Back to Journals » ClinicoEconomics and Outcomes Research » Volume 12
Incremental Costs Associated with Length of Hospitalization Due to Viral Pneumonia: Impact of Intensive Care and Economic Implications of Reducing the Length of Stay in the Era of COVID-19
Authors Wu N, Kuznik A, Wang D, Moretz C, Xi A, Kumar S, Hamilton L
Received 4 September 2020
Accepted for publication 6 November 2020
Published 2 December 2020 Volume 2020:12 Pages 723—731
DOI https://doi.org/10.2147/CEOR.S280461
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Giorgio Colombo
Ning Wu,1 Andreas Kuznik,1 Degang Wang,1 Chad Moretz,2 Ann Xi,2 Shambhavi Kumar,2 Laurie Hamilton2
1Health Economics and Outcomes Research, Regeneron Pharmaceuticals, Tarrytown, NY, USA; 2Avalere Health, Washington, DC, USA
Correspondence: Andreas Kuznik
Health Economics and Outcomes Research, Regeneron Pharmaceuticals, Tarrytown, NY, USA
Tel +1 914 847 1889
Email [email protected]
Background: Emerging trial data for treatment of COVID-19 suggest that in addition to improved clinical outcomes, these treatments reduce length of hospital stay (LOS). However, the economic value of a shortened LOS is unclear.
Objective: To estimate incremental costs per day of hospitalization for a patient with influenza or viral pneumonia, as a proxy for COVID-19; ICU costs associated with invasive mechanical ventilation (iMV) were also determined.
Methods: Retrospective analysis of claims-based data was conducted using the IBM MarketScan® Commercial Claims and Encounters and Medicare Supplemental and Coordination of Care and the Medicare Fee-for-Service claims databases for hospitalizations due to influenza/viral pneumonia between January 2018 and June 2019. Cases were stratified as uncomplicated hospitalizations or with ICU. Ordinary least squares regression, excluding LOS or costs exceeding the 99th percentile (base case), was used to estimate incremental costs per day; a sensitivity analysis included all qualified hospitalizations. Additional sensitivity analyses used weighting methodology.
Results: Among 6055 and 118,419 hospitalizations in the commercially insured and Medicare databases, respectively, 5958 and 116,552 hospitalizations, respectively, represented the base case. Estimated incremental base case costs per additional inpatient day were $2158 and $3900 in the commercial population for uncomplicated hospitalizations and hospitalizations with ICU, respectively, and $475 and $668, respectively in the Medicare population. Estimated incremental base case costs per additional ICU day were $5254 and $608 for Commercial and Medicare populations, respectively. Higher absolute costs were estimated in the sensitivity analysis on all qualified hospitalizations; the weighted sensitivity analyses generally showed that estimates were stable. Use of iMV increased costs by $35,482 and $13,101 in the commercial and Medicare populations, respectively.
Conclusion: The incremental daily cost of a hospitalization is substantial for US patients with commercial insurance and for Medicare patients. These findings may help quantify the economic value of COVID-19 treatments that reduce LOS.
Keywords: viral pneumonia, hospitalizations, intensive care unit, length of stay, mechanical ventilation, costs
Introduction
The emergence of SARS-CoV-2 and its rapid spread into a global pandemic resulted in the implementation of diverse non-pharmaceutical interventions in many countries in an attempt to flatten the curve. While it has been argued that such policies vary in effectiveness and that voluntary self-restraint may play a primary role at least partly independent of these interventions,1 there has nevertheless been high rates of hospitalizations among patients with symptoms of COVID-19. Many of these patients require an extended length-of-stay (LOS) and therapy that often necessitates management within the setting of an intensive care unit (ICU), including the need for invasive mechanical ventilation (iMV),2–4 which has previously been suggested to be a major driver of ICU costs for other disease states.5,6
Current responses to the immediate need for care of COVID-19 patients include a renewed focus on existing management strategies that may be appropriately applied to these patients and rapid development of new pharmacologic agents to improve patient outcomes and reduce LOS. A reduction in LOS enables allocation of scarce resources such as the need for freeing hospital beds during a surge. For example, the study of remdesivir for management of hospitalized patients with COVID-19 showed a shortened recovery time relative to placebo, resulting in an LOS that was reduced by 4 days.7
Another factor that is relevant to resource allocation is the cost burden of hospitalization, especially when reimbursement is based on Diagnosis Related Groups (DRGs), which provide a set rate of reimbursement according to the diagnosis rather than cost-based payment for actual resources used. Hospitalization costs are not only dependent on the disease and the interventions administered, but are also determined by the length of stay (LOS). While technologies and therapeutic interventions that may be used in an inpatient setting may improve patient outcomes and enhance recovery, it is also important to determine the economic benefits of such interventions, including the potential cost savings that may be associated with a reduction in LOS. For example, as previously shown for community acquired pneumonia, even a short reduction in LOS may be of economic benefit.8,9
As has been highlighted by Kozma et al,9 sequential days of inpatient stays do not have uniform costs, suggesting the need for estimating an average reduction in cost per unit of time (ie, one day less of LOS) using methodologies that capture the variability in costs associated with different LOS duration. However, the rapid evolution in management of patients with COVID-19 limits the availability of claims data that may be appropriate for estimating the economic impact of a reduction in LOS. Therefore, the purpose of the current analysis was to estimate the average incremental costs associated with each additional hospitalized day with and without ICU due to influenza/viral pneumonia as a proxy for COVID-19 including examining the costs that are associated with use of iMV in the ICU.
