Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Increased Surgical Duration Associated With Prolonged Hospital Stay After Isolated Posterior Cruciate Ligament Reconstruction
Authors Swindell HW ![]() , Boddapati V, Sonnenfeld JJ
, Boddapati V, Sonnenfeld JJ ![]() , Trofa DP, Fleischli JE, Ahmad CS, Popkin CA
, Trofa DP, Fleischli JE, Ahmad CS, Popkin CA ![]()
Received 20 May 2019
Accepted for publication 30 September 2019
Published 10 December 2019 Volume 2019:15 Pages 1417—1425
DOI https://doi.org/10.2147/TCRM.S216384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Hasani W Swindell,1 Venkat Boddapati,1 Julian J Sonnenfeld,1 David P Trofa,1 James E Fleischli,2 Christopher S Ahmad,1 Charles A Popkin1
1Department of Orthopedic Surgery, Columbia University Medical Center, New York, NY, USA; 2Shoulder and Elbow Center, OrthoCarolina Sports Medicine Center, Charlotte, NC, USA
Correspondence: Charles A Popkin
Department of Orthopedic Surgery, Columbia University Medical Center, 622 West 168th Street, PH – 11, New York, New York 10032, USA
Tel +1 212-305-4787
Email [email protected]
Purpose: Although often performed using a variety of reconstructive techniques and strategies, no clinically significant differences presently exist between the approaches available for isolated PCL reconstructions. Given the operatively challenging nature of these procedures, there lies a potentially increased risk of postoperative complications and healthcare expenditures. Our investigation sought to identify patient and surgical risk factors associated with prolonged hospital stays following isolated PCL reconstruction and determine the incidence of 30-day complications after PCL reconstruction using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database.
Method: Patients undergoing isolated PCL reconstructions between 2005 and 2016 were identified in the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database using Current Procedural Terminology codes. Baseline patient and operative characteristics were evaluated as possible risk factors for overnight hospital admissions following PCL reconstruction and analyzed using multivariate analyses.
Results: A total of 249 patients were identified. Multivariate analyses demonstrated that increased operative duration >120 mins (OR 5.04, CI 2.44–10.40; p <0.001) was associated with an increased risk of overnight hospital stay. Major complications occurred in 0.4% (N=1), and minor complications occurred in 0.8% (N=2) with overall complications occurring in 1.2% (N=3) of all patients. Wound dehiscence was the only major complication while superficial surgical site infection and deep vein thrombosis were the only minor complications. 34.1% (N=85) of patients required an overnight hospital stay postoperatively.
Conclusion: Surgical duration >120 mins carried an increased risk of overnight hospital stay after isolated PCL reconstructions. As there are presently minimal significant clinical differences between current PCL reconstruction techniques, improved surgeon familiarity and comfort with a single technique is recommended to decrease operative time and avoid prolonged hospital stays and healthcare expenditures.
Level of evidence: III, retrospective comparative study.
Keywords: operative time, overnight hospital stays, healthcare expenditures, American College of Surgeons National Surgical Quality Improvement Program, NSQIP
Introduction
Knee arthroscopy is one of the most common surgical procedures in the United States with meniscectomy, meniscal repair and cruciate ligament reconstruction composing the majority.1 With otherwise low rates of associated complications and a rising incidence of arthroscopic surgeries performed among patients of all ages, there has also been a concomitant increase in the proportion of procedures performed as outpatients with <1% of arthroscopies performed in an inpatient setting.1,2 An isolated PCL rupture is a relatively uncommon injury, as tears of the PCL are often associated with concurrent knee pathology such as anterior cruciate ligament (ACL), medial collateral ligament or posterolateral corner injuries.3,4 In a review of 222 acute knee injuries, Fanelli et al found that 38.3% involved PCL-related injuries, but only 3.5% were isolated PCL injuries. However, other investigations have studied cohorts with isolated PCL ruptures in up to 18% of patients, and comprising nearly 2% of all American high school knee injuries.5–7
The PCL was classically believed to be composed of independently functioning posteromedial and anterolateral bundles with the latter preventing posterior tibial translation in flexion and the posteromedial bundle more active in extension.8,9 However, more recent biomechanical analyses now suggest more synergistic actions of the two bundles as a result of their anatomical and spatial attachments about the femur and tibia.10–13 Operative management of PCL ruptures is indicated in the setting of concomitant injury to the surrounding collateral ligaments, ACL or meniscus with nonoperative management recommended for isolated and lower severity injuries. The argument for nonoperative management of isolated ruptures is based on the purported intrinsic healing potential of the PCL, although concerns remain on the ligament healing in a lax or attenuated position.14–16 Despite good subjective functional scores and evidence of healing on MRI in the acute postinjury period for conservatively managed isolated PCL tears, less than satisfactory objective scores have been reported.14–19 Additionally, there has been evidence of increased radiographic progression of osteoarthritis and decreased functional outcomes in isolated PCL tears with increasing time from injury, specifically found in 23% of patients at 7 years of follow up, and 41% at 14 years of follow-up.17–19 Several strategies currently exist for PCL reconstruction from single-bundle or double – bundle reconstructions to transtibial and tibial inlay tibial graft fixation strategies however as it stands, no clinically significant differences in outcomes have been uncovered.20–24
Thus, consideration of operative management in select patients has become a topic of discussion; however, given the relatively technically challenging aspects of PCL reconstruction compared to its corollary in anterior cruciate ligament reconstructions, therein lies the potential for increased healthcare expenditures and complications from PCL reconstruction if the appropriate risk stratification or degree of surgical preparation is not performed. To date, most complications with PCL injuries, either isolated or in the setting of associated injuries, are related to residual posterior laxity,21,25,26 popliteal artery laceration or occlusion,27,28 osteonecrosis of the medial femoral condyle29 proximal tibial fracture30 heterotopic ossification in the posterior capsule and decreased knee flexion.5,31 However, given the relatively low rate of reconstruction, most of these complications have been restricted to case reports or small series without any definitive reports on an overall incidence of complications.32 The American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database has previously been applied to examine complications in a multitude of orthopedic procedures2,33–37 however, to date, we are unaware of any study that has analyzed the prolonged length of stay after isolated PCL reconstructions.
