Back to Journals » Journal of Pain Research » Volume 12
Increased frequency of urine drug testing in chronic opioid therapy: rationale for strategies for enhancing patient adherence and safety
Authors DiBenedetto DJ ![]() , Wawrzyniak KM
, Wawrzyniak KM ![]() , Schatman ME
, Schatman ME ![]() , Shapiro H
, Shapiro H ![]() , Kulich RJ
, Kulich RJ ![]()
Received 26 April 2019
Accepted for publication 23 June 2019
Published 23 July 2019 Volume 2019:12 Pages 2239—2246
DOI https://doi.org/10.2147/JPR.S213536
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
David J DiBenedetto1,2, Kelly M Wawrzyniak1,2, Michael E Schatman1,3, Hannah Shapiro1,4, Ronald J Kulich2,5
1Research and Network Development, Boston PainCare, Waltham, MA, USA; 2Department of Diagnostic Sciences, Tufts School of Dental Medicine, Boston, MA, USA; 3Deparment of Public Health and Community Medicine, Tufts School of Medicine, Boston, MA, USA; 4Department of Biopsychology, Tufts University, Medford, MA, USA; 5Department of Anesthesia Critical Care and Pain Medicine, Harvard Medical School, Massachusetts General Hospital, Boston, MA, USA
Objective: To determine the average amount of time required to detect opioid aberrancy based upon varying frequencies of urine drug testing (UDT) in a community-based, tertiary care pain management center.
Subjects: This study was a retrospective analysis of 513 consecutive patients enrolled in a medication management program, receiving chronic opioid therapy between January 1, 2018 and December 31, 2018.
Methods: Data were extracted from medical records including age at start of the study period, sex, ethnicity, marital status, and smoking status. UDT was performed at each prescribing visit via semi-quantitative immunoassay, and at the discretion of the clinician, a sample was sent for external confirmation using gas chromatography or mass spectrometry testing to clarify questions of inconsistency with patients’ reports or prescribed medications. For purposes of the study, “opioid aberrancy” was defined through inconsistent UDT.
Results: One hundred and fifteen patients (22.4%) had at least one inconsistent UDT during the study period, and 160 (2.8%) of all UDTs were inconsistent. At this rate of inconsistency, it was determined that with monthly screening, it would require up to 36 months to detect a single aberrancy, and semi-annual testing would require as long as 216 months to detect an aberrancy.
Conclusions: More frequent UDT can be helpful in terms of earlier detection of opioid aberrancy. This has significant implications for helping avoid misuse, overdose, and potential diversion. Furthermore, early detection will ideally result in earlier implementation of treatment of the emotional and behavioral factors causing aberrancy. Such early intervention is more likely to be successful in terms of reducing substance misuse in a chronic pain population, providing a higher degree of patient adherence and safety, as well as producing superior overall patient outcomes. Finally, economic benefits may include substantial savings through avoidance of the necessity for drug rehabilitation and the empirically established higher costs of treating opioid misuse comorbidities.
Keywords: urine drug testing, frequency, opioid safety, economic benefits
Introduction
The use of “universal precautions” in opioid prescribing has been recommended since 2005,1 with urine drug toxicology (UDT) considered a crucial aspect of cautious risk mitigation. Although not necessarily a panacea, UDT has been demonstrated through a number of studies and reviews2–5 to have at least moderate efficacy for increasing prescription safety. The 2016 Centers for Disease Control and Prevention (CDC) Opioid Prescribing Guideline6 recommends UDT not only at the initiation of treatment with opioids, but periodically during the course of treatment as a means of increasing patient safety.
Despite numerous recommendations for UDT use in pain medicine, there is no consensus regarding the ideal frequency of testing, with considerable variance in these recommendations. Individual studies of the efficacy of UDT in reducing aberrancy and increasing adherence have been published, suggesting that repeated testing results in improvements in these areas. Results of a 2011 retrospective, longitudinal study7 demonstrated that the incidence of illicit drug use among pain patients decreased as continued UDT was performed, although subject attrition due to being discharged from practices secondary to detected aberrancy may have been a confounding variable. A large retrospective analysis of 3 years of data collected from 2008 to 20118 identified an increase in opioid adherence in all opioids studied with more frequent testing. A 2014 investigation of cancer patients on opioids9 determined that those patients with “inconsistent” UDTs were more likely to have had a large number of prior visits in which UDT was not performed. A more recent retrospective study10 demonstrated improved pain patient adherence with repeated quantitative UDT. The results of this investigation10, as in the study previously mentioned,7 may be suspect due to attrition caused by the study site’s policy of “zero tolerance”, with patient treatment discontinued when illicit drugs were found in their systems. Furthermore, the authors did not report the frequency of testing in the study, although stated that “compliant patients” are routinely tested 2–4 times/year.