Methods
Data Source
Claims data for this retrospective study were derived from two sources: the Medicare-Fee-for-Service (FFS) database and the IBM MarketScan® Commercial Claims and Encounters and Medicare Supplemental and Coordination of Care database. The Medicare-FFS database consists of 100% Medicare Parts A/B claims. In contrast, the MarketScan database is a national employer-sponsored insurance claims database that encompasses a variety of commercial fee-for-service and capitated health plans including Medicare supplemental plans such as Medicare Advantage and Medigap. While longitudinal records of inpatient services, outpatient services, long-term care, and prescription drug claims are available in these databases, the current analysis focused only on use and costs of inpatient service.
All data were deidentified and HIPAA (Health Insurance Portability and Accountability Act of 1996) compliant. Since the study did not involve the collection, use, or transmittal of individual identifiable data, Institutional Review Board approval was not required.
Case and Cohort Identification
The study period covered admission records between January 1, 2018 and June 30, 2019. Case inclusion required age at hospital admission to be ≥ 18 in the commercially insured population, and ≥ 65 for the Medicare-FFS population. Cases were hospitalizations due to influenza or viral pneumonia, and were identified if any of the following International Classification of Disease 10th revision, Clinical Modification (ICD-10-CM) diagnosis codes were in the primary/discharge diagnosis position: J09 (Influenza due to certain identified influenza virus), J10 (Influenza due to other identified influenza virus), J11 (Influenza due to unidentified influenza virus), J12 (Viral pneumonia, not elsewhere classified), and J80 (Acute respiratory distress syndrome) if this was accompanied by at least one code with a viral diagnosis (J09, J10, J11, or J12) in the secondary position. For the Medicare-FFS analysis, hospitalizations were identified via primary or discharge diagnoses. For the commercial analysis, qualifying hospitalizations were identified only via primary diagnosis because discharge diagnoses were not available.
Hospitalizations with extracorporeal membrane oxygenation (ECMO) were excluded from the analysis, as were hospitalizations with invasive mechanical ventilation (iMV) but no ICU. These hospitalizations were excluded since the number of hospitalizations with ECMO was small and there is a wide distribution of costs,10 and hospitalizations with iMV but no ICU typically are associated with surgical procedures that specifically require iMV and have characteristics different from hospitalizations requiring iMV use due to pneumonia. Identification of ECMO and iMV was based on procedure and DRG codes listed in Table S1. For DRG codes that are designated for hospitalizations with either ECMO or iMV (DRG 003, 004, 207, 208, or 870), the hospitalization was grouped as iMV if it was associated with the relevant DRG code but had no ECMO procedure codes.
Cases were stratified into cohorts identified as either uncomplicated hospitalizations, defined as hospitalizations without ICU, or hospitalizations with ICU use.
Outcomes
For all hospitalizations that met the inclusion criteria, length of stay (LOS) and costs were estimated from the available claims; costs were the total of patient paid and plan paid, and were adjusted to 2019 dollars based on the medical component of the Consumer Price Index (https://www.bls.gov/data/). The main outcome of interest was the incremental cost per additional inpatient day, which was estimated for uncomplicated stays and those that included ICU; incremental costs per each additional ICU day were also estimated separately.
Statistical Analysis
Descriptive statistics were used to characterize the hospitalizations. Since the analysis was based on hospitalizations rather than patients, single patients may have had multiple hospitalizations in the database.
