")
Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 15
Increased Risk of Acute Lymphoblastic Leukemia in Adult Patients with GSTM1 Null Genetic Polymorphism
Authors Abdalhabib EK , Alzahrani B, Alanazi F, Algarni A , Ibrahim IK , Mohamed HA, Hamali HA , Mobarki AA, Dobie G , Saboor M
Received 29 December 2021
Accepted for publication 4 March 2022
Published 15 March 2022 Volume 2022:15 Pages 227—234
DOI https://doi.org/10.2147/PGPM.S356302
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Martin H Bluth
Ezeldine K Abdalhabib,1 Badr Alzahrani,1 Fehaid Alanazi,1 Abdulrahman Algarni,2 Ibrahim Khider Ibrahim,3 Hozifa A Mohamed,4,5 Hassan A Hamali,6 Abdullah A Mobarki,6 Gasim Dobie,6 Muhammad Saboor6,7
1Department of Clinical Laboratory Sciences, College of Applied Medical Sciences, Jouf University, Al-Qurayyat, Saudi Arabia; 2Department of Medical Laboratory Technology, College of Applied Medical Sciences, Northern Borders University, Arar, Saudi Arabia; 3Department of Hematology, Faculty of Medical Laboratory Sciences, Al Neelain University, Khartoum, Sudan; 4Department of Molecular Biology, Faculty of Medical Laboratory Sciences, Al Neelain University, Khartoum, Sudan; 5Department of Molecular Biology, Faculty of Medical Laboratory Sciences, Sudan International University, Khartoum, Sudan; 6Department of Medical Laboratory Technology, Faculty of Applied Medical Sciences, Jazan University, Jazan, Saudi Arabia; 7Medical Research Center (MRC), Jazan University, Jazan, Saudi Arabia
Correspondence: Muhammad Saboor, Department of Medical Laboratory Technology, Faculty of Applied Medical Science, Jazan University, Jazan, Saudi Arabia, Tel +966 54 495 9029, Email [email protected]
Purpose: Glutathione S-transferases (GSTT1 and GSTM1) detoxify various endogenous and exogenous compounds and provide cytoprotective role against reactive species. This study aimed to assess the frequency of GSTT1, and GSTM1 polymorphisms in newly diagnosed Sudanese adult patients with acute lymphoblastic leukemia (ALL) and to evaluate the association of these polymorphisms with age, gender and type of ALL.
Patients and Methods: This case–control study included 128 adult Sudanese, untreated newly diagnosed patients with ALL, aged 18 to 74 years and 128 age-gender matched healthy controls. Deletional polymorphisms of GSTT1 and GSTM1 genes were genotyped through a multiplex polymerase chain reaction (PCR) assay using β-globin gene as an internal positive control.
Results: The genotypic frequency of GSTT1 null polymorphism was 22.7% in cases and 14.8% in controls (OR = 1.68, P = 0.111). Statistically significant differences were noted in the frequencies of GSTM1 null polymorphism in cases and controls (OR = 3.7, P = < 0.001). Combined GSTT1 null and GSTM1 null gene polymorphisms showed statistically significant difference in patients with ALL as compared to controls (OR = 6.5, CI 95% = 1.42– 29.74, P < 0.001).
Conclusion: Irrespective of age at diagnosis, gender, and phenotype of ALL, GSTM1 null polymorphism either alone or in combination with GSTT1 null polymorphism poses significantly increased risk of developing ALL in adults.
Keywords: GSTT1, GSTM1, polymorphism, acute lymphoblastic leukemia
Introduction
Acute lymphoblastic leukemia (ALL) is a lymphoproliferative neoplastic disorder characterized by malignant proliferation, impaired differentiation, maturation and accumulation of lymphoid progenitors in the bone marrow and their presence in the blood and/or extramedullary sites.1 Approximately 80% of ALL cases are reported in children, although relatively uncommon it has devastating effects in adult patients. Because of the relapse, the cure rates range between 40–50% in adult patients with ALL and the 5–year overall survival is just 30–40%.1,2 Ethnicity has also shown positive association with the incidence and outcome of ALL.3 Although, the exact etiology of ALL is not well defined, certain genetic disorders (Down syndrome, Fanconi’s anemia, Bloom syndrome, ataxia telangiectasia and Nijmegen breakdown syndrome), ionizing radiation, chemicals (pesticides, benzene), and viral infections (Epstein-Barr Virus and Human Immunodeficiency virus) have been proved to be the predisposing factors for the development of ALL. Additionally, somatic chromosomal aberrations including t (12;21) [ETV6-RUNX1], t(1;19) [TCF3-PBX1], t(9;22) [BCR-ABL1] are the hallmark of ALL.1
Hematopoietic precursor cells’ DNA damages are instrumental for the development of leukemia. Amongst others, reactive species produced either endogenously or exogenously by environmentally encountered carcinogens can damage the DNA of hematopoietic progenitors.4 Glutathione S-transferases (GTs) are oxidative stress Phase II detoxification enzymes, encoded by eight highly polymorphic genes. In addition to several functions, GTs play an instrumental role in the detoxification of various endogenous and exogenous compounds (carcinogens, chemotherapeutic drugs, and environmental pollutants) by catalyzing conjugation of glutathione (GSH) and protects the tissues from the toxic effects of reactive electrophiles.5–7 Polymorphisms of the GTs genes including GSTT1, located on chromosome 1q13.3, and GSTM1, on chromosome 22q11.2, might encode loss–of–function enzymes compromising the activity of GTs leading to several types of malignancies including hematological neoplasms.4, 8–12 Furthermore, administration of chemotherapeutic drugs in patients with malignancies could also develop secondary neoplasia due to the impaired detoxification process of GTs.12,13
Literature shows conflicting results of GSTT1 and GSTM1 polymorphisms and their association with the risk for developing ALL.4, 14–25 GSTM1 polymorphism has shown increased risk of developing ALL in children while GSTT1 was found not to predispose to childhood ALL.26 Additionally, patients with combined genotype (GSTT1 null and GSTM1 null) were found to be at slight increased risk of relapse.27 In a meta-analysis of 30 published case control studies, significantly increased risk of ALL showed association with GSTM1 and GSTT1 null genotypes {pooled ORs 1.24 (95% CI 1.17–1.31) and 1.30 (95% CI 1.06–1.60), respectively}.28 Several studies have evaluated the association of GSTT1 and GSTM1 polymorphisms as predisposing genetic risk factors for the development of chronic myeloid leukemia in Sudanese population.5,29,30 However, data about these polymorphisms in patients with ALL is scarce in Sudanese. This study aimed to investigate GSTT1, and GSTM1 polymorphisms in newly untreated diagnosed Sudanese adult patients with ALL and to evaluate the association of these polymorphisms with age, gender and phenotype of ALL.
