")
Back to Journals » Research and Reports in Neonatology » Volume 10
Individualizing Oral Feeding Assessment and Therapies in the Newborn
Received 6 March 2020
Accepted for publication 1 May 2020
Published 20 May 2020 Volume 2020:10 Pages 23—30
DOI https://doi.org/10.2147/RRN.S223472
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Robert Schelonka
Dara Azuma,1 Jill L Maron2
1Division of Neonatal-Perinatal Medicine, Tufts Medical Center, Boston, MA, USA; 2Mother Infant Research Institute, Tufts Medical Center, Boston, MA, USA
Correspondence: Jill L Maron
Mother Infant Research Institute, Tufts Medical Center, 800 Washington Street, Boston, MA 02111 Tel +1-617-636-0766
Fax +1-617-636-1469
Email [email protected]
Abstract: Oral feeding competency is a milestone most infants must achieve prior to discharge. It is a developmentally complex task that requires integration of multiple sensory inputs, central nervous system maturation, motor coordination, and respiratory stability. While ensuring safety during oral feeding is important to reduce morbidities, we must optimize developmental windows to expedite feeding maturation. Currently, many of the assessments and therapies related to oral feeding skills focus solely on nutritive and non-nutritive sucking. Yet, this essential reflex is only one component of oral feeding. Specific challenges faced by individual newborns are often unique, and delays in development in any one of the many systems involved in oral feeding can lead to prolonged oral feeding maturation. Expanding the field to go beyond targeting oral motor skills to consider all aspects of feeding maturity, inclusive of sensory integration and hunger signaling, is needed to advance care. As technology continues to develop at a rapid pace, the field must compare the efficacy of these clinical and technologic assessments and therapies. In this review, we will address the complexity of neonatal feeding, review assessment tools and interventions for feeding safety and developmental readiness, and propose an individualized, multi-faceted approach to oral feeding evaluation and intervention.
Keywords: oral feeding, neonate, prematurity
Introduction
For the majority of premature newborns, oral feeding competency is required prior to discharge from the Neonatal Intensive Care Unit (NICU). While feeding challenges are nearly universal in the premature neonatal population, specific challenges faced by individual newborns are often unique. There is an intricate interplay between the central nervous system (CNS), respiratory system, and neuromuscular system during successful oral feeding. Delayed or disrupted development in any one system may result in prolonged oral feeding maturation. Many current assessment tools and interventions focus on the suck, swallow, breathe reflex required for feeding safety, but lack assessment of other developmental milestones required for feeding readiness, such as sensory integration and hunger signaling. Major gaps in knowledge exist between data generated from assessment tools and how best to integrate these findings into clinical care practice. There is a need for randomized controlled clinical trials (RCTs) to fill these knowledge gaps and to identify which populations respond to each targeted therapy. We must balance optimizing developmental windows to expedite feeding maturation, while avoiding risks of developing feeding aversion or worsening respiratory disease. In this review, we will address the complexity of neonatal feeding, review assessment tools and interventions for feeding safety and developmental readiness, and propose an individualized, multi-faceted approach to oral feeding evaluation and intervention.
Complexities of Oral Feeding
Oral feeding is the most complex neurodevelopmental task of the newborn.1 Sustained, successful oral feeding involves integrated sensory input from touch, vision, olfaction, and taste. In addition, motor output must coordinate safe and simultaneous sucking, swallowing, and airway protection, while the CNS must inform memory and hunger signaling mechanisms.2 Feeding in neonates also includes caregiver-infant interactions to support bonding between parent and child and requires recognition of infant feeding cues.1 Given the intricate interplay between the CNS, respiratory system, and neuromuscular system required for oral feeding success, it is not surprising that the majority of preterm infants confront feeding challenges or that their ability to orally feed is a major determinant of hospital length of stay. Identifying which system(s) is prohibiting oral feeding success remains a significant challenge for neonatal caregivers.
Importance of Developing Oral Feeding Skills
Understanding the developmental limitation to a newborn’s oral feeding success may inform both the short- and long-term health and developmental outcomes for the infant.3,4 For example, developmental pathways required for oral feeding lay the foundation for the development of speech emergence. While structural defects, such as a cleft lip and/or palate, may delay feeding in the neonatal period and impact speech emergence due to associated hearing deficits, one of the first indications that a newborn without facial anomalies may have delayed development in speech is his or her ability to feed in the neonatal period.5 The ability to successfully feed and speak is dependent upon shared oral motor and neurological pathways. Recent research has shown that salivary gene expression of the forkhead box protein 2 (FOXP2) correlates with oral feeding success in the preterm infant.5 Conversely, mutations in this gene have been linked to speech-language delays.6 Furthermore, infants with feeding difficulties are at risk for feeding-related readmissions, such as failure to thrive, leading to increased health-care-related costs and morbidities,7 and families of infants with feeding difficulties often struggle daily for extended periods of time to ensure that their infant can consume the adequate amount of calories needed for appropriate growth. This level of familial stress is significant and should not be overlooked.8 Thus, not only is oral feeding a basic requirement for most infants prior to discharge from the NICU, development of these skills can inform future growth and developmental success.
