Back to Journals » Journal of Healthcare Leadership » Volume 15
Individual Characteristics That Promote or Prevent Psychological Safety and Error Reporting in Healthcare: A Systematic Review
Authors Wawersik DM, Boutin Jr ER, Gore T, Palaganas JC
Received 3 April 2022
Accepted for publication 13 July 2022
Published 17 April 2023 Volume 2023:15 Pages 59—70
DOI https://doi.org/10.2147/JHL.S369242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
Dawn M Wawersik,1,2 Emile R Boutin Jr,1 Teresa Gore,3 Janice C Palaganas1,4
1MGH Institute of Health Professions, Boston, MA, USA; 2Henry Ford College, Dearborn, MI, USA; 3Nova Southeastern University, Fort Lauderdale, FL, USA; 4Harvard Medical School, Boston, MA, USA
Correspondence: Dawn M Wawersik, Email [email protected]
Background: Healthcare errors continue to be a safety issue and an economic burden that causes death, increased length of stays, and emotional trauma to families and the person who commits the error. Speaking up and error reporting within a safety culture can reduce the incidence of error; however, this is complex and multifaceted.
Aim: This systematic review investigates individual characteristics that support or prevent speaking up behaviors when adverse events occur. This study further explores how organizational interventions designed to promote error reporting correlate to individual characteristics and perceptions of psychological safety.
Methods: A systematic review of peer-reviewed articles in healthcare that contain characteristics of an individual that promote or prevent error reporting was conducted. The search yielded 1233 articles published from 2015 to 2021. From this set, 81 full-text articles were assessed for eligibility and ultimately extracted data from 28 articles evaluated for quality using Joanna Briggs Institute critical appraisal tools©.
Principal Findings: The primary themes for individual character traits, values, and beliefs that influence a person’s decision to speak up/report an error include self-confidence and positive perceptions of self, the organization, and leadership. Education, experience and knowledge are sub themes that relate to confidence. The primary individual characteristics that serve as barriers are 1) self-preservation associated with fear and 2) negative perceptions of self, the organization, and leadership.
Conclusion: The results show that an individual’s perception of their environment, whether or not it is psychologically safe, may be impacted by personal perceptions that stem from deep-seated personal values. This exposes a crucial need to explore cultural and diversity aspects of healthcare error reporting and how to individualize interventions to reduce fear and promote error reporting.
Keywords: speaking up, error reporting, psychological safety, healthcare error, individual characteristics, systematic review
Introduction
Healthcare errors profoundly and negatively impact patients, families, healthcare providers, organizations, and communities.1 The World Health Organization2 estimates that 2.6 million deaths occur per year in low- and middle-income countries, and errors cause harm to one out of 10 patients in high-income countries, half of which are preventable One possible and powerful mechanism to prevent error is to report errors after the adverse event or speak up at the moment to prevent the event from occurring.3 However, research has shown that the fear of consequences for speaking up or reporting often outweighs the motivation to do so.4
In response to the burden of healthcare errors, the Joint Commission5 issued a sentinel event alert and a call to action to create ‘safety cultures’ in healthcare organizations, including error reporting systems and psychologically safe environments. Psychological safety is a belief that it is safe speak up and is a critical component of any healthcare team or organization to promote the free flow of ideas, innovations, and difficult conversations.6
Research shows that people are more likely to speak up if they feel psychologically safe.7 However, due to human factors, psychologically safe environments cannot exist all the time, and errors are inevitable.6 Therefore, healthcare leadership must find ways to individualize interventions to help people overcome fear to speak up and report errors.
Unfortunately, there is a paucity in the literature regarding the impact of individual characteristics that promote speaking up behaviors as they relate to organizational culture and interventions. This systematic review investigates the individual characteristics that drive decision-making when faced with the decision whether or not to report an error. Ultimately, the goal is to encourage organizational leadership to narrow the gap between individual beliefs and administrative policy to support error reporting. To better understand the literature, we sought to answer:
- What individual characteristics promote psychological safety and error reporting in healthcare?
- What individual characteristics serve as barriers to psychological safety and healthcare error reporting?
Definitions
For the purposes of this review, the researchers define individual characteristics as aspects of a person’s knowledge, skills, behaviors, and attitudes that make up an individual’s personality that determines problem-solving, decision-making, and influence a person’s perceptions and actions. We also consider the term organizational factors to be the influences of corporate culture, policies, procedures, or practices that affect processes and actions taken during an event.
The Joint Commission5 describes three elements of safety culture as 1) Just culture: people are encouraged to report safety issues but are held accountable for reckless behaviors, 2) Reporting culture: people report errors and near misses, 3) Learning Culture: a culture in which the organization is willing to learn from errors and make necessary changes as needed.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for systematic reviews guidelines (PRISMA) 2020 guidelines.8 Systematic reviews allow the researcher to identify problems in current research or generate new theories.8 The reviewers chose the systematic review process because error reporting is a well-researched area in healthcare. Therefore, the abundance of the literature for a scoping review would be too broad and time-consuming to narrow down, considering the specific nature of the research questions.
