cleaners, Ethiopia
Introduction
Infection prevention and control (IPC) refers to the measures, practices, protocols, and procedures that can prevent and control the risk of infection and the transmission of micro-organisms in healthcare settings.1 Infection prevention and control is a central component of safe and high-quality service delivery at the facility level.2 Evidence-based best practices for infection prevention and control guide healthcare providers to ensure safe, high-quality care for patients, visitors, healthcare workers, and the healthcare environment.3 When infection prevention and control measures are poorly implemented, the risk of acquiring infections through exposure to blood, body fluids, or contaminated materials in healthcare settings is substantial4 and has several consequences.5
Healthcare-associated infections (HCAIs) are infections that occur when a person becomes infected with a pathogen while receiving care in a healthcare setting and are the most common adverse events in global healthcare systems. They are a major cause of preventable diseases, deaths, and increase health costs.6 Many HCAIs are caused by micro-organisms present on the patient’s body (resident flora) or from transient sources such as healthcare workers’ hands, contaminated equipment, or the environment.7 The spread of these organisms usually results from breaches of core components of IPC measures, such as hand hygiene, disinfection and sterilization of instruments, and use of Personal Protective Equipment (PPE), safe disposal of wastes, sharps, and handling soiled linen as well as personal health and safety education, immunization programs, and post-exposure prophylaxis.8–11 The use of effective and low-cost IPC measures possibly reduces the burden of HCAIs by at least 30%.12 Despite the availability of these low-cost IPC strategies, compliance with standard IPC practices remains very low, especially in low- and middle-income countries.13
Globally, HCAIs affect hundreds of millions of people each year.2,14 Over 90% of these infections occur in resource-limited countries, mostly in Africa, where infections are more prevalent and adherence to standard precautions can be poor.15 In addition, 15% of healthcare wastes are considered hazardous,16 which subsequently results in adverse healthcare outcomes such as prolonged hospital stays, long-term disability, increased antimicrobial resistance, massive additional financial burden on healthcare systems, high costs to patients and their families, and unnecessary deaths.2,14,17
Coronavirus disease 2019 (COVID-19) has presented itself as a global pandemic in a short period, resulting in a rapid shift in the curve of infected patients, increasing mortality rates, a huge global economic burden, and a widespread mobilization of medical resources around the world.18 COVID is associated with diseases of varying severity.18,19 The most common modes of spread of the disease are coughing, sneezing, inhalation of droplets, and contact with the mucous membranes of the mouth, nose, and eyes.18 The Viral load is higher and persists longer in patients with severe COVID. Healthcare workers, including cleaning staff, who came into contact with infected patients rapidly became infected with COVID-19.20 Vaccines have been the foremost factor in the fight against viral diseases. However, vaccine hesitancy has been a global challenge. Reasons for vaccine hesitancy around the world range from religious concerns to associations with adverse health effects.21 Many patients experience prolonged symptoms after COVID-19 infection, which can affect their quality of life (QOL).22
Identifying risk groups and sources of infection, understanding the routes of transmission, and educating patients and staff in healthcare facilities are important in preventing HCAIs.23,24 Cleaners are the non-medical staff responsible for cleaning wards, sorting and washing linen, and disposing of waste.25 Cleaners play a critical role in IPC because they work in areas where they are in close contact with both patients and medical waste.26,27 The high burden of HCAIs is due to a lack of IPC measures, which have been neglected due to limited resources, poor sanitation, and hygiene practices.28 There is a paucity of research investigating the extent and factors influencing the practice of IPC among healthcare cleaners, particularly in developing countries like Ethiopia. A study conducted in South Asia found that out of 100 cleaners, only 68% had benefited from infection prevention and control training.29 A study conducted in Tanzania showed that the majority of cleaners (93.3%) had not received any training on infection prevention and occupational risk reduction. Due to a lack of knowledge from training, (31.9%) of cleaners improperly disposed of waste, and (7.2%) suffered needlestick injuries from needles hidden in bed linen.30
Cleaners work in areas where the transmission of infection occurs handily.31 Thus, cleaners are involved in major activities that predispose them to infections,32 and most people in jobs are often untrained, unmotivated, underpaid, and undervalued by other stakeholders in healthcare facilities.33 It is reported that IPC adherence is closely linked with support from management.34,35 To achieve a sustainable reduction in HCAIs and needlestick injuries, these marginalized workers and their contributions must be fully recognized.32 However, various multifaceted factors play a great role in achieving the goal of IPC, like level of education, knowledge of IPC, attitude towards IPC, availability of PPE and materials, human power, training towards IPC, policy, and guidelines, and essential environmental health conditions.2,36,37
It is impossible to improve the IPC of cleaners and thereby reduce HCAIs without adequate attention and assessment of the current IPC practices of cleaners. In addition, there has been no research among healthcare cleaners in Ethiopia to assess the factors that influence the practice of IPC. The assessment of factors influencing IPC practices among cleaners is crucial for developing successful strategies for implementing infection prevention programs and interventions. Therefore, this study was conducted to assess infection prevention and control practices and associated factors among healthcare cleaners in Gondar City, northwestern Ethiopia.
Materials and Methods
Study Design, Period, and Setting
An institution-based cross-sectional study was conducted from May to June 2022. The study was conducted in public and private health facilities in Gondar City. Gondar City is located in northwestern Ethiopia, at a distance of 740 kilometers from Addis Ababa, the capital of Ethiopia. The city has 12 sub-city administrations with a population of over 300,000. In the city, there are 8 public health centers, 47 private health institutions, and one public comprehensive specialized hospital. These health facilities provide preventive, curative, inpatient, and outpatient services, treatment of common psychiatric disorders, dental services, and other services to 15,000–25,000 people in rural areas and 40,000 people in urban areas.38
Study Participants
All cleaners working in public and private healthcare in Gondar City were the source population, whereas the study population consisted of all cleaners who worked in all healthcare in Gondar City during the study period.
Eligibility Criteria
Participants with at least one year of experience and who were available throughout the data collection period were eligible for the study, while those who had a critical illness or were known to be pregnant, on maternity leave, or on sabbatical leave were excluded from the study.
Sample Size Determination and Sampling Procedure
The sample size for this study is determined by using the single population proportion formula,39 considering 50% proportion of the cleaners have good infection prevention and control practices, since there is no previous related study with and 95% confidence interval and 5% margin of error. By using single proportion formula:  Where: n = initial sample size, Z = 1.96, the corresponding Z-score for the 95% CI, Proportion (P)= 50%, d = Margin of error = 5%, then
Where: n = initial sample size, Z = 1.96, the corresponding Z-score for the 95% CI, Proportion (P)= 50%, d = Margin of error = 5%, then  . After considering the 10% non-response rate the final sample size was 422. However, due to the small number of healthcare cleaners working in Gondar City, all healthcare cleaners were surveyed using a random sampling technique. During the study period, about 428 health cleaners were working in all healthcare facilities of Gondar City.
. After considering the 10% non-response rate the final sample size was 422. However, due to the small number of healthcare cleaners working in Gondar City, all healthcare cleaners were surveyed using a random sampling technique. During the study period, about 428 health cleaners were working in all healthcare facilities of Gondar City.
Data Collection Tools and Procedures
Data were collected using a semi-structured interviewer-administered questionnaire. The questionnaire was developed after reviewing relevant literature and adapting the contents to fit the context of healthcare cleaners.25,40–42 The questionnaire was divided into four domains, including socio-demographic, behavioral, and organizational factors, as well as the knowledge and practices of healthcare cleaners regarding IPC. The questionnaire was originally drafted in English and then translated into Amharic, the local language of the study area, by the authors and language experts to ensure that respondents could understand the questionnaire.