Feeding and Breathing: The Need for Randomized Controlled Trials
The most common limitation to the initiation of oral feeding trials in the premature neonatal population is respiratory compromise. Infants who require respiratory support such as continuous positive airway pressure (CPAP) or high flow nasal cannula (HFNC) are either prohibited or limited from participating in oral feeding attempts due to the increased risk of aspiration.9 When, and if, an infant should be allowed to feed while on significant respiratory support remains unknown. Great variation in clinical practices exists across NICUs with no clear consensus regarding safety or risk of morbidity. Determining when and if an infant should be allowed to orally feed while on moderate respiratory support (CPAP  5L/min) will require randomized controlled clinical trials whereby infants, stratified by post-menstrual age (PMA), are randomized to attempt or not attempt oral feeding trials. Episodes of desaturation, aspiration, and cardiorespiratory instability, along with PMA at which full oral feeding success is obtained and the development of feeding aversions will need to be recorded and compared between groups. Trials will likely need to be multi-center and large enough to account for variables that may affect feeding success including sex, gestational age and co-morbidities. Only when such trials are conducted will the field have the necessary data to inform practice and improve feeding outcomes.
5L/min) will require randomized controlled clinical trials whereby infants, stratified by post-menstrual age (PMA), are randomized to attempt or not attempt oral feeding trials. Episodes of desaturation, aspiration, and cardiorespiratory instability, along with PMA at which full oral feeding success is obtained and the development of feeding aversions will need to be recorded and compared between groups. Trials will likely need to be multi-center and large enough to account for variables that may affect feeding success including sex, gestational age and co-morbidities. Only when such trials are conducted will the field have the necessary data to inform practice and improve feeding outcomes.
Recently, Dumpa et al,9 published a retrospective, pre-post analysis study examining feeding morbidities between those infants who were and were not allowed to orally feed on CPAP. Their study demonstrated that infants who were prohibited from feeding while on CPAP learned to orally feed at similar post-menstrual ages than those infants who were allowed to feed while on respiratory support. These data suggest that oral feeding on CPAP merely resulted in protracted, less efficient, oral feeding attempts. This study demonstrates the need to better understand the balance between optimization of developmental windows when the newborn is receptive to oral feeding trials, with the risk of worsening lung disease, feeding aversion, and failure to thrive. There is an imperative to perform both observational outcome studies, as well as RCTs, to systematically monitor outcome measures that can be used to define safety parameters and inform care.
Neonatal Phenotypes and Oral Feeding Challenges
Beyond premature infants, NICUs care for a wide variety of patients with varying phenotypes that impact feeding ability. Infants with facial anomalies, congenital heart disease, or genetic disorders may have difficulty with one or more of the complex neurodevelopment and physical components required for oral feeding.10–13 Infants with facial deformities may have maldeveloped or malformed facial structures, muscles, and/or nerves.10 Infants with congenital heart disease often require mechanical ventilation prohibiting oral feeding altogether or may not be allowed to feed enterally due to concern about gut perfusion.11 Infants with genetic or neurologic conditions affecting tone (ie Down Syndrome,12 neuromuscular disorders13) may have difficulty creating an effective suck. Each of these phenotypes presents unique challenges to caregivers and requires a multidisciplinary team to work with the infant and his or her family to overcome specific physical limitations impacting oral feeding success. Identification of individual barriers to oral feeding provides an important opportunity to integrate targeted, emerging, supportive feeding tools and strategies that are highlighted elsewhere in this review to achieve optimal outcomes.
Interestingly, maternal complications during pregnancy are also known to impact infant feeding skills. Newborns born to women with gestational diabetes have been identified as yet another population of poor oral feeders. One study explored the sucking patterns of infants of diabetic mothers and found that newborns of insulin-treated mothers had fewer sucking bursts, as well as a decreased number of sucks per burst, consistent with a more immature sucking pattern. The authors concluded that these findings suggested that infants of diabetic mothers had neuroimmaturity compared to control subjects.14 However, there is a paucity of literature addressing feeding issues in infants of diabetic mothers, suggesting that alternative hypotheses may explain this unique feeding phenotype and highlighting the need for future research in these newborns.