Incremental costs per additional inpatient day were estimated for the commercially insured population and the Medicare population using three different statistical methods. For each method, separate models were fit for uncomplicated hospitalizations, hospitalizations that included ICU, and ICU costs alone. The primary analysis used ordinary least squares regression (OLS), and was conducted for a base case scenario that excluded hospitalizations with LOS or costs that exceeded the 99th percentile. The OLS analysis averaged the costs across all additional days beyond the first day, and adjusted for other variables that could impact costs. The rationale for excluding the top 1% was to exclude outliers that likely have a large influence on estimated regression coefficients. However, as a sensitivity analysis to assess whether the regression coefficients are stable with the presence of cost outliers, the OLS was also fit using the full cohort for each model. Age group, sex, and geographic region of residence were included as covariates in all OLS models, and for the OLS model for hospitalizations with ICU, iMV was also included as a covariate.
The other two methods of estimating incremental costs were also conducted as sensitivity analyses. The second method considered weighted incremental costs (cost differences between adjacent days of the LOS), which were estimated as previously described by Kozma et al.9 This method takes into account the varying LOS and the fact that costs are not evenly distributed during a stay. In brief, the first step was to calculate the average cost per stay by LOS. Second, the average cost difference between adjacent groups of different LOS was calculated (eg, mean cost of LOS = 5 minus mean cost of LOS = 4). Finally, the weighted difference across all LOS groups was calculated, where the weighting represents the number of hospitalizations in the LOS group. Given that there was generally a small sample that had high LOS, the calculation was capped at the 99th percentile of the LOS distribution. Furthermore, the ICU analyses were not stratified by the presence of iMV, since in the commercial database there were less than 100 hospitalizations with both iMV and ICU use, and the sample sizes per LOS group were less than 10.
The third method was also adapted from Kozma et al,9 and applied a weighted beta to adjust for potential differences in demographics, with the beta representing the increase or decrease in total payment for hospitalization per unit increase in days, with age group, sex and region kept constant. The sequence was to first fit the OLS on hospitalizations with LOS = n and LOS = n+1, with different LOS included as one categorical measure rather than a continuous measure. Next, the model was fit for each LOS pair up to the 99th percentile of LOS, with age group, sex, region of residence, and an indicator of iMV use included. Finally, the weighted average of the fitted regression coefficient was calculated for LOS from each model, where the weight represents the number of hospitalizations in LOS = n+1.
Results
Characteristics of the Cohorts
The attrition table (Table S2) shows that in the commercially insured population, a total of 6055 hospitalizations in 6000 unique patients met all criteria; 54 had a second qualifying hospitalization, and one patient had a third. After excluding the top 1% of LOS and costs, there were 4602 uncomplicated hospitalizations and 1356 hospitalizations with ICU for the base case analysis.
In the Medicare-FFS database, attrition after meeting all criteria resulted in identification of 116,338 unique patients (Table S2). Of these patients, 2081 had multiple qualifying hospitalizations during this period, resulting in a total of 118,419 hospitalizations. After excluding 1867 hospitalizations with LOS and/or total costs above the respective 99th percentiles, the base case study analysis consisted of 116,552 hospitalizations (88,716 uncomplicated and 27,836 hospitalizations with ICU) among 114,617 patients. Readmission hospitalizations due to reasons other than the qualifying criteria were excluded from the analysis.
Although the Medicare FFS database represented an older population relative to those who were commercially insured, within each database, the identified cohorts had similar demographic characteristics (Table 1); no differences were observed in characteristics between the base case and all qualified hospitalization populations (data not shown). While all cohorts had a majority of females (53.7–59.1%), the mean ages of the Medicare-FFS cohorts (79.8–80.8 years) were substantially higher than those from the commercial database (61.2–63.0 years). The LOS was generally longer for hospitalizations with ICU than uncomplicated hospitalizations, and stays were also longer in the Medicare-FFS population relative to the commercially insured population (Table 1).