The sociodemographic domain of the questionnaire included variables such as age, sex, educational status, marital status, monthly salary, work experience, work unit/room, and hours worked per day. The behavioral and organizational domain of the questionnaire included characteristics such as substance use (alcohol drinking, cigarette smoking, and khat chewing), training regarding IPC, presence of an IPC committee, health and safety supervision, availability of IPC guidelines in the working unit/room, availability of medical examination, availability of soap and hand rub alcohol, availability of PPE, and availability of the HBV vaccine.
The third domain of the questionnaire contained questions about knowledge of IPC. In this section, the healthcare cleaner’s knowledge of IPC was assessed using 12-item questions. The questions focused on knowledge of hand hygiene, post-exposure prophylaxis, principles of cleaning, and the use of PPE/D. Each question was followed by two possible answers (ie, yes or no). The knowledge score was then calculated and dichotomized from the total score into good knowledge of IPC for ≥70% of correct responses and poor knowledge of IPC for <70% of correct responses. The fourth domain of the questionnaire included IPC practice. The IPC practice of healthcare cleaners was assessed for the components of IPC interventions using 10-item questions to determine what they do to prevent and control infection. These included maintaining hand hygiene, wearing PPE/D, disposing of waste safely, receiving hepatitis vaccinations, using the IPC guideline in the workplace, preparing disinfectant solutions within the guidelines, and tendency to report exposure to blood and other body fluids. Each question had two possible answers, yes or no. For analysis, a scoring system was used in which the respondent’s “yes” or “no” answers to the questions were assigned “1” or “0” points respectively. The cleaners’ IPC practice score was then calculated and dichotomized from the total score into good IPC practice for ≥70% correct responses and poor IPC practice for <70% correct responses. The questionnaire used in the current study has shown validity and reliability in previous studies conducted in the country.2,43
Variables of the Study and Measurement
Infection prevention and control (IPC) practice: this is the outcome variable of the study, and the IPC practice of healthcare cleaners was assessed for the components of IPC measures such as maintaining hand hygiene, use of PPE/D, hepatitis immunization, safe disposal of waste, instrument decontamination and disinfection practices, changing work clothes after work, preparation of disinfectant solutions within the guidelines, and workplace injury reporting. There were ten IPC practice questions with “yes” or “no” options. Cleaners who scored 70% or more correct responses from the total score of IPC practice questions were considered to have good practice of IPC, and poor practice of IPC for <70% correct responses.40,41
Independent variables: sociodemographic factors (age, sex, marital status, working experience, etc.), behavioral and organizational factors (substance use, training of IPC, Presence of IPC committee, health and safety supervision, availability of soap and hand rub alcohol, availability of PPE, etc.), and knowledge of IPC.
Knowledge of IPC: healthcare cleaners who scored 70% or higher on a total number of twelve knowledge-related questions about IPC were considered to have good knowledge of IPC, and cleaners who scored less than 70% correct responses were considered to have poor knowledge of IPC.40
Healthcare cleaners: ward attendants (those responsible for cleaning the interior wards) or grounds laborers (those responsible for cleaning the exterior grounds).44
Training on IPC: training provided by management to cleaners in the last 12 months on key components of IPC interventions such as hand hygiene, use of appropriate PPE, post-exposure prophylaxis (PEP), safe use of cleaning chemicals, instrument decontamination, and disinfection, healthcare waste management, safe disposal of waste, sharps and handling of soiled laundry.45
Data Quality Assurance
We recruited four final-year Environmental and Occupational Health and Safety students for data collection and one environmental health lecturer as supervisor. Two days of training were offered for data collectors and supervisors on topics related to research objectives, clarity of questions, the confidentiality of information, and consent in the study. The training was given in lecture and discussion ways. The questionnaires were pretested one week before the actual data collection period on 21 samples that were not included in the final analysis and the relevant modifications were made before the actual data collection was conducted. Problems encountered during the data collection process were resolved through on-The-spot discussions with the principal investigator, supervisor, and data collectors. The investigators double-checked the completeness and accuracy of all completed questionnaires daily.
Data Management and Statistical Analysis
The collected data were checked for completeness, entered into EpiData version 4.6, and exported to Stata version 14 software for analysis. Frequency distributions, percentages, means, and standard deviations were used for the description of the results. The multicollinearity assumption was checked using the variance inflation factor (VIF) and found to be acceptable (all variables had VIF <5 values). The reliability of the questionnaire was tested using Cronbach’s alpha (α). Accordingly, Cronbach’s alpha (α) value for the IPC practice was 0.78. Thus, Cronbach’s alpha (α) value for the IPC knowledge was 0.75. As a result, the internal consistency of the questionnaire in reproducing what had previously been measured using the instrument was considered acceptable, since Cronbach alpha values of 0.70 or higher indicate acceptable internal consistency.46 Cross-tabulation was employed to analyze the relationship between groups. Using binary logistic regression analysis, we fitted each predictor variable separately into a bivariate logistic regression model to explore associations with the dependent variable (IPC practice). Explanatory variables with p-values < 0.2 in the bivariate analysis were exported to the multivariable logistic regression model using the backward conditional variable selection method to control for the potential effects of confounders. The adjusted odds ratio (AOR) with 95% confidence intervals (CIs) and a p-value < 0.05 were applied to establish the significance of associations in the multivariable logistic regression model. The Hosmer and Lemeshow goodness-of-fit test was used to check the model fitness (P>0.05).
Results
Socio-Demographic Characteristics of Study Participants
A total of 390 cleaners participated in this study, giving a response rate of 91.12%. Regarding healthcare facilities, about two-thirds (66.9%) of cleaners worked in the hospital. Most of those surveyed, 294 (75.1%), were female. More than half, 199 (51.1%) of the participants were in the age group between 20 and 29 years old. The mean (±SD) age of the participants was 31.45 (±7.64) years. The majority of respondents, 222 (56.9%) were married. Regarding educational status, 183 (46.9%) of the cleaners had completed secondary school, 179 (45.9) had attended the primary level of education, and 28 (7.2%) could not read and write. The mean work experience (±SD) of the cleaners was 4.78 (±2.85). Regarding their working units, 178 (45.6%), 88 (22.6%), 69 (17.7%), and 55 (14.1%) were cleaning wards, laboratory, emergency, and OPD rooms respectively. Out of the total participants, 266 (68.2%) had less than 5 years of cleaning experience, and the majority 327 (83.8%) of the participants spent 8 or fewer hours at work daily (Table 1).