Search Strategies
This study is a systematic review of the research literature published between January 2015 and May 2021. The initial search returned over 15,000 results, which resulted in adding 2015 as a year limitation to the inclusion criteria. Limiting the year to 2015 limited the results to a manageable number and ensured the most current research results, which is essential due to the rapidly evolving nature of this topic.
The search strategy was developed and reviewed by an expert librarian. Databases searched included ERIC, PubMed, CINAHL, CINAHL Complete, and Medline. In addition, the references of included studies were examined for possible inclusion (ie, ancestry search). Broad search terms were used due to the lack of a standardized definition for medical error9 and many synonyms for both medical errors and speaking up. For this reason, we included terms used synonymously in the literature, such as “healthcare error” and “voice behaviors.” A complete list of search terms can be seen in Appendix A.
The final search was conducted on May 21, 2021, and returned 3871 results, plus 25 articles from the ancestry search. Next, the principal investigator reviewed titles, removed irrelevant articles, and uploaded the remaining 1269 articles to Covidence©, an online systematic review application, for screening.10
Inclusion & Exclusion Criteria
After removing 36 duplicates, 1233 studies were screened against title and abstract based on inclusion and exclusion criteria agreed upon by the reviewers.
Articles were eligible for inclusion if:
- the population described or studied included at least one healthcare professional or pre-licensure learner (eg, medical students, nursing students),
- the title or abstract-mentioned psychological safety, speaking up behaviors, error reporting or similar (ie, medication error, adverse event, incident report), just culture or equivalent (eg, blame-free, non-punitive, fair blame culture),
- published in a peer-reviewed journal in the years 2015–2021, and
- met quality assessment criteria using Joanna Institute critical appraisal tools.11
Records were excluded if they:
- did not meet the inclusion criteria,
- focused solely on the validation of assessment tools,
- focused on patients or patient outcomes versus employees,
- focused on organizational factors rather than individual or clinician characteristics, or
- were not focused on psychological safety, healthcare error reporting, or speaking up.
Non-research literature, such as opinion papers and continuing education articles, were included providing all other criteria were met. There were no language or country of origin limits.
Screening Process
Two reviewers screened ten titles and abstracts based on the eligibility criteria and met to discuss any disagreements. Once the inclusion/exclusion criteria were determined and interrater reliability was confirmed, independent screening of abstracts was conducted.
In the full-text screening phase, the reviewers selected five articles to screen that differed in methodology and met to discuss any disagreements for interrater reliability. Then, reviewers independently reviewed the full text and met weekly to discuss and resolve conflicts or disputes.
Based on inclusion/exclusion criteria, 1150 articles were excluded, two were not retrieved, and 81 were assessed for full-text eligibility. In addition, references for included articles were screened, and 25 additional items were added via ancestry searches for full-text review. One of those 25 citations was in Spanish. All other citations retrieved were in English. Finally, a total of 78 items were excluded based on exclusion criteria resulting in the inclusion of 28 articles. The PRISMA flow diagram in Figure 1 shows this process.
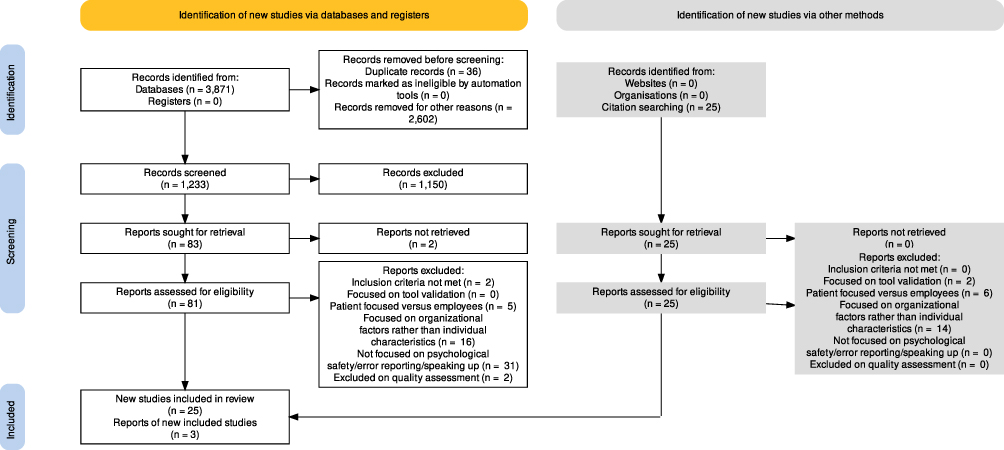 |
Figure 1 Prisma flow diagram. |
Notes: PRISMA flow diagram adapted from Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. Common Creative.8
Data Extraction Process
Two researchers created a data extraction table to capture data relevant to the study’s aim. Table 1 displays the final data extraction table One reviewer read and extracted data for all articles. Two additional researchers were invited to the study, and each read and extracted data from half of the articles, ensuring that two reviewers reviewed each article. Additionally, one researcher, fluent in Spanish, was assigned the one Spanish article, translating extraction data to English for other researchers and the analysis process. All other articles were in English. A fourth reviewer met with the team to discuss themes and resolve conflicts. Consensus was reached on all 28 included articles.
