Back to Journals » Clinical Interventions in Aging » Volume 17
Increased One-Year Mortality Among Elderly Patients After Radical Cystectomy for Muscle-Invasive Bladder Cancer: A Retrospective, Observational Comparative Study
Authors Lemiński A ![]() , Kaczmarek K, Gołąb A, Kotfis K
, Kaczmarek K, Gołąb A, Kotfis K ![]() , Skonieczna-Żydecka K
, Skonieczna-Żydecka K ![]() , Słojewski M
, Słojewski M
Received 9 December 2021
Accepted for publication 15 February 2022
Published 10 March 2022 Volume 2022:17 Pages 255—263
DOI https://doi.org/10.2147/CIA.S352890
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Artur Lemiński,1 Krystian Kaczmarek,1 Adam Gołąb,1 Katarzyna Kotfis,2 Karolina Skonieczna-Żydecka,3 Marcin Słojewski1
1Department of Urology and Urological Oncology, Pomeranian Medical University, Szczecin, Poland; 2Department of Anesthesiology, Intensive Therapy and Acute Intoxications, Pomeranian Medical University, Szczecin, Poland; 3Department of Biochemical Sciences, Pomeranian Medical University, Szczecin, Poland
Correspondence: Artur Lemiński, Department of Urology and Urological Oncology, Pomeranian Medical University, al. Powstańców Wielkopolskich 72, Szczecin, 70-111, Poland, Tel +48-91-466-1101, Fax +48-91-466-1100, Email [email protected] Katarzyna Kotfis, Department of Anesthesiology, Intensive Therapy and Acute Intoxications, Pomeranian Medical University, al. Powstańców Wielkopolskich 72, Szczecin, 70-111, Poland, Tel +48-91-466-1146, Fax +48-91-466-1144, Email [email protected]
Introduction: Muscle invasive bladder cancer (MIBC) is a common malignancy amongst elderly. Increasing life expectancy, prevalence of smoking, lifelong exposure to environmental pollutants and immunosenescence contribute to growing number of cases. Traditionally, radical cystectomy (RC) with pelvic lymph node dissection (PLND) constituted the mainstay of treatment for MIBC, but despite proven feasibility in elderly population, it has been associated with significant burden of morbidity, mortality, and complications.
Study Objective: We aimed to re-evaluate the safety and efficacy of RC amongst the elderly patients with MIBC.
Material and Methods: This single-center, retrospective, observational comparative study was conducted among 568 patients who underwent RC due to MIBC between 2003 and 2021. We evaluated the influence of chronological age (< 70 vs ≥ 70 years) on clinical, demographic, and pathological variables related to MIBC and RC.
Results: Elderly patients had similar clinical and pathological features of disease compared to their younger counterparts; nonetheless, they more often received simplified urinary diversion, ie ureterostomy (60.25% vs 39.33%, p< 0.001) and had no PLND (15.76% vs 8.5%, p=0.01) during RC. Furthermore, more elderly patients were treated for secondary MIBCs and fewer had history of smoking. Severe complication and 90-day mortality rates were comparable between groups; however, the elderly had significantly higher all-cause mortality at one year post RC (46.67% vs 33.25%, p=0.003). On multivariate analysis, one-year mortality risk was independently associated with elderly age (HR=2.119, 95% CI: 1.227– 3.660, p=0.007), rural residency (HR=1.760, 95% CI: 1.043– 2.968, p=0.034), extravesical extension of tumor (HR=2.109, 95% CI: 1.155– 3.850, p=0.015), lymph node metastasis (HR=2.268, 95% CI: 1.290– 3.987, p=0.004) and omission of PLND (HR=6.064, 95% CI: 2.926– 12.568, p< 0.001).
Conclusion: Radical cystectomy in elderly patients is associated with significant one-year mortality. Our study emphasizes the unmet need for considerate planning of treatment for MIBC in potentially vulnerable groups of elderly patients. Efforts are needed to reliably identify those unlikely to benefit from surgery and facilitate patient-centered choice of alternative therapies.
Keywords: urinary bladder neoplasms, cystectomy, elderly, outcomes, urinary diversion, patient-centered care
Introduction
Urothelial bladder cancer (UBC) is a prevalent malignancy in elderly population. Apart from well-established environmental risk factors like tobacco smoking and occupational exposure to carcinogens, aging of the population significantly contributes to increasing incidence of UBC.1 Incidence rates from the Surveillance, Epidemiology and End Results (SEER) database range from 70 per 100,000 for 65–69 years old, to 174 per 100,000 for octogenarians.2 Age dependence of UBC, along with latency between carcinogen exposure and development of cancer are likely driven by interactions of exposure intensity and duration, genetic susceptibility and increasingly studied phenomenon of immunosenescence.3 Majority of patients are being diagnosed in their sixth or seventh decade of life, with approximately 25% of new cases presenting with muscle-invasive bladder cancer (MIBC). Moreover, a substantial proportion of high-risk and very high-risk non-muscle invasive UBCs will eventually progress to MIBC despite conservative management.4 Correspondingly, there is an increasing population of elderly patients with MIBC that creates new challenges for personalized, multidisciplinary approach to therapy. Radical cystectomy (RC) with pelvic lymph-node dissection (PLND), preceded by neoadjuvant chemotherapy (NAC) is considered standard of surgical approach to treatment for MIBC, but despite proven feasibility in geriatric population, it remains a morbid operation, carrying significant risk of complications and early mortality.5–7 More recently, a bladder sparing combined modality treatment (CMT) has been advocated as a less invasive option for geriatric patients with MIBC however, despite similar long-term outcomes to RC, the procedure remains underutilized, and elderly patients offered substandard forms of treatment.8–10
We therefore aimed to re-evaluate the safety and efficacy of RC amongst our patients with MIBC with specific attention paid to the elderly part of the cohort. We hypothesized that the adverse events of RC will occur more frequently in older patients compared to younger ones whilst treatment efficacy would decrease with age.
