Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Increased Incidence of Chronic Obstructive Pulmonary Disease in Women Due to Long-Term Passive Smoking
Authors Liu Z, Jiao M, Lv J, Han Q
Received 12 April 2025
Accepted for publication 23 July 2025
Published 7 August 2025 Volume 2025:20 Pages 2745—2752
DOI https://doi.org/10.2147/COPD.S534060
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Zhenkun Liu,* Mingzhi Jiao,* Jiling Lv, Qizheng Han
Department of Respiratory Medicine, Shandong Second Provincial General Hospital, Jinan, Shandong, 250000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiling Lv, Department of Respiratory Medicine, Shandong Second Provincial General Hospital, No. 4 Duanxing West Road, Jinan, Shandong, 250000, People’s Republic of China, Tel +8615508603200, Email [email protected] Qizheng Han, Department of Respiratory Medicine, Shandong Second Provincial General Hospital, No. 4 Duanxing West Road, Jinan, Shandong, 250000, People’s Republic of China, Tel +8615168863190, Email [email protected]
Objective: To investigate the impact of long-term passive smoking on the pathogenesis of chronic obstructive pulmonary disease (COPD) in women.
Methods: We conducted a community-based cross-sectional study involving 2,360 women aged ≥ 40 years in Jinan, China (October 1, 2022-April 30, 2023). Participants underwent comprehensive assessments including pulmonary function tests (spirometry), hematological analyses, and structured questionnaires evaluating COPD symptoms and passive smoking exposure. Based on exposure history, subjects were stratified into long-term passive smoking (LPS, n = 610) and non-passive smoking (NPS, n = 1,750) cohorts.
Results: Comparative analysis revealed significant pulmonary function impairment in the LPS group versus NPS controls: lower FEV1 (2.97± 0.61 vs 3.25± 0.37 L, p < 0.05), reduced FEV1% predicted (78.20± 10.18 vs 81.47± 14.69, p < 0.05), decreased FEV1/FVC ratio (83.32± 11.20 vs 87.23± 10.32%, p < 0.05). Small airway dysfunction was more pronounced in LPS participants, evidenced by: diminished MEF75% (77.58± 11.95 vs 86.08± 14.02 L/s, p < 0.05), reduced MEF50% (62.76± 19.79 vs 89.36± 16.78 L/s, p < 0.05), lower MMEF (80.87± 12.80 vs 87.46± 11.26 L/s, p < 0.05). The LPS group demonstrated: higher prevalence of preserved ratio impaired spirometry (PRISm, 5.74% vs 2.91%); increased annual exacerbation frequency (p < 0.05), elevated systemic inflammatory markers (p < 0.05), greater symptom severity (p < 0.05).
Conclusion: Our findings demonstrate that chronic passive smoke exposure constitutes an independent risk factor for COPD development in women, associated with higher disease prevalence, accelerated pulmonary function decline, increased exacerbation frequency and enhanced systemic inflammation.
Keywords: women, passive smoking, chronic obstructive pulmonary disease, pulmonary function, preserved ratio impaired spirometry
Introduction
Chronic obstructive pulmonary disease (COPD) is a chronic respiratory disorder characterized by persistent airflow limitation and respiratory symptoms. Although COPD is a preventable and treatable disease, it ranks as the fifth leading cause of death in China,1 remains a major contributor to global morbidity and mortality, is now one of the top three causes of death worldwide2,3 The pathogenesis of COPD is multifactorial, involving complex interactions between gene-environment.4,5 Tobacco smoking and the inhalation of toxic particles and gases from household and outdoor air pollution are the main environmental exposures leading to COPD.6,7 Among these factors, cigarette smoking is predominant, accounting for 80–90% of COPD cases in Western countries and 72% in China.8 Earlier smoking initiation, prolonged duration, higher cumulative exposure (pack-years), deeper smoke inhalation, and accelerated annual decline in forced expiratory volume in one second (FEV1) are strongly associated with increased COPD risk and mortality in smokers compared to non-smokers.9 Quit smoking is useful to improve the symptoms, respiratory function and metabolic parameters of COPD patients.10 Notably, 25–51% of COPD patients report no history of active smoking.7,11 The 2018 China Adult Tobacco Survey revealed that 68.1% of non-smokers are exposed to secondhand smoke (SHS), which contains numerous toxic and carcinogenic compounds.12 SHS exposure represents a critical public health concern, with even transient contact inducing adverse effects on respiratory, cardiovascular, immune, and endocrine systems.13,14 Epidemiological studies implicate SHS in the etiology of cardiovascular diseases,15 childhood asthma,16 and lung cancer,17,18 contributing to an estimated 1% of global mortality.19 Mechanistically, SHS shares pathophysiological pathways with active smoking, including oxidative stress and airway inflammation, thereby increasing risks of respiratory symptoms and COPD development.20,21 While direct causal evidence linking SHS to COPD incidence remains limited, a large European prospective case-control study identified SHS as a significant risk factor for COPD.18 Longitudinal investigations, including the Singapore Chinese Health Study and a 17-year Chinese cohort, demonstrate associations between SHS exposure and elevated COPD mortality.22,23 However, conflicting findings from US case-control24 and Hong Kong COPD patient studies25 highlight ongoing controversies regarding SHS-related COPD risk in non-smokers.
