Back to Journals » Drug Design, Development and Therapy » Volume 20
Indication Expansion Dynamics and Trial Characteristics of Novel Multi-Indication Anti-Cancer Drugs in China (2000–2024): A Cross-Sectional Study
Authors Chen X ![]() , Li H, Ou S
, Li H, Ou S ![]() , He Z
, He Z ![]() , Zheng D, Luo J
, Zheng D, Luo J ![]() , Jiang Q
, Jiang Q
Received 3 July 2025
Accepted for publication 23 December 2025
Published 6 January 2026 Volume 2026:20 551402
DOI https://doi.org/10.2147/DDDT.S551402
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Leonidas D. Panos
Xiaoyi Chen,1 Huan Li,1 Shunlong Ou,2 Zhisan He,1 Dongni Zheng,1,3 Jing Luo,4 Qian Jiang2
1Department of Pharmacy, Sichuan Clinical Research Center for Cancer, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, School of Medicine, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 2Department of Pharmacy, Sichuan Clinical Research Center for Cancer, Sichuan Cancer Hospital & Institute, Sichuan Cancer Center, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 3Department of Pharmacy, The Fifth People’s Hospital of Chengdu, Chengdu, Sichuan, People’s Republic of China; 4Department of Pharmacy, The Second People’s Hospital of Yibin, Yibin, Sichuan, People’s Republic of China
Correspondence: Qian Jiang, Email [email protected]
Purpose: To perform a cross-sectional analysis of the indication expansion trends and pivotal trial features of novel multi-indication anti-cancer drugs approved in China from 2000 to 2024.
Methods: We conducted a cross‑sectional review of 74 novel multi-indication anti-cancer drugs approved by the National Medical Products Administration (NMPA) in China from 2000 to 2024, encompassing 265 total indications. Data were collected from multiple sources, including the NMPA, the Center for Drug Evaluation (CDE) of the NMPA, the National Healthcare Security Administration (NHSA), ClinicalTrials.gov, and drug package inserts. Descriptive statistics and Fisher’s exact test (two-tailed) or the χ2-test with Monte Carlo simulation, were used to analyze indication and clinical trial characteristics across indication approval sequence.
Results: Of the 74 drugs, 32 (43%) held two indications, 23 (31%) held three, and 19 (26%) held four or more. Solid tumors accounted for 80% of all indications, most commonly non–small cell lung cancer. Immune checkpoint inhibitors (ICIs) exhibited the greatest expansion, with the most extensively approved drug reaching 14 indications. However, the inclusion of these drugs in the National Reimbursement Drug List (NRDL) did not keep pace with their market approval. Sequential approvals across indications showed significant differences in treatment type (P< 0.001), NMPA approval type (P=0.008), trial arms (P=0.009), trial design (P=0.030), and single-arm endpoints (P< 0.001).
Conclusion: Regulatory reforms facilitated the approval of novel multi-indication anti-cancer drugs, although NRDL inclusion has not kept pace. Targeted therapies dominate, while ICIs, though fewer, show the broadest indication expansion. Most drugs are approved for two to three indications, mainly in solid tumors, and later approvals were associated with different regulatory pathways than earlier ones.
Keywords: NMPA approval, multi-indication, indication expansion, targeted therapy, pivotal trial
A Letter to the Editor has been published for this article.
Introduction
Cancer incidence and mortality rates have risen steadily in recent years. According to the 2024 data from the International Agency for Research on Cancer (IARC) (GLOBOCAN), nearly 20 million new cancer cases and 9.74 million cancer deaths were reported globally in 2022.1 By 2050, the number of new cases is projected to reach 35 million. In Asia, cancer incidence and mortality account for 49.2% and 56.1% of the global total, respectively.1 Notably, China reports the highest number of cases, with approximately 4.825 million new cancer cases and 2.574 million deaths in 2022, reflecting a continuous upward trend in both incidence and mortality rates compared to historical data.2 In light of the alarming rise in cancer incidence and mortality worldwide, the urgent need for more effective treatment strategies has intensified. This escalating disease burden has not only spurred intensified research efforts in oncology but also prompted regulatory agencies to streamline approval processes for innovative therapies.
According to data from the US Food and Drug Administration (FDA), the approval rate for novel anti-cancer indications has increased since the beginning of the 21st century, partly due to the emergence of targeted therapies and the introduction of new treatment methods. Kinase inhibitors are the product category with the highest number of approved products and indications, while immune checkpoint inhibitors, although first approved only in 2011, have the second-highest number of approvals, following kinase inhibitors. This growth can be partially attributed to the higher volume of new drug applications, as well as the expansion of indications for drugs that were previously approved, with the latter now making up the majority of application.3
With the advancement of drug registration and approval system reforms in China, such as priority review and conditional approval, and in response to the growing medical needs related to various malignancies, anti-cancer drugs have become a key focus of drug development, particularly novel anti-cancer drugs.4,5 As a result, the number of newly approved indications for novel anti-cancer drugs has grown rapidly. For instance, pembrolizumab, initially approved for melanoma,6 has expanded to over 10 cancer type,7–14 including non-small cell lung cancer (NSCLC) and gastric cancer, exemplifying the trend of multi-indication development. In this context, “novel anti-cancer drugs” refer to agents with novel mechanisms of action, including small-molecule inhibitors, monoclonal antibodies, antibody-drug conjugates, and other innovative therapies,15,16 which differ fundamentally from traditional cytotoxic chemotherapies by targeting specific molecular pathways or modulating the immune system to address significant unmet medical needs. Within this category, “novel multi-indication anti-cancer drugs” are defined as those that have obtained regulatory approval for two or more distinct cancer indications following their initial approval, encompassing both the original and subsequently approved supplemental indications.
While the expansion of novel multi-indication anti-cancer drugs has become an established trend in the United States and Europe, with many drugs obtaining more supplemental indications within a few years after their initial approval,17–20 China has started relatively late in this regard. Since 2015, reforms by the National Medical Products Administration (NMPA), including priority review, conditional approval, and acceptance of overseas clinical data have fundamentally reshaped the approval pathway for innovative oncology drugs.21 However, existing research on novel multi-indication anti-cancer drugs approved in China remains limited, primarily focusing on regulatory timelines22,23 and clinical trial approvals,24 with little systematic analysis of each drug’s distinct indications or the patterns governing the sequence of multi-indication approvals.
Against the backdrop of concurrent regulatory reform and pharmaceutical innovation, this study systematically analyzes the indication-specific characteristics and pivotal clinical trial features of novel multi-indication anti-cancer drugs in China, with a focus on comparisons across the indication approval sequence. Such analysis can elucidate drug approval and market entry patterns and provide empirical evidence to guide drug development, inform decision-making, promote coordinated review practices, and ultimately improve drug accessibility.
Methods
Selection Criteria and Search Strategy
This study included all novel multi-indication anti-cancer drugs approved in China from the first approval in 2000 up to November 30, 2024. The inclusion date was defined based on the earliest approved indication of each drug.
The research subjects are derived from the 2023 edition of the Clinical Practice Guidelines for Novel Anti-cancer Drugs. The inclusion criteria for this study were as follows: (1) novel multi-indication anti-cancer drugs included in the 2023 edition of the Clinical Practice Guidelines for Novel Anti-cancer Drugs; (2) indications approved by the NMPA in China as of November 30, 2024; and (3) indications approved in the Chinese version of the package insert as of November 30, 2024. The exclusion criteria were: (1) novel anti-cancer drugs with single indications in the 2023 edition of the Clinical Practice Guidelines for Novel Anti-cancer Drugs; (2) indications not approved by the NMPA as of November 30, 2024; (3) drugs used for non-oncological indications; and (4) chimeric antigen receptor T-cell (CAR-T) immunotherapy.