The aim of this study was to identify patient and surgeon-related risk factors associated with prolonged hospital stays following isolated PCL reconstruction. A secondary aim was to determine the incidence of 30-day complications after PCL reconstruction using the ACS-NSQIP database. We hypothesized that increased body mass index and operative time would increase the risk of prolonged postoperative hospital stays. We suspected obesity and prolonged surgical duration would predispose patients to an increased risk of perioperative complications thus requiring extended postoperative monitoring and a prolonged hospital stay.
Materials And Methods
This was a retrospective study using the ACS – NSQIP database. This large, multicenter registry contains prospectively collected data on patients undergoing surgery at over 400 hospitals around the United States. Data is collected by trained surgical clinical reviewers who follow patients’ medical charts, collecting demographics, comorbidities, intraoperative variables, and 30-day postoperative major and minor complications based on specified criteria. As such, the NSQIP is a high-quality, accurate database for studying preoperative complications38–41 and has been widely used to investigate complications of orthopedic procedures.33,34,36,38 This database is helpful to our research question because the large sample size provides us with the ability to document rates and risk factors, for relatively rare perioperative complications in less common procedures such as isolated PCL reconstructions. Access to this database was obtained by placing an electronic request through the ACS NSQIP website, and thus institutional review board approval was not required to query this publicly accessible de-identified database.
Patient Selection
The database was surveyed of all cases with the Current Procedural Terminology (CPT) code 29889 (arthroscopically aided posterior cruciate ligament repair/augmentation or reconstruction) and excluded cases with the following primary/concurrent CPT codes: 29888 (arthroscopically aided anterior cruciate ligament repair/augmentation or reconstruction), 27405 (repair of torn collateral ligament or capsule), 27427 (extra-articular ligamentous reconstruction or augmentation), 27428 (open, extra-articular ligamentous reconstruction or augmentation) and 27407 (repair of torn cruciate ligament or capsule) to identify all isolated, elective PCL reconstructions within the database from 2005 to 2016. Those with missing demographic information such as age, height, weight, or sex were excluded from this study. In total, 207 of the 456 patients with a CPT of 29889 met one or more of the exclusion criteria and were removed from the investigation, most commonly for concurrent ligamentous injury (Figure 1).
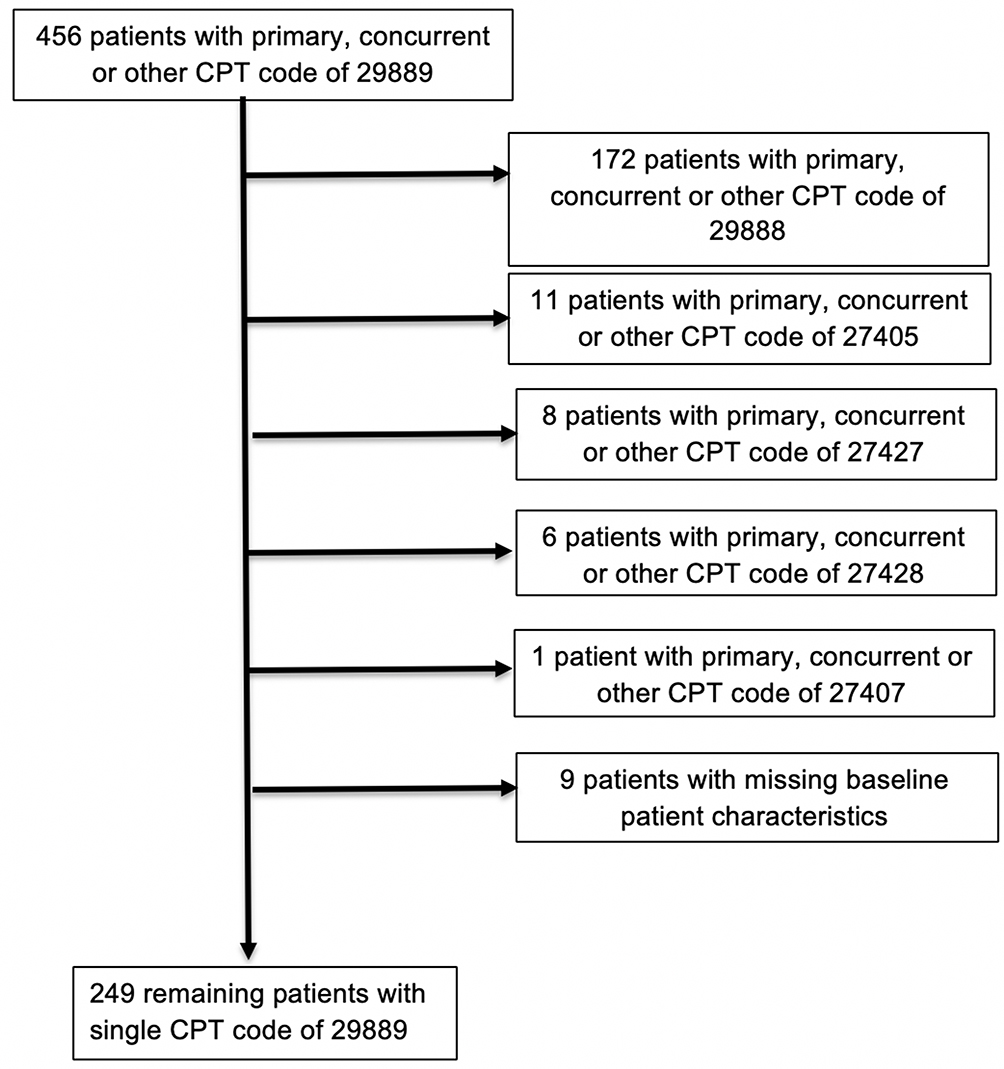 |
Figure 1 STROBE diagram of included and excluded cases of posterior cruciate ligament reconstruction [29889 = arthroscopically aided posterior cruciate ligament augmentation or reconstruction, 29888 = arthroscopically aided anterior cruciate ligament repair/augmentation or reconstruction, 27405 = repair of torn collateral ligament or capsule, 27427 = extra-articular ligamentous reconstruction (augmentation), 27428 = open, extra-articular ligamentous reconstruction (augmentation), 27407 = repair of torn cruciate ligament or capsule]. |
Data Collection
Complications were divided into major and minor categories similar to the manner performed in prior literature.34,38 An overall complication rate, including both major and minor complications, was also included. Patient and surgical characteristics were defined by the ACS and were included in the NSQIP database. Demographic information including age and gender was assessed. Variables that were also analyzed include body mass index (BMI; calculated from patient height and weight, categorized according to the World Health Organization classifications)42 American Society of Anesthesiologists (ASA) classifications, and comorbidities including history of hypertension, diabetes mellitus, tobacco use, and chronic obstructive pulmonary disease (COPD). American Society of Anesthesiology classification was analyzed as a dichotomous value to differentiate the effects of mild versus severe systemic disease on prolonged hospital stay.43 The complications that were assessed are presented in Table 1. The number of patients who required post-procedure overnight hospital stay ≥1 day was also determined.