Materials and Methods
All study participants in this case–control study were Sudanese, and included 128 adult patients diagnosed with ALL, aged 18 to 74 years (75 males and 53 females) and 128 normal healthy controls (88 males and 40 females). Patients were recruited from the Radiation and Isotope Center in Khartoum (RICK) during December 2019 and June 2021, before starting the treatment. This study was approved by the ethical committee at Al-Neelain University in Khartoum, Sudan. In accordance with the Declaration of Helsinki, each participant provided written informed consent. There was no previous history or diagnosis of other malignancies among the patients enrolled in the study. All patients were diagnosed by hemato–oncologists through complete blood count, bone marrow examination, and flow cytometry. To represent the same age range and ethnic background as the patients, controls from the same geographic area were selected with no prior history or evidence of malignancy. A structured questionnaire was used to record clinical and demographic data. A total of three mL of EDTA anticoagulated venous blood samples was collected from the subjects for PCR analysis after establishing the diagnosis of ALL.
DNA Extraction
Using a commercially available kit (QIAamp® DNA Mini kit; Qiagen GmbH, Hilden, Germany), DNA was isolated from peripheral blood samples according to the manufacturer’s protocol. The quantity and quality of extracted DNA was verified using gene quant device (Amersham Biosciences – Biochrom LTD, Cambridge CB4, England). Until analysis, aliquots of the extracted DNA samples were stored at –20°C.
Molecular Analysis
The genomic DNA was used for the analysis of GSTT1 and GSTM1 gene polymorphisms through multiplex polymerase chain reaction (PCR) assay using β–Globin gene as an internal positive control. PCR reaction was carried out utilizing a total volume of 25 µL which was prepared by adding 100–150 ng of genomic DNA in a 10x PCR buffer mixture containing 0.5 units of Taq polymerase, 1.5 µM MgCl2, and 200 µM dNTPs. The specific primers used and PCR conditions were similar to those described by Agrawal et al.31 An agarose gel electrophoresis was used to examine the banding patterns of the amplified products. A PCR product with 268 bp indicated successful amplification. Based on the presence or absence of a band at 480 bp and 215 bp, GSTT1 and GSTM1 genotypes were identified respectively. This method does not distinguish heterozygous and homozygous null (GSTT1 and GSTM1) genotypes.
Statistical Analysis
The statistical analysis including descriptive statistics of mean, standard deviation, odds ratio (OR) with a confidence interval (CI) of 95% were performed using statistical package for social sciences (SPSS) for Windows (Chicago, IL, USA) version 23. The genotype distributions of patients and controls were compared using Pearson’s chi-square tests. In addition, quantitative variables were also tested using an independent t-test. Statistical significance was determined by a P value less than 0.05.
Results
This study evaluated the association of GSTT1 and GSTM1 genetic polymorphisms in newly diagnosed patients with ALL and normal healthy individuals. Demographic data ie, gender, age and type of ALL are depicted in Table 1. Male patients were 58.6% while female patients with ALL were 41.4%. Mean age of the patients and controls did not exhibit any statistically significance. A total of 80.5% patients had B–ALL while the rest had T–ALL.
 |
Table 1 Demographic Characteristics of the Studied Subjects |
Findings of this study show that GSTT1 gene was present in 85.2% of the normal controls and 77.3% of the patients as shown in Table 2. The genotypic frequency of GSTT1 null polymorphism was 22.7% in cases and 14.8% in controls (OR= 1.68, P = 0.111). Statistically significant differences were noted in the frequencies of GSTM1 null polymorphism in cases and controls (OR= 3.7, P = <0.001) (Table 2).