Sex-specific analyses reveal notable disparities: 14.1% of males with airflow obstruction are non-smokers compared to 26.8% of females.26 Over the past two decades, COPD prevalence has remained higher in females across most age groups.27,28 Emerging evidence suggests that biological vulnerabilities in never-smoking women may interact with SHS exposure to amplify COPD susceptibility.29,30 This study aims to elucidate the relationship between passive smoking and COPD risk in females, providing evidence to advocate for smoke-free public policies and reduce SHS exposure among women.
Materials and Methods
Study Population
A total of 2,360 female volunteers aged ≥40 years (mean age: 55.6 years; range: 40–86) were recruited from homogeneous communities in western Jinan between October 1, 2022, and April 30, 2023. Inclusion criteria: All subjects were free of active smoking, they were divided into long-term passive smoking group (LPS, n = 610) and non-passive smoking group (NPS, n1,750) according to whether they were exposed to long-term secondhand smoke indoors (≥0.5/d for ≥5 years). The LPS group was further categorized according to the duration of exposure: <2 0 years group; 20≤ group <30 group; ≥30 years group. Exclusion criteria: (1) active smokers; (2) unclear spousal smoking history; (3) occupational dust exposure; (4) acute respiratory infections; (5) contraindications for spirometry; (6) chronic hepatic/renal diseases, severe cardiovascular pathologies, immunologic disorders, malignancies, hematologic diseases, pregnancy/lactation, or psychocognitive impairments affecting questionnaire validity. The experiments were carry out in accordance with the Declaration of Helsinki (2013) of the World Medical Association and the protocol received ethical approval from the Institutional Review Board of Shandong Second Provincial General Hospital, with written informed consent obtained from all participants.
Study Design
Questionnaire Survey
Trained investigators administered standardized questionnaires to assess demographic characteristics (age, marital status, education level), clinical parameters (annual acute exacerbation frequency), and respiratory symptoms using the modified Medical Research Council (mMRC) dyspnea scale (range: 0–4) and the COPD Assessment Test (CAT) scale (range: 0–40).
Pulmonary Function Testing
Spirometry was performed using Jaeger Masterscreen PFSystem (CareFusion, Germany) following ATS/ERS guidelines. COPD diagnosis followed 2021 GOLD criteria.31 All pulmonary function test values are results post-bronchodilation.
Arterial Blood Gas and Complete Blood Count
Arterial blood gas: Measured using GEM 3000 analyzer (Instrumentation Laboratory, USA) under room air conditions. Complete blood count: Analyzed via Mindray BC-6800 hematology system (Shenzhen, China).
Statistical Analysis
Data analyzed with SPSS 23.0 (IBM, USA). Categorical data are summarized as frequencies and percentages. For continuous data, normally distributed variables are summarized as mean ± SD and never-normally distributed variables as median (interquartile range [IQR]). Between-group comparisons: Independent t-test (normal distribution). Mann–Whitney U-test (non-normal distribution). Statistical significance thresholds: p < 0.05.
Results
Baseline Characteristics
No significant differences were observed in age, BMI, marital status, education, or alcohol consumption between groups (Table 1).