Data on the characteristics of novel multi-indication anti-cancer drugs, including drug profiles, indication features, and key clinical trial attributes at the time of approval, were collected through a cross-sectional survey of the NMPA, its Center for Drug Evaluation (CDE), the National Healthcare Security Administration (NHSA), ClinicalTrials.gov, and drug package inserts. The search timeframe was set to cover all records from the inception of each database up to November 30, 2024.
Data Extraction
Two researchers independently extracted data using a predefined structured Excel spreadsheet and cross-checked the accuracy and completeness of the information. Any discrepancies were resolved through discussion. Extracted information included, but was not limited to: (1) drug characteristics (domestic or imported, exclusivity, mechanism of action, route of administration, drug type, and targeted tumor types); (2) indication characteristics (treatment regimen, line of therapy, approval type, approval date, target, and inclusion in insurance coverage); and (3) pivotal clinical trial characteristics (NCT numbers, study design, trial phase, and outcome measures). For indications supported by multiple trials, the pivotal clinical trial reported in the CDE review was included, with preference given to the trial with the largest sample size and highest phase; if no pivotal trial was specified, the trial with the largest sample size and highest phase that best aligned with the approved indication in the drug label was selected.
Statistical Analysis
Statistical analyses were reported for the entire sample of novel multi-indication anti-cancer drugs. Descriptive statistics were used to examine drug, indication, and clinical trial characteristics. Categorical variables were presented as frequencies and percentages. For novel multi-indication anti-cancer drugs, we compared the distribution of collected variables across first, second, third, fourth, fifth, sixth, seventh, eighth, ninth, tenth, eleventh, twelfth, thirteenth, and fourteenth approved indications using Fisher’s exact test (two-tailed) or the χ2-test with Monte Carlo simulation. Statistical analyses were performed using IBM SPSS 27.0, Excel 2019, and Origin 2024, with P < 0.05 indicating statistical significance. P-values reflect differences across indication approval sequences, rather than overall prevalence.
Results
Sample Overview
A total of 124 drugs were identified from the 2023 edition of the Guidelines for Clinical Application of Novel Anti-cancer Drugs (Table S1). After excluding non-oncological therapies and CAR-T immunotherapies, 120 drugs were included, with 311 approved indications identified across major databases (Table S2).
After excluding novel anti-cancer drugs with only a single approved indication, 74 multi-indication novel anti-cancer drugs were identified, corresponding to a total of 265 approved indications (Table S3). The data screening process is detailed in Figure 1. The exclusion list is detailed in Tables S4 and S5.
 |
Figure 1 Flow Diagram of the Screening for Novel Multi-indication Anti-cancer Drugs Approved by the National Medical Products Administration as of November 30, 2024. Abbreviation: NMPA, National Medical Products Administration. |
Drug Characteristics: Trends in the Approval of Novel Multi-Indication Anti-Cancer Drugs
The novel multi-indication anti-cancer drugs approved cumulative number (exhibits a consistent upward trajectory, by the NMPA from 2000 to 2024 with a marked acceleration after 2015. By 2024, the total number reached 74, highlighting the growing focus on developing such drugs. The annual number of new additions, however, shows considerable fluctuations. While the annual additions remained below 4 before 2019, they surged significantly afterward, peaking at 18 in 2020. Subsequently, the annual additions declined, stabilizing at lower levels in recent years (Figure 2a).
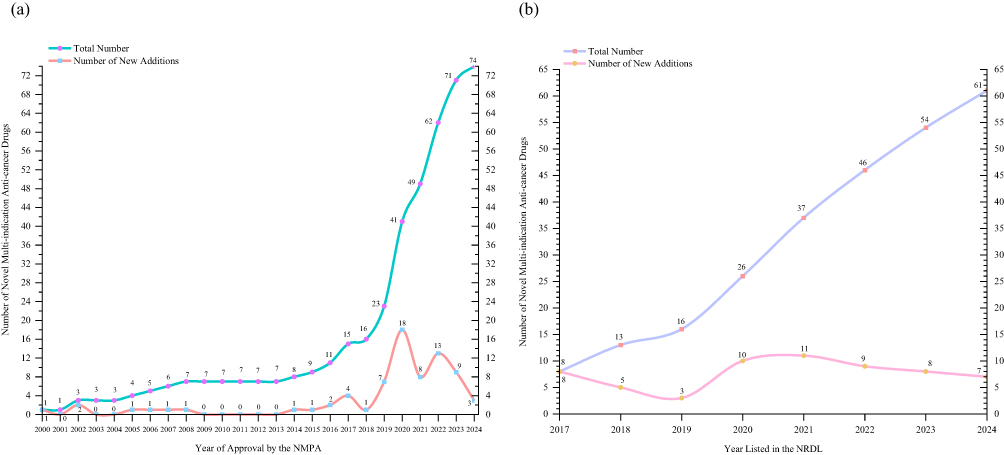 |
Figure 2 Trends in the Approval of Novel Multi-indication Anti-cancer Drugs. (a) displays the cumulative total number (green line) and annual new additions (Orange line) of novel multi-indication anti-cancer drugs approved by the NMPA from 2000 to 2024. The data highlights a steady increase in cumulative approvals over time, with significant growth after 2015, and fluctuations in annual new approvals, peaking in 2020 with 18 drugs. Since the earliest indication was approved in China in 2000, the analysis starts from that year. (b) displays the trends in the cumulative total number (purple line) and annual number of new additions (pink line) of novel multi-indication anti-cancer drugs included in the NRDL from 2017 to 2024. The cumulative number steadily increased from 8 in 2017 to 61 in 2024, while the annual new additions fluctuated, peaking at 11 in 2021. Since the China National Healthcare Security Administration (NHSA) was established in 2018, the analysis starts from 2017. Abbreviations: NMPA, National Medical Products Administration; NRDL, National Reimbursement Drug List. |
Between 2017 and 2024, the cumulative number of novel multi-indication anti-cancer drugs listed in the National Reimbursement Drug List (NRDL) expanded from 8 to 61. The annual number of newly included drugs increased from 3 in 2019 to 10 in 2020 and 11 in 2021, but subsequently declined to 9, 8, and 7 in 2022, 2023, and 2024, respectively, suggesting a deceleration in the pace of NRDL expansion (Figure 2b).
Drug Characteristics: Characteristics of Novel Anti-Cancer Drugs with Multiple Indications
Among the 74 novel multi-indication anti-cancer drugs approved in China, imported drugs dominated, comprising 47 (64%) of the total, while domestic drugs accounted for 27 (36%). Of these, 65% (48 drugs) were exclusively produced, while the remaining 35% (26 drugs) were non-exclusively produced. In terms of mechanisms of action, targeted therapies were the most common, with 56 drugs (76%), while immune regulators only 18 drugs (24%).
Regarding administration routes, oral formulations were the most prevalent, accounting for 43 drugs (58%), likely due to their impact on patient adherence and convenience. Intravenous formulations followed, comprising 31 drugs (42%). In terms of product types, small molecules (44 drugs, 59%) and antibodies (25 drugs, 34%) dominated the market, while antibody-drug conjugates (ADCs) (5 drugs, 7%) remained relatively underrepresented.
The distribution of indications revealed that most drugs targeted solid tumors (72%), with hematologic cancers accounting for 16%, and 12% addressing both types. As for the number of indications, the majority of drugs were approved for two indications (43%), indicating a limitation in indication expansion. However, a small subset of drugs exhibited broad clinical applicability, with the highest number of indications reaching 14 (3%). Notably, the maximum number of indications for a single drug was 14 such as pembrolizumab, highlighting its extensive potential across multiple cancer types.