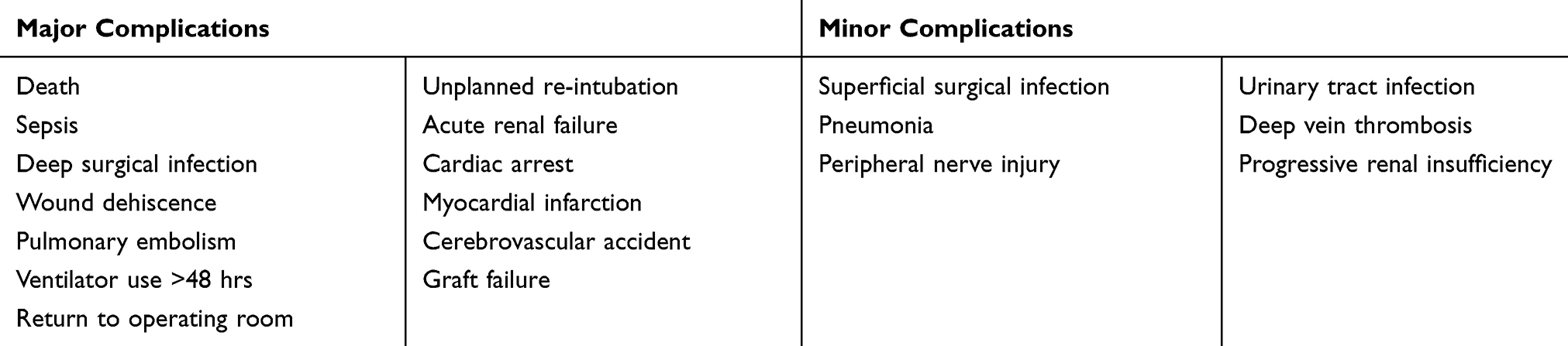 |
Table 1 Major And Minor Perioperative Complications Analyzed Within NSQIP Database |
Statistical Analysis
Statistical analysis was performed using SPSS version 23 (IBM, Armonk, NY). The rates of perioperative complications, readmissions and overnight hospital stays were compared with χ2 tests. A multivariate logistic regression analysis with an overnight length of hospital stay ≥1 day as an outcome variable and baseline patient and operative characteristics as covariates was performed. Regression analysis was performed to identify independent risk factors for overnight hospital stays. A statistically significant p – value was defined as <0.05. Given the use of multiple statistical comparisons within the analysis, a Bonferroni correction was also performed.
Results
In total, 249 isolated PCL reconstruction cases were identified. Of the patients studied, 137 (55%) were <30 years of age, 168 (67.5%) had BMI < 30, 43 (19.7%) were smokers and 77.9% were male (Table 2). The majority of cases (159, 63.9%) lasted more than 120 mins. Based on multivariate analyses, surgical duration lasting more than 120 mins (odds ratio [OR] = 5.04, CI 2.44–10.40; p <0.001) was a statistically significant independent predictor of overnight hospital stay. Use of general anesthesia, BMI >30, increased age >40 years, ASA classification of III or IV, and cigarette use were associated with overnight hospital stays postoperatively; however, these risk factors did not reach statistical significance (Table 3). In terms of complications, major perioperative events occurred in 1 (0.4%) patient and minor complications occurred in 2 (0.8%) patients. Minor complications included wound dehiscence (n = 1, 0.4%), superficial surgical site infection (n = 1 0.4%) and symptomatic deep vein thrombosis requiring treatment (n = 1, 0.4%). Overall, 85 (34.1%) patients remained in the hospital overnight postoperatively.
