Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Inetetamab-Based Regimens for Patients with HER2-Positive Metastatic Breast Cancer: A Real-World Retrospective Study
Authors Chen L, Huang J ![]() , Chen X, Lan X, Song L, Xie X, Bai X, Du C
, Chen X, Lan X, Song L, Xie X, Bai X, Du C
Received 8 August 2025
Accepted for publication 20 December 2025
Published 30 December 2025 Volume 2025:17 Pages 1427—1437
DOI https://doi.org/10.2147/BCTT.S556110
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Liping Chen, Jiayi Huang, Xuelian Chen, Xiaofeng Lan, Lin Song, Xiaofeng Xie, Xue Bai, Caiwen Du
Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital & Shenzhen Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Shenzhen, Guangdong, People’s Republic of China
Correspondence: Caiwen Du, Email [email protected]
Background: Inetetamab is a Chinese-origin recombinant anti-HER2 monoclonal antibody. Herein, we assessed the efficacy and safety of inetetamab-containing regimens in patients with HER2-positive metastatic breast cancer (MBC).
Patients and Methods: We retrospectively reviewed the medical records of patients with HER2-positive MBC who received inetetamab-containing regimens as a salvage treatment in metastatic setting from December 2020 to April 2024. The primary endpoint was progression-free survival (PFS) in the total population (TP). Patients with brain metastases were also included. Secondary endpoints were objective response rate (ORR), disease control rate (DCR), and safety.
Results: At the data cut-off date of June 1, 2024, a total of 90 patients were included in this analysis. Median follow-up duration was 7.2 months (IQR 3.6– 13.1). The median PFS was 12.0 months (95% confidence interval [CI] 7.3 to 17.0 months) in the TP. The median PFS in the subgroup with brain metastases reached 10.0 months (95% CI 5.9 to NA months). The ORR was 46.6% (42/90), and the DCR was 92.2% (83/90). The most frequently combined chemotherapy was vinorelbine (83/90,92.2%). The most frequently concomitant targeted drug was pyrotinib (70/90,77.8%). The median PFS not reached for first-line, 15.9 months (95% CI 11.9 to NA months) for second-line, and 5.9 months (95% CI 4.4 to 12.2 months) for third-line or later therapy. Cox univariate and multivariate analyses demonstrated that lines of treatment were the only significant predictive factor for PFS (first- and second-line vs third-line or above: 15.9 vs 5.9 months, p=0.0021). The toxicity was tolerable. The most frequent grade 3 or 4 treatment-related adverse events were diarrhea (12.2%).
Conclusion: Inetetamab offers a promising option and a manageable safety profile for HER2-positive MBC who pretreated with multiple-line therapies. Meanwhile, inetetamab plus small-molecule TKIs regimens shows good anti-tumor efficacy for MBC with brain metastases, which deserves further validation in a larger group trial.
Keywords: inetetamab, HER2-positive metastatic breast cancer, pretreated, safety
Introduction
According to GLOBOCAN 2020, Breast cancer (BC) is the most common cancer among women in China and abroad.1 Human epidermal growth factor receptor 2 (HER2)-positive patients account for approximately 15–20% of breast cancers.2 HER2-positive BC represented a more aggressive subtype, with higher tumor grade, more recurrence, and poorer prognosis in the absence of systemic therapy.3–5 Although huge progresses have been achieved in treating HER2-positive BC, metastatic disease remains incurable. Nearly all the metastatic breast cancer (MBC) patients will suffer from disease progression after first-line treatment with trastuzumab.6,7 In the last decades, the development of multiple anti-HER2 agents, including monoclonal antibodies, tyrosine kinase inhibitors (TKIs) and antibody drug conjugates (ADCs),8 has significantly improved the survival of patients with HER2-positive BC. However, in China, a huge proportion of patients with HER2-positive MBC have to abandon treatment due to high expenditure on drugs like ADCs which are not included in medical insurance.9 Continuous inhibition of the HER2 pathway offers a survival benefit to MBC patients treated with trastuzumab beyond progression.10 A combination of anti-HER2 antibodies and chemotherapy are still needed through first- and later-line treatment.