Regarding guidelines, the 2016 CDC Guideline6 recommends UDT “at least annually”. This may be insufficient, however. A 2012 UDT guideline11 recommends individualized risk assessment and performance of UDT based on low (1–2/year), moderate (3–4/year), or high (4/year “or every month, office visit, or every drug refill”). However, the utility of such a recommendation becomes questionable given the lack of consensus regarding strategies for stratifying risk. A recent American Academy of Pain Medicine consensus guideline12 is somewhat more conservative. It recommends stratifying patients into three groups based on risk, in addition to testing “at least annually for low-risk patients, two or more times per year for moderate-risk patients, and three or more times per year for high-risk patients”. To its credit, this guideline recommends utilization of a number of validated psychometric risk tools in order to more accurately stratify patient risk classification.
Although the above investigations are suggestive of benefits of more frequent UDT within the context of considering or actively managing the patient on chronic opioid therapy (COT), there is a paucity of recent, high-quality literature examining the utility of testing more frequently as opposed to less often. This lack of recent literature perhaps relates to dramatic changes in attitudes toward opioid analgesia for chronic pain over the past several years. Furthermore, the financial burden associated with frequency of testing largely remains largely unaddressed, and its importance cannot be overstated at this time in which “behavioral economics” in medicine are under greater scrutiny than in the past.13 Thus, the purpose of the current study was to gain insight into the broad implications of more frequent compared to less frequent UDT in regard to uncovering aberrant behavior associated with COT, utilizing data reflective of the current opioid zeitgeist as opposed to that of the period in which previous studies were conducted. Additionally, the complexities of the relationship between frequency of UDT and potential overall cost-savings will be discussed.
Methods
With confirmation from the Tufts University Institutional Review Board that this retrospective chart review study does not constitute human subjects research, data were extracted from the electronic health record for patients receiving COT between January 1, 2018 and December 31, 2018, inclusive. These data were deidentified, and thus met the confidentiality standards set forth by the Declaration of Helsinki. Data were excluded from analyses if patients were not enrolled in the opioid prescribing program at the pain center (eg, UDT as part of opioid risk assessment but never received opioids, or received one short prescription post-interventional procedure).
Study population
Patients at this community-based, tertiary care, patient-centered specialty practice for chronic painful conditions (musculoskeletal, spine, multifocal, fibromyalgia and other diffuse pain complaints, headache and facial pain, etc.) are treated through an interdisciplinary approach to care with a focus on functional outcomes. There are a number of specialists at the pain center, including interventional pain medicine physicians, nurse practitioners, psychologists and social workers, a neurologist, a sleep medicine physician, physical rehabilitation specialists, a laboratory director and technician, and a pharmacist. The pain center has a structured COT program that requires a thorough interdisciplinary opioid risk assessment prior to enrollment. This includes clinical interviews with behavioral medicine clinicians, a nurse practitioner, and the physical rehabilitation physician, a UDT, review of the prescription monitoring program report, review of medical records, and a number of self-report questionnaires (Screener and Opioid Assessment for Patients with Pain-Revised, Current Opioid Misuse Measure (COMM), Patient Health Questionnaire-9 item for depression, Roland Morris Disability Questionnaire modified from “back pain” to “pain”, World Health Organization Disability Assessment Schedule 2.0). All evaluation information is reviewed in a weekly interdisciplinary team meeting including a pain physician, behavioral medicine practitioners, nurse practitioners, a physical rehabilitation physician, the laboratory director, and the pharmacist to determine appropriateness for enrollment into the COT program, risk for aberrant drug behavior, and plan of care. There are currently approximately 500 patients maintained on COT, and a UDT is performed at the time of each prescribing visit while enrolled in the program. Those determined to have a low level of risk and on a stable regimen are followed monthly for prescribing visits (and monthly UDT), while those with a moderate level of risk for opioid misuse are followed bi-weekly for prescribing visits and are typically also required to meet with a behavioral medicine provider bi-weekly to address risk factors, adherence, etc. Those with the highest level of risk and/or multiple concerning aberrancies undergo weekly prescribing and behavioral medicine visits with UDT to monitor safety, address behavioral and psychosocial factors contributing to risk, and to evaluate for a substance use disorder. Any changes to a patient’s plan of care, frequency of monitoring, or discharge from COT are discussed in the team meeting prior to implementation.
Data collection
All data were collected as part of routine clinical care and extracted from the electronic health record. Demographic data included age at start of the study period, sex, ethnicity, and marital status.
Opioid dose in milligrams morphine equivalent (MME) was captured at each prescribing visit, and was calculated based upon the prescribed opioid medications using the conversions described by the Washington State Agency Medical Directors’ Group.14 Mean MME at start of the study period for all subjects was used to describe the sample.