Infants born to women who abused narcotics during pregnancy also have a unique feeding phenotype whereby they often exhibit an uncoordinated and inefficient sucking pattern, followed by hyperphagia.15,16 A report recently published by Yen et al,16 examined the expression of feeding and reward regulatory genes in infants exposed and not exposed to opioids in utero to better elucidate molecular mechanisms that may be responsible for this unique feeding behavior. They found that the reward gene, dopamine receptor 2 (DRD2), was significantly upregulated in male infants who required pharmacotherapy for withdrawal symptoms compared to their female counterparts and that expression levels of the gene positively correlated to oral consumption in the first week of life. The authors concluded that in opioid exposed infants, food may serve as a surrogate for the reward signaling once provided by opioids in utero and that this molecular pathway may help explain why males are more likely to require pharmacotherapy for withdrawal symptoms than females. While these examples are not intended to be exhaustive of all infants who encounter feeding difficulties in the neonatal period, they do highlight the variety of feeding problems addressed in the NICU and emphasize the need to avoid a universal treatment strategy to address the unique oral feeding issues seen. Currently, many of the assessments and therapies related to oral feeding skills focus solely on nutritive and non-nutritive sucking. Yet, this essential reflex is only one component of oral feeding. Expanding the field to go beyond targeting oral motor skills to consider all aspects of feeding maturity, inclusive of sensory integration and hunger signaling, is needed to advance care.
Feeding Safety Assessments
Assessment of oral motor feeding skills is needed to identify when an infant is ready to safely feed by mouth. It is well established that infants, particularly, preterm infants, will often feed better and earlier at the breast than with the bottle and that non-nutritive sucking at the breast can expedite oral feeding maturation.17 However, if an infant is fed prior to the attainment of a sufficient suck, swallow, breathe reflex, they are placed at risk for aspiration, hypoxia, and increased energy expenditure.1 The need to assess feeding safety has led to the development of numerous clinical and physical oral motor feeding assessment tools that allow caregivers to identify infants who are ready to attempt oral feeding. Clinical assessments often examine the infant at the breast, during bottle feeding, or both and are applicable only to healthy preterm or full-term infants without complex medical conditions.18 Physical assessments have evolved in complexity over time and though initially focused on non-nutritive sucking have now progressed to assessment of nutritive sucking.3,4,18–23 These formal screening instruments allow clinicians, nurses, and therapists to evaluate progression of feeding safety.24 A secondary goal of these oral motor assessments is to predict developmental outcomes.3,4,25,26 In the next section of this review, we will present several clinical and physical assessment modalities and discuss their clinical and developmental prognostic value.
Clinical Oral Motor Assessments
The Neonatal Oral Motor Assessment Scale (NOMAS)27 is the most commonly used clinical oral motor assessment tool reported in the literature.25 NOMAS is an observational tool that focuses on oral motor sucking patterns and can be used over time for early identification of infants at risk for neurodevelopmental delays. It can be used to assess infants during both breast and bottle feeding.18 It requires a three-day training course with recertification every two years for proper administration. NOMAS has been found to be clinically valid in the short term by correlating feeding assessment results with nursing reports and a clinical history of poor feeding.27 However, limitations to NOMAS have included a poor predictive value with regard to feeding development at two years of age,25,26 as well as motor, speech and language, and neurobehavioral developmental delays.25,28
An alternative feeding assessment tool is the infant-driven feeding (IDF) assessment approach that is commonly used in clinical settings. This approach goes beyond safety and strives to incorporate the infant’s interest in feeding and overall neurobehavioral state. Additionally, IDF standardizes documentation of any special caregiver techniques required for successful feeding. The goals of IDF are to foster feeding that is “safe, functional, nurturing, and individually and developmentally appropriate”.29 A review of the literature regarding IDF techniques, however, again highlights a need for RCTs to determine its ability to accurately inform care. Quality improvement projects have shown conflicting results regarding the efficacy of IDF with regard to achievement of full oral feeds and shortened length of stay.30 In 2012 and 2016, Cochrane Reviews examined the utility of these clinical assessment tools to inform feeding practice.31,32 In both analyses, the authors concluded that the field was lacking in informative assessment tools and highlighted the need for future RCTs comparing these instruments with alternative tools and strategies. While clinical assessments of oral motor skills are inexpensive, provide a more objective method to assess feeding readiness and track development of oral motor skills, with some even having the ability to identify infants at risk for developmental delays, the inherent subjectivity of these platforms mandates alternative, supplemental approaches to assessment. Namely, there is a need to develop more objective measures of oral performance including physical measurement of sucking parameters.