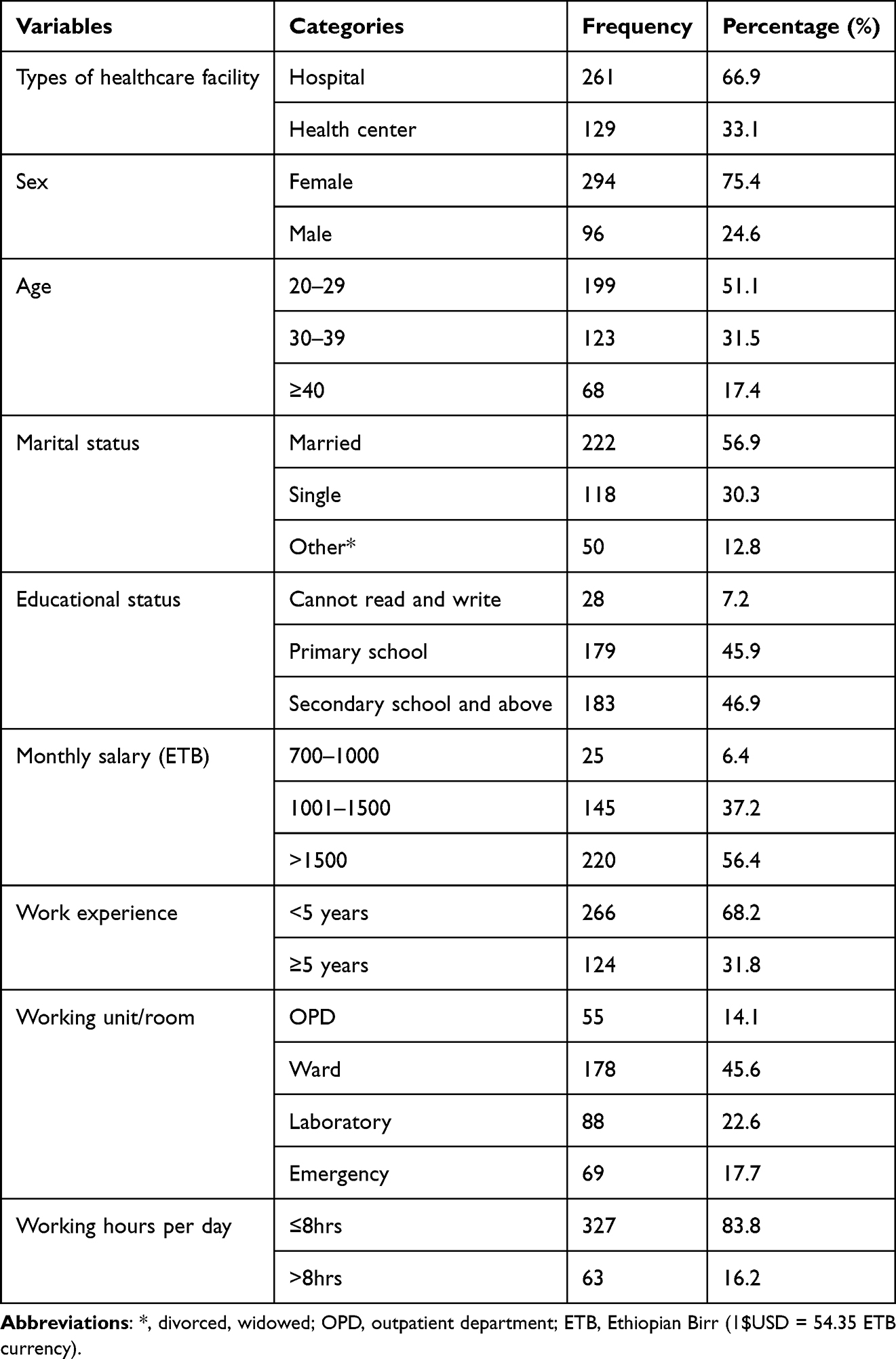 |
Table 1 Socio-Demographic Characteristics of Cleaners Working in Healthcare Facilities in Gondar City, Northwest Ethiopia, 2022 (N=390) |
Behavioral and Organizational Factors
Of the study participants, only 85 (21.80%) reported having an alcohol drinking habit. Whereas, 12 (3.1%) of the respondents had cigarette smokers, and eight (2.1%) of them described they were chewing khat. The majority, 205 (52.6%) of cleaners had taken IPC training in the last 12 months and only 45 (11.5%) of them participated in the IPC committee. Of the total study participants 247 (63.3%) of them indicated that they have regular supervision in their workplace. Nearly half, 191 (49.0%) of cleaners reported that IPC guidelines were available in their working room/department. The majority, 294 (75.4%) of cleaners stated there was adequate soap and hand rub alcohol in the working environment and above three-fourths (75.6%) of respondents answered there is also adequate PPE in the workplace (Table 2).
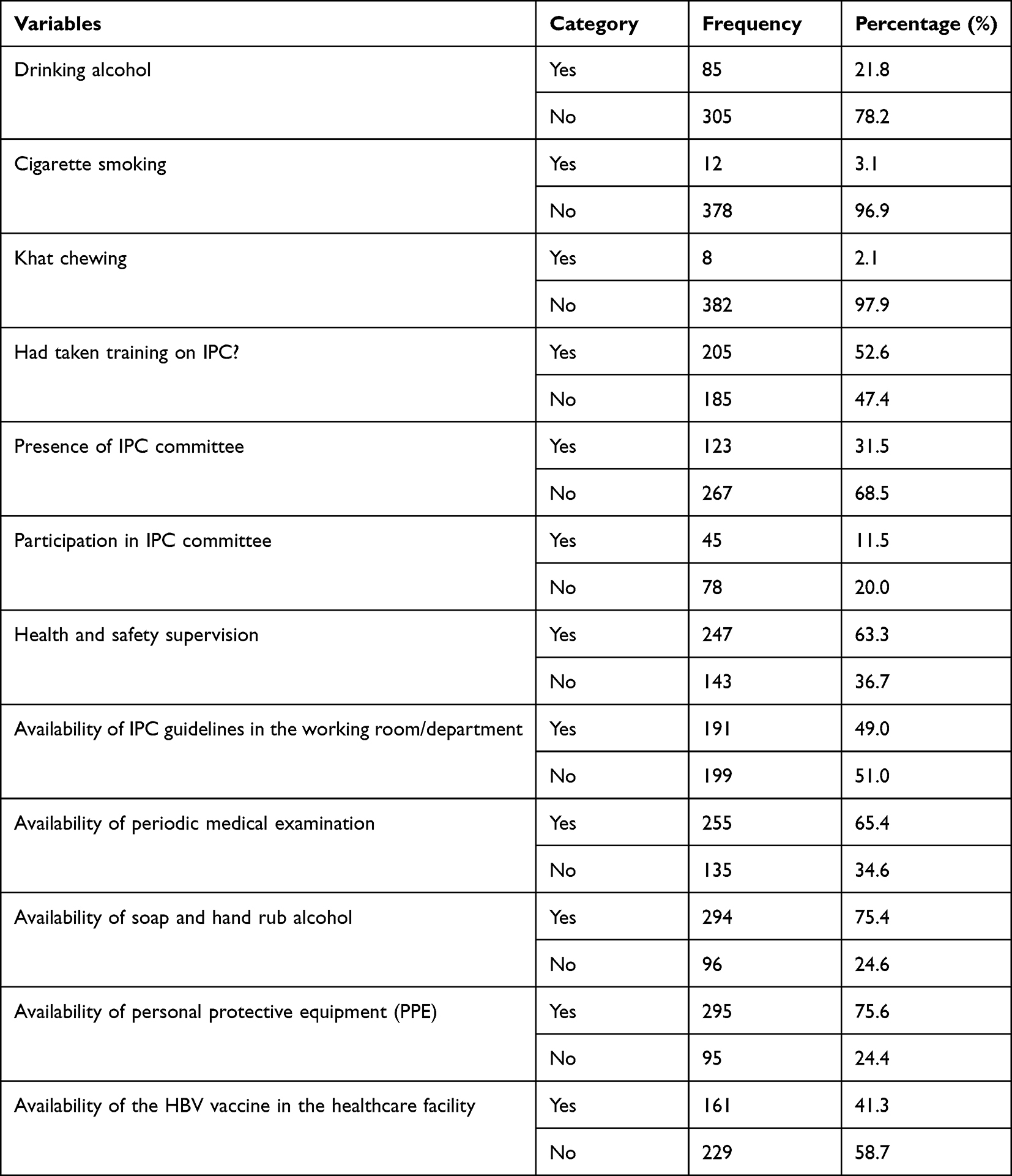 |
Table 2 Behavioral and Organizational Characteristics of Cleaners Working in Healthcare Facilities of Gondar City, Northwest Ethiopia, 2022 (N=390) |
Knowledge About Infection Prevention and Control
Overall, 186 (47.7%) of the cleaners reported good knowledge of IPC, whereas 204 (52.3%) of the respondents reported poor knowledge of IPC. Among the respondents, 274 (70.3%) of them heard about IPC principles. Among cleaners, 277 (71%) of them know the proper healthcare waste segregation system. Among the respondents, 305 (78.2%), 299 (76.7%), and 307 (78.7%) knew that disinfection, wearing PPE/D, and washing hands with soap or alcohol-based antiseptics prevent transmission of healthcare-acquired infections, respectively. Of the respondents, 246 (63.1%) knew the procedure of hand washing practice and about 312 (80%) respondents knew when to perform handwashing or critical times for washing their hands. Among 390 cleaners, only 149 (38.2%) of them knew safety boxes should be ¾ filled before closing and sealing, and merely half (51%) of cleaners knew how to prepare a 0.5% chlorine solution. The mean (±SD) score of the knowledge questions was 6.9 (±1.8) (Table 3).