In terms of reimbursement, 61 drugs (82%) of the 74 approved drugs were reimbursed under national healthcare programs, while the remaining 13 drugs (18%) were not included in the reimbursement list. This indicates that most novel multi-indication anti-cancer drugs are supported by insurance, although a considerable proportion are not yet reimbursed. Additionally, statistical analysis revealed that not all indications approved for the ten novel multi-indication anti-cancer drugs, including disitamab vedotin, pertuzumab, nimotuzumab, ceritinib, ensartinib, lorlatinib, iruplinalkib, chidamide, and candonilimab, are covered by national healthcare reimbursement. This indicates a lag in the alignment of healthcare insurance coverage with drug approvals. Despite these drugs being approved for multiple indications, the slower pace of updates in insurance policies means that many patients may not be able to benefit from reimbursement for all indications (Table 1).
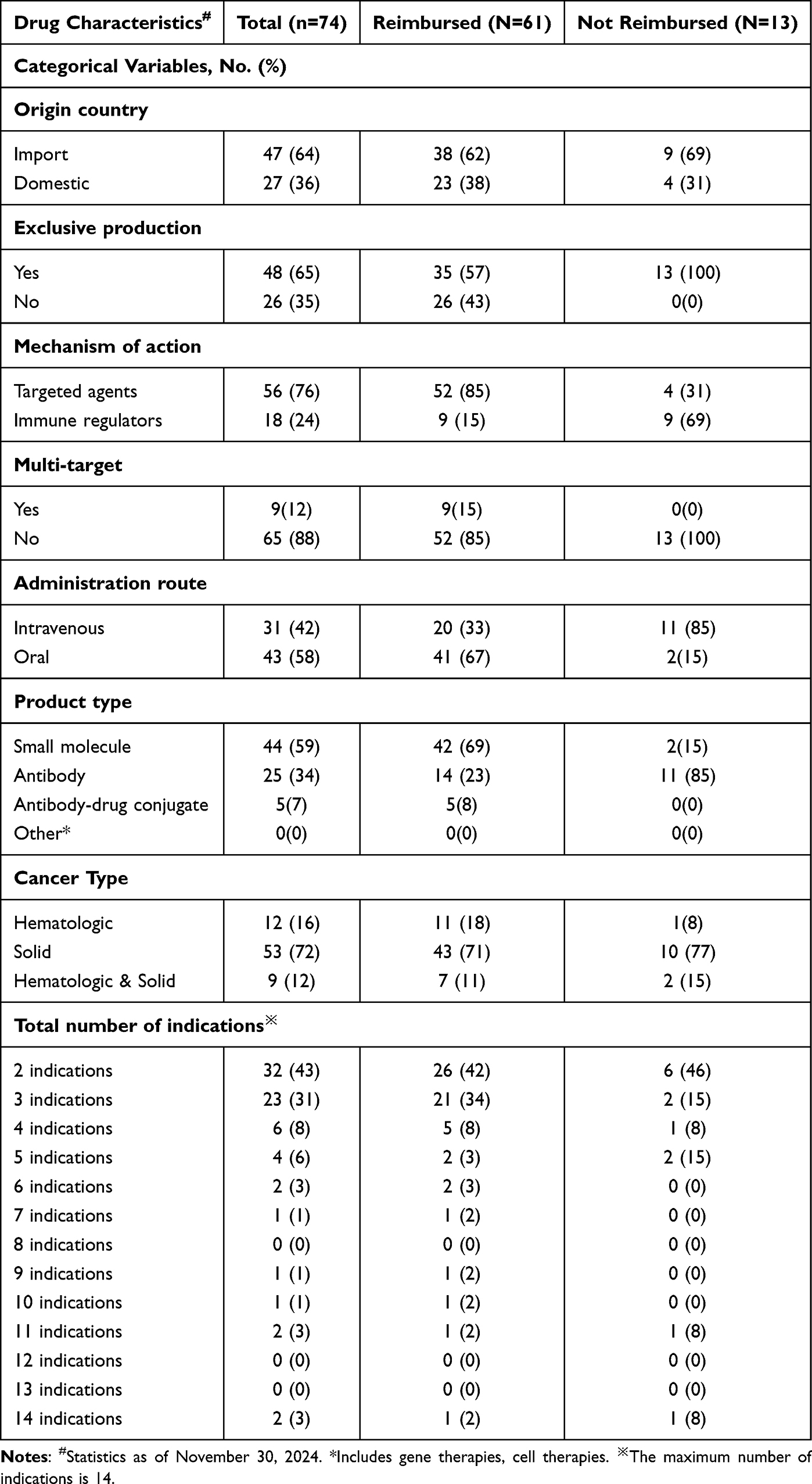 |
Table 1 Drug Characteristics of Novel Multi-Indication Anti-Cancer Drugs in China |
Indication Characteristics: Compared Across Approval Sequence in Novel Multi-Indication Anti-Cancer Drugs
Among the 265 approved indications of novel multi-indication anti-cancer drugs in China, solid tumor indications accounted for the majority (80%, 211/265), while hematologic malignancies indications represented 20% (54/265). Regarding treatment types, monotherapy was the predominant treatment type (56%, 149/265), and combination therapy accounted for 44% (116/265). Biomarker-associated indications accounted for 40% (107/265) of approvals, while 60% (158/265) were biomarker-independent. Most approved indications (91%, 242/265) targeted advanced-stage tumors, whereas only a small proportion (9%, 23/265) were for early-stage tumors. With respect to the line of therapy, 48% (127/265) of indications were approved for first-line treatment, 28% (74/265) for second-line treatment, and 8% (22/265) for third-line or beyond. Additionally, indications spanning both first- and second-line treatments accounted for only 2% (4/265), whereas those encompassing all lines of therapy were extremely rare (1%, 2/265).
In terms of reimbursement status, 75% (200/265) of indications were included in the reimbursement list, while the remaining 25% (65/265) were not covered. Regarding approval pathways, standard approval accounted for 35% (92/265), priority approval for 20% (52/265), conditional approval for 16% (42/265), and special approval for 11% (30/265). Breakthrough approval was rare, covering only 1% (4/265) of indications. Additionally, data on approval pathways were unavailable for 17% (45/265) of indications.
When comparing variation across the sequence of indication approvals, statistically significant differences were observed in treatment type (P<0.001), NMPA approval type (P=0.008), trial arms (P=0.009), trial design (P=0.030), and single-arm endpoints (P<0.001). In contrast, no significant variation was detected in cancer type (P>0.990), biomarker (P=0.515), stage (P=0.089), line of therapy (P=0.084), and reimbursed (P=0.378) (Table 2).