Materials and Methods
Ethical Approval
This single-center, retrospective, observational comparative study was exempt from further review by the Institutional Review Board (Bioethical Committee) of the Pomeranian Medical University, Szczecin, Poland (protocol number KB-0012/136/11/2021/Z) and was conducted with respect to regulations set forth by the Declaration of Helsinki. Involved patients were routinely consented for participation in research, specifically for use of their anonymized treatment data for scientific purposes.
Study Population
We included 568 patients who underwent RC due to pathologically confirmed MIBC at the Department of Urology and Urological Oncology of the Pomeranian Medical University, Szczecin, Poland between 2003 and 2021. We evaluated the influence of patients chronological age (<70 years vs ≥70 years) on variables related to their treatment for MIBC. Clinical data included gender, urban vs rural residence, smoking status/history, RC delay, exposure to NAC. Surgical variables comprised type of surgical approach: laparoscopic vs open, number of removed lymph nodes, types of urinary diversion, incidence of severe complications and proportion of palliative cystectomies. Pathologic features of disease included local stage distribution, lymph node and surgical margin status, and were complemented with short term (90-day and 1-year) overall mortality rates. We performed two separate evaluations of early mortality: one encompassing the entire study cohort, and additional with censoring of palliative procedures. Cystectomies were considered palliative in cases of cT4b and/or M1 MIBCs. Complications were graded with Clavien-Dindo system, with grades 3 to 5 considered severe. We excluded patients who underwent partial bladder resections and those with previous pelvic radiotherapy. Due to retrospective nature of the study some of data was not available for the entire study cohort, hence some of the analyses were performed on smaller samples.
Statistical Analysis
Data was checked for internal consistency by 2 independent reviewers. Descriptive statistics included mean and standard deviation (SD) for normally distributed data. Normality of distribution and homogeneity of variance were evaluated with Shapiro–Wilk test and Levene test, respectively. Qualitative data was presented as numbers and expressed in percentages. Data was presented in two age categories ie, <70 and ≥70 years old. Single variables were compared using an independent t-test for parametric variables, and a Chi-square test for non-parametric variables. Univariate and multivariate stepwise approach Cox Proportional Hazard models were performed to assess risk factors of one-year overall mortality. Covariates in multivariate model included: age, residence status, smoking status, primary vs progressing MIBC, pathologic T-stage and pathologic N-stage. We considered the p value <0.05 statistically significant and all p values were two-sided. All tests were performed with Statistica software, version 13.5 (StatSoft, Inc., Tulsa, OK, USA).
Results
The study cohort comprised 76.24% of men and gender proportions were consistent within analyzed age subgroups. Median age within the elderly cohort was 74 years (IQR 71.5–77 years), as compared to 62 years (IQR 57–66 years) for the remaining study population, p<0.001. The majority of patients included in our study underwent an upfront RC with eventual adjuvant treatment depending on final pathologic stage (n=464). The multidisciplinary, NAC-based approach has been routinely offered to patients eligible for cisplatin since 2017 and NAC was administered before RC to 104 patients until the mid-2021. The overall uptake of NAC over the period analyzed in present study averaged 18.3% and there was no significant difference in exposure to NAC between the elderly patients and remaining study population.
Regarding risk factors of UBC, the majority of patients in our study cohort (88.52%) reported history of smoking. Within analyzed subgroups: only 5.33% of elderly patients were actively smoking at the time of treatment, 78.67% were former smokers, whereas 16% never smoked. These proportions were significantly different in a subgroup of younger patients with 30.77% of active smokers, 59.76% of former smokers and 9.47% of nonsmokers, respectively, p<0.001 (Table 1). Moreover, there was significantly higher proportion of secondary MIBCs: 40.24%, resulting from progression of non-muscle invasive UBC amongst the elderly, compared to the remaining study population: 22.95%, p=0.004. Slightly lower proportion of seniors reported rural residence: 20% vs 29.03%, p=0.027. Of note, there was no significant difference in delay of surgical treatment between both study groups (Table 1).