The COMM was administered at the initial opioid risk assessment and approximately every 4 months at a prescribing visit as part of routine care and ongoing risk evaluation.15,16 Mean COMM at start of the study period for all subjects was used to describe the sample and to compare rates of aberrancy between those patients with COMM scores <9 indicating low risk for opioid misuse, and those ≥9 indicating high risk for opioid misuse. The cutoff score of 9 was used in accordance with that used in the original validation study.15
UDT was performed via semi-quantitative immunoassay (see Table 1 for UDT cutoff concentration levels) and, at the discretion of the clinician, a sample was sent for external confirmation testing using gas chromatography/mass spectrometry (GC/MS) testing to clarify any discrepancies in the semi-quantitative immunoassay results. UDT results were entered into the medical record as “consistent” or “inconsistent” and these data were extracted from the medical record for analysis. A “consistent” UDT result was defined as having a urine sample with the presence of all prescribed medications reported by patients to have been taken within the past 48 hrs as prescribed, and the absence of all illicit substances tested. An “inconsistent” UDT result was defined as any of the following: 1) the sample contained a non-prescribed controlled substance or illicit substance and/or its metabolite, 2) the absence of an opioid prescribed for daily use or its metabolite, or 3) an adulterated sample such as urine with a temperature out of range of human body temperature. In cases in which there were GC/MS results for the same encounter date as semi-quantitative immunoassay results, the GC/MS results were used in the data set.
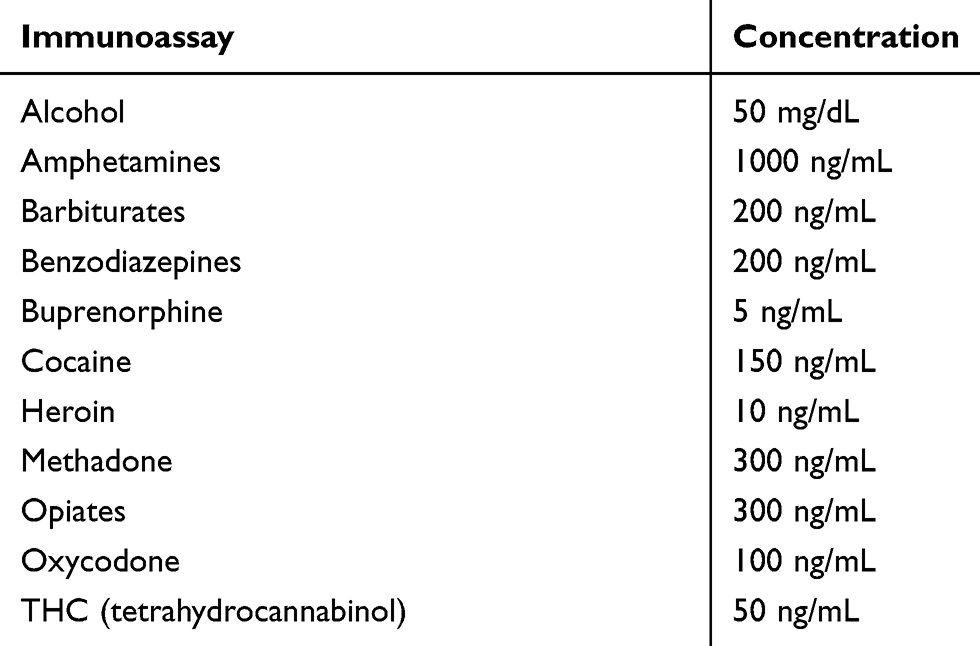 |
Table 1 Urine drug toxicology immunoassay cutoff concentrations |
Statistical analysis
Descriptive statistics (means, standard deviations, counts, percentages) were used to describe the sample in terms of demographics, initial MME, initial COMM score, and rate of inconsistent UDT. A Z-test of two proportions with α=0.05 was used to compare the proportion of patients with one or more inconsistent UDT during the study period between those with an initial COMM score of <9 and those ≥9.
Results
Data from 513 patients were included in the study. Table 2 presents the demographic and clinical information of the sample. A total of 5772 UDTs were included in the analysis, with 69 of these involving external GC/MS results in place of internal immunoassay results. Across all patients, UDTs were obtained at a frequency of 0.89 months (ie, slightly more frequent than monthly).