Inetetamab (Cipterbin®)11 is an innovative anti-HER2 monoclonal antibody developed by Shanghai CP Guojian Pharmaceutical Co. in China. Inetetamab is an Fc-engineered anti-HER2 monoclonal antibody, distinct from trastuzumab,with modification at positions 359 and 361 in the CH3 domain. Similar to margetuximab, this engineering enhances its binding to the activating Fcγ receptor CD16A and reduces affinity for the inhibitory receptor CD32B, thereby potentiating antibody-dependent cellular cytotoxicity (ADCC). The products demonstrated a comparable anti-tumor efficacy to that of trastuzumab in vivo.12 Inetetamab possesses distinct mechanistic features that set it apart from trastuzumab and margetuximab. The HOPES study confirmed the significant efficacy and manageable safety of the combination of vinorelbine for HER2-positive MBC.13 While clinical trials have established the efficacy of inetetamab, real-world evidence is still in need. For instance, a recent large-scale retrospective study of 329 Chinese patients with HER2-positive MBC demonstrated promising activity and safety of inetetamab in first- and second-line settings.14 Furthermore, our team’s previous multicenter, retrospective, real-world study (ILLUMINE) supports the efficacy of combining inetetamab with pyrotinib.15 Despite these valuable insights, data on the use of inetetamab in later lines of therapy and in specific subgroups, such as those with brain metastases (BM), remains limited. The current study is aimed to provide real-world evidence by analyzing the data from our center on study of inetetamab-based treatment strategies for patients with HER2-positive MBC.
Materials and Methods
Study Design
This was a single-center study, which retrospectively reviewed the medical data of consecutive patients with HER2-positive MBC treated with inetetamab at National Clinical Research Center for Cancer/Cancer Hospital & Shenzhen Hospital (Shenzhen, Guangdong, China) between December 2020 and April 2024. This study, involving human subjects, was conducted in accordance with the Helsinki Declaration. This study received approval from the Institutional Review Board and Ethics Committee of the National Cancer Hospital & Shenzhen Hospital (Approval No. YW2024-26-1). Because this study was retrospective and observational in design and all patient data were anonymized, the Ethics Committee waived the requirement for written informed consent.
Patients and Treatment
The inclusion criteria were as follows: female patients, age ≥18 years old, histologically confirmed HER2-positive MBC (including hormone receptor positive/negative breast cancer), at least two cycles of inetetamab, and complete medical records. HER2 status was defined as 3+ based on immunohistochemistry (IHC) or 2+ with gene amplification by fluorescence in situ hybridization (FISH) staining of primary or metastatic lesion samples. The exclusion criteria were patients with no measurable or evaluable metastatic lesions defined by the Response Evaluation Criteria in Solid Tumors (RECIST); or those lost to follow-up. The last follow-up was conducted on June 1, 2024.
All eligible patients were treated with inetetamab-based therapy. Inetetamab was administrated at a dose of 6 mg/kg of body weight intravenously per 21 days, with an initial loading dose of 8 mg/kg. Other anti-HER2 targeted agents and chemotherapy were allowed to be used in combination with inetetamab.
End Points
The primary end point was PFS, which was defined as the time gap between date of initiation of first inetetamab-based regimens to the date of documented disease progression or death from any cause or the last follow-up. The secondary end points included the objective response rate (ORR, defined as the percentage of patients who had a confirmed complete response or partial response); disease control rate (DCR, defined as the percentage of patients who had a confirmed complete response or partial response or stable disease for at least 4 weeks); and safety.
Data Collection and Assessment
The baseline characteristics of the patients were collected, including general information (age, sex, ECOG score), tumor characteristics (TNM stage, pathology, hormone receptor and HER2 status, and metastatic site), and treatment information (previous chemotherapy/targeted therapy, radiation, or surgery history, and (neo)adjuvant therapy history).