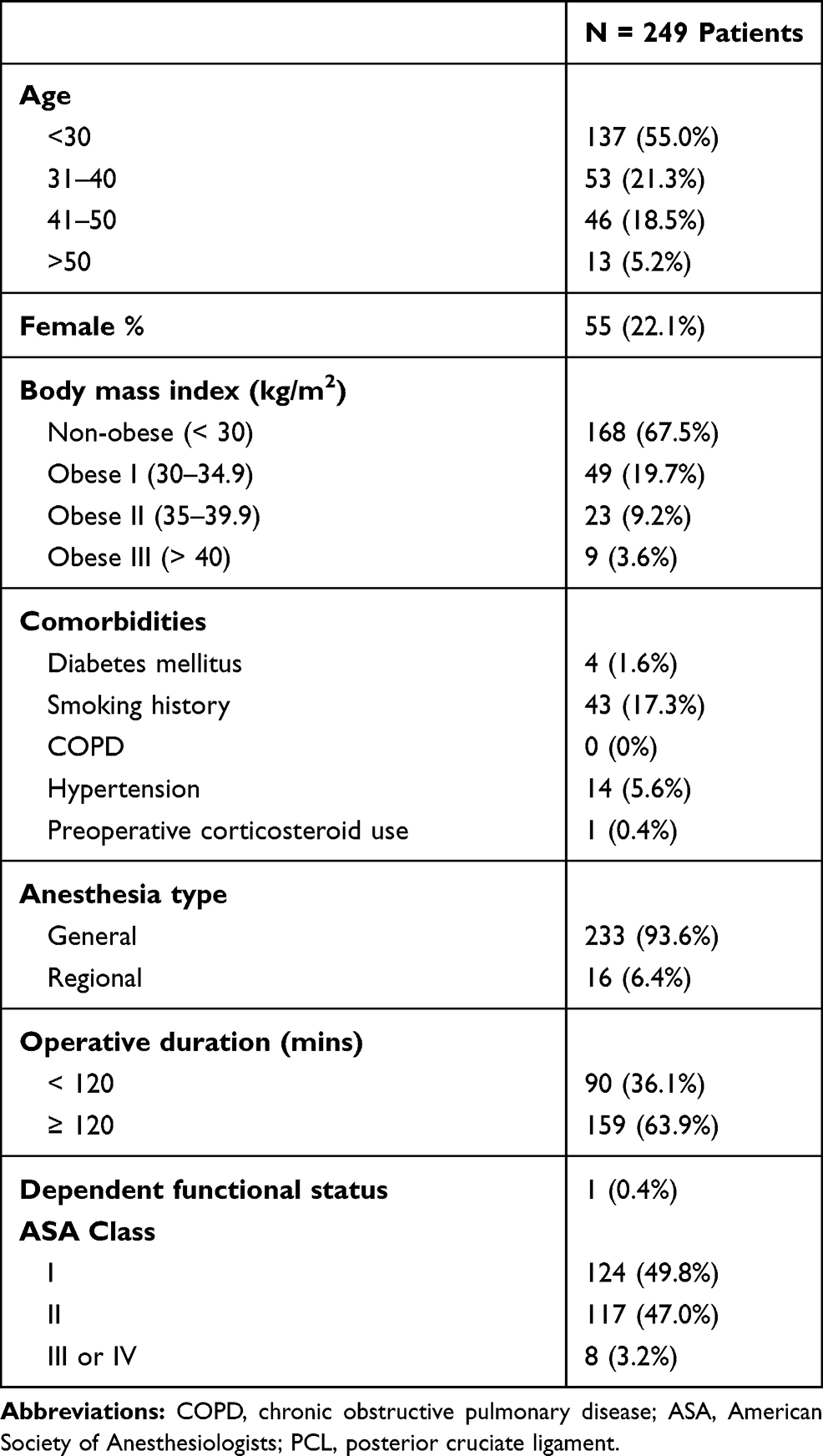 |
Table 2 Baseline Patient And Operative Characteristics Of Patients Undergoing PCL Reconstruction |
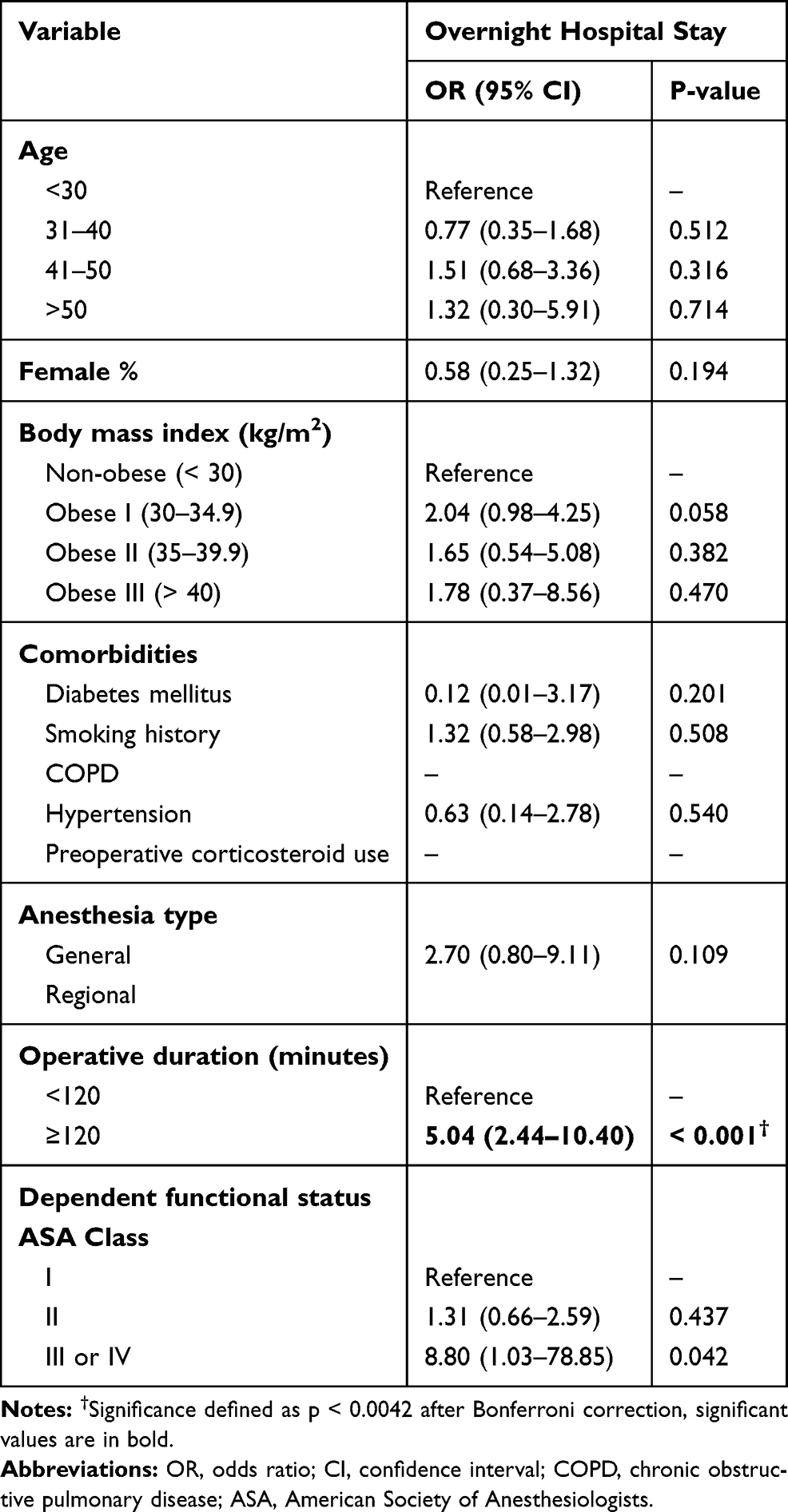 |
Table 3 Independent Risk Factors For Adverse Outcomes By Multivariate Logistic Regression |
Discussion
This study used a large, prospectively collected and multi-institutional registry, to identify patient and surgical risk factors associated with prolonged hospital stays following isolated PCL reconstruction. Overall, 34.1% of patients remained in the hospital for at least one night postoperatively. Multivariate analyses subsequently found prolonged operative time >120 mins to be an independent risk factor for postoperative overnight hospital admissions following PCL reconstruction. In addition, we found the overall rate of complications after PCL reconstruction was found to be 1.2%.