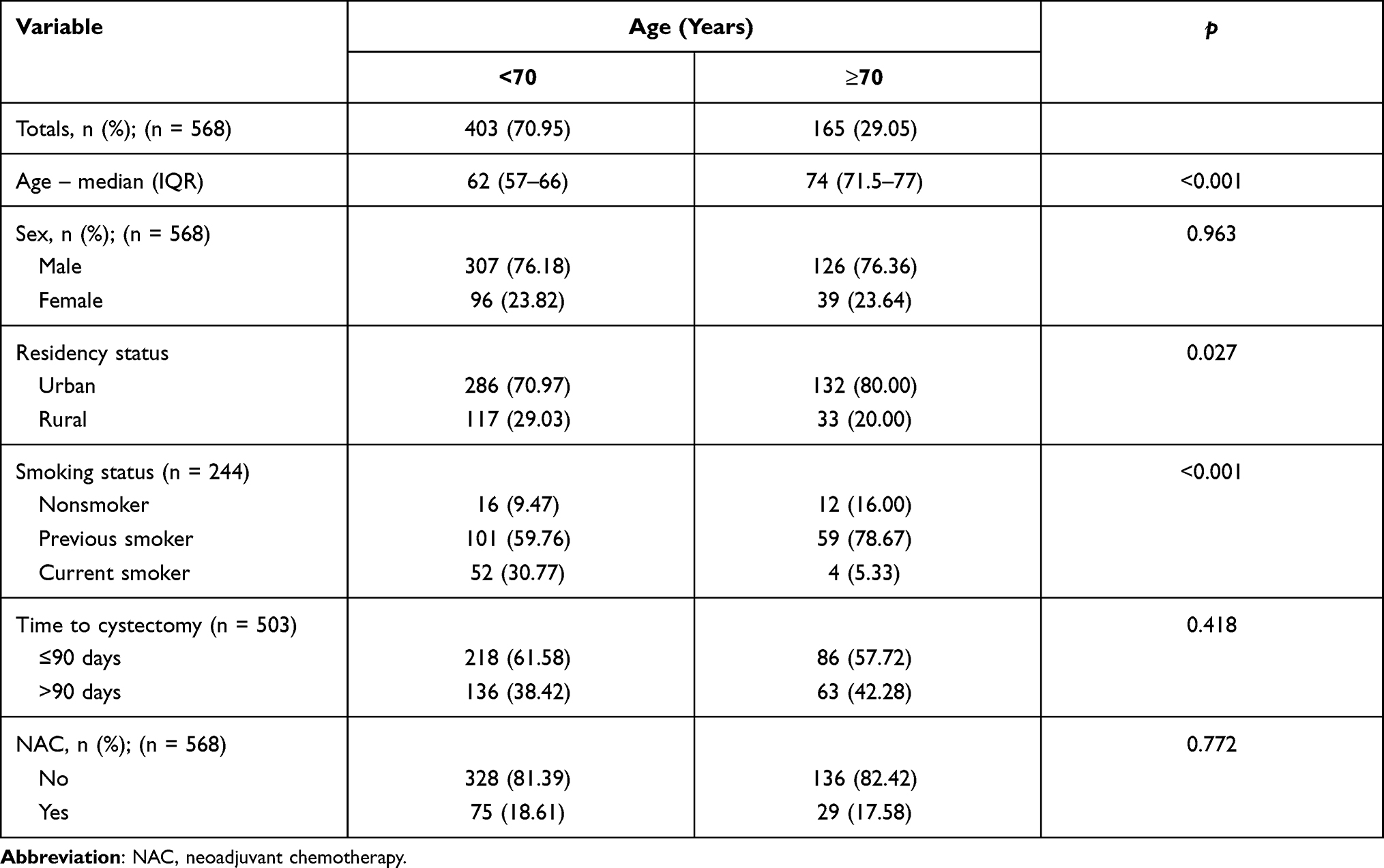 |
Table 1 Baseline Patients’ Characteristics |
Considering surgical technique of RC, there were similar proportions of palliative cystectomies in both study groups with: 6.7% and 6.06% for younger and older patients respectively, p=0.779. However, older patients were more likely to receive simplified urinary diversion with higher proportion of ureterostomies than remaining study population: 60.25% vs 39.33%. Consistently, there were significant differences in proportions of patients with ileal conduits and orthotopic neobladders: 38.51% and 1.24% versus 53.21% and 7.46% for the elderly and younger patients respectively, p<0.001 (Table 2). No PLND was performed during RC in 15.76% of the elderly patients (pNx), as opposed to 8.5% of younger patients, p=0.01, despite comparable local stage distribution, and proportion of node-negative disease in both subgroups (Table 3). The 90-day all-cause mortality rates were comparable in both groups, however there was significantly higher one-year all-cause mortality among elderly patients: 46.67% as compared to 33.25% in their younger counterparts, p=0.003 (Table 4), with corresponding HR=2.119 95% CI (1.227–3.660), p=0.007. After censoring of palliative cystectomies (10 and 27 patients from the elderly and younger groups respectively), the one-year overall mortality remained significantly higher in elderly: 43.8%, as compared to 30.85% in younger subgroup, p=0.004 (Table 5). Moreover, in multivariate analysis, older age remained an independent risk factor for increased one-year all-cause mortality, along with rural residency, higher pathologic stage, positive and unknown lymph node status (Table 6).