All patients underwent regular check-ups, including physical examination, laboratory examinations, electrocardiogram, and imaging (computed tomography or positron emission tomography/CT (PET/CT) or contrast-enhanced magnetic resonance imaging). Tumor response was evaluated retrospectively by the treating physician based on routinely collected imaging data and assessed according to RECIST version 1.1. Imaging was performed per routine clinical practice, typically every 2 treatment cycles. Patients with missing or off-schedule imaging assessments were censored at the date of their last available radiographic evaluation. Safety evaluations were conducted every cycle. Adverse events were graded using the National Cancer Institute Common Terminology Criteria for Adverse Events version 5.0. The study did not interfere with any physician’s decisions and did not change any treatment.
Statistical Analysis
All data were analyzed using R4.2.2 (http://www.Rproject.org; The R Foundation, Vienna, Austria) and GraphPad Prism 5 software (GraphPad Software, Inc., La Jolla, CA, USA). Descriptive analysis was utilized to display clinicopathological features. The Kaplan–Meier method was used to estimate PFS. Additionally, Cox univariate models were used to identify the predictive variables for PFS, presented as hazard ratios (HR), and corresponding 95% confidence intervals (CIs). All reported p values were two-sided, with p<0.05 being regarded as statistically significant.
Results
Patient Clinicopathological Characteristics
Between December 2020 and April 2024, a total of 104 patients treated with inetetamab were recruited. Only 90 patients were eligible for the study, according to inclusion and exclusion criteria (Figure 1). The cutoff date for follow-up was June 1,2024. The median follow-up time for this study was 7.2 months (range: 3.6 to 38.1 months).
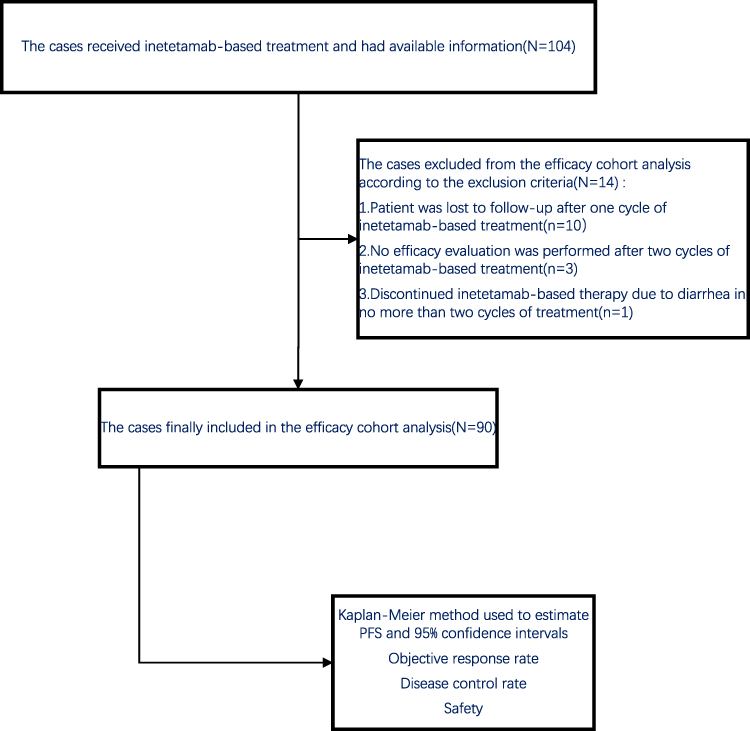 |
Figure 1 Flow diagram of the analysis. |
The baseline characteristics of the patients are shown in Table 1. All the patients were female, the median age at diagnosis was 45.0±10.9 years. Fifty-seven patients (63.3%) were aged over 40 years old at diagnosis. Eighty-five patients (94.4%) were invasive ductal cancer. Forty-six patients (51.1%) were estrogen receptor (ER) and/or progesterone receptor (PR) positive. For HER2 status, HER2 3+ by IHC was recorded in 71 patients (78.9%), and HER2 2+ by IHC and amplification by FISH in 19 patients (21.1%). Thirty-five patients (38.9%) had Grades 1–2 histological of tumors, and 35 patients (38.9%) had Grades 3–4 histological of tumors. Twenty-three patients (25.6%) had de novo stage IV disease at their first diagnosis. Forty-five patients (50.0%) had liver/lung metastases and 30 (33.3%) of them had brain metastases at baseline. Of those patients with brain metastases, 22 patients had received local therapies including whole-brain radiotherapy (WBRT), stereotactic radiotherapy (SRT) or surgery plus SRT before inetetamab. Most of the patients (67/90, 74.4%) had received anti-HER2 therapy with trastuzumab in metastatic setting. Thirty-nine (43.3%) of them had received pertuzumab, 54 patients (60%) had received TKIs (pyrotinib (42.2%), lapatinib (12.2%), apatinib (4.4%),and neratinib (1.1%)) for their metastatic disease. Four patients were previously treated with TDM-1. One of them was previously treated with trastuzumab deruxtecan (T-Dxd). The median lines of treatment were 3(range 1–8). Twenty-one patients (23.3%) received inetetamab-based regiment as first-line therapy; 36 patients (40.0%) received at least 3 lines of therapy in the metastatic setting.