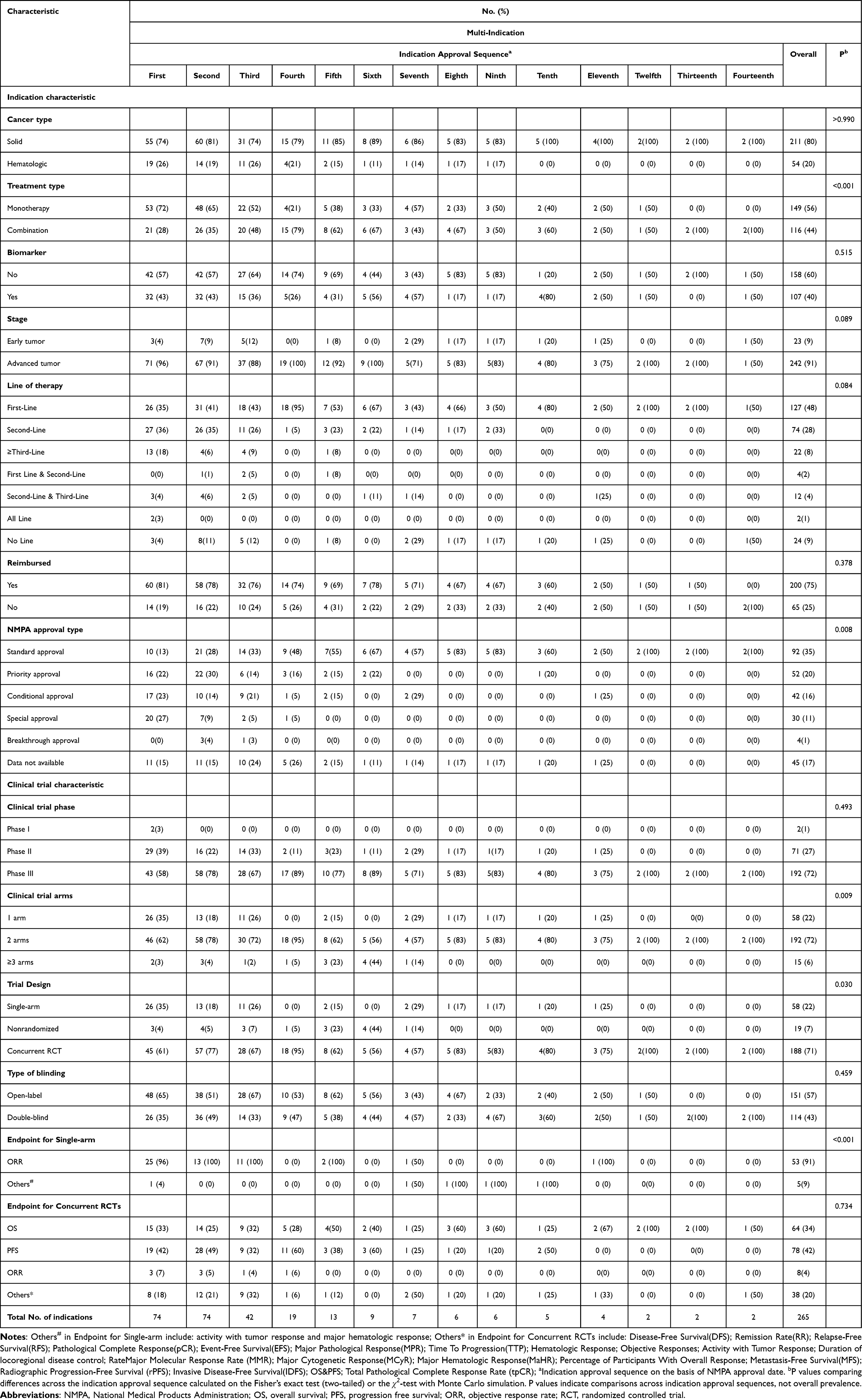 |
Table 2 Indication and Clinical Trial Characteristics Compared Across Indication Approval Sequence in Novel Multi-Indication Anti-Cancer Drugs |
Indication Characteristics: Market Access Characteristics of Drug-Indication Pairs for Novel Multi-Indication Anti-Cancer Drugs in China
By visualizing approval timelines, cumulative indications, and target characteristics for small molecule drugs, monoclonal antibodies, and ADCs, this cross-sectional analysis delineates the development of novel multi-indication anti-cancer drugs, highlighting the growing trend of expanding therapeutic applications across diverse cancer types. The visualization also highlights distinct target categories and the inclusion of drugs not yet incorporated into the NRDL, adding further depth to the analysis (Figure 3).
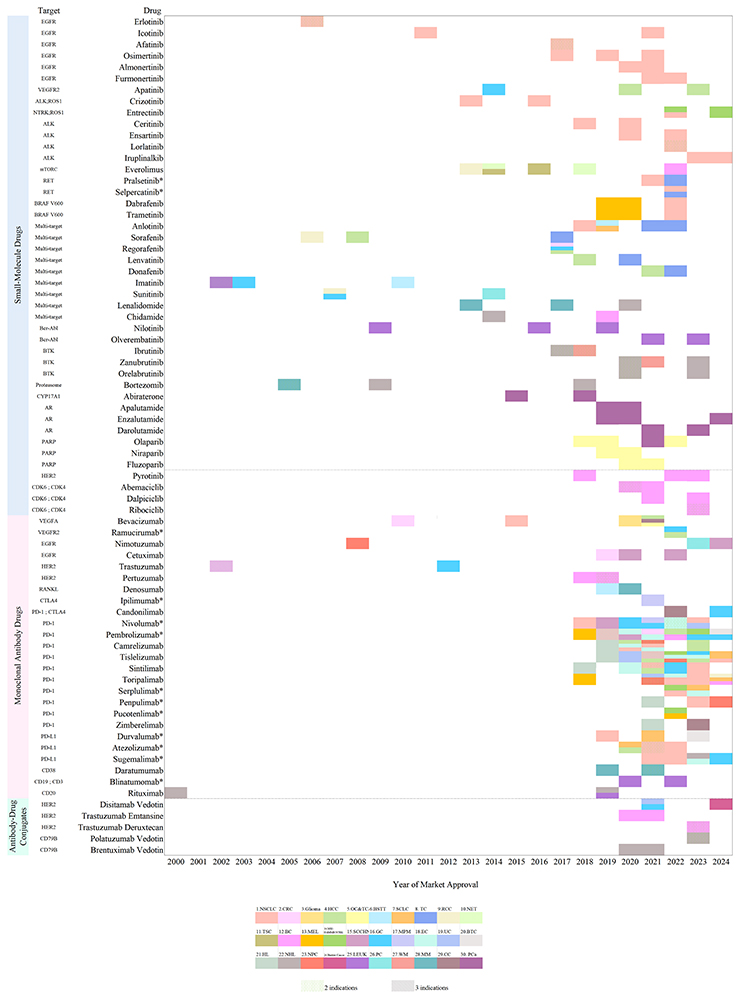 |
Figure 3 Characteristics of Indication Approvals for Novel Multi-indication Anti-cancer Drugs in China. Figure 3 illustrates the timeline, target distribution, and cumulative indications of small molecule drugs, monoclonal antibody drugs, and antibody-drug conjugates (ADCs) approved in China for oncological indications between 2000 and 2024. The y-axis lists the drug names, grouped by drug category (small molecule drugs, monoclonal antibodies, and ADCs) and target, while the x-axis represents the year of market approval. Each colored block corresponds to a specific indication for a drug, with distinct colors representing different cancer types. Drugs marked with an asterisk (*) indicate those not yet included in the National Reimbursement Drug List (NRDL) in China. Multiple indications for the same drug are represented by overlapping or additional blocks, with transparency highlighting such instances of repetition. Cancer types referenced in the figure include: 1. NSCLC, Non-small-cell Lung Cancer; 2. CRC, Colorectal Cancer; 3. Glioma; 4. HCC, Hepatocellular Carcinoma; 5. OC&TC&PC, Ovarian Cancer & Tubal Cancer & Tubal Cancer; 6. BSTT, Bone and Soft Tissue Sarcomas; 7. SCLC, Small Cell Lung Cancer; 8. TC, Thyroid Cancer; 9. RCC, Renal Cell Carcinoma; 10. NET, Neuroendocrine Tumor; 11. TSC, Tuberous Sclerosis Complex; 12. BC, Breast Cancer; 13. MEL, Melanoma; 14. MSI-H/dMMR/NTRK Microsatellite Instability-High/Mismatch Repair deficient/ Neurotrophic Tyrosine Receptor Kinase; 15. SCCHN, Squamous Cell Carcinoma of the Head and Neck; 16. GC, Gastric Cancer; 17. MPM, Malignant Pleural Mesothelioma; 18. EC, Esophageal Cancer; 19. UC, Urothelial Carcinoma; 20. BTC, Biliary Tract Cancer; 21. HL, Hodgkin Lymphoma; 22. NHL, Non-Hodgkin Lymphoma; 23. NPC, Nasopharyngeal Carcinoma; 24. Bladder Cancer; 25. LEUK, Leukemia; 26. PC, Pancreatic Cancer; 27. WM, Waldenström Macroglobulinemia; 28. MM, Multiple Myeloma; 29. CC, Cervical Cancer; 30. PCa, Prostate Cancer. The targets and cancer types featured in the figure include: EGFR, Epidermal Growth Factor Receptor; VEGFR2, Vascular Endothelial Growth Factor Receptor 2; ALK, Anaplastic Lymphoma Kinase; NTRK, Neurotrophic Receptor Tyrosine Kinase; ROS1, Proto-Oncogene 1; mTORC1, Mammalian Target of Rapamycin Complex; RET, Rearranged during Transfection; BRAF V600, B-Raf Proto-Oncogene (V600 Mutation); Multi-target, ≥ three targets; Bcr-Abl, Breakpoint cluster region-Abelson; BTK, Bruton’s Tyrosine Kinase; Proteasome, Protein Complex for Protein Degradation; CYP17A1, Cytochrome P450 17A1; AR, Androgen Receptor; PARP, Poly (ADP-Ribose) Polymerase; HER2, Human Epidermal Growth Factor Receptor 2; CDK4, Cyclin-Dependent Kinase 4; CDK6, Cyclin-Dependent Kinase 6; VEGFA, Vascular Endothelial Growth Factor A; VEGFR2, Vascular Endothelial Growth Factor Receptor 2; RANKL, Receptor Activator of Nuclear Factor Kappa-B Ligand; CTLA-4, Cytotoxic T-Lymphocyte-Associated Protein 4; PD-1, Programmed Cell Death Protein 1; PD-L1, Programmed Death-Ligand 1; CD38, Cluster of Differentiation 38; CD19, Cluster of Differentiation 19; CD3, Cluster of Differentiation 3; CD20, Cluster of Differentiation 20; CD79B, Cluster of Differentiation 79B. |
In solid tumors, NSCLC has the highest number of indications, with 54 indications corresponding to 30 drugs. This is followed by breast cancer, which has 24 indications corresponding to 12 drugs. Gastric cancer and liver cancer rank third, each with 15 indications corresponding to 13 drugs and 12 drugs, respectively. Among other solid tumors, esophageal cancer has 12 indications corresponding to 8 drugs; prostate cancer has 10 indications corresponding to 5 drugs; ovarian cancer, fallopian tube cancer, or primary peritoneal cancer has 8 indications corresponding to 4 drugs; thyroid cancer has 7 indications corresponding to 6 drugs; nasopharyngeal carcinoma has 7 indications corresponding to 5 drugs; melanoma has 7 indications corresponding to 5 drugs; small cell lung cancer