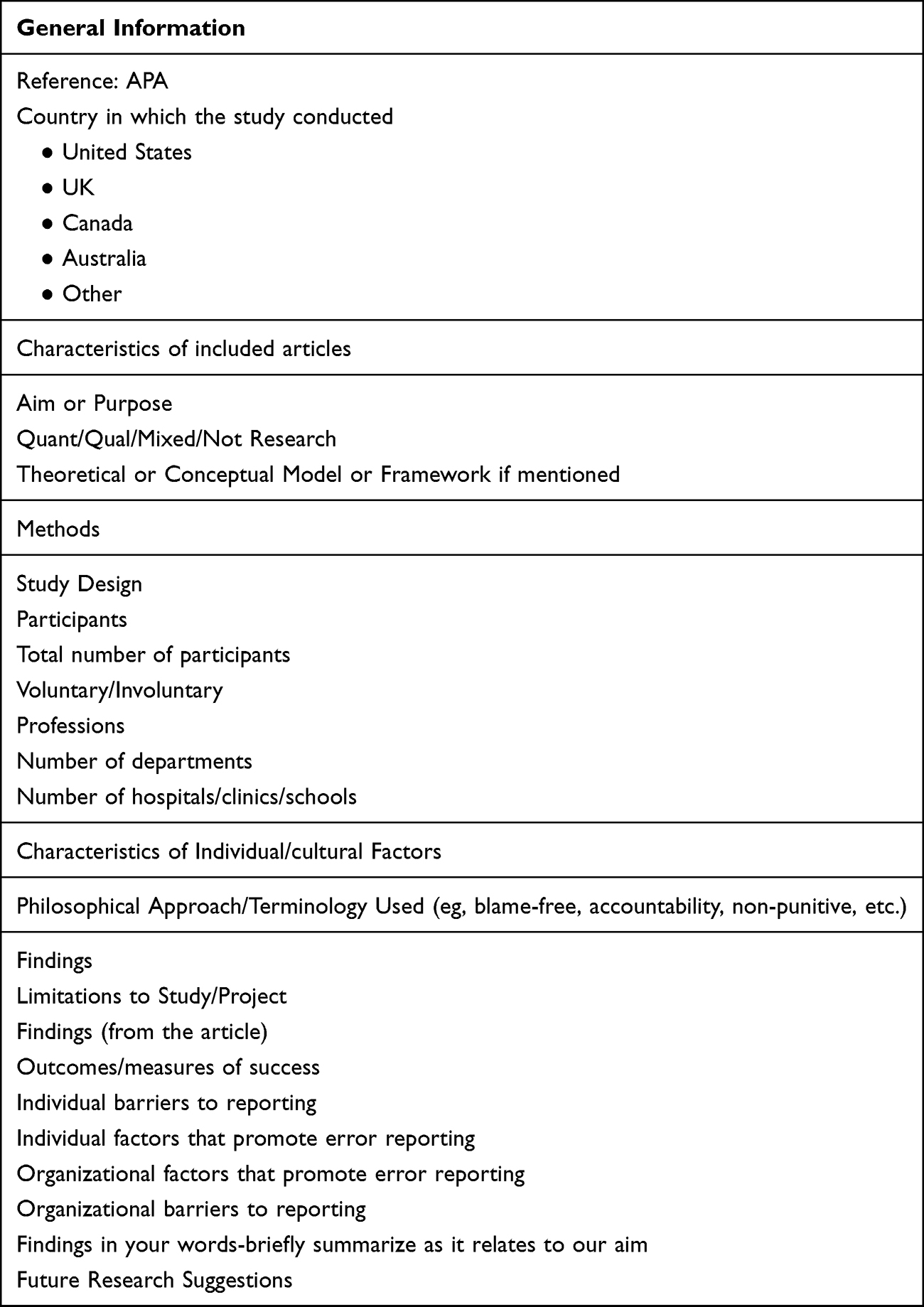 |
Table 1 Data Extraction Table |
Each article was also reviewed to determine the reported outcomes on Kirkpatrick’s level of evaluation. The purpose was to determine what levels of evidence are currently reported in the literature. The Kirkpatrick Levels of evaluation is a globally recognized model for evaluating programs.12 Therefore, we evaluated studies using the same levels; reaction, learning/satisfaction, behavior, results. We also evaluated for return on investment (ROI) from the Phillips model for measuring the impact of healthcare programs.13 Understanding the level of evidence currently in the literature can provide insight as to whether or not interventions are working and cost effective. It also tells us where research is currently focused which will provide a roadmap of where research is needed in regard to evidence on error reporting and speaking up behaviors.
Findings
We identified 28 primary articles that described individual characteristics that promote psychological safety or error reporting barriers. Supplementary Table 1 includes article descriptions, country of origin, research methodologies, and Kirkpatrick’s levels for each included article.
The majority of the studies reported outcomes at Kirkpatrick’s Level 1, reactions, and level 3, behaviors. Two articles were identified at Kirkpatrick‘s level 4 (results).12 None of the studies that met inclusion criteria reported evidence level 2 (learning) or return on investment.
Country of origin was diverse, with ten from the United States (US) and 18 from various other countries. Research methodology also varied with twelve qualitative, ten quantitative approaches, four mixed methods, and two not research (ie, editorials or opinion papers).