 |
Table 1 The Baseline Characteristics of the Patients |
Treatment Administration
The drugs in combination with inetetamab are presented in Table 2. Most patients were treated with inetetamab combined with chemotherapy and other HER2-targeted therapies. Combined chemotherapeutic agents included vinorelbine (83, 92.2%), nab-paclitaxel (5, 5.6%), pirarubicin (1, 1.1%), and utidelone (1, 1.1%). For the choice of combined anti HER2-targeted treatment, the most common was pyrotinib (70,77.8%), followed by pertuzumab (8, 8.9%). Four patients received only inetetamab and chemotherapy.
 |
Table 2 Treatment Administration |
Efficacy
By the end of follow-up, 52 patients had experienced disease progression and 13 patients had died, and 38 patients remained progression-free. The median PFS was 12 months (95% CI 7.3 to 17 months, Figure 2) in total cohort and was 10 months in the group of brain metastases (95% CI 5.9 to NA months, Figure 3). There was a statistically difference in PFS (15.9 vs 5.9 months, p=0.0021) between the first- and second-line and third-line or above subgroups (seen in Figure 4A). Patients without liver/lung metastases seemed to obtain a longer PFS than those with liver/lung disease, but the difference was not significant (15.8 vs 7.3 months, p=0.1) (seen in Figure 4B). The PFS was similar (11.9 vs 12 months, p=0.57) between the HR-positive and HR-negative subgroups (seen in Figure 4C).
 |
Figure 2 Kaplan-Meter curves of progression-free survival in overall cohort. |
 |
Figure 3 Kaplan-Meter curves of progression-free survival in brain metastases. |
 |
Figure 4 Kaplan-Meter curves of progression-free survival for patients. (A) Patients stratified by treatment lines; (B) Patients with liver/lung metastases or not; (C) Patients stratified by hormone-receptor status. |
The evaluations of efficacy are presented in Table 3. CR was achieved in 2 (2.2%) patients, and PR was achieved in 40 (44.4%) patients, and SD was achieved in 41 (45.6%) patients. The ORR and the DCR were 46.6% and 92.2%, respectively. Additionally, 7 (7.8%) patients showed progressive disease at the first assessment. At the time of data cutoff, 52 (57.8%) patients show progression.
 |
Table 3 Evaluation of Efficacy |
Univariate and multivariate analyses were performed to identify predictive factors of PFS for the 90 patients. As shown in Table 4, by means of Cox univariate and multivariate analyses, we found that lines of treatment were the independent prognostic factor for PFS (hazard ratio [HR] 0.4322; 95% CI 0.2495 to 0.7487; p = 0.00277; HR 0.3189; 95% CI 0.136 to 0.7477; p = 0.00857; respectively).
 |
Table 4 Univariate and Multivariate Analyses |
A total of 30 patients with brain metastases were included. The median PFS in the subgroup with brain metastases reached 10.0 months (95% CI 5.9 to NA months). Twenty-nine patients were treated with inetetamab plus small-molecule TKIs. The median lines of treatment were 2(range 1–4). All patients were treated with trastuzumab before inetetamab. Eighteen patients were treated with TKIs before.