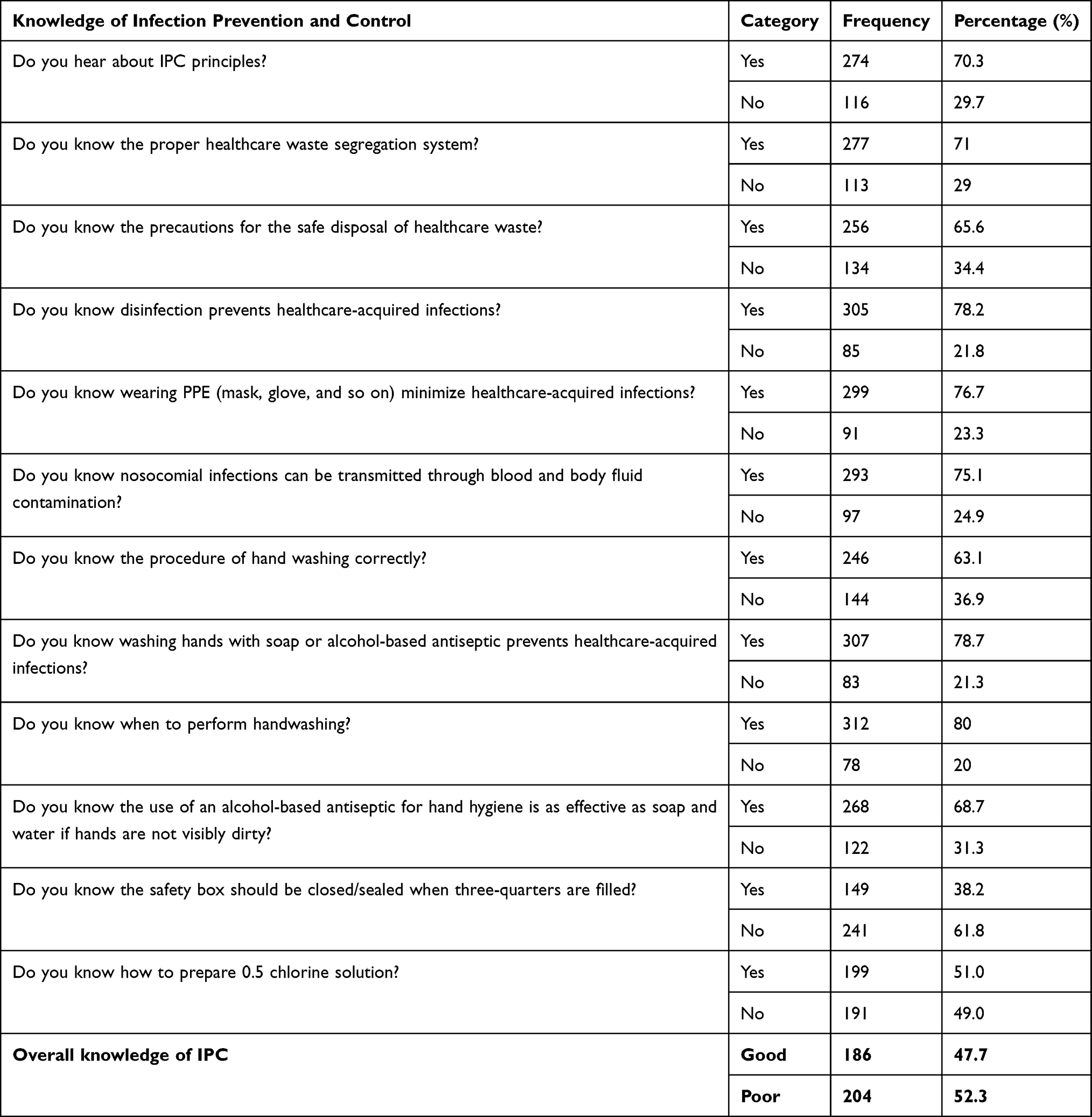 |
Table 3 Knowledge About Infection Prevention and Control Among Cleaners Working in Healthcare Facilities in Gondar City, Northwest Ethiopia, 2022 (N=390) |
Infection Prevention and Control Practice
In this study, the overall good IPC practice was found to be 52.3% [95% CI (47.2, 56.4)]. Among the study participants, 286 (73.3%) of them wash their hands with antiseptics/soap after handling medical wastes, and half (50%) of them use PPE to prevent the risk of transmission of healthcare-acquired infections. More than half, 203 (52.0%) of participants used sodium hypochlorite (Berekina) to clean the workplace. Of the total respondents, 164 (42.0%) of them used available IPC guidelines to minimize HCAIs. The majority, 325 (83.3%) of cleaners, reported a workplace injury or accidental exposure to blood and bodily fluids (Table 4).