Posterior cruciate ligament reconstruction can be a technically challenging endeavor as the risk of serious and limb or life-threatening injury is a legitimate concern. These considerations could play a role in increasing operative time if the surgeon is unfamiliar with such a procedure. Cadaveric studies note, on average, 29.1 mm separating the mid-PCL from the popliteal artery and 9.7 mm between the proximal PCL fovea and the popliteal artery.44 The degree of knee flexion intraoperatively can further influence this anatomic relationship as greater flexion increases the distance between the tibial insertion of the PCL and the popliteal artery.45 Laceration to the popliteal artery can occur with tibial tunnel drilling, yet similar injury is also possible during posteromedial portal creation or following manipulation of the posterior capsule.32 Although several techniques have been suggested to manage such concerns, such as creating safety incisions, limited capsular releases, or use of the tibial inlay technique, it is impossible to gauge surgeon comfort with such interventions when these difficulties arise intraoperatively.5,46,47
Given the relatively infrequent nature of these procedures and close proximity to critical anatomic structures, there is much to be said about the level of surgeon comfort when indicating and performing these procedures. For example, the transtibial technique is known to be subject to the potential “killer turn” on the posterior aspect of the proximal tibia that can lead to graft abrasion from the sharp graft angulation at the intra-articular portion of the tibial tunnel.48 As a result, the inlay technique was proposed to avoid this sharp bending angle and potential graft injury.49 Despite the proposed improvements in surgical ease, there have been no clinically important differences in Tegner or Lysholm scores, nor differences in residual laxity.50 Furthermore, when comparing single bundle and double-bundle reconstructions, Qi et al’s systematic review by Qi et al found no clear differences in clinical outcomes.51 More recently, Chahla sought to investigate differences in outcomes between double and single-bundle reconstructions 2 years postoperatively. Although both procedures led to an increased patient-reported outcomes and knee stability, double-bundle reconstruction showed improved posterior stability and International Knee Documentation Committee (IKDC) Scores. Yet, there were no other significant differences across other patient-reported outcomes.52 As with most procedures, a learning curve exists before which a surgeon can become facile with a given procedure. Within PCL reconstructions, a variety of procedures and techniques exist with similar functional and objective outcomes however varying levels of difficulty depending on surgeon familiarity. This inference cannot be definitively proven from our study; however, deeper investigation is merited to elucidate if there is a connection between overnight hospital stay in PCL reconstructions, operative duration and surgeon experience.
Under the growing quality-based reimbursement model within orthopedic surgery, physicians must become more cognizant of modifiable risk factors that can reduce adverse outcomes such as increased hospital length of stay for traditionally outpatient procedures.53,54 Across more recent arthroscopy literature, increasing operative time has been associated with increased healthcare utilization in the form of increased risk of readmissions after elective shoulder arthroscopy, and an increased risk of adverse events, extended the length of stay and readmissions in isolated ACL reconstruction.55–57 The findings of our investigation are similar to those of prior studies as the previously unreported variable of procedure length is identified as a factor that may be used for risk stratification in outpatient PCL reconstruction. As there is no clear consensus, at this time, on the overarching clinical and objective benefits between many of the current reconstruction strategies presently available, as surgeons prepare for these cases, the focus should be on decreasing operative time by using more familiar techniques in order to reduce the risk of unexpected health expenditures. Although there is paucity of literature on the subject, surgeon comfort level and the concept of a learning curve associated with PCL reconstruction is a valuable area of interest that could further explain our findings and guide surgeons as they look to surgically manage PCL injuries.