Safety
The safety assessments of inetetamab-based therapy are summarized in Table 5. The most common adverse events (frequency ≥ 10%) were diarrhea (52.2%), vomiting/ nausea (20%), fatigue (20%), and leukopenia (18.9%). Other recorded adverse events included aspartate aminotransferase increase (5.6%), anemia (4.4%), creatinine increase (3.3%), thrombocytopenia (2.2%), peripheral neuritis (2.2%, and hand-foot syndrome (2.2%). The most frequent grade 3 adverse events were diarrhea (12.2%). No grade 4 diarrhea or cardiac-related events were reported. No treatment-related deaths were reported. However, the majority of AEs were unrelated to inetetamab use. Diarrhea, the most common adverse event, is mostly related with the combinations with pyrotinib. The incidence of decline of left ventricle ejection fraction was 2%. No patients stopped inetetamab because of side effects during treatment.
 |
Table 5 Safety Assessment |
Discussion
In our study, inetetamab-based regimens demonstrated promising efficacy and good safety profile in pretreated HER2 positive MBC. Forty percent of the patients had received more than three prior treatment lines, with the majority previously treated by trastuzumab in the (neo)adjuvant setting. Nevertheless, the median PFS of all 90 patients reached 12 months (95% CI,7.3–17months). The result of this study implies that inetetamab-based regimens may exhibit potential antitumor activity in later-line settings.
About 30% of early-stage patients ultimately developed into advanced breast cancer. Advanced breast cancer is still incurable at present, the 5-year survival rate of advanced breast cancer was only 20%, and the median overall survival was 2–3 years.16 As is well known, anti-HER2 therapy with trastuzumab and chemotherapy significantly reduced the risk of death and disease progression in HER2-positive MBC.17,18 The addition of pertuzumab or pyrotinib to trastuzumab and chemotherapy has revolutionized the regimen for first-line therapy for HER2 positive MBC19,20 in previous large scale clinical studies. However, most of the enrolled patients are not treated by trastuzumab. Standard second-line therapy of the antibody-drug conjugate trastuzumab deruxtecan (T-Dxd) is far from that one could pay due to the high prices not covered by medical insurance in China. Hence, anti-HER2 regimens more suitable for Chinese people is still in unmet need in clinical practice.
Like margetuximab, inetetamab is an Fc-modified anti-HER2 mAb with improved antibody-dependent cell-mediated cytotoxicity (ADCC) effect than trastuzumab.21 In the Phase III SOPHIA trial, margetuximab plus chemotherapy could prolong the mPFS over trastuzumab (5.8 vs 4.9 months),22 indicating that the enhancement of ADCC can make advantage of survival. However, the clinical data of inetetamb is mainly based on the HOPES study.13 The HOPES study was designed in 2009 in China when trastuzumab was still unreachable due to expensive cost. In HOPES study, inetetamab combined with vinorelbine is designed for patients who had not received any anti-HER2-targeted therapy. Our study represented the general population of patients with HER2 positive MBC who were usually pretreated with multiple anti-HER2 agents. What’s more, most patients in our study received dual anti-HER2 treatment of inetetamab in combination with pertuzumab or pyrotinib. While the single-arm, retrospective nature of this study precludes definitive comparative conclusions, the observed mPFS of 12.0 months, is encouraging. These real-world findings generate the hypothesis that inetetamab-based regimens could offer meaningful clinical benefit in these populations. Future prospective studies are needed to validate these results and define the optimal positioning of inetetamab within the HER2-positive treatment sequence. In the second-line treatment, mPFS of our study was 15 months, and the third-line or above treatment in our study, the mPFS was 5.9 months, which was similar to that reported in previous study.23–25 In addition, we analyzed the predictive factors of PFS, and found that patients who were treated with inetetamab as a first- and second-line had much longer PFS (treated as first- and second-line vs third-line or above: 15.9 vs 5.9 months, p=0.0021). Thus, we propose that the preferred use of inetetamab in early lines might be more effective.