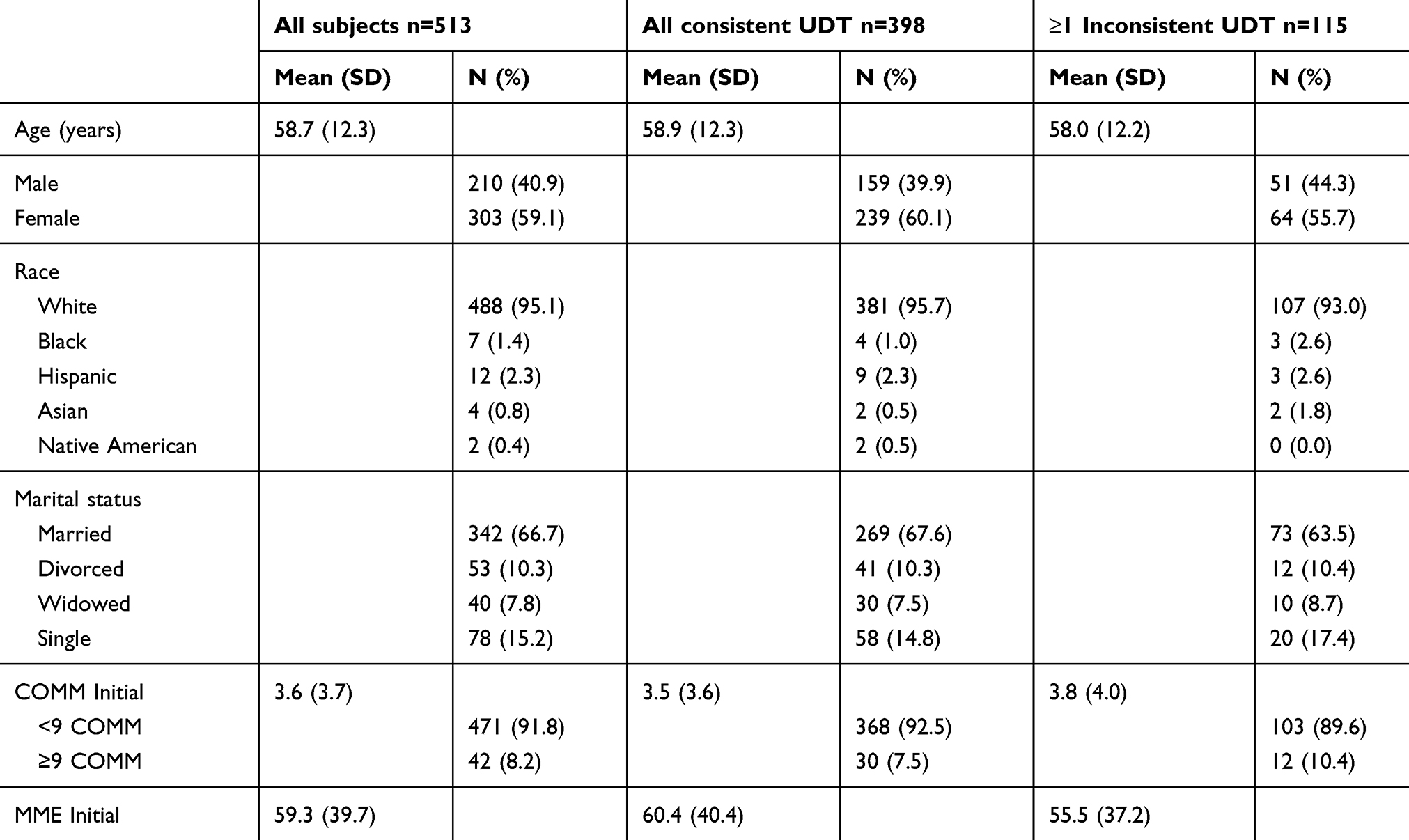 |
Table 2 Demographics and clinical characteristics |
One hundred and fifteen patients (22.4%) had at least one inconsistent UDT during the 12-month study period. Table 2 presents demographic and clinical information for the subgroup of the sample with at least one inconsistent UDT and the subgroup with entirely consistent UDT during the study period. One hundred and sixty (2.8%) of the total 5772 UDT obtained during the study period were inconsistent. Four hundred and seventy-one patients (91.8%) had an initial COMM score <9, and 103 in this group (21.9%) had at least one inconsistent UDT during the study period. Forty-two patients (8.2%) had an initial COMM score ≥9 and 12 in this group (28.6%) had at least one inconsistent UDT during the study period. This difference in proportion of patients with aberrancy was not significantly different (p=0.84).
Readers interested in the raw data from this study can access the full data set (please put link here).
Discussion
The results of this study indicate a low rate of inconsistent UDT over the course of a calendar year for 513 patients on COT who were tested at least monthly while prescribed COT. Furthermore, the UDT inconsistency rates that were detected in our data were low compared to those extant in the literature. For example, a 2015 systematic review and data synthesis17 reported rates of opioid misuse as measured solely by UDT ranging from approximately 3% to 75%. The rate of aberrancy reported in the current study is also lower than the 9.1% rate of aberrancy previously reported in a population of patients receiving COT at our center in 2014.18 It should be noted, however, that these studies predated the implementation of the 2016 CDC Guideline, and the subsequent change in the zeitgeist of opioid prescribing and risk mitigation makes comparison of results dubious.