Limitations
There are several limitations to our investigation. The ACS-NSQIP database lacks qualitative postoperative complication data and thus we are unable to identify specific causes behind the reported complications and exact reasons for why patients remained admitted postoperatively. Despite a large number of institutions contributing to the ACS-NSQIP database, it does not capture data from independent outpatient surgical centers. As such, we are unable to generalize our findings to PCL reconstructions performed in surgery centers. In addition, the database lacks orthopedic specific data of such as graft choice, operative indications, the selection of single or double-bundle reconstruction, DVT prophylaxis, postoperative weight-bearing status, pain scores, postoperative range of motion restrictions, patient-reported outcome scores, comparisons between preoperative and postoperative physical examination or symptom scores, and outcomes of interest following PCL reconstruction such as residual laxity or strength. Due to the relative rarity of isolated PCL reconstructions, our sample size may have limited our ability to identify statistically significant associations between patient and surgeon-related risk factors and adverse outcomes. Furthermore, although no prior study has reported on the incidence of complications after isolated PCL reconstruction, the relatively low incidence of complications and operative cases found amongst the cohort studied within the NSQIP database may have precluded further analyses. A prior investigation on anterior cruciate ligament reconstruction used the same database and reported a complication rate of 1.34% in the early postoperative period across 4933 patients.38 In comparison, our study yielded a much smaller study sample of 249 patients but noted a 1.2% incidence of complications. Given the large differences in sample size, we would caution making any definitive claims on the incidence of complications following isolated PCL reconstruction and how it compares to other arthroscopic procedures. Similar to prior research utilizing ACS-NSQIP while data are obtained through trained surgical clinical reviewers and subject to audits by the ACS58 it may suffer from limitations common to large outcome databases including a lack of granularity to the data, as well as improper documentation or coding by individual physicians and medical groups contributing to the database. Although we mention discussions in the literature regarding the argument against nonoperative management, we are unable to make the claim that this procedure is being performed more frequently as no information is available on recent trends in isolated PCL reconstructions. Ultimately, larger prospective cohort or randomized controlled studies with long-term follow-up and homogenous patient populations are needed to better illustrate the complete complication profile, demographics and operative indications following isolated PCL reconstructions. The use of the ACS-NSQIP database allowed us to determine patient and surgical risk factors associated with prolonged hospital stays across a relatively uncommon arthroscopic procedure by using prospectively, and rigorously collected data obtained from a multitude of institutions. It is our hope that our findings will highlight patient and surgeon-specific factors that can increase the risk of further healthcare expenditures for traditionally outpatient procedures.
Conclusion
Surgical duration >120 mins carried an increased risk of overnight hospital stay after isolated PCL reconstructions. As there are presently minimal significant clinical differences between current PCL reconstruction techniques, improved surgeon familiarity and comfort with a single technique is recommended to decrease operative time and avoid prolonged hospital stays and healthcare expenditures.
Disclosure
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. No funds were received in support of this study. Outside of the submitted work, James E Fleischli has received research support from Arthrex. Inc and Smith and Nephew. Christopher S. Ahmad has received IP royalties, consulting fees and research support from Arthrex, Inc, Stock or stock options from At Peak, publishing royalties, financial or material support from Lead Player, Research support from Major League Baseball, and research support from Stryker. Charles A Popkin has received financial or material support and research support from Arthrex, Inc., financial or material support from Smith & Nephew and personal fees from Gotham Surgical Solutions. Hasani W Swindell, Venkat Boddapati, Julian J Sonnenfeld and David P Trofa declare that they have no conflict of interest.
References
1. Kim S, Bosque J, Meehan JP, Jamali A, Marder R. Increase in outpatient knee arthroscopy in the United States: a comparison of National Surveys of Ambulatory Surgery, 1996 and 2006. J Bone Jt Surgery-American Vol. 2011;93(11):994–1000. doi:10.2106/JBJS.I.01618
2. Martin CT, Pugely AJ, Gao Y, Wolf BR. Risk factors for thirty-day morbidity and mortality following knee arthroscopy. J Bone Jt Surg Am Vol. 2013;95(14):
3. Becker EH, Watson JD, Dreese JC. Investigation of multiligamentous knee injury patterns with associated injuries presenting at a level I trauma center. J Orthop Trauma. 2013;27(4):226–231. doi:10.1097/BOT.0b013e318270def4
4. Fanelli GC. Posterior cruciate ligament rehabilitation: how slow should we go? Arthroscopy. 2008;24(2):234–235. Accessed December 31, 2018. doi:10.1016/j.arthro.2007.09.009
5. Fanelli GC, Monahan TJ. Complications in posterior cruciate ligament and posterolateral corner surgery. Oper Tech Sports Med. 2001;9(2):96–99. doi:10.1053/OTSM.2001.21912
6. Spiridonov SI, Slinkard NJ, LaPrade RF. Isolated and combined grade-III posterior cruciate ligament tears treated with double-bundle reconstruction with use of endoscopically placed femoral tunnels and grafts: operative technique and clinical outcomes. J Bone Joint Surg Am. 2011;93(19):1773–1780. doi:10.2106/JBJS.J.01638
7. Fanelli GC, Edson CJ. Posterior cruciate ligament injuries in trauma patients: part II. Arthroscopy. 1995;11(5):526–529. Accessed December 31, 2018.. doi:10.1016/0749-8063(95)90127-2
8. Girgis FG, Marshall JL, Monajem A. The cruciate ligaments of the knee joint. Anatomical, functional and experimental analysis. Clin Orthop Relat Res. (106):216–231. Accessed December 31, 2018.