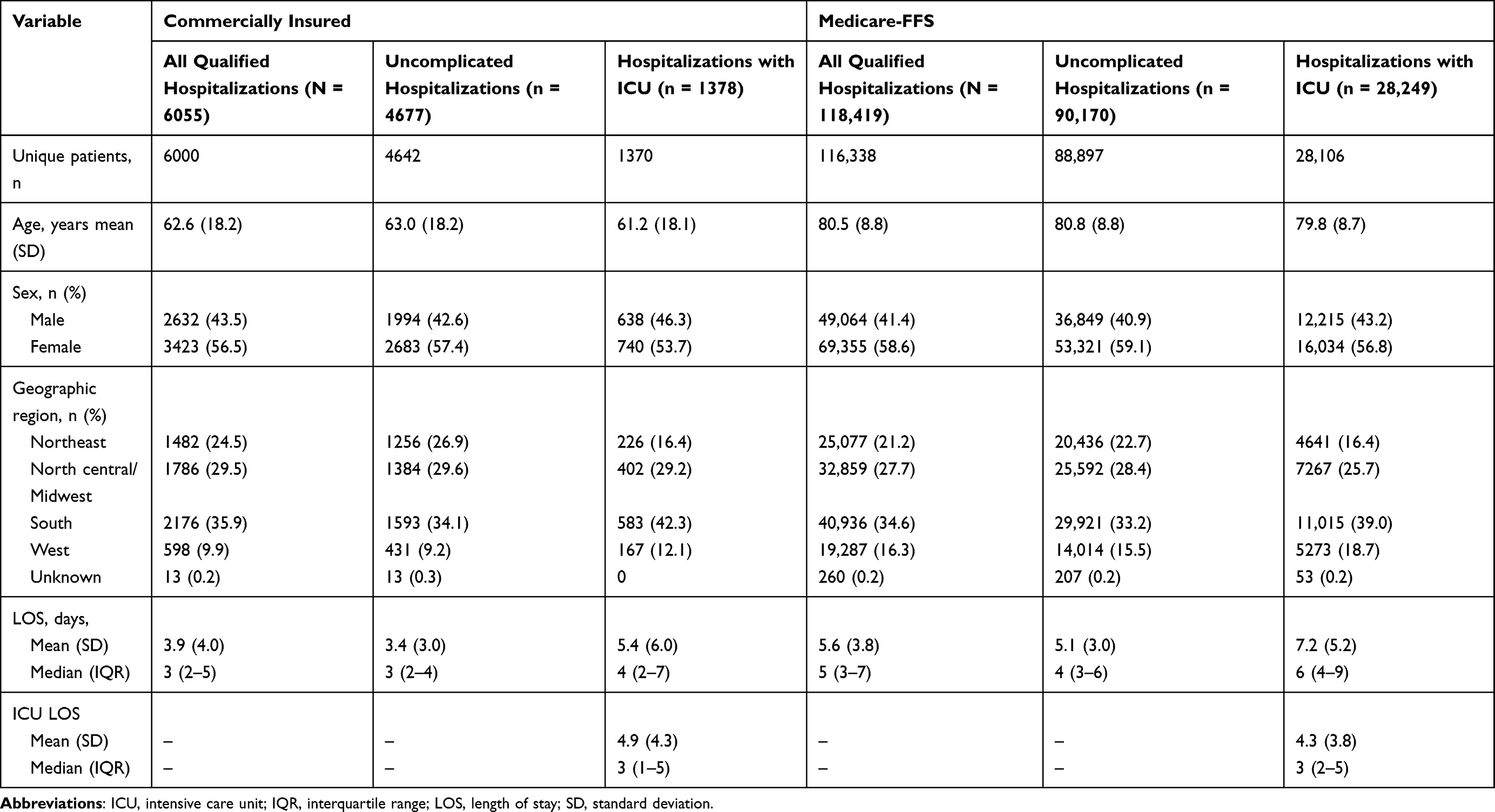 |
Table 1 Characteristics of Hospitalization Stays for Influenza or Viral Pneumonia |
Commercially Insured Population
Mean total costs for uncomplicated hospitalizations for viral pneumonia in the commercially insured population were lower than for the sensitivity analysis on the all-qualified hospitalizations, $15,652 and $16,970, respectively (Figure 1A), reflecting exclusion of LOS or costs that exceeded the 99th percentile. Similarly, mean total costs of hospitalizations with ICU were lower in the base case than for all qualified hospitalizations with ICU, $26,532 and $32,469, respectively.