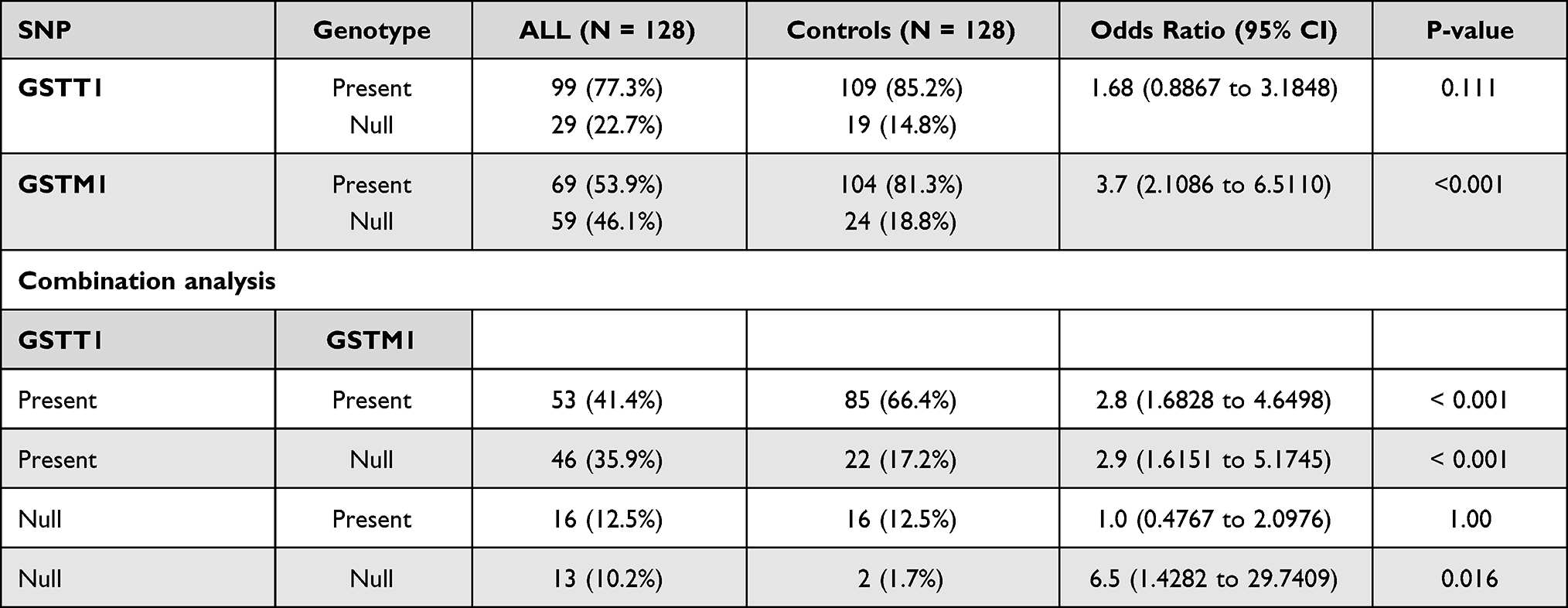 |
Table 2 Genotypes Distribution in the ALL Cases and Control Groups |
Combination analysis of GSTT1 and GSTM1 polymorphisms showed statistically significant association with ALL. In healthy controls, the frequencies of the simultaneous presence of GSTT1 and GSTM1 genes were higher as compared to patients with ALL (p<0.001) as shown in Table 2. Additionally, significant difference was observed in controls as compared to patients with ALL in the frequencies when GSTT1 gene was present and GSMT1 was absent (OR= 2.9, P <0.001). Contrary to this finding, statistically no significant difference was observed when GSTM1 gene was present and GSTT1 was absent in controls as compared to patient group. Furthermore, both GSTT1 null and GSTM1 null genes polymorphisms showed statistically significant difference in patients with ALL as compared to controls (OR= 6.5, CI 95%= 1.42–29.74, P <0.001) (Table 2).
Table 3 shows the genotypic distribution of GSTT1 and GSTM1 polymorphisms in B–ALL. GSTT1 polymorphism did not exhibit any association with B–ALL while GSTM1 null genetic polymorphism showed positive association with B–ALL as shown in Table 3. Similarly, the combination analysis showed statistically significant association of GSTT1 null and GSTM1 null polymorphisms with B–ALL as compared to controls (Table 3).