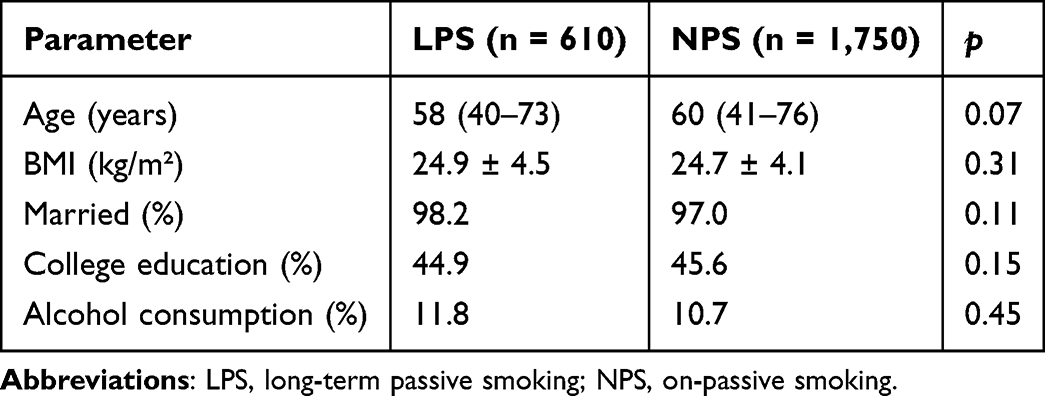 |
Table 1 Baseline Characteristics |
Laboratory and Pulmonary Function Parameters
The long-term passive smoking group showed significantly lower EFV1 (2.97+0.61 vs 3.25+0.37; p < 0.05), FEV1% predicted (78.20 ± 10.18 vs 81.47 ± 14.69; p < 0.05) and FEV1/FVCex% (83.32 ± 11.20 vs 87.23 ± 10.32; p < 0.05). Compromised small airway function parameters including MEF75% (77.58 ± 11.95 vs 86.08 ± 14.02), MEF50% (62.76 ± 19.79 vs 89.36 ± 16.78), and MMEF (80.87 ± 12.80 vs 87.46 ± 11.26) (all p< 0.05)).; alongside elevated WBC counts (9.33 ± 7.94 vs 7.31 ± 2.67; p < 0.05) and HB (137.02±23.66 vs 124.88±18.86; p < 0.05); Preserved ratio impaired spirometry (PRISm) cases was more frequent in the exposed group (p < 0.05) (Table 2).
 |
Table 2 Laboratory and Pulmonary Function Parameters (Mean ± SD) |
COPD Symptoms and Exacerbations
Compared to the NPS group, the LPS group had more severe airflow obstruction (p < 0.01) (Table 3). The COPD in LPS group reported more frequent acute exacerbations (p < 0.05), prolonged cough/sputum duration (p < 0.05), and higher mMRC (p < 0.05) and CAT scores (p < 0.05) (Table 4).
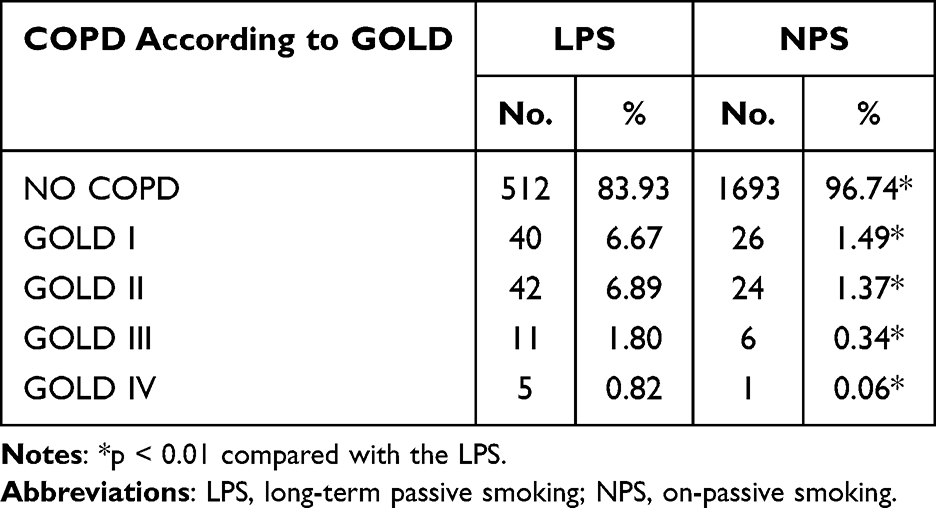 |
Table 3 COPD Grade According to GOLD |
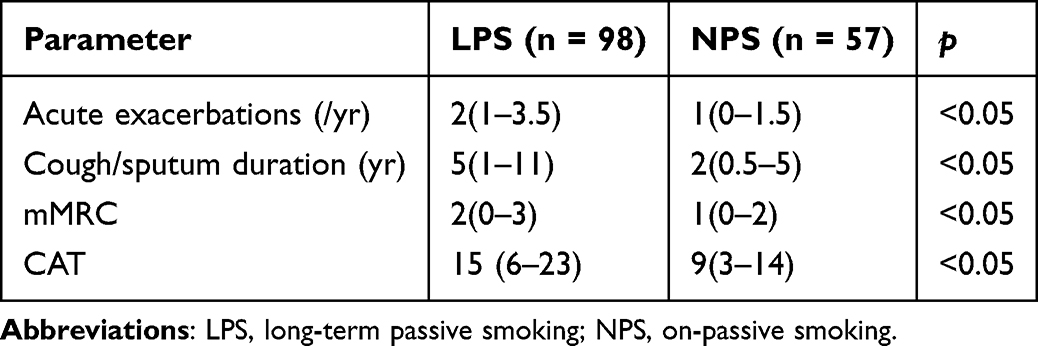 |
Table 4 COPD Symptoms and Exacerbations (Median [IQR]) |
Discussion
COPD is a globally recognized common respiratory disorder that severely threatens human health, characterized by high disability and mortality rates, imposing substantial economic and psychological burdens on both society and families. In China, the incidence, prevalence, and disease burden of COPD significantly exceed those in Western developed countries, establishing it as a critical public health concern.32 While smoking remains the single greatest risk factor for COPD, over half of COPD cases are estimated to be attributable to other causes,11 with a notably higher proportion occurring among non-smokers.26 Recent epidemiological data from China33 reveal a 13.7% prevalence of COPD among adults aged ≥40 years, with gender-specific rates of 19.0% in males and 8.1% in females. Approximately 100 million COPD patients exist nationwide, including 31.5 million females (32%). Previous studies indicate greater secondhand smoke exposure among female non-smokers,34–36 with higher COPD prevalence in non-smoking African American women compared to Caucasians, potentially linked to passive smoking.16–19 Passive smoking ≥30 minutes/day can trigger early pathological changes such as oxidative stress,37,38 so we used this as a limit for passive smoking to investigate the association between passive smoking and COPD in Chinese women.