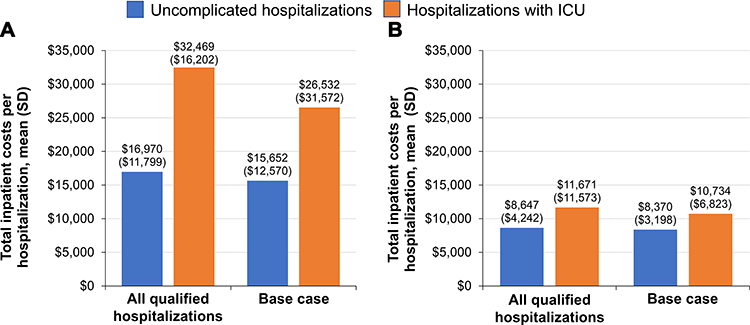 |
Figure 1 Total costs of inpatient stays among the commercially insured (A) and Medicare Fee-for-Service (B) populations. |
The base case estimated incremental costs of each additional day for uncomplicated hospitalizations were $2158 with incremental costs of $3900 for hospitalizations that included ICU, and incremental costs of $5254 per additional ICU day (Table 2). In the OLS sensitivity analysis (all qualified hospitalizations), the incremental costs were $2537, $5646, and $6853 for each additional uncomplicated, hospitalization with ICU, and ICU day, respectively. The sensitivity analyses based on weighted differences and weighted beta also resulted in costs per additional day that were generally consistent with the base case (Table 2).
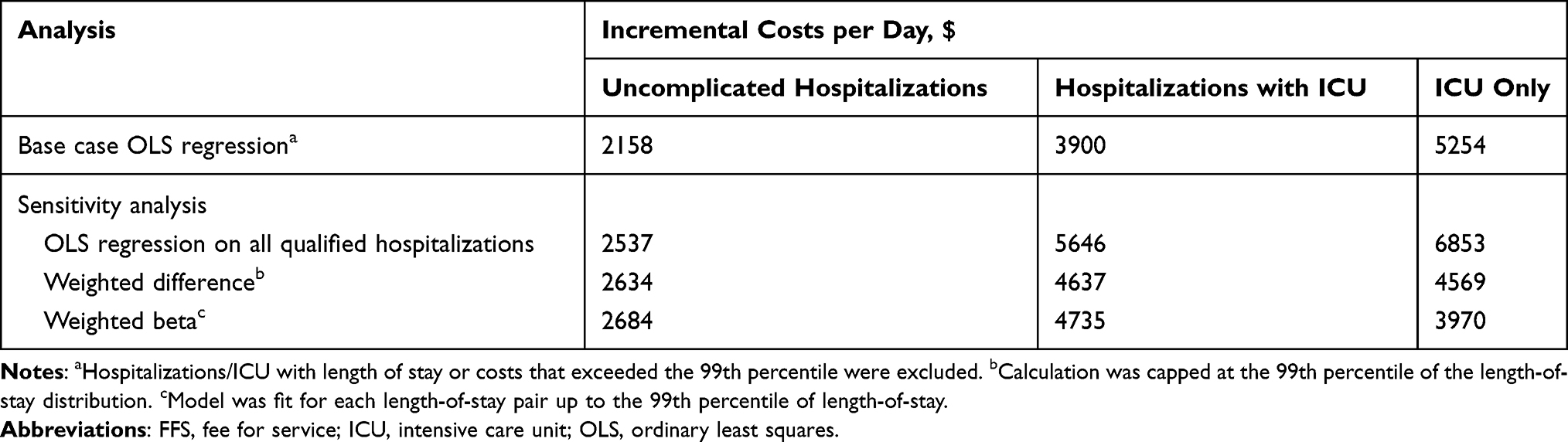 |
Table 2 Estimated Incremental Costs per Additional Day of Hospitalization in the Commercially Insured Population |
The impact of iMV on costs was estimated by including an indicator for use of any iMV in the OLS models for ICU (Table S3). Such use of iMV was associated with costs that would add $35,482 to the costs of hospitalization in the base case, and $19,759 in the sensitivity analysis on all hospitalizations.
Medicare-FFS Population
As shown in Figure 1B for the Medicare-FFS population, the mean total costs were generally similar for all hospitalizations and the base case for both uncomplicated hospitalizations, $8647 and $8370, respectively, and hospitalizations with ICU $11,671 and $10,734, respectively. Estimated incremental costs in the base case OLS model for the Medicare-FFS population were $475, $668, and $608 per additional inpatient day for uncomplicated hospitalizations, hospitalizations that include ICU, and ICU only, respectively (Table 3). In the OLS sensitivity analysis, incremental costs per additional day were $623 for uncomplicated hospitalizations, $1150 for hospitalizations with ICU, and $1260 for ICU. Incremental costs per additional day using weighted differences and weighted beta were similar to the base case, except for slightly lower incremental costs per additional ICU day in the weighted beta model (Table 3).