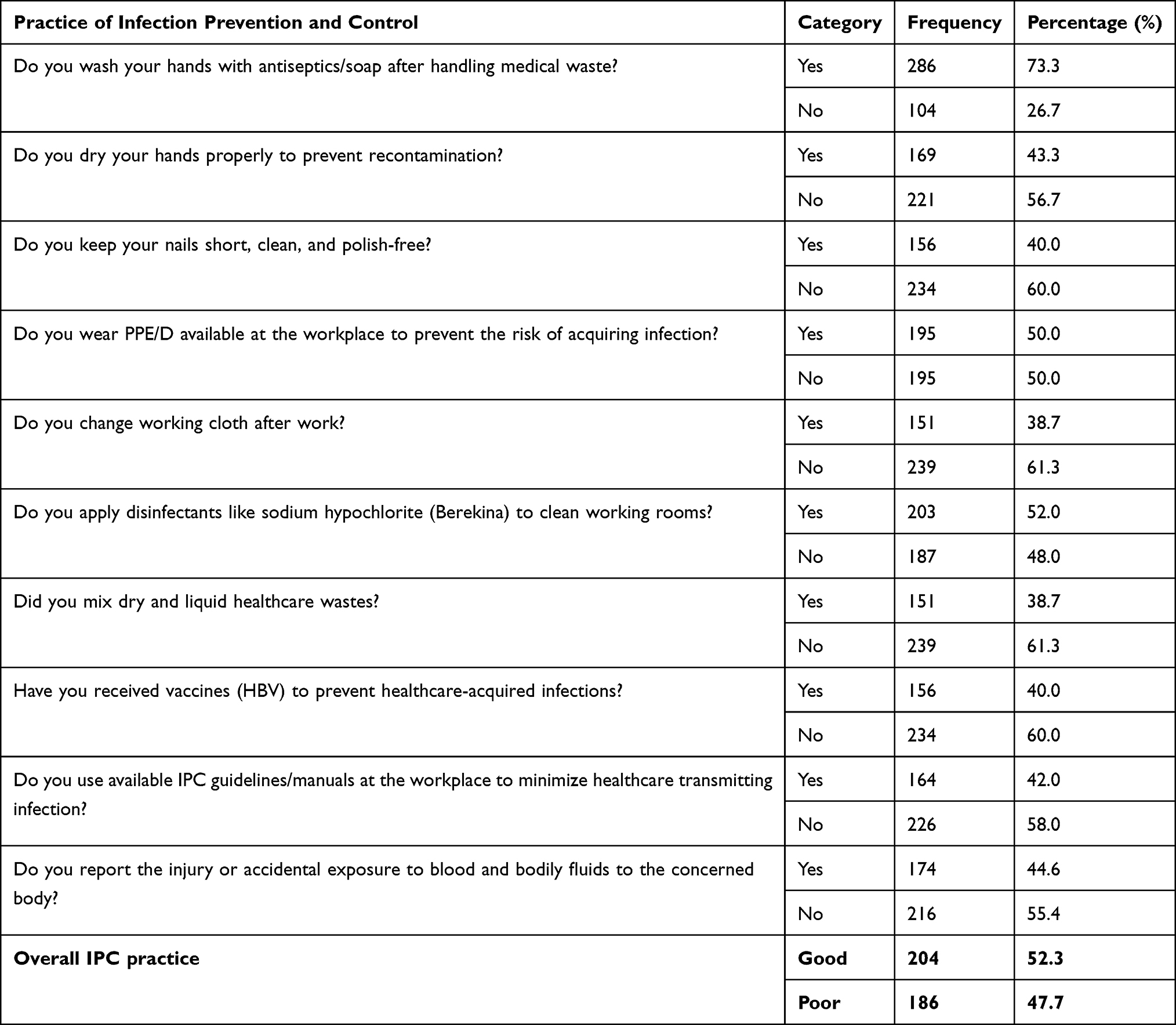 |
Table 4 Infection Prevention and Control Practice of Healthcare Cleaners Among Cleaners Working in Healthcare Facilities in Gondar City, Northwest Ethiopia, 2022 (N=390) |
Factors Associated with Infection Prevention and Control Practice
In the bivariable binary logistic regression analysis, sex, service years, availability of personal protective equipment (PPE) at the workplace, presence of the IPC committee, availability of IPC guidelines in the working room/department, and knowledge of IPC were significant factors associated with IPC practice (p-value <0.2). However, after controlling for confounding variables in the final model (multivariable binary logistic regression analysis), only knowledge of IPC and availability of IPC guidelines in the working department have been identified as independent predictors of IPC practices (p-value <0.05) among cleaners working in healthcare facilities.
Multivariable logistic regression analysis revealed that cleaners who had good knowledge of IPC were 1.56 times more likely to have good IPC practices than those who had poor knowledge of IPC [AOR = 1.56, 95% CI (1.03–2.37)]. In addition, the availability of IPC guidelines in the working departments was 1.54 times more likely to enhance the IPC practices of the cleaners [AOR = 1.54, 95% CI (1.01–2.33)] (Table 5).
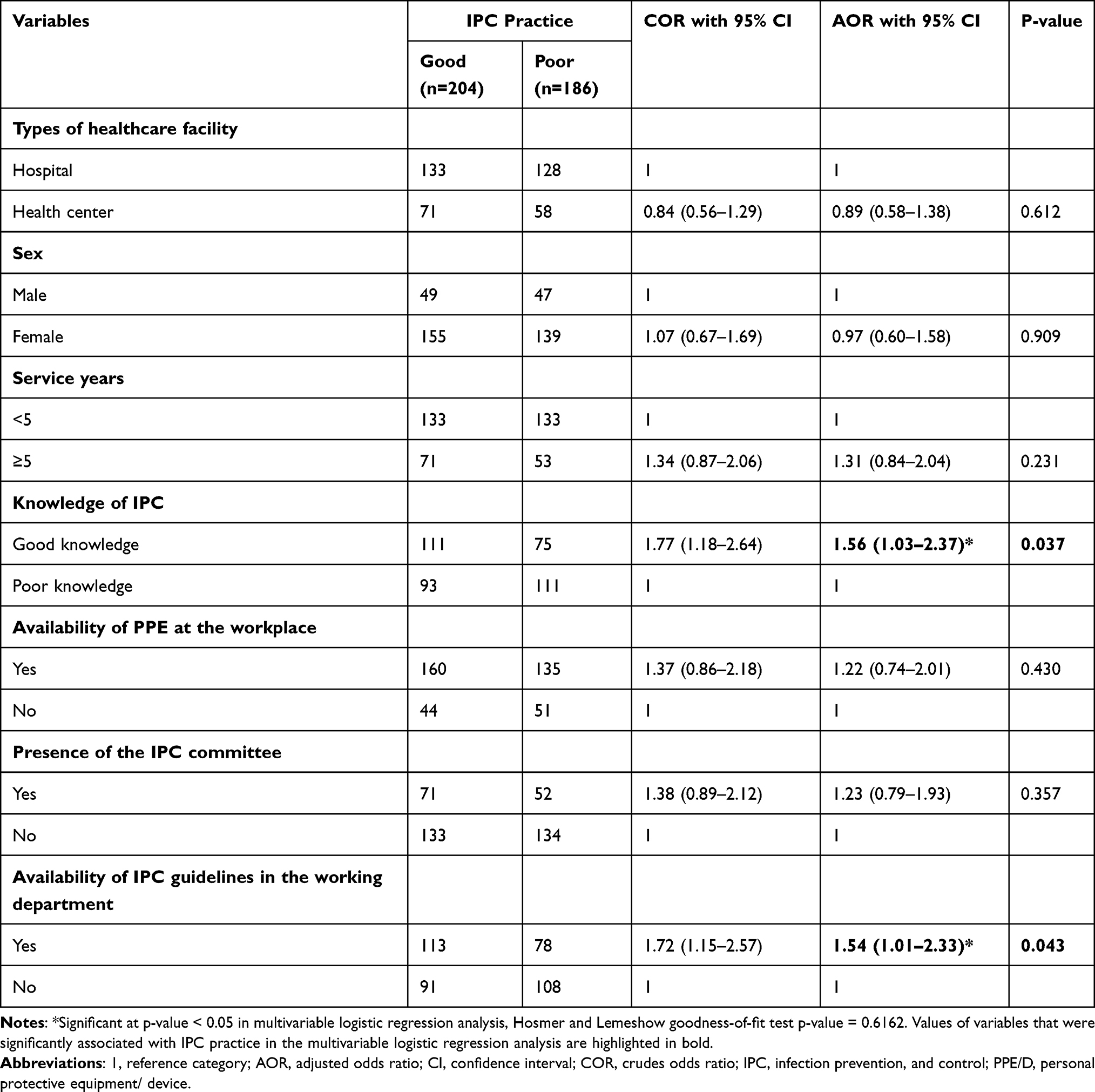 |
Table 5 Logistic Regression Analysis of Factors Associated with Infection Prevention and Control Practice Among Cleaners Working in Healthcare Facilities in Gondar City, Ethiopia, 2022 (N=390) |
Discussion
Globally, healthcare-associated infections remain a major cause of patient morbidity and mortality. The main source of healthcare-acquired pathogens can be attributed to cross-infection via the hands of healthcare personnel, who have become contaminated through direct contact with the patient or indirectly by touching contaminated environmental surfaces. Infection prevention practice is fundamental to quality of care and essential to protecting healthcare cleaners, healthcare workers, patients, and communities from tremendous infectious diseases. Healthcare institution cleaning has been shown to impact rates of HCAIs and good environmental hygiene is critical to quality care, yet those tasked with the role of ensuring a safe and clean environment often go unrecognized as members of the healthcare workforce.47 Understanding the magnitude and investigating the determinants of IPC practice plays a paramount role in establishing effective prevention and control strategies for this neglected frontline healthcare workforce. Therefore, this study attempted to assess infection prevention and control practice and its associated factors among cleaners working in healthcare facilities in Gondar City, Northwest Ethiopia.