Distinct from prior COPD-passive smoking studies,14,15 this research employs the diagnostic gold standard post-bronchodilator pulmonary function testing31 and specifically examines Chinese females. Furthermore, we eliminated confounding from active smoking by excluding current/former smokers. Spirometry, the gold standard for COPD diagnosis, quantifies airflow limitation severity. COPD was defined as post-bronchodilator FEV1/FVC <70%, with severity staged by FEV1% predicted. Airflow limitation leads to pulmonary hyperinflation, evidenced by elevated RV/TLC. Compared to non-passive smoking controls, the long-term passive smoking group demonstrated significantly reduced the FEV1, FEV1/FVC and FEV1% predicted, alongside increased RV/TLC, indicating substantial large airway damage from chronic passive smoke exposure. PRISm, an alternative designation for GOLD-Unclassified, identifies individuals with normal FEV1/FVC ratios but abnormal lung function (post-bronchodilator FEV1 <80% predicted),39 distinguishing this pattern from restrictive and nonspecific abnormalities. PRISm patients carry elevated risks for developing airflow obstruction,39,40 with female PRISm-to-COPD progression strongly predicted by passive smoking.41 Our study revealed higher PRISm prevalence in long-term passive smokers. Additionally, significant between-group differences emerged in small airway function indices, consistent with smoking-related COPD patterns of severe small airway obstruction and emphysema, validating small airway vulnerability in females. Both active and passive smoking thus induce concurrent large and small airway damage, leading to irreversible pulmonary impairment and progressive airflow obstruction, ultimately increasing COPD risk. The elevated COPD prevalence in female passive smokers aligns with previous findings.29
The mMRC scale, recommended by GOLD guidelines for dyspnea assessment,31 correlates well with COPD symptoms, health status,42 and mortality prediction.43,44 For COPD patients, the CAT can predict the health status deterioration, depression, mortality and exacerbation risk (Jones et al 2009).45,46 Our results demonstrate significantly prolonged cough/sputum duration, higher mMRC and CAT scores in passive smoking COPD patients versus controls, suggesting passive smoking exacerbates symptoms, potentially increases mortality, more severe symptoms and risk of acute exacerbation. Acute exacerbation history remains the strongest exacerbation predictor independent of GOLD staging.47 Analysis revealed significantly more prior-year exacerbations in passive smokers, indicating passive smoke exposure as a high-risk factor for acute COPD episodes in women.