Physical Oral Motor Assessments
There are several devices on the market that provide data on an infant’s sucking characteristics. In their earliest iteration, these devices involved simple pressure transducers used to measure sucking, then advanced to include bedside algorithmic analysis of nutritive sucking data to provide real-time assessment of interventions during feeding.3,4,21,22,33 Early devices used a pressure transducer and digital recorder to measure sucking pressure, frequency and duration. Data were processed to form graphic displays of the pressure recordings and were analyzed later frame by frame.3,34 Results showed an increase in sucking pressure, frequency, duration and efficiency as infants matured.34 As for the prognostic value of objective sucking measures, Mizuno and colleagues showed that abnormal sucking patterns and failure to show improvement in sucking patterns correlated to poor neurodevelopmental outcomes at 18 months of age.3 Additionally, sucking patterns were more predictive of neurodevelopmental outcomes than were cranial head ultrasounds or neurologic assessments.3 Medoff-Cooper et al used a pressure transducer and suck maturity index (composite score of number of sucks, mean number of sucks per burst, and mean pressure maximum across all sucking bursts), at 34 and 40 weeks’ PMA, and demonstrated a correlation with 12-month developmental outcomes.4 The limitations of the aforementioned studies are that these devices did not provide real-time data interpretation of suck patterns.
Emerging technology attempts to address these limitations. The nfant® Feeding Solution (NFANT Labs, Marietta GA, USA) provides data during feeding that allows caregivers to intervene to improve feeding performance.21 The device consists of a disposable nfant coupling device that connects a bottle to a standard nipple. A sensor is connected to the coupling device and measures nipple movement. Real-time data on nipple movement can be displayed on a mobile application that allows for immediate feedback on feeding performance and intervention.21,22,33 Additionally, these data allow for analysis of how sucking patterns change for an infant throughout the feed.21 Algorithms applied to data collected after each session are used to describe suck patterns and characteristics such as frequency, amplitude, and smoothness.22,33 One of the limitations of the nfant® Feeding Solution is that it cannot be used to assess infants while breastfeeding, however the device can provide an overall assessment of suck dynamics and maturation. Studies have shown changes in suck characteristics over time in a single infant, as well as different characteristics in preterm and full-term infants. Contrary to the findings of Mizuno34 regarding sucking patterns, Capilouto et al demonstrated that preterm infants had higher suck frequency, shorter suck duration, and lower suck smoothness compared to their full-term counterparts.22 As we learn more about how suck characteristics change with infant development, such characteristics may help track maturation of feeding skills over time and identify infants at risk feeding and developmental delays.
Oral Motor Interventions
In addition to feeding assessment tools, many interventions have been developed in hopes of finding a treatment that leads to earlier achievement of oral feeds. As many of the feeding readiness screening tools have focused on infant sucking skills, so, too, have feeding therapies. Therapies have progressed from simple bedside clinical oral motor interventions to technology based somatosensory stimulation.11,20,35 Care-giver oral motor intervention in infants with congenital heart disease reduced length of stay and increased the percentage of patients who achieved full oral feeding at the time of discharge, although the differences were not statistically significant.6 Additionally, an oral stimulation program, which consisted of stroking perioral and intraoral structures in preterm infants led to achievement of full oral feedings one week earlier, greater overall intake and improved rate of milk transfer.35 A meta-analysis showed that these simple oral motor interventions reduced the time of transition from tube feeding to full oral feeding, shortened hospitalization, and increased feeding efficiency, suggesting that these bedside interventions may improve oral feeding.36 Advancement in technology has led to the development of the NTrainer System (Innara Health, Olathe, Kansas, USA), which delivers patterned oral somatosensory stimulation to train the premature infant how to transition from a non-nutritive to a more mature nutritive sucking pattern. Infants exposed to the NTrainer showed vast improvement in non-nutritive sucking parameters compared to their controls. Additionally, daily percentage of oral feeding increased in the NTrainer group.20
Emerging Technology
As new technology continues to make its way into the diagnosis and treatment of neonates, the field must evaluate the utility and clinical applicability of these advances to deliver accurate and cost-effective care. For instance, videofluoroscopic swallowing studies are currently reserved for a select, high-risk, neonatal population, due to concerns for radiation exposure in the newborn and the need for trained staff to safely administer and expertly interpret the study. New technology has allowed for fiberoptic endoscopic evaluation of swallowing (FEES), a radiation-free alternative to the videofluoroscopic swallowing study that provides direct visualization of the pharynx and larynx through a transnasal fiberoptic laryngoscope at the bedside. This approach allows providers to detect penetration and aspiration and receive immediate feedback on bedside interventions such as position changes and different nipple flow. A recent retrospective study looked at feeding related desaturations due to presumed aspiration in 62 premature infants. Seventy-one percent of subjects were found to have aspiration and/or penetration. Based on the FEES assessment, several treatments were recommended and there was a 61% reduction in desaturations, compared to a 29% reduction in patients without aspiration as a cause of desaturations.37 While this technology can transform the care of neonates, there is a need for more quality studies to examine the best application of such advances.