Next, we investigated how individual character traits, values, and beliefs influence a person’s decision to speak up/report an error. Table 2 displays the complete list of the most significant individual characteristics that promote error reporting found in the literature.
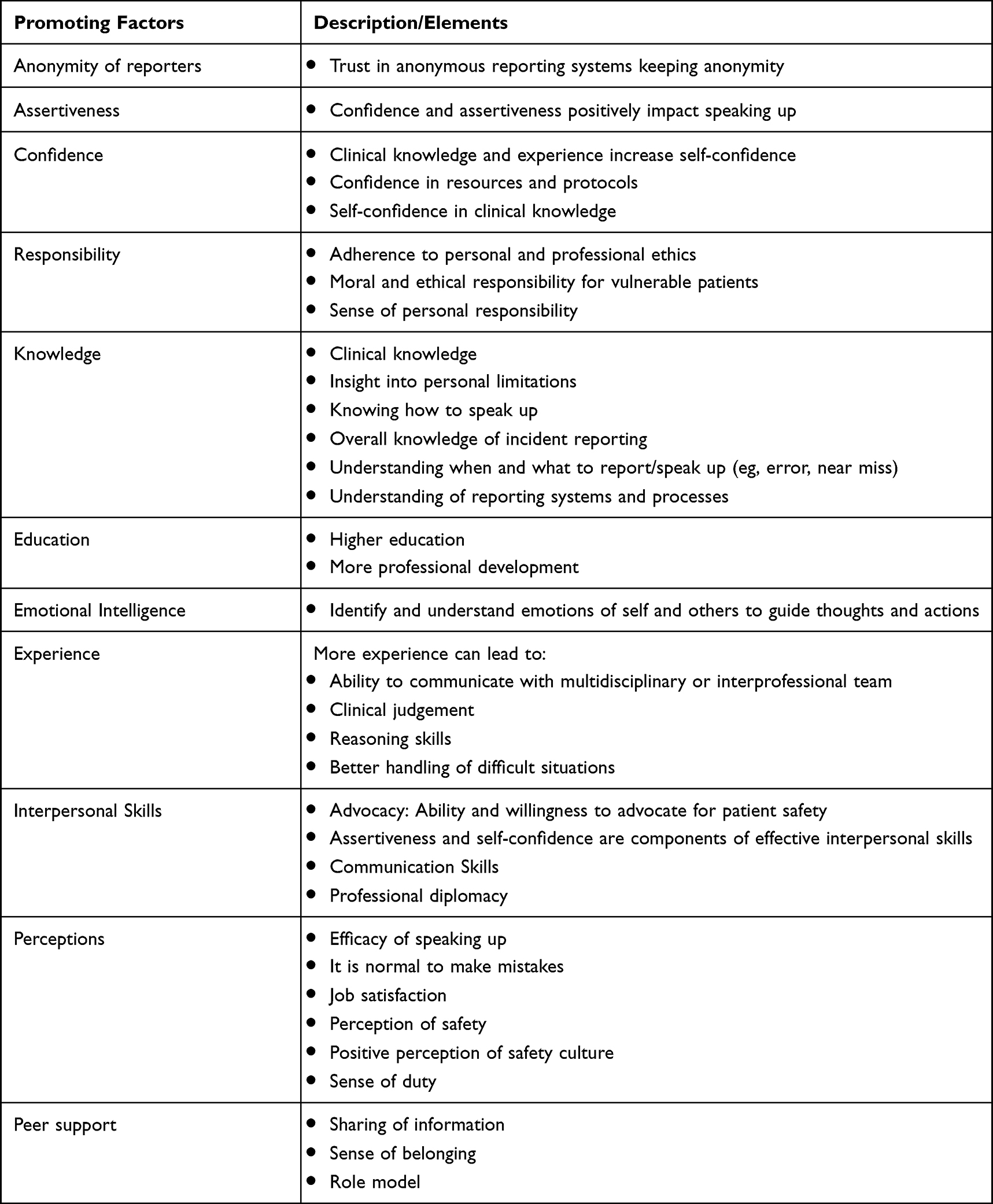 |
Table 2 Themes Identified for Individual Characteristics That Promote Speaking Up/Error Reporting |
We summarize the answers to our research questions focusing on the overarching themes:
Individual Characteristics That Promote Psychological Safety and Error Reporting in Healthcare
The primary themes for individual characteristics that promote reporting are: positive perceptions of self, the organization, and leadership21,25,27,28 and confidence.3,16,18,23 Experience16,18,25,26 and knowledge14,16,18,20,21 are primary sub themes related to confidence.