9. Van Dommelen BA, Fowler PJ. Anatomy of the posterior cruciate ligament. A review. Am J Sports Med. 1989;17(1):24–29. doi:10.1177/036354658901700104
10. Ahmad CS, Cohen ZA, Levine WN, Gardner TR, Ateshian GA, Mow VC. Codominance of the individual posterior cruciate ligament bundles. An analysis of bundle lengths and orientation. Am J Sports Med. 2003;31(2):221–225. doi:10.1177/03635465030310021101
11. Harner CD, Janaushek MA, Kanamori A, Yagi M, Vogrin TM, Woo SL-Y. Biomechanical analysis of a double-bundle posterior cruciate ligament reconstruction. Am J Sports Med. 2000;28(2):144–151. doi:10.1177/03635465000280020201
12. Kennedy NI, Wijdicks CA, Goldsmith MT, et al. Kinematic analysis of the posterior cruciate ligament, part 1: the individual and collective function of the anterolateral and posteromedial bundles. Am J Sports Med. 2013;41(12):2828–2838. doi:10.1177/0363546513504287
13. Papannagari R, DeFrate LE, Nha KW, et al. Function of posterior cruciate ligament bundles during in vivo knee flexion. Am J Sports Med. 2007;35(9):1507–1512. doi:10.1177/0363546507300061
14. Jacobi M, Reischl N, Wahl P, Gautier E, Jakob RP. Acute isolated injury of the posterior cruciate ligament treated by a dynamic anterior drawer brace. J Bone Joint SurgBr.2010;92-B(10):1381–1384. doi:10.1302/0301-620X.92B10.24807
15. Shelbourne KD, Davis TJ, Patel DV. The natural history of acute, isolated, nonoperatively treated posterior cruciate ligament injuries. A prospective study. AmJSportsMed. 1999;27(3):276–283. doi:10.1177/03635465990270030201
16. Tewes DP, Fritts HM, Fields RD, Quick DC, Buss DD. Chronically injured posterior cruciate ligament: magnetic resonance imaging. Clin Orthop Relat Res. 1997;(335):224–232. Accessed December 31, 2018. doi:10.1097/00003086-199702000-00022
17. Keller PM, Shelbourne KD, McCarroll JR, Rettig AC. Nonoperatively treated isolated posterior cruciate ligament injuries.AmJSportsMed. 1993;21(1):132–136. doi:10.1177/036354659302100122
18. Patel DV, Allen AA, Warren RF, Wickiewicz TL, Simonian PT. The nonoperative treatment of acute, isolated (partial or complete) posterior cruciate ligament-deficient knees: an intermediate-term follow-up study.HSSJ.2007;3(2):137–146. doi:10.1007/s11420-007-9058-z
19. Shelbourne KD, Clark M, Gray T. Minimum 10-year follow-up of patients after an acute, isolated posterior cruciate ligament injury treated nonoperatively. Am J Sports Med.2013;41(7):1526–1533. doi:10.1177/0363546513486771
20. Berg EE. Posterior cruciate ligament tibial inlay reconstruction. Arthroscopy. 1995;11(1):69–76. Accessed March 26, 2019. doi:10.1016/0749-8063(95)90091-8
21. Hermans S, Corten K, Bellemans J. Long-term results of isolated anterolateral bundle reconstructions of the posterior cruciate ligament. Am J Sports Med. 2009;37(8):1499–1507. doi:10.1177/0363546509333479
22. MacGillivray JD, Stein BES, Park M, Allen AA, Wickiewicz TL, Warren RF. Comparison of tibial inlay versus transtibial techniques for isolated posterior cruciate ligament reconstruction: minimum 2-year follow-up.Arthroscopy. 2006;22(3):320–328. doi:10.1016/j.arthro.2005.08.057
23. Panchal HB, Sekiya JK. Open tibial inlay versus arthroscopic transtibial posterior cruciate ligament reconstructions.Arthrosc J Arthrosc Relat Surg. 2011;27(9):1289–1295. doi:10.1016/j.arthro.2011.04.007
24. Wijdicks CA, Kennedy NI, Goldsmith MT, et al. Kinematic analysis of the posterior cruciate ligament, part 2: a comparison of anatomic single- versus double-bundle reconstruction.AmJSportsMed. 2013;41(12):2839–2848. doi:10.1177/0363546513504384
25. Park SE, Stamos BD, DeFrate LE, Gill TJ, Li G. The effect of posterior knee capsulotomy on posterior tibial translation during posterior cruciate ligament tibial inlay reconstruction.AmJSportsMed. 2004;32(6):1514–1519. doi:10.1177/0363546504265594
26. Adachi N, Ochi M, Uchio Y, Iwasa J, Ishikawa M, Shinomiya R. Temporal change of joint position sense after posterior cruciate ligament reconstruction using multi-stranded hamstring tendons. Knee Surg Sports TraumatolArthrosc.2007;15(1):2–8. doi:10.1007/s00167-006-0127-5
27. Makino A, Costa-Paz M, Aponte-Tinao L, Ayerza MA, Muscolo DL. Popliteal artery laceration during arthroscopic posterior cruciate ligament reconstruction. Arthroscopy.2005;21(11):1396. doi:10.1016/j.arthro.2005.08.028
28. Wu R-W, Hsu -C-C, Wang C-J. Acute popliteal artery occlusion after arthroscopic posterior cruciate ligament reconstruction.Arthroscopy. 2003;19(8):889–893. Accessed December 31, 2018.. doi:10.1016/S0749-8063(03)00747-3
29. Athanasian EA, Wickiewicz TL, Warren RF. Osteonecrosis of the femoral condyle after arthroscopic reconstruction of a cruciate ligament. Report of two cases. J Bone Joint Surg Am. 1995;77(9):1418–1422. AccessedDecember31,2018.. doi:10.2106/00004623-199509000-00018
30. Malek MM, Fanelli GC. Technique of arthroscopically assistedPCLreconstruction.Orthopedics. 1993;16(9):961–966. Accessed December 31, 2018.