This study revealed that out of the 390 healthcare cleaners, 204 (52.3%) of them had good IPC practice 52.3% [95% CI (47.2, 56.4)]. Our finding was higher compared to a study in Addis Ababa with good safety precaution practice of 35.7%.42 The difference could be due to the measurement tool used. In this study, we used 70% as a cut-off point out of ten (10) questions, while studies conducted in Addis Ababa used 75% as a cut-off point out of fourteen (14) questions. However, our finding was lower than a study conducted in South Africa, which showed that over 57% of cleaners reported moderately good infection control practices, while 23% of them had poor infection control practices.25 The difference might be due to differences in the study setting, healthcare cleaners’ work experience, and job training. Another explanation for the variance could be the different training experiences the study participants had in infection prevention and control. In a study conducted in South Africa, the majority (87%) of the cleaners had been trained in infection control. It is expected that all of them should have displayed better practices of infection control because of the in-service training, which is done every year. This is on-job training, which is done to remind employees about what they were trained on initially and to update them on new developments regarding IPC.
Our study sample comprised a larger number of 294 (75.4%) females than males, and their mean (±SD) age was 31.45 (±7.64) with an age range of 20–58 years. Most of the cleaner’s ages were found in the age group of 20 to 29 years. This could be because most cleaning activities were performed by female cleaning staff in a young age group. Notably, other studies done in Nigeria,48 Sudan,49 and Addis Ababa50 present similar age and gender distributions. Even though there is no association between sex and the practice of infection prevention, the practice of infection prevention was higher among female cleaners than among males (39.7% vs 12.6%, respectively). The reason for the increased frequency of infection prevention practice among females in this study could be due to the large number of female cleaner participants (75.4%) compared to their male cleaner counterparts (24.6%). The other possible explanation for the difference could be due to a difference in sex might be due to females’ natural ability to obey rules and regulations.
The results of this study showed that 204 (52.3%) of the participants had poor knowledge of IPC, with 95% CI (48.3, 58.2). This result was comparable to findings from studies in Addis Ababa (48.8%)42 and South Africa (50%).25 This finding is evidence that there are gaps in the knowledge of IPC among healthcare cleaning staff. Even though some of the knowledge questions were answered correctly, there are some specific and important areas where knowledge is lacking, such as the preparation of chlorine solution, hand washing procedures, and waste separation systems, which require careful consideration during training and capacity building. This result highlights that knowledge plays a crucial role in ensuring that cleaning staff follow the rules that will lead to the elimination of healthcare-associated infections and ensure compliance with infection prevention and control practices.25,41
The study found that healthcare cleaners who had good knowledge of infection prevention and control were 1.56 times more likely to have good infection prevention and control practices than those who did not. Research from China51 and other comparable studies52,53 confirm this conclusion. This finding could explain the good knowledge and practice score owned by surveyed cleaners given the fact that training in the most recent infection prevention and control guidelines could upgrade their knowledge and skills by enabling them to easily understand and consistently apply critical standards of infection prevention and control practice. In addition, up-to-date knowledge and skills in cleaning and disinfection could also increase the confidence of cleaners in complying with recommended guidelines, thereby improving IPC practice. Awkwardly, good knowledge does not guarantee for good practice.54–56
In the current study, healthcare cleaners who had infection prevention and control guidelines had a 1.54 higher likelihood of having good infection prevention and control practices than those who did not. This concurs with earlier investigations conducted in Ethiopia57,58 and Australia.59 This may be explained by the fact that healthcare facility cleaners with infection prevention and control guidelines were more likely to receive current information and feel vulnerable to healthcare-acquired infections, which enhanced their practice of infection prevention and control.60 The WHO recommends that all primary healthcare facilities create their standard operating procedures (SOPs) based on national infection prevention and control recommendations.61 The creation and execution of infection prevention and control guidelines are the essential elements of infection prevention and control programs at all healthcare facilities.13,61
Strengths and Limitations of the Study
As there is a scarcity of data on infection prevention and control practices and associated factors among cleaners working in a healthcare facility in Ethiopia, the result of this study could pave the way for further scientific studies in the area. The findings of the study should be taken into consideration in light of the following limitations. First, our study did not use multilevel analysis, which is the ideal alternative to address nested data since there might be a dependency between health facility factors and the practice of cleaners at an individual level. Second, due to the cross-sectional nature of the data, it does not show a temporal relationship between independent variables and the outcome variable. Despite these limitations, we feel that the study provides a reasonably accurate assessment of infection prevention and control practices and associated risk factors among study participants.
Conclusions
This study found that 186 out of 390 healthcare cleaners had poor IPC practices. The results of the study also showed that more than half of healthcare cleaners had poor knowledge of infection prevention. The finding underlines the importance of good IPC knowledge and the accessibility of IPC guidelines to improve IPC practices among healthcare cleaning staff. The findings of this study also highlight that behavioral change interventions and paying attention, particularly to nonclinical staff such as cleaners in health care settings, are critical to reducing infection in health care settings. It is recommended that the knowledge of healthcare cleaners about IPC be improved through training, supervision, and monitoring of their practice about IPC. Healthcare facilities should also be encouraged to establish and promote IPC guidelines for the workplace. Accordingly, the Ethiopian Ministry of Health should strive to promote safe work practices following IPC guidelines and improve the working environment of healthcare cleaning staff to ensure a functioning system that promotes the effective use of IPC techniques by healthcare cleaning staff. There is also a need to review existing policies and develop new policies that target this vulnerable population in healthcare. In addition, continuous supervision is recommended to improve healthcare cleaning staff compliance with infection prevention and control.
Data Sharing Statement
All datasets pertinent to the work are included within the article. Detailed raw data analyzed for the work reported can be available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted following the tenets of the Helsinki Declaration. Ethical clearance was obtained from the Institutional Ethical Review Board (IRB) of the University of Gondar with ethics reference number: IRB-EOHS-523-2022. Before data collection, an official letter of support from the University of Gondar was submitted to the Central Gondar Zone Health Office and each health facility to be surveyed. Permission to conduct the study was obtained from the head of each health facility. Each study participant provided a written, voluntarily signed informed consent after the purpose, risks, and benefits of the study were explained. All personal identifiers were removed to ensure confidentiality. As well, the data collected were only entered and analyzed on the principal investigator’s computer, which was password protected.