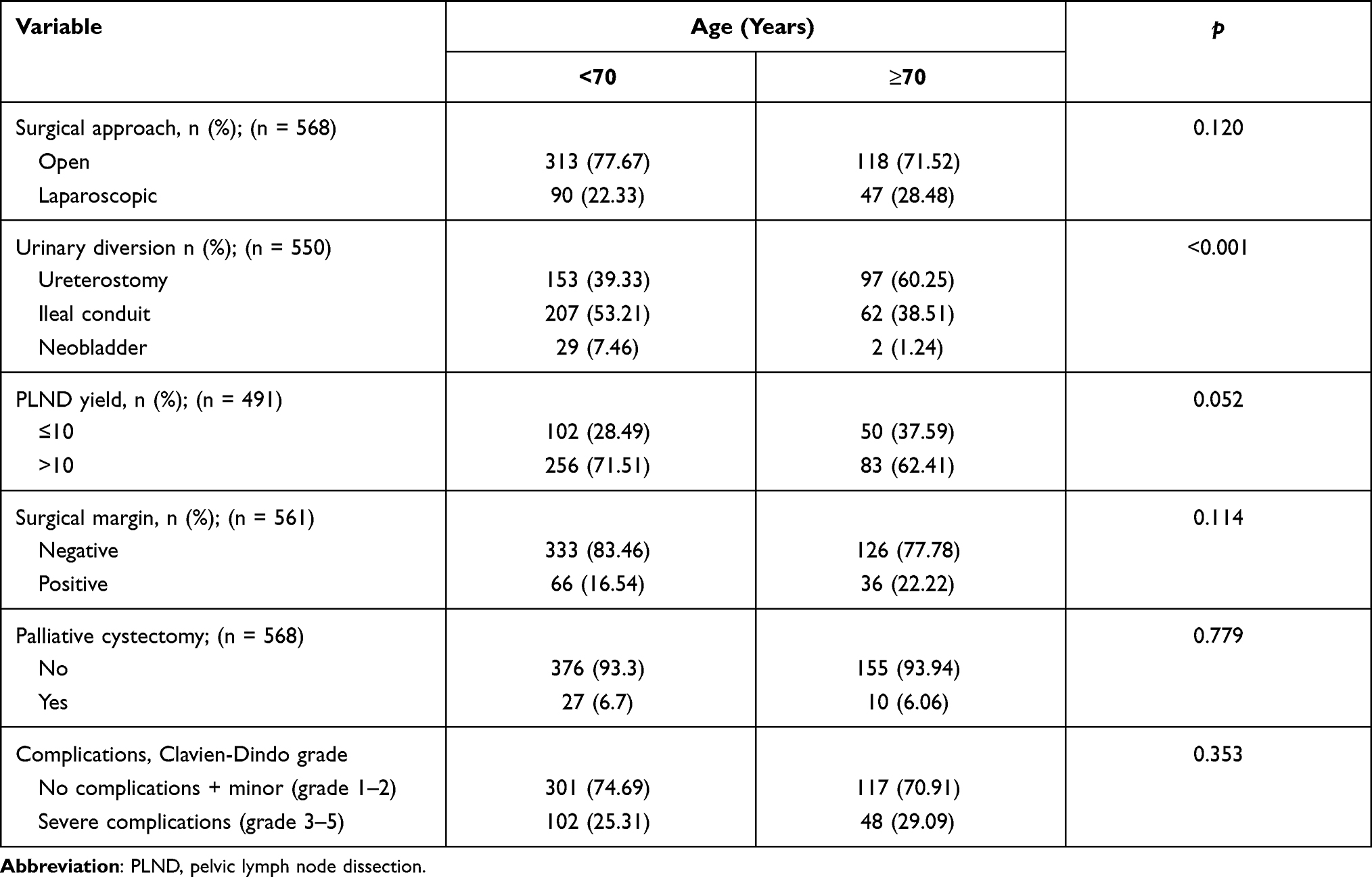 |
Table 2 Variables Related to Radical Cystectomy |
 |
Table 3 Pathologic Features of Bladder Cancer |
 |
Table 4 Short-Term Mortality Data of Entire Cohort |
 |
Table 5 Short-Term Mortality Data with Censoring of Palliative Cases |
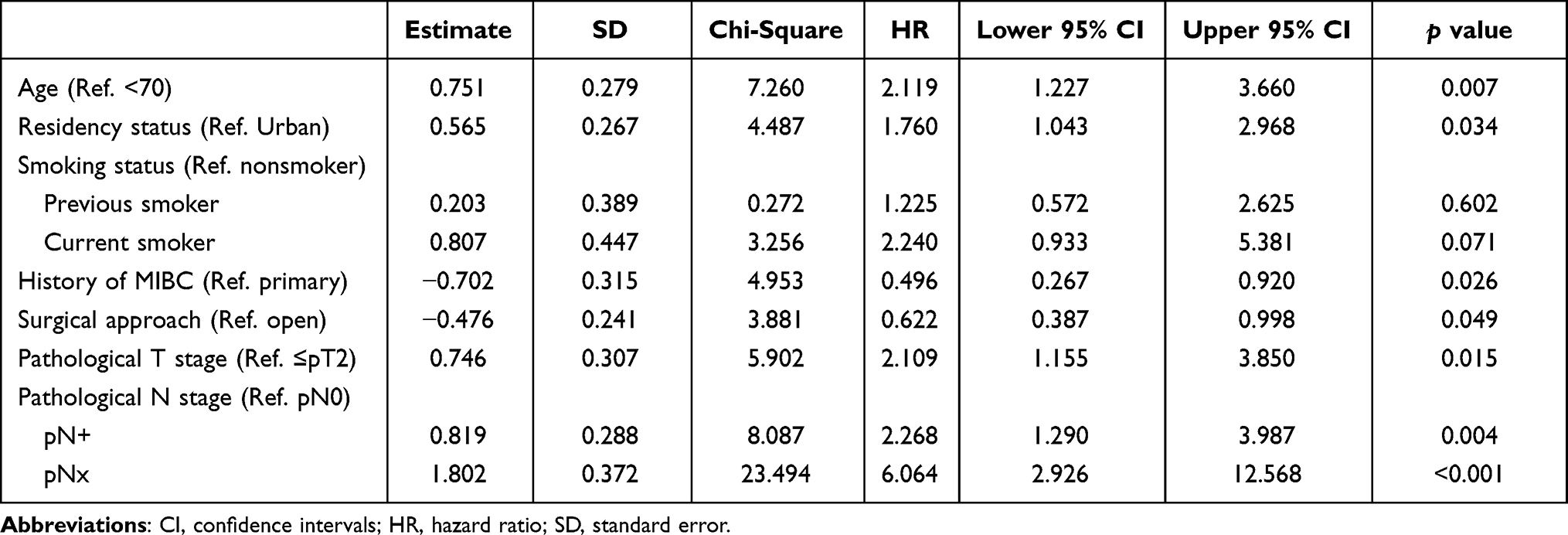 |
Table 6 Multivariate Stepwise Cox Regression Analysis of Individual Risk Factors Predicting One-Year All-Cause Mortality After Radical Cystectomy |
Discussion
Our study has shown that older age is an independent risk factor for increased one-year all-cause mortality among patients with muscle-invasive bladder cancer undergoing radical cystectomy, along with rural residency, higher pathologic stage, positive and unknown lymph node status. The early mortality rates, evaluated at 90-days, were comparable between the two subgroups. Our results emphasize the unmet need for considerate planning of treatment for MIBC in potentially vulnerable groups of elderly patients. Efforts are needed to reliably identify those unlikely to benefit from surgery and facilitate patient-centered choice of alternative therapies.
Planning treatment of MIBC in the elderly patient population has never been more complex. First of all, debate is ongoing on the very definition of an old age.11 With increasing life expectancy in developed countries and corresponding tendency for healthier lifestyle, a historical threshold of an old age established at 65 years, is becoming increasingly inadequate in prediction of patient’s physiological performance.12 At the same time, population of patients with bladder cancer includes a significant proportion of those “biologically older”, suffering from multiple comorbid conditions which stem from long-term exposure to smoking.13,14 Several authors demonstrated clinical utility of RC even in octogenarians,14–16 nevertheless we chose the age threshold of 70 years, which more adequately identifies “true elderly” patients within Polish population, still characterized by lower life expectancy compared to Western countries.17,18 Similar age threshold was adopted in a study of Görgel et al which evaluated the outcomes of RC among elderly patients in Turkey.19
Patients from the elderly group were nearly twice more often treated for secondary MIBC, resulting from progression of a non-muscle invasive disease on conservative management, than their younger counterparts. Since the majority of UBCs present as non-muscle invasive disease, patients who progress on endoscopic and intravesical treatment are likely to be older. In a systematic review and meta-analysis of Pones et al patients with secondary MIBCs were on average 13 months older than those with primary MIBCs, but had no significant difference in long-term overall survival.20 This is in contrast to several previous studies, reporting unfavorable long-term outcomes of RC in patients with secondary MIBCs, including inferior response to neoadjuvant chemotherapy.21–23
Our study found a very high proportion of patients with history of smoking, yet older patients were significantly less likely to actively smoke at the time of treatment. Given that significant part of our elderly population had secondary MIBCs, this may represent the influence of longer duration of urological care with education on harms of smoking. The diagnosis of UBC and the upcoming/ongoing treatment for cancer provide a suitable opportunity to address lifestyle modifications, as patients are more likely to get motivated and quit smoking.24 Unfortunately, as Bjurlin et al revealed in their study among over 600 American urologists, only one in five regularly discussed smoking cessation with patients with UBC, whereas 55.6% never did so.25 Therefore, urologists shall recognize their role in patient education, and specifically in patients with bladder cancer, they should guide the change towards healthier lifestyle.26 Of note, we found that 16% of elderly patients had no history of tobacco exposure, compared to 9.5% of their