has 6 indications corresponding to 6 drugs; head and neck squamous cell carcinoma has 5 indications corresponding to 4 drugs; colorectal cancer has 4 indications corresponding to 4 drugs; renal cell carcinoma has 4 indications corresponding to 4 drugs; urothelial carcinoma has 4 indications corresponding to 4 drugs; microsatellite instability-high or mismatch repair-deficient tumors have 4 indications corresponding to 4 drugs; cervical cancer has 3 indications corresponding to 3 drugs; bone and soft tissue sarcoma has 2 indications corresponding to 2 drugs; neuroendocrine tumors have 2 indications corresponding to 1 drug; tuberous sclerosis complex-associated tumors have 2 indications corresponding to 1 drug; pleural mesothelioma has 2 indications corresponding to 2 drugs; biliary tract cancer has 2 indications corresponding to 2 drugs; pancreatic cancer has 2 indications corresponding to 2 drugs; glioma has 1 indication corresponding to 1 drug, and bladder cancer has 1 indication corresponding to 1 drug.
Among hematological malignancies, non-Hodgkin lymphoma has the highest number of indications, with 21 indications corresponding to 10 drugs. This is followed by leukemia, which has 11 indications corresponding to 5 drugs, and multiple myeloma, ranking third, with 8 indications corresponding to 4 drugs. For other hematological malignancies, Hodgkin lymphoma has 5 indications corresponding to 5 drugs, and Waldenström’s macroglobulinemia has 2 indications corresponding to 2 drugs.
In the early 2000s, the landscape was predominantly characterized by small molecule inhibitors, with most drugs targeting a single cancer type. For example, erlotinib and imatinib, which were among the first targeted therapies, were initially approved for specific cancers such as NSCLC and chronic myeloid leukemia, respectively. These drugs laid the groundwork for targeted therapy by exploiting molecular vulnerabilities in tumor cells. The dominant targets during this period included the Epidermal Growth Factor Receptor (EGFR) and the Breakpoint Cluster Region-Abelson (BCR-ABL), reflecting the focus on specific oncogenic drivers. However, multi-indication approvals were limited, reflecting the nascent stage of biomarker-guided drug development and the relatively narrow focus of early clinical trials.
From 2015 onwards, the approval landscape shifted dramatically, with a significant increase in the number of monoclonal antibodies and ADCs achieving multi-indication approvals. Monoclonal antibodies such as trastuzumab and bevacizumab demonstrated a clear trend toward expanding indications beyond their initial approvals, targeting additional malignancies such as gastric, colorectal, and ovarian cancers. The ability to expand the clinical application of these drugs was facilitated by advances in biomarker identification and companion diagnostic tools, which allowed for better patient stratification and targeted treatment. The targets of monoclonal antibodies, such as Human Epidermal Growth Factor Receptor 2 (HER2), Vascular Endothelial Growth Factor (VEGF), and Programmed Cell Death Protein 1 (PD-1), became central to the development of therapies addressing multiple cancer types. This period also saw a greater integration of drugs targeting immune checkpoints, including Cytotoxic T-Lymphocyte-Associated Protein 4 (CTLA-4) and Programmed Cell Death Ligand 1 (PD-L1), which broadened the scope of immune modulation in cancer therapy.
Immunotherapies, particularly immune checkpoint inhibitors, emerged as a transformative class of drugs during this period. Agents like pembrolizumab and nivolumab initially gained approval for melanoma but rapidly expanded to other indications, including NSCLC, head and neck squamous cell carcinoma, urothelial carcinoma, and more recently, biomarker-defined cancers such as microsatellite instability-high or mismatch repair-deficient tumors, regardless of the tissue of origin. This paradigm shift reflects a move toward tumor-agnostic approvals, driven by an improved understanding of the tumor microenvironment and the role of immune modulation in cancer therapy.
The rise of ADCs in recent years has further contributed to the trend of multi-indication drug development. ADCs such as trastuzumab emtansine (T-DM1) and trastuzumab deruxtecan (T-DXd) combine the specificity of monoclonal antibodies with the cytotoxicity of chemotherapy, allowing for precise delivery of cytotoxic agents to tumor cells while minimizing off-target effects. These agents have been approved for multiple HER2-positive cancers, including breast, gastric, and colorectal cancers, showcasing their potential to target various tumor types sharing a common molecular target. Other emerging targets in the ADC category include Cluster of Differentiation 79B (CD79B), underscoring the diversity of target strategies within this drug class.