Brain metastasis is a late event for MBC, which occurs in approximately 50% of patients with HER2+ breast cancer, with a median survival of 7 to 18 months after diagnosis.26,27 Radiation and surgery are currently the main local treatment approaches for the brain metastases.28 In recent years, a growing number of TKIs and ADCs produce an antitumor effect on the brain. However, options are limited for the control of breast cancer with brain metastasis patients. In KAMILLA study, trastuzumab emtansine in the 398 patients with baseline BM obtained a mPFS of 5.5 months.29 And in HER2CLIMB study, tucatinib combined with trastuzumab and capecitabine could significantly prolong the mPFS to 9.9 months in BM patients.30 In the BM subgroup in our study, the mPFS was 10 months. While direct comparisons are not feasible, the promising PFS and notable activity in patients with brain metastases observed in our study generate the hypothesis that this inetetamab-based therapy could be a valuable treatment option in these clinical contexts. The favorable outcomes observed in our study can likely be attributed to the predominant use of inetetamab combined with pyrotinib. Pyrotinib-based combination therapy was efficient to treat HER2 positive brain metastasis.31–33 The mPFS observed in patients with BM in this study was consistent with the findings of the ILLUMINE trial.15 The novel combination of inetetamab of pyrotinib might be an alternative regimen for this group of patients.
In terms of toxicity, incidences of AEs in this study were similar to previous reports and no new AEs were found. The majority of AEs were Grades 1–2, and the Grades 3–4 AEs were due to the combination agents, including diarrhea, leukopenia. Hence, inetetamab and trastuzumab are equivalently safe, and well tolerated, making it a candidate option besides trastuzumab.
Conclusion
Our study indicates that inetetamab-based regimens are effective for HER2 positive MBC with acceptable toxicity, providing a treatment option for such patients. However, this study has several limitations. Firstly, it is a single-center retrospective study, which makes it vulnerable to selection bias as patient inclusion depends on available records and clinical decisions. Secondly, the sample size is small, potentially reducing the statistical power. Thirdly, the median follow-up time is short, the first-line treatment was not reached, and no benefits of OS were observed. In the future, it needs to be confirmed the efficacy through large-scale prospective randomized controlled clinical studies, which would help to address these limitations and provide more conclusive evidence for clinical practice.
Acknowledgments
We would like to express our gratitude to the patients, their families, and all those who have contributed to this study.
The authors are grateful to all who have contributed to this research.
This research was presented as a poster at the 2024 San Antonio Breast Cancer Symposium (Presentation ID: P5-05-08).