Current smokers and those suffering from other environmental exposures have increased mucous cells as well as cellular hyperplasia in small and large airways.48,49 COPD patient might produce neutrophils nearly 25-fold greater than in healthy, so neutrophilic inflammation may contribute to emphysema in COPD during acute inflammatory. Analogous to smoking-related COPD’s elevated neutrophil counts,50–52 passive smoking females also exhibited significantly higher neutrophil levels. These pathological changes manifest as bronchial mucosal congestion/edema, abnormal smooth muscle contraction, airway narrowing, impaired gas exchange, and alveolar hyperinflation, collectively aggravating respiratory symptoms.7
Smoke-free laws have been adopted to protect against exposure to smoke in some public locations increasingly.53 Many studies have found protective associations between smoke-free policies and COPD-related hospitalizations, mortality and 30-day hospital readmissions.54–56 There are many studies especially for smoke-free policies in children,57 but little about women.58,59 The World Health Organization needs more research on tobacco use among women and tobacco control policies for women specific.58,60,61 Our findings further support the need for public health interventions targeted to never-smoking women, recommending implementation of smoke-free policies in both homes and the workplace.35,58
In conclusion, the present study demonstrates that long-term passive smoking significantly increases the risk and severity of COPD among women. Specifically, long-term passive smoking is associated with reduced pulmonary function, exacerbated inflammation, and increased frequency of acute exacerbations. Notably, a high prevalence of preserved ratio impaired spirometry was observed in the LPS population, suggesting early airflow limitation. This finding further supports the health benefits of legislation to reduce secondhand smoke exposure among women. However, potential biases in participant selection or unaccounted confounders may affect the interpretation of the findings and conclusions, therefore, it is recommended that more in-depth validation studies to refine evidence be conducted by expanding the sample size.
Acknowledgments
This work was supported in part by grants from the Foundation of Shandong Province Science and Technology of Traditional Chinese Medicine (M-2022191) and Institutional Project (2023MS09).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang H, Naghavi M, Allen C, et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1459–1544. doi:10.1016/s0140-6736(16)31012-1
2. Halpin DMG, Celli BR, Criner GJ, et al. The GOLD summit on chronic obstructive pulmonary disease in low- and middle-income countries. Int J Tuberc Lung Dis. 2019;23(11):1131–1141. doi:10.5588/ijtld.19.0397
3. Meghji J, Mortimer K, Agusti A, et al. Improving lung health in low-income and middle-income countries: from challenges to solutions. Lancet. 2021;397(10277):928–940. doi:10.1016/s0140-6736(21)00458-x
4. Agustí A, Melén E, DeMeo DL, Breyer-Kohansal R, Faner R. Pathogenesis of chronic obstructive pulmonary disease: understanding the contributions of gene-environment interactions across the lifespan. Lancet Respir Med. 2022;10(5):512–524. doi:10.1016/s2213-2600(21)00555-5
5. Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007;370(9589):765–773. doi:10.1016/s0140-6736(07)61380-4
6. Sin DD, Doiron D, Agusti A, et al. Air pollution and COPD: GOLD 2023 committee report. Eur Respir J. 2023;61(5):2202469. doi:10.1183/13993003.02469-2022
7. Yang IA, Jenkins CR, Salvi SS. Chronic obstructive pulmonary disease in never-smokers: risk factors, pathogenesis, and implications for prevention and treatment. Lancet Respir Med. 2022;10(5):497–511. doi:10.1016/s2213-2600(21)00506-3
8. Vozoris NT, Stanbrook MB. Smoking prevalence, behaviours, and cessation among individuals with COPD or asthma. Resp Med. 2011;105(3):477–484. doi:10.1016/j.rmed.2010.08.011