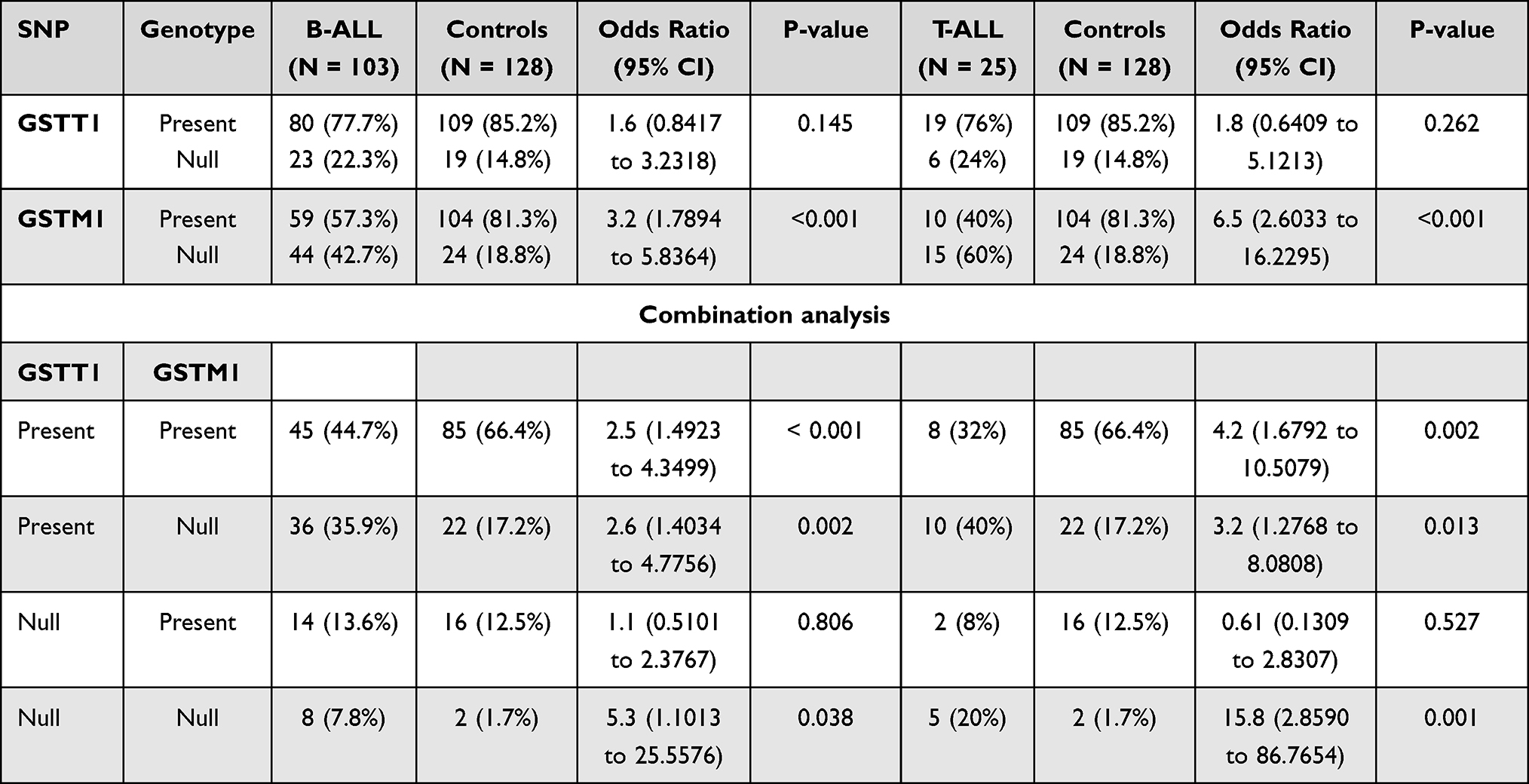 |
Table 3 Genotypes Distribution in the B–ALL/T–ALL Cases and Control Groups |
GSTM1 null polymorphism was more prevalent in patients with T–ALL as compared to normal control (60% vs 18.8% respectively) while GSTT1 did not show any difference in T–ALL and controls as shown in Table 3. Similar to B–ALL, T–ALL also showed statistically significant difference in GSTT1/GSTM1 (present), GSTT1 present/GSTM1 null polymorphism and GSTT1 null/GSTM1 null polymorphisms in controls and patient group (Table 3). However, when GSTM1 gene was present and GSTT1 was absent (GSTT1 null) no association was observed in patient group as compared to controls (OR= 0.61, CI 95%= 0.13–2.83, P=0.527). Further analysis of the results showed that there was no association between the GSTT1 and GSTM1 polymorphisms with age (less than mean Vs more than mean), gender and phenotype of ALL as shown in Table 4.
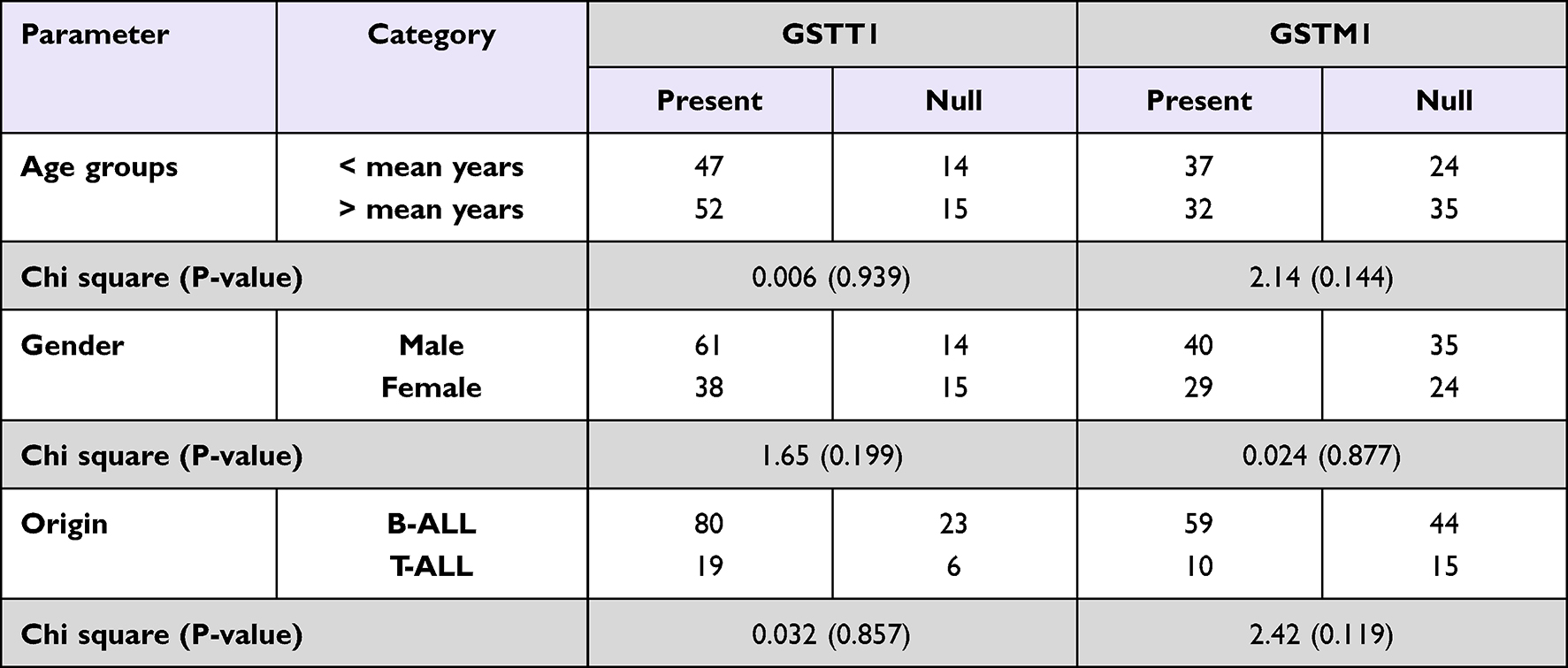 |
Table 4 Distribution of the Studied Polymorphisms Among ALL Patients According to Age Group, Gender, and Origin of Disease |
Discussion
Glutathione S-transferases are pivotal in maintaining cellular homeostasis by providing cytoprotection from environmental carcinogens, toxins, byproducts of oxidative stress and drugs. Additionally, cell signaling, post-translational modifications, cell proliferation, differentiation, cellular apoptosis, anti-inflammatory, proinflammatory, prevention of DNA damages, and resistance to chemotherapeutic drugs are other non–enzymatic function of GTs.12,32 GSTT1 and GSTM1 genetic polymorphisms are associated with loss–of–function mutations that leads to the complete loss of activities of these enzymes.16 In the present study, GSTT1 and GSTM1 genetic polymorphisms were investigated in newly diagnosed adult patients with ALL in Sudanese population. Several studies have investigated the association of GSTT1 and GSTM1 deletions in patients with acute leukemia with conflicting results. This risk has been evaluated in a limited number of studies in adult ALL patients, and largely focused on children with ALL due to a higher incidence occurring in children as compared to adults.