Acknowledgments
The authors would like to thank the University of Gondar for providing ethical clearance. The authors are also very grateful to all the data collectors, the supervisor, and the study participants.
Author Contributions
All authors made substantial intellectual contributions to the work reported, whether in the conception, study design, execution and acquisition of data, analysis, and interpretation or all of these parts; participated in drafting the manuscript, critical review or revision of the article; have read and approved the final version; selected and settled the journal to which the article submitted; and approved accountability in all aspects of the work reported.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mostafa H. Infection prevention and control. 1997.
2. Sahiledengle B, Gebresilassie A, Getahun T, Hiko D. Infection prevention practices and associated factors among healthcare workers in governmental healthcare facilities in Addis Ababa. Ethiop J Health Sci. 2018;28(2):177–186. doi:10.4314/ejhs.v28i2.9
3. Damani N. Manual of Infection Prevention and Control. USA: Oxford University Press; 2019.
4. FMOH. Infection Prevention and Patient Safety: Reference Manual for Service Providers and Managers in Healthcare Facilities of Ethiopia. FMOH; 2010.
5. Ibrahim FAA. Nurses knowledge, attitudes, practices and familiarity regarding disaster and emergency preparedness–Saudi Arabia. Am J Nurs Sci. 2014;3(2):18–25. doi:10.11648/j.ajns.20140302.12
6. Al-Tawfiq JA, Tambyah PA. Healthcare associated infections (HAI) perspectives. J Infect Public Health. 2014;7(4):339–344. doi:10.1016/j.jiph.2014.04.003
7. Haque M, Sartelli M, McKimm J, Bakar MA. Health care-associated infections–an overview. Infect Drug Resist. 2018;11:2321. doi:10.2147/IDR.S177247
8. World Health Organization. Report on the Burden of Endemic Health Care-Associated Infection Worldwide. World Health Organization; 2011.
9. Oosthuysen J, Potgieter E, Fossey A. Compliance with infection prevention and control in oral health-care facilities: a global perspective. Int Dent J. 2014;64(6):297–311. doi:10.1111/idj.12134
10. Rutala WA, Weber DJ. Disinfection, sterilization, and control of hospital waste. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Elsevier; 2015:3294.
11. Postnatal Care. Federal Democratic Republic of Ethiopia Ministry of Health. Ethiopia: Postnatal Care; 2003.
12. World Health Organization. Health Care Without Avoidable Infections: The Critical Role of Infection Prevention and Control. World Health Organization; 2016.
13. Storr J, Twyman A, Zingg W, et al. Core components for effective infection prevention and control programmes: new WHO evidence-based recommendations. Antimicrob Resist Infect Control. 2017;6:1–18. doi:10.1186/s13756-016-0149-9
14. Nelson S, Stone PW, Jordan S, et al. Patient safety climate: variation in perceptions by infection preventionists and quality directors. Interdiscip Perspect Infect Dis. 2011;2011:1–7. doi:10.1155/2011/357121
15. World Health Organization. The World Health Report 2002: Reducing Risks, Promoting Healthy Life. World Health Organization; 2002.
16. Padmanabhan K, Barik D. Health Hazards of Medical Waste and Its Disposal. In: Energy from Toxic Organic Waste for Heat and Power Generation. Elsevier; 2019:99–118.
17. World Health Organization. Infection Prevention and Control in Health Care: Time for Collaborative Action. World Health Organization; 2010.
18. Umakanthan S, Sahu P, Ranade AV, et al. Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19). Postgrad Med J. 2020;96(1142):753–758. doi:10.1136/postgradmedj-2020-138234
19. Cheng VC, Lau SK, Woo PC, Yuen KY. Severe acute respiratory syndrome coronavirus as an agent of emerging and reemerging infection. Clin Microbiol Rev. 2007;20(4):660–694. doi:10.1128/CMR.00023-07
20. Haines A, de Barros EF, Berlin A, Heymann DL, Harris MJ. National UK programme of community health workers for COVID-19 response. Lancet. 2020;395(10231):1173–1175. doi:10.1016/S0140-6736(20)30735-2
21. Umakanthan S, Patil S, Subramaniam N, Sharma R. COVID-19 vaccine hesitancy and resistance in India explored through a population-based longitudinal survey. Vaccines. 2021;9(10):1064. doi:10.3390/vaccines9101064
22. Umakanthan S, Monice M, Mehboob S, Jones CL, Lawrence S. Post acute (long) COVID-19 quality of life. Front Public Health. 2023;11:1163360. doi:10.3389/fpubh.2023.1163360
23. Collins AS. Preventing health care–associated infections. 2011.
24. Yamazhan T, Taşbakan MI, Çalik Ş, Pullukcu H, Sipahi OR, Ulusoy S. Evaluation of the knowledge of hospital cleaning staff about prevention of nosocomial infections. Turk J Med Sci. 2009;39(1):77–80.
25. Peta MR. Knowledge, attitudes and practices of general assistants towards infection control at Letaba hospital. In: Unpublished Master of Public Health Dissertation. Johannesburg: University of the Witwatersrand; 2014.
26. Bartley JM, Olmsted RN, Haas J. Current views of health care design and construction: practical implications for safer, cleaner environments. Am J Infect Control. 2010;38(5):S1–S12. doi:10.1016/j.ajic.2010.04.195
27. Maina JW. Knowledge, attitude and practice of staff on segregation of hospital waste: a case study of a tertiary private hospital in Kenya. Eur Sci J. 2018;14(9):401–417.
28. Desta M, Ayenew T, Sitotaw N, Tegegne N, Dires M, Getie M. Knowledge, practice and associated factors of infection prevention among healthcare workers in Debre Markos referral hospital, Northwest Ethiopia. BMC Health Serv Res. 2018;18(1):1–10. doi:10.1186/s12913-018-3277-5
29. Lopchan M, Gurung G, Rajbanshi L, Osti C, Baniya A. Knowledge and attitude towards infection control among supporting staffs of Chitwan Medical College, Bharatpur, Chitwan. J Chitwan Med Coll. 2016;6(1):40–47. doi:10.3126/jcmc.v6i1.16654
30. Chalya PL, Seni J, Mushi MF, et al. Needle-stick injuries and splash exposures among health-care workers at a tertiary care hospital in north-western Tanzania. Tanzan J Health Res. 2015;17(2):154.
31. Mbim EN, Mboto CI, Agbo BE. A review of nosocomial infections in Sub-Saharan Africa. Br Microbiol Res J. 2016;15(1):1–11. doi:10.9734/BMRJ/2016/25895
32. Cross S, Gon G, Morrison E, et al. An invisible workforce: the neglected role of cleaners in patient safety on maternity units. Glob Health Action. 2019;12(1):1480085. doi:10.1080/16549716.2018.1480085
33. Peters A, Otter J, Moldovan A, Parneix P, Voss A, Pittet D. Keeping Hospitals Clean and Safe Without Breaking the Bank; Summary of the Healthcare Cleaning Forum 2018. Springer; 2018.