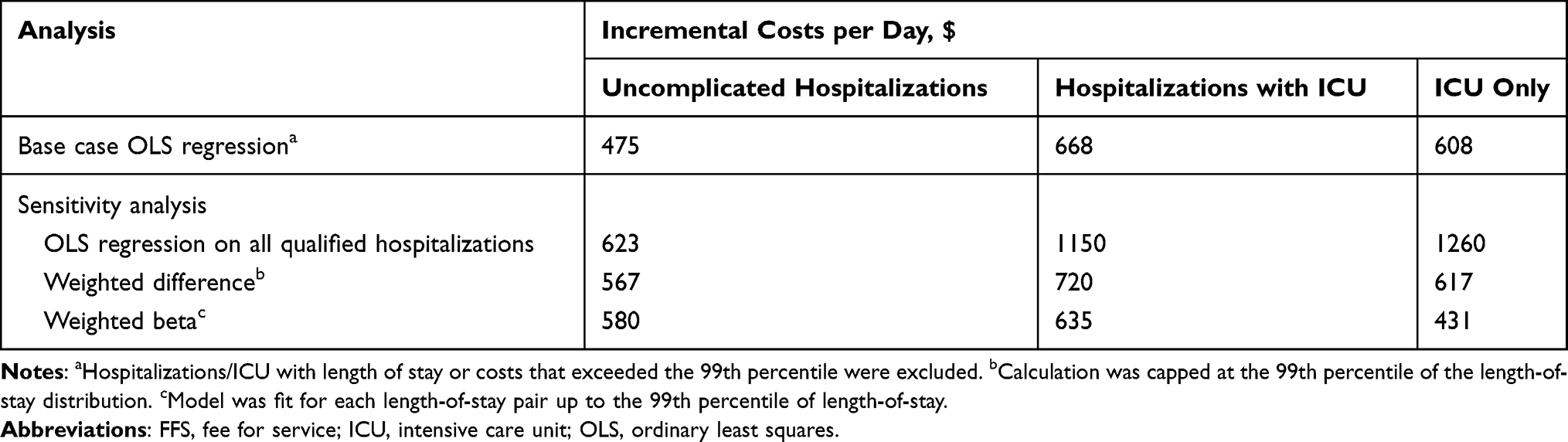 |
Table 3 Estimated Incremental Costs per Additional Day of Hospitalization in the Medicare Fee-for-Service Population |
The estimated costs associated with iMV use in the Medicare-FFS population would add $13,101 and $16,215 to the costs of hospitalization in the base case and sensitivity analysis on all qualified hospitalizations, respectively (Table S4).
Discussion
While daily cost variability inherent to hospitalizations is dependent on the diagnosis and management strategies, this study provides an estimate of the average incremental costs associated with each additional day of hospitalization with and without use of ICU for viral pneumonia, as well as for each additional ICU day by itself. These values can be useful to further determine potential cost savings resulting from treatment-related reductions in LOS, especially as a proxy for viral respiratory diseases such as COVID-19, and may also serve as an estimator in economic analyses. However, actual cost savings resulting from a reduction in LOS resulting from existing or new therapies will also be dependent on the cost of those therapies.
Considering both the base case and the sensitivity analyses for uncomplicated hospitalizations, which taken together suggested that the estimates of incremental costs were robust, the average cost per additional day for an uncomplicated hospitalization may be expected to range from $2158 to $2684 for commercially insured patients, and from $475 to $623 among Medicare-FFS patients. While the commercial costs appear to be similar to the $2273–$2373 in year 2009 dollars reported by Kozma et al9 as cost savings for eliminating a day of hospitalization for community acquired pneumonia, it should be noted that since that study did not stratify by ICU use, those values do not necessarily represent uncomplicated hospitalizations.
For hospitalizations with ICU as well as when the ICU stays were considered separately, the sensitivity analysis on all hospitalizations showed that while estimates of incremental costs were generally stable, average costs per additional day were slightly higher relative to the base case, likely reflecting outliers in these cost categories. These results also suggest that the cost of outliers when ICU is included is greater than outlier costs among uncomplicated hospitalizations, which is not surprising given that patients in the ICU usually require a greater intensity of care.
Across the analyses, it may be expected that the average cost per additional day of hospitalization with ICU would be within the range of $3900–$5646 for commercially insured patients, with each additional day of ICU costing $3970–$6853. Similarly, for Medicare-FFS patients, stays with ICU would be within the range of $635–$1150, with each additional day in ICU costing $431 to $1260. Incremental costs for Medicare-FFS patients were substantially lower than those for the commercially insured population, since these costs represent fixed pricing based on DRGs, with the same reimbursement regardless of the LOS.