Funding
This work was supported by funds from Sanming Project of Medicine in Shenzhen (No. SZSM202211012, and No.SZSM202411002); Cancer Hospital Chinese Academy of Medical Sciences, Shenzhen Center+E010324040; China Health Care Foundation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Prat A, Pineda E, Adamo B, et al. Clinical implications of the intrinsic molecular subtypes of breast cancer. Breast. 2015;24 Suppl 2:S26-35. doi:10.1016/j.breast.2015.07.008
3. Waks AG, Winer EP. Breast cancer treatment: a review. JAMA. 2019;321(3):288–300. doi:10.1001/jama.2018.19323
4. Radenkovic S, Konjevic G, Isakovic A, Stevanovic P, Gopcevic K, Jurisic V. HER2-positive breast cancer patients: correlation between mammographic and pathological findings. Radiat Prot Dosimetry. 2014;162(1–2):125–128. doi:10.1093/rpd/ncu243
5. O’Grady S, Morgan MP. Microcalcifications in breast cancer: from pathophysiology to diagnosis and prognosis. Biochim Biophys Acta Rev Cancer. 2018;1869(2):310–320. doi:10.1016/j.bbcan.2018.04.006
6. Al Sukhun S, Temin S, Barrios CH, et al. Systemic treatment of patients with metastatic breast cancer: ASCO resource-stratified guideline. JCO Glob Oncol. 2024:
7. Vernieri C, Milano M, Brambilla M, et al. Resistance mechanisms to anti-HER2 therapies in HER2-positive breast cancer: current knowledge, new research directions and therapeutic perspectives. Crit Rev Oncol Hematol. 2019;139:53–66. doi:10.1016/j.critrevonc.2019.05.001
8. Najjar MK, Manore SG, Regua AT, Lo HW. Antibody-drug conjugates for the treatment of HER2-positive breast cancer. Genes. 2022;13(11). doi:10.3390/genes13112065
9. Li J, Wang S, Wang Y, et al. Disparities of trastuzumab use in resource-limited or resource-abundant regions and its survival benefit on HER2 positive breast cancer: a real-world study from China. Oncologist. 2017;22(11):1333–1338. doi:10.1634/theoncologist.2017-0088
10. Extra JM, Antoine EC, Vincent-Salomon A, et al. Efficacy of trastuzumab in routine clinical practice and after progression for metastatic breast cancer patients: the observational Hermine study. Oncologist. 2010;15(8):799–809. doi:10.1634/theoncologist.2009-0029
11. Zhou X, Yu J, Wang W, et al. A Phase I dose-escalation study of a biosimilar trastuzumab in Chinese metastasis breast cancer patients. Springerplus. 2015;4:803. doi:10.1186/s40064-015-1603-5
12. Zhang X, Chen J, Weng Z, et al. A new anti-HER2 antibody that enhances the anti-tumor efficacy of trastuzumab and pertuzumab with a distinct mechanism of action. Mol Immunol. 2020;119:48–58. doi:10.1016/j.molimm.2020.01.009
13. Bian L, Xu BH, Di LJ, et al. Phase III randomized controlled, multicenter, prospective study of recombinant anti-HER2 humanized monoclonal antibody (Cipterbin) combined with vinorelbine in patients with HER2 positive metastatic breast cancer: the HOPES study. Zhonghua Yi Xue Za Zhi. 2020;100(30):2351–2357. doi:10.3760/cma.j.cn112137-20200116-00105
14. Zhang J, Mu Y, Zhang H, et al. Efficacy and safety of inetetamab-containing regimens in patients with HER2-positive metastatic breast cancer in first-line/second-line setting. Front Oncol. 2025;15:1564888. doi:10.3389/fonc.2025.1564888
15. Jin N, Tian M, Zha M, et al. Combined treatment of inetetamab plus pyrotinib and vinorelbine in managing advanced HER2-positive breast cancer patients (ILLUMINE): a multicenter, retrospective, real-world study. Transl Breast Cancer Res. 2025;6:31. doi:10.21037/tbcr-25-7
16. Gonzalez-Angulo AM, Morales-Vasquez F, Hortobagyi GN. Overview of resistance to systemic therapy in patients with breast cancer. Adv Exp Med Biol. 2007;608:1–22. doi:10.1007/978-0-387-74039-3_1
17. Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344(11):783–792. doi:10.1056/NEJM200103153441101
18. Marty M, Cognetti F, Maraninchi D, et al. Randomized phase II trial of the efficacy and safety of trastuzumab combined with docetaxel in patients with human epidermal growth factor receptor 2-positive metastatic breast cancer administered as first-line treatment: the M77001 study group. J Clin Oncol. 2005;23(19):4265–4274. doi:10.1200/JCO.2005.04.173