9. Kohansal R, Martinez-Camblor P, Agustí A, Buist AS, Mannino DM, Soriano JB. The natural history of chronic airflow obstruction revisited: an analysis of the Framingham offspring cohort. Am J Respir Crit Care Med. 2009;180(1):3–10. doi:10.1164/rccm.200901-0047OC
10. Pezzuto A, Ricci A, D’Ascanio M, et al. Short-term benefits of smoking cessation improve respiratory function and metabolism in smokers. Int J Chron Obstruct Pulmon Dis. 2023;18:2861–2865. doi:10.2147/copd.S423148
11. Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in non-smokers. Lancet. 2009;374(9691):733–743. doi:10.1016/s0140-6736(09)61303-9
12. Soleimani F, Dobaradaran S, De-la-Torre GE, Schmidt TC, Saeedi R. Content of toxic components of cigarette, cigarette smoke vs cigarette butts: a comprehensive systematic review. Sci Total Environ. 2022;813:152667. doi:10.1016/j.scitotenv.2021.152667
13. Flouris AD, Metsios GS, Carrillo AE, et al. Acute and short-term effects of secondhand smoke on lung function and cytokine production. Am J Respir Crit Care Med. 2009;179(11):1029–1033. doi:10.1164/rccm.200812-1920OC
14. Flouris AD, Vardavas CI, Metsios GS, Tsatsakis AM, Koutedakis Y. Biological evidence for the acute health effects of secondhand smoke exposure. Am J Physiol Lung Cell Mol Physiol. 2010;298(1):L3–l12. doi:10.1152/ajplung.00215.2009
15. Ono K, Ono H, Toi Y, et al. Association of immune-related pneumonitis with clinical benefit of anti-programmed cell death-1 monotherapy in advanced non-small cell lung cancer. Cancer Med. 2021;10(14):4796–4804. doi:10.1002/cam4.4045
16. Bjerg-Bäcklund A, Perzanowski MS, Platts-Mills T, Sandström T, Lundbäck B, Rönmark E. Asthma during the primary school ages--prevalence, remission and the impact of allergic sensitization. Allergy. 2006;61(5):549–555. doi:10.1111/j.1398-9995.2006.01027.x
17. Brennan P, Buffler PA, Reynolds P, et al. Secondhand smoke exposure in adulthood and risk of lung cancer among never smokers: a pooled analysis of two large studies. Int J Cancer. 2004;109(1):125–131. doi:10.1002/ijc.11682
18. Vineis P, Airoldi L, Veglia F, et al. Environmental tobacco smoke and risk of respiratory cancer and chronic obstructive pulmonary disease in former smokers and never smokers in the EPIC prospective study. BMJ. 2005;330(7486):277. doi:10.1136/bmj.38327.648472.82
19. Oberg M, Jaakkola MS, Woodward A, Peruga A, Prüss-Ustün A. Worldwide burden of disease from exposure to second-hand smoke: a retrospective analysis of data from 192 countries. Lancet. 2011;377(9760):139–146. doi:10.1016/s0140-6736(10)61388-8
20. Cheng SL, Lin CH, Chu KA, et al. Update on guidelines for the treatment of COPD in Taiwan using evidence and GRADE system-based recommendations. J Formos Med Assoc. 2021;120(10):1821–1844. doi:10.1016/j.jfma.2021.06.007
21. Kopa-Stojak PN, Pawliczak R. Comparison of the effects of active and passive smoking of tobacco cigarettes, electronic nicotine delivery systems and tobacco heating products on the expression and secretion of oxidative stress and inflammatory response markers. A systematic review. Inhal Toxicol. 2024;36(2):75–89. doi:10.1080/08958378.2024.2319315
22. He Y, Jiang B, Li LS, et al. Secondhand smoke exposure predicted COPD and other tobacco-related mortality in a 17-year cohort study in China. Chest. 2012;142(4):909–918. doi:10.1378/chest.11-2884
23. David GL, Koh WP, Lee HP, Yu MC, London SJ. Childhood exposure to environmental tobacco smoke and chronic respiratory symptoms in non-smoking adults: the Singapore Chinese health study. Thorax. 2005;60(12):1052–1058. doi:10.1136/thx.2005.042960
24. Behrendt CE. Mild and moderate-to-severe COPD in nonsmokers: distinct demographic profiles. Chest. 2005;128(3):1239–1244. doi:10.1378/chest.128.3.1239
25. Chan-Yeung M, Ho AS, Cheung AH, et al. Determinants of chronic obstructive pulmonary disease in Chinese patients in Hong Kong. Int J Tuberc Lung Dis. 2007;11(5):502–507.