Positive Perceptions of Self, the Organization, and Leadership
Understanding frames that individuals possess to interpret their surroundings, also considered deep-seated values and beliefs, will help understand perceptions that drive them to report.25 For example, a positive perception of personal safety and the ability to freely express thoughts and ideas without feeling attacked, increases the likelihood of reporting.21,31 In addition, individuals who perceive their role models as supportive, their colleagues as receptive to questions, and mutual respect in the workplace will feel more psychologically safe and are more likely to report.16
Psychological safety and the self-perception of moral and ethical responsibility to advocate for vulnerable patients are also individual characteristics that promote speaking up behaviors.16,25 In addition, people who believe they have a duty to their profession and believe they are making a difference are also more likely to report.25
Confidence
Confidence was identified as a critical factor to promote speaking up.3,16,18,20,23 Aydon et al16 contend that confidence supports assertiveness that, in turn, reinforces speaking up behaviors. In addition, confidence comes with knowledge and experience.18 Shepherd et al18 found that physicians perceived that with more experience, organizational cultural factors have a less negative impact on their ability to learn from errors.
The perception that one can trust organizational protocols and resources15 increases knowledge and, combined with experience, increases self-confidence.16 Trustworthy protocols are especially needed for someone not knowledgeable,15,16 such as a new graduate. Level of confidence further influences other individual characteristics that are essential for error reporting and speaking up. For example, skillful interpersonal communication requires confidence, a skill that is under-developed in many newly graduated health professionals.23 Consequently, training in communication skills will increase confidence.21 In addition, training specifically in handling conflict will also increase confidence, which increases assertiveness, increasing the ability to speak up.16
Knowledge, Education, and Experience Relate to Confidence
The level of an individual’s knowledge is a clear marker for psychological safety in error reporting,14,16,20,21 where lack of knowledge serves as a barrier and more knowledge promotes psychological safety and error reporting. Uncertainty about definitions, unawareness of reporting systems, and lack of knowledge of the process are barriers31 that need to be rectified by the organization.
However, knowledge and education affect error reporting is inconsistent in our findings. On one hand, Vrbjnak et al32 stated that, in some cases, the frequency of reporting was higher among nurses with higher levels of education. On the other hand, Chegini et al29 reported that, in some studies, Associate Degree nurses are more likely to report than the nurses with a higher level of education.
Additionally, Vrbjnak et al32 found evidence that nurses with more professional development and continuing education or advanced nurse training are linked to underreporting.32 Contributing to this evidence, Chegini et al29 cited a study in which managers and staff with higher education are more likely to report. This phenomenon may be explained by the fact that many nurses hold high positions with high degrees and people that hold high-level positions often feel safer.26
Another interesting contradiction: Lee et al24 found that nurse education was not a significant predictor of error reporting. They further noted that years of experience did not substantially impact error reporting.24 However, some studies reported that more work experience resulted in more confidence. More experience also means knowing what to look for and better handling difficult situations. However, Vrbnjak et al32 reported that while some studies show that nurses with more years of experience have a greater fear of consequences, some studies said that more experience means less fear.
Edmonson et al26 found that education and experience affected reporting differently in health professions positions in academic institutions, such as tenured faculty or university administration, versus acute care facility positions. For example, those with tenure and more experience in education positions are more likely to report than non-tenured or newer faculty. Error reporting for those in acute care positions depends more on status and hierarchy.17 The higher the level in the organization, the greater the perception of psychological safety.17,26 This evidence suggests that the nature of a person’s job, duties and position in the hierarchy impacts psychological safety and speaking up.
Individual Characteristics That Serve as Barriers to Error Reporting?
Primary individual characteristic themes for barriers (see Table 3 for a complete list of barriers):
 |
Table 3 Themes Identified for Individual Characteristics That Serve as Barriers to Speaking Up/Error Reporting |
· Self-preservation associated with fear was outlined in 15 articles.
· Negative perceptions of self, the organization, and leadership were discussed in eight of the included articles.
Fear and perceptions are the most common barriers in the literature, emphasizing the need for creating psychologically safe environments to overcome these barriers and facilitate error reporting. Creating supportive environments by building team rapport will improve psychological safety at the team level. For example, learning one another’s names and discussing educational goals, personal successes, and failures establishes a team dynamic and a shared mental model.21 In addition, discussing errors as a team normalizes mistakes as an acceptable part of development.21
Self-Preservation Associated with Fear
Self-preservation related to fear was the most common barrier found in the literature. Specifically, fear of blame,14,23,29,33,36 creating a negative impression,22,28 and fear of negative consequences or repercussions1,3,21,30,33,35,36 were the most common. Previous negative experiences making or reporting an error, such as being labeled a “snitch” or a “tattletale”,23,25 or disciplinary consequences1,3,21,30,33,35 served as self-preservation barriers.32
Negative Perceptions of Self, the Organization, and Leadership
Differing personalities can cause friction and decrease confidence in speaking up.16 In addition, these personality differences may lead to the perception that colleagues are unapproachable or the feeling of a hostile work environment, particularly if there is naming, blaming, or shaming involved.23 Psychological safety and error reporting are also negatively impacted by perceptions of ineffective leadership,26 exhaustion, and heavy workloads,16 contributing to negative feelings and preventing error reporting.
Similarly, if individuals believe that error is inevitable25 or that speaking up does not yield positive change or outcome, they will not report.19,21,30 Additionally, if a person speaks up and receives a negative response or consequence, they are likely not to speak up again. Past experiences drive actions32 and are more powerful than accountability and personal responsibility. In addition, previous experience plays a role in determining perceptions and intent.32 Encountering a negative consequence has a damaging impact on error reporting.1 If past experiences shape perceptions, then it can be assumed that having a bad experience when reporting will negatively affect and prevent reporting again.