younger counterparts. Overall, there was 11.5% of never-smoking patients in our population, which is in keeping with data from questionnaire study from Westhoff et al, who found no tobacco exposure in 12% of their cohort of 1793 patients.27 The proportion of UBC cases attributable to occupational exposure is declining, with a review paper of Burger et al assuming 20% of UBCs being related to occupational carcinogens, whereas epidemiological studies from Westhoff et al and Rushton et al reported on much lower proportions of 5 and 7.1%, respectively.27–29 Bearing above in mind, it remains plausible that higher proportion of tobacco unrelated UBCs amongst senior patients may represent a longer latency carcinogenesis related to low intensity occupational and environmental exposure to carcinogens facilitated by immunosenescence.3 The phenomenon of immunological aging is being widely studied in many fields of medicine, including geriatric oncology in the context of disease pathogenesis and response to treatment, particularly in the era of immunotherapy with checkpoint inhibitors.30,31
Our study showed that despite comparable pathologic stage distributions of disease, elderly patients more frequently underwent simplified surgery compared to those from younger subgroup. This included omission of PLND in nearly 16% of RCs (pNx) and simplified urinary diversion in a form of ureterostomy in 60% of patients. Importantly, patients in whom PLND was not performed (pNx) had six-fold higher risk of one-year all-cause mortality than had node-negative patients, indicating that the reason for omission of PLND was unresectable nodal disease, rather than intention for reducing morbidity of RC in a potentially vulnerable subgroup of elderly patients. These findings are consistent with the study from Abdollah et al, who recognized a detrimental effect of PLND omission during RC on survival across a broad range of local stages. The authors analyzed data from SEER database, and found that omitting PLND took place in one-quarter of RCs leading to significantly increased cancer-specific mortality in organ-confined and overall mortality in locally advanced (pT3-4) UBC respectively.32 Results from our study corroborate the widely recognized tendency for elderly patients with MIBC to receive substandard forms of therapy – a tendency often associated with inferior treatment outcomes.33,34 In a national patient cohort analysis John et al evaluated treatment choices for nonmetastatic MIBC in England and found that 47% of 2519 patients diagnosed in 2016 received nonradical therapy. Radical radiation therapy and RC were offered to 29% and 24% of patients respectively. Notably, the median age of patients in this cohort reached 76 years, emphasizing the need to appropriately address the issue of curative treatment for MIBC in progressively aging population.10 Whenever RC is considered, the role of thorough patient preparation should not be underestimated. This may include preoperative pathways like “Cystocare”, which comprises medical optimization of comorbidities, gradual increase in exercise, nutritional education and psychological support within support group meetings.35 In a postoperative setting, the enhanced multidisciplinary care pathways like ERAS (Enhanced Recovery After Surgery) and NEEW (Nutrition, Exercise, Education and Wellness) were also reported to improve early outcomes.36,37 In line with previous reports, our study found that RC in the elderly population is feasible and may be accomplished without incurring an excessive risk of severe complications, compared to younger patients.19 Moreover, 90-day mortality rates observed in our study (4.47% and 7.27% for younger and older patients respectively) remain consistent with data from the literature. The study from Porter et al evaluated data from the State of Washington, and reported 90-day unadjusted mortality rates after RC of 5.4%, 6.9% and 8.4% for high, medium and low volume hospitals respectively, whereas Nielsen et al found an overall 90-day mortality rate of 7.2% in their National Cancer Database analysis.7,38