26. Hagstad S, Ekerljung L, Lindberg A, Backman H, Rönmark E, Lundbäck B. COPD among non-smokers - report from the obstructive lung disease in Northern Sweden (OLIN) studies. Respir Med. 2012;106(7):980–988. doi:10.1016/j.rmed.2012.03.010
27. Akinbami LJ, Liu X. Chronic obstructive pulmonary disease among adults aged 18 and over in the United States, 1998-2009. NCHS Data Brief. 2011;2011(63):1–8.
28. Whittemore AS, Perlin SA, DiCiccio Y. Chronic obstructive pulmonary disease in lifelong nonsmokers: results from NHANES. Am J Public Health. 1995;85(5):702–706. doi:10.2105/ajph.85.5.702
29. Greaves LJ, Richardson LA. Tobacco use, women, gender, and chronic obstructive pulmonary disease: are the connections being adequately made? Proc Am Thorac Soc. 2007;4(8):675–679. doi:10.1513/pats.200706-079SD
30. Ntritsos G, Franek J, Belbasis L, et al. Gender-specific estimates of COPD prevalence: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2018;13:1507–1514. doi:10.2147/copd.S146390
31. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2017.
32. Chen X, Sun W, Li S, Wang X, Huang M, Ji N. Current status of prevention and treatment of respiratory diseases in primary care in China: a cross-sectional study. BMC Pulm Med. 2022;22(1):156. doi:10.1186/s12890-022-01956-6
33. Fang L, Gao P, Bao H, et al. Chronic obstructive pulmonary disease in China: a nationwide prevalence study. Lancet Respir Med. 2018;6(6):421–430. doi:10.1016/s2213-2600(18)30103-6
34. Gakidou E, Afshin A, Abajobir AA, et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1345–1422. doi:10.1016/s0140-6736(17)32366-8
35. Huque R, Siddiqi K. Smoke-free homes: the final frontier. Tob Prev Cessat. 2021;7(October):63. doi:10.18332/tpc/142772
36. Zhai C, Hu D, Yu G, et al. Global, regional, and national deaths, disability-adjusted life years, years lived with disability, and years of life lost for the global disease burden attributable to second-hand smoke, 1990-2019: a systematic analysis for the global burden of disease study. Sci Total Environ. 2023;862:160677. doi:10.1016/j.scitotenv.2022.160677
37. Mulla SA, Bedia AS, Nimmagadda HK, Bedia S, Patil AH. Evaluation of salivary alkaline phosphatase levels in passive smokers of different age groups. Cureus. 2023;15(7):e41336. doi:10.7759/cureus.41336
38. Ma C, Huang Y, Li S, et al. Trends in exposure to secondhand smoke among adolescents in china from 2013-2014 to 2019: two repeated national cross-sectional surveys. JMIR Public Health Surveill. 2023:
39. Wan ES, Castaldi PJ, Cho MH, et al. Epidemiology, genetics, and subtyping of preserved ratio impaired spirometry (PRISm) in COPDGene. Respir Res. 2014;15(1):89. doi:10.1186/s12931-014-0089-y
40. Martinez FJ, Agusti A, Celli BR, et al. Treatment trials in young patients with chronic obstructive pulmonary disease and pre-chronic obstructive pulmonary disease patients: time to move forward. Am J Respir Crit Care Med. 2022;205(3):275–287. doi:10.1164/rccm.202107-1663SO
41. Higbee DH, Granell R, Davey Smith G, Dodd JW. Prevalence, risk factors, and clinical implications of preserved ratio impaired spirometry: a UK Biobank cohort analysis. Lancet Respir Med. 2022;10(2):149–157. doi:10.1016/s2213-2600(21)00369-6
42. Bestall JC, Paul EA, Garrod R, Garnham R, Jones PW, Wedzicha JA. Usefulness of the medical research council (MRC) dyspnoea scale as a measure of disability in patients with chronic obstructive pulmonary disease. Thorax. 1999;54(7):581–586. doi:10.1136/thx.54.7.581
43. Sundh J, Janson C, Lisspers K, Ställberg B, Montgomery S. The dyspnoea, obstruction, smoking, exacerbation (DOSE) index is predictive of mortality in COPD. Prim Care Respir J. 2012;21(3):295–301. doi:10.4104/pcrj.2012.00054
44. Nishimura K, Izumi T, Tsukino M, Oga T. Dyspnea is a better predictor of 5-year survival than airway obstruction in patients with COPD. Chest. 2002;121(5):1434–1440. doi:10.1378/chest.121.5.1434
45. Jones PW, Harding G, Berry P, Wiklund I, Chen WH, Kline Leidy N. Development and first validation of the COPD assessment test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
46. Karloh M, Fleig Mayer A, Maurici R, Pizzichini MMM, Jones PW, Pizzichini E. The COPD assessment test: what do we know so far?: a systematic review and meta-analysis about clinical outcomes prediction and classification of patients into GOLD stages. Chest. 2016;149(2):413–425. doi:10.1378/chest.15-1752
47. Magda S. Susceptibility to exacerbation in chronic obstructive pulmonary disease - Data from the ECLIPSE study. Maedica. 2010;5(3):223–224.