Therefore, conflict management training is critical in dealing with someone that spoke up inappropriately.37 When individuals speak up or come forward to report an error, they must be appropriately managed to prevent negatively impacting their perception of speaking up. It is also essential to teach people how to manage a situation where the message was not received or had negative repercussions. It is equally necessary for leadership to teach individuals how to handle a negative reaction or receive backlash after speaking up or reporting.
Finally, the literature calls for anonymous reporting systems.14,32,35 However, other research shows that anonymity breeds distrust and feeds into negative perceptions of the organization and colleagues.38 Current and 360 feedback are anonymous, but anonymity may create inappropriate behavior because the individual that made the error may make incorrect assumptions about the reporter. Instead of reinforcing trust, these assumptions potentially build mistrust. Anonymity is also unhealthy because it sends the wrong message that direct, honest feedback delivered with compassion and sensitivity is harmful and unhealthy.38
Discussion
This study reveals that confidence is integral to error reporting. Healthcare leadership can provide all the appropriate tools but understanding the characteristics that drive individuals’ decision-making processes and meeting them where they are, is essential for these environments to thrive. Educational interventions and training are not enough to improve speaking up behaviors and create psychologically safe environments.4,26 However, some suggestions for creating supportive environments to increase psychological safety begin with developing team familiarity. For example, building interpersonal relationships by learning one another’s names39,40 and discussing educational goals establish a team dynamic and a shared mental model.40 In addition, discussing failures helps to normalize failure to encourage reporting.40
This literature review further reveals that Healthcare error reporting systems success is dependent not only on the organizational culture, policies, and procedures, but also an individual’s ability to feel psychologically safe. Additionally, individuals that are confident, trust leadership, and possess a sense of duty to their profession and responsibility to their patients are more likely to speak up than people who do not have those perceptions. Therefore, it is critical for healthcare leadership to work with individuals to build positive perceptions. Leadership training in how to respond when someone reports or speaks up is critical to building positive perceptions to promote future error reporting and speaking up behaviors.
It is also critical for healthcare organizations to evaluate the effectiveness and value of current speaking up initiatives and error reporting systems. The lack of Kirkpatrick’s level four in the literature, evaluating the benefits of the initiatives, indicates the need to evaluate the impact of current programs on patient safety. Additionally, no included literature investigated the return on investment. Benefit versus cost of error reporting programs and how they relate to patient safety is an essential piece of knowledge needed to know if what we are doing is working.
The findings in this systematic review identifies a gap in current literature regarding the effect of current systems on patient safety but also adds an innovative approach to error reporting processes and guiding speaking up behaviors. Research and education in healthcare error typically focuses on errors from an organizational perspective in terms of policies and expectations. This study shows that individual’s deep-seated values and beliefs drive perceptions and decisions. Error reporting and speaking up behaviors could be improved by identifying those perceptions and working to meet people where they are.
Limitations
This systematic literature review had some limitations. First, twenty of the twenty-nine articles included voluntary participants. Voluntary bias is a limitation as it only represents a subset of the population and may not represent the entire population of interest.41
Another limitation is that the search strategy returned only one non-English study. This was likely due to search limitations and our criteria. In other words, the inclusion and exclusion criteria were set to exclude literature that focused on organizational culture as the researchers were studying organizational factors to promote error reporting in a simultaneous literature review for comparison. Therefore, it should not be assumed that there is no research beyond the English-speaking world.
Future Directions
This study identified several areas around psychological safety in need of future study:
- To date, there is a lack of research that investigates cultural influence31 and gender roles34 on employee perceptions of psychological safety.
- Although a supportive organizational environment and minimizing stress relate to optimal learning, it does not necessarily affect psychological safety. More research is needed to address burnout and its effect on psychologically safe environments.40
- There is a need for research interventions to improve psychological safety by considering individual characteristics and perceptions that drive decision-making and how to intervene when a decision such as speaking up is high risk.
- Further research is needed to determine the relationship between leadership effectiveness, psychological safety, and speaking up.
Effective leadership was described as a necessary element of psychological safety.26 However, effective leadership is a broad term, and the definition is based on the employee’s perception. Further research is needed to define effective leadership and determine the relationship between leadership effectiveness and psychological safety32 and speaking up.
Conclusion
Healthcare leadership’s challenges with healthcare errors and reporting are well known, multidimensional and complex problems. However, organizations are composed of people with individual characteristics, perceptions, and beliefs that influence decision-making and may deter people from reporting errors regardless of the organizational culture. In other words, regardless of leadership attempts to influence people to report, there may be underlying reasons for an individual’s perception and decision not to report. Although individual characteristics are only one aspect that impact error reporting, these personal values and ideas within a diverse population should be considered when creating policies, faculty development, and follow-up for errors.