34. Donaghy J. Organisational support improves adherence to infection prevention and control guidelines. Evid Based Nurs. 2022;25(1):10. doi:10.1136/ebnurs-2020-103305
35. van Hout D, Hutchinson P, Wanat M, et al. The experience of European hospital-based health care workers on following infection prevention and control procedures and their wellbeing during the first wave of the COVID-19 pandemic. PLoS One. 2022;17(2):e0245182. doi:10.1371/journal.pone.0245182
36. Aliyu AS, Badawi AH, Umar NY, Abubakar F, Sani BBW. Epidemiological study on hospital acquired infections and infection prevention and control among health care workers in Specialist Hospital Bauchi State, Nigeria. ARC J Public Health Commun Med. 2020;5(3):1–13.
37. Adams J, Bartram J, Chartier Y. Essential Environmental Health Standards for Health Care. World Health Organization; 2008.
38. Abiye S, Yitayal M, Abere G, Adimasu A. Health professionals’ acceptance and willingness to pay for hepatitis B virus vaccination in Gondar City Administration governmental health institutions, Northwest Ethiopia. BMC Health Serv Res. 2019;19(1):1–7. doi:10.1186/s12913-019-4671-3
39. Daniel WW, Cross CL. Biostatistics: A Foundation for Analysis in the Health Sciences. Wiley; 2018.
40. Bayleyegn B, Mehari A, Damtie D, Negash M. Knowledge, attitude and practice on hospital-acquired infection prevention and associated factors among healthcare workers at University of Gondar comprehensive specialized hospital, Northwest Ethiopia. Infect Drug Resist. 2021;14:259. doi:10.2147/IDR.S290992
41. Alhumaid S, Al Mutair A, Al Alawi Z, et al. Knowledge of infection prevention and control among healthcare workers and factors influencing compliance: a systematic review. Antimicrob Resist Infect Control. 2021;10(1):1–32. doi:10.1186/s13756-021-00957-0
42. Belay Tesfaye G, Tessema TT, Dinka TG. Safety precaution practices and associated factors among public hospital cleaners: case in Addis Ababa, Ethiopia. IJRES. 2020;8:10–21.
43. Markos T, Sinkie SO, Garedew MG. Compliance with infection prevention practices and associated factors among health professionals in the public hospitals of Kembata Tembaro Zone, south Ethiopia. Health Sci J. 2021;15(7):1–9.
44. Tesfaye AH, Engdaw GT, Aragaw FM, Kabito GG. Prevalence and risk factors of work-related contact dermatitis symptoms among healthcare cleaners during the COVID-19 pandemic in Northwest Ethiopia: a multicentre cross-sectional survey. BMJ open. 2022;12(11):e069019. doi:10.1136/bmjopen-2022-069019
45. Manchanda V, Suman U, Singh N. Implementing infection prevention and control programs when resources are limited. Curr Treat Options Infect Dis. 2018;10:28–39. doi:10.1007/s40506-018-0142-3
46. Taber KS. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res Sci Educ. 2018;48:1273–1296. doi:10.1007/s11165-016-9602-2
47. Quinn MM, Henneberger PK, Braun B, et al. Cleaning and disinfecting environmental surfaces in health care: toward an integrated framework for infection and occupational illness prevention. Am J Infect Control. 2015;43(5):424–434. doi:10.1016/j.ajic.2015.01.029
48. Ilesanmi OS, Omotoso B, Falana D. Hazards of hospital cleaners in a tertiary health facility in Southwest Nigeria. Int J Occup Safety Health. 2014;4(1):5–10. doi:10.3126/ijosh.v4i1.10083
49. Abdelhalim M, Elawad AE, Elawad MA. Knowledge, attitude, and practices among cleaners towards health care waste in Omdurman and Bahry teaching hospitals. 2017.
50. Mariam FA, Alemu ZA. Medical waste handling practice and associated factors among cleaners in public hospitals under Addis Ababa Health Bureau, Addis Ababa, Ethiopia. J Med Health Sci. 2018;7(4):14–23.
51. Luo Y, He G-P, Zhou J-W, Luo Y. Factors impacting compliance with standard precautions in nursing, China. Int J Infect Dis. 2010;14(12):e1106–e1114. doi:10.1016/j.ijid.2009.03.037
52. Alice TE, Akhere A, Ikponwonsa O, Grace E. Knowledge and practice of infection control among health workers in a tertiary hospital in Edo state, Nigeria. Direct Res J Health Pharm. 2013;1(2):20–27.
53. Sarani H, Balouchi A, Masinaeinezhad N, Ebrahimitabs E. Knowledge, attitude and practice of nurses about standard precautions for hospital-acquired infection in teaching hospitals affiliated to Zabol University of Medical Sciences (2014). Glob J Health Sci. 2016;8(3):193. doi:10.5539/gjhs.v8n3p193
54. Iliyasu G, Dayyab FM, Habib ZG, et al. Knowledge and practices of infection control among healthcare workers in a Tertiary Referral Center in North-Western Nigeria. Ann Afr Med. 2016;15(1):34. doi:10.4103/1596-3519.161724
55. Madan AK, Raafat A, Hunt JP, Rentz D, Wahle MJ, Flint LM. Barrier precautions in trauma: is knowledge enough? J Trauma Acute Care Surg. 2002;52(3):540–543. doi:10.1097/00005373-200203000-00020
56. Amoran O, Onwube O. Infection control and practice of standard precautions among healthcare workers in northern Nigeria. J Glob Infect Dis. 2013;5(4):156. doi:10.4103/0974-777X.122010
57. Temesgen C, Demissie M. Knowledge and practice of tuberculosis infection control among health professionals in Northwest Ethiopia; 2011. BMC Health Serv Res. 2014;14(1):1–7. doi:10.1186/s12913-014-0593-2
58. Assefa J, Diress G, Adane S. Infection prevention knowledge, practice, and its associated factors among healthcare providers in primary healthcare unit of Wogdie District, Northeast Ethiopia, 2019: a cross-sectional study. Antimicrob Resist Infect Control. 2020;9(1):1–9. doi:10.1186/s13756-020-00802-w
59. Mitchell BG, Say R, Wells A, Wilson F, Cloete L, Matheson L. Australian graduating nurses’ knowledge, intentions and beliefs on infection prevention and control: a cross-sectional study. BMC Nurs. 2014;13(1):1–7. doi:10.1186/s12912-014-0043-9
60. Haile TG, Engeda EH, Abdo AA. Compliance with standard precautions and associated factors among healthcare workers in Gondar University Comprehensive Specialized Hospital, Northwest Ethiopia. J Environ Public Health. 2017;2017:1–8. doi:10.1155/2017/2050635
61. Tartari E, Tomczyk S, Pires D, et al. Implementation of the infection prevention and control core components at the national level: a global situational analysis. J Hosp Infect. 2021;108:94–103. doi:10.1016/j.jhin.2020.11.025
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge and Practice of Wound Care and Associated Factors among Nurses Working in South Wollo Zone Government Hospitals, Ethiopia
Tegegne B, Yimam F, Mengesha Yalew Z, Wuhib M, Mekonnen L, Asmamaw Yitayew Y, Ademe S, Tsegaye D, Eshetie Y, Chanie M
Chronic Wound Care Management and Research 2022, 9:1-11
Published Date: 20 July 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Palliative Care Practice and Associated Factors Among Nurses Working in Chronic Care Units of Tertiary Hospitals in Ethiopia: A Cross-Sectional Study
Gembe M, Tariku T, Tesfaye T, Hailu EH
Nursing: Research and Reviews 2024, 14:45-58
Published Date: 8 February 2024