A recent, exciting area of discovery has been the use of neonatal salivary gene expression profiles to assess feeding readiness in the newborn. As highlighted throughout this review, achievement of oral feeding is not solely dependent on the development of a mature suck but is also dependent upon maturation of appetite signaling and sensory input. Historically, gaining access to such information in the developing newborn was seemingly impossible. Using mere microliters of neonatal saliva, our laboratory has demonstrated that a wealth of developmental information, as it directly relates to oral feeding, can be assessed in real-time. Through a series of publications and observational studies, our laboratory has demonstrated that saliva can simultaneously provide real-time information on the gene expression of multiple developmenal domains that inform feeding readiness. Initial research has shown that over 2000 genes related to feeding, digestion, and development were expressed in neonatal saliva and were significantly up- or down-regulated as infants gained oral feeding skills.38 Additional work identified a key modulator of hunger signaling, the neuropeptide Y2 receptor, NPY2R. In a cohort of over 100 neonatal subjects, salivary expression of NPY2R was found to have a 95% positive predictive value in identifying infants with an immature oral feeding pattern.39 This research led to the development of a salivary feeding diagnostic assay based upon the salivary profiles of an additional 360 preterm and term neonates.40 The platform is composed of five genes representative of hunger signaling, sensory integration and facial development and is the basis for an ongoing National Institutes of Health randomized controlled clinical trial.41 If successful, the platform holds great promise for improving feeding outcomes by identifying infants with specific developmental delays that would allow for targeted therapies specific to that neonate in order to improve short- and long-term outcomes. Such interventions would include increased skin-to-skin in infants lagging in sensory integration, implementation of training devices such as the NTrainer in infants with a delayed nutritive suck progression pattern, or closer long-term monitoring for infants with disrupted hypothalamic signaling affecting hunger and satiety signaling pathways who may be at risk for failure to thrive in the first months of life (Figure 1). Salivary profiles may also inform novel therapies and properly identify those infants who would most benefit from them.
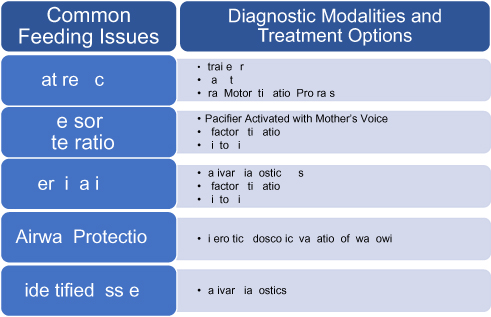 |
Figure 1 Common feeding issues and their diagnostic modalities and treatment options. |
Novel Therapies
Novel therapies have focused on the importance of sensory integration to expedite feeding. Use of a pacifier-activated music player (PAM) with mother’s voice increased oral feeding rate, volume of oral intake and number of oral feedings following five days of therapy. Additionally, the use of PAM with mother’s voice led to achievement of full volume feeds seven days earlier than infants in the control group.42 In the follow-up study of feeding outcomes, control infants demonstrated a statistically significant increase in parental report of problems chewing solid food, hospitalizations related to feeding problems in the first year of life and aspiration events requiring intervention in the first three months of life.43 A study on olfactory stimulation found that there may be a developmental window in which olfactory stimulation with maternal breast milk may improve feeding outcomes. Infants born at  31 weeks’ gestation who received olfactory stimulation with their mother’s milk during feeding learned to feed sooner than age-matched controls. However, the effect was lost in infants born at >31 weeks’ gestation suggesting a window for optimal olfactory stimulation to improve oral feeding outcome.44
31 weeks’ gestation who received olfactory stimulation with their mother’s milk during feeding learned to feed sooner than age-matched controls. However, the effect was lost in infants born at >31 weeks’ gestation suggesting a window for optimal olfactory stimulation to improve oral feeding outcome.44
The Need for an Individualized Developmental Approach
While some interventions have been shown to be effective, the field is in need of an individualized, multifaceted approach to feeding therapy. We can no longer take a one-size-fits all approach to neonatal feeding. Using neonatal salivary gene expression analysis, providers may be able to identify barriers individual infants face and provide targeted and developmentally appropriate interventions to promote oral feeding skills (Figure 1). Additionally, salivary gene expression analysis may help to identify those infants who are safe to start oral feeding, reducing morbidities associated with premature feeding. Providers can track expression of genes related to the development of cranial nerves and appetite regulation to optimize the timing of olfactory, auditory, and oral therapies for each individual infant. Saliva may also allow us to identify infants at risk for future developmental delays such as delayed speech emergence and allow for targeted intervention to improve long-term outcomes. Individualized identification of barriers to feeding may also inform the care of our NICU graduates upon discharge from the hospital. One study from Italy highlighted the need for guidelines with regard to the introduction of complimentary foods in low birthweight populations.45 As our graduates continue with catch up growth and development through two years of age, nutrition and early intervention are of utmost importance. Targeted developmental interventions and developmentally appropriate introduction of complimentary foods will optimize growth and development beyond the NICU.