A closer examination of the data reveals that the trend toward multi-indication approvals is not only a reflection of technological advancements but also a strategic approach to maximize the therapeutic and economic potential of oncology drugs. The development of drugs with broad applicability aligns with the principles of precision medicine, which emphasize tailoring therapies to the molecular and genetic profiles of patients’ tumors. Moreover, the ability to repurpose established drugs for new indications reduces the time and cost associated with drug development, enabling faster access to effective therapies for patients with unmet medical needs. The inclusion of drugs not incorporated into the Chinese NRDL (marked with an asterisk in Figure 3) highlights potential barriers to patient accessibility, emphasizing the need for policy strategies to improve affordability and availability. Many of these drugs, despite their clinical efficacy, face challenges in market penetration due to their high cost or limited reimbursement.
The result of Figure 3 underscores the dynamic evolution of oncology drug development, with a clear shift from single-indication therapies to agents capable of addressing multiple cancer subtypes. This trend is particularly evident in the post-2015 era, where regulatory frameworks and advances in molecular oncology have enabled the rapid expansion of indications for many therapies. By highlighting the cumulative indications of anticancer drugs over time, the data emphasize the critical role of multi-indication development in improving patient outcomes, expanding treatment options, and addressing the heterogeneity of cancer. The results also suggest that future efforts in oncology drug development will continue to prioritize strategies that optimize the clinical utility of therapeutic agents across a broader spectrum of cancers, further enhancing their impact on global cancer care.
Indication Characteristics: Cancer Type Proportions Among Multi-Indication Anti-Cancer Drugs Approved in China
A total of 74 novel multi-indication anti-cancer drugs covering 265 approved indications were identified. Among these, 43% (32/74) were approved for two indications, 31% (23/74) for three, and 26% (19/74) for four or more indications, categorized into three groups based on the number of approved indications: 32 drugs with two indications (Figure 4a), 23 drugs with three indications (Figure 4b), and 19 drugs with four or more indications (Figure 4c).
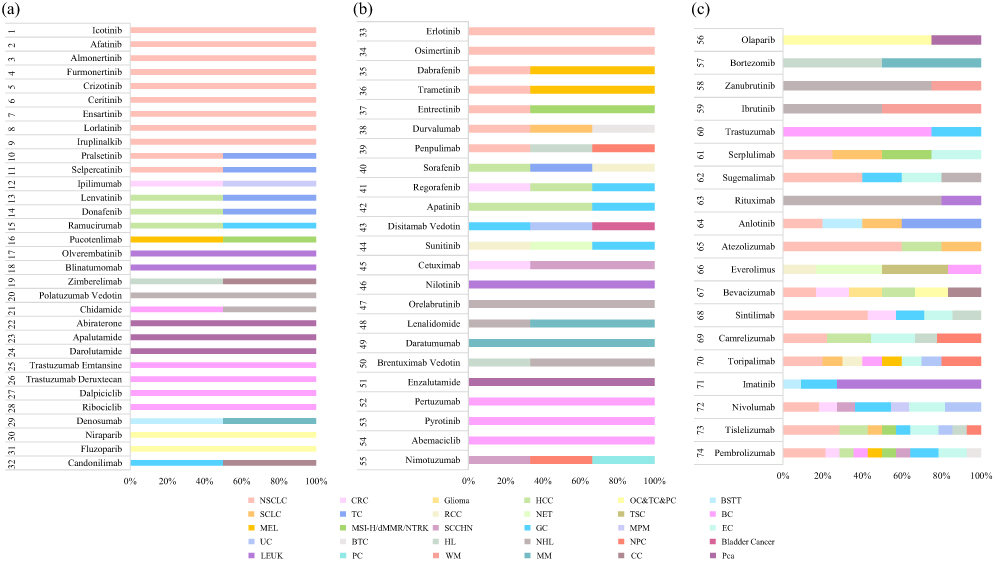 |
Figure 4 Proportion of Cancer Type Among Novel Multi-indication Anti-cancer Drugs Approved in China. (a) Novel multi-indication anti-cancer drugs with two approved indications. (b) Novel multi-indication anti-cancer drugs with three approved indications. (c) Novel multi-indication anti-cancer drugs with four or more approved indications. Each bar represents a specific drug, with segments indicating the proportion of indications across different cancer types. Abbreviations: NSCLC, Non-small-cell Lung Cancer; CRC, Colorectal Cancer; Glioma; HCC, Hepatocellular Carcinoma; OC&TC&PC, Ovarian Cancer & Tubal Cancer & Tubal Cancer; BSTT, Bone and Soft Tissue Sarcomas; SCLC, Small Cell Lung Cancer; TC, Thyroid Cancer; RCC, Renal Cell Carcinoma; NET, Neuroendocrine Tumor; TSC, Tuberous Sclerosis Complex; BC, Breast Cancer; MEL, Melanoma; MSI-H/dMMR/NTRK Microsatellite Instability-High/Mismatch Repair deficient/ Neurotrophic Tyrosine Receptor Kinase; SCCHN, Squamous Cell Carcinoma of the Head and Neck; GC, Gastric Cancer; MPM, Malignant Pleural Mesothelioma; EC, Esophageal Cancer; UC, Urothelial Carcinoma; BTC, Biliary Tract Cancer; HL, Hodgkin Lymphoma; NHL, Non-Hodgkin Lymphoma; NPC, Nasopharyngeal Carcinoma; Bladder Cancer; LEUK, Leukemia; PC, Pancreatic Cancer; WM, Waldenström Macroglobulinemia; MM, Multiple Myeloma; CC, Cervical Cancer; PCa, Prostate Cancer. |
For drugs with two indications (Figure 4a), a significant portion targeted NSCLC, reflecting its high prevalence and priority in drug development. Additional indications in this category often included cancers such as small cell lung cancer and colorectal cancer.
Drugs with three indications (Figure 4b) demonstrated broader applicability, with NSCLC and colorectal cancer remaining dominant, while other cancers, such as renal cell carcinoma, gastric cancer, and hepatocellular carcinoma, also appeared. This group highlights an effort to expand therapeutic applications to diverse but prevalent cancers.
The 19 drugs with four or more indications (Figure 4c) showcased the highest degree of versatility. These drugs addressed a wide array of solid tumors, such as breast cancer and prostate cancer, as well as hematologic malignancies, including Hodgkin’s lymphoma and multiple myeloma. A notable feature of this group was the inclusion of innovative immune checkpoint inhibitors and targeted therapies, which are frequently associated with multiple cancer types due to their mechanism of action.
In general, the distribution of indications highlights a clear emphasis on treating high-prevalence cancers, with NSCLC consistently being the most addressed across all groups. Additionally, the data illustrate a trend toward developing drugs with expanded indications, particularly those leveraging modern therapeutic strategies, such as precision medicine and immunotherapy.