The time to discovery of an aberrancy is dependent upon the rate of inconsistent UDT, with the identification of aberrancy occurring sooner in practice environments experiencing higher rates of UDT inconsistency. Using the obtained 2.8% rate of inconsistent UDT, monthly screening would take as long as 36 months to identify an aberrancy, while quarterly or semi-annual screening could take decades to identify one. It should be noted that the time to discovery for aberrant behavior may vary widely within subgroups of our study population given the heterogeneous nature of our sample with regards to their risk for engaging in aberrant behavior. While it may be interesting to extrapolate our data to the rates of aberrancy previously reported, a thorough review of the literature indicates that no studies examining the frequency of UDT aberrancy have been published in at least 5 years. As such, any extrapolation would be arbitrary (given the dramatic change in the opioid zeitgeist over the past several years), and accordingly would likely be meaningless. Furthermore, even if the rate of aberrancy experienced in the majority of practice settings in which COT is prescribed is lower than rates previously published, the implications of any one opioid aberrancy could have costly consequences including diversion, overdose, or death, and therefore may justify the use of more frequent UDT.
Many of the guidelines and previously published studies recommend that patients who are at low risk be tested less frequently, while moderate to high-risk patients be tested more frequently. However, opioid risk evaluations may not be a reliable predictor of opioid aberrancy, as they commonly rely on data derived from medical record reviews and risk assessment tools that are both heavily dependent upon subjective patient self-report. In such evaluations, only UDT results, information derived from prescription drug monitoring programs, or documented incidents of overdose provide objective data. The use of UDT data is critical to this assessment process, particularly given the evidence indicating extremely weak correlations between patient self-report, provider reports (as assessed by the Aberrant Behavior Checklist), and objective UDT results.19 Empirically, UDT-identified aberrancy in the chronic pain population has been linked to prior and/or current substance abuse20,21 as well as potential diversion.22 The frequency of UDT also has predictive value, as patients prescribed opioids at Veterans Administration (VA) hospitals in which UDT was performed more frequently were found to be less likely to attempt suicide than those prescribed opioids at VA hospitals ordering less frequent UDT.23 A more recent VA study24 determined that more frequent UDT not only predicted fewer suicide attempts but also fewer overdose-related events. Such predictive value of UDT becomes even more important given recently articulated concerns that psychometric tools for assessing aberrancy may have strong sensitivity and specificity without adequate predictive value.25
Almost a decade ago, McCarberg noted that aberrant drug-related behaviors “are poorly defined and represent a continuum ranging from least to most aberrant”.26 As such, the transition from appropriate utilization of opioid analgesics to misuse/abuse is quite difficult to track, and prescribers generally have difficulty identifying the point at which patients cross this threshold.27 While many advocate for the utilization of opioid risk screening tools among patients at risk for aberrant behavior, these tools lack validity scales to ensure (or at least predict) the veracity of the responses. Furthermore, the intended purposes of these instruments are fairly transparent, and higher risk patients responding in a manner suggesting lower-than-actual risk has been documented.28 Although early studies of the COMM15,16,29 substantiated the validity of the measure through significant relationships with UDT results, both the current study and another 2019 investigation30 of HIV-positive patients taking opioids did not find a significant relationship. These more recent findings may be reflective of the changes in opioid prescribing and monitoring occurring over the past few years. Additionally, these results may indicate that a self-report measure for risk of opioid misuse is not sufficiently sensitive for determining future risk for opioid aberrancy, and further underscores the importance of UDT in patients receiving COT.
Several analyses have considered the economic impact of opioid-related aberrancy in patients with chronic pain. Although the current study did not examine economic variables, per se, a discussion of the costs associated with aberrancy and the failure to detect it should be presented. A 2005 study31 determined that annual direct health care costs for opioid abusers were more than eight times higher than those for non-abusers. Societal costs of prescription opioid abuse were estimated at over $55 billion annually in a 2011 study,32 which included health care costs, lost productivity, and criminal justice costs. A similar figure was obtained in another 2011 study of the costs of nonmedical use of prescription opioids.33 By 2013, this figure had risen to $72.5 billion annually.34 More recently, annual excess health care costs among individuals abusing prescription opioids who were privately insured were determined to range from $14,054 to $20,546.35 Additionally, the longer the duration of opioid aberrancy, the more likely that the user will progress to non-oral routes of administration,36 with non-oral use associated with even more severe morbidity and mortality.37 Risks and costs associated with progression to non-oral administration of prescription opioids may include transition to even more deadly illicit opioids38 as well as infectious disease transmission.39 Clearly, delay in identifying opioid aberrancy is not in anyone’s best financial interest – including that of patients, their physicians, or those who insure them. Finally, that such a low percentage of our urine samples required relatively expensive confirmatory testing by an external laboratory represents additional support for the cost-efficiency of the Boston PainCare UDT model.