In this study, the most prevalent type of ALL was B –ALL (80.5% of the cases) which is similar to the reported rates.3 In the current study, although the frequency of GSTT1 null polymorphism was higher in patients as compared with controls (22.7% Vs 14.8%); this difference was statistically insignificant (p>0.05). Furthermore, no association between GSTT1 polymorphism and ALL susceptibility was found. In comparison to GSTT1 polymorphism, GSTM1 null polymorphism was highly prevalent in patients with ALL as compared to controls (46.1% vs 18.8%). It is evident that patients with GSTM1 null polymorphism were at 3.7–folds increased risk of developing ALL. Literature shows contradictory reports regarding the frequency of GSTT1 null and GSTM1 null phenotypes and its association with ALL; for a quick review please refer to Table 5. A study conducted in Pakistan on adults reports no association of either GSTM1 null polymorphism or GSTT1 gene deletion and ALL susceptibility among adult patients.33 Another study on children with ALL reported low risk for leukemia in GSTM1 null polymorphism while GSTT1 polymorphism did not exhibit any increased risk of ALL. This was presumed that these differences in the susceptibility to ALL and GSTT1 and GSTM1 null phenotypes could be attributed to ethnic differences, age, treatment and follow up duration.34
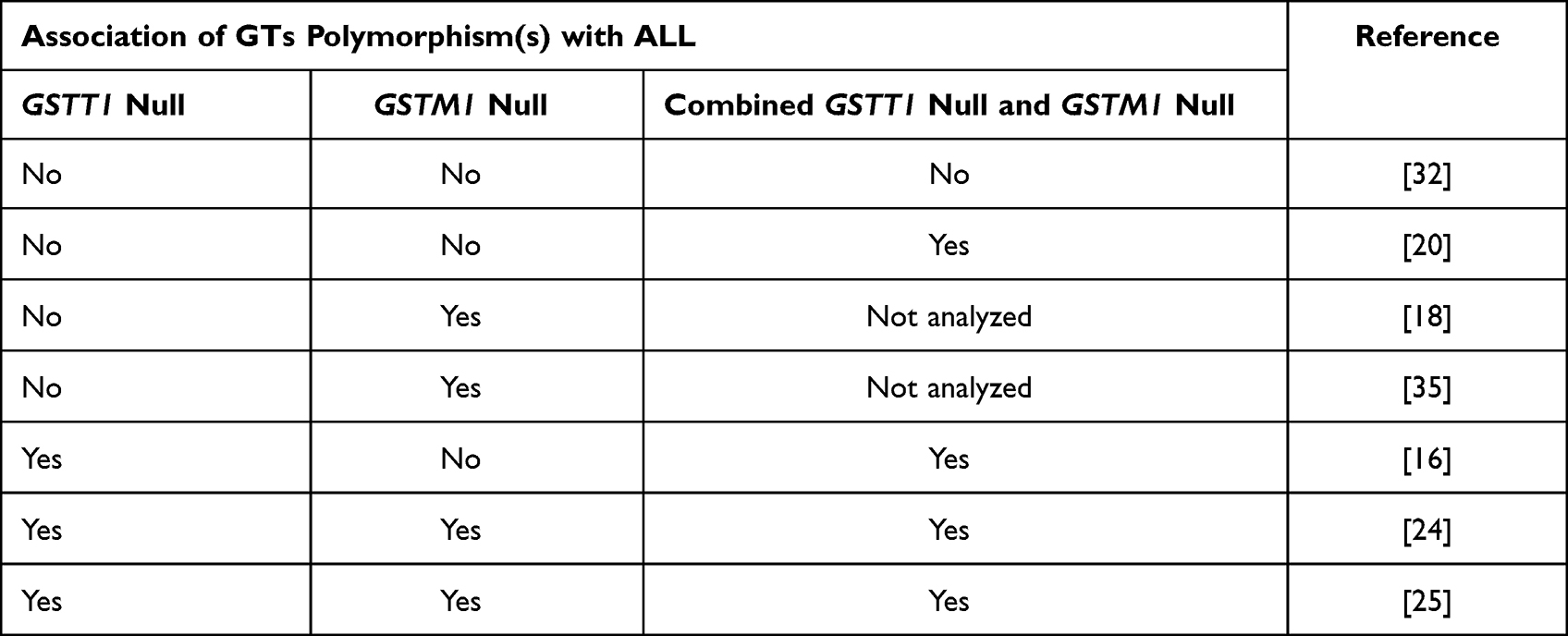 |
Table 5 Association of GSTT1 and GSTM1 Polymorphisms in Patients with ALL Reported in Different Studies |
The combined effect of GSTT1 and GSTM1 genetic polymorphisms was evaluated with a presumption that it may have significant association with the risk of ALL as compared to single genetic variant. When combination analysis was carried out it was noted that the frequencies of GSTT1 and GSTM1 genes were markedly lower in the patient group as compared to controls (OR= 2.8). This finding signifies the pathognomonic role of these genes in neoplastic disorders. It is interesting to note that when GSTM1 null polymorphisms was detected either alone or along with GSTT1 null polymorphisms, significant association was observed with ALL susceptibility. Patients with GSTT1 null and GSTM1 null polymorphisms were 6.5 times more likely to develop ALL as compared to normal individuals (Table 2). Similar findings were also noted when the prevalence of GSTT1 and GSTM1 was analyzed in the subtype of ALL ie, B – and T – cell type. GSTT1 null phenotype did not show any statistical difference in cases as compared to controls while patients