Notwithstanding, nearly half of operated seniors from our cohort died within one year from surgery. This high mortality rate signifies the unmet need for appropriate patient selection and multidisciplinary treatment planning amongst the elderly and frail patients. The planning process shall integrate evidence-based standards of care, at the same time considering individual aspects related to aging, comorbidities, reduced physiologic reserve, cognitive and self-care capabilities along with availability of support in place of residence.33,39 We found risk of one-year mortality significantly higher in patients living in rural areas, which signifies the detrimental effects of limited access to specialist medical care, nursing support and greater distance to treating hospital. These findings are in keeping with study by Deuker et al, who reported on higher overall and cancer specific mortality among rural residents with bladder cancer, compared to patients living in urban areas.40 Furthermore, rural residency was associated with increased mortality among cancer patients for most of evaluated cancer types and locations.41
Our study has several limitations which need to be acknowledged. We retrospectively analyzed data from a single academic tertiary department gathered over 17 years and looked at the correlations between chronological age and several clinical, demographic, and pathological variables, to provide some real-world evidence on how elderly patients handle the surgical treatment of MIBC. Given the 12-year difference between median ages in our study subgroups, we have not performed a typical long-term overall survival analysis, as this comparison could have been biased due to differences in life expectancy and competing mortality between these two subgroups. Instead, we decided to limit survival assessment to 90-day and one-year mortality rates, to better assess the clinical utility of bladder extirpation among the elderly. Moreover, we had no pre- and post-surgery quality-of-life data available for analysis, hence were unable to evaluate if RC meets eventual palliative objectives in this vulnerable cohort of patients. Additionally, we were lacking robust data on comorbidities or performance scores for significant part of the cohort, and we were unable to incorporate biological age into our multivariate model. For the same reason, we had to constrain some of our analyses to smaller samples thus reducing power (ie smoking status, primary versus secondary MIBC). We had limited data on smoking with either “active”, “past” or “non-smoking” status reported, without information on duration and intensity of exposure. Despite these shortcomings, we trust our study provides significant insights on value of RC among elderly patients. With advances in surgical techniques and perioperative care more of these vulnerable and frail patients would survive radical cystectomy, but as our study demonstrated, this will not translate into survival advantage in substantial proportion of them. Those unlikely to benefit from surgery shall be identified early and offered curative alternatives, likely with broader utilization of CMT.42
Conclusion
Radical cystectomy in elderly is associated with substantial burden of one-year mortality, emphasizing the need for considerate planning of treatment for muscle-invasive bladder cancer in this vulnerable group of patients. A thorough geriatric, oncological, and anesthetic evaluation of elderly patients is mandatory, and decision on radical cystectomy shall be taken within multidisciplinary team only after careful consideration of available alternatives.
Abbreviations
CMT, combined modality treatment; HR, hazard ratio; IQR, interquartile range; MIBC, muscle invasive bladder cancer; NAC, neoadjuvant chemotherapy; PLND, pelvic lymph nodes dissection; RC, radical cystectomy; SD, standard deviation; UBC, urothelial bladder cancer.