Although the treatment of opioid misuse/abuse can be problematic, it is important to recognize that many of the emotional and behavioral issues that contribute to the aberrant use of opioids, non-prescribed prescription and illicit drugs can be addressed clinically. However, early intervention in cases of opioid aberrancy is likely to be easier, more successful, and less expensive to treat than longstanding opioid use disorders.29 Importantly, early and aggressive intervention in response to aberrancy and comorbid emotional and behavioral issues potentially results in the ability to continue opioid analgesics as a treatment for these patients, which is imperative at a time in which efficacious and cost-effective chronic pain treatment options appear to be dwindling. Some of the treatments of early stage opioid aberrancy that have empirical and/or consensus support include increased patient education regarding opioids,40 switching to abuse-deterrent formulations,41 use of multimodal rather than unimodal opioid pain management strategies,42 opioid rotation,43 and the provision of behavioral services.44
This study relies on data from a convenience sample with a single year study period collected at a community-based, tertiary care pain treatment facility that is particularly devoted to thorough and consistent opioid risk mitigation. The unique nature of our clinic's approach to opioid risk mitigation potentially poses both a strength and a limitation of our study. Had we simply discharged patients upon initial aberrancy as was done in earlier studies of "zero tolerance" clinics that were cited,7,10 it is likely that our overall rate of aberrancy on UDT would have been even lower. However, the reduced rates of opioid aberrancy that were identified in this study may reflect the risk reduction created by the delivery of education and psychological treatments commonly administered as an aspect of the clinic’s COT program. As such, the rate of aberrancy may be higher and the time needed to identify opioid aberrancy lower than those reported in this study than in facilities in which resources for education, behavioral intervention, and risk mitigation are more limited. Conversely, that the data were collected in a community-based facility can also be seen as a strength, as the study population was reflective of the type of complex patients treated in both specialty pain practices and primary care, thereby potentially increasing the generalizability of our results. For purposes of this study, we relied upon inconsistent UDTs as the objective indicator of aberrancy, and the COMM as the only risk measure. While the lack of significant relationship between these measures may indicate the inadequacy of self-reported measures in predicting aberrant behaviors, there may exist other more effective risk assessment tools that would help define the optimal use of UDT among subgroups receiving COT. Although the cutoffs of semi-quantitative UTDs utilized in the present study are more sensitive than are the dipstick immunoassays typically used in pain medicine,45 we acknowledge that in the best of all possible worlds, all testing would be done with even more sensitive technologies such as GC/MS. However, doing so would not be economically feasible, either for the clinic or its patients, and could potentially result in even lower frequencies of testing, thereby increasing the risk of identifying aberrancies at later stages.
Conclusions
Despite the inherent risks, the use of opioids in the management of chronic pain will likely continue given the limitations associated with the majority of pain treatment modalities and issues of insurance coverage. While a single aberrancy does not necessarily translate to an overdose death, the potential cost of treating substance abuse-related morbidities and the likelihood of a catastrophic outcome both increase the longer aberrant opioid behaviors remain undetected. The use of frequent drug testing remains a vital component in the mitigation of opioid-related morbidity and mortality as there remain inadequate means to predict and detect aberrant behavior among patients receiving such treatment.
Disclosure
Dr Schatman serves as a consultant to Kaleo Pharma and Quest Diagnostics. The authors report no other conflicts of interest in this work.
References
1. Gourlay DL, Heit HA, Almahrezi A. Universal precautions in pain medicine: a rational approach to the treatment of chronic pain. Pain Med. 2005;6(2):107–112. doi:10.1111/j.1526-4637.2005.05031.x
2. Manchikanti L, Manchukonda R, Pampati V, et al. Does random urine drug testing reduce illicit drug use in chronic pain patients receiving opioids? Pain Physician. 2006;9(2):123–129.
3. Starrels JL, Becker WC, Alford DP, et al. Systematic review: treatment agreements and urine drug testing to reduce opioid misuse in patients with chronic pain. Ann Intern Med. 2010;152:712–720. doi:10.7326/0003-4819-152-11-201006010-00004
4. Matteliano D, Chang YP. Describing prescription opioid adherence among individuals with chronic pain using urine drug testing. Pain Manag Nurs. 2015;16(1):51–59. doi:10.1016/j.pmn.2014.04.001
5. Wiseman LK, Lynch ME. The utility of universal urinary drug screening in chronic pain management. Can J Pain. 2018;2(1):37–47. doi:10.1080/24740527.2018.1425980
6. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain - United States, 2016. MMWR Recomm Rep. 2016;65(1):1–49. doi:10.15585/mmwr.rr6501e1
7. Pesce A, West C, Rosenthal M, et al. Illicit drug use in the pain patient population decreases with continued drug testing. Pain Physician. 2011;14(2):189–193.