with B–ALL were more prone (3.2 times) to develop ALL with GSTM1 null polymorphism. Furthermore, in B-ALL patients with combined GSTT1 null and GSTM1 null polymorphisms were 5.3 times risk of development of ALL. In T–ALL, identical findings were noted (Table 3). As the role of GTs in the detoxification process is well-established, the null polymorphisms of GSTT1 and GSTM1 could be linked with increased risk of leukemogenesis due to lack of the enzymatic activity of both these genes disposing DNA to oxidative damages. Significantly more than 3–times increased risk of ALL in patients has been reported in GSTT1 null and GSTM1 null genotypes.11,16,24 Similarly, more than 4–folds increased risk of ALL with combined GSTT1 null and GSTM1 null polymorphisms has also been reported by Baba et al.16
Additionally, association of GSTT1 and GSTM1 polymorphisms with age, gender and subtype of ALL was also assessed in the current study. Patients with more than mean age (45.05±14.1) presented no risk of ALL with GSTT1 and GSTM1 polymorphisms (p =0.939) as compared to patients with age less than the mean. Similarly, insignificant difference was also observed in relation to gender (p=0.199) and subtype of ALL (p=0.857) and GSTT1 and GSTM1 polymorphisms. These findings are similar to other reports.17,24,35 A study by Dunna et al24 also reported no association of gender with increased risk of ALL, as with age. Furthermore, another study has also reported no association of increased risk of ALL with age at diagnosis, gender, total leukocyte count, B– or T– cell type, cytogenetic abducts, or treatment outcome.22
It is a well–known fact that GTs demonstrate tissue specificity in humans, ie, GSTA are exclusively expressed in liver and kidneys, GSTM are found in brain, lymphocytes, muscles and testes, and GSTP are expressed in spleen, kidneys hepatic ducts, and placenta. It has been found that GSTM1 are found in predominantly in lymphoblasts while GSTT1 are expressed in erythroid precursors.36 This could be the possible explanation of the increased risk for the development of ALL in individuals with GSTM1 null polymorphism.
In conclusion, irrespective of age at diagnosis, gender, and phenotype of ALL; GSTM1 null polymorphism either alone or in combination with GSTT1 null polymorphism significantly increases the probability of developing ALL in adult.