Acknowledgments
The authors would like to thank Dr Marta Wiącek, Dr Barbara Zawisza-Lemińska and prof. Andrzej Ciechanowicz for their valuable support and critical remarks on study design.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Richters A, Aben KKH, Kiemeney LA. The global burden of urinary bladder cancer: an update. World J Urol. 2020;38(8):1895–1904. doi:10.1007/s00345-019-02984-4
2. National Cancer Institute. SEER*Explorer: an interactive website for SEER cancer statistics; surveillance research program. Available from: https://seer.cancer.gov/explorer/.
3. Lian J, Yue Y, Yu W, Zhang Y. Immunosenescence: a key player in cancer development. J Hematol Oncol. 2020;13(1). doi:10.1186/s13045-020-00986-z
4. Sylvester RJ, Rodríguez O, Hernández V, et al. European Association of Urology (EAU) Prognostic Factor Risk Groups for Non–muscle-invasive Bladder Cancer (NMIBC) incorporating the WHO 2004/2016 and WHO 1973 classification systems for grade: an update from the EAU NMIBC guidelines panel[Formula present]. Eur Urol. 2021;79(4):480–488. doi:10.1016/j.eururo.2020.12.033
5. Witjes JA, Bruins HM, Cathomas R, et al. European Association of Urology guidelines on muscle-invasive and metastatic bladder cancer: summary of the 2020 guidelines. Eur Urol. 2020. doi:10.1016/j.eururo.2020.03.055
6. Krajewski W, Zdrojowy R, Tupikowski K, Małkiewicz B, Kołodziej A. How to lower postoperative complications after radical cystectomy - a review. Cent Eur J Urol. 2016;69(4):370–376. doi:10.5173/CEJU.2016.880
7. Porter MP, Gore JL, Wright JL. Hospital volume and 90-day mortality risk after radical cystectomy: a population-based cohort study. World J Urol. 2011;29(1):73–77. doi:10.1007/s00345-010-0626-3
8. Zhong J, Switchenko J, Jegadeesh NK, et al. Comparison of outcomes in patients with muscle-invasive bladder cancer treated with radical cystectomy versus bladder preservation. Am J Clin Oncol Cancer Clin Trials. 2019;42(1):36–41. doi:10.1097/COC.0000000000000471
9. Giacalone NJ, Shipley WU, Clayman RH, et al. Long-term outcomes after bladder-preserving tri-modality therapy for patients with muscle-invasive bladder cancer: an updated analysis of the Massachusetts General Hospital experience. Eur Urol. 2017;71(6):952–960. doi:10.1016/j.eururo.2016.12.020
10. John JB, Varughese MA, Cooper N, et al. Treatment allocation and survival in patients diagnosed with nonmetastatic muscle-invasive bladder cancer: an analysis of a national patient cohort in England. Eur Urol Focus. 2021;7(2):359–365. doi:10.1016/J.EUF.2020.01.013
11. Denton FT, Spencer BG. Some demographic consequences of revising the definition of “old age” to reflect future changes in life table probabilities. Can J Aging. 2002;21(3):349–356. doi:10.1017/S0714980800001677
12. Khan KT, Hemati K, Donovan AL. Geriatric physiology and the frailty syndrome. Anesthesiol Clin. 2019;37(3):453–474. doi:10.1016/j.anclin.2019.04.006
13. Garg T, Young AJ, Kost KA, et al. Burden of multiple chronic conditions among patients with urological cancer. J Urol. 2018;199(2):543–550. doi:10.1016/J.JURO.2017.08.005
14. Elsayed AS, Aldhaam NA, Brownell J, et al. Perioperative and oncological outcomes of robot-assisted radical cystectomy in octogenarians. J Geriatr Oncol. 2020;11(4):727–730. doi:10.1016/J.JGO.2019.07.010
15. Xie S, Zhao Z, Feng B, et al. A comparative study of perioperative and survival outcomes of robot-assisted radical cystectomy in patients over 80 and under 80 years old. World J Surg Oncol. 2021;19(1):1–9. doi:10.1186/S12957-021-02312-4/TABLES/4
16. Froehner M, Koch R, Hübler M, et al. Predicting 90-day and long-term mortality in octogenarians undergoing radical cystectomy. BMC Urol. 2018;18(1). doi:10.1186/S12894-018-0402-Z
17. Office for National Statistics. Living longer: is age 70 the new age 65? - Office for National Statistics. Office for National Statistics; 2019. Available from: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/ageing/articles/livinglongerisage70thenewage65/2019-11-19.