8. Yee DA, Hughes MM, Guo AY, et al. Observation of improved adherence with frequent urine drug testing in patients with pain. J Opioid Manage. 2014;10(2):111–118. doi:10.5055/jom.2014.0200
9. Arthur JA, Edwards T, Lu Z, et al. Frequency, predictors, and outcomes of urine drug testing among patients with advanced cancer on chronic opioid therapy at an outpatient supportive care clinic. Cancer. 2016;122(23):3732–3739. doi:10.1002/cncr.30240
10. Knezevic NN, Khan OM, Beiranvand A, et al. Repeated quantitative urine toxicology analysis may improve chronic pain patient compliance with opioid therapy. Pain Physician. 2017;20(2S):S135–S145.
11. Owen GT, Burton AW, Schade CM, et al. Urine drug testing: current recommendations and best practices. Pain Physician. 2012;15(3 Suppl):ES119–ES133.
12. Argoff CE, Alford DP, Fudin J, et al. Rational urine drug monitoring in patients receiving opioids for chronic pain: consensus recommendations. Pain Med. 2018;19(1):97–117. doi:10.1093/pm/pnx285
13. Lubarsky DA, French MT, Gitlow HS, et al. Why money alone can’t (always) “nudge” physicians: the role of behavioral economics in the design of physician incentives. Anesthesiology. 2019;130(1):154–170. doi:10.1097/ALN.0000000000002373
14. Washington State Agency Medical Directors’ Group (AMDG) in collaboration with an expert advisory panel, actively practicing providers, public stakeholders, and senior state officials. Interagency Guideline on Prescribing Opioids for Pain 2015. Available from: http://www.agencymeddirectors.wa.gov/Files/2015AMDGOpioidGuideline.pdf.
15. Butler SF, Budman SH, Fernandez KC, et al. Development and validation of the current opioid misuse measure. Pain. 2007;130(1–2):144–156. doi:10.1016/j.pain.2007.01.014
16. Butler SF, Budman SH, Fanciullo GJ, et al. Cross validation of the current opioid misuse measure to monitor chronic pain patients on opioid therapy. Clin J Pain. 2010;26:770–776. doi:10.1097/AJP.0b013e3181f195ba
17. Vowles KE, McEntee ML, Julnes PS, et al. Rates of opioid misuse, abuse, and addiction in chronic pain: a systematic review and data synthesis. Pain. 2015;156(4):569–576. doi:10.1097/01.j.pain.0000460357.01998.f1
18. DiBenedetto DJ, Weed VF, Wawrzyniak KM, et al. The association between cannabis use and aberrant behaviors during chronic opioid therapy for chronic pain. Pain Med. 2018;19(10):1997–2008. doi:10.1093/pm/pnx222
19. Nikulina V, Guarino H, Acosta MC, et al. Patient vs provider reports of aberrant medication-taking behavior among opioid-treated patients with chronic pain who report misusing opioid medication. Pain. 2016;157(8):1791–1798. doi:10.1097/j.pain.0000000000000583
20. Bakhai S, Thilagar B, Reynolds JL, et al. Correlates of opiate misuse based on aberrant urine drug tests for patients on chronic opiate therapy in a safety-net, academic primary care clinic. J Opioid Manag. 2018;14(1):23–33. doi:10.5055/jom.2018.0426
21. Nugent SM, Yarborough BJ, Smith NX, et al. Patterns and correlates of medical cannabis use for pain among patients prescribed long-term opioid therapy. Gen Hosp Psychiatry. 2018;50:104–110. doi:10.1016/j.genhosppsych.2017.11.001
22. Lovejoy TI, Morasco BJ, Demidenko MI, et al. Reasons for discontinuation of long-term opioid therapy in patients with and without substance use disorders. Pain. 2017;158:526–534. doi:10.1097/j.pain.0000000000000796
23. Im JJ, Shachter RD, Oliva EM, et al. Association of care practices with suicide attempts in US Veterans prescribed opioid medications for chronic pain management. J Gen Intern Med. 2015;30:979–991. doi:10.1007/s11606-015-3220-y
24. Brennan PL, Del Re AC, Henderson PT, et al. Healthcare system-wide implementation of opioid-safety guideline recommendations: the case of urine drug screening and opioid-patient suicide- and overdose-related events in the Veterans Health Administration. Transl Behav Med. 2016;6(4):605–612. doi:10.1007/s13142-016-0423-7
25. Bailey RW, Vowles KE. Using screening tests to predict aberrant use of opioids in chronic pain patients: caveat emptor. J Pain. 2017;18(12):1427–1436. doi:10.1016/j.jpain.2016.12.014