Acknowledgments
The authors extend their appreciation to the Deputyship for Research & Innovation, Ministry of Education in Saudi Arabia for funding this work through the grant number “375213500”. The authors would like to extend their sincere appreciation to the central Laboratory at Jouf University for support this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Terwilliger T, Abdul-Hay M. Acute lymphoblastic leukemia: a comprehensive review and 2017 update. Blood Cancer J. 2017;7(6):e577. doi:10.1038/bcj.2017.53
2. Paul S, Kantarjian H, Jabbour EJ. Adult acute lymphoblastic leukemia. Mayo Clin Proc. 2016;91(11):1645–1666. doi:10.1016/j.mayocp.2016.09.010
3. Xu K, Feng Q, Wiemels JL, de Smith AJ. Disparities in acute lymphoblastic leukemia risk and survival across the lifespan in the United States of America. J Transl Genet Genomics. 2021;218–239. doi:10.20517/jtgg.2021.20
4. Suneetha KJ, Nancy KN, Rajalekshmy KR, Sagar TG, Rajkumar T. Role of GSTM1 (Present/Null) and GSTP1 (Ile105Val) polymorphisms in susceptibility to acute lymphoblastic leukemia among the South Indian population. Asian Pacific J Cancer Prev. 2008;9(4):733–736.
5. Idris HME, Elderdery AY, Khalil HB, Mills J. Genetic polymorphism of GSTP1, GSTM1 and GSTT1 genes and susceptibility to chronic myeloid leukaemia. Asian Pacific J Cancer Prev. 2020;21(2):499–503. doi:10.31557/APJCP.2020.21.2.499
6. Cummins I, Dixon DP, Freitag-Pohl S, Skipsey M, Edwards R. Multiple roles for plant glutathione transferases in xenobiotic detoxification. Drug Metab Rev. 2011;43(2):266–280. doi:10.3109/03602532.2011.552910
7. Board PG, Menon D. Structure, function and disease relevance of Omega-class glutathione transferases. Arch Toxicol. 2016;90(5):1049–1067. doi:10.1007/s00204-016-1691-1
8. Louie SM, Grossman EA, Crawford LA, et al. GSTP1 is a driver of triple-negative breast cancer cell metabolism and pathogenicity. Cell Chem Biol. 2016;23(5):567–578. doi:10.1016/j.chembiol.2016.03.017
9. Duvoix A, Delhalle S, Blasius R, et al. Effect of chemopreventive agents on glutathione S-transferase P1-1 gene expression mechanisms via activating protein 1 and nuclear factor kappaB inhibition. Biochem Pharmacol. 2004;68(6):1101–1111. doi:10.1016/j.bcp.2004.05.032
10. Tang ZH, Zhang C, Cheng P, et al. Glutathione-S-transferase polymorphisms (GSTM1, GSTT1 and GSTP1) and acute leukemia risk in Asians: a meta-analysis. Asian Pacific J Cancer Prev. 2014;15(5):2075–2081. doi:10.7314/APJCP.2014.15.5.2075
11. Moulik NR, Parveen F, Kumar A, Agrawal S. Glutathione-S-transferase polymorphism and acute lymphoblastic leukemia (ALL) in north Indian children: a case-control study and meta-analysis. J Hum Genet. 2014;59(9):529–535. doi:10.1038/jhg.2014.66
12. Cerliani MB, Pavicic W, Gili JA, Klein G, Saba S, Richard S. Cigarette smoking, dietary habits and genetic polymorphisms in GSTT1, GSTM1 and CYP1A1 metabolic genes: a case-control study in oncohematological diseases. World J Clin Oncol. 2016;7(5):395–405. doi:10.5306/wjco.v7.i5.395
13. Mossallam GI, Abdel Hamid TM, Samra MA. Glutathione S-transferase GSTM1 and GSTT1 polymorphisms in adult acute myeloid leukemia; its impact on toxicity and response to chemotherapy. J Egypt Natl Canc Inst. 2006;18(3):264–273.