Clinical Trial Characteristics: Pivotal Clinical Trial Characteristics of Novel Multi-Indication Anti-Cancer Therapies at Market Approval
Among the 265 indications approved for novel multi-indication anti-cancer drugs, the majority were supported by clinical trials in Phase III (192, 72%), followed by Phase II (71, 27%), with only 2 indications (1%) based on Phase I trials. In terms of clinical trial arms, two-arm trials were predominant, accounting for 192 indications (72%), while single-arm trials supported 58 indications (22%), and trials with three or more arms accounted for 15 indications (6%). Regarding trial design, nonrandomized trials supported 19 indications (7%), while randomized controlled trials (RCTs) contributed to 188 indications (71%). Open-label studies were the most frequent, supporting 151 indications (57%), whereas double-blind trials accounted for 114 indications (43%). The findings highlight that the majority of approved indications relied on robust Phase III clinical trial data and randomized controlled trials. However, the prevalence of open-label studies suggests the need for further efforts to strengthen blinding in trial designs, particularly for subsequent indications.
In the analysis of clinical endpoints, single-arm trials predominantly relied on objective response rate (ORR) as the primary endpoint, with 91% (53/58) of such trials utilizing ORR, while only 9% (5/58) employed other alternative endpoints, such as activity with tumor response and major hematologic response. In contrast, concurrent RCTs primarily focused on long-term efficacy measures, with progression-free survival (PFS) and overall survival (OS) being the most common endpoints, accounting for 42% (78/188) and 34% (64/188) of trials, respectively. Other endpoints, including disease-free survival (DFS), remission rate (RR), relapse-free survival (RFS), pathological complete response (pCR), event-free survival (EFS), major pathological response (MPR), and several molecular and hematologic response measures, were also utilized in various trials. ORR was used as the primary endpoint in only 4% (8/188) of the indications, whereas alternative endpoints, such as disease control rate, quality of life measures, and molecular and hematologic responses, were employed in 20% (38/188) of the indications. These findings indicate that single-arm trials prioritize ORR as a feasible and efficient endpoint for initial drug approval. However, for later-stage indications, RCTs increasingly adopt OS and PFS as primary endpoints.
When comparing variation across the sequence of indication approvals, statistically significant differences were observed in clinical trial arms (P=0.009), trial design (P=0.030), and endpoint for single-arm (P<0.001). In contrast, no significant variation was detected in clinical trial phase (P=0.493), type of blinding (P=0.459), and endpoint for concurrent RCTs (P=0.734) (Table 2).
Discussion
This study provides the first systematic analysis of drug characteristics, indications, and clinical trial data underlying the NMPA approval of 74 novel multi-indication anti-cancer drugs (totaling 265 indications) in China.
The analysis demonstrates that novel multi-indication anticancer agents approved in China since the early 21st century exhibit alignment with global oncology research priorities, particularly through advancements in molecularly targeted therapeutic modalities and bioactive inhibitor technologies.3 While previous studies, such as Zhou et al25 have analyzed anti-tumor drugs reimbursed up to 2023, they did not evaluate the annual trend of drugs included in the national reimbursement list following the establishment of the NHSA. Our study reveals that novel multi-indication anti-cancer drugs are added to the national reimbursement drug list each year, with only a small proportion of drugs not included in the list overall.
By comparing the indication approval sequence for novel multi-indication anti-cancer drugs, this study reveals that drug development and regulatory approval processes are predominantly focused on solid tumors. This trend aligns with the global landscape of oncology treatments26 and FDA approval characteristics across indication approval sequences.27 The majority of approved indications are concentrated on advanced tumors and first-line therapies. However, the limited approvals for early-stage tumors or multi-line treatment indications highlight the ongoing need for further exploration and innovation, particularly in the prevention or cure of early-stage cancers. The significant variability in reimbursement status (75% included vs 25% excluded) across approvals and the dominance of standard and priority approval pathways emphasize the influence of regulatory and policy frameworks in shaping access to these therapies.28,29 Despite the low proportion of breakthrough approvals, the increasing adoption of expedited pathways, such as priority and conditional approvals, signals an adaptive regulatory environment fostering innovation while addressing unmet medical needs.30
This cross-sectional analysis presents the approval timelines and cumulative indication characteristics of small molecule drugs, monoclonal antibodies, and ADCs for novel multi-indication anti-cancer drugs in China. The results show that NSCLC has the highest number of approved indications, followed by breast cancer, gastric cancer, and liver cancer, which are closely associated with the significant disease burden and therapeutic needs of malignancies in China.2,31
The visualization of drug-indication pairs reveals a progressive expansion of indications across various cancer types, emphasizing the diversification of target characteristics. Among approved indications, small molecule drugs and monoclonal antibodies predominate, with immune checkpoint inhibitors standing out as particularly prominent in the approval of expanded indications. Of particular interest was the observation that novel multi-indication anti-cancer agents approved for two or three indications constituted the largest fraction, in contrast to drugs with ≥4 indications, which were least frequent. Within this latter group, immune checkpoint inhibitors comprised the majority. Consistent with previous research,32 the market access trends of immune checkpoint inhibitors demonstrate an initial focus on rare diseases with unmet medical needs, followed by subsequent expansions into more common cancers. However, Beaver et al33 have highlighted the significant homogeneity among PD-1/PD-L1 inhibitors and called for a halt to the indiscriminate development of “me-too” PD-1/PD-L1 inhibitor drugs. Furthermore, the absence of effective molecular markers, coupled with safety concerns, tolerability issues, and primary drug resistance, warrants further investigation.34–36
The analysis of pivotal clinical trial characteristics for novel multi-indication anti-cancer drugs reveals important trends in the approval process. In subsequent approvals for indication expansions, the majority were supported by Phase III clinical trials, randomized, double-blind studies. This indicates that regulatory agencies prioritize high-quality data from Phase III trials during indication expansions, which aligns with the findings of Ruuskanen et al,17 where extensions of indications are based on improved quality of evidence compared to the first accepted indications.
There may be some possible limitations in this study. First, there is no detailed data analysis of outcome measures such as OS and PFS for novel multi-indication anti-cancer drugs approved in China. Second, the study does not compare the approval landscape in China with that of other countries. Future research could explore these aspects in more detail.
Conclusions
Regulatory reforms facilitated the approval of novel multi-indication anti-cancer drugs. However, the inclusion of novel multi-indication anti-cancer drugs in the NRDL has not kept pace with their market approvals, suggesting a misalignment between regulatory approval and reimbursement processes. Furthermore, in China, targeted therapies dominate among these drugs, whereas ICIs are fewer in number but exhibit the broadest indication expansion. Overall, targeted therapies, particularly small-molecule agents, constitute the majority, with most drugs approved for two to three indications, mainly targeting solid tumors. Moreover, sequential indication approvals showed significant differences across multiple dimensions, suggesting that later approvals were associated with different regulatory pathways than earlier ones.
Data Sharing Statement
All the data supporting the conclusions are presented in the Article or in the supplementary materials. All data used in this study are freely available through NMPA, CDE, NHSA, ClinicalTrials.gov, and drug package inserts.
Funding
This study was funded by the National Natural Science Foundation of China (grant number 72204039) and the Wu Jieping Medical Foundation Clinical Research Special Grant (grant number 320.6750.2025-6-29).