For perspective, the 4-day reduction in LOS reported with remdesivir7 could, using the base case scenario, potentially lower the costs of an uncomplicated hospitalization by $8632 and the cost of a hospitalization with ICU by $15,600 among commercially insured patients. These reductions approximate the overall $12,000 in savings that the maker of remdesivir claims would result from an earlier hospital discharge;11 the cost of a course of remdesivir treatment for COVID-19 is $3120 for commercially insured patients. In a Medicare-FFS patient, reductions resulting from a 4-day shorter LOS would be $1900 and $272 for uncomplicated and ICU hospitalizations, respectively; remdesivir costs are $2340 for treatment that is government subsidized. It should be noted that omission of costs associated with a shortened LOS was a shortcoming of a recent Institute for Clinical and Economic Review (ICER) analysis modeling the cost recovery of remdesivir, although the secondary cost-effectiveness model conducted by ICER did account for LOS.12
As shown by the iMV coefficients in the OLS analyses for ICU, use of iMV can be expected to increase the overall hospitalization costs by an average of $35,482 and $13,101 in the commercially insured and Medicare-FFS populations, respectively, although identification of iMV was based on DRG and procedure codes in claims, which precluded accurate estimation of the duration of iMV use and incremental costs per additional inpatient day. A counterintuitive finding was that the additional costs associated with iMV in the commercially insured population were higher in the base case than the sensitivity analysis on all qualified hospitalizations. The position of outliers in the model affects the beta for the iMV estimate, and thus the presence of outliers without iMV and high costs and/or those with iMV but low costs could account for these observed results.
Two recent studies on the costs of iMV can provide additional context to these results. The first study, a meta-regression analysis, showed that iMV substantially increased daily ICU costs by 25% and suggested that LOS is likely to be an important contributor to the iMV cost component.5 However, that study not only noted the paucity of information available on the economic impact of iMV, but also appeared to focus on duration of LOS as an effect of ventilator-assisted pneumonia. That focus is in contrast to the current study, which considered use of iMV as treatment for a primary diagnosis of pneumonia. The second study, relying on data from a single center in the German health system further confirmed iMV as a driver of ICU costs, and showed that while there is variability in the contribution of iMV to the overall daily costs of ICU, respiratory conditions are associated with the highest relative increase in daily costs due to use of iMV (94%) relative to other conditions that may require such use.13 Overall, the available data indicate that reduction in iMV, even in the absence of a reduction in ICU LOS may result in economic benefits, although the relationships among LOS, iMV use, and daily ICU costs need to be more fully characterized.
An important limitation of this study is that it reflects costs associated with viral pneumonia, and although this may be considered a reasonable proxy for COVID-19, the results should be prudently interpreted, since generalizability to hospital stays for other conditions, including COVID-19, is uncertain. Further research is needed to confirm the present methodology within a COVID-19 specific inpatient cohort once such records are adjudicated and become available in commercial and Medicare-FFS claims databases. In this regard, it should also be noted that while there is large variability in LOS for the COVID-19 hospitalizations, many COVID-19 patients have LOS longer than those with viral pneumonia in the current study, especially among COVID-19 patients who require ICU and/or iMV.2–4,14,15 Moreover, the models do not take into consideration additional costs that may be potentially incurred during public health emergencies related to infectious diseases, as additional protocols may be implemented to limit exposure of health workers to infectious pathogens, thereby further increasing the daily cost of inpatient care. The potential for miscoding is a limitation that is associated with databases such as the ones used in the current analysis. Another limitation, as previously mentioned, is that the analyses relied on an indicator for iMV. The exclusion of ECMO may also be considered a limitation, since this treatment modality is also cost-intensive. However, ECMO itself may be associated with prolonged ICU LOS and ventilator support as well as high mortality in patients with viral pneumonia,16 and while it has been used in patients with COVID-19, its therapeutic role in this disease has yet to be determined.
Conclusion
This study provides estimates of the average incremental cost for each additional day of hospitalization with and without use of the ICU. The results can be used to determine the magnitude of economic savings that may be achieved with various reductions in LOS, and emphasize the potential value of drugs that can result in early hospital discharge. Sensitivity analyses further demonstrated that the estimates were robust to methodological variations. This robustness suggests the utility of the estimates in economic analyses to identify additional cost offsets that may demonstrate economic benefits of therapies that reduce LOS, such as new technologies or drugs for the treatment of COVID-19.