Conclusions
There are many exciting and emerging assessment tools to evaluate infant oral feeding readiness and safety. Training devices, sensory tools, developmental platforms, and safety assessments all play an important role in improving feeding outcomes and reducing feeding morbidities in this at-risk population. However, future randomized controlled studies are needed to compare the efficacy of these clinical and technologic assessments to determine which assessment best identifies infants with feeding difficulties and those at risk for developmental delays. Additionally, studies are needed to determine which populations within the NICU benefit from each intervention and if there is a developmental window in which interventions are most effective. There is also a need to determine the clinical utility of incorporating salivary gene expression profiles into neonatal care. Many of these assessments and interventions can be used for both breastfeeding and bottle feeding infants although there is a gap in physical motor assessments for babies actively breastfeeding. Individualized approaches to improve neonatal oral feeding outcomes can only be achieved when due diligence and scientific rigor are performed. Identifying which interventions will most benefit which infant is the challenge before us. Only then can we truly impact and improve feeding outcomes in the premature neonatal population.
Funding
NICHD R01 HD086088.
Disclosure
Dr Jill Maron is a Principal Investigator on a NICHD-funded R01 trial: R01 HD086088; Somatosensory Modulation of Salivary Gene Expression and Oral Feeding in Preterm Infants. The authors report no other conflicts of interest in this work.
References
1. Delaney AL, Arvedson JC. Development of swallowing and feeding: prenatal through first year of life. Dev Disabil Res Rev. 2008;14(2):105–117. doi:10.1002/ddrr.16
2. Suarez AN, Noble EE, Kanoski SE. Regulation of memory function by feeding-relevant biological systems: following the breadcrumbs to the hippocampus. Front Mol Neurosci. 2019;12. doi:10.3389/fnmol.2019.00101
3. Mizuno K, Ueda A. Neonatal feeding performance as a predictor of neurodevelopmental outcome at 18 months. Dev Med Child Neurol. 2005;47(5):299–304. doi:10.1017/s0012162205000587
4. Medoff-Cooper B, Shults J, Kaplan J. Sucking behavior of preterm neonates as a predictor of developmental outcomes. J Dev Behav Pediatr. 2009;30(1):16–22. doi:10.1097/DBP.0b013e318196b0a8
5. Zimmerman E, Maki M, Maron J. Salivary FOXP2 expression and oral feeding success in premature infants. Mol Case Stud. 2016;2(1):a000554. doi:10.1101/mcs.a000554
6. Hurst JA, Baraitser M, Auger E, Graham F, Norell S. An extended family with a dominantly inherited speech disorder. Dev Med Child Neurol. 1990;32(4):352–355. doi:10.1111/j.1469-8749.1990.tb16948.x
7. Underwood MA, Danielsen B, Gilbert WM. Cost, causes and rates of rehospitalization of preterm infants. J Perinatol. 2007;27(10):614–619. doi:10.1038/sj.jp.7211801
8. Lefton-Greif MA, Okelo SO, Wright JM, Collaco JM, McGrath-Morrow SA, Eakin MN. Impact of children’s feeding/swallowing problems: validation of a new caregiver instrument. Dysphagia. 2014;29(6):671–677. doi:10.1007/s00455-014-9560-7
9. Dumpa V, Kamity R, Ferrara L, Akerman M, Hanna N. The effects of oral feeding while on nasal continuous positive airway pressure (NCPAP) in preterm infants. J Perinatol. 2020. doi:10.1038/s41372-020-0632-2
10. Caron CJJM, Pluijmers BI, Joosten KFM, et al. Feeding difficulties in craniofacial microsomia: a multicenter retrospective analysis of 755 patients. J Craniomaxillofac Surg. 2018;46(10):1777–1782. doi:10.1016/j.jcms.2018.07.017