Disclosure
The authors report no conflicts of interest regarding the content of this article.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–17. doi:10.3322/caac.21834
2. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
3. Scott EC, Baines AC, Gong Y, et al. Trends in the approval of cancer therapies by the FDA in the twenty-first century. Nat Rev Drug Discov. 2023;22(8):625–640. doi:10.1038/s41573-023-00723-4
4. Li G, Liu Y, Xie C, Zhou Q, Chen X. Characteristics of expedited programmes for cancer drug approval in China. Nat Rev Drug Discov. 2021;20(6):416. doi:10.1038/d41573-021-00080-0
5. McCall C. China’s oncology drug market on the rise. Lancet Oncol. 2021;22(5):586–587. doi:10.1016/S1470-2045(21)00176-5
6. Si L, Zhang X, Shu Y, et al. A phase Ib study of pembrolizumab as second-line therapy for chinese patients with advanced or metastatic melanoma (KEYNOTE-151). Transl Oncol. 2019;12(6):828–835. doi:10.1016/j.tranon.2019.02.007
7. Gandhi L, Rodríguez-Abreu D, Gadgeel S, et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N Engl J Med. 2018;378(22):2078–2092. doi:10.1056/NEJMoa1801005
8. Kojima T, Shah MA, Muro K, et al. Randomized phase III KEYNOTE-181 study of pembrolizumab versus chemotherapy in advanced esophageal cancer. J Clin Oncol. 2020;38(35):4138–4148. doi:10.1200/JCO.20.01888
9. Burtness B, Harrington KJ, Greil R, et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, Phase 3 study. Lancet. 2019;394(10212):1915–1928. doi:10.1016/S0140-6736(19)32591-7
10. André T, Shiu KK, Kim TW, et al. Pembrolizumab in microsatellite-instability-high advanced colorectal cancer. N Engl J Med. 2020;383(23):2207–2218. doi:10.1056/NEJMoa2017699
11. Qin S, Chen Z, Fang W, et al. Pembrolizumab versus placebo as second-line therapy in patients from Asia with advanced hepatocellular carcinoma: a randomized, double-blind, phase III trial. J Clin Oncol. 2023;41(7):1434–1443. doi:10.1200/JCO.22.00620
12. Schmid P, Cortes J, Pusztai L, et al. Pembrolizumab for early triple-negative breast cancer. N Engl J Med. 2020;382(9):810–821. doi:10.1056/NEJMoa1910549
13. Rha SY, Oh DY, Yañez P, et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for HER2-negative advanced gastric cancer (KEYNOTE-859): a multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 2023;24(11):1181–1195. doi:10.1016/S1470-2045(23)00515-6
14. Kelley RK, Ueno M, Yoo C, et al. Pembrolizumab in combination with gemcitabine and cisplatin compared with gemcitabine and cisplatin alone for patients with advanced biliary tract cancer (KEYNOTE-966): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2023;401(10391):1853–1865. doi:10.1016/S0140-6736(23)00727-4
15. Huang X, Zhu M, Chen R, et al. Innovative drugs promote precision cancer therapy. CCB. 2023;2(1):1. doi:10.1007/s44272-023-00002-8
16. Monk BJ, Patel MR, Toker S, Subbiah V, Gordan LN. Development of anti-cancer medicines in the current era. Cancer Treatment Res Commun. 2025;45:101002. doi:10.1016/j.ctarc.2025.101002
17. Ruuskanen AM, Kurko T, Sarnola K, Klintrup K, Koskinen H. New cancer medicines in Europe 2010-2020: comparison of medicines with or without extensions of indications. BMJ Open. 2024;14(10):e083549. doi:10.1136/bmjopen-2023-083549
18. Stoelinga J, Bloem LT, Russo M, Kesselheim AS, Feldman WB. Comparing supplemental indications for cancer drugs approved in the US and EU. Eur J Cancer. 2024;212:114330. doi:10.1016/j.ejca.2024.114330
19. Patterson JA, Motyka J, Salih R, Nordyke R, O’Brien JM, Campbell JD. Subsequent indications in oncology drugs: pathways, timelines, and the inflation reduction act. Ther Innov Regul Sci. 2025;59(1):102–111. doi:10.1007/s43441-024-00706-6
20. Michaeli DT, Mills M, Michaeli T, Miracolo A, Kanavos P. Initial and supplementary indication approval of new targeted cancer drugs by the FDA, EMA, Health Canada, and TGA. Invest New Drugs. 2022;40(4):798–809. doi:10.1007/s10637-022-01227-5
21. Zhu X, Zhang J. Regulatory efforts to address the access gap for foreign new drugs in China: the priority review program and related policies. Global Health Res Policy. 2025;10(1):7. doi:10.1186/s41256-024-00396-5
22. Li Q, Peng N, Jiang L, et al. Regulatory and clinical outcomes of priority-reviewed innovative cancer drugs in China between 2015 and 2024: an observational study. BMC Cancer. 2025;25(1):1175. doi:10.1186/s12885-025-14580-4
23. Luo X, Du X, Li Z, Qian F, Yang Y. Assessment of the delay in novel anticancer drugs between china and the united states: a comparative study of drugs approved between 2010 and 2021. Clin Pharmacol Ther. 2023;113(1):170–181. doi:10.1002/cpt.2755
24. Yang J, Yang J, Hu YJ. Characteristics of clinical trials of new oncology drugs approved in China. doi:10.1002/cncr.35106.
25. Zhou J, Lu H, Pan J. Association of launch price and clinical value with reimbursement decisions for anticancer drugs in China. Int J Health Policy Manag. 2024;13:8150. doi:10.34172/ijhpm.2024.8150
26. Wu Q, Qian W, Sun X, Jiang S. Small-molecule inhibitors, immune checkpoint inhibitors, and more: FDA-approved novel therapeutic drugs for solid tumors from 1991 to 2021. J Hematol Oncol. 2022;15(1):143. doi:10.1186/s13045-022-01362-9
27. Michaeli DT, Michaeli T. Overall survival, progression-free survival, and tumor response benefit supporting initial US food and drug administration approval and indication extension of new cancer drugs, 2003-2021. J Clin Oncol. 2022;40(35):4095–4106. doi:10.1200/JCO.22.00535
28. Zhu H, Zhu J, Zhou Y, et al. Impact of the national reimbursement drug list negotiation policy on accessibility of anticancer drugs in China: an interrupted time series study. Front Public Health. 2022;10:921093. doi:10.3389/fpubh.2022.921093
29. Liu Y, Zhang N, Xie C, et al. Evolution of drug regulations and regulatory innovation for anticancer drugs in China. Acta Pharm Sin B. 2022;12(12):4365–4377. doi:10.1016/j.apsb.2022.08.004
30. Su L, Liu S, Li G, et al. Trends and characteristics of new drug approvals in China, 2011-2021. Ther Innov Regul Sci. 2023;57(2):343–351. doi:10.1007/s43441-022-00472-3
31. Qiu H, Cao S, Xu R. Cancer incidence, mortality, and burden in China: a time-trend analysis and comparison with the United States and United Kingdom based on the global epidemiological data released in 2020. Cancer Commun. 2021;41(10):1037–1048. doi:10.1002/cac2.12197
32. Michaeli DT, Mills M, Kanavos P. Value and price of multi-indication cancer drugs in the USA, Germany, France, England, Canada, Australia, and Scotland. Appl Health Econ Health Policy. 2022;20(5):757–768. doi:10.1007/s40258-022-00737-w
33. Beaver JA, Pazdur R. The wild west of checkpoint inhibitor development. N Engl J Med. 2022;386(14):1297–1301. doi:10.1056/NEJMp2116863
34. Holder AM, Dedeilia A, Sierra-Davidson K, et al. Defining clinically useful biomarkers of immune checkpoint inhibitors in solid tumours. Nat Rev Cancer. 2024;24(7):498–512. doi:10.1038/s41568-024-00705-7
35. Morad G, Helmink BA, Sharma P, Wargo JA. Hallmarks of response, resistance, and toxicity to immune checkpoint blockade. Cell. 2021;184(21):5309–5337. doi:10.1016/j.cell.2021.09.020
36. Kalbasi A, Ribas A. Tumour-intrinsic resistance to immune checkpoint blockade. Nat Rev Immunol. 2020;20(1):25–39. doi:10.1038/s41577-019-0218-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.