14. Alves S, Amorim A, Ferreira F, Norton L, Prata MJ. The GSTM1 and GSTT1 genetic polymorphisms and susceptibility to acute lymphoblastic leukemia in children from north Portugal. Leukemia. 2002;16(8):1565–1567. doi:10.1038/sj.leu.2402543
15. Joseph T, Kusumakumary P, Chacko P, Abraham A, Pillai MR. Genetic polymorphism of CYP1A1, CYP2D6, GSTM1 and GSTT1 and susceptibility to acute lymphoblastic leukaemia in Indian children. Pediatr Blood Cancer. 2004;43(5):560–567. doi:10.1002/pbc.20074
16. Baba SM, Pandith AA, Shah ZA, et al. GSTT1null and rs156697 polymorphism in GSTO2 influence the risk and therapeutic outcome of B-acute lymphoblastic leukemia patients. Front Oncol. 2021;11:1–10. doi:10.3389/fonc.2021.714421
17. Bolufer P, Collado M, Barragán E, et al. The potential effect of gender in combination with common genetic polymorphisms of drug-metabolizing enzymes on the risk of developing acute leukemia. Haematologica. 2007;92(3):308–314. doi:10.3324/haematol.10752
18. Suneetha KJ, Nirmala Nancy K, Rajalekshmy KR, Rama R, Sagar TG, Rajkumar T. Role of glutathione-s-transferase and CYP1A1FNx012A polymorphisms in the therapy outcome of south Indian acute lymphoblastic leukemia patients. Indian J Med Paediatr Oncol. 2011;32(1):25–29. doi:10.4103/0971-5851.81886
19. Krajinovic M, Labuda D, Richer C, Karimi S, Sinnett D. Susceptibility to childhood acute lymphoblastic leukemia: influence of CYP1A1, CYP2D6, GSTM1, and GSTT1 genetic polymorphisms. Blood. 1999;93(5):1496–1501. doi:10.1182/blood.V93.5.1496
20. Chen HC, Hu WX, Liu QX, et al. Genetic polymorphisms of metabolic enzymes CYP1A1, CYP2D6, GSTM1 and GSTT1 and leukemia susceptibility. Eur J Cancer Prev. 2008;17(3):251–258. doi:10.1097/CEJ.0b013e3282b72093
21. Pakakasama S, Mukda E, Sasanakul W, et al. Polymorphisms of drug-metabolizing enzymes and risk of childhood acute lymphoblastic leukemia. Am J Hematol. 2005;79(3):202–205. doi:10.1002/ajh.20404
22. Davies SM, Bhatia S, Ross JA, et al. Glutathione S-transferase genotypes, genetic susceptibility, and outcome of therapy in childhood acute lymphoblastic leukemia. Blood. 2002;100(1):67–71. doi:10.1182/blood.v100.1.67
23. Haranatha RP, Kaiser J. Polymorphisms in the GST (M1 andT1) gene and their possible association with susceptibility to childhood acute lymphocytic leukemia in Indian population. African J Biotechnol. 2006;5(16):1454–1456. doi:10.4314/ajb.v5i16.43138
24. Dunna NR, Vure S, Sailaja K, et al. Deletion of GSTM1 and T1 genes as a risk factor for development of acute leukemia. Asian Pacific J Cancer Prev. 2013;14(4):2221–2224. doi:10.7314/APJCP.2013.14.4.2221
25. Rollinson S, Roddam P, Kane E, et al. Polymorphic variation within the glutathione S-transferase genes and risk of adult acute leukaemia. Carcinogenesis. 2000;21(1):43–47. doi:10.1093/carcin/21.1.43
26. Kampouraki E, Goulielmos GN, Stiakaki E. Understanding the role of genetics in childhood acute lymphoblastic leukemia (Review). World Acad Sci J. 2020;2(5):1–10. doi:10.3892/wasj.2020.54
27. Leonardi DB, Abbate M, Riccheri MC, et al. Improving risk stratification of patients with childhood acute lymphoblastic leukemia: glutathione-S-Transferases polymorphisms are associated with increased risk of relapse. Oncotarget. 2017;8(1):110–117. doi:10.18632/oncotarget.8606
28. Ye Z, Song H. Glutathione s-transferase polymorphisms (GSTM1, GSTP1 and GSTT1) and the risk of acute leukaemia: a systematic review and meta-analysis. Eur J Cancer. 2005;41(7):980–989. doi:10.1016/j.ejca.2005.01.014
29. Muddathir ARM, Abdallah EI, Khabour OF, Abdelgader RE, Elgari MM. Age- and gender-independent association of glutathione S-transferase null polymorphisms with chronic myeloid leukemia. Bosn J Basic Med Sci. 2019;19(4):350–354. doi:10.17305/bjbms.2019.4176
30. Abdalhabib EK, Jackson DE, Alzahrani B, et al. Combined GSTT1 null, GSTM1 null and XPD Lys/Lys genetic polymorphisms and their association with increased risk of chronic myeloid leukemia. Pharmgenomics Pers Med. 2021;14:1661–1667. doi:10.2147/PGPM.S342625
31. Agrawal D, Gupta S, Agarwal D, Gupta OP, Agarwal M. Role of GSTM1 and GSTT1 polymorphism: susceptibility to oral submucous fibrosis in the north Indian population. Oncology. 2011;79(3–4):181–186. doi:10.1159/000318533
32. Singh RR, Reindl KM. Glutathione S-transferases in cancer. Antioxidants. 2021;10(701):1–25. doi:10.3390/antiox10050701
33. Zehra A, Zehra S, Ismail M, Azhar A. Glutathione S-transferase M1 and T1 gene deletions and susceptibility to Acute Lymphoblastic Leukemia (All) in adults. Pakistan J Med Sci. 2018;34(3):666–670. doi:10.12669/pjms.343.14911
34. Weich N, Nuñez MC, Galimberti G, et al. Polymorphic variants of gstm1, gstt1, and gstp1 genes in childhood acute leukemias: a preliminary study in Argentina. Hematology. 2015;20(9):511–516. doi:10.1179/1607845415Y.0000000007
35. Bolufer P, Barragan E, Collado M, Cervera J, López JA, Sanz MA. Influence of genetic polymorphisms on the risk of developing leukemia and on disease progression. Leuk Res. 2006;30(12):1471–1491. doi:10.1016/j.leukres.2006.01.016
36. Wang L, Groves MJ, Hepburn MD, Bowen DT. Glutathione S-transferase enzyme expression in hematopoietic cell lines implies a differential protective role for T1 and A1 isoenzymes in erythroid and for M1 in lymphoid lineages. Haematologica. 2000;85(6):573–579.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.