This systematic review provides evidence of individual characteristics that promote psychological safety and error reporting. We also provide evidence of individual characteristics that serve as barriers for psychological safety and error reporting. Interventions may be taken by healthcare leadership to foster the characteristics that promote psychological safety and error reporting and alleviate the barriers. Future studies that focus on the gaps identified in this review may further build upon our findings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. There are no conflicts of interest to disclose at this time. There were no sources of funding for this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. White RM, Delacroix R. Second victim phenomenon: is ‘just culture’ a reality? An integrative review. Appl Nurs Res. 2020;56:151319. doi:10.1016/j.apnr.2020.151319
2. Patient safety. World Health Organization. Available from: https://www.who.int/news-room/fact-sheets/detail/patient-safety#:~:text=Every%20year%2C%20millions%20of%20patients,and%20poor%2Dquality%20health%20care.&text=Medication%20errors%20are%20a%20leading,42%20billion%20annually%20(10).
3. Hémon B, Michinov E, Guy D, Mancheron P, Scipion A. Speaking up about errors in routine clinical practice: a simulation-based intervention with nursing students. Clin Simulation Nursing. 2020;45:32–41. doi:10.1016/j.ecns.2020.03.003
4. O’Donovan R, McAuliffe E. A systematic review exploring the content and outcomes of interventions to improve psychological safety, speaking up and voice behaviour. BMC Health Serv Res. 2020;20(1):101. doi:10.1186/s12913-020-4931-2
5. The Joint Commission, USA. The essential role of leadership in developing a safety culture. Sentinel Event Alert. 2017;12(57):1–8.
6. Edmondson AC. The Fearless Organization: Creating Psychological Safety in the Workplace for Learning, Innovation, and Growth. Hoboken (NJ): John Wiley & Sons; 2019.
7. Clark TR. The 4 Stages of Psychological Safety Defining the Path to Inclusion and Innovation. Oakland, CA: Berrett-Koehler Publishers, Inc; 2020.
8. Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. doi:10.1136/bmj.n160
9. Barkell NP, Snyder SS. Just culture in healthcare: an integrative review. Nurs Forum. 2021;56(1):103–111. doi:10.1111/nuf.12525
10. Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available from: www.covidence.org.
11. Critical appraisal tools. JBI. Available from: https://jbi.global/critical-appraisal-tools.
12. Kirkpatrick DL, Kirkpatrick JD. Evaluating Training Programs: The Four Levels. San Francisco: BK, Berrett-Koehler; 2012.
13. Phillips JJ, Buzachero V, Phillips P, Phillips Z. Measuring ROI in Healthcare: Tools and Techniques to Measure the Impact and ROI in Healthcare Improvement Projects and Programs: Tools and Techniques to Measure the Impact and ROI in Healthcare Improvement Projects and Programs. McGraw Hill Professional; 2013.
14. Lee W, Kim SY, Lee SI, Lee SG, Kim HC, Kim I. Barriers to reporting of patient safety incidents in tertiary hospitals: a qualitative study of nurses and resident physicians in South Korea. Int J Health Plann Manage. 2018;33(4):1178–1188. doi:10.1002/hpm.2616
15. Marshall C, Van Der Volgen J, Lombardo N, et al. Approach to Assess the Impact of an Interprofessional Education Medical Error Simulation. Am J Pharm Educ. 2020;84(2):7133. doi:10.5688/ajpe7133
16. Aydon L, Hauck Y, Zimmer M, Murdoch J. Factors influencing a nurse’s decision to question medication administration in a neonatal clinical care unit. J Clin Nurs. 2016;25(17–18):2468–2477. doi:10.1111/jocn.13277
17. Derickson R, Fishman J, Osatuke K, Teclaw R, Ramsel D. Psychological safety and error reporting within Veterans Health Administration hospitals. J Patient Saf. 2015;11(1):60–66. doi:10.1097/PTS.0000000000000082
18. Shepherd L, LaDonna KA, Cristancho SM, Chahine S. How Medical Error Shapes Physicians’ Perceptions of Learning: an Exploratory Study. Acad Med. 2019;94(8):1157–1163. doi:10.1097/ACM.0000000000002752
19. Siewert B, Hochman MG. Improving Safety through Human Factors Engineering. Radiographics. 2015;35(6):1694–1705. doi:10.1148/rg.2015150107
20. Fagan A, Parker V, Jackson D. A concept analysis of undergraduate nursing students speaking up for patient safety in the patient care environment. J Adv Nurs. 2016;72(10):2346–2357. doi:10.1111/jan.13028
21. Landgren R, Alawadi Z, Douma C, Thomas EJ, Etchegaray J. Barriers of Pediatric Residents to Speaking Up About Patient Safety. Hosp Pediatr. 2016;6(12):738–743. doi:10.1542/hpeds.2016-0042
22. Rosenbaum L. Cursed by Knowledge - Building a Culture of Psychological Safety. N Engl J Med. 2019;380(8):786–790. doi:10.1056/NEJMms1813429
23. Sahay A, Hutchinson M, East L. Exploring the influence of workplace supports and relationships on safe medication practice: a pilot study of Australian graduate nurses. Nurse Educ Today. 2015;35(5):e21–e26. doi:10.1016/j.nedt.2015.01.012
24. Lee SE, Vincent C, Dahinten VS, Scott LD, Park CG, Dunn Lopez K. Effects of Individual Nurse and Hospital Characteristics on Patient Adverse Events and Quality of Care: a Multilevel Analysis. J Nurs Scholarsh. 2018;50(4):432–440. doi:10.1111/jnu.12396
25. Hewitt T, Chreim S, Forster A. Sociocultural Factors Influencing Incident Reporting Among Physicians and Nurses: understanding Frames Underlying Self- and Peer-Reporting Practices. J Patient Saf. 2017;13(3):129–137. doi:10.1097/PTS.0000000000000130
26. Edmondson AC, Higgins M, Singer S, Weiner J. Understanding psychological safety in health care and education organizations: a comparative perspective. Res Hum Dev. 2016;13(1):65–83. doi:10.1080/15427609.2016.1141280
27. Mateu EG, Flores CM, López VF, Cid BG, Miralles JG. La comunicación de los efectos adversos en un servicio de urgencias. Metas de enfermería. 2020;23(1):25–32.