11. Indramohan G, Pedigo TP, Rostoker N, Cambare M, Grogan T, Federman MD. Identification of risk factors for poor feeding in infants with congenital heart disease and a novel approach to improve oral feeding. J Pediatr Nurs. 2017;35:149–154. doi:10.1016/j.pedn.2017.01.009
12. Stanley MA, Shepherd N, Duvall N, et al. Clinical identification of feeding and swallowing disorders in 0–6 month old infants with down syndrome. Am J Med Genet A. 2019;179(2):177–182. doi:10.1002/ajmg.a.11
13. van den Engel-hoek L, de Groot IJM, de Swart BJM, Erasmus CE. Feeding and swallowing disorders in pediatric neuromuscular diseases: an overview. J Neuromuscul Dis. 2015;2(4):357–369. doi:10.3233/JND-150122
14. Bromiker R, Rachamim A, Hammerman C, Schimmel M, Kaplan M, Medoff-Cooper B. Immature sucking patterns in infants of mothers with diabetes. J Pediatr. 2006;149(5):640–643. doi:10.1016/j.jpeds.2006.07.034
15. Shephard R, Greenough A, Johnson K, Gerada C. Hyperphagia, weight gain and neonatal drug withdrawal. Acta Paediatr. 2002;91(9):951–953. doi:10.1111/j.1651-2227.2002.tb02883.x
16. Yen E, Kaneko-Tarui T, Ruthazer R, Harvey-Wilkes K, Hassaneen M, Maron JL. Sex-dependent gene expression in infants with neonatal opioid withdrawal syndrome. J Pediatr. 2019;214:60–65. doi:10.1016/j.jpeds.2019.07.032
17. John H, Suraj C, Padankatti S, Sebastian T, Rajapandian E. nonnutritive sucking at the mother’s breast facilitates oral feeding skills in premature infants: a pilot study. Adv Neonat Care. 2018;19:110–117. doi:10.1097/ANC.0000000000000545
18. Bickell M, Barton C, Dow K, Fucile S. A systematic review of clinical and psychometric properties of infant oral motor feeding assessments. Dev Neurorehabil. 2018;21(6):351–361. doi:10.1080/17518423.2017.1289272
19. Song D, Jegatheesan P, Nafday S, et al. Patterned frequency-modulated oral stimulation in preterm infants: a multicenter randomized controlled trial. PLoS One. 2019;14(2):e0212675. doi:10.1371/journal.pone.0212675
20. Barlow SM, Finan DS, Lee J, Chu S. Synthetic orocutaneous stimulation entrains preterm infants with feeding difficulties to suck. J Perinatol. 2008;28(8):541–548. doi:10.1038/jp.2008.57
21. Capilouto GJ, Cunningham TJ. Objective assessment of a preterm infant’s nutritive sucking from initiation of feeding through hospitalization and discharge. Neonatal Intensive Care. 2016;29(1):40–45.
22. Capilouto GJ, Cunningham TJ, Giannone PJ, Grider D. A comparison of the nutritive sucking performance of full term and preterm neonates at hospital discharge: a prospective study. Early Hum Dev. 2019;134:26–30. doi:10.1016/j.earlhumdev.2019.05.007
23. Pineda R, Dewey K, Jacobsen A, Smith J. Non-nutritive sucking in the preterm infant. Amer J Perinatol. 2019;36(3):268–276. doi:10.1055/s-0038-1667289
24. Gennattasio A, Perri E, Baranek D, Rohan A. Oral feeding readiness assessment in premature infants. MCN Am J Matern Child Nurs. 2015;40(2):96–104. doi:10.1097/NMC.0000000000000115
25. Longoni L, Provenzi L, Cavallini A, Sacchi D, Scotto Di Minico G, Borgatti R. Predictors and outcomes of the Neonatal Oral Motor Assessment Scale (NOMAS) performance: a systematic review. Eur J Pediatr. 2018;177(5):665–673. doi:10.1007/s00431-018-3130-1
26. Zarem C, Kidokoro H, Neil J, Wallendorf M, Inder T, Pineda R. Psychometrics of the neonatal oral motor assessment scale. Dev Med Child Neurol. 2013;55(12):1115–1120. doi:10.1111/dmcn.12202
27. Braun MA, Palmer MM. A pilot study of oral-motor dysfunction in “at-risk” infants. Phys Occup Ther Pediatr. 1985;5(4):13–26. doi:10.1080/J006v05n04_02
28. Tsai S-W, Chen C-H, Lin M-C. Prediction for developmental delay on Neonatal Oral Motor Assessment Scale in preterm infants without brain lesion. Pediatr Int. 2010;52(1):65–68. doi:10.1111/j.1442-200X.2009.02882.x