19. Swain SM, Baselga J, Kim SB, et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med. 2015;372(8):724–734. doi:10.1056/NEJMoa1413513
20. Ma F, Yan M, Li W, et al. Pyrotinib versus placebo in combination with trastuzumab and docetaxel as first line treatment in patients with HER2 positive metastatic breast cancer (PHILA): randomised, double blind, multicentre, phase 3 trial. BMJ. 2023:
21. Wang T, Zhang P, Di L, et al. Efficacy and safety of inetetamab in combination with chemotherapy as first-line treatment of HER2-positive metastatic breast cancer: a subgroup analysis in the HOPES study. Transl Breast Cancer Res. 2022;3:15. doi:10.21037/tbcr-21-42
22. Rugo HS, Im SA, Cardoso F, et al. Efficacy of margetuximab vs trastuzumab in patients with pretreated ERBB2-positive advanced breast cancer: a phase 3 randomized clinical trial. JAMA Oncol. 2021;7(4):573–584. doi:10.1001/jamaoncol.2020.7932
23. Krop IE, Kim SB, Gonzalez-Martin A, et al. Trastuzumab emtansine versus treatment of physician’s choice for pretreated HER2-positive advanced breast cancer (TH3RESA): a randomised, open-label, phase 3 trial. Lancet Oncol. 2014;15(7):689–699. doi:10.1016/S1470-2045(14)70178-0
24. Rugo HS, Im SA, Cardoso F, et al. Margetuximab versus trastuzumab in patients with previously treated HER2-Positive Advanced Breast Cancer (SOPHIA): final overall survival results from a randomized phase 3 trial. J Clin Oncol. 2023;41(2):198–205. doi:10.1200/JCO.21.02937
25. Saura C, Oliveira M, Feng YH, et al. Neratinib plus capecitabine versus lapatinib plus capecitabine in HER2-Positive metastatic breast cancer previously treated with >/= 2 HER2-directed regimens: phase III NALA trial. J Clin Oncol. 2020;38(27):3138–3149. doi:10.1200/JCO.20.00147
26. Olson EM, Najita JS, Sohl J, et al. Clinical outcomes and treatment practice patterns of patients with HER2-positive metastatic breast cancer in the post-trastuzumab era. Breast. 2013;22(4):525–531. doi:10.1016/j.breast.2012.12.006
27. Deluche E, Antoine A, Bachelot T, et al. Contemporary outcomes of metastatic breast cancer among 22,000 women from the multicentre ESME cohort 2008-2016. Eur J Cancer. 2020;129:60–70. doi:10.1016/j.ejca.2020.01.016
28. Ramakrishna N, Anders CK, Lin NU, et al. Management of advanced human epidermal growth factor receptor 2-positive breast cancer and brain metastases: ASCO guideline update. J Clin Oncol. 2022;40(23):2636–2655. doi:10.1200/JCO.22.00520
29. Montemurro F, Delaloge S, Barrios CH, et al. Trastuzumab emtansine (T-DM1) in patients with HER2-positive metastatic breast cancer and brain metastases: exploratory final analysis of cohort 1 from KAMILLA, a single-arm phase IIIb clinical trial(☆). Ann Oncol. 2020;31(10):1350–1358. doi:10.1016/j.annonc.2020.06.020
30. Lin NU, Borges V, Anders C, et al. Intracranial efficacy and survival with tucatinib plus trastuzumab and capecitabine for previously treated HER2-Positive breast cancer with brain metastases in the HER2CLIMB trial. J Clin Oncol. 2020;38(23):2610–2619. doi:10.1200/JCO.20.00775
31. Ma X, Li Y, Li L, et al. Pyrotinib-based treatments in HER2-positive breast cancer patients with brain metastases. Ann Med. 2022;54(1):3085–3095. doi:10.1080/07853890.2022.2139411
32. Gao M, Fu C, Li S, et al. The efficacy and safety of pyrotinib in treating HER2-positive breast cancer patients with brain metastasis: a multicenter study. Cancer Med. 2022;11(3):735–742. doi:10.1002/cam4.4481
33. Nader-Marta G, Martins-Branco D, Agostinetto E, et al. Efficacy of tyrosine kinase inhibitors for the treatment of patients with HER2-positive breast cancer with brain metastases: a systematic review and meta-analysis. ESMO Open. 2022;7(3):100501. doi:10.1016/j.esmoop.2022.100501
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.