28. Ridley CH, Al-Hammadi N, Maniar HS, et al. Building a Collaborative Culture: focus on Psychological Safety and Error Reporting. Ann Thorac Surg. 2021;111(2):683–689. doi:10.1016/j.athoracsur.2020.05.152
29. Chegini Z, Kakemam E, Asghari Jafarabadi M, Janati A. The impact of patient safety culture and the leader coaching behaviour of nurses on the intention to report errors: a cross-sectional survey. BMC Nurs. 2020;19:89. doi:10.1186/s12912-020-00472-4
30. Rich A, Viney R, Griffin A. Understanding the factors influencing doctors’ intentions to report patient safety concerns: a qualitative study. J R Soc Med. 2019;112(10):428–437. doi:10.1177/0141076819877542
31. Newman A, Donohue R, Eva N. Psychological safety: a systematic review of the literature. Human Resource Manage Rev. 2017;27(3):521–535. doi:10.1016/j.hrmr.2017.01.001
32. Vrbnjak D, Denieffe S, O’Gorman C, Pajnkihar M. Barriers to reporting medication errors and near misses among nurses: a systematic review. Int J Nurs Stud. 2016;63:162–178. doi:10.1016/j.ijnurstu.2016.08.019
33. Ali LAI, Saifan AR, Alrimawi I, Atout M, Salameh B. Perceptions of nurses about reporting medication administration errors in Jordanian hospitals: a qualitative study. Appl Nurs Res. 2021;59:151432. doi:10.1016/j.apnr.2021.151432
34. Alser M, Böttcher B, Alfaqawi M, Jlambo A, Abuzubaida W, Abu-El-Noor N. Undergraduate medical students’ attitudes towards medical errors and patient safety: a multi-center cross-sectional study in the Gaza Strip, Palestine. BMC Med Educ. 2020;20(1):447. doi:10.1186/s12909-020-02375-z
35. Halperin O, Bronshtein O. The attitudes of nursing students and clinical instructors towards reporting irregular incidents in the medical clinic. Nurse Educ Pract. 2019;36:34–39. doi:10.1016/j.nepr.2019.02.018
36. Gilmartin HM, Langner P, Gokhale M, et al. Relationship Between Psychological Safety and Reporting Nonadherence to a Safety Checklist. J Nurs Care Qual. 2018;33(1):53–60. doi:10.1097/NCQ.0000000000000265
37. Roth CG, Eldin KW, Padmanabhan V, Friedman EM. Twelve tips for the introduction of emotional intelligence in medical education. Med Teach. 2019;41(7):746–749. doi:10.1080/0142159X.2018.1481499
38. Rubin IM, Campbell TJ. The ABCs of Effective Feedback: a Guide for Caring Professionals. J Healthcare Quality. 1999;21(4):44.
39. O’Donovan R, McAuliffe E. Exploring psychological safety in healthcare teams to inform the development of interventions: combining observational, survey and interview data. BMC Health Serv Res. 2020;20(1):810. doi:10.1186/s12913-020-05646-z
40. Swendiman RA, Edmondson AC, Mahmoud NN. Burnout in Surgery Viewed Through the Lens of Psychological Safety. Ann Surg. 2019;269(2):234–235. doi:10.1097/SLA.0000000000003019
41. Salkind NJ, eds. Encyclopedia of Research Design. Thousand Oaks, CA: SAGE Publications, Inc; 2010. doi:10.4135/9781412961288
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patient-Centered Care Experiences of First-Generation, South Asian Migrants with Chronic Diseases Living in High-Income, Western Countries: Systematic Review
Vakil K, Desse TA, Manias E, Alzubaidi H, Rasmussen B, Holton S, Mc Namara KP
Patient Preference and Adherence 2023, 17:281-298
Published Date: 1 February 2023
Servant Leadership in the Healthcare Literature: A Systematic Review
Demeke GW, van Engen ML, Markos S
Journal of Healthcare Leadership 2024, 16:1-14
Published Date: 3 January 2024
Promoting Speaking Up Through Interprofessional Identity Triggers in a Mixed-Profession Simulation Scenario: Two Group Double-Blinded Pre-Test-Only Design
Kuipers R, Reinke L, Tulleken J, Reinders JJ
Journal of Multidisciplinary Healthcare 2025, 18:5521-5533
Published Date: 4 September 2025