31. Irrgang JJ, Harner CD. Loss of motion following knee ligamentreconstruction.SportsMed. 1995;19(2):150–159.doi:10.2165/00007256-199519020-00006
32. Zawodny SR, Miller MD. Complications of posterior cruciate ligament surgery. Sports Med Arthrosc. 2010;18(4):269–274. doi:10.1097/JSA.0b013c181f2fc2
33. Basques BA, Gardner EC, Varthi AG, et al. Risk factors for short-term adverse events and readmission after arthroscopic meniscectomy: does age matter? Am J Sports Med. 2015;43(1):169–175. doi:10.1177/0363546514551923
34. Martin CT, Gao Y, Pugely AJ, Wolf BR. 30-day morbidity and mortality after elective shoulder arthroscopy: a review of 9410 cases. J Shoulder Elb Surg.2013;22(12):1667–1675.e1. doi:10.1016/j.jse.2013.06.022
35. Shields E, Thirukumaran C, Thorsness R, Noyes K, Voloshin I. An analysis of adult patient risk factors and complications within 30 days after arthroscopic shoulder surgery. Arthrosc J Arthrosc Relat Surg. 2015;31(5):807–815. doi:10.1016/j.arthro.2014.12.011
36. Boddapati V, Fu MC, Schairer WW, et al. Increased shoulder arthroscopy time is associated with overnight hospital stay and surgical site infection. Arthrosc J ArthroscRelatSurg.2018;34(2):363–368. doi:10.1016/j.arthro.2017.08.243
37. Waterman BR, Dunn JC, Bader J, Urrea L, Schoenfeld AJ, Belmont PJ. Thirty-day morbidity and mortality after elective total shoulder arthroplasty: patient-based and surgical risk factors. J Shoulder Elb Surg.2015;24(1):24–30. doi:10.1016/j.jse.2014.05.016
38. Cvetanovich GL, Chalmers PN, Verma NN, Cole BJ, Bach BR. Risk factors for short-term complications of anterior cruciate ligament reconstruction in the United States. Am J Sports Med. 2016;44(3):618–624. doi:10.1177/0363546515622414
39. Cima RR, Lackore KA, Nehring SA, et al. How best to measure surgical quality? Comparison of the Agency for Healthcare Research and Quality Patient Safety Indicators (AHRQ-PSI) and the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) postoperative adverse events at a single institution. Surgery. 2011;150(5):943–949. doi:10.1016/j.surg.2011.06.020
40. Hutter MM, Rowell KS, Devaney LA, et al. Identification of surgical complications and deaths: an assessment of the traditional surgical morbidity and mortality conference compared with the American College of Surgeons-National Surgical Quality Improvement Program.JAmCollSurg. 2006;203(5):618–624. doi:10.1016/j.jamcollsurg.2006.07.010
41. Davenport DL, Holsapple CW, Conigliaro J. Assessing surgical quality using administrative and clinical data sets: a direct comparison of the University HealthSystem Consortium Clinical Database and the National Surgical Quality Improvement Program data set. Am J Med Qual. 2009;24(5):395–402. doi:10.1177/1062860609339936
42. World Health Organization: BMI Classification. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
43. Hackett NJ, De Oliveira GS, Jain UK, Kim JYS. ASA class is a reliable independent predictor of medical complications and mortality following surgery. Int J Surg. 2015;18:184–190. doi:10.1016/J.IJSU.2015.04.079
44. Cosgarea AJ, Kramer DE, Bahk MS, Totty WG, Matava MJ. Proximity of the popliteal artery to the PCL during simulated knee arthroscopy: implications for establishing the posterior trans-septal portal. J Knee Surg. 2006;19(3):181–185. Accessed December 31, 2018.. doi:10.1055/s-0030-1248103
45. Matava MJ, Sethi NS, Totty WG. Proximity of the posterior cruciate ligament insertion to the popliteal artery as a function of the knee flexion angle: implications for posterior cruciate ligament reconstruction. Arthroscopy. 2000;16(8):796–804. AccessedDecember31,2018. doi:10.1053/jars.2000.18243
46. Ahn JH, Wang JH, Lee SH, Yoo JC, Jeon WJ. Increasing the distance between the posterior cruciate ligament and the popliteal neurovascular bundle by a limited posterior capsular release during arthroscopic transtibial posterior cruciate ligament reconstruction. AmJSportsMed.2007;35(5):787–792. doi:10.1177/0363546506297908
47. Miller MD, Kline AJ, Gonzales J, Beach WR. Vascular risk associated with a posterior approach for posterior cruciate ligament reconstruction using the tibial inlay technique.JKneeSurg.2002;15(3):137–140. Accessed December 31, 2018. http://www.ncbi.nlm.nih.gov/pubmed/12152973.
48. LaPrade CM, Civitarese DM, Rasmussen MT, LaPrade RF. Emerging updates on the posterior cruciate ligament. Am J Sports Med. 2015;43(12):3077–3092. doi:10.1177/0363546515572770
49. May JH, Gillette BP, Morgan JA, Krych AJ, Stuart MJ, Levy BA. Transtibial versus inlay posterior cruciate ligament reconstruction: an evidence-based systematic review. J Knee Surg. 2010;23(2):73–79. Accessed March 27, 2019. doi:10.1055/s-0030-1267468
50. Shin Y-S, Kim H-J, Lee D-H. No clinically important difference in knee scores or instability between transtibial and inlay techniques for PCL reconstruction: a systematic review. ClinOrthopRelatRes. 2017;475(4):1239–1248. doi:10.1007/s11999-016-5176-6
51. Qi Y-S, Wang H-J, Wang S-J, Zhang -Z-Z, Huang A-B, Yu J-K. A systematic review of double-bundle versus single-bundle posterior cruciate ligament reconstruction. BMC MusculoskeletDisord.2016;17:45. doi:10.1186/s12891-016-0896-z
52. Chahla J, Moatshe G, Cinque ME, et al. Single-bundle and double-bundle posterior cruciate ligament reconstructions: a systematic review and meta-analysis of 441 patients at a minimum 2 years’ follow-up. ArthroscJArthroscRelatSurg.2017. doi:10.1016/j.arthro.2017.06.049
53. Porter ME. A strategy for health care reform — toward a value-based system. N Engl J Med. 2009;361(2):109–112. doi:10.1056/NEJMp0904131
54. Pierce RG, Bozic KJ, Bradford DS. Pay for Performance in Orthopaedic Surgery. Clin Orthop Relat Res.2007;PAP:87–95. doi:10.1097/BLO.0b013e3180399418
55. Hill JR, McKnight B, Pannell WC, et al. Risk factors for 30-day readmission following shoulder arthroscopy. Arthrosc J Arthrosc Relat Surg. 2017;33(1):55–61. doi:10.1016/j.arthro.2016.06.048
56. Agarwalla A, Gowd AK, Liu JN, et al. Effect of operative time on short-term adverse events after isolated anterior cruciate ligament reconstruction. Orthop J Sport Med. 2019;7(2):232596711882545. doi:10.1177/2325967118825453
57. Boddapati V, Fu MC, Nwachukwu BU, et al. Procedure length is independently associated with overnight hospital stay and 30-day readmission following anterior cruciate ligament reconstruction. Knee Surg Sport Traumatol Arthrosc. 2019. doi:10.1007/s00167-019-05622-z
58. American College of Surgeons - National Surgical Quality Improvement Program. American College of Surgeons - National Surgical Quality Improvement Program. Available from: https://www.facs.org/quality-programs/acs-nsqip/participant-use. Published 2014.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.