18. Karanikolos M, Adany R, McKee M. The epidemiological transition in Eastern and Western Europe: a historic natural experiment. Eur J Public Health. 2017;27(suppl_4):4–8. doi:10.1093/EURPUB/CKX158
19. Görgel SN, Şefik E, Balci U, Özer K, Girgin C, Dinçel Ç. The feasibility of radical cystectomy in elderly patients. Turk J Urol. 2014;40(1):9–14. doi:10.5152/TUD.2014.09735
20. Pones M, D’andrea D, Mori K, et al. Differential prognosis and response of denovo vs. secondary muscle‐invasive bladder cancer: an updated systematic review and meta‐analysis. Cancers. 2021;13(10):2496. doi:10.3390/CANCERS13102496
21. Vlaming M, Kiemeney LA, van der Heijden AG. Survival after radical cystectomy: progressive versus De novo muscle invasive bladder cancer. Cancer Treat Res Commun. 2020;25:100264. doi:10.1016/J.CTARC.2020.100264
22. Ge P, Wang L, Lu M, et al. Oncological outcome of primary and secondary muscle-invasive bladder cancer: a systematic review and meta-analysis. Sci Rep. 2018;8(1). doi:10.1038/S41598-018-26002-6
23. Pietzak EJ, Zabor EC, Bagrodia A, et al. Genomic differences between “primary” and “secondary” muscle-invasive bladder cancer as a basis for disparate outcomes to cisplatin-based neoadjuvant chemotherapy. Eur Urol. 2019;75(2):231–239. doi:10.1016/J.EURURO.2018.09.002
24. Bassett JC, Matulewicz RS, Kwan L, McCarthy WJ, Gore JL, Saigal CS. Prevalence and correlates of successful smoking cessation in bladder cancer survivors. Urology. 2021;153:236–243. doi:10.1016/j.urology.2020.12.033
25. Bjurlin MA, Goble SM, Hollowell CMP. Smoking cessation assistance for patients with bladder cancer: a National Survey of American Urologists. J Urol. 2010;184(5):1901–1906. doi:10.1016/J.JURO.2010.06.140
26. Sosnowski R, Przewoźniak K. The role of the urologist in smoking cessation: why is it important? Urol Oncol. 2015;33(1):30–39. doi:10.1016/J.UROLONC.2014.07.011
27. Westhoff E, Maria De Oliveira-neumayer J, Aben KK, Vrieling A, Kiemeney LA. Low awareness of risk factors among bladder cancer survivors: new evidence and a literature overview. Eur J Cancer. 2016;60:136–145. doi:10.1016/J.EJCA.2016.03.071
28. Burger M, Catto JWF, Dalbagni G, et al. Epidemiology and risk factors of urothelial bladder cancer. Eur Urol. 2013;63(2):234–241. doi:10.1016/j.eururo.2012.07.033
29. Rushton L, Bagga S, Bevan R, et al. Occupation and cancer in Britain. Br J Cancer. 2010;102(9):1428–1437. doi:10.1038/sj.bjc.6605637
30. Hong H, Wang Q, Li J, Liu H, Meng X, Zhang H. Aging, cancer and immunity. J Cancer. 2019;10(13):3021–3027. doi:10.7150/JCA.30723
31. Kotfis K, Wittebole X, Jaschinski U, et al. A worldwide perspective of sepsis epidemiology and survival according to age: observational data from the ICON audit. J Crit Care. 2019;51:122–132. doi:10.1016/J.JCRC.2019.02.015
32. Abdollah F, Gandaglia G, Thuret R, et al. Incidence, survival and mortality rates of stage-specific bladder cancer in United States: a trend analysis. Cancer Epidemiol. 2013;37(3):219–225. doi:10.1016/j.canep.2013.02.002
33. Kessler ER, Kukreja JB, Geiger CL, Fischer SM. Treating elderly patients with muscle-invasive bladder cancer. J Natl Compr Cancer Netw. 2020;18(6):783–790. doi:10.6004/jnccn.2020.7585
34. Prout GR, Wesley MN, Yancik R, Ries LAG, Havlik RJ, Edwards BK. Age and comorbidity impact surgical therapy in older bladder carcinoma patients: a population-based study. Cancer. 2005;104(8):1638–1647. doi:10.1002/cncr.21354
35. Lemiński A, Kaczmarek K, Bańcarz A, Zakrzewska A, Małkiewicz B, Słojewski M. Educational and psychological support combined with minimally invasive surgical technique reduces perioperative depression and anxiety in patients with bladder cancer undergoing radical cystectomy. Int J Environ Res Public Health. 2021;18(24):13071. doi:10.3390/ijerph182413071
36. Aldhaam NA, Elsayed AS, Hussein AA, et al. Impact of perioperative multidisciplinary rehabilitation pathway on early outcomes after robot-assisted radical cystectomy: a matched analysis. Urology. 2021;147:155–161. doi:10.1016/J.UROLOGY.2020.05.113
37. Hanna P, Zabell J, Osman Y, et al. Enhanced recovery after surgery (ERAS) following radical cystectomy: is it worth implementing for all patients? World J Urol. 2021;39(6):1927–1933. doi:10.1007/S00345-020-03435-1
38. Nielsen ME, Mallin K, Weaver MA, et al. Association of hospital volume with conditional 90-day mortality after cystectomy: an analysis of the National Cancer Data Base. BJU Int. 2014;114(1):46–55. doi:10.1111/bju.12566
39. Dybowski B. Competing risks of cystectomy – from calculator to decision. Cent Eur J Urol. 2017;70(1):128. doi:10.5173/CEJU.2016.943
40. Deuker M, Stolzenbach LF, Collà Ruvolo C, et al. Bladder cancer stage and mortality: urban vs. rural residency. Cancer Causes Control. 2021;32(2):139–145. doi:10.1007/s10552-020-01366-1
41. Hashibe M, Kirchhoff AC, Kepka D, et al. Disparities in cancer survival and incidence by metropolitan versus rural residence in Utah. Cancer Med. 2018;7(4):1490–1497. doi:10.1002/cam4.1382
42. Guancial EA, Roussel B, Bergsma DP, et al. Bladder cancer in the elderly patient: challenges and solutions. Clin Interv Aging. 2015;10:939–949. doi:10.2147/CIA.S74322
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.