Acknowledgments
This study was funded by Regeneron Pharmaceuticals Inc. The authors acknowledge E. Jay Bienen, PhD, for medical writing support, which was funded by Regeneron Pharmaceuticals Inc. The analyses were conducted by Regeneron and Avalere Health.
Disclosure
Ning Wu, Andreas Kuznik, and Degang Wang are employees and stockholders of Regeneron Pharmaceuticals Inc., and Chad Moretz, Ann Xi, Shambhavi Kumar, and Laurie Hamilton are employees of Avalere Health. The authors report no other conflicts of interest in this work.
References
1. Maloney W, Taskin T. Determinants of social distancing and economic activity during COVID-19: a global view. COVID Econ. 2020;13:157–177.
2. Suleyman G, Fadel RA, Malette KM, et al. Clinical characteristics and morbidity associated with coronavirus disease 2019 in a series of patients in metropolitan detroit. JAMA Netw Open. 2020;3(6):e2012270. doi:10.1001/jamanetworkopen.2020.12270
3. Petrilli CM, Jones SA, Yang J, et al. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ. 2020;369:m1966. doi:10.1136/bmj.m1966
4. Cummings MJ, Baldwin MR, Abrams D, et al. Epidemiology, clinical course, and outcomes of critically ill adults with COVID-19 in New York City: a prospective cohort study. Lancet. 2020;395(10239):1763–1770. doi:10.1016/S0140-6736(20)31189-2
5. Kaier K, Heister T, Motschall E, Hehn P, Bluhmki T, Wolkewitz M. Impact of mechanical ventilation on the daily costs of ICU care: a systematic review and meta regression. Epidemiol Infect. 2019;147:e314. doi:10.1017/S0950268819001900
6. Kahn JM, Rubenfeld GD, Rohrbach J, Fuchs BD. Cost savings attributable to reductions in intensive care unit length of stay for mechanically ventilated patients. Med Care. 2008;46(12):1226–1233. doi:10.1097/MLR.0b013e31817d9342
7. Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the treatment of Covid-19 - preliminary report. N Engl J Med. 2020;383(19):1813–1826. doi:10.1056/NEJMoa2007764
8. Raut M, Schein J, Mody S, Grant R, Benson C, Olson W. Estimating the economic impact of a half-day reduction in length of hospital stay among patients with community-acquired pneumonia in the US. Curr Med Res Opin. 2009;25(9):2151–2157. doi:10.1185/03007990903102743
9. Kozma CM, Dickson M, Raut MK, et al. Economic benefit of a 1-day reduction in hospital stay for community-acquired pneumonia (CAP). J Med Econ. 2010;13(4):719–727. doi:10.3111/13696998.2010.536350
10. Harvey MJ, Gaies MG, Prosser LA. US and international in-hospital costs of extracorporeal membrane oxygenation: a systematic review. Appl Health Econ Health Policy. 2015;13(4):341–357. doi:10.1007/s40258-015-0170-9
11. An Open Letter from Daniel O’Day, Chairman & CEO, Gilead Sciences [press release]; June 29. 2020. Available from: https://www.gilead.com/news-and-press/press-room/press-releases/2020/6/an-open-letter-from-daniel-oday-chairman--ceo-gilead-sciences.
12. Institute for clinical and economic review. alternative pricing models for remdesivir and other potential treatments for COVID-19; 2020 [updated June 24, 2020]. Available from: https://icer-review.org/wp-content/uploads/2020/06/ICER-COVID_Revised_Report_20200624.pdf.
13. Kaier K, Heister T, Wolff J, Wolkewitz M. Mechanical ventilation and the daily cost of ICU care. BMC Health Serv Res. 2020;20(1):267. doi:10.1186/s12913-020-05133-5
14. Bhatraju PK, Ghassemieh BJ, Nichols M, et al. Covid-19 in critically ill patients in the Seattle Region - case series. N Engl J Med. 2020;382(21):2012–2022. doi:10.1056/NEJMoa2004500
15. Richardson S, Hirsch JS, Narasimhan M, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. 2020;323(20):2052–2059. doi:10.1001/jama.2020.6775
16. Sukhal S, Sethi J, Ganesh M, Villablanca PA, Malhotra AK, Ramakrishna H. Extracorporeal membrane oxygenation in severe influenza infection with respiratory failure: a systematic review and meta-analysis. Ann Card Anaesth. 2017;20(1):14–21. doi:10.4103/0971-9784.197820
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.