29. Ludwig SM, Waitzman KA. Changing feeding documentation to reflect infant-driven feeding practice. Newborn Infant Nurs Rev. 2007;7(3):155–160. doi:10.1053/j.nainr.2007.06.007
30. Settle M, Francis K. Does the infant-driven feeding method positively impact preterm infant feeding outcomes? Adv Neonatal Care. 2019;19(1):51–55. doi:10.1097/ANC.0000000000000577
31. Crowe L, Chang A, Wallace K. Instruments for assessing readiness to commence suck feeds in preterm infants: effects on time to establish full oral feeding and duration of hospitalisation. Cochrane Database Syst Rev. 2016;(8):CD005586. doi:10.1002/14651858.CD005586.pub3
32. Crowe L, Chang A, Wallace K. Instruments for assessing readiness to commence suck feeds in preterm infants: effects on time to establish full oral feeding and duration of hospitalisation. Cochrane Database Syst Rev. 2012;(4). doi:10.1002/14651858.CD005586.pub2
33. Capilouto G, Cunningham T, Mullineaux D, Tamilia E, Papadelis C, Giannone P. Quantifying neonatal sucking performance: promise of new methods. Semin Speech Lang. 2017;38(02):147–158. doi:10.1055/s-0037-1599112
34. Mizuno K, Ueda A. The maturation and coordination of sucking, swallowing, and respiration in preterm infants. J Pediatr. 2003;142(1):36–40. doi:10.1067/mpd.2003.mpd0312
35. Fucile S, Gisel EG, Lau C. Effect of an oral stimulation program on sucking skill maturation of preterm infants. Dev Med Child Neurol. 2005;47(3):158–162. doi:10.1017/s0012162205000290
36. Tian X, Yi L-J, Zhang L, et al. Oral motor intervention improved the oral feeding in preterm infants: evidence based on a meta-analysis with trial sequential analysis. Medicine. 2015;94(31):e1310. doi:10.1097/MD.0000000000001310
37. Vetter‐Laracy S, Osona B, Roca A, Peña‐Zarza JA, Gil JA, Figuerola J. Neonatal swallowing assessment using fiberoptic endoscopic evaluation of swallowing (FEES). Pediatr Pulmonol. 2018;53(4):437–442. doi:10.1002/ppul.23946
38. Maron JL. Insights into neonatal oral feeding through the salivary transcriptome. Int J Pediatr. 2012;2012:195153. doi:10.1155/2012/195153
39. Maron JL, Johnson KL, Dietz JA, Chen ML, Bianchi DW. Neuropeptide Y2 receptor (NPY2R) expression in saliva predicts feeding immaturity in the premature neonate. PLoS One. 2012;7(5):e37870. doi:10.1371/journal.pone.0037870
40. Khanna P, Maron JL, Walt DR. Development of a rapid salivary proteomic platform for oral feeding readiness in the preterm newborn. Front Pediatr. 2017;5:268. doi:10.3389/fped.2017.00268
41. Barlow SM, Maron JL, Alterovitz G, et al. Somatosensory modulation of salivary gene expression and oral feeding in preterm infants: randomized controlled trial. JMIR Res Protoc. 2017;6(6):e113. doi:10.2196/resprot.7712
42. Chorna OD, Slaughter JC, Wang L, Stark AR, Maitre NL. A pacifier-activated music player with mother’s voice improves oral feeding in preterm infants. Pediatrics. 2014;133(3):462–468. doi:10.1542/peds.2013-2547
43. Hamm EL, Chorna OD, Stark AR, Maitre NL. Feeding outcomes and parent perceptions after the pacifier-activated music player with mother’s voice trial. Acta Paediatr. 2015;104(8):e372–e374. doi:10.1111/apa.13030
44. Davidson J, Ruthazer R, Maron JL. optimal timing to utilize olfactory stimulation with maternal breast milk to improve oral feeding skills in the premature newborn. Breastfeed Med. 2019;14(4):230–235. doi:10.1089/bfm.2018.0180
45. Baldassarre ME, Di Mauro A, Pedico A, et al. Weaning time in preterm infants: an audit of italian primary care paediatricians. Nutrients. 2018;10(5):616. doi:10.3390/nu10050616
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.