26. McCarberg BH. Chronic pain: reducing costs through early implementation of adherence testing and recognition of opioid misuse. Postgrad Med. 2011;123(6):132–139. doi:10.3810/pgm.2011.11.2503
27. Ducoffe AR, York A, Hu DJ, et al. National Action Plan for adverse drug event prevention: recommendations for safer outpatient opioid use. Pain Med. 2016;17(12):2291–2304. doi:10.1093/pm/pnw106
28. Finkelman MD, Kulich RJ, Butler SF, et al. An investigation of completion times on the Screener and Opioid Assessment for Patients with Pain - revised (SOAPP-R). J Pain Res. 2016;9:1163–1171. doi:10.2147/JPR.S123454
29. Wasan AD, Butler SF, Budman SH, et al. Psychiatric history and psychologic adjustment as risk factors for aberrant drug-related behavior among patients with chronic pain. Clin J Pain. 2007;23(4):307–315. doi:10.1097/AJP.0b013e3180330dc5
30. Colasanti J, Lira MC, Cheng DM, et al. Chronic opioid therapy in people living with Human Immunodeficiency Virus: patients’ perspectives on risks, monitoring, and guidelines. Clin Infect Dis. 2019;68(2):291–297. doi:10.1093/cid/ciy452
31. White AG, Birnbaum HG, Mareva MN, et al. Direct costs of opioid abuse in an insured population in the United States. J Manag Care Pharm. 2005;11:469–479.
32. Birnbaum H, White A, Schiller M, et al. Societal costs of prescription opioid abuse, dependence, and misuse in the United States. Pain Med. 2011;12:657–667. doi:10.1111/j.1526-4637.2011.01075.x
33. Hansen RN, Oster G, Edelsberg J, et al. Economic costs of nonmedical use of prescription opioids. Clin J Pain. 2011;27(3):
34. Katz NP, Birnbaum H, Brennan MJ, et al. Prescription opioid abuse: challenges and opportunities for payers. Am J Manag Care. 2013;19:295–302.
35. Meyer R, Patel AM, Rattana SK, et al. Prescription opioid abuse: a literature review of the clinical and economic burden in the United States. Popul Health Manag. 2014;17:372–387. doi:10.1089/pop.2013.0098
36. Butler SF, Black RA, Serrano JM, et al. Characteristics of prescription opioid abusers in treatment: prescription opioid use history, age, use patterns, and functional severity. J Opioid Manag. 2010;6:
37. Butler SF, Black RA, Cassidy TA, et al. Abuse risks and routes of administration of different prescription opioid compounds and formulations. Harm Reduct J. 2011;8:29. doi:10.1186/1477-7517-8-30
38. Pollini RA, Banta-Green CJ, Cuevas-Mota J, et al. Problematic use of prescription-type opioids prior to heroin use among young heroin injectors. Subst Abuse Rehabil. 2011;2(1):173–180. doi:10.2147/SAR.S24800
39. Piggott DA, Muzaale AD, Mehta SH, et al. Frailty, HIV infection, and mortality in an aging cohort of injection drug users. PLoS One. 2013;8(1):e54910. doi:10.1371/journal.pone.0054910
40. Merlin JS, Young SR, Starrels JL, et al. Managing concerning behaviors in patients prescribed opioids for chronic pain: a Delphi study. J Gen Intern Med. 2018;33(2):166–176. doi:10.1007/s11606-017-4211-y
41. Alexander L, Mannion RO, Weingarten B, et al. Development and impact of prescription opioid abuse deterrent formulation technologies. Drug Alcohol Depend. 2014;138:1–6. doi:10.1016/j.drugalcdep.2014.02.006
42. Wiedemer NL, Harden PS, Arndt IO, et al. The opioid renewal clinic: a primary care, managed approach to opioid therapy in chronic pain patients at risk for substance abuse. Pain Med. 2007;8:573–584. doi:10.1111/j.1526-4637.2006.00254.x
43. Gatti A, Reale C, Luzi M, et al. Effects of opioid rotation in chronic pain patients: ORTIBARN study. Clin Drug Investig. 2010;30(suppl 2):39–47. doi:10.2165/1158413-S0-000000000-00000
44. Garland EL, Manusov EG, Froeliger B, et al. Mindfulness-oriented recovery enhancement for chronic pain and prescription opioid misuse: results from an early-stage randomized controlled trial. J Consult Clin Psychol. 2014;82(3):448–459. doi:10.1037/a0035798
45. Melanson SE, Ptolemy AS, Wasan AD. Optimizing urine drug testing for monitoring medication compliance in pain management. Pain Med. 2013;14(12):1813–1820. doi:10.1111/pme.12207
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.