48. Mullen JB, Wright JL, Wiggs BR, Paré PD, Hogg JC. Structure of central airways in current smokers and ex-smokers with and without mucus hypersecretion: relationship to lung function. Thorax. 1987;42(11):843–848. doi:10.1136/thx.42.11.843
49. Wright JL, Ngai T, Churg A. Effect of long-term exposure to cigarette smoke on the small airways of the Guinea pig. Exp Lung Res. 1992;18(1):105–114. doi:10.3109/01902149209020654
50. Güldaval F, Polat G, Doruk S, et al. What are the differences between smoker and non-smoker COPD cases? Is it a different phenotype? Turk Thorac J. 2021;22(4):284–288. doi:10.5152/TurkThoracJ.2021.20147
51. Ramírez-Venegas A, Montiel-Lopez F, Falfan-Valencia R, Pérez-Rubio G, Sansores RH. The “slow horse racing effect” on lung function in adult life in chronic obstructive pulmonary disease associated to biomass exposure. Front Med Lausanne. 2021;8:700836. doi:10.3389/fmed.2021.700836
52. Salvi SS, Brashier BB, Londhe J, et al. Phenotypic comparison between smoking and non-smoking chronic obstructive pulmonary disease. Respir Res. 2020;21(1):50. doi:10.1186/s12931-020-1310-9
53. Hyland A, Barnoya J, Corral JE. Smoke-free air policies: past, present and future. Tob Control. 2012;21(2):154–161. doi:10.1136/tobaccocontrol-2011-050389
54. Stallings-Smith S, Zeka A, Goodman P, Kabir Z, Clancy L. Reductions in cardiovascular, cerebrovascular, and respiratory mortality following the national Irish smoking ban: interrupted time-series analysis. PLoS One. 2013;8(4):e62063. doi:10.1371/journal.pone.0062063
55. Kent BD, Sulaiman I, Nicholson TT, Lane SJ, Moloney ED. Acute pulmonary admissions following implementation of a national workplace smoking ban. Chest. 2012;142(3):673–679. doi:10.1378/chest.11-2757
56. Dusemund F, Baty F, Brutsche MH. Significant reduction of AECOPD hospitalisations after implementation of a public smoking ban in Graubünden, Switzerland. Tob Control. 2015;24(4):404–407. doi:10.1136/tobaccocontrol-2013-051290
57. Radó MK, Mölenberg FJ, Sheikh A, et al. Impact of expanding smoke-free policies beyond enclosed public places and workplaces on children’s tobacco smoke exposure and respiratory health: protocol for a systematic review and meta-analysis. BMJ Open. 2020;10(10):e038234. doi:10.1136/bmjopen-2020-038234
58. Fallin-Bennett A, Parker KA, Miller A, Ashford K, Hahn EJ. Smoking and tobacco-free policies in women’s residential substance use disorder treatment facilities: a community-engaged approach. Nicotine Tob Res. 2018;20(11):1386–1392. doi:10.1093/ntr/ntx211
59. Greaves LJ, Hemsing NJ. Sex, gender, and secondhand smoke policies: implications for disadvantaged women. Am J Prev Med. 2009;37(2 Suppl):S131–7. doi:10.1016/j.amepre.2009.05.012
60. World Health Organization. WHO Framework Convention on Tobacco Control. Geneva, Switzerland: World Health Organization; 2005.
61. World Health Organization. Gender, Women and the Tobacco Epidemic; 2010.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.